

Key Points
Question
Is topical synthetic hypericin ointment, 0.25%, activated with visible light an effective and safe photodynamic therapy (PDT) for early-stage mycosis fungoides−cutaneous T-cell lymphoma (MF/CTCL)?
Findings
This multicenter phase 3 randomized clinical trial including 169 patients with MF/CTCLfound that topical hypericin PDT was more effective than placebo after 1 cycle of treatment for 6 weeks (index lesion response rate, 16% vs 4%); responses increased to 40% after 2 cycles, 49% after 3 cycles, and were seen in patch and plaque lesions. Adverse events were primarily mild application-site skin reactions.
Meaning
Topical synthetic hypericin activated with visible light is an effective and well-tolerated PDT for early-stage MF/CTCL.
Abstract
Importance
Given that mycosis fungoides−cutaneous T-cell lymphoma (MF/CTCL) is chronic, there is a need for additional therapies with minimal short- and long-term adverse effects. Topical synthetic hypericin ointment, 0.25%, activated with visible light is a novel, nonmutagenic photodynamic therapy (PDT).
Objectives
To determine the efficacy and safety of topical synthetic hypericin ointment, 0.25%, activated with visible light as a nonmutagenic PDT in early-stage MF/CTCL.
Design, Settings, and Participants
This was a multicenter, placebo-controlled, double-blinded, phase 3 randomized clinical trial (FLASH study) conducted from December 2015 to November 2020 at 39 academic and community-based US medical centers. Participants were adults (≥18 years) with early-stage (IA-IIA) MF/CTCL.
Interventions
In cycle 1, patients were randomized 2:1 to receive hypericin or placebo to 3 index lesions twice weekly for 6 weeks. In cycle 2, all patients received the active drug for 6 weeks to index lesions. In cycle 3 (optional), both index and additional lesions received active drug for 6 weeks.
Main Outcomes and Measures
The primary end point was index lesion response rate (ILRR), defined as 50% or greater improvement in modified Composite Assessment of Index Lesion Severity (mCAILS) score from baseline after 6 weeks of therapy for cycle 1. For cycles 2 and 3, open label response rates were secondary end points. Adverse events (AEs) were assessed at each treatment visit, after each cycle, and then monthly for 6 months. Data analyses were performed on December 21, 2020.
Results
The study population comprised 169 patients (mean [SD] age, 58.4 [16.0] years; 96 [57.8%] men; 120 [72.3%] White individuals) with early-stage MF/CTCL. After 6 weeks of treatment, hypericin PDT was more effective than placebo (cycle 1 ILRR, 16% vs 4%; P = .04). The ILRR increased to 40% in patients who received 2 cycles of hypericin PDT (P < .001 vs cycle 1 hypericin) and to 49% after 3 cycles (P < .001 vs cycle 1 hypericin). Significant clinical responses were observed in both patch and plaque type lesions and were similar regardless of age, sex, race, stage IA vs IB, time since diagnosis, and number of prior therapies. The most common treatment-related AEs were mild local skin (13.5%-17.3% across cycles 1-3 vs 10.5% for placebo in cycle 1) and application-site reactions (3.2%-6.9% across cycles 1-3 vs 4% for placebo in cycle 1). No drug-related serious AEs occurred.
Conclusion and Relevance
The findings of this randomized clinical trial indicate that synthetic hypericin PDT is effective in early-stage patch and plaque MF/CTCL and has a favorable safety profile.
Trial Registration
ClinicalTrials.gov Identifier: NCT02448381
This randomized clinical trial of hypericin ointment, 0.25%, for patients with early-stage mycosis fungoides−cutaneous T-cell lymphoma examines lesion response rates and adverse events to determine the efficacy and safety of this novel photodynamic therapy.
Introduction
Mycosis fungoides−cutaneous T-cell lymphoma (MF/CTCL) is a rare non-Hodgkin lymphoma of skin-homing malignant T-cells presenting as patches or plaques in early stages and may progress to tumors, erythroderma, and/or extracutaneous sites in advanced stages.1,2 Early-stage MF/CTCL is treated with primarily skin-directed therapies.2,3 Use of current skin-directed therapies are limited by (1) acute toxic effects (contact dermatitis with topical chemotherapy/retinoids, alopecia with radiation therapy, local inflammation with imiquimod, phototoxic effects of UV light), (2) long-term cumulative toxic effects (skin atrophy with topical corticosteroids, skin cancers with some types of long-term UV phototherapy, alopecia/anhidrosis/fibrosis from radiation therapy), or (3) inadequate efficacy in plaques (vs patches) because of reduced skin penetration. Given MF/CTCL chronicity, short-term tolerability and long-term safety are important treatment considerations supporting an urgent need for additional CTCL skin-directed therapies.
Hypericin, naturally found in plants (Hypericum genus),4,5,6 is tumoricidal as a stand-alone drug7,8,9,10,11,12 and with activation by visible light.4,13,14,15,16,17,18,19,20 It is preferentially absorbed into malignant cells, particularly in vivo.7,21 However, in vitro noncancerous cells can also absorb hypericin.8,22,23 Other factors contributing to its tumoritropic attributes are blood flow, vessel permeability, and affinity for interstitial constituents.24 Visible light in the yellow-red spectrum (range, 500-650 nm) is expected to penetrate 1 to 2 mm into the skin20,25 and activates hypericin localized in the perinuclear region within the endoplasmic reticulum and Golgi apparatus.26,27 Activated hypericin triggers the caspase-signaling cascade through reactive oxygen species resulting in apoptosis via the mitochondrial pathway.28 In vitro, hypericin inhibits malignant T-cell proliferation and induces apoptosis in CTCL and adult T-cell leukemia cell lines compared with normal T-cells.29,30 Synthetic hypericin was nonmutagenic in 2 Ames tests and an in vitro cytogenetic assay.
