

Abstract
The present study aims to describe accelerometer‐assessed physical activity (PA) patterns and fulfillment of PA recommendations in a large sample of middle‐aged men and women, and to study differences between subgroups of socio‐demographic, socio‐economic, and lifestyle‐related variables. A total of 27 890 (92.5% of total participants, 52% women, aged 50–64 years) middle‐aged men and women with at least four days of valid hip‐worn accelerometer data (Actigraph GT3X+, wGT3X+ and wGT3X‐BT) from the Swedish CArdioPulmonary bioImage Study, SCAPIS, were included. In total, 54.5% of daily wear time was spent sedentary, 39.1% in low, 5.4% in moderate, and only 0.1% in vigorous PA. Male sex, higher education, low financial strain, born in Sweden, and sedentary/light working situation were related to higher sedentary time, but also higher levels of vigorous PA. High BMI and having multiple chronic diseases associated strongly with higher sedentary time and less time in all three PA intensities. All‐year physically active commuters had an overall more active PA pattern. The proportion fulfilling current PA recommendations varied substantially (1.4% to 92.2%) depending on data handling procedures and definition used. Twenty‐eight percent was defined as having an “at‐risk” behavior, which included both high sedentary time and low vigorous PA. In this large population‐based sample, a majority of time was spent sedentary and only a fraction in vigorous PA, with clinically important variations between subgroups. This study provides important reference material and emphasizes the importance of a comprehensive assessment of all aspects of the individual PA pattern in future research and clinical practice.
Keywords: accelerometery, pattern, physical Activity, population‐based, SCAPIS Study, sedentary
1. INTRODUCTION
In November 2020, WHO updated the current global recommendations on physical activity (PA) and sedentary behavior for health, 1 which largely rely on studies using self‐report. However, self‐report is associated with lower predictive validity, 2 , 3 a common overestimation of PA and underestimation of sedentary time when compared with sensor‐based methods (mainly accelerometery). 4 This has been reinforced in studies showing large differences in the proportion of a population fulfilling the criteria for PA recommendations when evaluated by self‐report. 5 Self‐report may also mask possible differences within a population due to variation in interpretation of the questions used and show weaker associations to morbidity and mortality, compared with accelerometer‐assessed PA. 2 , 3
At the same time as the new WHO recommendations were launched, the first harmonized meta‐analysis on the joint association of sensor‐based sedentary time and moderate‐to‐vigorous PA (MVPA) on all‐cause mortality risk was presented, 6 emphasizing the concept of evaluating both these behaviors in conjunction for a more correct interpretation of risk. In combination with other research showing the independent important contribution of several aspects of the daily PA pattern for metabolic status and chronic disease risk, 7 , 8 it is highly relevant to in a high‐resolution and valid way describe the PA pattern and its variation within the general population as well as in clinically relevant subgroups.
Accelerometery has during the last decades increasingly been used in population‐based studies, and a rising number of papers have presented data on population PA levels using hip‐ or wrist‐worn accelerometers. 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 However, many of these studies comprise smaller samples sizes with less power for multiple sub‐group analyses 10 , 11 , 12 , 14 , 17 or do not report all aspects constituting the daily PA pattern (time in sedentary, low‐ moderate‐ and vigorous‐intensity PA). 9 , 15 , 16 Also, although the fast‐developing accelerometery methodology of today is recording movement using three axes, tri‐axial accelerometer data on population level is limited 9 , 18 and comparisons with uni‐axial accelerometer data is scarce. 18
In the present study, we used hip‐worn accelerometery data from the Swedish CArdioPulmonary bioImage Study (SCAPIS) to a) to describe accelerometer‐assessed PA patterns and fulfillment of PA recommendations in a large sample of middle‐aged men and women; and b) to study potential differences between subgroups of socio‐demographics, socioeconomics, and lifestyle‐related variables. We hypothesized that participants would spend most of their time in sedentary, with a stepwise lower proportion of daily time spent in PA with higher intensities. Further, we hypothesized that the PA pattern would vary between the defined subgroups, and that fulfillment of PA recommendations would be generally low.
2. MATERIAL AND METHODS
SCAPIS is a large Swedish cohort of randomly selected participants from the general population in six regions in Sweden. The overarching aim was to characterize participants with respect to cardiopulmonary and metabolic health. 19 The SCAPIS data collection was carried out between 2013 and 2018 as a multicenter study at Swedish university hospitals; Gothenburg, Malmö/Lund (south/west of Sweden), Linköping, Stockholm, Uppsala (lower middle/east of Sweden), and Umeå (north of Sweden). Each site aimed to recruit 5000 individuals from the respective municipality areas. Recruitment was performed as sex and age (50–54, 55–59, and 60–64 years) stratified random selection in the municipality areas. The participants visited the test site on two to three occasions within a 2‐week period, depending on local logistic arrangement. During the first visit, the participant filled in an extensive questionnaire on lifestyle and living conditions and wore an accelerometer for seven days to monitor the daily PA pattern.
The study was approved by the ethics board at Umeå and Gothenburg University, respectively (Dnr 2016–511–31 M and 638–16), and it adhered to the Declaration of Helsinki. All participants provided written informed consent prior to data collection. The SCAPIS study and design has previously been described by Bergstrom et al. 19
2.1. Assessment of physical activity patterns
Sensor‐based sedentary behavior and PA patterns were derived from tri‐axial accelerometers, ActiGraph model GT3X+, wGT3X+ and wGT3X‐BT (3%, 15% and 82% of participants, respectively), ActiGraph LCC, Pensacola, FL, USA). The participants wore the accelerometers for seven days. Participants were instructed to wear the accelerometer in an elastic belt over the right hip during all waking hours, except during water‐based activities, and to return after the wearing period. ActiLife v.6.13.3 software was used to initialize the accelerometers and to download and process the collected data. The accelerometer recorded raw data (sample rate set to 30 Hz) from three axes. As data analyzing methods are rapidly evolving, different suggested data handling procedures and raw accelerometer analyses are available. 20 , 21 However, as there is no consensus of best practice for analyzing accelerometer data available yet, we chose to use the data handling procedures and cut‐offs used in most previous papers to enable comparisons with previous research (see below). Hence, raw accelerometer data were combined into a resulting vector, extracted as 60‐second epochs using a low‐frequency extension filter, and expressed in counts per minute (cpm). Non‐wear time was defined as 60 or more consecutive minutes with no movement (0 cpm), with allowance for maximum 2 min of counts between 0 and 199 cpm. Wear time was calculated as 24 hours minus non‐wear time. Participants with a minimum of 600 min of valid daily wear time for at least 4 days were included. 22
Total PA was expressed in daily mean tri‐axial vector magnitude cpm. Sedentary time was defined as <200 cpm, 23 low intensity PA (LIPA) as 200–2689 cpm, moderate intensity PA (MPA) as 2690–6166 cpm, and vigorous PA (VPA) as ≥6167 cpm. 24 A prolonged sedentary bout was defined as ≥20 min of cpm below 200 (definition based on previous experimental data 25 ), with no allowance for interruption above threshold. As daily wear time varied between study participants above the minimum of 600 min per day, the PA pattern is presented as both average minute per day and percentage of wear time spent in different intensity‐specific categories. The percentage of the study population meeting different defined PA recommendations was also analyzed. Recently, updated WHO guidelines recommend that adults (18–64 years) should engage in at least 150–300 min of MPA, or at least 75–150 min of VPA, or an equivalent combination of MPA and VPA, throughout the week. 1 To elucidate the variation in proportion meeting with the recommendations between strata, we assessed the prevalence of participants meeting six different criteria; 150 (lowest achievable criterion) and 300 (highest achievable criterion) minutes of MPA per week, 75 (lowest achievable criterion) and 150 (highest achievable criterion) minutes of VPA per week, as well as a combination of MPA and VPA of 150 and 300 min. For participants with less than 7 days of valid data, a daily average of at least 10.7, 21.4, and 42.8 min per day was used for the thresholds 75, 150, and 300 min per week, respectively.
