

Abstract
Nicola M McKeown and colleagues advocate for the importance of translating the health impact of high fibre diets to patients and clients, with emphasis placed on incorporating a variety of plant based foods to achieve dietary fibre recommendations
Historically, fibre was defined simply as plant “roughage,” and health professionals might still be under the impression that fibre is a single entity. But, like most other nutrients, fibre is much more complex than it first seems, and most people today fall short of meeting dietary recommendations for this nutrient. Modern day diets are very different from those of our ancestors, which contained substantially more fibre because they consumed a variety of plant based foods.1 Ancestral humans might have consumed as much as 100 g of fibre daily.1 Today, adults in North America consume an average of 17 g of dietary fibre daily; intakes are slightly higher in European countries (18 g to 24 g a day).2
The definition of dietary fibre has evolved from “remnants of plant cells that are resistant to digestion by human enzymes”3 in the 1970s to the more complex global definition outlined in 2009 by the Codex Alimentarius Commission (box 1).4 Although there has been considerable debate over the past few decades about the terminology and analytical methodology used to define dietary fibre, most definitions now include carbohydrates with three or more monomeric units.2 This includes some well known prebiotic fibres, such as fructans and inulins.2 Despite scientific advances in the field, consumer confusion persists, and current intakes of dietary fibre fall short in many populations worldwide.
Box 1. Codex Alimentarius definition of dietary fibre.
Carbohydrate polymers with 10 or more monomeric units* that are not hydrolysed by endogenous enzymes in the human small intestine, categorised as:
Edible carbohydrate polymers naturally occurring in the food as consumed
Carbohydrate polymers obtained from food raw material by physical, enzymatic, or chemical† means and shown to have a physiological benefit on health as indicated by generally accepted scientific evidence to competent authorities
Synthetic carbohydrate polymers that have been shown to have a physiological benefit on health as indicated by generally accepted scientific evidence to competent authorities
*The decision on whether to include carbohydrates of 3-9 monomeric units should be left to national authorities
†Also referred to as isolated fibres. Isolated and synthetic fibres are also called “added fibres” and “functional fibres.”
Not all dietary fibres are created equally
Consumers and healthcare professionals might not understand the complexity of dietary fibre, thinking that it is a single nutrient found in plant foods. Daily recommended fibre intakes and food labels refer to dietary fibre without considering the source, type, quality, or physiological effects. Additional complexity relates to the fact that isolated or synthetic fibres can be added to foods and beverages as ingredients, and the same fibres might have multiple names. Importantly, there are several distinct classes of fibre that deliver different health benefits.5 One key message for consumers and health professionals to understand is that, although all added fibres in foods contribute towards the recommended daily intake, different isolated fibres deliver different health benefits based on their physiochemical properties (solubility, viscosity) and physiological effects (fermentability) (fig 1).
Fig 1.

Functional properties of dietary fibre. Colours identify dietary fibres that have the same functional properties. Red: soluble, viscous fermentable fibre; green: soluble, viscous, non-fermentable fibre; purple: soluble, non-viscous, fermentable fibre; black: soluble, non-viscous, fermentable fibre; blue: insoluble, partially fermentable; orange: insoluble, non-fermentable
Soluble, viscous fibres such as oat β-glucan, for example, reduce serum cholesterol and improve glycaemic control, whereas insoluble fibres such as coarse wheat and rye brans have a faecal bulking effect and might promote regular laxation.5 Dietary fibres are fermentable to some extent, but the degree to which they are fermented varies from low (cellulose, hemicelluloses, wheat bran) to moderate (β-glucans, gums, pectins, resistant starch) and high (prebiotic fibres such as inulin and oligofructose). A common misconception is that all insoluble fibres are entirely non-fermentable, but evidence indicates that the majority of fibres will result in changes in the composition of the microbiota, owing to competitive interactions.6
Various authorities have recently evaluated the evidence linking isolated and synthesised fibre intake to physiological benefits for health (box 2).7 8 9
Box 2. Physiological health benefits attributed to isolated or synthetic fibres.
