

1. CASE PRESENTATION
An 18‐year‐old male without any significant medical history presented to the emergency department (ED) for evaluation of severe generalized abdominal pain that began immediately after sliding head first into second base during a baseball game. He also reported 2 episodes of non‐bloody, non‐bilious vomiting. Upon arrival, the patient was in moderate distress secondary to pain and with the following vital signs: temperature 36.8°C, blood pressure 117/75 mmHg, heart rate 127 beats per minute, respiratory rate 19 breaths per minute, and oxygen saturation 100% on room air. Physical examination revealed significant diffuse abdominal tenderness to palpation; however, the abdomen was without rebound, guarding, or peritoneal signs. A focused assessment with sonography for trauma (FAST) examination was subsequently performed that demonstrated intra‐abdominal free fluid (Figure 1). General surgery was immediately consulted based on the abnormal point‐of‐care ultrasound (POCUS) findings. Computed tomography of the abdomen/pelvis confirmed a moderate amount of fluid and blood within the peritoneal cavity as well as a localized mesenteric hematoma of the right mid lower abdomen (Figure 2). The patient was taken for emergent diagnostic laparoscopy converted to an open small bowel resection with findings of a large mesenteric hematoma with intra‐abdominal hemorrhage secondary to a mesenteric vessel tear at a ruptured Meckel's diverticulum.
FIGURE 1.
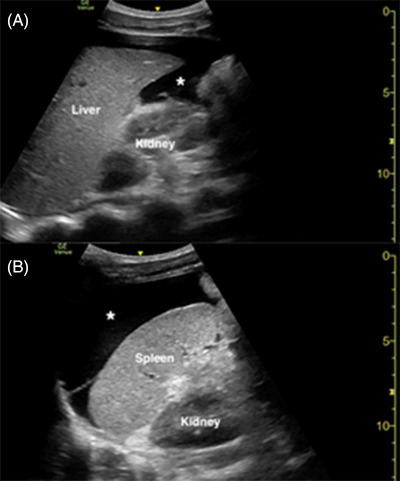
Point‐of‐care ultrasound demonstrating intra‐abdominal free fluid (asterisk) in the caudal liver edge of a longitudinal right upper quadrant view (A) and in the subphrenic space of a longitudinal left upper quadrant view (B)
FIGURE 2.
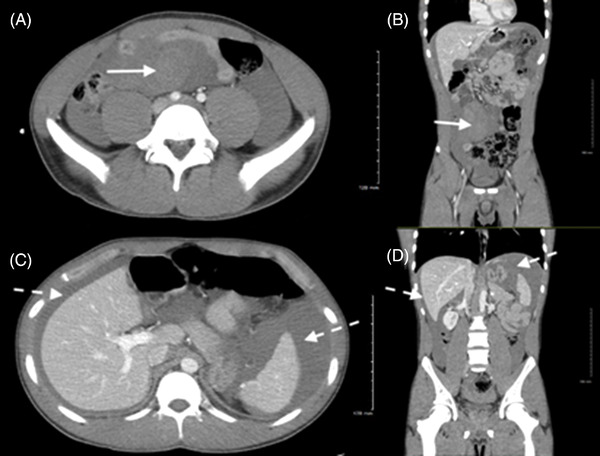
Computed tomography of the abdomen/pelvis demonstrating a localized mesenteric hematoma (solid arrow) of the right mid lower abdomen in axial (A) and coronal (B) planes. Computed tomography of the abdomen/pelvis demonstrating a moderate amount of fluid and blood (dotted arrows) within the peritoneal cavity in axial (C) and coronal (D) planes
2. DIAGNOSIS
Mesenteric hematoma with intra‐abdominal hemorrhage from ruptured Meckel's diverticulum.
3. DISCUSSION
The FAST examination, which is highly specific for detecting intra‐abdominal free fluid, is an essential bedside tool for the ED evaluation of trauma. 1 , 2 , 3 , 4 , 5 To the best of our knowledge, this is the first description of emergency physician‐performed FAST, which identified a rare complication of intra‐abdominal hemorrhage from a ruptured Meckel's diverticulum. Pertinent to our case, a positive FAST conveys valuable prognostic information in normotensive patients with blunt abdominal trauma. 6 , 7 The POCUS ultrasound findings were critical in expediting confirmatory imaging and emergent surgical consultation. This report illustrates the imperative role of a timely FAST for hemodynamically stable patients in the particular setting of blunt abdominal trauma.
CONFLICTS OF INTEREST
The authors have nothing to disclose.
DISCLAIMER
This research was supported in part by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Harris J, Vassallo S, Finan CD, Kalivoda EJ. Point‐of‐care ultrasound evaluation of blunt abdominal trauma. JACEP Open. 2022;3:e12786. 10.1002/emp2.12786
REFERENCES
- 1. Melniker LA, Leibner E, McKenney MG, et al . Randomized controlled clinical trial of point‐of‐care, limited ultrasonography for trauma in the emergency department: the first sonography outcomes assessment program trial. Ann Emerg Med. 2006;48(3):227‐235. [DOI] [PubMed] [Google Scholar]
- 2. Tsui CL, Fung HT, Chung KL, et al. Focused abdominal sonography for trauma in the emergency department for blunt abdominal trauma. Int J Emerg Med. 2008;1(3):183‐187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Patel NY, Riherd JM. Focused assessment with sonography for trauma: methods, accuracy, and indications. Surg Clin North Am. 2011;91(1):195‐207. [DOI] [PubMed] [Google Scholar]
- 4. O'Brien KM, Stolz LA, Amini R, et al. Focused assessment with sonography for trauma examination: reexamining the importance of the left upper quadrant view. J Ultrasound Med. 2015;34(8):1429‐1434. [DOI] [PubMed] [Google Scholar]
- 5. Lobo V, Hunter‐Behrend M, Cullnan E, et al. Caudal edge of the liver in the right upper quadrant (RUQ) view is the most sensitive area for free fluid on the FAST exam. West J Emerg Med. 2017;18(2):270‐280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Moylan M, Newgard CD, Ma OJ, et al. Association between a position ED FAST examination and therapeutic laparotomy in normotensive blunt trauma patients. J Emerg Med. 2007;33(3):265‐271. [DOI] [PubMed] [Google Scholar]
- 7. Dammers D, El Moumni M, Hoogland II, et al. Should we perform a FAST exam in haemodynamically stable patients presenting after blunt abdominal injury: a retrospective cohort study. Scand J Trauma Resusc Emerg Med. 2017;25(1):1. [DOI] [PMC free article] [PubMed] [Google Scholar]