Two sensitivity analyses were performed. In the first, we analyzed data extracted as 5‐second epochs, keeping all other procedures identical to the 60‐second epochs analyses described above. In the second, we aimed to compare our data with previous research presenting fulfillment of national guidelines in general population samples. However, previous papers have mainly used uni‐axial data for this purpose. As large discrepancy in cpm generated by uni‐axial and tri‐axial data exist, as well as in cut‐offs used to define MPA and VPA, we re‐analyzed the present data using uni‐axial accelerometer recordings according to the same proceeding as presented above. Uni‐axial MPA was defined as cpm ≥2020 and VPA as ≥5999, in accordance with previous surveys. 16
Joint analyses based on tri‐axial data, including low or medium vs. high sedentary time and time in VPA and MPA, respectively, were performed. Time in VPA and MPA was categorized according to the levels from WHOs guidelines for PA (low VPA <75 min/week and low MPA<150 min/week). 1 As no limit for sedentary time is specified in the guidelines, we defined high daily sedentary time as 9.5 h/day, which has been associated with an increased risk for all‐cause mortality. 26 As wear time varied between participants, mainly affecting time in sedentary (see Additional file 1), we translated the 9.5 h/day into percentage of hypothetical 16 hours of awaking time (9.5 h/16.0 h = 59.4%), which was used as the cut‐off for high sedentary time. Furthermore, in this study, we defined a potential “at‐risk” joint behavior of sedentary and VPA, as well as sedentary and MPA, to be highly sedentary (>9.5 h/day) and low VPA (<75 min/week) or low MPA (<150 min/week), respectively. A “low‐risk” behavior was identified as either high sedentary but high VPA or MPA, or low to medium sedentary and medium to high VPA or MPA. 27
2.2. Other measurements
Measurements of body mass and height were assessed during the first visit to the test center, and body mass index (BMI) was calculated. Highest educational attainment, employment status, financial strain, civil status, country of birth, smoking habits, commuting habits, and physical working situation were all self‐reported (see questions in Additional file 2) and grouped as described in Figures 2A and 2B. Prevalent chronic condition was defined as reporting none, one, two, or three of the following; diagnosed disease or surgical treatment for cardiovascular disease (myocardial infarction, angina pectoris, stroke, congestive heart failure, and atrial fibrillation), lung disease, and/or rheumatic disease.
FIGURE 1.
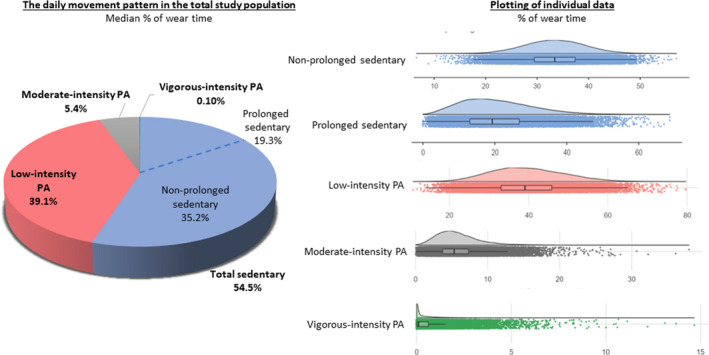
Distribution of time spent in sedentary and in physical activity of different intensities presented as percent of median wear time (pie chart, left) and by plotting individual data (density plots with individual data and boxplot, right)
FIGURE 2.
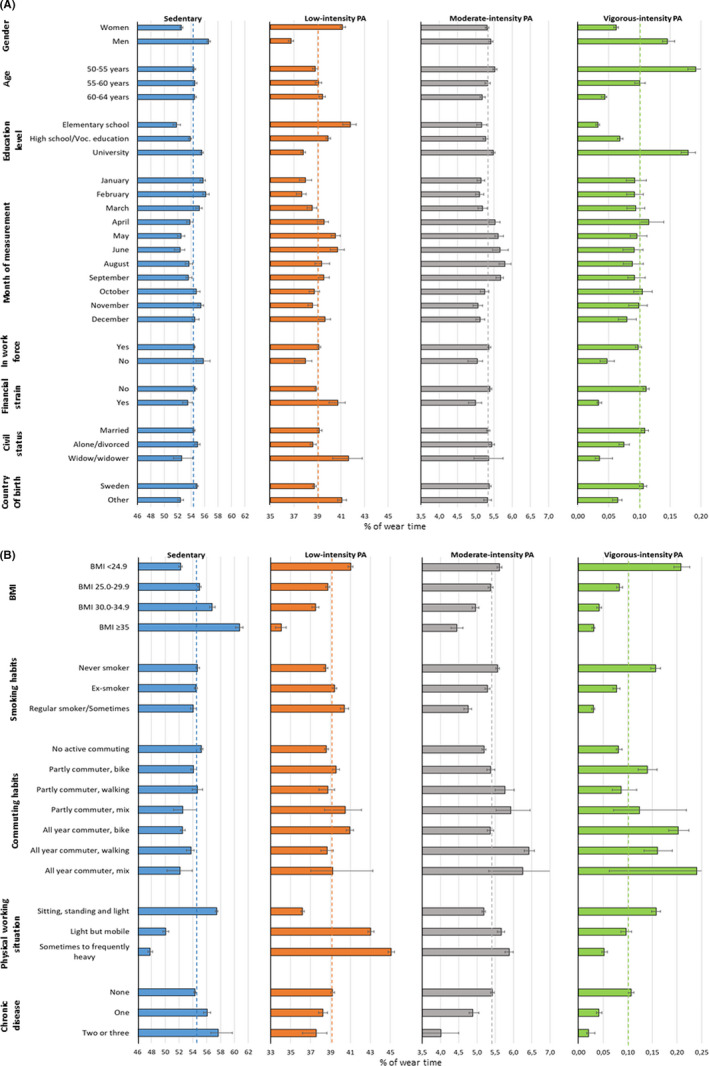
(A) Median total physical activity and percent of median wear time for time spent in sedentary and in physical activity of different intensities, with 95% CI, in relation to gender, age, month, and socio‐demographics. Dashed line indicates the median for the total population. (B) Median total physical activity and percent of median wear time for time spent in sedentary and in physical activity of different intensities, with 95% CI, in relation to BMI, smoking, commuting habits, physical working situation, and number of chronic diseases. Dashed line indicates the median for the total population
2.3. Representativeness analysis of included data
To compare the cohort of men and women included from SCAPIS with general Swedish population, we retrieved public available data for the years 2013–2018 on BMI, educational level, and country of birth from Statistics Sweden (www.scb.se) and on smoking habits from the Public Health Agency of Sweden (https://www.folkhalsomyndigheten.se/). Included and excluded participants from the SCAPIS cohort were compared for central variables (Additional file 3).