In clinical trials for other indications, systemic hypericin dose-limiting toxicity was phototoxicity, which led to the development of synthetic hypericin ointment (HyBryte) as a topical photodynamic therapy (PDT) activated by noncarcinogenic visible spectrum light. A phase 2 clinical trial of synthetic hypericin PDT demonstrated a statistically significant reduction in early-stage MF/CTCL skin lesions after 6 weeks of treatment (overall response rate, 58.3%; 7 of 12 patients) and was well-tolerated.31 In addition, given its nonmutagenic mechanism of action, hypericin PDT has a potential safety advantage over traditional UV phototherapy for long-term use in patients with MF. We report the efficacy and safety of treatment with hypericin PDT vs placebo in patients with early-stage MF/CTCL in this large placebo-controlled randomized clinical trial.
Methods
Design
The FLASH study was a phase 3, placebo-controlled, double-blind, multicenter randomized clinical trial conducted to evaluate the efficacy and safety of synthetic hypericin ointment PDT in patients with early-stage MF/CTCL (stages IA-IIA per international guidelines32). The trial protocol is available in Supplement 1. As agreed with the US Food and Drug Administration (FDA) at the time of the study design, given the lack of consensus of standard first-line skin-directed therapies for early-stage MF/CTCL, a placebo comparator was chosen to better elucidate the drug’s biologic activity, maximize ability to adequately blind treatments, and collect concurrent placebo response data during a reasonable but limited time period. Adults with stage IA-IIA MF/CTCL, and 3 or more evaluable and discrete patch and plaque lesions were enrolled and treated twice weekly during a 6-week cycle for up to 3 cycles (Figure 1): cycle 1, randomized to active drug vs placebo treatment of the 3 prospectively identified index lesions (primary efficacy end point cycle); cycle 2, crossover of patients in the placebo group to receive index-lesion treatment, as well as all cycle 1 patients who received active drug but had not achieved index-lesion complete clinical response in cycle 1; and cycle 3 (optional), open-label treatment of all lesions (index and nonindex) selected by the patient and physician.
Figure 1. Study Schema.

Abbreviation: ITT, intent-to-treat population.
The study protocol was approved by each study site’s independent institutional review board in accordance with ethical principles of the Declaration of Helsinki.33 The study was consistent with the International Conference on Harmonization and Good Clinical Practice guidelines and applicable regulatory requirements and in compliance with the protocol. Written informed consent was obtained from all patients before study participation. The study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guidelines.
Participants
Adult patients (≥18 years) with stage IA-IIA MF/CTCL (≥3 patch and/or plaque lesions) were enrolled at 39 academic and community-based US medical centers. Exclusion criteria included use of topical steroids or other skin-directed therapies (eg, nitrogen mustard) on index lesions within 2 weeks of enrollment; treatment with psoralen UV-A or narrow band UV-B phototherapy, topical carmustine, systemic steroids, or other systemic CTCL therapies within 3 weeks; exposure to electron beam irradiation in the treatment field within 3 months; having substantial systemic immunosuppression; experiencing spontaneous improvement in condition; or having advanced MF/CTCL (stage IIB-IV; tumor, erythrodermic). All enrolled cases were confirmed by skin biopsy.
Intervention
Before randomization, 3 representative index lesions (to include patch and plaque lesions if both present) were identified for treatment and evaluation (Figure 1A). Patients were randomized 2:1 to either hypericin, 0.25%, or placebo ointments (cycle 1 only). Ointment was applied to each index lesion, covered with opaque dressing or clothing for 18 to 24 hours, followed by administration of visible light (range, 500 to 650 nm using an Ultralite Panelite). Light treatment started at 5 joules per cm2 (J/cm2) and increased by 1 J/cm2 with each treatment until a mild skin reaction was seen in treated lesions (grade 1 erythema) or until a maximum light dose of 12 J/cm2 was reached. Index lesions were treated twice weekly for each 6-week cycle. Treatment response was assessed after a 2-week rest period (week 8 for cycle 1, week 16 for cycle 2, and week 24 for cycle 3) to allow treatment-induced skin reactions to subside. Posttreatment outcomes were evaluated in all patients 6 months after the last treatment cycle evaluation visit (at 48 weeks/12 months for those who completed cycle 3).
Outcomes and Measures
The primary objective was to evaluate the ability of the initial 6-week course (cycle 1) of hypericin PDT to induce a treatment response, defined as a 50% or more improvement in the cumulative modified Composite Assessment of Index Lesion Severity (mCAILS) score from baseline to the 8-week evaluation visit. The mCAILS score for each index lesion is the sum of the severity subscores of 4 categories: erythema, scaling, plaque elevation, and surface area. Severity was graded from 0 (none) to 8 (severe) for erythema and scaling; 0 to 3 for plaque elevation; and 0 to 18 for surface area.34
A secondary objective evaluated the effect of a second 6-week course of treatment (cycle 2) on index lesions with less than complete response in the initial cycle 1 hypericin PDT and to extend the data on the response rate of hypericin PDT in untreated lesions (after cycle 1, placebo patients crossover). In the optional, open-label portion of the study (cycle 3), the objective was to determine the effect of hypericin PDT treatment with maximal coverage, including assessment of systemic hypericin blood levels. Study investigators were specifically trained on index lesion selection criteria and mCAILS scoring during site initiation visits and when new personnel joined the study. Additionally, the same study investigator was expected to perform all mCAILS scores throughout the study for a given patient to ensure consistency.
