

Abstract
Background
The life expectancy of people with intellectual disabilities has increased. The implications of ageing have resulted in changes in their support needs and challenges to support staff. Access to evidence based strategies for support staff providing care to elderly with intellectual disabilities remains scarce. A systematic review was conducted to provide an overview of available psychosocial interventions.
Methods
Four databases were searched and assessed according to the PRISMA guidelines. A narrative, integrative method of analysis was conducted to synthesise quantitative and qualitative data.
Results
The 36 studies included in the review reported on interventions aimed at either identifying and meeting the needs or perceptions of older individuals or at improving their behaviour and skills. Furthermore, the role of support staff in the implementation of interventions was either active, assisting or undefined.
Conclusions
This overview of studies could contribute to the existing body of knowledge and help to optimise psychosocial support for a growing population.
Keywords: ageing, intellectual disability, psychosocial interventions, support, systematic review
1. INTRODUCTION
Similar to the dynamics of ageing in the general population, the life expectancy of people with intellectual disabilities is increasing, due to improved living conditions and better medical care (Mulryan et al., 2021). The ageing process is different for older people with intellectual disabilities, however, as their lifelong disabilities place them at increased risk of developing age‐related deficiencies (e.g., multiple chronic health impairments, including cardiovascular and respiratory issues) at a relatively young age (Hermans & Evenhuis, 2014). Furthermore, the occurrence of psychotic disorders is 10 times higher for older people with intellectual disabilities, who are also more likely to experience dementia, personality disorders, anxiety and mood disorders, as compared to the general population (Axmon et al., 2017; Hermans et al., 2013). The early onset of age‐related physical and cognitive declines is especially common amongst individuals with severe or multiple impairments or specific genetic syndromes (e.g., Down syndrome) (Coppus, 2013). In summary, older people with intellectual disabilities are considered a particularly vulnerable group. Their ageing processes are relatively complex and, as such, they pose challenges to their overall healthcare (WHO, 2018).
The early onset and complexity of the ageing process result in changes to the support needs of people with intellectual disabilities as they grow older. For example, older people with intellectual disabilities require more assistance with daily living skills (e.g. personal hygiene) and maintaining acquired skills, and they are likely to need adjustments in the frequency and pace of daytime activities to correspond to their current abilities (Shooshtari et al., 2011; Thalen et al., 2021). In addition to posing new challenges for older people with intellectual disabilities and their families, the implications of ageing pose challenges to support staff and healthcare organisations (e.g., mental health problems; Prasher et al., 2021). A different approach is needed in order to ensure optimal care and support. Along with the changing support needs of older people with intellectual disabilities, the capacities of their social networks to provide active support are likely to decrease, as their contacts are ageing as well (McCausland et al., 2016). In addition, older people with intellectual disabilities face the loss of loved ones, and many have no partner or children to care for them later in life (Ryan et al., 2014). Such changes in social networks intensify their appeal to support services, thus making them increasingly dependent on support staff to maintain their quality of life (QoL) (Thalen et al., 2021).
It is unclear whether support staff are prepared for their significant role in meeting the changing support needs of older people with intellectual disabilities (Kåhlin et al., 2016). Although many Western countries have a long tradition of supporting older people (e.g., through person‐centred care), access to evidence‐based support strategies remains scarce (Alftberg et al., 2021; Innes & McCabe, 2012). Moreover, most available interventions are medically/physically oriented and aimed at assessing effects within the physical domain of well‐being (e.g., a treadmill walking programme to improve leg muscle strength; changing medication to decrease the risk of falling; Schepens et al., 2019). The implications of ageing extend beyond physical deficiencies (i.e., physical well‐being), however, and the need for support in other domains of life (e.g., social well‐being) are likely to change as well (X. et al., ). For this reason, interventions other than those of a medical nature are also relevant to the support of older people with intellectual disabilities. Additional knowledge regarding available psychosocial interventions that can help to optimise support for older people with intellectual disabilities would be beneficial, especially for support staff who must address the changing support needs of older people with intellectual disabilities on a daily basis.
To help address this gap in the available knowledge, we conducted a systematic literature review aimed at providing an overview of existing non‐pharmacological and non‐physical interventions for older people with intellectual disabilities. We directed particular attention to the various foci of psychosocial interventions and the role of support staff in the application of these interventions. The central research questions in this review study are as follows:
What is the focus of the psychosocial interventions documented in the international literature for serving older people with intellectual disabilities?
What role do support staff have in the application of these psychosocial interventions?
2. METHOD
2.1. Search strategy
In accordance with the PRISMA statement (Liberati et al., 2009), the databases of Embase, Psych INFO, MedLine and Cochrane were systematically searched on 12 April 2019, using a search string constructed with assistance from an experienced information specialist. To be included, studies had to be published in English in peer‐reviewed journals between January 2000 and April 2019. An updated search was conducted on 24 September 2020. Table 1 provides an overview of the search terms and strategy that were employed in the Embase database, using Emtree terms (i.e., a controlled vocabulary thesaurus used for indexing papers) and additional text words for ‘ageing’, ‘intellectual disability’ and ‘(psycho) social wellbeing’. The other databases use similar thesaurus systems (e.g., Medline uses MeSH terms). We used these terms, as we were interested in sourcing all studies that applied psychosocial interventions to older people with intellectual disabilities (Bramer et al., 2017).
TABLE 1.
Search strategy for Embase database
| Embase final search strategy |
| ('intellectual impairment'/de OR 'mental deficiency'/exp OR 'learning disorder'/de OR 'mentally disabled person'/de OR 'developmental disorder'/de OR (((intellect* OR learning OR development*) NEXT/1 (defect* OR deficit* OR deficien* OR dysfunction* OR disab* OR impair* OR disorder* OR retard* OR handicap*)) OR ((mental*) NEXT/1 (defect* OR deficit* OR deficien* OR dysfunction* OR disab* OR impair* OR handicap*)) OR retard* OR idiocy OR (down* NEAR/3 syndrome*) OR prader‐willi OR fragile‐x):ab,ti,kw) AND ('aged'/exp OR 'middle aged'/exp OR 'aging'/de OR 'dementia'/de OR 'elderly care'/de OR (elder* OR ((aged OR older) NEAR/6 (care OR subject* OR person* OR adult* OR women OR woman OR female* OR men OR man OR male*)) OR very‐old* OR frail* OR old*‐age* OR oldest‐old* OR ((aged OR older) NEXT/1 (people OR subject* OR person* OR population*)) OR senior* OR dementia OR aging OR ageing OR late‐life):ab,ti,kw) AND ('quality of life'/exp OR 'wellbeing'/de OR 'psychological well‐being'/de OR 'personal development'/de OR 'self determination'/de OR 'autonomy'/de OR 'personal autonomy'/de OR 'human relation'/de OR 'social participation'/de OR 'daily life activity'/exp OR 'adaptive behavior'/exp OR 'social adaptation'/exp OR 'social competence'/exp OR 'social interaction'/de OR independence/de OR 'self esteem'/de OR 'self concept'/de OR 'satisfaction'/de OR ((quality NEAR/3 life) OR wellbeing OR well‐being OR (adapt* NEAR/3 behav*) OR (psychological* NEAR/3 adjustment*) OR wellness OR (personal NEAR/3 development) OR self‐determin* OR autonomy OR ((human OR personal* OR interpersonal* OR social*) NEAR/3 (relation* OR interaction* OR contact)) OR ((social* OR communit*) NEAR/3 (participat* OR abilit* OR skill* OR adapt* OR competenc* OR interaction*)) OR ((everyday* OR every‐day* OR daily) NEAR/6 (activit* OR participat*)) OR existential* OR meaningfull OR independence OR (self NEXT/1 (esteem OR image)) OR relaxation OR relatedness OR comfort OR satisfied OR satisfying OR satisfaction*):ab,ti,kw) NOT (parent/exp/mj OR (child* OR young*‐adult* OR parent* OR mother* OR father* OR paternal):ti) NOT (juvenile/exp NOT adult/exp) NOT ([animals]/lim NOT [humans]/lim) NOT ([Conference Abstract]/lim) AND [English]/lim |
2.2. Study selection
To determine the inclusion and exclusion criteria and achieve an accurate and structured selection of studies, we applied the approach of Population, Intervention, Comparison, Outcomes and Study Design(s) (PICOS; Liberati et al., 2009), as shown in Table 2. Population was specified as older people (≥50 years of age) with intellectual disabilities. The age criterion was chosen in line with Hermans and Evenhuis (2014), in order to account for premature ageing and the early onset of age‐related deficiencies. No distinction was made between specific sub‐groups within the population of older people with intellectual disabilities (e.g., Down syndrome, dementia or level of functioning). Three additional criteria were applied for the inclusion of studies involving participants both older and younger than 50 years: (1) separate results for the participants of ≥50 years, or (2) a specific focus on the population of ageing people with intellectual disabilities (in those cases, a lower age limit of ≥40 years was allowed) or (3) evidence that there were no statistically significant differences between the younger and older participants. With regard to the intervention, studies were required to address psychosocial, non‐medical/physical interventions. The comparison component was not applicable to this review. The outcome of studies referred to all possible measures that directly or indirectly concerned an aspect of the psychosocial well‐being of older people with intellectual disabilities. Finally, in light of the research questions and the aim of this review, both quantitative, qualitative and mixed‐method studies were included, and therefore the study design component referred to all empirical studies.
TABLE 2.
Inclusion and exclusion criteria applied in the present study
| Inclusion criteria |
|
|
|
|
| Exclusion criteria |
| Participants |
|
|
|
| Intervention |
|
|
|
| General |
|
|
|
The selection process for studies consisted of four phases: identification, screening, eligibility and inclusion (see Figure 1). In the identification phase, records were identified in four different databases, according to the search strategy described above, and duplicates were eliminated. This phase was followed by a two‐step process for screening the remaining 5378 studies. In the first step, each study was screened independently based on the exclusion criteria (see Table 2) by the first author and one of two senior researchers experienced in conducting and supervising systematic reviews on title and abstract (Pair 1: MT and WvO; Pair 2: MT and KV). Studies clearly meeting the exclusion criteria (e.g., studies about the general population or review studies) were excluded. The agreement between the three researchers was 96.9%. In case of disagreement within pairs, the third researcher was consulted or, when in doubt, the study was included for further assessment of the full text.
FIGURE 1.
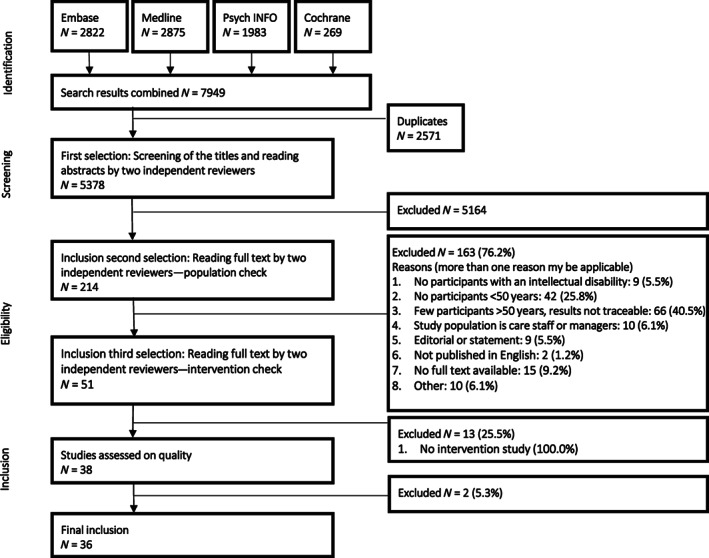
Flowchart of the study selection for this systematic review
In the eligibility phase, the remaining studies were distributed amongst the same pairs for independent review of the full text. In this phase, 214 full‐text articles were assessed based on both the inclusion and the exclusion criteria (see Table 2). The agreement between the three researchers was 92.0%. Disagreements regarding full‐text articles were first discussed with a third researcher to reach consensus. In case of persistent doubt and complex decisions, a fourth researcher (PE) was consulted until full consensus was reached. After the full‐text studies were included, the reference lists of these remaining articles were hand searched and checked by the first author for potentially other relevant intervention studies. This resulted in the screening of two additional full‐text articles, which were assessed for eligibility according to the methods outlined above.