Lower blood glucose levels
Reduce postprandial blood glucose or insulin levels, or both
Lower total or LDL cholesterol levels, or both
Lower blood pressure
Improve laxation
Decrease transit time
Increase gastrointestinal mineral absorption
Reduce energy intake via increased satiety
Favourable modulation of gut microbiota
Natural fibre containing foods such as fruits, vegetables, legumes, and whole grains have long been known to deliver health benefits that can be attributable to dietary fibre, the diverse array of nutrients and phytochemicals found in these foods, and synergistic interplay between the two.10 11 Strong evidence from observational studies shows that populations with a large proportion of plant based, fibre rich diets (vegans, vegetarians) or those whose dietary patterns are characterised as being high in plant foods have greater protection against developing chronic disease.12 13
Current recommendations and dietary intakes
Recommendations around adequate intakes of dietary fibre differ around the world and by age group, but 25-30 g or more daily is widely recommended for adults.2 14 Recommended intakes were established as those required for maintaining normal laxation and cardiovascular health, although emerging evidence points to benefits extending well beyond these through modulation of the gut microbiota.15 In Europe and North America, grain based foods are the predominant contributors to dietary fibre, followed by vegetables, potatoes, and fruits, with little contribution from legumes, nuts, and seeds.2
Strikingly, a comprehensive overview of dietary fibre recommendations versus actual intakes found that only a small proportion of the global population meets the recommendations for dietary fibre intake.2 16 Why is this? In most countries, dietary guidelines emphasise foods rather than nutrients, and most people are not meeting the food based recommendations for fruits, vegetables, legumes, and whole grains, thereby falling short of their dietary fibre intake. People are unlikely to understand the type or quantity of individual foods or food combinations needed to achieve recommended dietary fibre intakes. Coupled with this, some consumers do not recognise the contribution of whole grains to fibre intake, and others do not know how to identify wholegrain, compared with refined grain, products.17 18 Despite the purported health benefits of dietary fibre, many consumers are eating highly processed, refined grains and too few fruits and vegetables, and some consumers might actively avoid carbohydrate rich foods for the health benefits purportedly associated with low carbohydrate diets. People in both situations are likely to fall short of meeting fibre recommendations. Examples of food sources of dietary fibre19 can help health professionals guide patients on selecting nutritious, carbohydrate based foods with a diversity of dietary fibre types. Advice should emphasise consuming adequate amounts of dietary fibre from various plant foods that are naturally high in fibre (box 3).
Box 3. Reaching fibre recommendations: eat a variety of plant based foods.
-
Global recommendations are to increase fruit and vegetable intake, specifically:
World Health Organization: at least 400 g (five portions) of fruit and vegetables a day
USA: two cups of fruit and 2.5 cups of vegetables for adults on diets aiming for 2000 kcal a day
UK: five a day programme (two fruit and three vegetables of 80 g each a day)
Meal plans with a target of 2000 kcal daily20 show that adults need to eat a variety of whole grains, legumes, nuts and seeds, and fruits and vegetables at meal and snack times to reach a target of 30 g or more fibre a day
Refined grain products—now widely consumed but containing low fibre levels—should be replaced with high fibre wholegrain products
Legumes (pulses) are recognised as a protein source but are often overlooked as a source of fibre, with half a cup of cooked legumes (85 g) containing, at a minimum, 4.5 g of dietary fibre
Adding one tablespoon of flax or chia seeds to salads or oatmeal will provide an estimated extra 3 g or 5 g of fibre, respectively.
Check nutrition labels to identify fortified high fibre cereals—some wheat or bran based products might have up to 11 g of dietary fibre per serving
Isolated fibres might be added to food products, most often for technological reasons (such as adding pectin to jam to make it firmer)
Foods with ≥3 g of fibre per 100 g, ≥1.5 g per 100 kcal, or ≥10% of daily reference value per serving can be named a “good source of fibre.” If twice as much fibre is present, they can be called “high fibre.”
