

Abstract
Background
Augmented reality (AR) is an interactive technology that uses persuasive digital data and real-world surroundings to expand the user's reality, wherein objects are produced by various computer applications. It constitutes a novel advancement in medical care, education, and training.
Objective
The aim of this work was to assess how effective AR is in training medical students when compared to other educational methods in terms of skills, knowledge, confidence, performance time, and satisfaction.
Methods
We performed a meta-analysis on the effectiveness of AR in medical training that was constructed by using the Cochrane methodology. A web-based literature search was performed by using the Cochrane Library, Web of Science, PubMed, and Embase databases to find studies that recorded the effect of AR in medical training up to April 2021. The quality of the selected studies was assessed by following the Cochrane criteria for risk of bias evaluations.
Results
In total, 13 studies with a total of 654 participants were included in the meta-analysis. The findings showed that using AR in training can improve participants' performance time (I2=99.9%; P<.001), confidence (I2=97.7%; P=.02), and satisfaction (I2=99.8%; P=.006) more than what occurs under control conditions. Further, AR did not have any effect on the participants’ knowledge (I2=99.4%; P=.90) and skills (I2=97.5%; P=.10). The meta-regression plot shows that there has been an increase in the number of articles discussing AR over the years and that there is no publication bias in the studies used for the meta-analysis.
Conclusions
The findings of this work suggest that AR can effectively improve performance time, satisfaction, and confidence in medical training but is not very effective in areas such as knowledge and skill. Therefore, more AR technologies should be implemented in the field of medical training and education. However, to confirm these findings, more meticulous research with more participants is needed.
Keywords: augmented reality, medical, training, virtual, meta-analysis
Introduction
Augmented reality (AR) is an interactive technology that uses persuasive digital data and real-world surroundings to expand the user's reality, wherein objects are produced by various computer applications [1,2]. Its use has become a widely debated topic among the medical community and has resulted in fertile ground for new types of research [3]. As a result, the health care sector and policy makers have been immediately able to realize the benefits of applying AR technologies, with education and training being noticeable applications of AR in medical settings [4-6]. However, since AR technologies enable learners to interact and visualize in 3D representations, medical professionals must have a vast amount of technological knowledge to efficiently adapt AR in practice [4,7,8]. Apart from the enormous benefits of AR for medical professionals, AR is also emerging as a useful guide for patient education and training, allowing physicians to clarify different surgical procedures and the functions of certain medications for patients and to explain new therapies in a more visual way [9-12]. Furthermore, AR can significantly improve a patient’s experience and advance knowledge on complex issues, and these benefits contribute and lead to better health outcomes [6].
There are many applications of AR in medical settings. Kamphuis et al [13], for example, reported that AR has reached a mature level of use in the field of anatomical engineering, for various technologies, and in physiological training. Further, surgical training has also been revolutionized by AR. Although integrating virtual reality (VR) and AR training into medical school and residency programs would necessitate prototype testing and entirely new teaching methods, AR has the potential to completely transform medical and science training [14-16]. Early adopters of AR innovations in medical training have noted several benefits, including the ability to simulate real-life scenarios without risking real-world consequences. Despite these advancements, there is still a lack of published experimental and observational work on the effectiveness and usefulness of AR in medical training and education [16].
In their work, Eckert et al [17] provided an overview of the development of AR applications in health care from 2012 to 2017. According to their findings, despite an increasing number of publications on AR in medicine, there have been no significant clinical trials on AR effectiveness. However, display-related domains tended to receive more research attention than other AR interventions.
The literature shows some discrepancies in the effectiveness of AR in medical training. To date, most of the meta-analysis research on the efficiency of VR and virtual patients in medical education has been carried out by Chen et al [18] and Kononowicz et al [19]. Their research has inspired this study, and there is some thematic overlap, but they presented their findings in a different way. However, to the best of our knowledge, no meta-analysis has been conducted to assess AR in medical training, with the exception of 2 studies—those by Williams et al [20] and Barsom et al [16], which conducted a systematic review with no meta-analysis. Therefore, filling this gap represents a significant addition to the literature. The primary goal of this study is to perform a meta-analysis on the efficacy of AR in 5 areas of learning and training. These include participants’ skills (eg, the ability to illustrate a certain process), knowledge (eg, the ability to understand a certain concept), confidence (eg, the ability to learn certain content with self-confidence), performance time (eg, the amount of time spent on a certain task), and satisfaction (eg, the level of learning fulfilment for a certain AR intervention). The findings of this work have many implications for policy makers, patients, medical students, and professionals and for using AR technology to facilitate learning and training mechanisms in the medical field. This meta-analysis seeks to address the following research questions (RQs):
RQ1: What are the characteristics of studies using AR in medical training?
RQ2: What kind of AR interventions were used to assist with medical training?
RQ3: Does the use AR have an effect on medical training when compared to other methods?
Methods
Overview
The Methods section discusses the approaches used to obtain specific publications as well as the constraints and eligibility requirements that were used [21]. Following that, an overview of the standards used to interpret the studies and associated variables is provided. This meta-analysis was carried out in compliance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [22]. A checklist of all PRISMA items is presented in Multimedia Appendix 1.
Eligibility Criteria
The meta-analysis included studies that (1) were published between 2013 and April 2021, (2) were written in English, and (3) primarily focused on AR for learning and training. Further, we excluded studies that (1) used other virtual platforms, such as VR and virtual patients, and (2) had no experimental data. However, based on the PICO (Population, Intervention, Comparison, Outcomes) framework, our final analysis incorporated various trials, including those with randomized controlled and mixed designs. Textbox 1 illustrates all of the PICO elements used for the inclusion criteria.