Statistical Analysis
The primary efficacy analyses were calculated in the intent-to-treat (ITT) population defined as all randomized patients who received 1 hypericin PDT treatment in each study group. The ITT population was defined for each treatment cycle. Safety analyses were conducted in the same population.
The primary end point for the trial was the proportion of treatment response (defined as ≥50% reduction in total mCAILS score) between the 2 treatment groups at the end of cycle 1. A patient was a responder if the cumulative mCAILS score of the 3 index lesions was 50% or more improvement compared with baseline. Patients with a cumulative mCAILS score of 0 were classified as having a complete clinical response (CR).
The data monitoring committee conducted 1 interim analysis (October 9, 2018), reviewed and locked data from 104 patients who had completed cycle 1 and the week 8 evaluation (primary end point). The interim analysis assessed the primary efficacy end point and key safety end points between treatments in an unblinded manner, and a sample size recalculation was performed. To preserve an overall type I error rate of 0.05, the alpha spending function approach with an O’Brien-Fleming type of stopping rule was used with a 2-sided significance level of α = .001 for the interim analysis and a 2-sided significance level of α = .049 for the final analysis.35 After the interim analysis, the data monitoring committee recommended that enrollment continue to a minimum of 160 evaluable patients.
A prospectively defined logistic regression analysis on treatment response was performed with treatment and baseline total mCAILS score as independent variables. Treatment difference was compared using the Wald test. Data analyses were performed on December 21, 2020, using SAS. version 9.1.3 (SAS Institute).
Results
From 39 sites across the US, 169 patients were randomized into the trial conducted from December 2015 to November 2020; however, 3 of these patients (2 to hypericin; 1 to placebo) did not participate because the investigator decided to change their therapeutic regimen (eFigure 1 in Supplement 2). The study’s ITT population comprised 166 patients (mean [SD] age, 58.4 [16.0] years; 96 [57.8%] men; 70 [42.2%] women; 4 [2.4%] Asian, 39 [23.5%] Black, 120 [72.3%] White, and 3 [1.8%] individuals of other race and ethnicity) who were randomized 2:1 to hypericin PDT (116 participants) or placebo (50 participants) in cycle 1 (2:1). The treatment populations were balanced in terms of demographic information, baseline disease characteristics, and prior therapy (Table 1). Of note, the study included patients relatively naive to treatment as well as those with multiple prior therapies. Patients in both treatment groups received a median of 12 study drug applications (maximum allowed) in cycle 1 (hypericin and placebo) and in both cycles 2 and 3.
Table 1. Demographic Information and Baseline Characteristics of the ITT Population.
| Characteristic | No. (%) | P value for comparisona | ||
|---|---|---|---|---|
| Hypericin | Placebo | Total | ||
| Participants, No. | 116 | 50 | 166 | NA |
| Men | 69 (59.5) | 27 (54.0) | 96 (57.8) | .51 |
| Women | 47 (40.5) | 23 (46.0) | 70 (42.2) | |
| Race | ||||
| Asian | 4 (3.4) | 0 (0.0) | 4 (2.4) | .15 |
| Black | 27 (23.3) | 12 (24.0) | 39 (23.5) | |
| White | 84 (72.4) | 36 (72.0) | 120 (72.3) | |
| Other responseb | 1 (0.9) | 2 (4.0) | 3 (1.8) | |
| Age, mean (SD) [range], y | 57.9 (15.9) [19-99] | 59.4 (16.3) [20-89] | 58.4 (16.0) [19-99] | .60 |
| Tumor stage | ||||
| IA | 72 (62.1) | 31 (62.0) | 103 (62.0) | .31 |
| IB | 39 (33.6) | 19 (38.0) | 58 (34.9) | |
| IIA | 5 (4.3) | 0 | 5 (3.0) | |
| Disease duration, mean (SD) [range], moc | 75.8 (78.9) [0.4-375.6] | 82.3 (91.2) [0.5-396.1] | 77.8 (82.5) [0.4-396.1] | .64 |
| Baseline mCAILS score, mean (SD) [range] | 32.6 (13.7) [8-73] | 32.6 (12.5) [3-55] | 32.6 (13.3) [3-73] | >.99 |
| Prior MF/CTCL therapies, median [range] | 3.0 [0-19] | 2.0 [0-12] | 3.6 (3.4) [0-19] | .08 |
Abbreviations: ITT, intent-to-treat population; mCAILS, modified Composite Assessment of Index Lesion Severity; MF/CTCL, mycosis fungoides−cutaneous T-cell lymphoma.
P value is calculated from t test for continuous variables and from χ2 test for categorical variables.
Includes any other race and/or Hispanic/Latino ethnicity.
Defined as time of first reported diagnosis of MF/CTCL to randomization.
Efficacy
After cycle 1 (6-week treatment plus 2-week rest; ie, week 8), the hypericin PDT-treated group had a statistically significant index lesion response rate (ILRR) of 16% (19 of 116 patients) compared with 4% in the placebo-treated group (2 of 50 patients; P = .04). The ILRR increased to 40% for the group that received hypericin PDT in both cycles 1 and 2 (44 of 110 patients vs hypericin PDT group after cycle 1; P < .001). After the optional cycle 3, the ILRR for the group that received hypericin PDT increased further to 49% (38 of 78 patients vs hypericin PDT group after cycle 1 and cycle 2; P = .05; Figure 2A).
Figure 2. Clinical Responses to Hypericin PDT, by Treatment Time, Disease Stage, and Prior Therapy.
