

Abstract
Glucagon-like peptide 1 receptor agonists (GLP-1RAs) have gained an important place in the management of diabetes management because of their exceptional glucose-lowering, weight lowering and cardiovascular (CV) benefits. Despite recommendations by various clinical practice guidelines and benefits, their usage in clinical practice was limited because of being injectable in nature. Oral semaglutide is a novel GLP-1RA with 94% homology to human GLP-1 which is co-formulated with absorption enhancer sodium N-(8-[2-hydroxybenzoyl] amino) caprylate (SNAC), that overcomes the challenges of peptide absorption in the acidic conditions of the stomach. Oral semaglutide has been evaluated in an extensive phase 3 clinical trial programme named Peptide Innovation for Early Diabetes Treatment (PIONEER) which demonstrated its robust glucose and weight lowering effects against other comparators. The evolution of the GLP-1RA class to include an oral pill will facilitate the use of this class of agents much earlier in the diabetes treatment cascade owing to wider acceptance from patients and clinicians alike. The current review discusses the various aspects of oral semaglutide and its place in clinical practice.
Keywords: CVOT, diabetes, GLP-1RA, oral semaglutide, PIONEER, weight loss
INTRODUCTION
Glucagon-like peptide 1 receptor agonists (GLP-1RAs) are one of the important classes of antidiabetic agents used in the management of type 2 diabetes. GLP-1RAs act on multiple pathophysiologies of type 2 diabetes (at least six [Pancreas (a and b cells), liver, muscle, brain, incretin] out of eight). GLP-1RAs have significant glucose-dependent HbA1c reduction, weight reduction, cardiovascular (CV) safety benefits and low risk of hypoglycaemia.[1,2,3,4] GLP-1RAs can be classified based on the route of administration, half-life, molecular weight and their human origin. Some of the GLP-1RAs are exenatide, liraglutide, albiglutide, dulaglutide, lixisenatide and semaglutide.[5]
Despite a plethora of advantages with GLP-1RAs, their usage is limited because of their injectable nature presenting challenges in the initiation and adherence to the use of GLP-1RAs. After decades of efforts and research, oral semaglutide, the first oral GLP-1RA, is recently being developed and is now available for use in routine clinical practice. This oral formulation of GLP-1RA will be able to address the challenges of poor patient acceptance, adherence and persistence.[6,7,8] This oral semaglutide formulation will be a game-changer in the management of diabetes with its multiple benefits. This mini-review discussed the various aspects of this oral formulation of oral semaglutide.
CHEMICAL STRUCTURE
Semaglutide is a human analogue of native GLP-1RA with minor modifications. Semaglutide is a GLP-1RA, which acts like other GLP-1RA when given via oral or s.c. route of administration. It is also available in doses of 0.5, 1 mg and 2 mg via s.c. route of administration.[9] It is hydrophilic, low molecular weight GLP-1RA. It has 94% structural homology with human glucagon-like peptide (GLP). In the semaglutide molecule, changes were done at three places: 8, 26 and 34 positions as seen in Figure 1. At the eighth position, alanine is replaced with alpha aminoisobutyric acid, which protects it from degradation by dipeptidyl peptidase-4 (DPP-4) enzymes. At the 26th position, the C-18 fatty acid chain is attached to lysine, which provides strong binding to albumin. At the 34th position, lysine is replaced with arginine, to prevent the wrong binding of the C-18 fatty diacid chain at the wrong position. The half-life of semaglutide is increased to 160 h with these structural modifications.[9]
Figure 1.

Structure of semaglutide
MECHANISM OF ORAL BIOAVAILABILITY
Oral administration of semaglutide or other GLP-1RAs leads to negligible bioavailability of 0.01%.[10,11] Protein and peptides like semaglutide get degraded by proteolytic enzymes and low pH. Moreover, due to high molecular weight, these are not able to permeate through GI epithelium leading to low absorption. This leads to lower absorption and lower bioavailability.[11,12] The site of absorption for semaglutide is the stomach. Various studies like ligation studies and scintographic studies showed stomach is the main site of absorption for semaglutide.[11,12]
The bioavailability of semaglutide has been increased by 100 times when formulated along with sodium N-(8-[2-hydroxybenzoyl] amino) caprylate (SNAC). SNAC is a small fatty acid derivative that promotes absorption across the gastric epithelium. SNAC increases the localized pH around the tablet and protects it from proteolytic degradation by enzymes and acidic pH. It helps in the absorption of semaglutide through the GI epithelium via the transcellular route. The action of SNAC is time- and concentration-dependent and is fully reversible.[11]
In various pharmacological studies, the dose of SNAC has been from 150 to 600 mg and it has been found that 300 mg of SNAC is the optimum dose to get maximum bioavailability. When co-formulated with 300 mg SNAC, 1% of semaglutide is usually absorbed in the stomach.[13]
DOSE FINDING STUDY
Based on a dose-finding study (Phase 2 trial) in which different doses of oral semaglutide (2.5, 5, 10, 20 and 40 mg) were studied and three doses of oral semaglutide 3, 7 and 14 mg were selected for phase 3 trials to have optimal benefit–risk profiles. All these doses were formulated along with 300 mg of SNAC.[14]
CLINICAL EVIDENCE/CLINICAL EFFICACY
Glycaemic efficacy
Oral semaglutide has been explored widely in a robust clinical trial programme named Peptide Innovation for Early Diabetes Treatment (PIONEER). In the PIONEER trial programme, oral semaglutide has been explored through various stages of diabetes from early duration to mid- and large duration of diabetes with various kinds of antidiabetic drugs as baseline medication. Oral semaglutide has also been used in the chronic kidney disease (CKD) population and for CV safety. In PIONEER clinical trial programme, 9543 subjects were enrolled and 5707 subjects have been randomized to oral semaglutide. Oral semaglutide has demonstrated up to a mean 1.5% reduction in HbA1c and up to 5 kg of weight loss in clinical trials. PIONEER trial programme has showed around 70% of subjects had achieved their glycaemic target of HbA1c <7%.[15,16,17,18,19,20,21,22] Tables 1 show the design of the PIONEER clinical trial programme.