Further information on reaching fibre goals: https://www.bda.uk.com/resource/fibre.html
Health benefits of fibre
Observational studies show that higher fibre intake has a strong protective association against risk of developing several chronic diseases, including cardiovascular disease,21 stroke,22 type 2 diabetes,23 24 colorectal cancer23 (fig 2a) and diverticular disease.27 In addition, a higher intake of fibre is linked to lower rates of cardiovascular disease and disease specific and all cause mortality (fig 2b).23 24 25 26 Consistent with this, based on two meta-analyses of data from prospective cohort studies, a 15-16% reduced risk of all cause mortality was found among people who consume high levels of fibre compared with those who consume lower levels.23 24 These analyses indicate that daily fibre intakes of 25-29 g are adequate, and intakes greater than 30 g a day would be even more beneficial.23 A growing number of people are following elimination diets that exclude fibre rich whole grains, such as “paleo,” “keto,” and gluten-free diets, and it is important to recognise that these people will lose the protective mechanisms linked to these foods, such as the cholesterol lowering and improved glycaemic control. Observational evidence indicates that higher intakes of fibre from cereal sources (that is, primarily whole grains) seem to provide a greater degree of protection against the development of type 2 diabetes (fig 2c). The observed protective associations are unlikely to be caused solely by the fibre subtypes, but rather arise from the interaction with the gut microbiota or the insulin sensitising nutrients found in whole grains.
Fig 2.
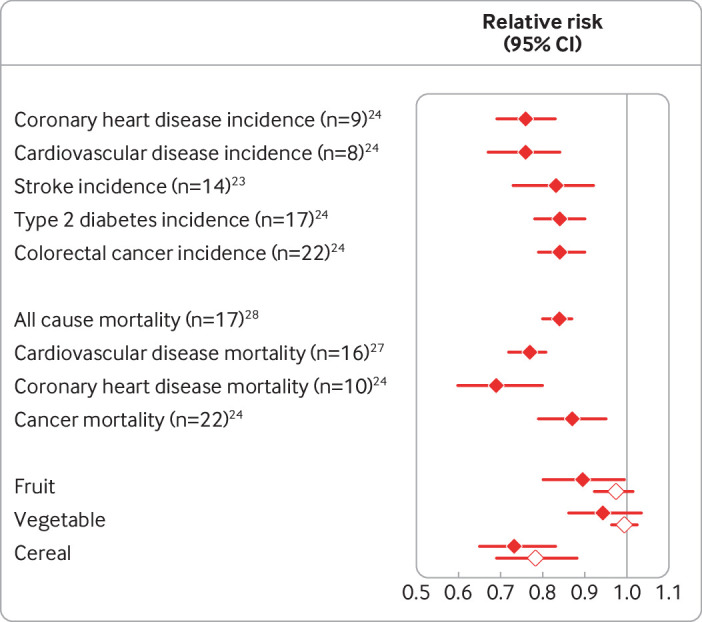
(a) Pooled relative risk estimates from meta-analysis of prospective cohort studies examining associations between dietary fibre and chronic disease risk. Mean follow-up time ranged from 9.2 years for coronary heart disease to 10.9 years for colon cancer and a median follow-up of 12 years for stroke. (b) Pooled relative risk23 25 or hazard ratio26 estimates from meta-analysis of prospective cohort studies examining the association between dietary fibre intake and mortality. Mean follow-up time ranged from 11.5 years for coronary heart disease to 13.2 years for cancer. (c) Pooled relative risks are from meta-analyses examining associations between fibre food sources and type 2 diabetes.23 Blue dots indicate the estimated risk derived from comparing the high to the low categories of dietary intake (n=10, prospective cohort), and the orange dots indicate the estimated risk derived from a dose-response analysis for 5 g cereal or 2 g fruit or vegetable (n=8, prospective cohort)
Fibre and gut health
The relation between gut microbiota and health has been extensively researched over the past decade. Many aspects of diet have been correlated with changes in microbiota composition,28 but dietary fibres have been identified as a critical determinant of gut microbiota composition and function.29 Fermentable fibres have been shown to result in distinct differences in gut microbiome composition and the production of healthy metabolites. More recently, research has shown that differences in gut microbiota composition between people lead to variability in how different fibres are fermented.30 31 Short chain fatty acids (butyrate, propionate, and acetate) derived from fermentation are crucial to health.29 These metabolites not only provide food for the colonic epithelium but can also be absorbed through the epithelium and potentially deliver a wide array of other physiological health benefits throughout the body (box 4).29
Box 4. Health promoting functions of short chain fatty acids.
