

Abstract
Objectives:
The study aimed to investigate the impact of Coronavirus disease (COVID-19) on the roles of hospital and community pharmacists in the United Arab Emirates (UAE) and to assess how COVID-19 has affected their roles concerning medication dispensing and review, patient education, and telepharmacy services.
Methods:
This was a face-to-face questionnaire-based study. A convenient sampling technique was used to collect responses from 428 licensed community and hospital pharmacists across the UAE. The study tool is a structured questionnaire. Data were cleaned and analysed through SPSS Version 26.
Results:
In terms of medication dispensing practice, 314 (73.4%) and 210 (49.1%) of pharmacists reported an increase in the dispensing of over the counter (OTC) medicines and antibiotics after COVID-19, respectively. Of the pharmacists included in the study, 380 (88.8%) and 328 (76.6%) reported an elevation in the engagement in patient education and medication review after COVID-19, respectively. On the other hand, 247 (57.7%) and 179 (41.8%) of pharmacists reported that the frequency of their pharmaceutical interventions and physicians’ acceptance of those interventions increased after COVID-19, which was significantly associated (p=0.01) with pharmacists’ ability to intervene on the dosage regimen of COVID-19 patient.
Conclusion:
Pharmaceutical care in the UAE has evolved after COVID-19, particularly in the aspects of medications dispensing, telepharmacy, and patient-centered services..
Keywords: Pharmaceutical Care, COVID-19, Telepharmacy, Information technology tools, Medication dispensing, Medication review, Patient education
INTRODUCTION
It all started with the flare-up of multiple pneumonia cases due to a novel Coronavirus disease (COVID-19) in Wuhan city, China.1 The rapid spread of the virus led to several human losses and infection of over 216 million people up to this date.2 The huge pressure on the facilities and outbreak of COVID-19 has been declared not only as an emergency but also as a pandemic.3 The entire globe has been challenged to overcome the stress, imbalance, anxiety, and the spread of this virus.4 The unprecedented impact of COVID-19 on numerous sectors included the social, the economical, and first and foremost, the health care system.5 Thus, incomputable duties and new responsibilities have been put on many sectors of life, particularly, the healthcare system.6
New challenges were faced by the healthcare providers in every aspect of their professions. Yet, pharmacists played a pivotal role in maintaining the integrity and balance within the health care system by shouldering new responsibilities and adapting their practices to accommodate the increased demand in the medical services during the pandemic.7
Indeed, pharmaceutical care has been seriously affected by the global health crisis.8 This made pharmacists more dedicated to play key roles in its management and in supporting the healthcare system.8 Pharmacists in the community pharmacies act as the first point of contact between patients and the healthcare system, especially in times of global lockdown, thus, their work was very supportive for all; the public, health care professionals and the government.3
New regulations and measures were put by the governmental bodies and the international institutes regarding the delivery of services in hospital and pharmacy settings. These changes included maintaining at least one-meter distance, wearing protective garments, reducing direct contact, regular PCR testing, continuous sanitization, and the list goes on.
These circumstances called for the expansion of telemedicine and telepharmacy services in many countries. These services were imposed not only to improve the access to healthcare for COVID-19 confirmed cases or for possibly infected patients, but also to help applying the published regulations for social distancing, reduce pressure on hospitals and clinics, and minimizing the contact for the high-risk individuals including but not limited to, elderly, children and individuals with cardiovascular diseases.10
The provision of telepharmacy included services of virtual consultation and home delivery of medications. In the United Arab Emirates (UAE), telepharmacy was implicated in various facilities, being one of the first countries in the Middle East to provide such a service. For that purpose, the department of health (DOH) has published standards on delivery of pharmacy medications by February 2020.11 In addition, the first licensed and approved mobile application for health care products was made available all across the UAE, namely, “ 800 pharmacy” which provides 24/7 delivery of over-the-counter (OTC) products, supplements and prescription only medications (POM).12 Telepharmacy was seen to not only increase patients access to pharmaceutical care, but also to reduce dispensing errors including both prescription-related errors and pharmacist counseling errors.13
Pharmaceutical care, as defined by the board of the Pharmaceutical Care Network Europe (PCNE), is the pharmacist’s contribution to the care of individuals in order to optimize medicine use and improve health outcomes.14 The new regulations concerning social distancing, in addition to the introduction of remote dispensing practices, have influenced a changed in the nature of the pharmaceutical care to be more patient oriented. A literature review conducted by Marília B. Visacri et al.,15 found that pharmacists’ main responsibility during the pandemic was to contribute through providing drug information to health care professionals and deliver adequate patient counseling and education. However, changes in the pharmaceutical care after COVID- 19 have not been studied adequately in the UAE. In fact, there are few studies that examined the changes in pharmacy practice after COVID-19. Our hypothesis is that COVID-19 has triggered fundamental transformation in the trends of medical practice, especially pharmacy given that pharmacists are the most accessible healthcare workers.16 Noticeably, this transformation may be not entirely due to COVID-19, but also other factors such as the need for patient-centered pharmacy practice to improve the quality of healthcare and reduce cost.17 Thus, we aim in our study to investigate the impact of COVID-19 on the role that hospital and community pharmacists can play in the UAE, focusing on medication dispensing and review, patient education, and telepharmacy services. This face-to-face interview structured based study was designed in a way that can explore this impact on the pharmacists’ role in a representative sample size of hospital and community pharmacists across different emirates in the UAE.