Table 1.
Study design of PIONEER clinical trials
| Trial ID (subjects) | Duration (weeks) | Oral semaglutide | Comparator | Randomization ratio | Blinding | Strat ification by background medication | Stratification by other parameters | Background antidiabetic medication during trial | ||
|---|---|---|---|---|---|---|---|---|---|---|
| PIONEER 1 (n=703) | 26 | 3 mg | 7 mg | 14 mg | Placebo | 1:1:1:1 | Double-blind | Japanese/non-Japanese | None | |
| PIONEER 2 (n=822) | 52 | 14 mg | Empagliflozin 25 mg | 1:1 | Open-label | No stratification | Met | |||
| PIONEER 3 (n=1864) | 78 | 3 mg | 7 mg | 14 mg | Sitagliptin 100 mg | 1:1:1:1 | Double-blind, double-dummy | Met/Met+SU | Japanese/non-Japanese | Met±SU |
| PIONEER 4 (n=711) | 52 | 14 mg | Liraglutide 1.8 mg and placebo | 2:2:1 | Double-blind, double-dummy | Met±SGLT2i | Japanese/non-Japanese | Met±SGLT2i | ||
| PIONEER 5 (n=324) | 26 | 14 mg | Placebo | 1:1 | Double-blind | Met/SU±Met/Basal insulin±Met | eGFR 30-44/45-59 mL/min/1.73m2 | Met±SU or basal insulin† | ||
| PIONEER 6 (n=3183) | Event-driven | 14 mg | Placebo | 1:1 | Double-blind | Presence of CVD or risk factors only | Add-on to standard of care | |||
| PIONEER 7 (n=504) | 52 | Flexible dose adjustment | Sitagliptin 100 mg | 1:1 | Open-label | Metformin/TZD/ SU/SGLT2i | 1–2 OADs (Met, SU, SGLT2i, TZD) | |||
| PIONEER 8 (n=731) | 52 | 3 mg | 7 mg | 14 mg | Placebo | 1:1:1:1 | Double-blind | Basal insulin/basal-bolus/premix insulin±Met | Japanese/non-Japanese | Basal or basal-bolus or premix insulin±Met |
A post-hoc analysis showed HbA1c reduction up to 2.6% in a sub-group of patients with a baseline HbA1c >9%.[23] Another post hoc analysis of PIONEER trials showed Asians were more respondent to semaglutide in terms of HbA1c reduction and weight reduction.[24] It is worth mentioning that in PIONEER 8 trial, most of the Asians (66) were Indians (51).[22]
EARLY STAGE OF DIABETES
PIONEER 1 has established the clinical efficacy of oral semaglutide as monotherapy and first-line drug after diet and exercise. This is a double-blinded, randomized controlled trial that evaluated the change in HbA1c at 26 weeks with placebo compared with oral semaglutide at doses of 3 mg, 7 mg and 14 mg (1:1:1:1) in 703 adult patients with untreated type 2 diabetes mellitus (T2DM). The duration of diabetes was 3.5 years, body mass index (BMI) 31.8 kg/m2 and mean HbA1c 8.0%. The dose was titrated on 4 weekly bases from 3 to 7 and 7 to 14 mg in their respective arms [Table 1].[16]
Significant HbA1c reduction has been seen with all three doses 3, 7 and 14 mg in comparison to placebo whereas weight reduction was significant with 7 and 14 mg in comparison to placebo. With oral semaglutide 14 mg dose, 80% of subjects have achieved their glycaemic target of HbA1c <7%. This trial presents robust evidence for the usage of oral semaglutide as monotherapy in an early stage of diabetes just after diet and exercise even before metformin. The regulatory approval for oral semaglutide is as an add-on to metformin or before, if metformin is contraindicated.[16]
MID STAGE DIABETES
Oral semaglutide has been explored in PIONEER 2, 3, 4 and 7 trials with mid-duration of diabetes ranging from 7.4 to 8.8 years.[17,18,19,20]