Acetate
Appetite regulation
Bacterial transformation to propionate and butyrate
Enhances mucosal production and secretion
Promotes goblet cell differentiation and expression of mucin related genes
Propionate
Appetite regulation
Anti-lipogenic, cholesterol lowering
Anti-inflammatory
Anti-carcinogenic
Promotes goblet cell differentiation and expression of mucin related genes
n-Butyrate
Enhances mucosal production and secretion
Energy source for intestinal epithelial cells (contributing to health gut wall). Decreases inflammation.
In terms of “gut health,” short chain fatty acids support the immune system and help provide mucosal protection through enhancement of mucosal secretion and anti-microbial peptides. Decreased diversity in the gut microbiota, in the context of low fibre diets, not only leads to reduced short chain fatty acid production but also an increase in the amount of mucin degrading bacteria. This might lead to inflammation and make the gut susceptible to pathogenic microbe exposure or pro-inflammatory and carcinogenic metabolites, potentially leading to an increased risk of colorectal cancer (fig 3).33
Fig 3.

Effect of low and high fibre diets on gut microbiota composition, diversity, and function in host physiology.6 CVD=cardiovascular disease; CHD=coronary heart disease; CAD=coronary artery disease; T2DM=type 2 diabetes mellitus32
Fibre and inflammatory bowel disease
The implications of all sources and types of dietary fibre in the development of inflammatory bowel disease (comprising Crohn’s disease and ulcerative colitis) remain largely unknown. There is limited evidence to indicate that low fibre diets or eliminating fibre rich foods is therapeutically beneficial for the prevention or management of inflammatory bowel disease. Despite this, people with inflammatory bowel disease reportedly eat less total fibre than the general population,34 and this might in part be attributed to medical advice to reduce fibre intake. A recent meta-analysis of data from six cohort studies found no protective association between dietary fibre and risk of ulcerative colitis, but greater fruit and vegetable intake led to a 41% reduced risk in developing Crohn’s disease.35 Thus, in terms of prevention, consuming a high fibre diet that includes vegetables, fruits, whole grains, and beans is advisable,36 but questions continue about whether any particular food has a role in the development of irritable bowel syndrome.
Colorectal cancer
Based on the review of the scientific evidence, O’Keefe advocated that higher dietary fibre intake, defined as 50 g or more daily, is required to produce sufficient levels of the metabolites that support colonic health and eliminate cancer risk biomarkers in the colonic mucosa.33 Based on a recent meta-analysis of data from seven cohorts, a higher intake of whole grains, a rich source of cereal fibre has been linked to a 13% reduction in the relative risk of colorectal cancer.23 These findings are supported by a more recently published prospective cohort study with over 15 years of follow-up and >10 000 incident cases of colorectal cancer—only fibre from cereal foods (through a greater intake of whole grains) was inversely associated with colorectal cancer incidence. Dietary fibre from other sources (fruits, vegetables, and beans) or classified by type (insoluble versus soluble), had similar protective trends in this study but did not reach significance. In this cohort, people with the highest intake of whole grains (1.3 servings (around 20 g) per 1000 kcal) had a 16% lower risk of colon cancer and 24% lower risk of rectal cancer than those with the lowest wholegrain intake (0.2 servings per 1000 kcal).37 The World Cancer Research Fund recently reported that consuming whole grains and foods containing dietary fibre was associated with a lower risk of colorectal cancer.38
Can fibre supplements help fill the fibre deficit gap?
With respect to disease prevention, the first line of defence is to encourage people to meet recommended intakes with an emphasis on foods rather than supplements. For the treatment of disease, there is a lack of evidence based research to support the use of most isolated fibre types. Recommending effective fibre supplements is complicated, and only a handful of common fibre supplements have clinically shown health benefits.39 It is important to recognise that some populations find it harder to reach fibre targets. Older adults, for example, who have lower dietary energy requirements, might need to eat foods with added fibre or take a fibre supplement. Most people, however, should be able to reach dietary recommended fibre intakes through diet, which can provide a variety of fibre types with the properties and physiological health benefits described above, as well as many other important nutrients and phytochemicals that might work synergistically with fibre.