2.4. Statistical analysis
Data were checked for normality using the Kolmogorov–Smirnov Test, and as most variables were skewed, descriptive data are presented as medians with 95% confidence intervals (CIs). To compare median cpm, minutes per day or median percentage of wear time in sedentary or PA of different intensities between subgroups, we used Mann–Whitney U‐test or Kruskal Wallis ANOVA and chi‐squared test, with p‐values adjusted for multiple testing (Benjamini‐Hochberg and Dwass‐Steel‐Critchlow‐Fligner). Odds ratios (ORs) with 95% CIs for "at‐risk" or "low‐risk" behavior for sedentary‐VPA or sedentary‐MPA were calculated using binary regression modelling adjusting for pre‐specified variables including sex, age, educational level, BMI, and smoking habits. Spearman rho correlation coefficients were interpreted as poor ≤0.2, fair 0.2 to 0.5, moderate >0.5 to 0.7, and strong as >0.7. Statistical analyses were performed by using SPSS (Statistical Package for the Social Sciences for Windows, 26.0.0.1, 2019, SPSS Inc., Chicago IL) and Jamovi (The jamovi project (2021) Version 1.6. Retrieved from https://www.jamovi.org/.
3. RESULTS
3.1. Study cohort
In total, 59 909 men and women were invited to the SCAPIS study, of which 30 154 (50.3%) participated. Of these, a total of 27 890 (92.5%) provided at least four days of valid accelerometer data (defined as ≥600 min of wear time) and were included in the present analyses. The majority, 66%, of the included participants had valid data for at least 7 days, and a further 21% for 6 days, 9% for 5 days, and 4% for 4 days. Of those excluded, n = 908 did not provide any accelerometer data and n=1356 participants had less than 4 days of valid data (Additional file 3). SCAPIS participants excluded were more often men, had higher BMI, were less likely to have a university degree, more likely to be smokers, and more likely to have at least one chronic disease.
The study population consisted of 14 537 women and 13 353 men, with a median age of 57.4 years. The majority of both women and men were in the work force, born in Sweden, were married or cohabitant and had no previous chronic condition (Table 1). Approximately half of the participants had a university degree, and few were under financial strain. Fifty‐six % of women and 72% of men were overweight or obese (BMI≥25.0), and every second individual was a never‐smoker. Compared with data from men and women of the same ages in the general Swedish population, significant but small differences were seen for BMI (SCAPIS cohort slightly more overweight/obese), educational level (a higher proportion with university degree in the SCAPIS cohort), and proportion born in Sweden (higher in the SCAPIS cohort), while the proportion of never‐smokers was significantly lower in the SCAPIS cohort.
TABLE 1.
Characteristics of the study population and comparison with general population data
| SCAPIS sample | General population | |||
|---|---|---|---|---|
| Women | Men | Women | Men | |
| n = 14 537 | n = 13 353 | |||
| Age (years) | 57.4 (53.7; 61.2) | 57.5 (53.7; 61.3) | ||
| Study site | ||||
| Gothenburg | 21% | 20% | ||
| Malmö | 21% | 19% | ||
| Stockholm | 16% | 17% | ||
| Linköping | 17% | 18% | ||
| Uppsala | 17% | 17% | ||
| Umeå | 8% | 8% | ||
| Number of valid accelerometer days | ||||
| 4 | 4% | 5% | ||
| 5 | 8% | 11% | ||
| 6 | 20% | 21% | ||
| 7 | 68% | 63% | ||
| In work force | 97% | 96% | ||
| Financial strain e | 8% | 6% | ||
| Married/cohabitant | 70% | 79% | ||
| Number of chronic diseases a | ||||
| None | 90% | 88% | ||
| One | 10% | 12% | ||
| Two or three | 1% | 1% | ||
| Waist (cm) | 88 (80; 97) | 99 (92; 106) | ||
| BMI (kg/m2) b | 25.6 (23.0; 29.0) | 26.8 (24.7; 29.4) | ||
| 1. BMI <24.9 | 45% | 28% | 50% c | 32% c |
| 2. BMI 25.0–29.9 | 36% | 51% | 35% c | 50% c |
| 4. BMI ≥30 | 20% | 21% | 15% c | 18% c |
| University degree | 49% | 41% | 48% c | 39% c |
| Born in Sweden | 84% | 85% | 81% c | 82% c |
| Never‐smokers | 47% | 52% | 56% c , d | 60% c , d |
Data are presented as median (Q1; Q3) or percentages.
Of either cardiovascular, lung, or rheumatic disease.
Weight and height for BMI calculation were self‐reported in general population data.
Significantly different from the SCAPIS sample, defined as general population proportion was not included in the 95% CI for the SCAPIS sample proportion.
General population data for age‐group 45–64 years.
Financial stain is defined as answering "No" to the question "If you were to suddenly end up in a situation where you had to raise SEK 20 000 (≈EURO 2000) in one week, would you be able to do it?"
3.2. Physical activity patterns
In the cohort, median cpm was 653 (Q1; 529 cpm to Q3; 791 cpm). A total of 54.5% (Q1; 47.0% to Q3; 61.2%) of wear time (median time 7 h and 54 min) were spent sedentary, of which 19.3% (13.1% to 26.8%) were spent in prolonged sedentary bouts. Moreover, 39.1% (33.0% to 45.9%; 5 h and 48 min) were spent in LIPA, 5.4% (3.7% to 7.4%; 48 min) in MPA and only 0.1% (0.02% to 0.62%; 1 min) in VPA, with a large inter‐individual variation (Figure 1, Additional file 4 and 5). Total PA was strongly correlated with time spent sedentary and in moderate intensity PA (Additional file 1). Moreover, there were poor to moderate correlations between the different components of the PA pattern, with time spent sedentary having a moderate correlation with wear time and a low correlation with time spent in VPA.
In the sensitivity analyses using data in 5‐second epoch length, median cpm was 639 (515 to 779 cpm). A total of 67.3% (61.4% to 72.6%) of wear time (median time 9 h and 50 min) were spent sedentary, of which 6.1% (3.4% to 10.3%) were spent in prolonged sedentary bouts. Moreover, 22.6% (18.7% to 26.9%) were spent in LIPA (3 h and 24 min), 8.8% (6.9% to 11.1%) (1 h and 20 min min) in MPA, and only 0.6% (0.3% to 1.2%) (5 min) in VPA. The variation with sex, age‐group, and educational level was similar as for 60‐second epoch analyses (Additional file 6).
Figures 2A and 2B describes the variation in median total PA as well as % of wear time for each component of the daily movement pattern, in different subgroups and in relation to the percent of median for the total population (dashed lines). Total PA largely demonstrated the opposite pattern compared with that of sedentary, and similar pattern to that of MPA. Men, higher educational level, low financial strain, being born in Sweden, and with mainly sitting/standing/light physical working situation showed similar profiles, which included higher time spent sedentary, less time in LIPA but more in VPA. The median time spent in VPA was very low, but with large variation between subgroups. Overweight/obese participants or those with one or more chronic diseases spend higher time in sedentary and less time in all PA intensities compared with lean and participants without the specified chronic conditions. There were small differences in sedentary time between age‐groups or smoking habits, however, with more time spent in MPA and VPA in younger and never‐ smokers. There were low variations in MPA and VPA over the year, however, with more time spent sedentary between October and March. All‐year commuters (bike or walking) had a more beneficial PA pattern compared with passive commuters, with less time in sedentary and more in PA.