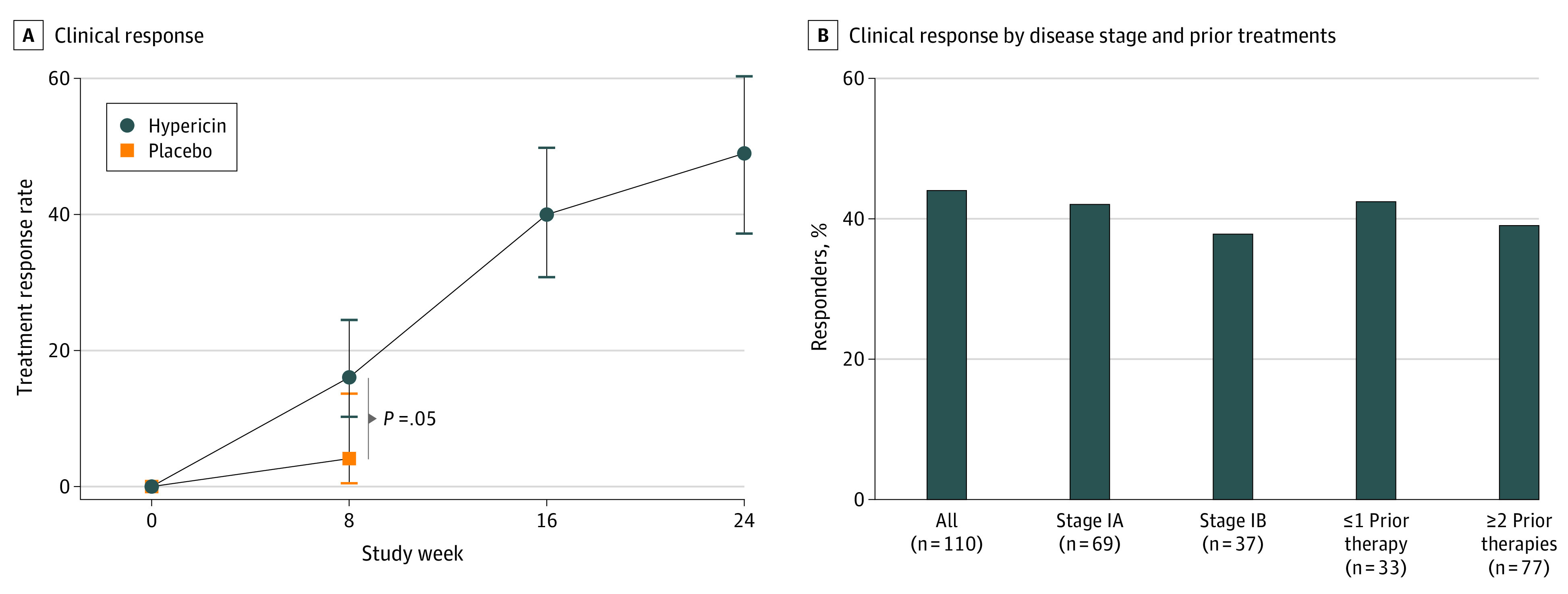
A, Week 8 represents the patient outcomes of cycle 1 with hypericin PDT (n = 116) or placebo (n = 50) for 6 wks plus a 2-wk rest period before evaluation; week 16, outcomes for patients who received hypericin PDT in cycle 1 and for 6 wks in cycle 2 (n = 44 of 110) plus another 2-wk rest; and week 24, outcomes for patients who received hypericin PDT in cycles 1 and 2 and continued with optional cycle 3 (n = 38 of 78) plus a 2-wk rest. The statistical significance of the RR comparison at the end of cycle 1 was calculated by logistic regression describing responder status when ≥50% improvement in cumulative mCAILS scores from baseline was seen as a function of treatment assignment and baseline mCAILS score. Errors bars describe the 95% CIs using the method of Clopper-Pearson. RRs in cycle 2 for patients who initially received placebo in cycle 1 (22%) were similar to the RRs in the patients receiving hypericin PDT in cycle 1 (16%); data not shown. B, Treatment RRs after 16 wk of hypericin PDT for patients receiving hypericin PDT in both cycles 1 and 2, as a function of disease stage (stages IA and IB; owing to small sample size, stage IIA data are not included) and previous CTCL therapy. Treatment RR was similar across these defined subpopulations. CTCL refers to cutaneous T-cell lymphoma; mCAILS, modified Composite Assessment of Index Lesion Severity; PDT, photodynamic therapy; and RRs, response rates.
Analysis of all patients who received hypericin PDT (ie, including those who received placebo in cycle 1 followed by hypericin PDT in cycle 2) demonstrated a consistent ILRR of 18% after 6 weeks of treatment and 40% after 12 weeks of treatment. The ILRR was similar in patients with MF/CTCL stage IA (42.0%; n = 69) vs stage IB (37.8%; n = 37) and across number of prior treatments (42.4% in patients receiving ≤1 prior treatment; 39.0% for ≥2 prior treatments; Figure 2B) as well as across age, sex, race, and time since MF/CTCL diagnosis. Only 5 patients with MF/CTCL stage IIA enrolled in the trial, and all were randomized to hypericin PDT; 4 of these 5 patients received treatment with a response rate of 25%.
Complete CRs were observed in each cycle (cycle 1, 2 of 166 participants; cycle 2, an additional 7 of 155; cycle 3, additional 6 of 110). All CRs were observed in patients receiving hypericin PDT. Among the 9 patients with CRs during the first 2 cycles, the median (range) age was 56 (20-79) years; 6 (67%) were women; 1 patient was Asian, 4 were Black, and 3 were White; 7 patients had MF/CTCL stage IA and 2 had stage IB; and the median (range) of prior therapies was 2 (0-6) therapies. The improvement in the number of CRs at the end of cycle 2 compared with the end of cycle 1 for those patients receiving hypericin PDT in both cycles (n = 110) was statistically significant (95% CI, 2.0-11.5; P = .03).