Policy suggestions to fill the fibre gap
There is little research focused on strategies specifically designed to target increasing dietary fibre intake in the population. Fibre is generally listed on processed foods, giving consumers that ability to choose foods rich in fibre. Closing the fibre gap will require consumers to choose recommended foods including fruits, vegetables, whole grains, and legumes. Many public health campaigns have promoted increasing these food groups with limited success. Continued recommendations to focus on increasing intakes of these fibre rich food groups are appealing to consumers and should result in increased fibre intakes.
Another strategy is to also target an increase in legume intake, which remains low with typical intakes of less than one serving a day.18 Recommendations to make half your grains whole and choose one pulse serving a day are more actionable for consumers.40 Policy changes that could improve fibre intake in the population include providing incentives to manufacturers to increase the availability of wholegrain and legume products, improving labelling (for example, on the front of packets), and increasing consumer outreach and education on the health benefits of fibre. Recent data from the United States indicate that consumers are still purchasing food products that contain substantially more refined grain than whole grain products, particularly those in lower income households or households with children.41 Consumer preference towards refined grain products is largely sensory based; thus, production of wheat varieties high in fibre, such as high amylose wheat, that retain the characteristics of white flour offer one strategy to increase fibre intake.42
Conclusion
The evidence is strong that healthy diets, in which fibre content is aligned with dietary recommendations, are protective against the development of cardiovascular disease, diabetes, cancer, cancer mortality, and all cause mortality.43
There is universal agreement among health professionals that fibre is an important component of the diet, and the health benefits of high dietary fibre containing diets have been recognised for some time.44 Many potential mechanisms are recognised to mediate the effects of high dietary fibre on health, either independently or synergistically with phytochemicals and nutrients in the food matrices. Continued research is needed to examine the mechanisms by which microbial diversity and changes in gut microbiota activity and bacterial enzymes influence health. In the future, experts might consider personalised dietary recommendations based on an individual’s gut microbiota composition.45 Increasing intake of dietary fibre is a highly promising nutritional target that might reduce risk of non-communicable diseases worldwide. But there is continued need for healthcare professionals and researchers to emphasise that fibre is a dietary component of public health concern, and there is an urgent need for policy efforts to target increasing dietary fibre intake in the population.
Key messages.
Higher intake of dietary fibre is associated with lower risk of several non-communicable diseases
Globally, dietary fibre intake is low, and there is a continued need for dietary advice to focus on incorporating a variety of fibre rich foods into one’s diet
Isolated and synthetic dietary fibres have different physiological health effects
Different types of fibre influence the gut microbiota composition, and changes in composition potentially deliver a diverse array of health benefits
Acknowledgments
We acknowledge the help of Caleigh Sawicki, postdoctoral research fellow at Brigham and Women’s Hospital/Harvard TH Chan School of Public Health for editorial proof reading and Kara Livingston, senior project manager, for assisting with figures, editing, and submission.
Web extra.
Extra material supplied by authors
Fibre in foods
Contributors and sources: The author group spans a wide range of expertise from nutritional epidemiology and public health to food technology, microbiology, and regulatory affairs. All authors have published in the area of dietary fibre and health, and JS, GCF Jr, and JWvdK are renowned experts in the fibre field. GCF Jr has expertise in fibre analysis and digestive physiology. JS has expertise in the role of fibre and whole grains (among other aspects of diet) in health and disease. JWvdK has expertise in food technology, microbiology, and regulatory affairs. NMM has expertise in diet and cardiometabolic disease risk. Sources of information for this article included systematic reviews and primary research articles based on randomised clinical trials, or prospective observational study designs as well as dietary guidelines. All authors contributed to drafting this manuscript, with NMM taking the lead role of writing the manuscript, and all authors providing intellectual input to improve the manuscript, as well as reading and approving the final version. NMM is the guarantor of the manuscript.