When patients fail to achieve glycaemic control while on metformin with or without other oral antihyperglycaemic agents, current treatment guidelines recommend considering a variety of options including GLP-1RAs, sodium-glucose co-transporter-2 (SGLT2) inhibitors, DPP-4 inhibitors, sulphonylureas and thiazolidinediones.[25,26]
PIONEER 2 trial is an open-label, randomized, parallel-group, multicentre trial in which 822 patients with T2DM were randomized to two arms of oral semaglutide 14 mg and empagliflozin 25 mg in a 1:1 ratio. The inclusion criteria were patients on baseline medication of metformin (≥1500 mg or maximal tolerated) for at least 90 days and HbA1c between 7% and 10.5%. The mean duration of T2DM was 7.4 years.[17]
Oral semaglutide 14 mg showed significant greater reduction in HbA1c in comparison to empagliflozin 25 mg at 26 (−0.5% [95% CI: −0.7%, −0.4%]) and 52 weeks. Oral semaglutide also showed a significant reduction in body weight in comparison to empagliflozin 25 mg at week 52 (−0.9 kg [95% CI: −1.6, −0.2 kg]). Empagliflozin did not show weight loss after 26 weeks whereas oral semaglutide showed a consistent weight reduction event at week 38. A significant reduction in waist circumference was also seen with oral semaglutide arm in comparison to empagliflozin. Most of the weight loss due to semaglutide was due to fat loss because of its action on satiety centres. More number of subjects (71.62%) have achieved their glycaemic targets in comparison to empagliflozin at the end of week 52. Most of the adverse events were mild to moderate in nature. Nausea is the most common side effect and has been seen in 19.8% of patients in the oral semaglutide arm. Oral semaglutide was well tolerated, with a safety profile consistent with that of GLP-1RAs. Thus, this trial establishes the efficacy and safety of oral semaglutide in patients with T2DM in addition to metformin in comparison to empagliflozin.[17]
PIONEER 3 trial was a randomized double-blind, double-dummy, parallel-group, multicentre, multinational phase 3a trial, which compared the efficacy, long-term adverse event (AE) profile and tolerability of oral semaglutide with sitagliptin as an add-on to metformin ± sulphonylurea in patients with T2DM. One thousand eight hundred and sixty-four patients with T2DM with HbA1c 7–10.5% and on background medication (metformin with or without a sulphonylurea for at least 90 days) were randomized to oral semaglutide 3, 7, 14 mg or sitagliptin 100 mg once daily (1:1:1:1) for 78 weeks. The mean duration of T2DM was 8.6 years.[18]
Oral semaglutide 7 and 14 mg significantly lowered HbA1c versus sitagliptin at weeks 26, 52 and 78 demonstrating superiority. Overall, oral semaglutide 7 and 14 mg showed greater reductions in HbA1c versus sitagliptin across overall and all baseline HbA1c subgroups (HbA1c at baseline (≤8.0%, >8.0–≤9.0%, >9.0%). A greater number of patients in the semaglutide 3- and 7-mg groups achieved an HbA1c <7% as compared with patients on sitagliptin. Oral semaglutide significantly lowered body weight versus sitagliptin at weeks 26, 52 and 78.[18] Gastrointestinal AEs were the most frequent AEs to cause premature discontinuation. Nausea was the most common AE with oral semaglutide 7 and 14 mg (up to 15.1%). Safety and tolerability profile of oral semaglutide was consistent with other GLP-1RAs.[18] PIONEER 3 establishes the oral semaglutide as a better option in comparison to sitagliptin in addition to metformin with or without sulphonylurea.