3.3. Fulfillment of national recommendations
The proportion of participants that met current national PA recommendations varied greatly, depending on how the recommendations were interpreted and whether uni‐ or tri‐axial data were used (Table 2). For example, using tri‐axial data and the lowest achievable criterion of a combination of MPA and VPA of 150 min/week yielded the highest fulfillment rate, 92.2%. Using uni‐axial data and the strictest criterion of 150 min/week of VPA resulted in the lowest fulfillment rate, 1.4%. In general, men, younger age‐group, higher educational level, and participants from the Stockholm SCAPIS‐test site had the highest rate of fulfillment of PA recommendations.
TABLE 2.
Proportion of the study population meeting current national recommendations regarding moderate‐ and vigorous‐intense physical activity
| 150 weekly MPA | 300 weekly MPA | 75 min weekly VPA | 150 weekly VPA | MPA+VPA 150 weekly | MPA+VPA 300 weekly | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Uni‐axial | Tri‐axial | Uni‐axial | Tri‐axial | Uni‐axial | Tri‐axial | Uni‐axial | Tri‐axial | Uni‐axial | Tri‐axial | Uni‐axial | Tri‐axial | |
| % | % | % | % | % | % | % | % | % | % | % | % | |
| Total | 73.9 | 91.4 | 33.2 | 58.1 | 4.9 | 14.0 | 1.4 | 4.9 | 75.8 | 92.2 | 39.0 | 64.0 |
| Sex | ||||||||||||
| 1. Men | 75.3 b | 91.3 | 34.8 b | 58.7 b | 6.2 b | 16.7 b | 1.9 b | 6.1 b | 77.5 b | 92.4 | 41.6 b | 65.7 b |
| 2. Women | 72.6 | 91.4 | 31.7 | 57.5 | 3.6 | 11.5 | 0.9 | 3.7 | 74.1 | 92.0 | 36.6 | 62.4 |
| Age‐groups | ||||||||||||
| 1. 50–55 years | 76.8 a | 93.8 a | 35.1 a | 61.5 a | 7.0 a | 18.5 a | 1.9 a | 6.5 a | 79.2 a | 94.7 a | 42.8 a | 68.8 a |
| 2. 56–60 years | 74.0 | 91.7 | 33.3 | 58.1 | 4.7 | 14.2 | 1.4 | 4.9 | 75.7 | 92.5 | 39.1 | 64.2 |
| 3. 61–65 years | 70.9 | 88.5 | 31.2 | 54.7 | 2.8 | 9.3 | 0.8 | 3.2 | 72.2 | 89.3 | 35.0 | 58.8 |
| Educational attainment | ||||||||||||
| 1. University degree | 79.6 a | 93.6 a | 37.1 a | 61.1 a | 6.2 a | 17.0 a | 1.7 a | 6.0 a | 81.7 a | 94.4 a | 44.4 a | 68.5 a |
| 2. High school/ Vocational education | 70.9 | 90.3 | 31.1 | 56.2 | 4.1 | 12.5 | 1.3 | 4.2 | 72.6 | 91.2 | 36.1 | 61.3 |
| 3. Elementary school | 62.6 | 86.6 | 25.9 | 53.4 | 2.3 | 7.7 | 0.7 | 2.6 | 63.9 | 87.4 | 29.0 | 56.5 |
| SCAPIS study site | ||||||||||||
| 1. Göteborg | 78.2 b , c , d , e , f | 92.1 b , c , d , e | 35.0 b , c , d , e | 57.1 c , d , f | 5.3 b , c | 14.7 b , c , e | 1.4 b | 5.0 b , c | 79.9 b , c , d , e , f | 92.9 b , c , d , e | 41.3 b , c , d , e | 63.8 b , c , d , f |
| 2. Malmö | 60.8 c , d , e , f | 89.7 c , f | 22.7 c , d , e , f | 55.5 c , f | 2.8 c , d , e , f | 11.5 c , d , e , f | 0.5 c , d , e , f | 3.7 c , d , e , f | 63.2 c , d , e , f | 90.6 c , f | 26.9 c , d , e , f | 60.2 c , e , f |
| 3. Stockholm | 81.9 d , e , f | 93.9 d , e , f | 45.4 d , e , f | 67.2 d , e , f | 6.3 e , f | 17.4 d , e , f | 1.9 | 6.3 d , e , f | 83.3 d , e , f | 94.3 d , e , f | 51.7 d , e , f | 72.6 d , e , f |
| 4. Linköping | 74.1 e | 90.5 | 31.1 e , f | 53.6 e , f | 5.6 f | 13.6 | 1.9 | 4.9 | 76.2 | 91.6 | 38.0 f | 60.0 e , f |
| 5. Uppsala | 76.1 | 90.6 | 33.2 f | 56.2 f | 4.9 | 13.2 | 1.4 | 4.7 | 77.7 | 91.5 | 39.2 | 62.5 f |
| 6. Umeå | 75.9 | 91.9 | 35.7 | 62.4 | 4.3 | 14.4 | 1.3 | 4.8 | 77.2 | 92.4 | 40.7 | 67.7 |
VPA, vigorous‐intensity physical activity; MPA, moderate‐intensity physical activity
Significance testing for differences in proportions between subgroups using Benjamini–Hochberg adjustment for multiple testing.
all subgroups different
different vs subgroup 2
different vs subgroup 3
different vs subgroup 4
different vs subgroup 5
different vs subgroup 6
3.4. Joint analyses of physical activity components using tri‐axial data
In the joint association analyses, 28% of the population had an “at‐risk” behavior with high time spent sedentary in combination with low time in VPA (red bar to the left in Figure 3). Moreover, 5.7% were identified to have an “at‐risk” behavior with high time spent sedentary and low time in MPA (red bar to the right in Figure 3). Conversely, a “low‐risk” behavior was identified in 11.3% of the participants for joint sedentary‐VPA analyses (green bars to the left in Figure 3). For joint analyses of sedentary and MPA, 76.6% were identified to have a “low‐risk” behavior (green bars to the right in Figure 3). Men, higher age, overweight/obese, and regular smokers were more likely to have both an at‐risk joint sedentary‐VPA and sedentary‐MPA behavior (Table 3). Higher age, overweight/obese, and regular smokers were also all less likely to have a low‐risk joint sedentary‐VPA and sedentary‐MPA behavior.
FIGURE 3.
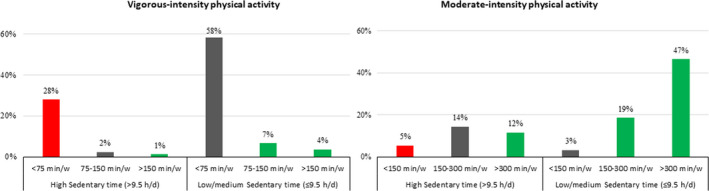
Joint association between time in sedentary time, VPA and MPA, in the total population, with red bars denoting “at‐risk” behaviors and green bars denoting “low‐risk”‐behaviors. Y‐axis represent % of total population
TABLE 3.