PICO (Population, Intervention, Comparison, Outcomes) framework.
Criteria and descriptions
-
Population
Sex (male or female)
Age (>15 years)
Target group (medical professionals, residents, patients, or students)
-
Intervention
All types of augmented reality technology used in training or learning.
-
Comparison
Augmented reality, nonaugmented reality, and conventional methods (eg, paper or pen, classes, simulations, or presentations)
-
Outcomes
Knowledge
Confidence
Skills
Performance time
Satisfaction
Information Source and Search Strategy
We conducted a web-based literature search in the Cochrane Library, PubMed, Embase, Web of Science and Google Scholar databases from February to April 2021. We also manually checked the reference lists of the eligible studies to identify and acquire additional relevant publications. We used the following set of keywords, terms, and logical operators: “augmented reality” OR “AR” OR “mixed reality” OR “patient simulation” AND “medical training” OR “medical education” OR “health professions training.” Some of the search strategies and terms used are presented in Multimedia Appendix 2. It is worth mentioning that the search strategies were slightly modified to suit each web-based database. EndNote X9 (Clarivate) software was used to manage and import the selected documents and to remove duplicates. This process was carried out by 2 authors (YB and GA) of this study.
Data Extraction
Data were placed into an extraction spreadsheet by using Microsoft Excel 2019. From each of the studies, information was extracted based on the study characteristics, designs, and participants. These data included the names of authors, the years of the studies, the locations of the studies, sample sizes, participant types, study designs, and interventions and outcomes. EndNote X9 was also used to obtain some publication data, such as titles, publishers, URLs, digital object identifiers, page numbers, issue numbers, and volume numbers. The process of data extraction was initially performed by 2 authors (HA and A Alwadain) and was then validated by another 2 authors (WNWA and LFC).
Risk of Bias Assessment
The quality of the studies was assessed by 2 authors (AB and A Alghail). We followed the criteria of the Cochrane Handbook for Systematic Reviews of Interventions [23] in the risk of bias assessment process. These include 7 domains that correspond to a particular kind of bias. Each domain was given a score (a “high risk,” “low risk,” or “unclear risk” of bias), and any disagreements among coauthors were settled via consensus.
Statistical Analysis
RevMan 5.4 (The Cochrane Collaboration) software was used to perform the risk of bias assessment; different scales were used by different authors to measure the outcomes; therefore, raw data could not be compared directly. Thus, the R 4.0.2 (R Foundation for Statistical Computing) software was used to transform raw data, so that STATA 14.0 (StataCorp LLC) could be used to run the analysis directly. The metacont package on R was used to transform the data on the sample sizes, SDs, and means of the control and AR groups. Data on the sample sizes, means, and SDs of only the AR groups were transformed by using the metamean package. Only 1 study [24] recorded the sample size and the proportion of participants on whom AR had a positive effect. The effect sizes and CIs were generated by using the two different packages. STATA 14.0 was used to generate the forest plot for each outcome, which used the transformed data (effect size and CI), via the metan command. The statistical heterogeneity among the selected studies was measured by using I2 in each analysis and a 5% significance level. The random effect model was selected for the analysis carried out because the true effect sizes underlying all studies were stochastic.
Results
Study Selection
From our initial search of 5 potential databases, we found a total of 1832 records. We identified a total of 1839 records, including relevant reference lists (n=7). Duplicate records (973/1839, 52.9%) were removed. Following that, a total of 866 of the 1839 (47.1%) studies were screened based on their titles, abstracts, and keywords, and 798 were excluded after applying the eligibility criteria. A total of 68 studies were downloaded and evaluated via full-text screening, of which 55 were excluded for various reasons (Figure 1). Finally, 13 studies with a total of 654 participants were eligible for the meta-analysis; 2 studies used the same set of participants for both the control and AR groups [25,26], while another 6 studies [27-32] that also measured both the control and AR groups divided the sample size.
Figure 1.
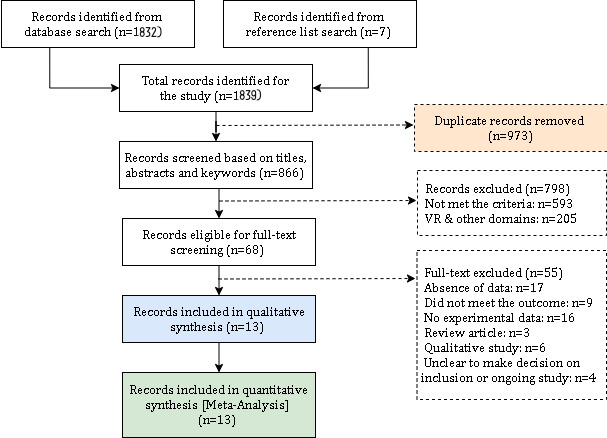
Study screening and selection flowchart. VR: virtual reality.