Finally, in the inclusion phase, the authors assessed the quality of the 38 eligible studies based on the Multi‐Method Appraisal Tool (MMAT, Hong et al., 2018). This instrument can be used to assess the quality of studies with different research designs. It has demonstrated good content validity and reliability (Pluye et al., 2011). The appraisals were discussed by three authors (MT, WvO and KV), and the quality criteria were rated as either positive or negative. In case of persistent doubt and complex decisions, a fourth researcher (PE) was consulted until full consensus was reached. Studies with a negative score on at least one of two MMAT screening questions or negative scores on all five MMAT quality criteria were classified for exclusion. As a second check, studies that had been classified for exclusion were assessed by an independent researcher experienced in conducting systematic reviews. If the independent researcher confirmed the absence of positive scores on MMAT indicators, the study was excluded from further analysis (see Figure 1). As a result, two studies with lower‐than‐acceptable quality were eliminated from further analyses, in accordance with the MMAT guidelines. Finally, outcome scores of the remaining studies were converted to three levels of quality: high (score 5 out of 5), moderate (score 3 or 4 out of 5) and low (score 1 or 2 out of 5) (see Table 3).
TABLE 3.
Characteristics of the included studies
| Author (year); country | Study design; MMAT score | Older participants | Study aim | Intervention; duration | Practitioners | Role of support staff | Outcome measures | Results |
|---|---|---|---|---|---|---|---|---|
| 1. Anderson and Kazantzis (2008); NZ | Multiple single‐case; Low (2/5) | N = 1 male with a mild intellectual disability and schizophrenia, ≥50 years | To evaluate a social problem‐solving training on an individual basis | Social problem‐solving skills training; 15 sessions | Psychologists | Assisting | AAMR (Nihira et al., 1993); Adapted Anxiety Inventory (Lindsay & Michie, 1988); Adapted Zung Depression Scale (Reiss & Benson, 1985); Adapted Rosenberg Self‐esteem Scale (Dagnan & Sandhu, 1999); Social Problem‐Solving Skills Measure (Loumidis, 1993) | All participants showed improvement in social problem‐solving skills (0.47%–0.57% change), and two participants showed improvement in depression (0.31%–0.40% change). No effects were found for anxiety or self‐esteem. Improvement was maintained at 4‐week follow‐up. |
| 2. Bai et al. (2014); HK a | Quasi‐experimental research; Moderate (4/5) | N = 32, 15 males and 17 females with mild to moderate intellectual disabilities, ≥50 years | To develop a training protocol of LSWp designed especially for older adults with mild‐to‐moderate levels of intellectual disability, and to evaluate the effectiveness of LSW | Life Story Work programme (LSWp); 6 months | Support staff (LSWp instructors) | Active | MIPQ (Ross & Oliver, 2003); VABS (Sparrow et al., 2005); PWI‐ID (Cummins & Lau, 2005) | The LSWp showed potential for improving QoL and preventing loss of interest and pleasure for older adults with intellectual disabilities. It also showed promise for enhancing their socialisation skills. Participants with better communication skills seemed to benefit more from the LSWp. |
| 3. Bidwell and Rehfeldt (2004); USA | Multiple‐baseline across three participants; Moderate (4/5) | N = 1 female with a severe intellectual disability, ≥50 years | To determine whether adults with severe mental retardation would acquire, generalise and maintain a domestic skill with an embedded social initiation by observing a model on a computer demonstrating the chained task | Video modelling intervention; 30 sessions | Researchers | Undefined | Observations of the percentage of steps performed accurately during baseline sessions and with regard to intervention, generalisation, and maintenance probes | All participants mastered the task and demonstrated generalisation across settings, stimuli and people. |
| 4. Brooks and Paterson (2010); UK | Observational (qualitative); Low (2/5) | N = 1 male with an intellectual disability and autistic spectrum disorder, ≥50 years | To consider the usefulness of using contact work with adults with learning disabilities and autistic spectrum disorders living in a residential setting | Contact work; 8 sessions | Speech and language therapists | Undefined | Observations using a measurement tool based on the categorisation of Prouty et al. (2002) | The data collected suggest that the approach had an immediate impact on the participant's contact behaviours, but it did not result in carry‐over from one session to another or to different contexts. |
| 5. Bucholz et al. (2008); USA a | Multiple‐baseline across periods; Moderate (4/5) | N = 1 male with an intellectual disability and Down syndrome, ≥50 years | To expand the body of research on the use of social stories and Literacy‐Based Behavioural Interventions, and on the improvement of work behaviour | Literacy‐based behavioural intervention; 22 sessions | Support staff | Active | Observations during baseline and intervention sessions | The participant made substantial improvements in his work behaviour as a result of the LBBI. It could be useful for reducing prompt dependence and increasing timely return to work. |
| 6. Chng et al. (2013); AUS a | Non‐concurrent multiple‐baseline across participants: Moderate (3/5) | N = 3 females with moderate intellectual disabilities, ≥50 years | To evaluate whether training mentors in Active Mentoring would yield (1) increased engagement in mainstream community group activities by older adults with ID, and (2) increase help from mentors for participation | Active mentoring; Active support style training intervention; n/a | Support staff, group members and volunteers | Assisting | Observations during community group activities using software (MOOSES; Tapp, 2009) | Active mentoring was effective in improving activity engagement, while showing no effect on social engagement. Overall, increases were observed in total engagement, supported engagement and independent activity engagement, relative to pre‐test. |
| 7. Conklin and Mayer (2011); USA | Multiple‐baseline across three participants; Moderate (4/5) | N = 1 female with a severe intellectual disability, ≥50 years | To document the outcomes of the learning and use of PECS, and to monitor associated target behaviours | Picture Exchange Communication System (PECS); 20 sessions | Researchers and students | Undefined | MAS (Durand, 1990) and observations during baseline, intervention and follow‐up sessions | Participants taught through the PECS increased their initiation of requests, thereby enhancing their independence and choice‐making. However, the majority of participants did not master all phases. |
| 8. Cooper and Browder (2001); USA a | Multiple‐baseline; High (5/5) | N = 8, six males and two females with severe to profound intellectual disabilities or dual diagnosis of mental retardation and mental illness, ≥46 years* | To utilise a self‐management staff‐training package to teach staff members to use the least intrusive assistance and honour choice in a community‐purchasing routine, and to evaluate the effect of the level of staff assistance on the learner's level of independent response | Multi‐component staff training package; n/a | Support staff | Active | Observations during baseline, post‐intervention and maintenance sessions | After staff members had received the intervention, participants increased the number of choice responses they made, in addition to enhancing their level of performance. |
| 9. Crook et al. (2016); UK a | Randomised single‐case series; Moderate (4/5) | N = 5, two males and three females with intellectual disabilities and dementia, ≥50 years | To evaluate aspects of Reminiscence Therapy in the form of life‐story books and rummage boxes, as compared to no intervention | Life‐story book and rummage box; 9 sessions | Researchers | Assisting | DCM (Bradford Dementia Group, 2005) | Combined data for all participants indicated that the two reminiscence conditions were associated with higher well‐being scores, as compared to the no‐intervention condition. |
| 10. Crowley et al. (2008); UK | Pre‐test/post‐test; Moderate (3/5) | N = 2 males with mild intellectual disabilities and a diagnosis of schizophrenia or bipolar disorder, ≥50 years | To evaluate a psychoeducation group programme by adapting programmes developed within the context of mental health services | Psychosis and intellectual disability psycho‐educational groups; 6 sessions | Group leaders | Assisting | Crown Self Esteem Scale and ‘What Do You Know about Psychosis?’ Questionnaire based on existing questionnaires (Smith & Birchwood, 1990) | All participants completed the programme and measures of psychosis knowledge showed increases post‐group. However, data on the measures were not collected from all participants (1 older person). |
| 11. Cuvo et al. (2001); USA | Controlled‐experimental; Moderate (3/5) | N = 2 males with profound intellectual disabilities, ≥50 years | To test the effect of a room with sensory equipment (i.e., Snoezelen Room) on stereotypical behaviour and engagement, as compared to a living room or outdoor activities | Snoezelen room; 12–18 sessions | Researchers | Undefined | Observations during baseline and intervention sessions | An increase in engagement was observed for the two older individuals (Snoezelen Room vs. living room), along with a decrease in stereotypical behaviour (outdoors, Snoezelen Room vs. living room). |
| 12. Darling and Circo (2015); USA | Multiple‐baseline across participants; Moderate (3/5) | N = 2, one male and one female with profound multiple intellectual disabilities, ≥50 years | To assess whether the repeated presentation of preferred items and activities during multiple periods of the day increases scores on happiness indices | Presenting preferred items and activities; 7–12 sessions | Support staff | Active | Observations during baseline and intervention sessions | The presentation of preferred items and activities increased scores on the indices of happiness, as compared to baseline rates. |
| 13. Dollar et al. (2012); USA | Multiple‐probe across three behaviours; Moderate (3/5) | N = 1 male with a severe intellectual disability, ≥50 years | To examine the effectiveness of simultaneous prompting to teach chained tasks (i.e., independent living and leisure skills) to individuals in their home environments | Simultaneous prompting; 28 sessions | Researchers | Undefined | Observations during baseline, intervention and maintenance sessions | Simultaneous prompting was effective in teaching independent living skills, but modifications were made throughout this study to reduce the number of errors during instructional and probe sessions. |
| 14. Fox et al. (2009); USA | Case series; Moderate (4/5) | N = 1 male with a severe intellectual disability and autistic disorder, ≥50 years | To conduct a pilot study of an accommodation programme for adults with autism, severe to profound mental retardation and significant behaviour problems | A community‐based accommodation programme; 5 years | Support staff | Active | Observations using daily data sheets during the baseline period and each year of participation in the programme | Following three to 6 years of participation in the accommodation programme, a significant treatment‐effect size was obtained for all participants (80% reduction in the targeted behaviour). |
| 15. Golisz et al. (2018); USA | Double‐baseline case study; Moderate (4/5) | N = 1 male with a moderate intellectual disability, ≥50 years | To address the limited evidence of the potential effectiveness of an approach involving the selection of activities and goals in order to support learning for adults with intellectual disabilities in the completion of a selected ADL task using ordinary technology | Task‐specific learning support; 1 month | Occupational therapy graduate students | Undefined | Modified participant‐centred interview (Law et al., 1998); BRIEF‐A (Goia et al., 2000) and direct performance‐based observations during baseline, intervention and post‐intervention | The functional performance of all participants on a task related to an activity of daily living improved in terms of accuracy and efficiency as cues from support workers were tapered off. |
| 16. Harper et al. (2013); USA | Multiple‐baseline across subjects; Moderate (4/5) | N = 1 male with a severe intellectual disability, ≥50 years | To evaluate a series of treatments designed to replace social avoidance with appropriate forms of social interaction | (a) vicarious reinforcement, (b) conditioning of social interactions, (c) stimulus fading, and (d) DRA plus EXT; 45 sessions in total | Therapists | Undefined | Observations during baseline and intervention sessions | DRA plus EXT was the only condition in which decreases in problem behaviour and increases in social interactions were observed reliably. Not all phases were implemented. |
| 17. Hoffman et al. (2019); NL | Pre‐experimental within‐group; Moderate (4/5) | N = 3 males with mild‐to‐moderate intellectual disabilities and visual impairment, ≥50 years | To determine the efficacy of technology‐assisted therapy for separation anxiety in reducing separation anxiety and challenging behaviour | Technology assisted therapy for separation anxiety; 17 to 18 weeks | Support staff | Active | ABCL (Tenneij & Koot, 2007); BSI (Wieland et al., 2012); PIMRA (Van Minnen et al., 1994); IDQOL (Hoekman et al., 2001) | Indications that the separation anxiety and challenging behaviour experienced by the participants decreased significantly, while their psychosocial functioning and QoL increased significantly. |