PIONEER 7 was a 52-week open-label trial that compared the efficacy and safety of once-daily oral semaglutide (with flexible-dose adjustment based on prespecified HbA1c and tolerability criteria to approximate treatment individualization in clinical practice) with the DPP-4 inhibitor sitagliptin, as an add-on to existing glucose-lowering medication (one or two oral antidiabetic agents, i.e., metformin, sulphonylureas, SGLT-2 inhibitors or thiazolidinediones), in patients with T2DM. Five hundred and four patients with T2DM were randomized into two arms - a flexible dose of oral semaglutide based on HbA1c and gastrointestinal tolerability (3 mg for 8 weeks, followed by either continuation of 3, 7 or 14 mg) or sitagliptin 100 mg once daily. The mean duration of T2DM was 8.8 years and HbA1c was between 7.5 and 9.5%.[19]
A greater proportion of patients achieved an HbA1c <7% with oral semaglutide (63%) as compared with sitagliptin 100 mg once daily (28%). Significant improvement in HbA1c (-0.5, 95% CI -0.7 to -0.4; P < 0.0001) and decrease in body weight (-1.9, 95% CI -2.6 to -1.2; P < 0.0001) at 52 weeks were achieved with oral semaglutide as compared with sitagliptin 100 mg. 9% of patients discontinued treatment in semaglutide arm due to AEs. The overall safety profile is consistent and in line with GLP-1RAs as a class. This trial establishes the superiority of flexible-dose adjustment of oral semaglutide, which is usually followed in clinical practise in comparison with sitagliptin.[19]
PIONEER 4 compares the efficacy and safety of oral semaglutide with a subcutaneously injected GLP-1 receptor agonist, liraglutide, and placebo in patients with T2DM uncontrolled on background metformin with or without an SGLT2 inhibitor. This is a 52-week, randomized, double-blind, double-dummy, active- and placebo-controlled, parallel-group, multicentred trial conducted at 100 trial sites in 12 countries. It included 722 patients with T2DM and baseline HbA1c between 7 and 9.5% randomized to oral semaglutide 14 mg once daily, liraglutide 1.8 mg once daily or placebo (2:2:1). The mean duration of T2DM was 7.6 years.[20]
The change in HbA1c at 26 weeks for each treatment group was −1.3%, −1.1% and −0.1% for semaglutide, liraglutide and placebo, respectively (P < 0.0001 for semaglutide versus placebo, and P = 0.0056 for semaglutide versus liraglutide). At 52 weeks, the change in HbA1c from baseline was superior for semaglutide as compared with liraglutide (−0.3% [95% CI: −0.4%, −0.1%]). Semaglutide was superior compared with liraglutide and placebo with regard to change in body weight at 26 weeks, with a reduction of 4.7, 3.2 and 0.7 kg, respectively (P < 0.0001 for all comparisons). A greater number of patients in the semaglutide group achieved an HbA1c <7% compared with the liraglutide and placebo groups. Oral semaglutide was superior to liraglutide and placebo in HbA1c reduction and body weight loss over both comparators at weeks 26 and 52. The safety and tolerability of oral semaglutide were consistent with liraglutide.[20]
Because many patients are reluctant to initiate or intensify therapy by injection, oral semaglutide might be an effective treatment option, potentially leading to earlier initiation of GLP-1 receptor agonist therapy in the diabetes treatment continuum of care. Thus, PIONEER 4 establishes oral semaglutide as a better option in comparison to injectable liraglutide in terms of better HbA1c reduction, weight loss and patient compliance.
LATE STAGE OF DIABETES
PIONEER 8 was a randomized, double-blind, placebo-controlled, parallel-group, multicentre, multinational trial. In this trial, 731 patients with T2DM inadequately controlled on insulin with or without metformin were randomized to oral semaglutide 3, 7 or 14 mg once daily or placebo once daily (1:1:1:1). The mean duration of diabetes was 15 years. Fifty-one patients from India were also enrolled in this trial. PIONEER 8 trial was done in the late stage of diabetes in patients already on different types of insulin.[21]
All doses of oral semaglutide showed a significant reduction in HbA1c and weight in comparison to placebo at weeks 26 and 52. With the use of oral semaglutide, there was a significant reduction in insulin dose with 3, 7 and 14 mg in comparison to placebo at weeks 26 and 52. The rate of hypoglycaemia was also not significantly different when compared with the placebo. Thus, PIONEER 8 trial establishes that oral semaglutide can be safe and effective even in the late stage of diabetes. Oral semaglutide can be used as a treatment intensification option even in addition to insulin.[21]
PIONEER 5 was a randomized, double-blind, placebo-controlled, parallel-group, multicentre, multinational trial that included 324 subjects with T2DM and estimated glomerular filtration rate (eGFR) 30–59 mL/min/1.73 m2, on stable doses of 1–2 oral antidiabetic drugs (OADs) (metformin, SU) and/or basal insulin for ≥ 90 days randomized to oral semaglutide 14 mg and placebo (1:1). The mean duration of T2DM was 14 years, and 60% of patients had an eGFR of 45 to <60 mL/min/1.73 m2.[22]
Oral semaglutide showed a significant reduction in HbA1c and weight. More number of patients achieved their glycaemic targets in comparison to placebo. Nausea was more frequent (19%) in the oral semaglutide arm. Thus, this trial showed similar HbA1c reductions in subjects with renal impairment compared to other PIONEER trials.[22]
Overall nausea rates were ~ 15% to 20% in patients treated with oral semaglutide. Despite the rates of nausea observed in the PIONEER trials, only a small increase in discontinuation of oral semaglutide as compared with the active drug arms was found.[15,16,17,18,19,20,21,22]