Consolidated response rates across all individual index lesions were similar in both patch and plaque lesions (patches identified by mCAILS plaque subscore of 0; plaques identified by mCAILS plaque subscore of 1, 2, or 3; Figure 3). Individual index lesions that achieved a mCAILS score of 0 after at least 6 weeks of hypericin PDT had a median duration of response (elapsed days with 50% of lesions retaining clearance) of 231 days.
Figure 3. Consolidated Response Rates Across All Individual Index Lesions, Patch vs Plaque.

Consolidated response rate of individual lesions (total vs patch vs plaque) at end of cycles 1 and 2 (all data are reported as a percentage of lesions achieving 50% or more improvement relative to baseline).
Durability of treatment response was improved with increased number of hypericin PDT cycles. A logistic regression model evaluating the duration of treatment response using the number of hypericin PDT cycles and the duration of previous disease as independent variables indicated a statistically significant correlation with the number of treatment cycles (standard error rate, 16.49; P = .01) but not with the previous duration of disease.
Safety
Overall across all treatment cycles (hypericin and placebo), treatment-emergent AEs of any causality (ie, any/all AEs that occurred during the entire study period regardless of relationship to study intervention) were reported in 70% of patients (116 of 166) and were similar in both treatment groups during cycle 1 with the exception of slightly more treatment-site AEs seen with hypericin PDT: skin reactions (16.4% hypericin PDT vs 10.5% placebo), pruritus (cycle 1, 5.2% hypericin PDT vs 4.0% placebo), application-site pain and/or irritation (cycle 1, 6.9% hypericin PDT vs 4.0% placebo), application-site pruritus (cycle 1, 4.3% hypericin PDT vs 2.0% placebo) that in some cases mildly increased with more prolonged treatment with hypericin PDT during cycles 2 and 3 (Table 2).
Table 2. Adverse Events Reported by 5% or More Patients in Any Treatment Group.
| Adverse event | No. (%) | |||||
|---|---|---|---|---|---|---|
| Cycle 1 | Hypericin | Total | ||||
| Hypericin | Placebo | Cycle 2 | Cycle 3 | Overall | ||
| Total participants, No. | 116 | 50 | 155 | 110 | 161 | 166 |
| Patients with ≥1 TEAEa | 56 (48.3) | 27 (54.0) | 66 (42.6) | 49 (44.5) | 108 (67.1) | 116 (69.9) |
| All skin/subcutaneous tissue-related disordersb | 19 (16.4) | 5 (10.0) | 21 (13.5) | 19 (17.3) | 48 (29.8) | 53 (31.9) |
| Pruritusb | 6 (5.2) | 2 (4.0) | 2 (1.3) | 5 (4.5) | 12 (7.5) | 14 (8.4) |
| URI | 8 (6.9) | 4 (8.0) | 2 (1.3) | 2 (1.8) | 12 (7.5) | 16 (9.6) |
| Viral URI | 4 (3.4) | 0 | 4 (2.6) | 4 (3.6) | 11 (6.8) | 11 (6.6) |
| Application-site painb | 8 (6.9) | 2 (4.0) | 5 (3.2) | 6 (5.5) | 16 (9.9) | 17 (10.2) |
| Application-site pruritusb | 5 (4.3) | 1 (2.0) | 5 (3.2) | 0 | 9 (5.6) | 9 (5.4) |
| Fatigue | 3 (2.6) | 1 (2.0) | 3 (1.9) | 2 (1.8) | 8 (5.0) | 9 (5.4) |
| Headache | 5 (4.3) | 3 (6.0) | 5 (3.2) | 2 (1.8) | 10 (6.2) | 13 (7.8) |
Abbreviations: AE, adverse event; TEAE, treatment-emergent adverse event; URI, upper respiratory tract infection.
TEAE was defined as an AE that was new or worsened in severity after the first dose of study drug and within 1 month following the last evaluation visit. Patients were counted only once for each AE they experienced. All adverse events were coded using the Medical Dictionary for Regulatory Activities, version 20. Most of the AEs were mild, required no intervention or treatment, and did not interfere with continued therapy use and study participation. AE-related discontinuation rate was 1.2% during the study.
TEAE of special interest.
Mild treatment-related AEs were reported in 23% (n = 38) of patients, moderate in 9% (n = 15), and severe in 3 (2%). Most of the AEs that were possibly related (11%) or related (15% ) to hypericin PDT were skin reactions including pruritus, hyperpigmentation, burning, pain, and irritation, and application-site pain and pruritus. The majority of these were mild, required no intervention or treatment, and did not interfere with continued treatment and study participation. During cycle 1, the study discontinuation rate was 5% of the hypericin PDT group and 10% of the placebo group. All patients who received hypericin PDT during cycles 1 through 3 had a study discontinuation rate during the treatment cycles of 5.0%, with only 1.2% being AE related.
A severe treatment-related AE occurred in 3 patients. One patient had application-site pain in cycle 3; it required no intervention and resolved. Another patient experienced erythema in cycle 1; it resolved after a pause in treatment, and treatment was resumed without issue. The third was a patient with application-site pain during cycle 1; the participant withdrew from the study.
There were 5 serious adverse events (SAEs) during the study, but all were considered unrelated to hypericin PDT; 4 were related to underlying medical conditions or medications unrelated to MF/CTCL. There were no deaths during the study. There were no clinically meaningful changes in any hematologic or clinical chemistry parameters, nor any trending changes in vital signs among the study participants. Systemic hypericin blood concentration was measured in 29 patients, sampled 24 hours after ointment application across the last 4 treatments in cycle 3 (time point of maximum exposure). No hypericin was detected in the blood using a validated method with a detection limit of 5 ng/mL.