| 18. Horovitz et al. (2010); USA a | Case study; Moderate (3/5) | N = 1 male with Down syndrome, profound intellectual disability, dementia and anxiety disorder, ≥50 years | To examine the effects of using contingent reinforcement of compliance as an intervention | Compliance training; 16 weeks | Therapists and support staff | Assisting | Functional Assessment Interview (O'Neill et al., 1997); Questions about Behavioural Function Scale (Singh et al., 2009) and observations during baseline, intervention and follow‐up sessions | Non‐compliance had decreased by 85.22% at follow‐up. |
| 19. Kruithof et al. (2018); NL | Theory‐based evaluation (qualitative research); Low (2/5) | N = 8, six males and two females with mild intellectual disabilities, ≥50 years | To bridge the knowledge gap regarding group‐oriented interventions intended to include the socially excluded in general and, more specifically, regarding social work interventions aimed at expanding networks and increasing societal participation | The communal table (social network intervention); 6–18 months (1 session per month) | Support staff | Active | Observations using field notes and interviews with participants | Although participants experienced conviviality and warmth, the intervention neither fulfilled its intended aims of expanding social networks and/or increasing societal participation, nor did these intended effects match the participants' motivations for participation. |
| 20. Lifshitz and Klein (2011); ISR a | Mixed‐method; Low (2/5) | N = 1 male with an intellectual disability, Down syndrome and dementia, ≥50 years | To describe a new method of mediation between staff members and adults with intellectual disabilities, and between staff members and elderly people with intellectual disabilities, either with or without dementia; MISC model | Mediational Intervention for Sensitising Caregivers (MISC); one time implementation | Support staff | Active | DRM (Evenhuis et al., 1990) and observations | Although the participant's memory difficulties remained, his daily life became somewhat easier and less stressful. He was able to learn new strategies to compensate for the deterioration in his short‐term memory and orientation in time and space. |
| 21. Martens et al. (2017); NL | Multiple‐baseline across subjects; Moderate (4/5) | N = 1 male with an intellectual disability and congenital deaf blindness, ≥50 years | To examine whether the IMAI‐based intervention is effective for people with congenital deaf blindness and intellectual disabilities | Intervention Model of Affective Involvement (IMAI); 20 sessions | Support staff | Active | Observations during baseline, intervention and follow‐up sessions | Indications that affective involvement increased after communication partners had been trained. |
| 22. Marwood and Hewitt (2012); UK | Mixed‐method; Moderate (3/5) | N = 2, one male and one female with mild intellectual disabilities and anxiety issues, ≥50 years | To investigate the effectiveness of a cognitive behavioural group intervention for individuals with learning disabilities who are experiencing anxiety | Anxiety group (cognitive behavioural therapy); 6 sessions | Psychologists | Assisting | Quality of Life Scale (Andrews & Withey, 1976); Glasgow Anxiety Scale (Mindham & Espie, 2003); HoNOS‐LD (Roy et al., 2002) and interviews with participants | Indications that the intervention was successful in treating anxiety for people with intellectual disabilities. However, no follow‐up was conducted, but interviews were held. |
| 23. McManus et al. (2014); IER | Case series; Moderate (3/5) | N = 3, two males and one female with mild intellectual disabilities and a chronic pain condition, ≥50 years | To examine the utility of some of the standard components of cognitive behavioural therapy for pain management, modified for use with people with intellectual disabilities | Feeling better (cognitive behavioural therapy for chronic pain in people with intellectual disabilities); 8 sessions | Psychologists | Assisting | The Pain Self‐Efficacy Scale for children (Bursch et al., 2006); Wechsler Abbreviated Scale for Intelligence (Wechsler, 1999); Pain Knowledge Scale; Coping Strategies questionnaire | Indications that participant scores on pain management knowledge, wellness‐focused coping and effectiveness of coping increased following intervention. However, these gains were generally not maintained at follow‐up. The intervention did not have the predicted beneficial effect on self‐efficacy or reduced use of illness‐focused coping strategies. |
| 24. Mevissen et al. (2011); NL | Case study (qualitative research); Moderate (3/5) | N = 1 female with a moderate to mild intellectual disability and PTSD, ≥50 years | To explore the applicability and efficacy of EMDR in people with mild intellectual disabilities who have experienced various types of negative life events | EMDR treatment; 13 sessions | Clinical psychologists | Assisting | Observations | In all cases, PTSD symptoms decreased, and the outcomes suggest the applicability of EMDR. Treatment effects remained at follow‐up and appeared to be most beneficial for the older person. |
| 25. Raftery et al. (2017); IER | Case studies; Low (2/5) | N = 2, one male and one female with mild intellectual disabilities and psychosis, ≥50 years | To ascertain the clinical benefits of an IPS programme over an 18‐month period and to examine its cost‐effectiveness | Intensive Personalised Support (IPS); 18 months | Researchers (IPS workers) | Undefined | CANDID‐R (Xenitidis et al., 2000); AMPS (Fisher et al., 2010); SAI‐E (Sanz et al., 1998), GAF (Spitzer et al., 1994); LQoLP‐EU (Van Nieuwenhuizen et al., 2001); BAI (Beck et al., 1988); Mental Health Recovery Star (Killaspy et al., 2012) | Reductions in psychopathology including anxiety symptoms, increased functioning and QoL were noted in all individuals. The IPS approach was clinically effective, particularly in addressing the psychosocial needs, psychological functioning, daily living skills and overall QoL of the participants. |
| 26. Randle‐Philips et al. (2016); UK | Mixed‐method; Low (2/5) | N = 1 female with an intellectual disability, ≥50 years | To explore whether an adapted tree‐of‐life narrative approach helped people with intellectual disabilities | Tree‐of‐life group (narrative therapy); 5 sessions | Clinical psychologists | Undefined | CORE‐LD (Brooks et al., 2013); Adapted Rosenberg Self‐Esteem Inventory (Dagnan & Sandhu, 1999); Tree of Life Questionnaire | No change was found on the quantitative measures of well‐being and self‐esteem. Participants reported benefitting from the peer support and social connectedness that the group offered, especially in relation to themes of loss and change in their lives. |
| 27. Samuel et al. (2008); UK | Multiple‐baseline across time‐series; Moderate (3/5) | N = 1 female with a profound intellectual disability, ≥50 years | To address a gap in the accumulated evidence on the effectiveness of Intensive Interaction | Intensive Interaction; 55 sessions | Support staff | Active | PVCS (Kiernan & Reid, 1987); questionnaire based on Interactive Sequence (Downs & Craft, 1997) and Physical Sociability Scale (Kellet, 2001); observations | Slight improvements or gains in communication and social abilities were noted. However, each participant developed differently. There was less evidence for improved quality of relationship. |
| 28. Schaap et al. (2019); NL a | Quasi‐experimental; High (5/5) | N = 113, 64 males and 49 females with intellectual disabilities and a mean age of 67 years | To examine the effect of DCM, as compared to care as usual, on the well‐being and QoL of older clients with intellectual disabilities | Dementia Care Mapping; 2 sessions | Support staff (DCM mappers) | Active | MIPQ (Petry et al., 2010); Quality of Living‐Questionnaire (CCE, 2013) | DCM achieved no significantly better or worse QoL than did care as usual. |
| 29. Stancliffe et al. (2015); AUS a | Pre‐test/post‐test; Moderate (4/5) | N = 29, 18 males and 11 females with intellectual disabilities, ≥46 years* | To examine the feasibility, types and duration of the attendance of participants in a mainstream community group, and to examine the outcomes of such attendance | Active mentoring; 3–6 months | Mentors (volunteers) and support staff | Assisting | HRQOL (Ware et al., 1993); UCLA Loneliness Scale (Russel, 1996); Worker Loneliness Questionnaire (Chadsey‐Rusch et al., 1992); GDS (Cuthill et al., 2003); Mini PAS‐ADD (Moss et al., 1998) and weekly logs | The members of the intervention group increased their community participation, made new social contacts and decreased their working hours. Intervention participants were more socially satisfied post‐intervention than were the members of the comparison group. |
| 30. Stannis et al. (2019); USA | Non‐current multiple‐baseline across participants; Low (2/5) | N = 1 male with a severe intellectual disability, ≥50 years | To evaluate a behavioural‐skills training programme that teaches adults with intellectual disabilities a response to bullying, and to evaluate in‐situ training if the skills taught in behavioural‐skills training fail to generalise to the natural environment | Behavioural skills and in situ training; 11 sessions (15–30 min) | Researchers | Assisting | Observations during baseline, intervention and follow‐up sessions | Behavioural‐skills training alone was successful in teaching the response to bullying to two participants. When behavioural skills training did not result in the use of the response to bullying, in‐situ training was effective for one participant, and in‐situ training plus an incentive was partly effective for the older person. |
| 31. Taber‐Doughty et al. (2010); USA | Single‐case, alternating treatment; Moderate (4/5) | N = 2, one male and one female with mild intellectual disabilities, ≥50 years | To evaluate and compare the effectiveness and efficiency of prompting when provided by on‐site standard care and by remote telecare staff on the independent performance of consumers when completing a series of novel, functionally related household tasks in their own homes | (Auditory) prompting; 20 sessions | Support staff | Active | Observations during baseline, intervention and follow‐up sessions | Telecare support had a positive effect and resulted in a greater percentage of task steps completed independently and greater levels of independent task performance for each task. |
| 32. Underwood et al. (2009); USA | Multiple‐baseline across subjects; Moderate (3/5) | N = 1 male with an intellectual disability, ≥50 years | To examine the efficacy of a systematic process for matching behavioural interventions to assessed function (or functions) of problem behaviour in a community‐based day programme | Function‐Based interventions; 8 weeks | Researchers and support staff | Assisting | Observation during baseline, intervention and maintenance sessions | The mean response rates of all the participants' replacement behaviours (appropriate interactions) increased immediately when the intervention was introduced, whereas the mean response rates of their target behaviours decreased. |
| 33. Van Puyenbroeck and Maes (2009); BE a | Quasi‐experimental pre‐test/post‐test; High (5/5) | N = 41, 17 males and 24 females with mild to moderate intellectual disabilities, ≥50 years | To evaluate the effect and goal attainment of a narrative‐reminiscence group programme | Reminiscence Group Work; 12 sessions | Researchers and support staff | Assisting | IDQOL (Hoekman et al., 2001); PSPC (Goverts et al., 2001); MIPQ (Ross & Oliver, 1999); FFPI (Hendriks et al., 1999); VITESSA (Van Puyenbroeck et al. 2005), interviews with participants and a group evaluation | No changes were detected in life satisfaction or perceived self‐competence. Mood did not yield an experimental treatment effect, but a significant increase in scores was observed over time. Interviews resulted in positive appraisals (i.e., worthwhile and meaningful). |
| 34. Vlaskamp and van der Putten (2009); NL | Quasi‐experimental; Moderate (4/5) | N = 3, one male and two females with profound multiple intellectual disabilities, ≥50 years | To determine how ISP actually works in practice | Individualised Support Programmes (ISPs); 2 years | Support staff | Active | QES (Zijlstra, 2003) | The effects on all participants were generally positive for aspects of communication, mood, contact, interaction and alertness. In addition, age had no significant influence on the number or content of the goals that were set. |
| 35. Wagemaker et al. (2017); NL a | N = 1 study; Low (2/5) | N = 5, two males and three females with moderate to severe intellectual disabilities, ≥50 years | To explore the potential and efficacy of robot‐based AAT in adults with moderate to severe intellectual disabilities using the robot seal Paro | Robot‐based Animal Assisted Therapy (AAT); 4 weeks | Support staff | Active | Young Child Session Rating Scale (Duncan et al., 2011); AOL (Vlaskamp et al., 2010) | For one participant, Paro had a positive influence on mood and alertness. For the other participants, no significant beneficial effects of Paro were observed. |
| 36. Watchman et al. (2020); UK a | Mixed‐method participatory action approach; High (5/5) | N = 14, five males and nine females with intellectual disabilities and dementia | To identify the effectiveness of psychosocial interventions in social care settings, and, uniquely, to explore the use of photo‐voice methodology to develop dialogue about dementia | Individualised psychosocial interventions; 6 months | Support staff | Active | QUALID (Weiner et al., 2000); NPI‐Q (Cummings et al., 1994); Goal Attainment Scale (Kiresuk & Sherman, 1968), interviews with participants and photo‐voice technology (Kiresuk & Sherman, 1968) | The results provide evidence from a range of data‐collection methods to support the effectiveness of person‐centred psychosocial interventions as part of a goal‐setting process in reducing agitation or distress and increasing QoL associated with dementia. Individualised psychosocial interventions have the potential to reduce distress or agitation. |
Studies specifically focused on ageing people with intellectual disabilities.