GI side effects are usually transient in nature and can be managed by proper patient counselling. The patient should be counselled about the GI AEs. GLP-1RA should be started with a lower dose of 3 mg and then accelerate the dose after 1 month as per recommended dosing conditions. If required, the patient can be on the same dose even for more time so that patient can tolerate the dose. Patients should be advised to avoid high fat-rich meals and reduce the portion size of their meals. The patient should eat smaller meals and stop eating when feeling full. Patients should keep them hydrated via drinking water and other fluids. If GI side effects appear, depending upon the severity of GI events, either dose can be reduced or maintained or treatment can be stopped for some time and started again after a few days. A strategy to incorporate treatment pause, dosing flexibility and education to support GLP-1RA therapy persistence was evaluated in the PIONEER 6 trial. If AEs were manageable, dose escalation was continued as per the given schedule. However, if the AEs are problematic, the investigators could reduce the dose and the dose escalation was resumed once the symptoms were diminished or resolved. The strategy also has an option for treatment pause if needed. Twenty-three percentage of patients receiving oral semaglutide had greater than or equal to one treatment pause, of which 72% had only one treatment pause. Overall, more than 80% of treatment completers finished on oral semaglutide 14 mg dose.[27]
CV SAFETY
PIONEER 6 was a Cardiovascular Outcome Trial (CVOT) designed to evaluate the CV safety of oral semaglutide in comparison to placebo. This trial included 3183 patients with uncontrolled T2DM who were either ≥50 years old with established CV disease or CKD or ≥60 years old with CV risk factors only randomized to oral semaglutide 14 mg or placebo in addition to standard of care. This was an event-driven trial and 122 events were planned. The trial was concluded with 137 events with a duration of 16 months. 15.3% had CV risk factors without established CV disease or CKD. This trial has met its primary endpoint with 21% reduction in 3-point major cardiovascular event (3P-MACE) for non-inferiority (HR: 0.79 [0.57; 1.11] P value for non-inferiority: <0.0001; P value for superiority: 0.1749). For CV death, a hazard ratio of 0.49 [0.27; 0.92] was observed, and for all-cause death, the hazard ratio was 0.51 [0.31; 0.84]. There were 206 participants in PIONEER 6 from India. Thus, this PIONEER 6 trial established the CV safety of oral semaglutide, and CV superiority is yet to be established. Although Semaglutide Unabated Sustainability in Treatment of Type 2 Diabetes (SUSTAIN) 6 trial showed a significant reduction of 26% in 3P-MACE with s.c. semaglutide in comparison to placebo.[28,29]
A CV superiority trial under the name of SOUL study is an ongoing trial, which will give more clarity on the CV superiority of oral semaglutide in the future.
PLACE IN THERAPY AS FIRST LINE, SECOND LINE AND THIRD LINE
PIONEER 1 trial established the efficacy and safety of oral semaglutide as first-line drug after diet and exercise in the early duration of diabetes. Oral semaglutide is indicated as an adjunct to diet and exercise to improve glycaemic control in adults with T2DM in addition to metformin or where metformin is contraindicated as per Indian regulatory authorities. Additionally, oral semaglutide can be used as an add-on to metformin as a second-line drug as per the label approval from India and US. PIONEER 2-trial oral semaglutide has shown a significant reduction in HbA1c and weight as second-line drug in addition to metformin in comparison to empagliflozin. PIONEER 3, 4 and 7 also depict the efficacy and safety of oral semaglutide as a second- and third-line drug. PIONEER 5 and 8 also showed efficacy and safety of oral semaglutide as a second- and third-line drug.[15,16,17,18,19,20,21,22,30,31]
Thus, oral semaglutide can be used across the spectrum of diabetes as a first-, second- and third-line drug.
ROBUST INDICATIONS
Indications for oral semaglutide are shown in Figure 2. Figure 3 shows the potential place of oral semaglutide as per international treatment recommendations.[30,32,33] Oral semaglutide is approved for use in all stages of CKD irrespective of eGFR without any dose adjustment as per the US prescribing information. It can also be used in hepatic impairment in Child-Pugh scores A, B and C without any dose adjustment.[30,31]
Figure 2.
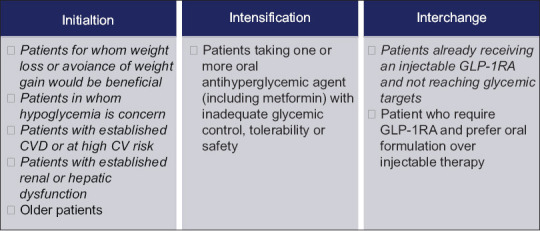
Indications for oral semaglutide
Figure 3.

Potential place of oral semaglutide in international treatment recommendations
POSOLOGY/DOSING CONDITIONS
Based on various pharmacological studies, dosing conditions have been optimized. Oral semaglutide has to be given after overnight fasting (~ 6 h) with up to 120 ml of water [Figure 4]. As food affects the absorption of semaglutide, post-dose fasting of 30 min is recommended before eating, drinking or taking any other medication. Oral semaglutide was initiated with the lowest dose and a 4-week dose escalation to reduce the risk of GI AEs.[14,30,34]
Figure 4.

Dosing conditions for oral semaglutide
DRUG–DRUG INTERACTIONS
Oral semaglutide has been found to be safe with most other commonly used drugs. Several other antidiabetic medications have been used as baseline medications in various PIONEER clinical trial programmes. Oral semaglutide delays gastric emptying. When co-administering oral medications, instruct patients to closely follow dosing instructions.