METHODOLOGY
Study design and sampling technique
This study was a face-to-face interview- based study conducted over three months (from December 2020, to March 2021) on a sample of hospital and community pharma cists across the UAE. With the presence of 110,000 licensed pharmacist in the UAE, the calculated minimum recommended sample size was 383 pharmacists (Calculation was done using Raosoft sample size calculator, with 5% margin of error, 95% confidence level and 50% response distribution).18 The study population included only pharmacists (n= 428) who have a valid pharmacy license in the UAE and who were consented/agreed to participate in the study. Pharmacists who were practicing for less than 6 months, those who were on training duty, or who were participating in another study were excluded. Additionally, we excluded pharmacists who were recruited after COVID-19 because they could not be able to anticipate the change in the practice before and after the pandemic. The study received the required ethical approvals from the Research Ethics Committee (REC) at Al-Ain University (AAU-REC-B3, Dec, 2020). A convenience sampling technique was used in this study.
Study tool
The study tool was a structured questionnaire, comprising of five major parts: First, sociodemographic questions. Second, questions about the medications dispensing practice of pharmacists after COVID-19. The participants answered multiple-choice questions with the choices: increased, decreased or the same as before, to describe the rate of medications in general, OTC, vitamins and antibiotics. Third, three questions about pharmacists’ role in patient counselling and education, where the responder had to choose the counseling areas and topics mostly discussed with patients during this period. Fourth, questions about pharmacists’ interventions and medication review. In this section, pharmacists had to describe their interventions upon prescriptions, physicians’ acceptance of their interventions and occurrence of medication related problems, with increased, decreased or the same as before COVID-19. The last fifth part, questions assessing to what extent pharmacy automation has been affected by COVID-19, specifically, remote dispensing of medications, remote filling of prescriptions, home delivery and virtual consultation.
Characteristics of participant’s
The following information was addressed: Age, gender, years of experience, place of work, occupation and education.
Validation and reliability testing of the study questionnaire
The questionnaire implemented in our study is pre-validated. Nevertheless, we tailored it to suit the aims of our study and the culture of the UAE. After few minor modifications, we invited three experts to revalidate the survey using a panel discussion technique, in which each expert grade each question of the survey from 0 to 10 and then we calculated the average score for each questionnaire item. The experts asked for some modifications and suggested adding an operational definition table to the manuscript. Additionally. we conducted a preliminary pilot testing to ensure understandability and practicality of the questionnaire. We calculated Cronbach’s alpha using SPSS to test the internal consistency of the survey items. Alpha coefficient was 0.76, which reflects acceptable degree of consistency.
Inclusion and exclusion criteria
Pharmacists (hospital/community) who have a valid pharmacy license in the UAE were included. The exclusion criteria were pharmacists who did not have a valid license, pharmacy technicians or trainees, and those who refused to participate.
There are several operational definitions adopted for this study were summarized in Table 1.
Table 1.
| Term | Definition |
|---|---|
| Antibiotics | Effective antibacterial agents required for preventive and curative measures, protecting patients from potentially fatal diseases and infections. |
| Medication Review | Medication review is a structured evaluation of a patient’s medicines with the aim of optimizing medicines use and improving health outcomes. |
| Medication Related Problems (MRPs) | A drug therapy problem is any undesirable event experienced by a patient that involves, or is suspected to involve, drug therapy, and that interferes with achieving the desired goals of therapy and requires professional judgment to resolve. |
| OTC (over the counter) medications | A medicine or device that can be bought without a doctor’s order or prescription. |
| Quarantine | Restriction of the activities and movement of well persons or animals who may have been exposed to a case of communicable disease. |
| Self-Isolation | A method used by an individual to be kept apart in seclusion from others for a period of time in an attempt to minimize the risk of transmission of an infectious disease. |
| Symptoms | * Subjective evidence of disease perceived by the patient. * An indication that a person has a condition or disease. |
| Telepharmacy | The use of electronic information and communication technologies to provide and support health care when distance separates the participants. |
Data collection
The final version of the questionnaire was written in English and Arabic languages and included closed-ended questions that covered different study aspects. The process of data collection was carried out over several stages. First, the data collectors were trained by the main investigator on completing and finalizing the study survey, and distributing the questionnaire. Second, the data collection team comprising three research associates approached eligible pharmacists in different hospital and community pharmacies in the UAE (n=698) and asked for their consent after briefing them about the study purposes and the estimated time needed to complete the questionnaire. Third, participants were given the choice to complete the questionnaire by themselves or by the research associates. The data collectors stayed with the participants while they are filling the questionnaire to answer any questions or clarify any confusion. Finally, the participants were informed about the confidentiality and anonymity of policy applied.