Study Characteristics
As presented in Table 1, the trials of the selected studies were performed in the following ten countries: Germany [27,28,30], the United States [24,31], the United Kingdom [33], Canada [34], Italy [35], Sweden [26], Finland [32], Switzerland [29], Spain [36], and South Korea [25]. Furthermore, 10 of the 13 studies, adopted a randomized control trial [24,26-29,32-36], 2 studies had a mixed design [30,31], and 1 study used a cohort approach [25]. The number of participants in the studies ranged between 4 and 372. With regard to these participants, 5 trials recruited medical and nursing students [25,27,28,30,31]; 2 trials involved pediatric and psychiatry residents [26,29]; 1 trial recruited visitors to a center [32]; and the remaining trials (n=5) included multiple participants, such as physicians, registered nurses, technicians, residents, students, clinicians, clients, hosts, and paramedics [24,33-36].
Table 1.
Characteristics of the selected studies.
| Author, year | Country | Brief description | Participants | Sample size, n (number of participants in each study group) | Study design | Outcomes |
| Albrecht et al, 2013 [27] | Germany | Comparing the effect of MARa to that of a textbook, with consideration for essential psychological qualities | Students | 10 (6 and 4) | RCTb | Skill and confidence |
| Balian et al, 2019 [24] | United States of America | Testing the feasibility of an ARc training system (Microsoft HoloLens) for CPRd among medical professionals | Physicians, nurses, and technicians | 51 (N/Ae) | RCT | Performance time and satisfaction |
| Ingrassia et al, 2020 [35] | Italy | Assessing the feasibility of an AR prototype for BLSDf training | Physicians, nurses, and residents | 26 (N/A) | RCT | Confidence and satisfaction |
| Kim et al, 2021 [25] | Korea | Evaluating the usability and feasibility of AR (smart glasses) for nursing training skills | Students | 30 (N/A) | Cohort | Skill, performance time, satisfaction, and knowledge |
| Kotcherlakota et al, 2020 [31] | United States of America | Assessing the use of AR (clinical simulation) in the management of pediatric asthma outcomes | Students | 21 (12 and 9) | Mixed | Confidence and satisfaction |
| Muangpoon et al, 2020 [33] | United Kingdom | Proposing an AR system (Microsoft HoloLens, 1st Gen) to improve the learning and teaching of DREg | Clinicians and students | 19 (N/A) | RCT | Skill, knowledge, and satisfaction |
| Noll et al, 2017 [28] | Germany | Assessing learning success by comparing learners with and without MAR | Students | 44 (22 and 22) | RCT | Knowledge and skill |
| Pantziaras et al, 2015 [26] | Sweden | Evaluating the impact of virtual patient training on the knowledge of stress disorder management and symptoms | Residents | 32 (N/A) | RCT | Knowledge |
| Savela et al, 2020 [32] | Finland | Investigating the features of MAR for learning and sociability | Visitors | 372 (231, 71, and 71) | RCT | Knowledge and satisfaction |
| Schiffeler et al, 2019 [30] | Germany | Assessing the effects of AR on interaction and communication | Students | 13 (7 and 6) | Mixed | Knowledge |
| Siebert et al, 2017 [29] | Switzerland | Evaluating whether the adaption of AR glasses with AHAh guidelines can reduce the time and deviation of essential lifesaving exercises throughout pediatric CPR when compared to those of PALSi | Residents | 20 (10 and 10) | RCT | Performance time and confidence |
| Vidal-Balea et al, 2021 [36] | Spain | Evaluating MAR games that teach and train people how to use pediatric medical applications (the games also monitor training progress) | Clients and hosts | 4 (N/A) | RCT | Performance time |
| Wang et al, 2017 [34] | Canada | Developing a telemedicine platform using AR (Microsoft HoloLens) to improve medical training remotely | Paramedics and students | 12 (N/A) | RCT | Performance time and satisfaction |
aMAR: mobile augmented reality.
bRCT: randomized controlled trial.
cAR: augmented reality.
dCPR: cardiopulmonary resuscitation.
eN/A: not applicable.
fBLSD: basic life support and defibrillation.
gDRE: digital rectal examination.
hAHA: American Heart Association.
iPALS: pediatric advanced life support.
In recent years, the use of AR in the medical field has attracted the attention of academics and researchers, as evidenced by the increasing number of publications devoted to AR. This is demonstrated by the fact that 8 of the 13 studies were conducted between 2019 and 2021. The characteristics of the selected studies, including the outcome measures, interventions, and types of participants, are shown in Table 1. Additional details regarding the AR and control groups are presented in Multimedia Appendix 3.
Risk of Bias
Figure 2 and Figure 3 present the risk of bias assessment, which was performed according to the Cochrane criteria. Of the 13 studies, 10 detailed randomized methods [24,26-28,30-33,35,36], while the rest of the studies (n=3) [25,29,34] reported no sequence generation methods. Only 3 trials reported concealment methods [25,32,34]. Furthermore, 3 studies reported dropouts [29,30,33] but did not go into detail about how they were handled. Due to the uniqueness of the intervention methods, no blinding methods were reported for participants in any of the trials. The blinding of assessors was used in 5 trials [26,27,29,35,36].
Figure 2.