Odds ratios (95% CI) for “at‐risk” and “low‐risk” behaviors of sedentary time, and VPA and MPA, respectively, in relation to sex, age‐group, educational level, BMI, and smoking
| ”At‐risk” sedentary‐VPA | ”Low‐risk” sedentary‐VPA | “At‐risk” sedentary‐MPA | ”Low‐risk” sedentary‐MPA | |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Women | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Men | 1.78 (1.68–1.88) | 1.54 (1.42–1.66) | 1.36 (1.22–1.52) | 0.69 (0.65–0.73) |
| 50–55 years | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| 56–60 years | 1.15 (1.07–1.23) | 0.76 (0.70–0.83) | 1.33 (1.15–1.53) | 0.86 (0.80–0.92) |
| 61–65 years | 1.23 (1.15–1.32) | 0.48 (0.44–0.53) | 1.89 (1.65–2.17) | 0.77 (0.72–0.83) |
| Elementary school | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| High school/Voc. education | 1.27 (1.14–1.41) | 1.42 (1.20–1.69) | 0.92 (0.78–1.09) | 0.91 (0.82–1.01) |
| University | 1.70 (1.53–1.89) | 1.69 (1.42–2.01) | 0.79 (0.66–0.94) | 0.87 (0.79–0.97) |
| BMI <24.9 kg/m2 | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| BMI 25.0–29.9 kg/m2 | 1.56 (1.46–1.66) | 0.55 (0.51–0.60) | 1.38 (1.20–1.59) | 0.74 (0.69–0.80) |
| BMI 30.0–34.9 kg/m2 | 2.47 (2.28–2.68) | 0.31 (0.26–0.35) | 2.30 (1.96–2.70) | 0.50 (0.46–0.54) |
| BMI ≥35 kg/m2 | 5.21 (4.61–5.88) | 0.15 (0.11–0.21) | 4.40 (3.63–5.34) | 0.27 (0.24–0.31) |
| Never smoker | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) |
| Ex‐smoker | 1.00 (0.94–1.06) | 0.95 (0.88–1.03) | 1.22 (1.08–1.38) | 0.94 (0.88–1.00) |
| Regular smoker/Sometimes | 1.19 (1.09–1.30) | 0.49 (0.42–0.57) | 2.36 (2.04–2.74) | 0.65 (0.59–0.71) |
All odds ratios adjusted for the other variables in the table. MPA; moderate‐intensity physical activity, VPA; vigorous‐intensity physical activity, BMI; body mass index
“At‐risk” behaviors equal high sedentary (>9.5 h/day) and low VPA (<75 min/week) or low MPA (<150 min/week). “Low‐risk” behaviors equal either high sedentary (>9.5 h/day) but simultaneous high VPA (≥150 min/week) or high MPA (≥300 min/week), or low to medium sedentary (≤9.5 h/day) and medium to high VPA (≥75 min/week) or MPA (≥150 min/week).
The analyses are based on tri‐axial data.
4. DISCUSSION
The main findings of the present study were that 54.5% of daily wear time was spent sedentary and as little as 0.1% was spent in VPA in a large population‐based sample of over 27 890 middle‐aged men and women. PA patterns varied between subgroups and with season. Male sex, higher educational level, low financial strain, being born in Sweden, and having a working situation with light physical demands were related to higher time spent sedentary, but also more time spent in vigorous PA. Higher BMI and number of chronic diseases had strong associations with higher sedentary time and less time in all PA intensities. A novel finding was that all‐year active commuters had an overall more beneficial PA pattern. Fulfillment of national PA recommendations varied substantially depending on the definition used and on whether uni‐ or tri‐axial data were analyzed. In the total study population, 5% and 28% were identified as having an “at‐risk” behavior including both high sedentary time and low time in MPA and VPA, respectively.
4.1. High levels of sedentary, almost no VPA
The present results are in concordance with previous research reporting that the majority of accelerometer wear time is spent being sedentary. 10 , 11 , 13 , 14 , 16 , 17 , 28 However, we report very low fraction of time spent in VPA, which is more rarely reported 14 , 16 as most studies present time in MVPA without distinction between MPA and VPA. Interestingly, we found low levels of VPA both using data requiring longer registration periods of VPA (60‐second epoch data, median time in VPA 1 min) or enabling shorter bouts of VPA to be registered (5‐second epoch data, median time in VPA 5 min). To capture time in VPA separately may have clinical importance. For example, VPA is for most individuals the main contributor for maintaining or increasing cardiorespiratory fitness, which in turn is an independent predictor for morbidity and mortality as well as daily function, 29 but has been reported to decline in the general population during the last decades. 30 , 31 In a recent randomized controlled trial with mortality as outcome, only the intervention arm with two added weekly sessions of high‐intensity training for 5 years (4 × 4 min per session) induced a lower all‐cause mortality risk in older adults (70–77 years at baseline). 32 In the present study, 22% of the participants had no VPA at all during wear time, and median time spent in VPA was 6 min/week (60‐second epoch length‐analyses). In the light of the WHO recommendation of 75 to 150 min/week, this figure is extremely low and indicates that VPA only marginally contributes to fulfillment of PA recommendations in the population. Importantly though, in clinical practice, we also have to consider potential side‐effects, where the potentially higher yield of high‐intensity activity is balanced to possible complications, due to the higher event‐risk of high‐intensity activity in patients with underlying cardiovascular disease. 33 Thus, the risk analysis is a part of any risk stratification, before starting a high‐intensity activity or sports. 34
4.2. Variations of PA within subgroups
The variations in PA patterns between subgroups confirm, but also expand, on previous study results. For example, we now confirm using tri‐axial accelerometer that men, lower educational level, unemployed, overweight or obese, with sedentary occupations, and those with chronic disease tend to spend more time being sedentary and corresponding less time in LIPA. 13 , 17 , 35 , 36 , 37 We also confirm that men, higher educational level, normal weight, and those without chronic disease spend more time in MVPA, 13 , 14 , 17 , 35 and that there is a variation over the year with more PA and less sitting during summer compared with winter season. 38 However, some new important aspects should be highlighted. Firstly, the distinction between MPA and VPA indicates that frequently reported differences in MVPA between sex, age‐groups, and educational level (more MVPA in men, younger age‐groups, and higher educational level) may largely be explained by variation in VPA rather than MPA (Figure 2A). Also, aggregation of VPA and MPA into MVPA masks the opposite trend of MPA and VPA between participants with a different physical working situation (Figure 2B). This may indicate that participants with heavy/strenuous occupation tasks are accumulating the higher MPA levels at work, while participants with light work tasks are accumulating their higher VPA levels in leisure time. This finding is highly interesting in relation to the ongoing debate of the PA paradox of different health effects by occupational and leisure time PA. 39 , 40
Further, the more beneficial PA profile for all‐year active commuters is important and has, to the best of our knowledge, not been reported before. All‐year commuters using bike or walking spent less time in sedentary, and more time in moderate and/or vigorous PA compared with passive commuters and partly commuters. It is also worth noticing the inability of hip‐worn accelerometers to correctly capture cycling activity and intensity, possibly underestimating the actual activity in bike commuters. Active commuters have previously been reported to have higher cardiorespiratory fitness, higher self‐reported exercise levels, and lower risk for cardiovascular disease, compared to passive commuters. 41 Active commuting provides an easily accessible and time‐efficient possibility to increase PA and health in the general population, but more studies are needed to confirm the effect on the full PA pattern.