Statistical analysis
Data sets were gathered and entered to an excel sheet, which was imported to the Statistical Package for Social Science (SPSS) version 26 (IBM Corporation, Armonk, NY, USA) for data analysis. We used Chi-square test and independent t test to measure differences between categorical and continuous variables, respectively. Errors bars with 95% confidence interval were also constructed (p<0.05 was considered an indicator of significant results).
RESULTS
Of the 698 pharmacists approached, 428 (61.3%) completed the questionnaire, of which 339 (79.2%) work in community settings, more than half (59.8%) were females, around one-third (30.1%) had from 6 to 10 years of experience, and the vast majority (81.3%) aged between 24 and 45 years (Table 2). More than half (54.9%) of recruited pharmacists were working in Abu Dhabi region. Around one-third of the pharmacists were working in Ras al-Khaimah, Sharjah, Ajman, Fujeirah and Umm al-Quwain. Of the 428 pharmacists who completed the questionnaire, 330 (77.1%) practiced teleconsultation, 232 (54.2%) filled prescriptions remotely during COVID-19, and 197 (46.0%) altered at least a prescription or a dosage regimen for a COVID-19 patient. There was a significant difference in pharmacists’ level of education across those who practiced teleconsultation during COVID-19 and those who did not. Differences in other sociodemographic characteristics did not lead to a significant difference in the proportion of pharmacists who practiced teleconsultation.
Table 2.
Sociodemographic information of pharmacists included in the study N = 428)
| Parameters | Total, n (%) | Practice teleconsultation, n (%) 330 (77.1%) | Do not practice teleconsultation, n (%) 98 (22.9%) | P value | |
|---|---|---|---|---|---|
| Gender | Female | 256 (59.8) | 195 (76.2) | 61 (23.8) | 0.576 |
| Male | 172 (40.2) | 135 (78.5) | 37 (21.5) | ||
| Age | 22-24years | 69 (16.1) | 59 (85.5) | 10 (14.5) | 0.096 |
| 25-45years | 348 (81.3) | 263 (75.6) | 85 (24.4) | ||
| > 45years | 11 (2.6) | 8 (72.7) | 3 (27.3) | ||
| Years of experience | <2 | 66 (15.4) | 50 (75.8) | 16 (24.2) | 0.236 |
| 2-5 | 168 (39.3) | 135 (80.4) | 33 (19.6) | ||
| 6-10 | 129 (30.1) | 97 (75.2) | 32 (24.8) | ||
| >10 | 65 (15.2) | 51 (78.4) | 14 (21.6 | ||
| Education | Bachelor of science | 359 (83.9) | 286 (79.7) | 73 (20.3) | 0.02 |
| Doctor of Pharmacy (MSc) | 52 (12.1) | 33 (63.5) | 19 (36.5) | ||
| Diploma | 16 (3.7) | 10 (62.5) | 6 (37.5) | ||
| Doctorate | 1 (0.2) | 1 (100.0) | 0 (0.0) | ||
| Place of work | Capital region (Abu Dhabi) | 235 (54.9) | 183 (77.9) | 52 (22.1) | 0.498 |
| Northern Region (Ras al-Khaimah, Sharjah, Ajman, Fujeirah and Umm al-Quwain) | 142 (33.2) | 110 (77.5) | 32 (22.5) | ||
| Central Region (Dubai) | 51 (11.9) | 36 (70.6) | 15 (29.4) | ||
| Setting type | Community | 339 (79.2) | 264 (77.9) | 75 (22.1) | 0.457 |
| Hospital | 89 (20.2) | 66 (74.2) | 23 (25.8) | ||
Data are presented as numbers (n) and percentages (%). Bold p values are significant results; p< 0.05. Pearson’s chi-squared test was used to measure differences in demographic information across pharmacists who practiced teleconsultation and those who did not.
In terms of medication dispensing practice, 314 (73.4%) and 210 (49.1%) of pharmacists reported an increase in the dispensing of OTC medicines and antibiotics after COVID-19, respectively (Table 3). Moreover, there were statistically significant differences in the rate of OTC medicines and antibiotics dispensing across pharmacists who altered at least a prescription or a dosage regimen for a COVID-19 patients and those who did not, whereas these rates were similar (no significant association) across pharmacists who filled prescriptions remotely and those who did not.