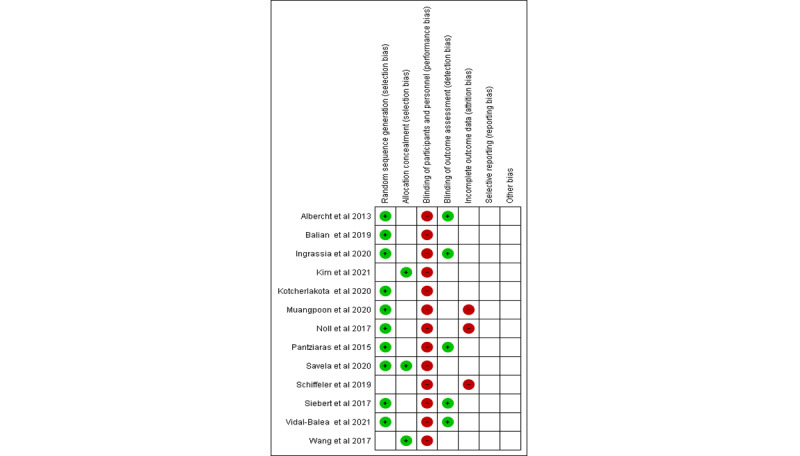
Figure 3.
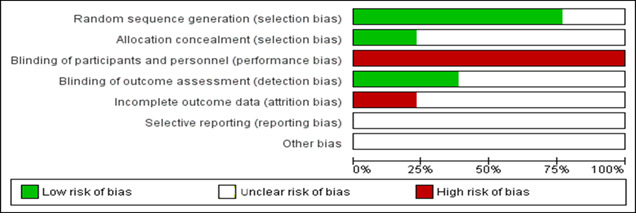
Overall risk of bias assessment of the selected studies.
Publication Bias
The most significant issue with meta-analyses is the possibility of bias and error arising from combining multiple studies, especially unrelated studies. Creating a funnel plot is one of the key methods used for testing common publication bias. The graphics in the funnel are obvious scatter plots for the effect size approximated in each selected study versus the unit of sample size reported in the studies [37]. If there is no bias, the graphic resembles an upside-down funnel. However, if a publication bias exists, the graphic should be asymmetric and distorted [38]. Figure 4 shows the funnel plot that we used to test for publication bias.
Figure 4.
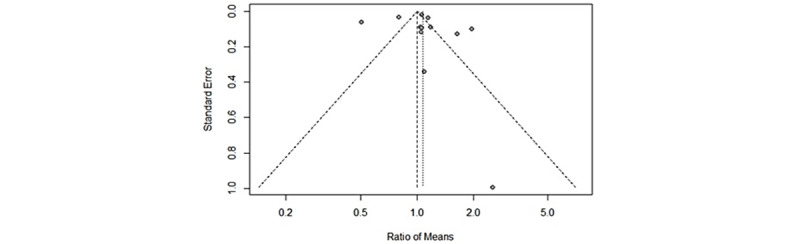
Funnel plot showing publication bias.
As can be seen in Figure 4, the 13 studies included in the meta-analysis are symmetrically placed on both sides of the vertical effect size line and are very close to the symmetrical and merged effect size lines. If there is no publication bias, studies should be distributed symmetrically on both sides of the vertical line depicting the merged effect size. If the studies are placed outside of the pyramid, they should be concentrated in the upper or middle parts of the plot. However, if there is a bias, most of the studies will be in the funnel plot's bottom part or in only 1 vertical line segment [39]. The effect sizes of the included studies are distributed in a symmetrical manner, with only 5 studies located outside of the pyramid. However, it is worth nothing that 4 of these studies are located in the upper part of the pyramid. This pattern shows that the studies included in this work have no publication bias.
As shown in Figure 5—the meta-regression plot—the true effect sizes between the control and AR groups are 1.8 for the 2013 study [27]; 0.9 for the 2015 study [26]; 2.2, 0.2, and −0.9 for the 2017 studies [28,29,34], respectively; 1.2 and 0.9 for the 2019 studies [24,30], respectively; 0.4, −1, 0.2, and 1.5 for the 2020 studies [31-33,35], respectively; and finally, −3.1 and 0.8 for the 2021 studies [25,36], respectively.
Figure 5.
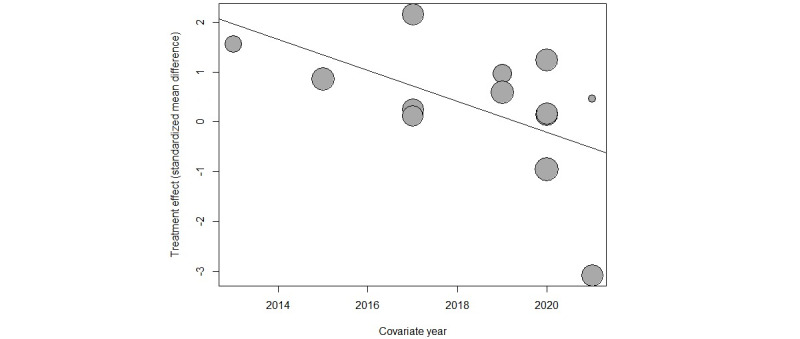
Meta-regression plot showing the publication years.
Results of the Meta-analysis
A meta-analysis was performed by using the data set in Multimedia Appendix 4 for each of the five outcomes (ie, knowledge [Multimedia Appendix 5], performance time [Multimedia Appendix 6], satisfaction [Multimedia Appendix 7], confidence [Multimedia Appendix 8], and skills [Multimedia Appendix 9]). The coding of the final analysis is also provided in Multimedia Appendix 10.
Knowledge
Only 6 of the 13 selected studies recorded knowledge as scores [25,26,28,30,32,33]. The total number of participants who measured their knowledge was 510. The findings from the plot (Figure 6) showed that there is no relationship between AR training and improvement in the participants' knowledge (Z=0.130; P=.90).
Figure 6.