2.3. Data extraction and analysis
Both general information (i.e., study and participant characteristics) and main results were presented briefly in order to provide a clear overview of the studies included (see Table 3). Subsequently, a narrative, integrative method of analysis was used to synthesise the quantitative and qualitative data (Whittemore & Knafl, 2005) addressed in the studies. The structure of the results was determined by the review questions and based on themes emerging from the analysis.
3. RESULTS
The results of this review are divided into three parts. First, a brief overview of the study characteristics is presented. This is followed by a description of the themes emerging from the analysis with regard to the focus of the psychosocial interventions included. Finally, the role of support staff in the application of these interventions is explained further.
3.1. Background and research quality
An overview of descriptive information for the 36 studies included is provided in Table 3. Of these studies, 14 were conducted in the USA, with 7 having been conducted in the UK, 7 in the Netherlands, 2 in Ireland, 2 in Australia and 1 each in Belgium, Hong Kong, Israel and New Zealand. The studies were based on a variety of designs. A quantitative approach was used in 29 studies (i.e., 12 multiple baseline designs, 9 case studies or case series, 4 quasi‐experimental designs, 3 pre‐post intervention designs and 1 controlled trial), with 4 studies using a mixed‐methods design and 3 being qualitative (i.e., 2 observational studies and 1 case study). Regarding the type of interventions, 11 behavioural interventions, 8 modelling and (social) skills interventions, 6 multi‐component interventions, 6 therapeutic interventions, 4 cognitive interventions and 1 social network intervention were included in this review. The quality assessment with the MMAT (Hong et al., 2018) resulted in 4 studies of high quality, 24 of moderate quality and 8 of low quality (see Table 3). Overall, the main methodological limitation concerned the lack of information of the origin of the measures and/or the relationship between the context of the study and its influence on the results (e.g., the researcher's perspective, role and interaction with participants). Studies with a score 2 out of 5 frequently lacked validation for both of these themes. In general, sample sizes were small, often no follow‐up data was collected or in some cases, outcome data was incomplete and information on procedural reliability was scarce resulting in the majority of studies being rated with moderate quality.
In all, 296 individuals (161 male and 135 female) aged ≥50 years with intellectual disabilities were involved in these studies, although only 11 studies focused specifically on the ageing population with intellectual disabilities. The remaining 25 studies either provided separate results for the group of participants aged ≥50 years or demonstrated that there were no statistically significant differences between the younger and older participants. In 26 studies, the participants' level of functioning was specified (e.g., mild, moderate, severe or profound). The other studies mentioned only that participants had intellectual disabilities. The focus of 16 studies was on participants with an intellectual disability and an additional diagnosis (e.g., dementia, Down syndrome, autistic disorder or visual impairment). All of the studies were conducted within the context of community and residential services for people with intellectual disabilities.
3.2. Focus of psychosocial interventions for older people with intellectual disabilities
To answer the first research question, relating to the focus of psychosocial interventions for older people with intellectual disabilities, the psychosocial interventions identified in the studies were subdivided into two main themes. The first theme covers interventions focusing on understanding older people with intellectual disabilities by identifying and meeting their individual needs and perceptions. The second theme covers interventions aimed at improving specific behaviours or skills in older people with intellectual disabilities.
3.2.1. Interventions for identifying and meeting unique and individual needs or perceptions of older people with intellectual disabilities (N = 17)
Interventions focusing on the perceptions of older people by identifying their individual preferences (N = 4)
Four studies were based on identifying the preferences of individual participants. First, two studies concerned interventions aimed to use active mentoring to meet the individual interests of 32 older people with moderate intellectual disabilities (Chng et al., 2013; Stancliffe et al., 2015). The results suggest that active mentoring generated sufficient improvements in activity engagement and increased community participation, thereby preventing inactivity, isolation and loneliness in retirement. Second, one study described the implementation of a standardised procedure for assessing the repeated presentation of preferred items and activities of participants (including two older people) with profound multiple disabilities during multiple periods of the day (Darling & Circo, 2015). Although this intervention led to a slight increase in the participants' scores on happiness indices, the relationships between variables were limited. Finally, the fourth study involved the implementation of an intervention examining the affective behaviour of participants (including one older person) with intellectual disabilities and congenital deaf blindness (Martens et al., 2017). Support staff members were trained to recognise individual affective behaviours, attuning to interactive behaviours and sharing meanings in order to improve the understanding of emotions. Although this training increased dyadic affective involvement, levels of affective involvement decreased during follow‐up.
Interventions aimed at understanding the perceptions of older people by exploring their individual life histories (N = 4)
In all, four studies described interventions in which 79 older participants with mild to moderate intellectual disabilities were invited to talk about their lives in general, as well as about memorable life events. Three studies implemented a variety of reminiscence techniques, including life‐story work and books (Bai et al., 2014), rummage boxes (Crook et al., 2016) and group sessions (Van Puyenbroeck & Maes, 2009), to explore outcomes in terms of life satisfaction, mood, well‐being and/or behaviour. All of the reminiscence techniques exhibited potential to improve the well‐being of participants. A fourth study involved the implementation of a narrative group therapy for people (including one older person) with intellectual disabilities (Randle‐Philips et al., 2016), inviting them to describe what they identified as important and significant in their lives. Although the older participant reported that the group had elevated her mood and that she had benefited from the peer support and social connections within the group, no changes were observed with regard to well‐being or self‐esteem.
Interventions aimed at adjusting the level of assistance for individual older people (N = 3)
Three interventions involved some form of focusing on the type and level of assistance provided to older individuals with intellectual disabilities. In one study, staff members were trained to provide the least intrusive form of assistance and to honour the choices made by eight older service users with severe to profound intellectual disabilities (Cooper & Browder, 2001). This intervention increased the number of choice responses, in addition to enhancing the participants' level of performance. In a second study, two different prompting procedures (physical presence and online assistance) were assessed. Although both procedures resulted in an increase in the completion of novel household tasks by people (including two older participants) with mild to moderate intellectual disabilities (Taber‐Doughty et al., 2010), the participants completed tasks more independently when the assistance was provided online. Finally, the third study explored the assistance potential of a robot seal, ‘Paro’, for five older individuals with intellectual disabilities. Paro had a positive influence on mood and alertness in only one participant (Wagemaker et al., 2017).
Intervention approaches involving the implementation of support focusing on the individual needs of older people (N = 6)
Whereas the previous sub‐themes concerned single interventions (i.e., one‐time interventions focusing on a single outcome), six studies described the implementation of a more comprehensive approach. These interventions were aimed at meeting individual needs by making structured observations and adjusting the support accordingly, broadly implementing a psychosocial approach and/or combining psychosocial interventions. One study examines the effect of Dementia Care Mapping on the well‐being and QoL of 113 older people with intellectual disabilities by coding what happened to these individuals during observations in communal areas of a group home (Schaap et al., 2019). The intervention did not generate any changes in QoL, as compared to care as usual. Another study was intended to make life less stressful for an older man with Down syndrome and dementia by implementing a mediational intervention for sensitising caregivers (MISC) (Lifshitz & Klein, 2011). The MISC provided support staff with strategies concerning the participant's individual emotional and cognitive needs, thereby helping them to improve their connection and interaction with him. A third study involved the development of an individual support programme (ISP) for people (including three older participants) with profound intellectual and multiple disabilities (Vlaskamp & van der Putten, 2009). The outcomes were generally positive with regard to communication, mood, contact, interaction and alertness. A fourth study concerned the implementation of a community‐based accommodation programme for participants (including one older person) with severe to profound intellectual disabilities and autism (Fox et al., 2009). This programme aimed to create a highly predictable environment that was customised to the unique characteristics, preferences and needs of each individual, thereby strengthening adaptive and pre‐vocational skills, while preventing the onset of challenging behaviour. The participant showed progress and reductions in challenging behaviour. Finally, two studies examined the implementation of multiple psychosocial interventions with people (including two older participants) with mild intellectual disabilities and psychotic disorders (Raftery et al., 2017) and 14 older people with intellectual disabilities and dementia (Watchman et al., 2020). These personalised approaches (e.g., social skills intervention, reminiscence, photo‐voice technology) apparently directed particular attention to the participants' psychosocial needs, psychological functioning, daily living skills and overall QoL. One study (Raftery et al., 2017) reported reductions in psychopathology (e.g., anxiety) and an increase in psychological functioning and QoL. Another study (Watchman et al., 2020) suggested that individualised psychosocial interventions could have the potential to reduce distress or agitation in older participants.
3.2.2. Interventions aimed at improving the behaviour and skills of older people with intellectual disabilities (N = 19)
Interventions aimed at decreasing or improving particular behaviours in older people (N = 3)
Two studies focused on decreasing particular behaviours—one by implementing a behavioural treatment for non‐compliance and public stripping in an older man with Down syndrome and dementia (Horovitz et al., 2010), and the other by evaluating the effect of a sensory‐equipment room (‘Snoezelen Room’) and outdoor activities on stereotypical behaviour (e.g. body‐rocking, mouthing and pica) of people (including two older participants) with profound intellectual disabilities (Cuvo et al., 2001). A third study evaluated the use of a literacy‐based behavioural intervention to improve employment behaviour in one older man with an intellectual disability and Down syndrome (Bucholz et al., 2008). A personalised story was read to him twice a day (prior to his morning break and lunch) for several days, in order to increase independence and improve returning to work on time. All three of these studies reported decreases in non‐compliance or stereotypical behaviour, as well as improvements in timely return to work.
Interventions aimed at teaching domestic and self‐care skills to older people (N = 3)
Behavioural interventions aimed at the improvement and mastery of various daily living skills by older people with intellectual disabilities were described in three studies. One study focused on teaching behaviour chains (e.g., folding clothes and turning on a CD/DVD player) to people (including one older participant) with severe intellectual disabilities in their home environments (Dollar et al., 2012). Another study involved the implementation and embedding of social initiation (i.e., serving coffee and sitting down with a peer) by using video modelling for people (including one older person) with severe intellectual disabilities (Bidwell & Rehfeldt, 2004). The third study aimed to improve the self‐care skills (e.g., tooth brushing and tying a necktie) of participants (including one older person) with moderate intellectual disabilities (Golisz et al., 2018). All three of these studies indicated positive outcomes following completion of the interventions.