Table 3.
Assessment of changes to medication dispensing and patient safety practices after COVID-19 (N = 428)
| Parameters | Altered at least a prescription or a dosage regimen for a COVID-19 patient | Filled prescriptions remotely | ||||
|---|---|---|---|---|---|---|
| Yes, n (%) Total = | No, n (%) Total= | P value | Yes, n (%) Total = | No, n (%) Total = | P value | |
| Medication dispensing | ||||||
| The rate of medication dispensing after COVID-19. | 0.084 | 0.127 | ||||
| Increased | 132 (55.7%) | 105 (44.3%) | 152 (64.1%) | 85 (35.9%) | ||
| Decreased | 65 (45.8%) | 77 (54.2%) | 80 (56.3%) | 62 (43.7%) | ||
| The rate of OTC medicines dispensing after COVID-19. | 0.006 | 0.076 | ||||
| Increased | 174 (55.4%) | 140 (44.6%) | 195 (62.1%) | 119 (37.9%) | ||
| Decreased | 27 (35.5%) | 49 (64.5%) | 37 (48.7%) | 39 (51.3%) | ||
| The rate of vitamins dispensing after COVID-19. | 0.073 | 0.893 | ||||
| Increased | 208 (50.6%) | 203 (49.4%) | 246 (59.9%) | 165 (40.1%) | ||
| Decreased | 5 (100%) | 0 (0%) | 3 (60%) | 2 (40%) | ||
| The rate of antibiotics dispensing after COVID-19. | 0.001 | 0.141 | ||||
| Increased | 131 (62.4%) | 79 (37.6%) | 136 (64.8%) | 74 (35.2%) | ||
| Decreased | 38 (35.8%) | 68 (64.2%) | 60 (56.6%) | 46 (43.4%) | ||
| Patient safety | ||||||
| Engagement in patient education after COVID-19. | 0.001 | 0.153 | ||||
| Increased | 195 (51.3%) | 185 (48.7%) | 219 (62%) | 134 (38%) | ||
| Decreased | 7 (25.9%) | 20 (74.1%) | 15 (55.6%) | 12 (44.4%) | ||
| Engagement in medication review after COVID-19. | 0.072 | 0.723 | ||||
| Increased | 178 (54.3%) | 150 (45.7%) | 200 (61%) | 128 (39%) | ||
| Decreased | 9 (37.5%) | 15 (62.5%) | 14 (58.3%) | 10 (41.7%) | ||
| Pharmaceutical intervention on prescriptions after COVID-19. | 0.563 | 0.001 | ||||
| Increased | 157 (63.6%) | 90 (36.4%) | 167 (67.6%) | 80 (32.4%) | ||
| Decreased | 11 (24.4%) | 34 (75.6%) | 17 (37.8%) | 28 (62.2%) | ||
| The rate of physicians’ acceptance of pharmacists’ interventions after COVID-19. | 0.001 | 0.008 | ||||
| Increased | 115 (64.2%) | 64 (35.8%) | 122 (68.2%) | 57 (31.8%) | ||
| Decreased | 19 (42.2%) | 26 (57.8%) | 20 (28.6%) | 50 (71.4%) | ||
| The rate of MRPs after COVID-19. | 0.001 | 0.203 | ||||
| Increased | 102 (64.2%) | 57 (35.8%) | 102 (64.2%) | 57 (35.8%) | ||
| Decreased | 12 (27.3%) | 32 (72.7%) | 21 (41.2%) | 30 (58.8%) | ||
| Patient access to pharmaceutical care after COVID-19? | 0.138 | 0.012 | ||||
| Increased | 178 (53.5%) | 155 (46.5%) | 209 (62.8%) | 124 (37.2%) | ||
| Decreased | 27 (43.5%) | 35 (56.5%) | 36 (58.1%) | 26 (41.9%) | ||
Those who answered same as before were excluded from this analysis. Bold p values indicate significant results p< 0.05. Data are presented as numbers (n) and percentages (%).
In terms of patient safety (Table 3), 380 (88.8%) and 328 (76.6%) of the pharmacists included in the study reported that their engagement in patient education and medication review increased after COVID-19, respectively. To a lesser extent, 247 (57.7%) and 179 (41.8%) of pharmacists conveyed that the frequency of their pharmaceutical interventions and physicians’ acceptance of those interventions increased after COVID-19, respectively. Additionally, 159 (37.1%) and 333 (77.8%) of pharmacists reported that the rate of MRPs and patient access to pharmaceutical care increased after COVID-19. There were statistically significant differences in the engagement in patient education and in the rate of physicians’ acceptance of pharmacists’ interventions after COVID-19 across pharmacists who altered at least a prescription or a dosage regimen for a COVID-19 patient and those who did not. Furthermore, there were statistically significant differences in the rate of pharmaceutical interventions, physicians’ acceptance, and patient access to pharmaceutical care across pharmacists who filled prescriptions remotely and those who did not.