Discussion
This double-blind, placebo-controlled phase 3 randomized clinical trial demonstrated that hypericin PDT is an effective and well-tolerated treatment for early-stage MF/CTCL. Hypericin PDT resulted in a significant improvement in ILRR compared with placebo in cycle 1 with continued improvement in cycle 2 and in optional cycle 3. A significantly greater proportion of patients treated with hypericin PDT had experienced CR after cycle 2. Importantly, treatment benefit was similar in patch and plaque lesions, suggesting enhanced depth of penetration with visible light spectrum wavelengths (eFigure 2 in Supplement 2), which would be an advantage over some current MF/CTCL skin-directed therapies. Notably, the treatment response rate of hypericin PDT in cycle 1 (16%) was considerably lower than previously observed in the prior phase 2 trial (58.3%) but still statistically significant compared with placebo treatment. One important consideration is the prior trial used different end point criteria to assess treatment response (reduction in lesion size) rather than the multifaceted mCAILS score used in this trial (ie, incorporating erythema, scaling, and thickness, as well as lesion size). The mCAILS score is the standard skin assessment tool for individual lesion clinical response assessment. It is recommended for all early-stage MF/CTCL clinical trials and endorsed by US and international MF/CTCL specialty group consensus publications.36
Hypericin PDT showed no evidence of systemic absorption and had an acceptable safety profile with possibly related or related AEs that were limited to pruritus, hyperpigmentation, burning, pain, irritation, and application-site pain and/or pruritus; all were self-limited. Having a variety of treatment options is critical for managing early-stage MF/CTCL. In addition to efficacy, other factors such as patient comorbidities, access, and AEs affect treatment selection. Hypericin PDT has a similar treatment schedule to traditional UV phototherapy but is more targeted to skin surface area and requires a light panel in the 500 to 650 nm spectrum that is potentially safer in patients with severe actinic skin damage and skin cancer history. Because hypericin PDT requires occlusion 12 to 24 hours after hypericin application, its use may be limited in certain anatomic sites (face), although site application limitations exist for all other current MF/CTCL skin-directed therapies (eg, topical chemotherapy not used in body folds or the central face).
Future directions include assessing clinical response and AEs with continuous hypericin PDT treatment without the 2-week rest periods and for longer periods to reflect real-world practice. Hypericin PDT is also potentially suited for administration with an at-home light unit and could be a valuable user-friendly option to improve access to treatment for patients who live far from a health care center and/or prefer the shift away from in-office treatments that occurred during the COVID-19 pandemic.
Limitations
Limitations of the study included incomplete information correlating clinical response with (1) skin pigmentation (Fitzpatrick scale), although no difference in response was observed across race; (2) clinical or histologic subtypes of MF/CTCL (eg, folliculotropic); (3) presence or absence of large-cell transformation because these were not required data for study entry, although folliculotropism or large-cell transformation were not specifically excluded.
Another study limitation was the short duration of treatment for each cycle (6-week treatment, 2-week rest before response assessment) and overall treatment period (maximum 6 months) which differs from real-world skin-directed treatment courses. However, during the trial design, placebo treatment of more than 8 weeks was considered unacceptable in patients with active MF/CTCL, thus a crossover design was used for cycle 2—patients initially randomized to placebo in cycle 1 could receive active treatment thereafter. These second and third cycles in which all patients received hypericin PDT allowed safety and efficacy assessments to be conducted during a longer treatment period. Outcomes at these later time points (ILRR, 40% and 49% at wk 16 and 24) demonstrated clinical response kinetics that were comparable to other MF/CTCL skin-directed therapies studied during longer clinical trial periods (eg, bexarotene gel, mechlorethamine gel).37,38,39 To date, all FDA-approved MF/CTCL therapies are indicated for disease refractory to previous MF/CTCL therapy. As demonstrated in Figure 2, hypericin PDT efficacy was similar irrespective of disease stage or refractory status (eg, ≥2 prior MF/CTCL therapies).
Conclusions
The FLASH randomized clinical trial demonstrated that hypericin PDT is a clinical advance for the field with its comparable efficacy in patch and plaque lesions and favorable short-term and, potentially, long-term safety profile. Given that MF/CTCL requires long-term disease management and that many patients using current skin-directed therapies experience short- and/or long-term adverse effects, limited access, and waning efficacy, these findings are an important contribution to MF/CTCL patient care.
