

Abstract
Objective:
There is ongoing discussion about whether sport participation is a risk or protective factor for eating disorders (EDs). Research is mixed, with some studies suggesting that athletes have higher mean levels of ED psychopathology compared to non-athletes, while other studies suggest the opposite effect or no differences. The purpose of the current meta-analysis was to identify whether female athletes reported higher mean levels of ED psychopathology compared to non-athletes.
Method:
Following PRISMA guidelines, we identified 56 studies that reported ED psychopathology for female athletes and non-athletes. A three-level random effects model of between- and within-study variance was completed for the following outcome variables: overall ED psychopathology, body dissatisfaction, drive for thinness, restricting, and loss-of-control eating.
Results:
Athletes reported lower levels of body dissatisfaction compared to non-athletes (g = −.21, p <.0001). Athletes and non-athletes reported similar levels of overall ED psychopathology, drive for thinness, restricting, and loss-of-control eating on average. Sport type significantly moderated standardized mean difference effect sizes of ED psychopathology in athletes versus non-athletes. Effect sizes comparing levels of drive for thinness, restricting, and loss-of-control eating in athletes versus non-athletes were larger for studies with athletes participating in aesthetic/lean sports compared to non-aesthetic/non-lean sports.
Discussion:
Findings from this meta-analysis could inform future ED prevention and treatment in female athletes by providing further evidence that athletes in aesthetic/lean sports may report higher levels of ED psychopathology. Participating in non-aesthetic/non-lean sports may be a protective factor for experiencing less body dissatisfaction.
Keywords: athletes, eating disorders, meta-analysis, review, females, disordered eating, body dissatisfaction, loss of control, restricting, restraint
Eating disorders (EDs) are serious mental-health conditions associated with high rates of medical complications and mortality (Mehler et al., 2010; Smink et al., 2012). Athletes experience both physical and psychological demands from sport that could increase their susceptibility to the development of EDs (Thompson & Sherman, 2011). Athletes follow intensive training schedules and endure internal pressures from self, as well as external pressures (e.g., from teammates, coaches, and sport systems) to maintain a specific weight or shape for the purposes of maximizing sport performance or meeting sport-based aesthetic ideals (de Bruin & Oudejans, 2018; Galli et al., 2017; Hagmar et al., 2008; Scott et al., 2019; Thiemann et al., 2015).
‘Aesthetic/lean’ sports encourage thinness and leanness to maximize sport performance or meet aesthetic ideals. Examples of aesthetic/lean sports include gymnastics, diving, rowing, figure skating, ballet, and long-distance running. ‘Non-aesthetic/non-lean’ sports do not emphasize thinness or leanness for aesthetics or performance. Examples of non-aesthetic/non-lean sports include most ball sports (e.g., volleyball, soccer, etc.) and strength-focused activities (e.g., shot put). Athletes competing in aesthetic/lean sports may be more susceptible to ED psychopathology compared to non-aesthetic/non-lean sports, due to the perception that weight/shape significantly alters performance in sport (Joy et al., 2016; Krentz & Warscburger, 2011; Krentz & Warschburger, 2013; Kong & Harris, 2015; Thompson & Sherman, 2010). Sport-related social pressures to maintain a certain physique can result in physical overtraining (e.g., training for too long, too often, or too intensely), as well as harmful eating behaviors (e.g., dietary restriction, self-induced vomiting, etc.) to alter shape and weight (Galli et al., 2017; Scott et al., 2019).
Despite the intention to improve sport performance, disordered-eating behaviors and overtraining in athletes can lead to Relative Energy Deficiency Syndrome [RED-S; (Tayne et al., 2019)], updated from the term ‘Female Athlete Triad.’ RED-S is a condition characterized by low energy availability resulting from an imbalance between energy expenditure and intake [i.e., more calories expended through physical activity than consumed through food; (Mountjoy et al., 2018; Tayne et al., 2019)]. RED-S may be indicative of an underlying ED and is a syndrome associated with injury, decreased sport performance, and several serious medical problems among athletes (Mountjoy et al., 2018; Tayne et al., 2019).
Although there is a large literature on EDs in athletes, the findings are mixed. Some studies found that athletes reported higher mean levels of ED psychopathology and higher prevalence of EDs compared to non-athletes (e.g., Holm-Denoma et al., 2009; Sundgot-Borgen & Torstveit, 2004), whereas other studies showed the opposite effect or no differences between athletes and non-athletes (e.g., Martinsen et al., 2010; Reinking & Alexander, 2005). Studies also differ in terms of what specific aspects of ED psychopathology are measured (e.g., body dissatisfaction, drive for thinness, restricting, and loss-of-control eating, etc.). Thus, it is unclear if athletes have higher or lower mean levels of ED psychopathology compared to non-athletes, and if certain subgroups of athletes are more at risk for EDs or protected from EDs compared to other subgroups of athletes. Without knowing differential risks for subgroups of athletes for different aspects of ED psychopathology (e.g., body dissatisfaction vs. restricting), it is unclear if and how to prioritize limited resources for further research and prevention efforts.