The findings of this study showed that preventive measures (97.9%), self-isolation and quarantine (93.7%), and dietary supplement (79.9%) were the top three counseling areas that pharmacists have been engaged in after COVID-19 (Figure 1).
Figure 1.
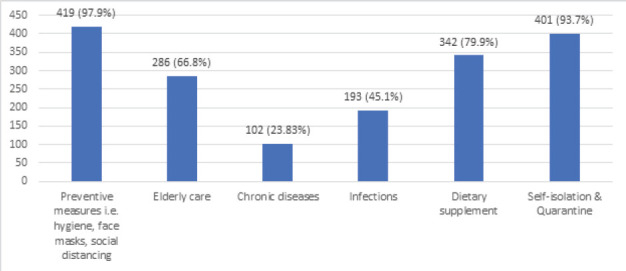
Counseling areas that pharmacists have been engaged in after COVID-19.
We tested whether the mean years of experience varied across the proportion of access to pharmaceutical care, the occurrence of MRPs, and the practice of remote medication dispensing (Figure 2). Our findings showed that among pharmacists who were working in community pharmacies (Figure 2a), there was a significant difference in the mean years of experience among pharmacists who reported a rise in the access of patients to pharmaceutical care compared to those who reported a reduction. Additionally, among pharmacists who did not report alteration of prescriptions for their patients (Figure 2b), there was a significant difference in the mean years of experience across pharmacists who reported an increase in the access of patients to pharmaceutical care and those who reported a decrease in the access of patients. However, the mean of years of experience was similar (no significant association) across pharmacists who reported an increase in the rate of MRPs after COVID-19 and those who reported decrease or same as before (Figure 2d), and across pharmacists who reported remote medication dispensing and those who did not (Figure 2e).
Figure 2.
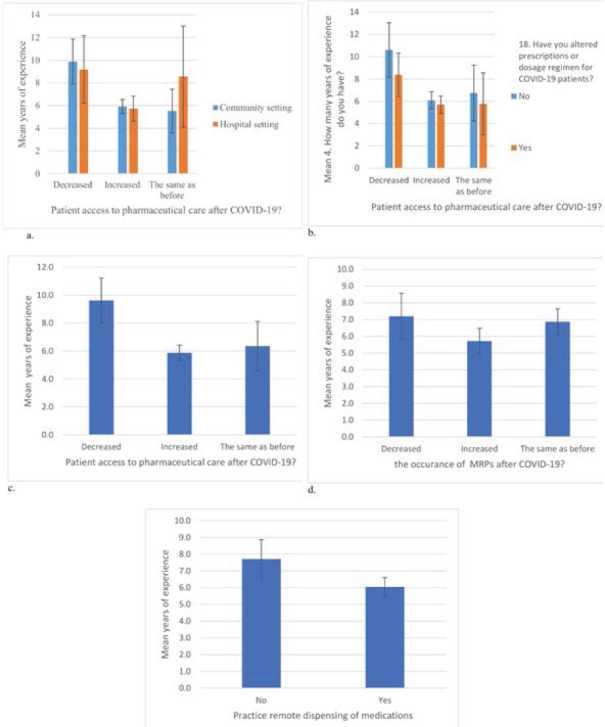
The impact of years of experience on pharmaceutical care changes after COVID-19 in UAE. Errors bars reflect 95% CI.
DISCUSSION
The current pandemic has impacted all aspects of life and caused substantial alteration to healthcare services worldwide.21 Although pharmaceutical care has been considerably evolved to alleviate the pandemic consequences and reduce the burden on healthcare systems in many parts of the world, 21 little is known about what actually has changed in pharmaceutical care after COVID-19 in the UAE. Therefore, this study aimed to investigate the impact of COVID-19 on the role of UAE community and hospital pharmacists in patient safety, medication dispensing, and public health.