No clinical significant increase in exposure to semaglutide has been seen on omeprazole. Several other commonly used drugs like lisinopril, warfarin, metformin, digoxin, ethinyloestradiol/levonorgestrel, rosuvastatin and furosemide have been evaluated but no clinically relevant change in the exposure of semaglutide has been seen in drug–drug interaction studies [Figure 5]. A slight increase in exposure of levothyroxine 33% (90% CI: 125-142) at a dose of 600 mcg has been seen when administered along with oral semaglutide. Hence, we advise patients on levothyroxine should be strict with their dosing schedule and take it after 30 min of oral semaglutide administration and regularly monitor their thyroid profiles.[35,36,37,38]
Figure 5.

Drug–drug interactions with oral semaglutide
Drugs with a low therapeutic index like warfarin should need to be monitored closely. Although it is usual practice to do international normalized ratio (INR) monitoring with drugs like warfarin.[35,36,37,38]
CONTRAINDICATIONS
It has not been studied in patients with a history of pancreatitis. It is not for the treatment of type 1 diabetes mellitus. It is not recommended in pregnancy and lactation. It is contraindicated in patients with a personal or family history of medullary thyroid cancers (MTC) or patients with multiple endocrine neoplasia syndrome type 2 (MEN2).[30]
FUTURE INDICATIONS AND TRIALS
Oral semaglutide has been explored with higher doses of 25 and 50 mg in ongoing PIONEER plus trials.[39] Another trial under the name PIONEER TEEN is ongoing to see the efficacy and safety of semaglutide in children and teenagers with age 10 years to 17 years.[40] PIONEER REAL is a global prospective, non-interventional single-arm real-world study with oral semaglutide.[41] EVOKE and EVOKE plus are ongoing trials to see the effect of oral semaglutide in Alzheimer’s disease.[42] SOUL is an ongoing CV superiority trial with an objective to prove CV benefits with this molecule.
SUMMARY
Oral semaglutide is the world’s first oral GLP-1RA. This molecule has shown its place in all stages of diabetes and in addition to various antidiabetic drugs as seen in the PIONEER clinical trial programme. Oral semaglutide shows significant HbA1c reduction and weight reduction in comparison to sitagliptin, empagliflozin and liraglutide also. It has proven CV safety with tolerable GI AE at par with other GLP-1RAs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Tahrani AA, Barnett AH, Bailey CJ. Pharmacology and therapeutic implications of current drugs for type 2 diabetes mellitus. Nat Rev Endocrinol. 2016;12:566–92. doi: 10.1038/nrendo.2016.86. [DOI] [PubMed] [Google Scholar]
- 2.Burgmaier M, Heinrich C, Marx N. Cardiovascular effects of GLP-1 and GLP-1-based therapies:Implications for the cardiovascular continuum in diabetes? Diabetic Med. 2013;30:289–99. doi: 10.1111/j.1464-5491.2012.03746.x. [DOI] [PubMed] [Google Scholar]
- 3.Saraiva FK, Sposito AC. Cardiovascular effects of glucagon-like peptide 1 (GLP-1) receptor agonists. Cardiovasc Diabetol. 2014;13:142. doi: 10.1186/s12933-014-0142-7. doi:10.1186/1475-2840-13-80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Marso SP, Daniels GH, Brown-Frandsen K, Kristensen P, Mann JF, Nauck MA, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375:311–22. doi: 10.1056/NEJMoa1603827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kalra S, Bhattacharya S, Kapoor N. Contemporary classification of glucagon-like peptide 1 receptor agonists (GLP1RAs) Diabetes Ther. 2021;12:2133–47. doi: 10.1007/s13300-021-01113-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chung SW, Hil-lal TA, Byun Y. Strategies for non-invasive delivery of biologics. J Drug Target. 2012;20:481–501. doi: 10.3109/1061186X.2012.693499. [DOI] [PubMed] [Google Scholar]
- 7.Hamman JH, Enslin GM, Kotze AF. Oral delivery of peptide drugs:Barriers and developments. BioDrugs. 2005;19:165–77. doi: 10.2165/00063030-200519030-00003. [DOI] [PubMed] [Google Scholar]
- 8.Jensen L, Helleberg H, Roffel A, van Lier JJ, Bjørnsdottir I, Pedersen PJ, et al. Absorption, metabolism and excretion of the GLP-1 analogue semaglutide in humans and nonclinical species. Eur J Pharm Sci. 2017;104:31–41. doi: 10.1016/j.ejps.2017.03.020. [DOI] [PubMed] [Google Scholar]
- 9.Kalra S, Sahay R. A review on semaglutide:An oral glucagon-like peptide 1 receptor agonist in management of type 2 diabetes mellitus. Diabetes Ther. 2020;11:1965–82. doi: 10.1007/s13300-020-00894-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Drucker DJ. Advances in oral peptide therapeutics. Nat Rev Drug Discov. 2020;19:277–89. doi: 10.1038/s41573-019-0053-0. [DOI] [PubMed] [Google Scholar]