Trial Protocol
eFigure 1. CONSORT Diagram
eFigure 2. Visible-Light Skin Penetration
Data Sharing Statement
References
- 1.Talpur R, Singh L, Daulat S, et al. Long-term outcomes of 1,263 patients with mycosis fungoides and Sézary syndrome from 1982 to 2009. Clin Cancer Res. 2012;18(18):5051-5060. doi: 10.1158/1078-0432.CCR-12-0604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dummer R, Vermeer MH, Scarisbrick JJ, et al. Cutaneous T cell lymphoma. Nat Rev Dis Primers. 2021;7(1):61. doi: 10.1038/s41572-021-00296-9 [DOI] [PubMed] [Google Scholar]
- 3.National Comprehensive Cancer Network . Cutaneous Lymphomas, version 2, 2022. Accessed June 22, 2022. https://www.nccn.org/guidelines
- 4.Durán N, Song PS. Hypericin and its photodynamic action. Photochem Photobiol. 1986;43(6):677-680. doi: 10.1111/j.1751-1097.1986.tb05646.x [DOI] [PubMed] [Google Scholar]
- 5.Kubin A, Wierrani F, Burner U, Alth G, Grünberger W. Hypericin: the facts about a controversial agent. Curr Pharm Des. 2005;11(2):233-253. doi: 10.2174/1381612053382287 [DOI] [PubMed] [Google Scholar]
- 6.Jendželovská Z, Jendželovský R, Kuchárová B, Fedoročko P. Hypericin in the Light and in the Dark: Two sides of the same coin. Front Plant Sci. 2016;7:560. doi: 10.3389/fpls.2016.00560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Noell S, Mayer D, Strauss WS, Tatagiba MS, Ritz R. Selective enrichment of hypericin in malignant glioma: pioneering in vivo results. Int J Oncol. 2011;38(5):1343-1348. [DOI] [PubMed] [Google Scholar]
- 8.Kamuhabwa AR, Agostinis P, D’Hallewin MA, Kasran A, de Witte PA. Photodynamic activity of hypericin in human urinary bladder carcinoma cells. Anticancer Res. 2000;20(4):2579-2584. [PubMed] [Google Scholar]
- 9.Anker L, Gopalakrishna R, Jones K, Law R, Couldwell W. Hypericin in adjuvant brain tumor therapy. Drugs Future. 1995;20(5):511-519. doi: 10.1358/dof.1995.020.05.305540 [DOI] [Google Scholar]
- 10.Blank M, Lavie G, Mandel M, et al. Antimetastatic activity of the photodynamic agent hypericin in the dark. Int J Cancer. 2004;111(4):596-603. doi: 10.1002/ijc.20285 [DOI] [PubMed] [Google Scholar]
- 11.Couldwell WT, Gopalakrishna R, Hinton DR, et al. Hypericin: a potential antiglioma therapy. Neurosurgery. 1994;35(4):705-709. doi: 10.1227/00006123-199410000-00017 [DOI] [PubMed] [Google Scholar]
- 12.Zhang W, Law RE, Hinton DR, Couldwell WT. Inhibition of human malignant glioma cell motility and invasion in vitro by hypericin, a potent protein kinase C inhibitor. Cancer Lett. 1997;120(1):31-38. doi: 10.1016/S0304-3835(97)00287-5 [DOI] [PubMed] [Google Scholar]
- 13.Chan PS, Koon HK, Wu ZG, et al. Role of p38 MAPKs in hypericin photodynamic therapy-induced apoptosis of nasopharyngeal carcinoma cells. Photochem Photobiol. 2009;85(5):1207-1217. doi: 10.1111/j.1751-1097.2009.00572.x [DOI] [PubMed] [Google Scholar]
- 14.Cavarga I, Brezáni P, Cekanová-Figurová M, Solár P, Fedorocko P, Miskovský P. Photodynamic therapy of murine fibrosarcoma with topical and systemic administration of hypericin. Phytomedicine. 2001;8(5):325-330. doi: 10.1078/0944-7113-00057 [DOI] [PubMed] [Google Scholar]
- 15.Cole CD, Liu JK, Sheng X, et al. Hypericin-mediated photodynamic therapy of pituitary tumors: preclinical study in a GH4C1 rat tumor model. J Neurooncol. 2008;87(3):255-261. doi: 10.1007/s11060-007-9514-0 [DOI] [PubMed] [Google Scholar]
- 16.Chen B, de Witte PA. Photodynamic therapy efficacy and tissue distribution of hypericin in a mouse P388 lymphoma tumor model. Cancer Lett. 2000;150(1):111-117. doi: 10.1016/S0304-3835(99)00381-X [DOI] [PubMed] [Google Scholar]
- 17.Chen B, Roskams T, de Witte PA. Antivascular tumor eradication by hypericin-mediated photodynamic therapy. Photochem Photobiol. 2002;76(5):509-513. doi: 10.1562/0031-8655(2002)076<0509:ATEBHM>2.0.CO;2 [DOI] [PubMed] [Google Scholar]
- 18.Du HY, Olivo M, Tan BK, Bay BH. Hypericin-mediated photodynamic therapy induces lipid peroxidation and necrosis in nasopharyngeal cancer. Int J Oncol. 2003;23(5):1401-1405. doi: 10.3892/ijo.23.5.1401 [DOI] [PubMed] [Google Scholar]
- 19.Besic Gyenge E, Forny P, Lüscher D, Laass A, Walt H, Maake C. Effects of hypericin and a chlorin based photosensitizer alone or in combination in squamous cell carcinoma cells in the dark. Photodiagnosis Photodyn Ther. 2012;9(4):321-331. doi: 10.1016/j.pdpdt.2012.03.006 [DOI] [PubMed] [Google Scholar]
- 20.Sanovic R, Verwanger T, Hartl A, Krammer B. Low dose hypericin-PDT induces complete tumor regression in BALB/c mice bearing CT26 colon carcinoma. Photodiagnosis Photodyn Ther. 2011;8(4):291-296. doi: 10.1016/j.pdpdt.2011.04.003 [DOI] [PubMed] [Google Scholar]
- 21.Kamuhabwa AA, Cosserat-Gerardin I, Didelon J, et al. Biodistribution of hypericin in orthotopic transitional cell carcinoma bladder tumors: implication for whole bladder wall photodynamic therapy. Int J Cancer. 2002;97(2):253-260. doi: 10.1002/ijc.1594 [DOI] [PubMed] [Google Scholar]