Competing interests: We have read and understood BMJ policy on declaration of interests and have the following interests to declare: NMM has received research funding from IFANS for the updating of a publicly available Dietary Fibre Database https://iafns.org/our-work/research-tools-open-data/dietary-fiber-database. NMM has in the past received funding for investigator initiated grants and for payment for serving as a consultant from General Mills Bell Institute of Health and Nutrition, speaker honorarium from Cereal Partners Worldwide, a gift-in kind to support dietary fibre research from P&G, and is an unpaid scientific adviser on the Oldways Whole Grains Council. NMM is currently supported by a grant from the NIH National Heart, Lung, Blood, and sleep disorders. GCF Jr, JS, and JWvdK have no conflict of interests to declare.
Patient involvement: No patient involvement.
Provenance and peer review: Commissioned; externally peer reviewed.
This article is part of series commissioned by The BMJ. Open access fees are paid by Swiss Re, which had no input into the commissioning or peer review of the articles. The BMJ thanks the series advisers, Nita Forouhi, Dariush Mozaffarian, and Anna Lartey for valuable advice and guiding selection of topics in the series.
References
- 1. Eaton SB. The ancestral human diet: what was it and should it be a paradigm for contemporary nutrition? Proc Nutr Soc 2006;65:1-6. 10.1079/PNS2005471 [DOI] [PubMed] [Google Scholar]
- 2. Stephen AM, Champ MM, Cloran SJ, et al. Dietary fibre in Europe: current state of knowledge on definitions, sources, recommendations, intakes and relationships to health. Nutr Res Rev 2017;30:149-90. 10.1017/S095442241700004X. [DOI] [PubMed] [Google Scholar]
- 3. Trowell H. Definition of dietary fiber and hypotheses that it is a protective factor in certain diseases. Am J Clin Nutr 1976;29:417-27. 10.1093/ajcn/29.4.417. [DOI] [PubMed] [Google Scholar]
- 4.Food and Agriculture Organization of the United Nations, World Health Organization. Codex Alimentarius. International Food Standards. Guidelines on Nutrition Labelling: CAC/GL 2-1985. https://www.fao.org/fao-who-codexalimentarius/codex-texts/guidelines/en/.
- 5. McRorie JW, Jr, McKeown NM. Understanding the physics of functional fibers in the gastrointestinal tract: an evidence-based approach to resolving enduring misconceptions about insoluble and soluble fiber. J Acad Nutr Diet 2017;117:251-64. 10.1016/j.jand.2016.09.021. [DOI] [PubMed] [Google Scholar]
- 6. Makki K, Deehan EC, Walter J, Bäckhed F. The impact of dietary fiber on gut microbiota in host health and disease. Cell Host Microbe 2018;23:705-15. 10.1016/j.chom.2018.05.012. [DOI] [PubMed] [Google Scholar]
- 7.Government of Canada. List of dietary fibres reviewed and accepted by health canada’s food directorate. 2021. https://www.canada.ca/en/health-canada/services/publications/food-nutrition/list-reviewed-accepted-dietary-fibres.html.
- 8.Center for Food Safety and Applied Nutrition. The declaration of certain isolated or synthetic non-digestible carbohydrates as dietary fiber on nutrition and supplement facts labels: guidance for industry. 2018. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-industry-declaration-certain-isolated-or-synthetic-non-digestible-carbohydrates-dietary
- 9.US Department of Health and Human Services. Questions and answers on dietary fiber. 2020. https://www.fda.gov/food/food-labeling-nutrition/questions-and-answers-dietary-fiber.
- 10. Mayor S. Eating more fibre linked to reduced risk of non-communicable diseases and death, review finds. BMJ 2019;364:1159. 10.1136/bmj.l159. [DOI] [Google Scholar]
- 11. Bechthold A, Boeing H, Schwedhelm C, et al. Food groups and risk of coronary heart disease, stroke and heart failure: A systematic review and dose-response meta-analysis of prospective studies. Crit Rev Food Sci Nutr 2019;59:1071-90. 10.1080/10408398.2017.1392288. [DOI] [PubMed] [Google Scholar]
- 12. Qian F, Liu G, Hu FB, Bhupathiraju SN, Sun Q. Association between plant-based dietary patterns and risk of type 2 diabetes: a systematic review and meta-analysis. JAMA Intern Med 2019;179:1335-44. 10.1001/jamainternmed.2019.2195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Kim H, Caulfield LE, Garcia-Larsen V, Steffen LM, Coresh J, Rebholz CM. Plant-based diets are associated with a lower risk of incident cardiovascular disease, cardiovascular disease mortality, and all-cause mortality in a general population of middle-aged adults. J Am Heart Assoc 2019;8:e012865. 10.1161/JAHA.119.012865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Scientific Advisory Committee on Nutrition. Carbohydrates and health. 2015. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/445503/SACN_Carbohydrates_and_Health.pdf.