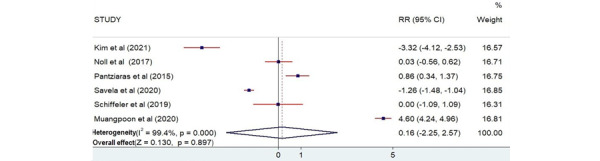
Forest plot showing the effectiveness of augmented reality on knowledge [25,26,28,30,32,33]. Weights are from the random-effects model. RR: risk ratio.
Skills
A total of 4 studies used skill as the outcome measurement [25,27,28,33]. The total number of participants that participated in measuring skill was 103. The plot (Figure 7) revealed that there is no statistical relationship between AR training and participants’ skills (Z=1.668; P=.10). There is high heterogeneity among the studies.
Figure 7.
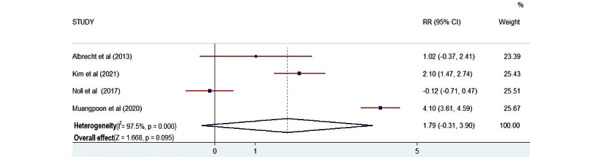
Forest plot showing the effectiveness of augmented reality on skills [25,27,28,33]. Weights are from the random-effects model. RR: risk ratio.
Confidence
In total, 4 studies recorded confidence outcomes [27,29,31,35]. The total number of participants who measured their confidence was 77. There was a statistical relationship between AR training and participants’ confidence, as the P value was significant according to the plot (Z=2.363; P=.02; Figure 8).
Figure 8.
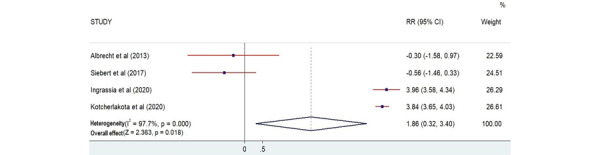
Forest plot showing the effectiveness of augmented reality on confidence [27,29,31,35]. Weights are from the random-effects model. RR: risk ratio.
Performance Time
Performance time was assessed as an outcome measure in 5 studies [24,25,29,34,36]. The total number of participants that participated in measuring performance time was 129. There was a statistical relationship between AR training and participants’ performance time because the P value was significant according to the plot (Z=4.596; P<.001; Figure 9).
Figure 9.
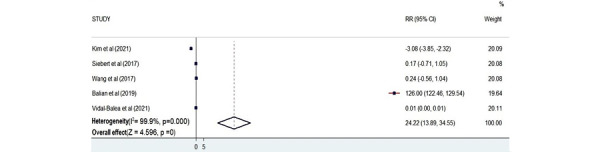
Forest plot showing the effectiveness of augmented reality on performance time [24,25,29,34,36]. Weights are from the random-effects model. RR: risk ratio.
Satisfaction
A total of 7 studies reported participants’ satisfaction [24,25,31-35]. The total number of participants who measured their satisfaction was 543. There was a statistical relationship between AR training and participants’ satisfaction according to the plot (Z=2.760; P=.006; Figure 10).
Figure 10.
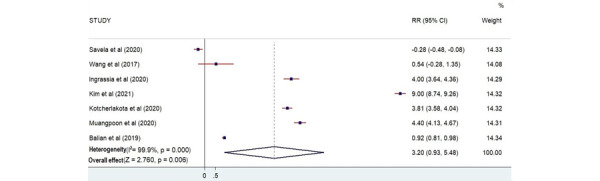
Forest plot showing the effectiveness of augmented reality on satisfaction [24,25,31-35]. Weights are from the random-effects model. RR: risk ratio.
Discussion
Main Findings
The usefulness of AR simulation methods in medical training was evaluated in this meta-analysis. In terms of skill outcomes, AR training did not outperform other educational methods for medical training. A study on the use of AR in medical education found that students’ skills improved after the intervention [25]. In terms of skill performance scores and success rates, it was found that AR groups did not exhibit any statistical relationships, even though each of the trials that reported skills (ie, those included in our study) used different education and training methods for their control groups.
There was a statistical difference (P=.02) between the AR and control groups in terms of confidence. Participants' confidence was improved by AR when compared to that of participants in control conditions. It was found that AR training had a greater effect on participants’ confidence.
The I2 values reported throughout the Results section are very high, indicating that there was a huge level of heterogeneity between studies. In terms of knowledge outcomes, participants who underwent AR training did not outperform those who used other educational methods for medical training. However, a previous study that looked at how AR affects learning found that AR was more effective for knowledge retention [27] and that students are more likely to make connections between concepts when they are in an interactive learning environment. As a result, more research into the impact of AR on knowledge in medical training is needed in the future.
Between the control and AR groups, there was a significant difference in participants’ satisfaction (P=.006). Of the 7 studies that recorded satisfaction as an outcome, 4 [25,32-34] indicated partial satisfaction. Some participants remarked on how difficult it is for AR technology to affect user satisfaction. As a result, we believe that participants’ satisfaction with AR training may vary depending on technical factors. AR technology will be better able to satisfy users as the technology advances.
A meta-analysis of performance time was also carried out. The findings suggested that AR was more effective than other training methods at reducing performance time. However, we found that AR was more efficient than other methods in enhancing performance time. The observed heterogeneity could have been due to the various research designs and settings used in the selected studies, such as surgical projects, AR devices, and control group training methods. One study [36] on the efficiency of AR endoscopy simulation training analyzed performance time based on real-world data and found no significant difference between the AR and control groups, but the evidence quality was poor. Other studies that measured performance time as an outcome found that AR can assist operators in reducing performance time [24,25].