Interventions aimed at teaching social and communication skills to older people (N = 7)
Seven studies focused primarily on improving social and communication skills or increasing social inclusion in order to prevent social isolation and expand social networks and societal participation. One study outlined an intervention in which the contact behaviour of people (including one older person) with intellectual disabilities and autism was explored and supported individually (Brooks & Paterson, 2010). A second study examined the learning and use of a picture exchange communication system by people (including one older person) with intellectual disabilities and severe communication deficits, as described by Conklin and Mayer (2010). This intervention was intended to increase the initiation of requests, independence and choice‐making of participants. A third study involved the application of principles of caregiver‐infant interaction (i.e., intensive interaction) to enhance the communication and social abilities of people (including one older person) with profound intellectual disabilities, as well as to enhance the responsiveness of support staff (Samuel et al., 2008). The results of these studies indicated that the interventions could potentially contribute to or improve participants' communication, initiation of requests and social abilities. Another study involved administering 15 individual training sessions in order to improve the social problem‐solving skills and reduce psychological distress of people (including one older person) with mild intellectual disabilities (Anderson & Kazantzis, 2008). Although the older participant showed improvement in social problem‐solving skills after receiving the training programme, no changes were observed with regard to anxiety, self‐esteem or depression. Two other studies involved the implementation and evaluation of a series of behavioural interventions aimed at replacing social avoidance and inappropriate social interaction with appropriate forms of social interaction (e.g., verbal communication skills) in people (including two older participants) with severe intellectual disabilities (Harper et al., 2013; Underwood et al., 2009). Both of these studies reported increases in social and appropriate behaviour and decreases in problem behaviour following the intervention. In the study by Harper et al. (2013), however, this was true for only one of the five behavioural interventions that were conducted. Finally, one study evaluated a group‐oriented intervention (i.e., ‘Communal Table’), in which monthly dinners were organised for people (including eight older participants) with mild intellectual disabilities at various community centres (Kruithof et al., 2018). Although the participants experienced conviviality and warmth, the intervention did not lead to any increase in their societal participation or the expansion of their social networks.
Interventions aimed at improving the coping skills of older people (N = 6)
The applicability of cognitive behavioural therapy (CBT) for improving the coping strategies and techniques of people (including six older participants) with mild intellectual disabilities was evaluated in three studies. In all cases, dual diagnoses (e.g., anxiety, chronic pain and symptoms of posttraumatic stress disorder) constituted reason to apply these interventions. Participants received multiple sessions intended to decrease symptoms of trauma (Mevissen et al., 2011), develop pain‐management skills (McManus et al., 2014) or learn about various concepts of anxiety and coping techniques (Marwood & Hewitt, 2012). Although all three of these studies indicated the applicability of CBT, the outcomes were somewhat variable. The use of CBT seemed to be most beneficial for the participants with regard to decreasing symptoms of trauma and anxiety. It was less successful for developing pain‐management skills, as the older participant showed lower levels of knowledge.
Three studies also described coping‐related interventions other than CBT. One evaluated the use of group‐wise psycho‐education for people (including two older participants) with mild intellectual disabilities and psychosis to increase their understanding of the concept of psychosis, the need for medication, the role of stress and early signs of relapse (Crowley et al., 2008). The older participants exhibited increased knowledge about psychosis following the intervention. Another study examined the ways in which a group of people (including three older participants) with mild to moderate intellectual disabilities coped with separation anxiety by applying technology‐assisted therapy (i.e., using a mobile phone and application) and teaching the concept of person permanence through repetition and the provision of a secure base and safe haven (Hoffman et al., 2019). The results indicate that the separation anxiety and challenging behaviour exhibited and experienced by the participants decreased significantly, while their psychosocial functioning and QoL increased significantly. The last of these three studies evaluated a response to bullying training for 4 victims of bullying (one older man with severe intellectual disability) (Stannis et al., 2019). To teach the older man some intended response to bullying, a behavioural skills training, an in situ training and an incentive phase were all necessary.
3.3. The role of support staff in interventions
To answer the second research question, relating to the role of support staff in the application of psychosocial interventions, the researchers deductively categorised all 36 of the identified interventions into three themes: interventions in which support staff had (1) an active role, (2) a mediating or assisting role or (3) no significant role or a role that remained undefined.
3.3.1. Interventions in which support staff have an active role (N = 15)
Fifteen of the studies described interventions in which support staff had an active role because they carried out the intervention themselves (see Table 3). Distinctions can nevertheless be made with regard to the intensity of their role and the skills that were required before the intervention could be applied (e.g., staff training). One distinct category consists of the nine studies that involved training staff members before they carried out the intervention (Bai et al., 2014; Bucholz et al., 2008; Cooper & Browder, 2001; Darling & Circo, 2015; Fox et al., 2009; Hoffman et al., 2019; Kruithof et al., 2018; Lifshitz & Klein, 2013; Martens et al., 2017; Samuel et al., 2008; Schaap et al., 2019; Taber‐Doughty et al., 2010; Vlaskamp & Van der Putten, 2009; Wagemaker et al., 2017; Watchman et al., 2020). For example, in a personalised day programme for adults with intellectual disabilities and autism (Fox et al., 2009), support staff were involved in both the selection of participants and the implementation of the programme. Before staff members implemented the programme independently, however, they were required to take specialised training, which consisted of several phases (e.g. an overview of autism and its implications for working with these individuals, role‐play exercises and feedback sessions). A similar approach was described in studies by Cooper and Browder (2001) and by Vlaskamp and van der Putten (2009), in which staff members were trained before starting the actual implementation of the intervention. A more extensive and comprehensive role for support staff was described in a study by Schaap et al. (2019), in which they examined the effect of Dementia Care Mapping on the well‐being and QoL of older people with intellectual disabilities. More specifically, staff members were selected to become trained observers, which subsequently enabled them to carry out the intervention. Following the observations, these staff members reported the results to other support staff members in order to help them to understand the behaviour of clients.
In contrast to the nine studies mentioned above, two studies described interventions in which support staff members played an active role, in addition to describing the competences that the staff members needed in order to carry out the intervention successfully. No staff training was included in these interventions. More specifically, Lifshitz and Klein (2011) implemented a customised programme involving the five parameters of the mediational intervention for sensitising caregivers (MISC) with a person with intellectual disabilities and dementia. As clearly described in the article, support staff members needed to be conscious of the key issues in their relationship with the client (i.e., their own perceptions of the client, themselves as caregivers and the emotional and cognitive needs of the client) before they were able to implement the parameters during daily activities. In another study, Bai et al. (2014) demonstrated that, in addition to being responsible for carrying out the intervention (i.e., the Life Story Work programme, or LSWp), support staff members helped participants to express their feelings concerning their life stories within a caring and accepting atmosphere.
Finally, four studies examined interventions in which support staff members were responsible for applying interventions by following instructions (Bucholz et al., 2008; Kruithof et al., 2018; Taber‐Doughty et al., 2010; Wagemaker et al., 2017). No additional staff training was provided prior to the implementation of the intervention. For example, in their study, Bucholz et al. (2008) described that support staff members had been responsible for accompanying a male participant to a private location, where they would read him a personalised story prior to his lunch break. In addition, support staff members were asked to use various levels of prompting if the participant was not returning to work. In the study by Wagemaker et al. (2017), support staff members were responsible for introducing, creating interaction with and withdrawing the robot seal Paro each day for a period of 8 weeks.
3.3.2. Interventions in which support staff have a mediating or assisting role (N = 12)
The second theme refers to 12 intervention studies in which a psychologist or researcher was largely responsible for carrying out the intervention (Anderson & Kazantzis, 2008; Chng et al., 2013; Crook et al., 2016; Crowley et al., 2008; Horovitz et al., 2010; Marwood & Hewitt, 2013; McManus et al., 2014; Mevissen et al., 2011; Stancliffe et al., 2015; Stannis et al., 2019; Underwood et al., 2009; Van Puyenbroeck & Maes, 2009). In these studies, support staff had a mediating or assisting role. The extent of their role and the level of their involvement in these interventions varied, and they were not always described in detail. For example, in three studies, the role of support staff changed over time, as they were expected to apply a number of intervention techniques, on the instruction of the therapist or researcher, in order to continue implementing the intervention (Horovitz et al., 2010; Underwood et al., 2009; Van Puyenbroeck & Maes, 2009).
In three other studies, the role of support staff was smaller than that described in the studies mentioned earlier within this theme (Marwood & Hewitt, 2012; McManus et al., 2014; Mevissen et al., 2011). More specifically, staff members played an important role as a source of information, and they were asked to assist with generalisation outside the treatment session and to assist participants with homework assignments, if necessary, and to practice skills with them between sessions.
Finally, the smallest mediating or assisting roles played by support staff were described in three studies, in which support staff members were present to assist, motivate or transfer information to the participant while the psychologist or researcher delivered the intervention (Anderson & Kazantzis, 2008; Crook et al., 2016; Crowley et al., 2008). For example, although Anderson and Kazantzis (2008) did not explicitly mention the role of support staff in their study on training in social problem‐solving skills for adults with intellectual disabilities, they did report that the presence of support staff during the intervention sessions was associated with greater continuity and follow‐through in problem solving.
3.3.3. Interventions in which support staff have no significant role or a role that remains undefined (N = 9)
The third category of interventions included nine studies in which the role of support staff remained undefined (Bidwell & Rehfeldt, 2004; Brooks & Paterson, 2010; Conklin & Mayer, 2011; Cuvo et al., 2001; Dollar et al., 2012; Golisz et al., 2018; Harper et al., 2013; Raftery et al., 2017; Randle‐Philips et al., 2016). The interventions addressed in these studies focused largely on teaching new, adaptive skills to individuals with intellectual disabilities or improving their behaviour (e.g., social avoidance). In the majority of the studies within this theme, the interventions were applied in separate settings (e.g., classrooms or therapy rooms) by therapists, researchers or students/undergraduates. The studies did not provide any information about the role of support staff in these psychosocial interventions for older people with intellectual disabilities.
4. DISCUSSION
The life expectancy of people with intellectual disabilities has increased in recent decades, due to improved living conditions and better medical care (Mulryan et al., 2021). Despite these advances, however, the implications of ageing with an intellectual disability are also posing new challenges for older people, their support staff and healthcare organisations (Prasher et al., 2021). It is unclear whether support staff are prepared to fulfil their significant role in meeting the needs of older people with intellectual disabilities (Kåhlin et al., 2016). For this reason, and because the existing body of overview studies focuses primarily on medical/physical interventions (Schepens et al., 2018), additional knowledge is needed with regard to the psychosocial interventions that are available and that could help to optimise support for older people with intellectual disabilities. This systematic review is intended to provide an overview of the available psychosocial, non‐medical/physical interventions for older people with intellectual disabilities. The review began by examining the focus of the interventions available in the international literature. The second step consisted of describing the role of support staff in the application of these interventions.
With regard to the focus of interventions, we were able to categorise all 36 interventions into two groups. The first group consisted of 17 interventions that focused primarily on identifying the unique needs and perceptions of older individuals with intellectual disabilities. Many of the studies in this group had been developed specifically for the target group of older people with intellectual disabilities. Despite differences in design, all of these studies were aimed at either gaining more insight into older individuals with intellectual disabilities (e.g., their life histories), recognising or meeting individual needs (e.g., the emotional and cognitive support needs of individuals), or implementing appropriate/adjusted care and support. The attention focused on individual needs and perceptions is consistent with the principles of person‐centred care (Kitwood, 1997). The concept of person‐centred care originated within the field of healthcare for older people without intellectual disabilities. Kitwood (1997) developed the theory of person‐centred care within the context of dementia care, thereby underscoring psychosocial needs and ‘seeing the person’. The results of this review, suggest that various aspects of person‐centred care have since been adopted within the context of psychosocial care and support for older people with intellectual disabilities. The emergence of person‐centred interventions that address the psychosocial support needs of older people may help caregivers to broaden the focus of their practice, which may tend to over‐emphasise the medical aspects of care (Fazio et al., 2018).