The findings of this study indicate that a significant proportion of hospital and community pharmacists in the UAE used information technology tools to provide virtual consultations, remote filling of prescriptions, and home delivery of medications. These information technology tools include video conferencing software and mobile applications. This was in line with the findings of a previous study conducted in the UAE to evaluate telepharmacy services in community pharmacies.23 They found that remote pharmaceutical care could reduce medication errors and increase patient access to care. These findings could be attributed to the efforts made by the UAE health officials during the pandemic, which include unlimited support and guidance to all governmental and private healthcare facilities including pharmacies to ensure mitigating the transmission of COVID-19, while maintaining healthcare services available for all individuals. For instance, from the early beginnings of this pandemic, the UAE issued regulations to facilitate the delivery of healthcare services remotely in community and hospital pharmacies.24 Additionally, pharmacists were continuously updated about the best infection control and prevention practices to counteract the spreading of the pandemic.25
In the current study, a significant number of pharmacists reported an increase in the dispensing of medications such as antibiotics. Our findings were consistent with Michael A. Campitelli et al.,26 who reported a considerable increase in the dispensing and use of medications with the potential of adverse events. These findings could be explained by the huge number of misinformation and rumors regarding COVID-19 medications, which led to uncontrolled self-medication, excessive-buying, and misuse of medications.27
The findings of our study also demonstrate that dispensing of antibiotics was significantly linked to pharmacists’ interventions or alterations to patients’ prescriptions. However, filling prescriptions remotely was not significantly associated with the rate of medication dispensing. These findings are consistent with previous studies that indicated a sharp increase in antibiotic dispensing and use during the pandemic.28,29
Our findings show that pharmacists’ engagement in patient-centered roles, such as patient education and medication review has increased. Additionally, pharmacists included in our study reported that physicians’ acceptance of their interventions increased after the pandemic, and this was significantly associated with pharmacists’ ability to intervene on the dosage regimen of COVID-19 patient. Our findings were consistent with several authors’ findings, which indicated that both hospital and community pharmacists have contributed to minimizing the spread of the virus by improving health promotion and public health awareness.30-32 This was achieved by counselling patients on COVID-19 and non-COVID-19-related symptoms and minor diseases, hence reducing the burden on physicians who felt overwhelmed during the pandemic.33
In this study, pharmacists working in community settings, who had less years of experience, were more likely to report an increase in access to pharmaceutical care, whereas, in hospital settings, variation in years of experience was not a significant factor in determining access to care. This could be attributed to the ability and skills of younger pharmacists in using information technology tools and being early adapters to the technological changes. The factor of years of experience did not impact access to care, which can be contributed to the facts that hospital pharmacists in the UAE are more likely to be trained on using information technology tools. Additionally, most hospitals have a unified or consistent work process in terms of remote healthcare services. Therefore, pharmacy managers and stakeholders should design and implement not only new technologies into pharmacy practice, but also training programs to enhance pharmacists’ skills.
Our findings indicated that the most common counseling areas that pharmacists have been engaged in after COVID-19 were preventive measures, self-isolation and quarantine, and dietary supplement. This highlights the evolved role of pharmacists and their contribution to the emergency response. The published literature showed consistent results.7,34
CONCLUSION
To sum up, our study was conducted in the UAE and included both hospital and community pharmacists from different geographic regions. We found that pharmaceutical care in the UAE has changed after COVID-19 in terms of medication dispensing, patient-centered roles, and remote services. This demonstrates the substantial position of pharmacists in pandemic preparedness and disaster management. Nonetheless, the change in pharmaceutical care needs intensive monitoring and evaluation to prevent the occurrence of adverse drug events and medication errors. Further studies to evaluate the change in the roles of hospital and community pharmacists separately can provide a better understanding of the nature and magnitude of pharmaceutical care future in the UAE.
Study limitations and future directions
The findings of this study should be discussed in terms of its limitations. First, the self-reporting nature of the study may incorporate bias into the findings, which cannot be eliminated without a direct observation of pharmacy daily practice in the UAE. However, given the limited resources we had, conducting a direct observational study was not feasible. Second, because pharmacists in the UAE have diverse educational backgrounds and different experiences, it was difficult to link the changes in pharmaceutical care to the level or the nature of pharmacy education. Therefore, we recommend further research to track educational factors that could attribute to pharmacists’ behavior during pandemics. Third, because some of the responses may pertain to each pharmacist experience and many not reflect pharmacy practice in the country, we have some concerns regarding the generalizability of the study findings. However, these concerns were addressed by validity and reliability measures prior to survey distribution. Fourth, this study did not address the impact of the pandemic on the rate, types, and severity of medication dispensing errors. Finally, given the nature of sampling of this study, there is a great chance for recall and selection bias in data collection. While we cannot rule out entirely the possibility of these events, we instructed data collectors to approach pharmacists who did not have any previous contact with. Nonetheless, these limitations could be utilized by research groups in the UAE for future investigations.
What is already known about the subject
Pharmacists’ roles have been evolved after the outbreak of Coronavirus disease (COVID-19).
New challenges to pharmacy practice have emerged after the outbreak of COVID-19.
Pharmacy regulations have been transformed in many countries after the outbreak of COVID-19.
What this study adds
The dispensing patterns of over-the-counter drugs and antibiotics have been changed after the outbreak of COVID-19, which needs monitoring and controlling.
The pharmacists’ interventions on patients’ dose regimen have been increased after the pandemic.