Strengths and Limitations
One of the main strengths of this work is being among the first meta-analyses to be conducted on the effectiveness of AR in medical training, which presents a significant contribution to the advancement of AR in the medical field. Furthermore, our work involved an assessment of 13 trials with a total of 654 participants from various countries.
Our work has some limitations as well. The first is that we only included articles that focused on AR as an intervention, which made it difficult to find a large number of studies. Second, some of the studies included in the review omitted information about allocation concealment, sequence generation, and blinding methods. Finally, the 13 trials we evaluated used different teaching and training methods for their control groups, which could lead to significant heterogeneity.
Conclusions
The effectiveness of AR training methods in the medical field was assessed in this work. The meta-analysis included 13 trials with a total of 654 participants that were completed between 2013 and 2021. In all trials, AR training was used as an intervention in AR groups, while conventional methods were used for control groups. Based on our findings, medical students' performance time, confidence, and satisfaction can be improved by using AR training and education methods. However, there was no statistical difference between the skills and knowledge that participants gained by undergoing AR training and those gained via conventional training methods. The use of AR should therefore be adopted in medical department training because of its significant effect on the performance time of participants. In general, AR should be used to expand knowledge and as a supplement to other simulation approaches to enhance clinical practice quality and safety. It is very noticeable that there are considerable gaps in the literature regarding the use of AR technology in medical training, and a limited number of studies exist, suggesting that further research efforts in this area are needed.
Acknowledgments
This research is supported by the Researchers Supporting Project (project number: RSP-2021/309), King Saud University, Riyadh, Saudi Arabia.
Abbreviations
- AR
augmented reality
- PICO
Population, Intervention, Comparison, Outcomes
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- RQ
research question
- VR
virtual reality
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Search strategies.
Augmented reality and control groups.
The data set.
Knowledge.
Performance time.
Satisfaction.
Confidence.
Skill.
R and Stata codes.
Footnotes
Authors' Contributions: YB conceptualized this meta-analysis. LFC and A Alwadain acquired funding. YB and GA conducted the investigation. YB, WNWA, GA, HA, A Alwadain, LFC, AB, and A Alghail contributed to the methodology. YB, HA, and A Alwadain were responsible for the resources used. YB was responsible for the software used. WNWA, HA, and A Alwadain supervised the meta-analysis. AB and A Alghail validated the meta-analysis. GA was responsible for data visualization. YB wrote the original manuscript draft. WNWA, GA, HA, A Alwadain, AB, LFC, and A Alghail reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest: None declared.
References
- 1.Dickey RM, Srikishen N, Lipshultz LI, Spiess PE, Carrion RE, Hakky TS. Augmented reality assisted surgery: a urologic training tool. Asian J Androl. 2016;18(5):732–734. doi: 10.4103/1008-682X.166436. http://www.ajandrology.com/article.asp?issn=1008-682X;year=2016;volume=18;issue=5;spage=732;epage=734;aulast=Dickey .166436 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Khor WS, Baker B, Amin K, Chan A, Patel K, Wong J. Augmented and virtual reality in surgery-the digital surgical environment: applications, limitations and legal pitfalls. Ann Transl Med. 2016 Dec;4(23):454. doi: 10.21037/atm.2016.12.23. doi: 10.21037/atm.2016.12.23.atm-04-23-454 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zhu E, Lilienthal A, Shluzas LA, Masiello I, Zary N. Design of mobile augmented reality in health care education: A theory-driven framework. JMIR Med Educ. 2015 Sep 18;1(2):e10. doi: 10.2196/mededu.4443. https://mededu.jmir.org/2015/2/e10/ v1i2e10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Blomqvist S, Seipel S, Engström M. Using augmented reality technology for balance training in the older adults: a feasibility pilot study. BMC Geriatr. 2021 Feb 26;21(1):144. doi: 10.1186/s12877-021-02061-9. https://bmcgeriatr.biomedcentral.com/articles/10.1186/s12877-021-02061-9 .10.1186/s12877-021-02061-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Malheiros O. Handbook of Research on Assertiveness, Clarity, and Positivity in Health Literacy. Hershey, Pennsylvania: IGI Global; 2022. Virtual reality and augmented reality as promoters of better health literacy: Analysing assertiveness, clear language, and positivity. [Google Scholar]
- 6.Susilawati E, Johari A, Marzal J, Anggereini E. Effectiveness of multimedia e-book and augmented reality on knowledge and skill of health science students: A systematic review. Journal of Client-Centered Nursing Care. 2022 May 01;8(2):99–110. doi: 10.32598/JCCNC.8.2.380.2. https://jccnc.iums.ac.ir/article-1-352-en.pdf . [DOI] [Google Scholar]