In our review, we also identified 19 interventions aimed at improving the behaviour and skills of older people with intellectual disabilities. Although these studies were generally not designed specifically for older people, the participant groups did include older people. The interventions within this theme focused largely on teaching self‐care or other skills, in order to enhance independence and social skills, while promoting problem‐solving abilities, coping skills for dealing with anxiety or chronic pain and behavioural treatments aimed at decreasing inappropriate behaviour. In light of the possible cognitive and physical decline of older people with intellectual disabilities, it is interesting to note that a large share of the available psychosocial interventions that are offered to older individuals continue to focus on the development of new skills. This finding suggests that support staff members are likely to consider applying existing interventions aimed at improving the skills and behaviour of adults within the context of care for older people with intellectual disabilities as well. In addition, it is not uncommon for psychosocial interventions that were initially developed for adults to be translated to the population of older people in general. The literature on regular healthcare contains examples of applications of a treatment for depression aimed at teaching skills to participants in order to improve their mood, change negative thinking patterns and increase their engagement in enjoyable activities. Although this intervention was originally developed for adults between the ages of 20 and 55 years, a variant of the course has been successfully implemented with older individuals (Cuijpers et al., 2011). These insights offer possibilities for the further development of interventions that are appropriate for older people with intellectual disabilities.
The second aim of the current review was to examine the role of support staff in the application of these interventions. As evidenced by the results, we were able to distinguish three types of roles for support staff in psychosocial interventions for older people with intellectual disabilities: active, mediating and undefined. The extent of the role, the level of involvement and the skills that must be acquired (e.g., through staff training) before the intervention could be applied varied, and these aspects were not always described in detail. In only 15 of 36 studies, support staff members were at least partially responsible for applying the actual intervention. At the same time, however, the results suggest that this group of professionals is particularly likely to be confronted with the changing support needs of older people with intellectual disabilities on a daily basis, and they have a particular need to know how to address matters of ageing in the care and support of people with intellectual disabilities (Kahlin et al., 2016; Thalen et al., submitted). Support staff may therefore have a considerable need for psychosocial interventions aimed at expanding their knowledge and their ability to provide sufficient care and support to older people with intellectual disabilities (Alftberg et al., 2021).
This review demonstrates that in scientific databases, relatively few psychosocial interventions are available for support staff members to apply directly in their daily work with older people with intellectual disabilities, which implies that they have little choice and opportunities to work with psychosocial interventions. In addition, the majority of psychosocial interventions were often carried out during a short period of time (e.g., a few individual sessions), with the aim of affecting a single outcome variable (e.g., happiness). Only a few interventions are part of larger, integrative and holistic support approaches that focus simultaneously on multiple aspects of the lives of older people with intellectual disabilities and the support provided to them. A few studies did describe the implementation of a more comprehensive approach that combined several psychosocial elements (e.g., Fox et al., 2009; Schaap et al., 2019). Future studies should therefore focus on developing and strengthening the theoretical base of integrative psychosocial interventions that involve support staff in an executive role. Support staff should ideally receive training in order to increase their relevant knowledge and skills in advance, thereby ensuring that they will be able to carry out the intervention appropriately (Innes & McCabe, 2012). Finally, when it comes to the support of older people with intellectual disabilities, a lack of an evidence base is still present (Thalen et al., 2021). The overview presented in this study provides valuable insights that may contribute to further research into the actual efficacy of the available psychosocial interventions and the implications for older people with intellectual disabilities or into topics not yet addressed and, thereby, increase the evidence base. Furthermore, in future research contextual factors should be taken into account, such as the potential differences in the access or delivery of support of older people with intellectual disabilities (e.g., rural vs. urban) or the role and involvement of family members in providing psychosocial support.
4.1. Limitations
It is important to acknowledge several limitations to this review. The exclusion of grey literature and studies published in languages other than English may have introduced a bias toward significant results and information from specific regions of the world. The consultation of four databases and the screening of the reference lists of included studies may be considered as limited. However, an additional hand search by the first author on Google Scholar did not lead to any new results. With regard to efficacy, we found indications that a great number of psychosocial interventions have the potential to make positive contributions to one or more of their established goals (e.g., identifying the needs and perceptions of older people with intellectual disabilities and improving their skills). In our review, however, we did not attempt to provide a thorough assessment of the effectiveness of the interventions that we identified. In the future, additional studies could further examine the effectiveness of the identified interventions for older people with intellectual disabilities. Furthermore, this review did not focus on the perceptions and experiences of older people themselves when receiving psychosocial interventions, as most interventions relied on observational methods to assess outcomes. Future review and empirical studies might therefore provide a more complete image by concentrating more on the actual experiences of older individuals with regard to receiving psychosocial interventions. Despite its limitations, this review provides an extensive overview of the available psychosocial interventions for older people with intellectual disabilities, as well as the focus of these interventions and the role of support staff in their application.
4.2. Conclusion
A systematic literature review was conducted with the goal of providing an overview of the available, non‐pharmacological and non‐physical interventions for older people with intellectual disabilities. We examined the various foci of existing psychosocial interventions for older people with intellectual disabilities, as well as the role of support staff in the application of these interventions. This overview may serve as a supplement to existing knowledge, thereby contributing to the optimisation of care and support for older people with intellectual disabilities. It could also enhance the further development of and theoretical support for evidence‐based psychosocial interventions.
CONFLICT OF INTEREST
The authors declare not to have any conflict of interest.
ACKNOWLEDGEMENT
The authors would like to thank Wichor Bramer, Information Specialist at Erasmus Medical Center Rotterdam, for his assistance with the literature search.
Thalen, M. , Volkers, K. M. , van Oorsouw, W. M. W. J. , & Embregts, P. J. C. M. (2022). Psychosocial interventions for older people with intellectual disabilities and the role of support staff: A systematic review. Journal of Applied Research in Intellectual Disabilities, 35(2), 312–337. 10.1111/jar.12953
DATA AVAILABILITY STATEMENT
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
REFERENCES
*Included studies in the systematic review
- Alftberg, Å. , Johansson, M. , & Ahlstrom, G. (2021). Ambivalence among staff regarding ageing with intellectual disabilities: Experiences and reflections. Journal of Intellectual Disabilities, 25(2), 192–209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- * Anderson, G. , & Kazantzis, N. (2008). Social problem‐solving skills training for adults with mild intellectual disability: A multiple case study. Behaviour Change, 25(2), 97–108. [Google Scholar]
- Andrews, F. M. , & Withey, S. B. (1976). Social indicators of well being. New York: Plenum Press. [Google Scholar]
- Axmon, A. , Ahlström, G. , & Höglund, P. (2017). Prevalence and treatment of diabetes mellitus and hypertension among older adults with intellectual disability in comparison with the general population. BMC Geriatrics, 17, 272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- * Bai, X. , Ho, D. W. H. , Fung, K. , Tang, L. , He, M. , Young, K. W. , & Kwok, T. (2014). Effectiveness of a life story work program on older adults with intellectual disabilities. Clinical Interventions in Aging, 9, 1865–1872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beck, A. T. , Epstein, N. , Brown, G. , & Steer, R. A. (1988). An inventory for measuring clinical anxiety: psychometric properties. Journal of Consulting and Clinical Psychology, 56, 893–897. [DOI] [PubMed] [Google Scholar]
- * Bidwell, M. A. , & Rehfeldt, R. A. (2004). Using video modeling to teach a domestic skill with an embedded social skill to adults with severe mental retardation. Behavioral Interventions, 19, 263–274. [Google Scholar]
- Bradford Dementia Group (2005). Evaluating dementia care: The dementia care mapping method (8th edn.). Bradford: University of Bradford. [Google Scholar]
- Bramer, W. M. , Rethlefsen, M. L. , Kleijnen, J. , & Franco, O. H. (2017). Optimal database combinations for literature searches in systematic reviews: A prospective exploratory study. Systematic Reviews, 6(245), 1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks, S. , & Paterson, G. (2011). Using contact work in interactions with adults with learning disabilities and autistic spectrum disorders. British Journal of Learning Disabilities, 39(2), 161–166. [Google Scholar]
- Brooks, M. , Davies, S. , & Twigg, E. (2013). A measure for feelings ‐ using inclusive research to develop a tool for evaluating psychological therapy (Clinical Outcomes in Routine Evaluation ‐ Learning Disability). British Journal of Learning Disabilities, 3(2), 77–101. [Google Scholar]
- * Bucholz, J. L. , Brady, M. P. , Duffy, M. L. , Scott, J. , & Kontosh, L. (2008). Using literacy‐based behavioral interventions and social stories to improve work behavior in employees with developmental disabilities. Education and Training in Developmental Disabilities, 43(4), 486–501. [Google Scholar]
- Bursch, B. , Tsao, J. C. I. , Meldrum, M. , & Zelter, L. K. (2006). Preliminary validation of the self‐efficacy scale for child functioning despite chronic pain (child and parent versions). Pain, 12, 35–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centre for Consultation and Expertise (CCE) (2013). Questionnaire quality of living (kwaliteit van bestaan). Zwolle: Centre for Consultation and Expertise. [Google Scholar]
- * Chng, J. P. L. , Stancliffe, R. J. , Wilson, N. J. , & Anderson, K. (2013). Engagement in retirement: An evaluation of the effect of active mentoring on engagement of older adults with intellectual disability in mainstream community groups. Journal of Intellectual Disability Research, 57(12), 1130–1142. [DOI] [PubMed] [Google Scholar]
- * Conklin, C. G. , & Mayer, G. R. (2011). Effects of implementing the Picture Exchange Communication System (PECS) with adults with developmental disabilities and severe communication deficits. Remedial and Special Education, 32(2), 155–166. [Google Scholar]
- * Cooper, K. J. , & Browder, D. M. (2001). Preparing staff to enhance active participation of adults with severe disabilities by offering choice and prompting performance during a community purchasing activity. Research in Developmental Disabilities, 22(1), 1–20. [DOI] [PubMed] [Google Scholar]