- 15. Alexander C, Swanson KS, Fahey GC, Garleb KA. Perspective: physiologic importance of short-chain fatty acids from nondigestible carbohydrate fermentation. Adv Nutr 2019;10:576-89. 10.1093/advances/nmz004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Miketinas D, Tucker W, Patterson M, et al. Usual dietary fiber intake in US adults with diabetes: NHANES 2013-2018. Curr Dev Nutr 2021;5(Suppl 2):1061. [Google Scholar]
- 17. Wilde P, Pomeranz JL, Lizewski LJ, Zhang FF. Consumer confusion about wholegrain content and healthfulness in product labels: a discrete choice experiment and comprehension assessment. Public Health Nutr 2020;23:3324-31. 10.1017/S1368980020001688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Korczak R, Slavin JL. Definitions, regulations, and new frontiers for dietary fiber and whole grains. Nutr Rev 2020;78(Suppl 1):6-12. 10.1093/nutrit/nuz061. [DOI] [PubMed] [Google Scholar]
- 19. Hojsak I, Benninga MA, Hauser B, et al. Benefits of dietary fibre for children in health and disease. Arch Dis Child 2022;archdischild-2021-323571. 10.1136/archdischild-2021-323571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.British Nutrition Foundation. BNF’s 7-day meal plan 2020 https://www.nutrition.org.uk/healthyliving/helpingyoueatwell/7-day-meal-plan.
- 21. Wu Y, Qian Y, Pan Y, et al. Association between dietary fiber intake and risk of coronary heart disease: A meta-analysis. Clin Nutr 2015;34:603-11. 10.1016/j.clnu.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 22. Zhang Z, Xu G, Liu D, Zhu W, Fan X, Liu X. Dietary fiber consumption and risk of stroke. Eur J Epidemiol 2013;28:119-30. 10.1007/s10654-013-9783-1. [DOI] [PubMed] [Google Scholar]
- 23. Reynolds A, Mann J, Cummings J, Winter N, Mete E, Te Morenga L. Carbohydrate quality and human health: a series of systematic reviews and meta-analyses. Lancet 2019;393:434-45. 10.1016/S0140-6736(18)31809-9. [DOI] [PubMed] [Google Scholar]
- 24. Veronese N, Solmi M, Caruso MG, et al. Dietary fiber and health outcomes: an umbrella review of systematic reviews and meta-analyses. Am J Clin Nutr 2018;107:436-44. 10.1093/ajcn/nqx082. [DOI] [PubMed] [Google Scholar]
- 25. Yang Y, Zhao LG, Wu QJ, Ma X, Xiang YB. Association between dietary fiber and lower risk of all-cause mortality: a meta-analysis of cohort studies. Am J Epidemiol 2015;181:83-91. 10.1093/aje/kwu257. [DOI] [PubMed] [Google Scholar]
- 26. Liu L, Wang S, Liu J. Fiber consumption and all-cause, cardiovascular, and cancer mortalities: a systematic review and meta-analysis of cohort studies. Mol Nutr Food Res 2015;59:139-46. 10.1002/mnfr.201400449. [DOI] [PubMed] [Google Scholar]
- 27. Aune D, Sen A, Norat T, Riboli E. Dietary fibre intake and the risk of diverticular disease: a systematic review and meta-analysis of prospective studies. Eur J Nutr 2020;59:421-32. 10.1007/s00394-019-01967-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Valdes AM, Walter J, Segal E, Spector TD. Role of the gut microbiota in nutrition and health. BMJ 2018;361:k2179. 10.1136/bmj.k2179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Fehlbaum S, Prudence K, Kieboom J, et al. In vitro fermentation of selected prebiotics and their effects on the composition and activity of the adult gut microbiota. Int J Mol Sci 2018;19:E3097. 10.3390/ijms19103097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Venkataraman A, Sieber JR, Schmidt AW, Waldron C, Theis KR, Schmidt TM. Variable responses of human microbiomes to dietary supplementation with resistant starch. Microbiome 2016;4:33. 10.1186/s40168-016-0178-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. De Paepe K, Kerckhof FM, Verspreet J, Courtin CM, Van de Wiele T. Inter-individual differences determine the outcome of wheat bran colonization by the human gut microbiome. Environ Microbiol 2017;19:3251-67. 10.1111/1462-2920.13819. [DOI] [PubMed] [Google Scholar]