- 7.Hu MH, Chiang CC, Wang ML, Wu NY, Lee PY. Clinical feasibility of the augmented reality computer-assisted spine surgery system for percutaneous vertebroplasty. Eur Spine J. 2020 Jul;29(7):1590–1596. doi: 10.1007/s00586-020-06417-4.10.1007/s00586-020-06417-4 [DOI] [PubMed] [Google Scholar]
- 8.Zhuang Y, Sun J, Liu J. Diagnosis of chronic kidney disease by three-dimensional contrast-enhanced ultrasound combined with augmented reality medical technology. J Healthc Eng. 2021 Mar 16;2021:5542822. doi: 10.1155/2021/5542822. doi: 10.1155/2021/5542822. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 9.Tang KS, Cheng DL, Mi E, Greenberg PB. Augmented reality in medical education: a systematic review. Can Med Educ J. 2020 Mar 16;11(1):e81–e96. doi: 10.36834/cmej.61705. http://europepmc.org/abstract/MED/32215146 .CMEJ-11-e081 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lee LN, Kim MJ, Hwang WJ. Potential of augmented reality and virtual reality technologies to promote wellbeing in older adults. Appl Sci (Basel) 2019 Aug 30;9(17):3556. doi: 10.3390/app9173556. https://www.mdpi.com/2076-3417/9/17/3556/htm . [DOI] [Google Scholar]
- 11.Yeung AWK, Tosevska A, Klager E, Eibensteiner F, Laxar D, Stoyanov J, Glisic M, Zeiner S, Kulnik ST, Crutzen R, Kimberger O, Kletecka-Pulker M, Atanasov AG, Willschke H. Virtual and augmented reality applications in medicine: Analysis of the scientific literature. J Med Internet Res. 2021 Feb 10;23(2):e25499. doi: 10.2196/25499. https://www.jmir.org/2021/2/e25499/ v23i2e25499 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Juanes-Méndez JA, Marcos-Pablos S, Velasco-Marcos MA, Izard SG. Technological Adoption and Trends in Health Sciences Teaching, Learning, and Practice. Hershey, Pennsylvania: IGI Global; 2022. Medical learning through simulations with immersive virtual reality and augmented reality devices. [Google Scholar]
- 13.Kamphuis C, Barsom E, Schijven M, Christoph N. Augmented reality in medical education? Perspect Med Educ. 2014 Sep;3(4):300–311. doi: 10.1007/s40037-013-0107-7. http://europepmc.org/abstract/MED/24464832 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gerup J, Soerensen CB, Dieckmann P. Augmented reality and mixed reality for healthcare education beyond surgery: an integrative review. Int J Med Educ. 2020 Jan 18;11:1–18. doi: 10.5116/ijme.5e01.eb1a. https://www.ijme.net/pmid/31955150 .ijme.11.118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Duarte ML, Santos LR, Júnior JBG, Peccin MS. Learning anatomy by virtual reality and augmented reality. A scope review. Morphologie. 2020 Dec;104(347):254–266. doi: 10.1016/j.morpho.2020.08.004.S1286-0115(20)30081-3 [DOI] [PubMed] [Google Scholar]
- 16.Barsom EZ, Graafland M, Schijven MP. Systematic review on the effectiveness of augmented reality applications in medical training. Surg Endosc. 2016 Oct;30(10):4174–4183. doi: 10.1007/s00464-016-4800-6. http://europepmc.org/abstract/MED/26905573 .10.1007/s00464-016-4800-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eckert M, Volmerg JS, Friedrich CM. Augmented reality in medicine: Systematic and bibliographic review. JMIR Mhealth Uhealth. 2019 Apr 26;7(4):e10967. doi: 10.2196/10967. https://mhealth.jmir.org/2019/4/e10967/ v7i4e10967 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Chen FQ, Leng YF, Ge JF, Wang DW, Li C, Chen B, Sun ZL. Effectiveness of virtual reality in nursing education: Meta-analysis. J Med Internet Res. 2020 Sep 15;22(9):e18290. doi: 10.2196/18290. https://www.jmir.org/2020/9/e18290/ v22i9e18290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kononowicz AA, Woodham LA, Edelbring S, Stathakarou N, Davies D, Saxena N, Car LT, Carlstedt-Duke J, Car J, Zary N. Virtual patient simulations in health professions education: Systematic review and meta-analysis by the Digital Health Education Collaboration. J Med Internet Res. 2019 Jul 02;21(7):e14676. doi: 10.2196/14676. https://www.jmir.org/2019/7/e14676/ v21i7e14676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Williams MA, McVeigh J, Handa AI, Lee R. Augmented reality in surgical training: a systematic review. Postgrad Med J. 2020 Sep;96(1139):537–542. doi: 10.1136/postgradmedj-2020-137600.postgradmedj-2020-137600 [DOI] [PubMed] [Google Scholar]
- 21.Baashar Y, Alhussian H, Patel A, Alkawsi G, Alzahrani AI, Alfarraj O, Hayder G. Customer relationship management systems (CRMS) in the healthcare environment: A systematic literature review. Comput Stand Interfaces. 2020 Aug;71:103442. doi: 10.1016/j.csi.2020.103442. http://europepmc.org/abstract/MED/34170994 .S0920-5489(19)30459-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Moher D, Altman DG, Liberati A, Tetzlaff J. PRISMA statement. Epidemiology. 2011 Jan;22(1):128; author reply 128. doi: 10.1097/EDE.0b013e3181fe7825.00001648-201101000-00022 [DOI] [PubMed] [Google Scholar]
- 23.Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, Cochrane Collaboration . Cochrane Handbook for Systematic Reviews of Interventions. Hoboken, NJ; Chichester, West Sussex: Wiley-Blackwell; 2019. p. 1119536618. [Google Scholar]