4.3. Joint sedentary and PA analyses
In the light of recent research on morbidity and mortality risks with different joint PA behaviors, 6 , 7 , 27 our findings of 28% of participants in the study having a joint “at‐risk” behavior with both high sedentary time and low VPA, and only 12% having a “low‐risk” behavior, are important. Corresponding values for MPA were 5% for “at‐risk” behavior and 78% for “low‐risk” behavior. In a recent paper, Chastin et al elaborated on the balance of sedentary time and time spent in different intensities of PA on all‐cause mortality, 42 and concluded that ≥2.5 min of MVPA per hour of daily sedentary time induced a similar magnitude of all‐cause mortality risk reduction, as obtained by being physically active according to the current recommendations. Similar elaborations with other outcomes (metabolic health and cardiovascular disease), and in different clinically relevant subgroups of the population, would provide interesting possibilities for interventions and recommendations to either increase time in MPA or VPA, or decrease time in sedentary, to achieve similar health benefits. This could be particularly important for subgroups with the highest disease risk, including obese individuals where a better prognosis for both morbidity and mortality in obese but active/fit patients has been shown. 43 In the present analyses, we observed an approximately 2.5 higher odds for a joint at‐risk behavior with obesity (BMI 30.0–34.9), and five‐fold higher odds for severe obesity (≥35.0), compared with normal weight, which indicate a likely coincident prevalence of inactivity/high sedentary and obesity/severe obesity in this large cohort.
4.4. Fulfillment of PA recommendations
Fulfillment rates varied considerably with data and definition used, so that using tri‐axial data and the lowest achievable criterion of a combination of 150 min/week of MPA and VPA yielded the highest fulfillment rate, 92.2%, while using uni‐axial data and the toughest criterion of 150 min/week of VPA resulted in the lowest fulfillment rate, 1.4%. The possibility for valid comparisons with previous reports are limited, as most studies have relied on the former WHO recommendations of 150 min of weekly MVPA, including only MVPA accumulated in bouts of 10 min. This has in general yielded much lower fulfillment rates, 3% to 25% in age‐matched samples 10 , 11 , 14 , 16 , 17 compared with the 76% in the present sample with ≥150 min/week of MVPA without the condition of 10‐min bouts. In two previous papers, fulfillment rates without the condition of 10‐min bouts were included, showing more comparable figures, 52% to 73%. 10 , 11 A paper analyzing fulfillment of 150 min of MVPA per week using both bout and non‐bout criteria, as well as uni‐ and tri‐axial accelerometer data, reported higher fulfillment when using tri‐axial data compared with uni‐axial, and non‐bout compared with 10‐min bout criteria. 18 Together with the present tri‐axial data and comparison with uni‐axial data, as well as fulfillment according to recently updated PA recommendations, we regard the present data from a large population‐based sample as a reference material for future studies rather than to confirm previously reported fulfillment rates.
4.5. Data handling considerations
Using accelerometery to study PA pattern and sedentary behavior provides a more valid measure than self‐report. 4 , 44 , 45 However, the results reported are still largely depending on choices made before data collection (such as accelerometer placement and sampling rate) and when analyzing collected data (such as data extraction and cut‐offs used), which should be considered when interpreting and comparing the data with previous studies. To shed light on some of the aspects during data handling, several sensitivity analyses were performed. Firstly, we studied the variance in PA pattern comparing raw data extracted into shorter (5‐second) and longer (60‐second) bouts. As expected from previous findings, more time was detected spent in sedentary (both prolonged and non‐prolonged) and MPA, and less in LIPA. 46 However, it was interesting that time spent in VPA was only slightly higher, median time 1 min vs 5 min, which strengthens the conclusion that VPA is only marginally contributing to guideline fulfillment. However, whether this may have clinical implications on different health outcomes has to be studied in more detail. It is likely that there are varying effects of epoch length across health outcomes. Secondly, we report large variations in fulfillment of PA recommendations depending on both the accelerometery data analyzed (uni‐ or tri‐axial) and definition used. Uni‐ and tri‐axial data are reported to have a strong, positive correlation, 47 which was also seen in the present data (r = 0.947, p < 0.001). Though, absolute cpm values from uni‐ and tri‐axial differ for the same PA performed (constantly lower for uni‐axial compared to tri‐axial data 47 ), but is not subsequently reflected in similar relative difference in cut‐offs used to define the recommended intensity (MVPA). This warrants a cautious comparison of tri‐axial data with, for example, uni‐axial derived thresholds for the estimation of morbidity or mortality risk. Recently, it was proposed that approximately 30 to 40 min of MVPA per day would attenuate the association between sedentary time and risk of death. 6 We are neither questioning the findings nor the threshold derived but want to highlight that using tri‐axial data to evaluate population fraction “at‐risk” according to this threshold is not feasible according to the above discussion. As for the GT3X‐monitor family, the removal of frequency filtering effects has been shown to increase relations to metabolic risk markers. 48 The use of un‐filtered data will most probably be more frequent in future studies. However, the impact on the proportion meeting PA recommendation is yet unknown, and should be investigated in a separate paper.
4.6. Strengths and limitations
The strengths of the present study include a representative sample of the randomly selected study population from six different geographical areas in Sweden, a low dropout rate and a high proportion of participants with valid accelerometer data. Moreover, accelerometers used to assess the PA pattern give a more valid estimate of actual daily movement patterns than self‐report methods do. The accelerometer data were collected throughout the year, removing systematic bias of season variability in PA and sedentary behavior; hence, we did not adjust for season in the analyses. Although participants were instructed to wear the accelerometer during awake time, overnight wear may be prevalent. We did not adjust for 24 h wear time, which may have influenced the proportion of time spent in sedentary (often more time) and PA of different intensities (often less time). Limitations with hip‐worn accelerometer include analyses of only sedentary behavior (and not sitting/standing/lying as separate behaviors), an underestimation of PA during cycling, 49 inability to detect load‐bearing, upper‐limb activities and water‐based activities. The joint analyses of different PA pattern are important, but the predictive validity has to be confirmed in association with different outcomes in future studies. Also, the possibility of actually being able to evaluate the fulfillment of the PA recommendation, which is based on self‐reported PA, using accelerometery is questionable. Caution must be applied when extrapolating the presented data to men and women outside the ages of the study participants.
5. PERSPECTIVES
In this large sample of middle‐aged men and women, we report that most of the awaking time is spent sedentary and only a fraction is spent in VPA, indicating that VPA is probably only marginally contributing to fulfillment of MVPA recommendations in this age‐group. Male sex, older age, obese, regular smokers, and those with one or more chronic diseases displayed a joint “at‐risk” behavior including high sedentary time and low MPA or VPA. The proportion of the study population fulfilling current PA recommendations varied substantially depending on data handling procedures and definition used. Regardless, the present study provides important references material and knowledge of the importance of a comprehensive assessment of all aspects of the individual PA pattern in middle‐aged, rather than just measuring total PA, which should be included in future research and clinical practice. The low engagement in VPA is of particular concern, especially as previous research has indicated a negative trend in cardiorespiratory fitness over the last decades in Sweden. 30 The great challenge remains to enhance the implementation of methods to increase the level of PA in middle‐aged adults, where the subgroups identified should be prioritized.
CONFLICT OF INTEREST
The author(s) declare(s) that they have no competing interests.
AUTHOR CONTRIBUTION
All authors contributed to the conception or design of the work. EEB, MB, ÖE, and GB contributed to the acquisition, analysis, or interpretation of data for the work. EEB, MB, and ÖE drafted the manuscript or substantively revised it. All authors revised it critically for important intellectual content. All authors critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The corresponding author, EEB, is the manuscripts guarantor and attests that all listed authors meet authorship criteria that no others meeting the criteria have been omitted and take the full responsibility for the overall content.