- 32. Zinöcker MK, Lindseth IA. The western diet-microbiome-host interaction and its role in metabolic disease. Nutrients 2018;10:E365. 10.3390/nu10030365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. O’Keefe SJ. The association between dietary fibre deficiency and high-income lifestyle-associated diseases: Burkitt’s hypothesis revisited. Lancet Gastroenterol Hepatol 2019;4:984-96. 10.1016/S2468-1253(19)30257-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Day AS, Davis R, Costello SP, Yao CK, Andrews JM, Bryant RV. The adequacy of habitual dietary fiber intake in individuals with inflammatory bowel disease: a systematic review. J Acad Nutr Diet 2021;121:688-708.e3. [DOI] [PubMed] [Google Scholar]
- 35. Milajerdi A, Ebrahimi-Daryani N, Dieleman LA, Larijani B, Esmaillzadeh A. Association of dietary fiber, fruit, and vegetable consumption with risk of inflammatory bowel disease: a systematic review and meta-analysis. Adv Nutr 2021;12:735-43. 10.1093/advances/nmaa145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Armstrong H, Mander I, Zhang Z, Armstrong D, Wine E. Not all fibers are born equal; variable response to dietary fiber subtypes in IBD. Front Pediatr 2021;8:620189. 10.3389/fped.2020.620189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Hullings AG, Sinha R, Liao LM, Freedman ND, Graubard BI, Loftfield E. Whole grain and dietary fiber intake and risk of colorectal cancer in the NIH-AARP Diet and Health Study cohort. Am J Clin Nutr 2020;112:603-12. 10.1093/ajcn/nqaa161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.World Cancer Research Fund, American Institute for Cancer Research. Diet, nutrition, physical activity and cancer: a global perspective. continuous update project expert report. 2018. https://www.wcrf.org/diet-activity-and-cancer/
- 39. McRorie J, Fahey G. Fiber supplements and clinically meaningful health benefits: identifying the physiochemical characteristics of fiber that drive specific physiologic effects. In: Taylor C, ed. The CRC Handbook on Dietary Supplements in Health Promotion. CRC Press, 2015. [Google Scholar]
- 40. Reyneke G, Hughes J, Grafenauer S. Consumer understanding of the Australian dietary guidelines: recommendations for legumes and whole grains. Nutrients 2022;14:1753. 10.3390/nu14091753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Dunford EK, Miles DR, Popkin B, Ng SW. Whole grain and refined grains: an examination of US household grocery store purchases. J Nutr 2022;152:550-8. 10.1093/jn/nxab382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Harris K, Overcash F, Belobrajdic D, Slavin J. Perspective: utilizing high amylose wheat flour to increase dietary fiber intake of children and adolescents: a health by stealth approach. Front Public Health 2022;10:817967. 10.3389/fpubh.2022.817967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Miller V, Webb P, Micha R, Mozaffarian D, Global Dietary Database . Defining diet quality: a synthesis of dietary quality metrics and their validity for the double burden of malnutrition. Lancet Planet Health 2020;4:e352-70. 10.1016/S2542-5196(20)30162-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Burkitt DP, Walker AR, Painter NS. Dietary fiber and disease. JAMA 1974;229:1068-74. 10.1001/jama.1974.03230460018013. [DOI] [PubMed] [Google Scholar]
- 45. Kolodziejczyk AA, Zheng D, Elinav E. Diet-microbiota interactions and personalized nutrition. Nat Rev Microbiol 2019;17:742-53. 10.1038/s41579-019-0256-8. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fibre in foods