- Coppus, A. M. W. (2013). People with intellectual disability: What do we know about adulthood and life expectancy? Developmental Disabilities Research Reviews, 18(6), 6–16. [DOI] [PubMed] [Google Scholar]
- Chadsey‐Rusch, J. , DeStefano, L. , O'Reilly, M. , Gonzalez, P. , & Collet‐Klingenberg, L. (1992). Assessing the loneliness of workers with mental retardation. Mental Retardation, 30, 85–92. [PubMed] [Google Scholar]
- * Crook, N. , Adams, M. , Shorten, N. , & Langdon, P. E. (2016). Does the well‐being of individuals with Down syndrome and dementia improve when using life story books and rummage boxes? A randomized single case series experiment. Journal of Applied Research in Intellectual Disabilities, 29(1), 483–410. [DOI] [PubMed] [Google Scholar]
- * Crowley, V. , Rose, J. , Smith, J. , Hobster, K. , & Ansell, E. (2008). Psycho‐educational groups for people with a dual diagnosis of psychosis and mild intellectual disability: A preliminary study. Journal of Intellectual Disabilities, 12(1), 25–39. [DOI] [PubMed] [Google Scholar]
- Cuijpers, P. , Andersson, G. , Donker, T. , & Van Straten, A. (2011). Psychological treatment of depression: Results of a series of meta‐analyses. Nordic Journal of Psychiatry, 65(6), 354–364. [DOI] [PubMed] [Google Scholar]
- Cummings, J. L. , Mega, M. , Gray, K. , Rosenberg‐Thompson, S. , Carusi, D. A. , & Gornbeing, J. (1994). The Neuropsychiatric Inventory: Comprehensive assessment of psychopathology in dementia. Neurology, 44(12), 2308–2314. [DOI] [PubMed] [Google Scholar]
- Cummins, R. A. , & Lau, A. L. D. (2005). Personal Wellbeing Index‐intellectual disability (3rd edn.). Melbourne: School of Psychology, Deakin University. [Google Scholar]
- Cuthill, F. M. , Espie, C. A. , & Cooper, S. A. (2003). Development and psychometric properties of the Glasgow Depression Scale for people with a learning disability: individual and carer supplement versions. The British Journal of Psychiatry, 182, 347–353. [DOI] [PubMed] [Google Scholar]
- * Cuvo, A. J. , May, M. E. , & Post, T. M. (2001). Effects of living room, Snoezelen room, and outdoor activities on stereotypic behavior and engagement by adults with profound mental retardation. Research in Developmental Disabilities, 22(3), 183–204. [DOI] [PubMed] [Google Scholar]
- Dagnan, D. , & Sandhu, S. (1999). Social comparison, self‐esteem and depression in people with intellectual disability. Journal of Intellectual Disability Research, 43(5), 372–379. [DOI] [PubMed] [Google Scholar]
- * Darling, J. A. , & Circo, D. K. (2015). Measuring happiness in individuals with profound multiple disabilities. Research in Developmental Disabilities, 47, 117–125. [DOI] [PubMed] [Google Scholar]
- * Dollar, C. A. , Fredrick, L. D. , Alberto, P. A. , & Luke, J. K. (2012). Using simultaneous prompting to teach independent living and leisure skills to adults with severe intellectual disabilities. Research in Developmental Disabilities, 33(1), 189–195. [DOI] [PubMed] [Google Scholar]
- Downs, C. , & Craft, A. (1997). Sex in context"A personal and social development programme for children and adults with profound and multiple impairments. Brighton: Pavilion. [Google Scholar]
- Durand, M. V. (1990). Severe behavior problems: A functional communication training approach. New York: Guilford. [Google Scholar]
- Duncan, B. I. , Miller, S. D. , & Sparks, J. A. (2011). The heroic client: A revolutionary way to improve effectiveness through client‐directed, outcome‐informed therapy. San Francisco, CA: Jossey Bass. [Google Scholar]
- Evenhuis, H. M. , Kengen, M. M. F. , & Eurlings, H. A. I. (1990). Dementia questionnaire for mentally retarded persons. Zwanerdam, The Netherlands: Hooge Burch Institute for Mentally Retarded People. [Google Scholar]
- Fazio, S. , Pace, D. , Flinner, J. , & Kallmyer, B. (2018). The fundamentals of person‐centered Care for Individuals with Dementia. The Gerontologist, 58(1), 10–19. [DOI] [PubMed] [Google Scholar]
- Fisher, A. G. , & Bray Jones, K. (2010). Assessment of motor and process skills. Development, standardization, and administration manual (7th edn.). Fort Collins, CO: Three Star Press. [Google Scholar]
- * Fox, R. A. , Holtz, C. A. , & Moist, A. M. (2009). A community‐based accommodation program for adults with autism and mental retardation. Education and Training in Developmental Disabilities, 44(1), 118–126. [Google Scholar]
- Goia, G. A. , Isquith, P. K. , Guy, S. C. , & Kenworthy, L. (2000). Behavior Rating Inventory of Executive Function: BRIEF. Odessa, FL: Psychological Assessment Resources. [Google Scholar]
- * Golisz, K. , Waldman‐Levi, A. , Swierat, R. P. , & Toglia, J. (2018). Adults with intellectual disabilities: Case studies using everyday technology to support daily living skills. British Journal of Occupational Therapy, 81, 514–524. [Google Scholar]
- Goverts, A. E. , van Westendorp, H. J. , Schuitemaker, M. , Hoekstra, S. , & Vermeer, A. (2000). Zelfwaargenomen competentie en sociale acceptatie bij mensen met een verstandelijke handicap; de ontwikkeling van een meetinstrument. Nederlands Tijdschrift Voor de Zorg aan verstandelijk gehandicapten, 26, 71–88. [Google Scholar]
- * Harper, J. M. , Iwata, B. A. , & Camp, E. M. (2013). Assessment and treatment of social avoidance. Journal of Applied Behavior Analysis, 46, 147–160. [DOI] [PubMed] [Google Scholar]
- Hermans, H. , Beekman, A. T. , & Evenhuis, H. M. (2013). Prevalence of depression and anxiety in older users of formal Dutch intellectual disability services. Journal of Affective Disorders, 144, 94–100. [DOI] [PubMed] [Google Scholar]
- Hermans, H. , & Evenhuis, H. M. (2014). Multimorbidity in older adults with intellectual disabilities. Research in Developmental Disabilities, 35, 776–783. [DOI] [PubMed] [Google Scholar]
- Hendriks, A. A. J. , Hofstee, W. K. B. , & De Raad, B. (1999). The Five‐Factor Personality Inventory (FFPI). Personality and Individual Differences, 27, 307–325. [Google Scholar]
- Hoekman, J. , Douma, J. C. H. , Kersten, M. C. O. , Schuurman, M. I. M. , & Koopman, H. M. (2001). IDQOL‐Intellectual disability qulity of life. De ontwikkeling van een instrument ter bepaling van de "kwaliteit van bestaan" van mensen met een verstandelijke handicap. Nederlands Tijdschrift Voor De Zorg Aan Verstandelijk Gehandicapten, 27, 207–225. [Google Scholar]
- * Hoffman, N. , Sterkenburg, P. S. , & Van Rensburg, E. (2019). The effect of technology assisted therapy for intellectually and visually impaired adults suffering from separation anxiety: Conquering the fear. Assistive Technology, 31(2), 98–105. [DOI] [PubMed] [Google Scholar]
- Hong, Q. N. , Fàbregues, S. , Bartlett, G. , Boardman, F. , Cargo, M. , Dagenais, P. , Gagnon, M. P. , Griffiths, F. , Nicolau, B. , O'Cathain, A. , Rousseau, M. C. , Vedel, I. & Pluye, P. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for information, 34(4), 285–291. [Google Scholar]
- * Horovitz, M. , Kozlowski, A. M. , & Matson, J. L. (2010). Compliance training in an adult with dementia of the Alzheimer's type and down syndrome. Clinical Case Studies, 9(2), 95–105. [Google Scholar]
- Innes, A. , & McCabe, L. (2012). Caring for older people with an intellectual disability: A systematic review. Maturitas, 72, 286–295. [DOI] [PubMed] [Google Scholar]
- Kåhlin I., Kjellberg A., Hagberg J. E. (2016). Ageing in people with intellectual disability as it is understood by group home staff. Journal of Intellectual and Developmental Disability, 41(1), 1–10. [Google Scholar]
- Kellett, M. C. (2001). 'Implementing Intensive Interaction', unpublished PhD thesis, Oxford Brookes University.
- Kiernan, C. , & Reid, B. (1987). Pre‐verbal Communication Schedule. Windsor: NFER‐Nelson. [Google Scholar]
- Kiresuk, T. J. , & Sherman, R. E. (1968). Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Mental Health Journal, 4(6), 443–453. [DOI] [PubMed] [Google Scholar]
- Killaspy, H. , White, S. , & King, M. (2012). Psychometric properties of the Mental Health Recovery Star. British Journal of Psychiatry, 201, 65–70. [DOI] [PubMed] [Google Scholar]
- Kitwood, T. (1997). Dementia reconsidered: The person comes first. Buckingham: Open University Press. [Google Scholar]
- * Kruithof, K. , Suurmond, J. , & Harting, J. (2018). Eating together as a social network intervention for people with mild intellectual disabilities: A theory‐based evaluation. International Journal of Qualitative Studies on Health and Well‐Being, 13(1), 1516089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Law, M. C. , Baptiste, S. , & Carswell, A. (1998). Canadian occupational performance measure. Ottawa, ON: Canadian Association of Occupational Therapists. [Google Scholar]
- Liberati, A. , Altman, D. G. , Tetzlaff, J. , Gøtzsche, P. , Ioannidis, J. P. A. , Clarke, M. , Devereaux, P. J. , Kleijnen, J. , & Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Medicine, 6, e1–e34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- * Lifshitz, H. , & Klein, P. S. (2011). Mediation between staff and elderly persons with intellectual disability with Alzheimer disease as a means of enhancing their daily functioning. Division on Autism and Developmental Disabilities, 46(1), 106–115. [Google Scholar]
- Loumidis, K. (1993). Learning disabilities (mental handicap) and social problem solving skills: Evaluation of a therapeutic training programme. Unpublished doctoral dissertation, Keele University, Staffordshire, England.
- Lindsay, W. R. , & Michie, A. M. (1988). Adaptation of the Zung self‐rating anxiety scale for people with a mental handicap. Journal of Mental Deficiency Research, 32, 485–490. [DOI] [PubMed] [Google Scholar]
- * Martens, M. A. W. , Janssen, M. J. , Ruijssenaars, W. A. J. J. M. , Huisman, M. , & Riksen‐Walraven, J. M. (2017). Fostering emotion expression and affective involvement with communication partners in people with congenital deafblindness and intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 30, 872–884. [DOI] [PubMed] [Google Scholar]
- * Marwood, H. , & Hewitt, O. (2012). Evaluating an anxiety group for people with learning disabilities using a mixed methodology. British Journal of Learning Disabilities, 41, 150–158. [Google Scholar]
- McCausland, D. , McCallion, P. , Cleary, E. , & McCarron, M. (2016). Social connections for older people with intellectual disability in Ireland: Results from wave one of IDS‐TILDA. Journal of Applied Research in Intellectual Disabilities, 29(1), 71–82. [DOI] [PubMed] [Google Scholar]
- * McManus, S. , Treacy, M. , & McGuire, B. (2014). Cognitive behavioural therapy for chronic pain in people with an intellectual disability: A case series using components of the feeling better programme. Journal of Intellectual Disability Research, 58, 296–306. [DOI] [PubMed] [Google Scholar]
- * Mevissen, L. , Lievegoed, R. , & de Jongh, A. (2011). EMDR treatment in people with mild ID and PTSD: 4 cases. Psychiatric Quarterly, 82, 43–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mindham, J. , & Espie, C. A. (2003). Glasgow Anxiety Scale for people with an intellectual disability (GAS‐ID): Development and psychometric properties of a new measure for use with people with mild intellectual disability. Journal of Intellectual Disability Research, 47, 22–30. [DOI] [PubMed] [Google Scholar]
- Moss, S. , Prosser, H. , Costello, H. , Simpson, N. , Patel, P. , & Rowe, S. (1998). Reliabiliy and validity of the PAS_ADD checklist for detecting psychiatric disorders in adults with intellectual disability. Journal of Intellectual Disability Research, 42, 173–183. [DOI] [PubMed] [Google Scholar]
- Mulryan, N. , Ambikapathy, A. , Tyrell, J. , & Sheerin, F. (2021). Psychopathology in older age. In Mental health, intellectual and developmental disabilities and the ageing process (pp. 31–44). Springer. [Google Scholar]
- Nihira, K. , Leland, H. , & Lambert, N. (1993). AAMR adaptive behavior scale ‐ residential and community (2nd ed.). Austin, TX: PRO‐ED, Inc. [Google Scholar]
- O'Neill, R. E. , Horner, R. H. , Albin, R. W. , Sprague, J. R. , Storey, K. , & Newton, J. S. (1997). Functional assessment and program development for problem behavior: A practical handbook (2nd edn.). Pacific Grove, CA: Brooks/Cole. [Google Scholar]
- Pluye, P. , Robert, E. , Cargo, M. , Bartlett, G. , O'Cathain, A. & Griffiths, F. (2011). Proposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies Reviews, pp. 1–8. McGill University, Montréal Available at: http://mixedmethodsappraisaltoolpublic.pbworks.com.