- 11.Buckley ST, Bækdal TA, Vegge A, Maarbjerg SJ, Pyke C, Ahnfelt-Rønne J, et al. Transcellular stomach absorption of a derivatized glucagon-like peptide-1 receptor agonist. Sci Transl Med. 2018;10:7047. doi: 10.1126/scitranslmed.aar7047. doi:10.1126/scitranslmed.aar7047. [DOI] [PubMed] [Google Scholar]
- 12.Renukuntla J, Vadlapudi AD, Patel A, Boddu SH, Mitra AK. Approaches for enhancing oral bioavailability of peptides and proteins. Int J Pharm. 2013;447:75–93. doi: 10.1016/j.ijpharm.2013.02.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Granhall C, Donsmark M, Blicher TM, Golor G, Søndergaard FL, Thomsen M, et al. Safety and pharmacokinetics of single and multiple ascending doses of the novel oral human GLP-1 analogue, oral semaglutide, in healthy subjects and subjects with type 2 diabetes. Clin Pharmacokinet. 2019;58:781–91. doi: 10.1007/s40262-018-0728-4. [DOI] [PubMed] [Google Scholar]
- 14.Davies M, Pieber TR, Hartoft-Nielsen ML, Hansen OKH, Jabbour S, Rosenstock J. Effect of oral semaglutide compared with placebo and subcutaneous semaglutide on glycemic control in patients with type 2 diabetes:A randomized clinical trial. JAMA. 2017;318:1460–70. doi: 10.1001/jama.2017.14752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Thethi TK, Pratley R, Meier JJ. Efficacy, safety and cardiovascular outcomes of once-daily oral semaglutide in patients with type 2 diabetes:The PIONEER programme. Diabetes Obes Metab. 2020;22:1263–77. doi: 10.1111/dom.14054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Aroda VR, Rosenstock J, Terauchi Y, Altuntas Y, Lalic NM, Morales Villegas EC, et al. PIONEER 1:Randomized clinical trial of the efficacy and safety of oral semaglutide monotherapy in comparison with placebo in patients with type 2 diabetes. Diabetes Care. 2019;42:1724–32. doi: 10.2337/dc19-0749. [DOI] [PubMed] [Google Scholar]
- 17.Rodbard HW, Rosenstock J, Canani LH, Deerochanawong C, Gumprecht J, Lindberg SØ, et al. Oral semaglutide versus empagliflozin in patients with type 2 diabetes uncontrolled on metformin:The PIONEER 2 trial. Diabetes Care. 2019;42:2272–81. doi: 10.2337/dc19-0883. [DOI] [PubMed] [Google Scholar]
- 18.Rosenstock J, Allison D, Birkenfeld AL, Blicher TM, Deenadayalan S, Jacobsen JB, et al. Effect of additional oral semaglutide vs sitagliptin on glycated hemoglobin in adults with type 2 diabetes uncontrolled with metformin alone or with sulfonylurea:The PIONEER 3 randomized clinical trial. JAMA. 2019;321:1466–80. doi: 10.1001/jama.2019.2942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pieber TR, Bode B, Mertens A, Cho YM, Christiansen E, Hertz CL, et al. PIONEER 7 investigators. Efficacy and safety of oral semaglutide with flexible dose adjustment versus sitagliptin in type 2 diabetes (PIONEER 7):a multicentre, open-label, randomised, phase 3a trial. Lancet Diabetes Endocrinol. 2019;7:528–39. doi: 10.1016/S2213-8587(19)30194-9. doi:10.1016/S2213-8587(19)30194-9. Epub 2019 Jun 9. Erratum in:Lancet Diabetes Endocrinol. 2019 Sep;7(9):e21. PMID:31189520. [DOI] [PubMed] [Google Scholar]
- 20.Pratley R, Amod A, Hoff ST, Kadowaki T, Lingvay I, Nauck M, et al. Oral semaglutide versus subcutaneous liraglutide and placebo in type 2 diabetes (PIONEER 4):A randomised, double-blind, phase 3a trial [published correction appears in Lancet 2019;394:e1] Lancet. 2019;394:39–50. doi: 10.1016/S0140-6736(19)31271-1. [DOI] [PubMed] [Google Scholar]
- 21.Zinman B, Aroda VR, Buse JB, Cariou B, Harris SB, Hoff ST, et al. Efficacy, safety, and tolerability of oral semaglutide versus placebo added to insulin with or without metformin in patients with type 2 diabetes:The PIONEER 8 trial. Diabetes Care. 2019;42:2262–71. doi: 10.2337/dc19-0898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mosenzon O, Blicher TM, Rosenlund S, Eriksson JW, Heller S, Hels OH, et al. Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5):A placebo-controlled, randomised, phase 3a trial [published correction appears in Lancet Diabetes Endocrinol 2019;7:e21] Lancet Diabetes Endocrinol. 2019;7:515–27. doi: 10.1016/S2213-8587(19)30192-5. [DOI] [PubMed] [Google Scholar]
- 23.Meier J, Bauer R, Blicher TM, Lingvay I, Treppendah M, Zinman B, et al. Abstract #51. OP 09. EASD 55th Annual Meeting. Sept 17, 2019 [Google Scholar]
- 24. [Last accessed on 2021 Dec 28]. Available from:https://www.easd.org/virtualmeeting/home.html#!resources/4ea9eeb7-096f-4c7c-9fd7-59c19faa083b .