- 24.Balian S, McGovern SK, Abella BS, Blewer AL, Leary M. Feasibility of an augmented reality cardiopulmonary resuscitation training system for health care providers. Heliyon. 2019 Aug 02;5(8):e02205. doi: 10.1016/j.heliyon.2019.e02205. https://linkinghub.elsevier.com/retrieve/pii/S2405-8440(19)35865-7 .S2405-8440(19)35865-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kim SK, Lee Y, Yoon H, Choi J. Adaptation of extended reality smart glasses for core nursing skill training among undergraduate nursing students: Usability and feasibility study. J Med Internet Res. 2021 Mar 02;23(3):e24313. doi: 10.2196/24313. https://www.jmir.org/2021/3/e24313/ v23i3e24313 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Pantziaras I, Fors U, Ekblad S. Training with virtual patients in transcultural psychiatry: do the learners actually learn? J Med Internet Res. 2015 Feb 16;17(2):e46. doi: 10.2196/jmir.3497. https://www.jmir.org/2015/2/e46/ v17i2e46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Albrecht UV, Folta-Schoofs K, Behrends M, von Jan U. Effects of mobile augmented reality learning compared to textbook learning on medical students: randomized controlled pilot study. J Med Internet Res. 2013 Aug 20;15(8):e182. doi: 10.2196/jmir.2497. https://www.jmir.org/2013/8/e182/ v15i8e182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Noll C, von Jan U, Raap U, Albrecht UV. Mobile augmented reality as a feature for self-oriented, blended learning in medicine: Randomized controlled trial. JMIR Mhealth Uhealth. 2017 Sep 14;5(9):e139. doi: 10.2196/mhealth.7943. https://mhealth.jmir.org/2017/9/e139/ v5i9e139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Siebert JN, Ehrler F, Gervaix A, Haddad K, Lacroix L, Schrurs P, Sahin A, Lovis C, Manzano S. Adherence to AHA guidelines when adapted for augmented reality glasses for assisted pediatric cardiopulmonary resuscitation: A randomized controlled trial. J Med Internet Res. 2017 May 29;19(5):e183. doi: 10.2196/jmir.7379. https://www.jmir.org/2017/5/e183/ v19i5e183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schiffeler N, Stehling V, Hees F, Isenhardt I. Effects of collaborative augmented reality on communication and interaction in learning contexts – Results of a qualitative pre-study. 2019 ASEE Annual Conference & Exposition; June 15-19, 2019; Tampa, Florida. 2019. Jun 15, [DOI] [Google Scholar]
- 31.Kotcherlakota S, Pelish P, Hoffman K, Kupzyk K, Rejda P. Augmented reality technology as a teaching strategy for learning pediatric asthma management: Mixed methods study. JMIR Nurs. 2020 Dec 02;3(1):e23963. doi: 10.2196/23963. http://europepmc.org/abstract/MED/34406970 .v3i1e23963 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Savela N, Oksanen A, Kaakinen M, Noreikis M, Xiao Y. Does augmented reality affect sociability, entertainment, and learning? A field experiment. Appl Sci (Basel) 2020 Feb 19;10(4):1392. doi: 10.3390/app10041392. https://www.mdpi.com/2076-3417/10/4/1392/htm . [DOI] [Google Scholar]
- 33.Muangpoon T, Osgouei RH, Escobar-Castillejos D, Kontovounisios C, Bello F. Augmented reality system for digital rectal examination training and assessment: System validation. J Med Internet Res. 2020 Aug 13;22(8):e18637. doi: 10.2196/18637. https://www.jmir.org/2020/8/e18637/ v22i8e18637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Wang S, Parsons M, Stone-McLean J, Rogers P, Boyd S, Hoover K, Meruvia-Pastor O, Gong M, Smith A. Augmented reality as a telemedicine platform for remote procedural training. Sensors (Basel) 2017 Oct 10;17(10):2294. doi: 10.3390/s17102294. https://www.mdpi.com/resolver?pii=s17102294 .s17102294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ingrassia PL, Mormando G, Giudici E, Strada F, Carfagna F, Lamberti F, Bottino A. Augmented reality learning environment for basic life support and defibrillation training: Usability study. J Med Internet Res. 2020 May 12;22(5):e14910. doi: 10.2196/14910. https://www.jmir.org/2020/5/e14910/ v22i5e14910 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Vidal-Balea A, Blanco-Novoa Ó, Fraga-Lamas P, Fernández-Caramés TM. Developing the next generation of augmented reality games for pediatric healthcare: An open-source collaborative framework based on ARCore for implementing teaching, training and monitoring applications. Sensors (Basel) 2021 Mar 07;21(5):1865. doi: 10.3390/s21051865. https://www.mdpi.com/resolver?pii=s21051865 .s21051865 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Üstün U, Eryılmaz A. A research methodology to conduct effective research syntheses: Meta-analysis. Education and Science. 2014;39(174):1–32. doi: 10.15390/eb.2014.3379. http://egitimvebilim.ted.org.tr/index.php/EB/article/view/3379/784 . [DOI] [Google Scholar]
- 38.Üstün U. To what extent is problem-based learning effective as compared to traditional teaching in science education? A meta-analysis study. OpenMETU. 2012. Sep, [2022-05-19]. https://open.metu.edu.tr/bitstream/handle/11511/22032/index.pdf .
- 39.Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis, 2nd Edition. Hoboken, NJ: John Wiley & Sons; 2021. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.
Search strategies.
Augmented reality and control groups.
The data set.
Knowledge.
Performance time.
Satisfaction.
Confidence.
Skill.
R and Stata codes.