- Prasher, V. P. , Davidson, P. W. , & Santos, F. H. (Eds.). (2021). Mental health, intellectual and developmental disabilities and the ageing process. Springer. [Google Scholar]
- Petry, K. , Kuppens, S. , Vos, P. , & Maes, B. (2010). Psychometric evaluation of the dutch version of the mood, interest and pleasure questionnaire (MIPQ). Research in Developmental Disabilities, 31(6), 1652–1658. [DOI] [PubMed] [Google Scholar]
- Prouty, G. , van Werde, D. , & Pörtner, M. (2002). Pre‐Therapy: Reaching contact‐impaired clients. Ross‐on Wye: PCCS Books. [Google Scholar]
- * Raftery, M. , Burke, K. , Murray, N. , O'Duinn, O. , Murray, I. , & Hallahan, B. (2017). An intensive personalised support approach to treating individuals with psychosis and co‐morbid mild intellectual disability. Irish Journal of Psychological Medicine, 34, 99–109. [DOI] [PubMed] [Google Scholar]
- * Randle‐Philips, C. , Farquhar, S. , & Thomas, S. (2016). Adapting and evaluating a tree of life group for women with learning disabilities. British Journal of Learning Disabilities, 44(4), 301–308. [Google Scholar]
- Reiss, S. , & Benson, B. (1985). Psychosocial correlates of depression in mentally retarded adults: I. Minimal social support and stigmatization. American Journal of Mental Deficiency, 89, 331–337. [PubMed] [Google Scholar]
- Ross, E. , & Oliver, C. (2003). Preliminary analysis of the psychometric properties of the Mood, Interest and Pleasure Questionnaire (MIPQ) for adults with severe and profound learning disabilities. British Journal of Clininal Psychology, 42(1), 81–93. [DOI] [PubMed] [Google Scholar]
- Roy, A. , Matthews, H. , Clifford, P. , Fowler, V. , & Martin, D. M. (2002). Health of the Nation Outcome Scales for people with Learning Disabilities (HoNOS‐LD). British Journal of Psychiatry, 180, 61–66. [DOI] [PubMed] [Google Scholar]
- Russell, D. W. (1996). UCLA Loneliness Scale (version 3): reliability, validity, and factor structure. Journal of Personality Assessment, 66, 20–40. [DOI] [PubMed] [Google Scholar]
- Ryan A., Taggart L., Truesdale‐Kennedy M., Slevin E. (2014). Issues in caregiving for older people with intellectual disabilities and their ageing family carers: a review and commentary. International Journal of Older People Nursing, 9(3), 217–226. [DOI] [PubMed] [Google Scholar]
- Sanz, M. , Constable, G. , Lopez‐Ibor, I. , Kemp, R. , & David, A. S. (1998). A comparative study of insight scales and their relationship to psychopathological and clinical variables. Psychological Medicine, 28, 437–446. [DOI] [PubMed] [Google Scholar]
- * Samuel, J. , Nind, M. , Volans, A. , & Scriven, I. (2008). An evaluation of intensive interaction in community living settings for adults with profound intellectual disabilities. Journal of Intellectual Disabilities, 12, 111–126. [DOI] [PubMed] [Google Scholar]
- Schepens, H. R. , Van Puyenbroeck, J. , & Maes, B. (2019). How to improve the quality of life of elderly people with intellectual disability: A systematic literature review of support strategies. Journal of Applied Research in Intellectual Disabilities, 32, 483–521. [DOI] [PubMed] [Google Scholar]
- * Schaap, F. D. , Finnema, E. J. , Stewart, R. E. , Dijkstra, G. J. , & Reijneveld, S. A. (2019). Effects of dementia care mapping on job satisfaction and caring skills of staff caring for older people with intellectual disabilities: A quasi‐experimental study. Journal of Applied Research in Intellectual Disabilities, 32, 1228–1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shooshtari, S. , Martens, J. , Burchill, C. , Dik, N. , & Naghipur, S. (2011). Prevalence of depression and dementia among adults with developmental disabilities in manitoba, canada. International Journal of Family Medicine, 1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, J. , & Birchwood, M. (1990). Relatives and patients as partners in the management of schizophrenia. British Journal of Psychiatry, 156, 654–660. [DOI] [PubMed] [Google Scholar]
- Singh, A. N. , Matson, J. L. , Mouttapa, M. , Pella, R. D. , Hill, B. D. , & Thorson, R. (2009). A critical item analysis of the QABF: Development of a short form assessment instrument. Research in Developmental Disabilities, 30, 782–792. [DOI] [PubMed] [Google Scholar]
- Sparrow, S. S. , Cicchetti, D. V. , & Balla, D. A. (2005). Vineland Adaptive Behavior Scales: Second Edition (Vineland‐II) ‐ Survey Interview Form/Caregiver Rating Form. Livonia, MN: Pearson Assessments. [Google Scholar]
- Spitzer, R. L. , Gibbon, M. , Williams, J. B. , & Endicott, J. (1994). Global Assessment of Functioning (GAF) Scale. Outcome Assessment in Clinical Practice (ed L. I. Sederer and R. Dickey) (76–78). Baltimore, MD: Williams & Wilkins. [Google Scholar]
- * Stancliffe, R. J. , Bigby, C. , Balandin, S. , Wilson, N. J. , & Craig, D. (2015). Transition to retirement and participation in mainstream community groups using active mentoring: A feasibility and outcomes evaluation with a matched comparison group. Journal of Intellectual Disability Research, 59(8), 703–718. [DOI] [PubMed] [Google Scholar]
- * Stannis, R. L. , Crosland, K. A. , Miltenberger, R. , & Valbuena, D. (2019). Response to bullying (RtB): Behavioral skills and in situ training for individuals diagnosed with intellectual disabilities. Journal of Applied Behavior Analysis, 52, 73–83. [DOI] [PubMed] [Google Scholar]
- * Taber‐Doughty, T. , Shurr, J. , Brewer, J. , & Kubik, S. (2010). Standard care and telecare services: Comparing the effectiveness of two service systems with consumers with intellectual disabilities. Journal of Intellectual Disability Research, 54(9), 843–859. [DOI] [PubMed] [Google Scholar]
- Tapp, J. (2009). MOOSES tm (Multi‐Option Observation System for Experimental Studies) for Window (version 3) [Computer Software and Manual]. Nashville, TN: Vanderbilt University, Office of Technology Transfer and Enterprise Development. [Google Scholar]
- Tenneij, N. H. , & Koot, H. M. (2007). A preliminary investigation into the utility of the adult behavior checklist in the assessment of psychology in people with low IQ. Journal of Applied Research in Intellectual Disabilities, 20(5), 391–400. [Google Scholar]
- Thalen, M. , van Oorsouw, W. M. W. J. , Volkers, K. M. , Taminiau, E. F. , & Embregts, P. J. C. M. (2021). Integrated emotion‐oriented care for older people with ID ‐ defining and understanding intervention components of a person‐centred approach. Journal of Policy and Practice in Intellectual Disabilities, 18(3), 178–186. [Google Scholar]
- Thalen, M. , van Oorsouw, W. M. W. J. , Volkers, K. M. & Embregts, P. J. C. M. (2021). Support needs of older people with intellectual disabilities: An exploratory study among psychologists in The Netherlands. Journal of Intellectual Disabilities. [DOI] [PMC free article] [PubMed]
- * Underwood, M. A. , Umbreit, J. , & Liaupsin, C. (2009). Efficacy of a systematic process for designing function‐based interventions for adults in a community setting. Education and Training in Developmental Disabilities, 44(1), 25–38. [Google Scholar]
- van Minnen A., Savelsberg P. M., Hoogduin K. A. L. (1994). A Dutch version of the Psychopathology Inventory for Mentally Retarded Adults (PIMRA). Research in Developmental Disabilities, 15(4), 269–278. [DOI] [PubMed] [Google Scholar]
- Van Nieuwenhuizen, C. , Schene, A. H. , Koeter, M. W. J. , & Huxley, P. J. (2001). The Lancashire Quality of Life Profile: modification and psychometric evaluation. Social Psychiatry Psychiatric Epidemiology, 36, 36–44. [DOI] [PubMed] [Google Scholar]
- Van Puyenbroeck, J. , Maes, B. , & Laeremans, P. (2005). Vitessa (Version 0.1) [Computer software; Available at https://ppw.kuleuven.be/pserg/vitessa]. University of Leuven, Belgium.
- * Van Puyenbroeck, J. , & Maes, B. (2009). The effect of reminiscence group work on life satisfaction, self‐esteem and mood of ageing people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 22(1), 23–33. [Google Scholar]
- * Vlaskamp, C. , & van der Putten, A. (2009). Focus on interaction: The use of an individualized support program for persons with profound intellectual and multiple disabilities. Research in Developmental Disabilities, 30(5), 873–883. [DOI] [PubMed] [Google Scholar]
- Vlaskamp, C. , Fonteine, H. , Tadema, A. , & Munde, V. (2010). Handleiding bij de lijst 'Alertheid van mensen met zeer ernstige verstandelijke en meervoudige beperkingen'. Groningen, The Netherlands: Stichting Kinderstudies. [Google Scholar]
- * Wagemaker, E. , Dekkers, T. J. , Agelink van Rentergem, J. A. , Volkers, K. M. , & Huizenga, H. M. (2017). Advances in mental health care: Five N = 1 studies on the effects of the robot seal Paro in adults with severe intellectual disabilities. Journal of Mental Health Research in Intellectual Disabilities, 10(4), 309–320. [Google Scholar]
- Ware, J. , Snow, K. K. , Kosinski, M. , & Grandek, B. (1993). SF36 Health survey manual and interpretation guide. Boston, MA: The Health Institute, New England Medical Centre. [Google Scholar]
- * Watchman, K. , Mattheys, K. , McKernon, M. , Andreis, F. , & Murdock, J. (2020). A person‐centred approach to implementation of psychosocial interventions with people who have an intellectual disability and dementia. A participatory action study. Journal of Applied Research in Intellectual Disabilities, 34(1), 164–177. [DOI] [PubMed] [Google Scholar]
- Wechsler, D. (1999). The Wechsler Abbreviated Scale for Intelligence. San Antonio, TX: The Psychological Corporation. [Google Scholar]
- Weiner, M. F. , Martin‐Cook, K. , Svetlik, D. A. , Saine, K. , Foster, B. , & Fontaine, C. S. (2000). The quality of life in late‐stage dementia (QUALID) scale. Journal of American Medical Directors Association, 1(3), 114–116. [PubMed] [Google Scholar]
- Wieland, J. , Wardenaar, K. J. , Fontein, E. , & Zitman, F. G. (2012). Utility of the brief symptom inventory (BSI) in psychiatric outpatients with intellectual disabilities. Journal of Intellectual Disability Research, 56(9), 843–853. [DOI] [PubMed] [Google Scholar]
- Whittemore, R. , & Knafl, K. (2005). The integrative review: Updated methodology. Journal of Advanced Nursing, 52, 546–553. [DOI] [PubMed] [Google Scholar]
- World Health Organisation (2018). Genes and chromosomal diseases. https://www.who.int/genomics/public/geneticdiseases/en/index1.html.
- Xenitidis, K. , Thornicroft, G. , Leese, M. , Slade, M. , Fotiadou, M. , Philp, H. , Sayer, J. , Harris, E. , McGee, D. , & Murphy, D. G. (2000). Reliability and validity of the CANDID ‐ a needs assessment instrument for adults with learning disabilities and mental health problems. British Journal of Psychiatry, 176, 473–478. [DOI] [PubMed] [Google Scholar]
- Zijlstra, H. P. (2003). Dansen met olifanten, een onderzoek naar de implementatie van het opvoedingsprogramma in de zorg voor mensen met ernstig meervoudige beperkingen (academisch proefschrift). Groningen, The Netherlands: Stichting Kinderstudies. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.