- 25.Garber AJ, Handelsman Y, Grunberger G, Einhorn D, Abrahamson MJ, Barzilay JI, et al. Consensus statement by the American association of clinical endocrinologists and American college of endocrinology on the comprehensive type 2 diabetes management algorithm –2020 executive summary. Endocr Pract. 2020;26:107–39. doi: 10.4158/CS-2019-0472. [DOI] [PubMed] [Google Scholar]
- 26.American Diabetes Association. 9. Pharmacologic approaches to glycemic treatment:Standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S125–43. doi: 10.2337/dc20-S009. [DOI] [PubMed] [Google Scholar]
- 27.Aroda V, Bauer R, Davies AL. Incorporating treatment pauses, dosing flexibility, and education to support GLP-1RA therapy persistence. [Last accessed on 2022 Feb 27];Poster presented at:81st Scientific Sessions of the American Diabetes Association, June 25 -29, 2021 [Google Scholar]
- 28.Husain M, Birkenfeld AL, Donsmark M, Dungan K, Eliaschewitz FG, Franco DR, et al. Oral semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2019;381:841–51. doi: 10.1056/NEJMoa1901118. [DOI] [PubMed] [Google Scholar]
- 29.Marso SP, Bain SC, Consoli A, Eliaschewitz FG, Jódar E, Leiter LA, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375:1834–44. doi: 10.1056/NEJMoa1607141. [DOI] [PubMed] [Google Scholar]
- 30.Oral semaglutide, US Prescribing information. [Last accessed on 2021 Dec 29]. Available from:https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/213051s000lbl.pdf .
- 31. [Last accessed on 2021 Dec 29];Oral semaglutide, Indian Prescribing information. [Google Scholar]
- 32.Brunton SA, Mosenzon O, Wright EE., Jr Integrating oral semaglutide into clinical practice in primary care:For whom, when, and how? Postgrad Med. 2020;132(Suppl 2):48–60. doi: 10.1080/00325481.2020.1798162. [DOI] [PubMed] [Google Scholar]
- 33.Seidu S, Mellbin L, Kaiser M, Khunti K. Will oral semaglutide be a game-changer in the management of type 2 diabetes in primary care? Prim Care Diabetes. 2021;15:59–68. doi: 10.1016/j.pcd.2020.07.011. [DOI] [PubMed] [Google Scholar]
- 34.Kalra S, Das AK, Sahay RK, Baruah MP, Tiwaskar M, Das S, et al. Consensus recommendations on GLP-1 RA use in the management of type 2 diabetes mellitus:South Asian task force. Diabetes Ther. 2019;10:1645–717. doi: 10.1007/s13300-019-0669-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bækdal TA, Borregaard J, Hansen CW, Thomsen M, Anderson TW. Effect of oral semaglutide on the pharmacokinetics of lisinopril, warfarin, digoxin, and metformin in healthy subjects. Clin Pharmacokinet. 2019;58:1193–203. doi: 10.1007/s40262-019-00756-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Baekdal T, Skibsted S, Manigandan E, Anderson TW, Albayaty M. Poster 714. EASD 54th Annual Meeting. 1-5 October, 2018 [Google Scholar]
- 37.Hauge C, Breitschaft A, Hartoft-Nielsen ML, Jensen S, Bækdal T. Poster SAT-140. ENDO 101st Annual Meeting and Expo. 23–26 March, 2019;4 [Google Scholar]
- 38.Jordy AB, Houshmand-Øregaard A, Hansen C, Granhall C, Christiansen E, Breitschaft A, et al. Poster 713. EASD 54th Annual Meeting. 1–5 October, 2018 [Google Scholar]
- 39.PIONEER PLUS. [Last accessed on 2022 Feb 26]. Available from:https://www.clinicaltrials.gov/ct2/show/NCT04707469 .
- 40.PIONEER TEEN. [Last accessed on 2022 Feb 26]. Available from:https://clinicaltrials.gov/ct2/show/NCT04596631 .
- 41.PIONEER REAL. [Last accessed on 2022 Feb 26]. Available from:https://clinicaltrials.gov/ct2/show/NCT04537637 .
- 42.EVOKE. [Last accessed on 2022 Feb 26]. Available from:https://clinicaltrials.gov/ct2/show/NCT04777396 .