6. DATA AVAILABLITY STATEMENT
Due to the nature of the sensitive personal data and study materials, they cannot be made freely available. However, by contacting the corresponding author or study organization (www.scapis.org), procedures for sharing data, analytic methods, and study materials for reproducing the results or replicating the procedure can be arranged following Swedish legislation.
Supporting information
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Ekblom‐Bak E, Börjesson M, Bergman F, et al. Accelerometer derived physical activity patterns in 27.890 middle‐aged adults: The SCAPIS cohort study. Scand J Med Sci Sports. 2022;32:866–880. doi: 10.1111/sms.14131
Funding information
The main funding body of The Swedish CArdioPulmonary bioImage Study (SCAPIS) is the Swedish Heart‐Lung Foundation. The study is also funded by the Knut and Alice Wallenberg Foundation, the Swedish Research Council and VINNOVA (Sweden‘s Innovation agency) the University of Gothenburg and Sahlgrenska University Hospital, Karolinska Institutet and Stockholm county council, Linköping University and University Hospital, Lund University and Skåne University Hospital, Umeå University and University Hospital, Uppsala University and University Hospital. Author EEB and ÖE were funded by grants from Skandia Risk & Hälsa. MB is supported by ALF‐grants from Västra Götalandsregionen (ALFGBG‐720691) and a grant from the Heart and Lung foundation (no 20180379). The study sponsors had no role in; designing the study; the collection, analysis, or interpretation of data; writing the report; the decision to submit the article for publication. The researcher and their work have been independent from the funders and all authors, external, and internal, had full access to all of the data (including statistical reports and tables) in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis
REFERENCES
- 1. Bull FC, Al‐Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54(24):1451‐1462. doi: 10.1136/bjsports-2020-102955 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Chau JY, Grunseit AC, Chey T, et al. Daily sitting time and all‐cause mortality: a meta‐analysis. PLoS One. 2013;8(11):e80000. doi: 10.1371/journal.pone.0080000 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Ekelund U, Dalene KE, Tarp J, Lee IM. Physical activity and mortality: what is the dose response and how big is the effect? Br J Sports Med. 2020;54(19):1125‐1126. doi: 10.1136/bjsports-2019-101765 [DOI] [PubMed] [Google Scholar]
- 4. Ekblom O, Ekblom‐Bak E, Bolam KA, et al. Concurrent and predictive validity of physical activity measurement items commonly used in clinical settings‐‐data from SCAPIS pilot study. BMC Public Health. 2015;15(1):978. doi: 10.1186/s12889-015-2316-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Tucker JM, Welk GJ, Beyler NK. Physical activity in U.S.: Adults compliance with the Physical Activity Guidelines for Americans. Am J prev med. 2011;40(4):454‐461. doi: 10.1016/j.amepre.2010.12.016 [DOI] [PubMed] [Google Scholar]
- 6. Ekelund U, Tarp J, Fagerland MW, et al. Joint associations of accelero‐meter measured physical activity and sedentary time with all‐cause mortality: a harmonised meta‐analysis in more than 44 000 middle‐aged and older individuals. Br J Sports Med. 2020;54(24):1499‐1506. doi: 10.1136/bjsports-2020-103270 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Ekelund U, Brown WJ, Steene‐Johannessen J, et al. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta‐analysis of data from 850 060 participants. Br J Sports Med. 2019;53(14):886‐894. doi: 10.1136/bjsports-2017-098963 [DOI] [PubMed] [Google Scholar]
- 8. Ekblom‐Bak E, Ekblom O, Bergstrom G, Borjesson M. Isotemporal substitution of sedentary time by physical activity of different intensities and bout lengths, and its associations with metabolic risk. Eur J Prev Cardiol. 2016;23(9):967‐974. doi: 10.1177/2047487315619734 [DOI] [PubMed] [Google Scholar]
- 9. Doherty A, Jackson D, Hammerla N, et al. Large Scale Population Assessment of Physical Activity Using Wrist Worn Accelerometers: The UK Biobank Study. PLoS One. 2017;12(2):e0169649. doi: 10.1371/journal.pone.0169649 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ekblom‐Bak E, Olsson G, Ekblom O, Ekblom B, Bergstrom G, Borjesson M. The Daily Movement Pattern and Fulfilment of Physical Activity Recommendations in Swedish Middle‐Aged Adults: The SCAPIS Pilot Study. PLoS One. 2015;10(5):e0126336. doi: 10.1371/journal.pone.0126336 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hagstromer M, Oja P, Sjostrom M. Physical activity and inactivity in an adult population assessed by accelerometry. Med Sci Sports Exerc. 2007;39(9):1502‐1508. doi: 10.1249/mss.0b013e3180a76de5 [DOI] [PubMed] [Google Scholar]
- 12. Sartini C, Wannamethee SG, Iliffe S, et al. Diurnal patterns of objectively measured physical activity and sedentary behaviour in older men. BMC Public Health. 2015;15(1):609. doi: 10.1186/s12889-015-1976-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Berkemeyer K, Wijndaele K, White T, et al. The descriptive epidemiology of accelerometer‐measured physical activity in older adults. Int J Behav Nutr Phys activity. 2016;13(1):2. doi: 10.1186/s12966-015-0316-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Clarke J, Colley R, Janssen I, Tremblay MS. Accelerometer‐measured moderate‐to‐vigorous physical activity of Canadian adults, 2007 to 2017. Health Rep. 2019;30(8):3‐10. doi: 10.25318/82-003-x201900800001-eng [DOI] [PubMed] [Google Scholar]
- 15. Lee IM, Shiroma EJ, Evenson KR, Kamada M, LaCroix AZ, Buring JE. Using Devices to Assess Physical Activity and Sedentary Behavior in a Large Cohort Study, the Women‘s Health Study. J Meas Phys Behav. 2018;1(2):60‐69. doi: 10.1123/jmpb.2018-0005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181‐188. doi: 10.1249/mss.0b013e31815a51b3 [DOI] [PubMed] [Google Scholar]
- 17. Hansen BH, Kolle E, Dyrstad SM, Holme I, Anderssen SA. Accelerometer‐determined physical activity in adults and older people. Med Sci Sports Exerc. 2012;44(2):266‐272. doi: 10.1249/MSS.0b013e31822cb354 [DOI] [PubMed] [Google Scholar]
- 18. Sagelv EH, Ekelund U, Pedersen S, et al. Physical activity levels in adults and elderly from triaxial and uniaxial accelerometry. The Tromso Study. Plos One. 2019;14(12):e0225670. doi: 10.1371/journal.pone.0225670 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Bergstrom G, Berglund G, Blomberg A, et al. The Swedish CArdioPulmonary BioImage Study: objectives and design. J Intern Med. 2015;278(6):645‐659. doi: 10.1111/joim.12384 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Migueles JH, Aadland E, Andersen LB, et al. GRANADA consensus on analytical approaches to assess associations with accelerometer‐determined physical behaviours (physical activity, sedentary behaviour and sleep) in epidemiological studies. Br J Sports Med. 2021;doi: 10.1136/bjsports-2020-103604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Arvidsson D, Fridolfsson J, Borjesson M. Measurement of physical activity in clinical practice using accelerometers. J Intern Med. 2019;286(2):137‐153. doi: 10.1111/joim.12908 [DOI] [PubMed] [Google Scholar]