Community pharmacists are engaged more in patient-centered roles after the outbreak of COVID-19.
A rapid advancement in the delivery of remote pharmaceutical services has been found.
DECLARATIONS
Authors statement
ZK, SM, RKH.: Proposal writing, Conceptualization and study design development, data collection, data analysis, results’ interpretation, manuscript drafting. AZM: study design development, survey securing, manuscript drafting and review, data analysis and critical appraisal. YA: Manuscript-drafting and review, study design development, data analysis, and literature review,
Funding
The authors of this research received no funding.
Declaration of competing interest
The authors have no relevant financial or non-financial interests to disclose.
Ethics approval
The study received the required ethical approvals from the Research Ethics Committee (REC) at Al-Ain University (AAU-REC-B3, Dec, 2020). A random convenience sampling technique was used in this study.
ABBREVIATIONS
UAE: United Arab Emirates, COVID-19: Coronavirus disease, PCNE: Pharmaceutical Care Network Europe, DOH: Department of health, OTC: Over-the-counter medications, POM: Prescription only medications, MRPs: Medication Related Problems
Acknowledgements
We would like to thank Al Ain University for facilitating our research project.
Contributor Information
Zelal Kharaba, Department of Clinical Sciences, AAU Health and Biomedical Research Center, College of Pharmacy, Al Ain University, Abu Dhabi, UAE. zelal.kharaba@aau.ac.ae.
Sedq A. Moutraji, Department of Clinical Sciences, College of Pharmacy, Al Ain University, Abu-Dhabi, UAE. Sedq.moutraji@hotmail.com
Rama A. Al Khawaldeh, Department of Clinical Sciences, College of Pharmacy, Al Ain University, Abu-Dhabi, UAE. Ramalkhawaldeh@gmail.com.
Yassen Alfoteih, Department of Dental Surgery, City University College of Ajman, Ajman, UAE. alfoteih@gmail.com.
Ahmad Z. Al Meslamani, Department of Clinical Sciences, AAU Health and Biomedical Research Center, College of Pharmacy, Al Ain University, Abu Dhabi, UAE. amaslamanie1095@gmail.com.
References
- 1.Novel coronavirus (2019-nCoV) 2021 [Google Scholar]
- 2.COVID Live Update:Cases and Deaths from the Coronavirus - Worldometer. 2021 [Google Scholar]
- 3.Team EE. Note from the editors:World Health Organization declares novel coronavirus (2019-nCoV) sixth public health emergency of international concern. Eurosurveillance. 2020;25(5):200131e. doi: 10.2807/1560-7917.ES.2020.25.5.200131e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wang C, Tee M, Roy AE, et al. The impact of COVID-19 pandemic on physical and mental health of Asians:A study of seven middle-income countries in Asia. PLoS One. 2021;16(2):e0246824. doi: 10.1371/journal.pone.0246824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mofijur M, Fattah MR, Alam MA, et al. Impact of COVID-19 on the social, economic, environmental and energy domains:Lessons learnt from a global pandemic. Sustain Prod Consum. 2021;26:343–359. doi: 10.1016/j.spc.2020.10.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ghibu S, Juncan AM, Rus LL, et al. The Particularities of Pharmaceutical Care in Improving Public Health Service during the COVID-19 Pandemic. Int J Environ Res Public Health. 2021;18(18):9776. doi: 10.3390/ijerph18189776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee DH, Watson KE, Al Hamarneh YN. Impact of COVID-19 on frontline pharmacists'roles and services in Canada:The INSPIRE Survey. Can Pharm J. 2021;154(6):368–373. doi: 10.1177/17151635211028253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ayati N, Saiyarsarai P, Nikfar S. Short and long term impacts of COVID-19 on the pharmaceutical sector. J Pharm Sci. 2020;28(2):799–805. doi: 10.1007/s40199-020-00358-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nadeem MF, Samanta S, Mustafa F. Is the paradigm of community pharmacy practice expected to shift due to COVID-19? Research in social &administrative pharmacy:RSAP. 2021;17(1):2046–2048. doi: 10.1016/j.sapharm.2020.05.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.DOH. DOH Standard on Tele-Medicine. 2020 [Google Scholar]
- 11.800 Pharmacy.