- 22.Huntosova V, Stroffekova K. Hypericin in the dark: foe or ally in photodynamic therapy? Cancers (Basel). 2016;8(10):E93. doi: 10.3390/cancers8100093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Huntosova V, Novotova M, Nichtova Z, et al. Assessing light-independent effects of hypericin on cell viability, ultrastructure and metabolism in human glioma and endothelial cells. Toxicol In Vitro. 2017;40:184-195. doi: 10.1016/j.tiv.2017.01.005 [DOI] [PubMed] [Google Scholar]
- 24.Van de Putte M, Roskams T, Vandenheede JR, Agostinis P, de Witte PA. Elucidation of the tumoritropic principle of hypericin. Br J Cancer. 2005;92(8):1406-1413. doi: 10.1038/sj.bjc.6602512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Avci P, Gupta A, Sadasivam M, et al. Low-level laser (light) therapy (LLLT) in skin: stimulating, healing, restoring. Semin Cutan Med Surg. 2013;32(1):41-52. [PMC free article] [PubMed] [Google Scholar]
- 26.Vandenbogaerde AL, Cuveele JF, Proot P, Himpens BE, Merlevede WJ, de Witte PA. Differential cytotoxic effects induced after photosensitization by hypericin. J Photochem Photobiol B. 1997;38(2-3):136-142. doi: 10.1016/S1011-1344(96)07446-5 [DOI] [PubMed] [Google Scholar]
- 27.Vandenbogaerde AL, Delaey EM, Vantieghem AM, Himpens BE, Merlevede WJ, de Witte PA. Cytotoxicity and antiproliferative effect of hypericin and derivatives after photosensitization. Photochem Photobiol. 1998;67(1):119-125. doi: 10.1111/j.1751-1097.1998.tb05174.x [DOI] [PubMed] [Google Scholar]
- 28.Garg AD, Agostinis P. ER stress, autophagy and immunogenic cell death in photodynamic therapy-induced anti-cancer immune responses. Photochem Photobiol Sci. 2014;13(3):474-487. doi: 10.1039/C3PP50333J [DOI] [PubMed] [Google Scholar]
- 29.Fox FE, Niu Z, Tobia A, Rook AH. Photoactivated hypericin is an anti-proliferative agent that induces a high rate of apoptotic death of normal, transformed, and malignant T lymphocytes: implications for the treatment of cutaneous lymphoproliferative and inflammatory disorders. J Invest Dermatol. 1998;111(2):327-332. doi: 10.1046/j.1523-1747.1998.00278.x [DOI] [PubMed] [Google Scholar]
- 30.Xu L, Zhang X, Cheng W, et al. Hypericin-photodynamic therapy inhibits the growth of adult T-cell leukemia cells through induction of apoptosis and suppression of viral transcription. Retrovirology. 2019;16(1):5. doi: 10.1186/s12977-019-0467-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Rook AH, Wood GS, Duvic M, Vonderheid EC, Tobia A, Cabana B. A phase II placebo-controlled study of photodynamic therapy with topical hypericin and visible light irradiation in the treatment of cutaneous T-cell lymphoma and psoriasis. J Am Acad Dermatol. 2010;63(6):984-990. doi: 10.1016/j.jaad.2010.02.039 [DOI] [PubMed] [Google Scholar]
- 32.Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(6):1713-1722. doi: 10.1182/blood-2007-03-055749 [DOI] [PubMed] [Google Scholar]
- 33.World Medical Association . World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. doi: 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
- 34.Olsen EA, Whittaker S, Kim YH, et al. ; International Society for Cutaneous Lymphomas; United States Cutaneous Lymphoma Consortium; Cutaneous Lymphoma Task Force of the European Organisation for Research and Treatment of Cancer . Clinical end points and response criteria in mycosis fungoides and Sézary syndrome: a consensus statement of the International Society for Cutaneous Lymphomas, the United States Cutaneous Lymphoma Consortium, and the Cutaneous Lymphoma Task Force of the European Organisation for Research and Treatment of Cancer. J Clin Oncol. 2011;29(18):2598-2607. doi: 10.1200/JCO.2010.32.0630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.O’Brien PC, Fleming TR. A multiple testing procedure for clinical trials. Biometrics. 1979;35(3):549-556. doi: 10.2307/2530245 [DOI] [PubMed] [Google Scholar]
- 36.Olsen EA, Whittaker S, Willemze R, et al. Primary cutaneous lymphoma: recommendations for clinical trial design and staging update from the ISCL, USCLC, and EORTC. Blood. 2021;blood.2021012057. doi: 10.1182/blood.2021012057 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Breneman D, Duvic M, Kuzel T, Yocum R, Truglia J, Stevens VJ. Phase 1 and 2 trial of bexarotene gel for skin-directed treatment of patients with cutaneous T-cell lymphoma. Arch Dermatol. 2002;138(3):325-332. doi: 10.1001/archderm.138.3.325 [DOI] [PubMed] [Google Scholar]
- 38.Heald P, Mehlmauer M, Martin AG, Crowley CA, Yocum RC, Reich SD; Worldwide Bexarotene Study Group . Topical bexarotene therapy for patients with refractory or persistent early-stage cutaneous T-cell lymphoma: results of the phase III clinical trial. J Am Acad Dermatol. 2003;49(5):801-815. doi: 10.1016/S0190-9622(03)01475-0 [DOI] [PubMed] [Google Scholar]
- 39.Lessin SR, Duvic M, Guitart J, et al. Topical chemotherapy in cutaneous T-cell lymphoma: positive results of a randomized, controlled, multicenter trial testing the efficacy and safety of a novel mechlorethamine, 0.02%, gel in mycosis fungoides. JAMA Dermatol. 2013;149(1):25-32. doi: 10.1001/2013.jamadermatol.541 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eFigure 1. CONSORT Diagram
eFigure 2. Visible-Light Skin Penetration
Data Sharing Statement