- 22. Migueles JH, Cadenas‐Sanchez C, Ekelund U, et al. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017;47(9):1821‐1845. doi: 10.1007/s40279-017-0716-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Aguilar‐Farias N, Brown WJ, Peeters GM. ActiGraph GT3X+ cut‐points for identifying sedentary behaviour in older adults in free‐living environments. J Sci Med Sport. 2014;17(3):293‐299. doi: 10.1016/j.jsams.2013.07.002 [DOI] [PubMed] [Google Scholar]
- 24. Sasaki JE, John D, Freedson PS. Validation and comparison of ActiGraph activity monitors. J Sci Med Sport. 2011;14(5):411‐416. doi: 10.1016/j.jsams.2011.04.003 [DOI] [PubMed] [Google Scholar]
- 25. Dunstan DW, Kingwell BA, Larsen R, et al. Breaking up prolonged sitting reduces postprandial glucose and insulin responses. Diabetes Care. 2012;35(5):976‐983. doi: 10.2337/dc11-1931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Ekelund U, Tarp J, Steene‐Johannessen J, et al. Dose‐response associations between accelerometry measured physical activity and sedentary time and all cause mortality: systematic review and harmonised meta‐analysis. BMJ. 2019;366:l4570. doi: 10.1136/bmj.l4570 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Ekelund U, Steene‐Johannessen J, Brown WJ, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta‐analysis of data from more than 1 million men and women. Lancet. 2016;388(10051):1302‐1310. doi: 10.1016/S0140-6736(16)30370-1 [DOI] [PubMed] [Google Scholar]
- 28. Shiroma EJ, Freedson PS, Trost SG, Lee IM. Patterns of accelerometer‐assessed sedentary behavior in older women. JAMA. 2013;310(23):2562‐2563. doi: 10.1001/jama.2013.278896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all‐cause mortality and cardiovascular events in healthy men and women: a meta‐analysis. JAMA. 2009;301(19):2024‐2035. doi: 10.1001/jama.2009.681 [DOI] [PubMed] [Google Scholar]
- 30. Ekblom‐Bak E, Ekblom O, Andersson G, et al. Decline in cardiorespiratory fitness in the Swedish working force between 1995 and 2017. Scand J Med Sci Sports. 2019;29(2):232‐239. doi: 10.1111/sms.13328 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Lamoureux NR, Fitzgerald JS, Norton KI, Sabato T, Tremblay MS, Tomkinson GR. Temporal Trends in the Cardiorespiratory Fitness of 2,525,827 Adults Between 1967 and 2016: A Systematic Review. Sports Med. 2019;49(1):41‐55. doi: 10.1007/s40279-018-1017-y [DOI] [PubMed] [Google Scholar]
- 32. Stensvold D, Viken H, Steinshamn SL, et al. Effect of exercise training for five years on all cause mortality in older adults‐the Generation 100 study: randomised controlled trial. BMJ. 2020;371:m3485. doi: 10.1136/bmj.m3485 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Thompson PD, Franklin BA, Balady GJ, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation. 2007;115(17):2358‐2368. doi: 10.1161/CIRCULATIONAHA.107.181485 [DOI] [PubMed] [Google Scholar]
- 34. Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021;42(1):17‐96. doi: 10.1093/eurheartj/ehaa605 [DOI] [PubMed] [Google Scholar]
- 35. Hagstromer M, Troiano RP, Sjostrom M, Berrigan D. Levels and patterns of objectively assessed physical activity–a comparison between Sweden and the United States. Am J Epidemiol. 2010;171(10):1055‐1064. doi: 10.1093/aje/kwq069 [DOI] [PubMed] [Google Scholar]
- 36. Cassidy S, Fuller H, Chau J, Catt M, Bauman A, Trenell MI. Accelerometer‐derived physical activity in those with cardio‐metabolic disease compared to healthy adults: a UK Biobank study of 52,556 participants. Acta Diabetol. 2018;55(9):975‐979. doi: 10.1007/s00592-018-1161-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Prince SA, Roberts KC, Reed JL, Biswas A, Colley RC, Thompson W. Daily physical activity and sedentary behaviour across occupational classifications in Canadian adults. Health Rep. 2020;31(9):13‐26. doi: 10.25318/82-003-x202000900002-eng [DOI] [PubMed] [Google Scholar]
- 38. Turrisi TB, Bittel KM, West AB, et al. Seasons, weather, and device‐measured movement behaviors: a scoping review from 2006 to 2020. Int J Behav Nutr Phys activity. 2021;18(1):24. doi: 10.1186/s12966-021-01091-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Holtermann A, Krause N, van der Beek AJ, Straker L. The physical activity paradox: six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br J Sports Med. 2018;52(3):149‐150. doi: 10.1136/bjsports-2017-097965 [DOI] [PubMed] [Google Scholar]
- 40. Dalene KE, Tarp J, Selmer RM, et al. Occupational physical activity and longevity in working men and women in Norway: a prospective cohort study. Lancet Public Health. 2021;6(6):e386‐e395. doi: 10.1016/S2468-2667(21)00032-3 [DOI] [PubMed] [Google Scholar]
- 41. Eriksson JS, Ekblom B, Kallings LV, et al. Active commuting in Swedish workers between 1998 and 2015‐Trends, characteristics, and cardiovascular disease risk. Scand J Med Sci Sports. 2020;30(2):370‐379. doi: 10.1111/sms.13581 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Chastin SFM, McGregor D, Biddle S, et al. Striking the right balance: evidence to inform combined physical activity and sedentary behaviour recommendations. J Phys Act Health Accepted for Publication. 2021. [DOI] [PubMed] [Google Scholar]
- 43. Sanchez‐Lastra MA, Ding D, Dalene KE, Ekelund U, Tarp J. Physical Activity and Mortality Across Levels of Adiposity: A Prospective Cohort Study From the UK Biobank. Mayo Clin Proc. 2021;96(1):105‐119. doi: 10.1016/j.mayocp.2020.06.049 [DOI] [PubMed] [Google Scholar]
- 44. Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self‐report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys activity. 2008;5:56. doi: 10.1186/1479-5868-5-56 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Prince SA, Cardilli L, Reed JL, et al. A comparison of self‐reported and device measured sedentary behaviour in adults: a systematic review and meta‐analysis. Int J Behav Nutr Phys activity. 2020;17(1):31. doi: 10.1186/s12966-020-00938-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Ayabe M, Kumahara H, Morimura K, Tanaka H. Epoch length and the physical activity bout analysis: an accelerometry research issue. BMC Res Notes. 2013;6(1):20. doi: 10.1186/1756-0500-6-20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Kelly LA, McMillan DG, Anderson A, Fippinger M, Fillerup G, Rider J. Validity of actigraphs uniaxial and triaxial accelerometers for assessment of physical activity in adults in laboratory conditions. BMC Med Phys. 2013;13(1):5. doi: 10.1186/1756-6649-13-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Fridolfsson J, Borjesson M, Ekblom‐Bak E, Ekblom O, Arvidsson D. Stronger Association between High Intensity Physical Activity and Cardiometabolic Health with Improved Assessment of the Full Intensity Range Using Accelerometry. Sensors (Basel). 2020;20(4):1118–doi: 10.3390/s20041118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Gatti AA, Stratford PW, Brenneman EC, Maly MR. GT3X+ accelerometer placement affects the reliability of step‐counts measured during running and pedal‐revolution counts measured during bicycling. J Sports Sci. 2016;34(12):11ss68‐1175. doi: 10.1080/02640414.2015.1096018 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material
Supplementary Material