- 12.Department of Health AD. Remote Healthcare Platform. https://doh.gov.ae/covid-19/Remote-Healthcare-Platform. 2020. [DOI]
- 13.Allemann SS, Van Mil JWP, Botermann L, et al. Pharmaceutical care:The PCNE definition 2013. Int J Clin Pharm. 2014;36(3):544–55. doi: 10.1007/s11096-014-9933-x. [DOI] [PubMed] [Google Scholar]
- 14.Visacri MB, Figueiredo IV, Lima T. Role of pharmacist during the COVID-19 pandemic:A scoping review. Res Soc Adm Pharm. 2021;17(1):1799–1806. doi: 10.1016/j.sapharm.2020.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ibrahim OM, Ibrahim RM, Ibrahim YA, et al. Shedding the light on Pharmacists'roles during COVID-19 global pandemic. Saudi Pharm J. 2022;30(1):14–27. doi: 10.1016/j.jsps.2021.12.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jordan D, Guiu-Segura JM, Sousa-Pinto G, et al. How COVID-19 has impacted the role of pharmacists around the world. Farm Hosp. 2021;45(2):89–95. doi: 10.7399/fh.11652. [DOI] [PubMed] [Google Scholar]
- 17.Sample Size Calculator by Raosoft, Inc [Google Scholar]
- 18.Cipolle RJ, Strand LM, Morley PC. Drug Therapy Problems. in Pharmaceutical Care Practice:The Patient-Centered Approach to Medication Management Services. 2012 [Google Scholar]
- 19.Al-Azzam SI, Alzoubi KH, AbuRuz S, et al. Drug-related problems in a sample of outpatients with chronic diseases:a cross-sectional study from Jordan. Ther Clin Risk Manag. 2016;12:233–9. doi: 10.2147/TCRM.S98165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Quteimat OM, Amer AM. SARS-CoV-2 outbreak:How can pharmacists help? Res Soc Adm Pharm. 2021;17(2):480–482. doi: 10.1016/j.sapharm.2020.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yimenu DK, Demeke CA, Kasahun AE. Impact of COVID-19 on Pharmaceutical Care Services and the Role of Community Pharmacists:A Multi-Center Cross-Sectional Study in Ethiopia. SAGE Open Nurs. 2021;7:23779608211025804. doi: 10.1177/23779608211025804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Department of Health AD. Remote Healthcare Platform. https://doh.gov.ae/covid-19/Remote-Healthcare-Platform. 2020.
- 23.Department of Health AD. Latest information on Coronavirus COVID-19. https://www.doh.gov.ae/covid-19. 2020.
- 24.Campitelli MA, Bronskill SE, Maclagan LC, et al. Comparison of Medication Prescribing Before and After the COVID-19 Pandemic Among Nursing Home Residents in Ontario, Canada. JAMA Netw Open. 2021;4(8):e2118441. doi: 10.1001/jamanetworkopen.2021.18441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hashmi FK, Atif N, Malik UR, et al. Misinformation in Wake of the COVID-19 Outbreak:Fueling Shortage and Misuse of Lifesaving Drugs in Pakistan. Disaster Med Public Health Prep. 2021;15(4):e32–e33. doi: 10.1017/dmp.2020.400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Knight BD, Shurgold J, Smith G, et al. The impact of COVID-19 on community antibiotic use in Canada:an ecological study. Clin Microbiol Infect. 2022;28(3):426–432. doi: 10.1016/j.cmi.2021.10.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gillies MB, Burgner DP, Ivancic L, et al. Changes in antibiotic prescribing following COVID-19 restrictions:Lessons for post-pandemic antibiotic stewardship. Br J Clin Pharmacol. 2022;88(3):1143–1151. doi: 10.1111/bcp.15000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Aruru M, Truong HA, Clark S. Pharmacy Emergency Preparedness and Response (PEPR):a proposed framework for expanding pharmacy professionals'roles and contributions to emergency preparedness and response during the COVID-19 pandemic and beyond. Res Soc Adm Pharm. 2021;17(1):1967–1977. doi: 10.1016/j.sapharm.2020.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cadogan CA, Hughes CM. On the frontline against COVID-19:Community pharmacists'contribution during a public health crisis. Res Soc Adm Pharm. 2021;17(1):2032–2035. doi: 10.1016/j.sapharm.2020.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hedima EW, Adeyemi MS, Ikunaiye NY. Community Pharmacists:On the frontline of health service against COVID-19 in LMICs. Res Social Adm Pharm. 2021;17(1):1964–1966. doi: 10.1016/j.sapharm.2020.04.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Linzer M, Stillman M, Brown R, et al. Preliminary Report:US Physician Stress During the Early Days of the COVID-19 Pandemic. Mayo Clin Proceedings Innov Qual Outcomes. 2021;5(1):127–136. doi: 10.1016/j.mayocpiqo.2021.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.El Bizri L, Jarrar LG, Ali WKA, et al. The role of community pharmacists in increasing access and use of self-care interventions for sexual and reproductive health in the Eastern Mediterranean Region:examples from Egypt, Jordan, Lebanon and Somalia. Heal Res Policy Syst. 2021;19(Suppl 1):49. doi: 10.1186/s12961-021-00695-0. [DOI] [PMC free article] [PubMed] [Google Scholar]