Several previous studies synthesized the research on ED psychopathology in athletes using meta-analytic techniques. Arcelus et al., (2014) completed a meta-analysis to summarize research studies focused on the prevalence of ED psychopathology and EDs among female dancers and non-dancers. Female dancers reported higher rates of ED psychopathology and diagnosable EDs compared to non-dancers (Arcelus et al., 2014). More specifically, ballet dancers showed evidence for a higher prevalence of EDs, specifically higher rates of anorexia nervosa and other specified feeding or eating disorder (OSFED), compared to other forms of dancing (Arcelus et al., 2014). Hausenblas and Downs (2001) completed a meta-analysis comparing athletes and non-athletes on measures of body image concerns. Findings from this meta-analytic review indicated that athletes reported lower levels of body dissatisfaction compared to non-athletes suggesting that athletes may experience some protective factors from EDs. Another meta-analysis compared levels of ED psychopathology in male athletes compared to non-athletes (Chapman & Woodman 2016). Findings indicated that male athletes and non-athletes did not differ significantly on measures of ED psychopathology, with the exception of men participating in wrestling who reported more ED psychopathology relative to non-athletes (Chapman & Woodman, 2016).
The last meta-analysis focusing on ED psychopathology in female athletes across several sports was published approximately 20 years ago (Smolak et al., 2000). Smolak et al. (2000) completed a meta-analysis of 33 studies to compare levels of ED psychopathology among athlete and non-athlete females. Studies were eligible for the meta-analysis if they included: 1) a sample of female athletes, 2) a measure of ED psychopathology, and 3) a statistic characterizing levels of ED psychopathology in athletes (e.g., mean and standard deviation, F test statistic, t test statistic, correlation coefficient, or the proportion of athletes scoring above a cut-off score). Thus, studies included in the Smolak et al. (2000) meta-analysis did not have to include a non-athlete control group. When a control group was not included, national norms were used, when available. Overall, results suggested that female athletes reported higher levels of ED psychopathology compared to non-athletes, although the effect size was very small (d = .07), possibly due to a large amount of heterogeneity. A slightly larger effect size was observed (d = .15) when limiting the analyses to studies of collegiate athletes and non-athletes. However, when limiting the analyses to high-school aged girls, there was no longer a significant difference between athletes and non-athletes (d = −.06). Differences also emerged based on sport type and sport level. Those who were involved in a dance/performance sport reported significantly more ED psychopathology compared to non-athletes (d = .42). However, there were no significant differences that emerged for swimmers, runners, or gymnasts when compared to non-athletes (d = −.01, −.06, and −.11). Elite athletes (i.e., competing professionally or at national/international levels) and lean athletes (e.g., gymnasts) reported higher rates of ED psychopathology compared to non-athletes (d = .22 and d = .28). Moreover, elite athletes participating in lean sports showed the largest effect for increased ED psychopathology compared to non-athletes (d = .52). Non-elite, non-lean athletes reported lower scores on ED psychopathology compared to non-athletes (d = −.22), suggesting a protective factor for those athletes participating at a lower level and in a sport that does not encourage leanness. Smolak et al. (2000) found that studies using the Eating Disorder Inventory [EDI; (Garner, 1991)] Drive for Thinness and the Eating Attitudes Test [(EAT); Garner & Garfinkel, 1979)] showed positive significant effects, such that athletes reported more ED psychopathology compared to non-athletes when the EAT and EDI Drive for Thinness were used compared to author-developed measures of body dissatisfaction. Athlete status appeared to be a protective factor for body dissatisfaction, such that athletes reported less body dissatisfaction compared to non-athletes.
The meta-analysis completed by Smolak et al. (2000) had several strengths, including broad inclusion criteria, which allows for broader generalizations and comparisons amongst many different types of athletes. Despite these strengths, an updated meta-analysis of ED psychopathology behaviors among female athletes is warranted for several reasons. First, there have been over 300 studies completed on the topic of “Athletes” and “Eating Disorders” in females since the first meta-analysis was published in 2000, representing a six-fold increase in available studies on the topic. Second, since the most recent comprehensive meta-analysis in females, researchers developed important guidelines for completing meta-analytic reviews and new statistical methods for examining heterogeneity and adjusting analyses for study interdependence (Gurevitch et al., 2018; Moher et al., 2009; Page et al., 2021). Given the large number of published studies over the past 20 years and the development of new standardized reporting methods and statistical procedures, an updated meta-analysis on the topic of female athletes and ED psychopathology is warranted. Although there was one recent meta-analysis on the topic of ED psychopathology in female athletes, it was narrow in scope by including only dancers (Arcelus et al., 2014). Thus, there has not been an updated meta-analysis on female athletes across sport disciplines. Given that a comprehensive meta-analysis on male athletes and non-athletes across sports was recently published (Chapman & Woodman, 2016), the current meta-analysis focused on female athletes.
The purpose of the current study was to complete an updated meta-analysis of studies comparing ED psychopathology among athletes versus non-athlete controls. We aimed to evaluate whether all athletes or specific sub-groups of athletes reported higher mean levels of ED psychopathology compared to their non-athlete counterparts. First, we hypothesized that athletes would report higher mean levels of overall ED psychopathology, drive for thinness, restricting, and loss-of-control eating compared to non-athletes, although, consistent with past meta-analytic research, we hypothesized that the effect would be small (Arcelus et al., 2014; Smolak et al., 2000). Second, we expected that athletes would report lower levels of body dissatisfaction compared to non-athletes, consistent with past meta-analytic research (Hausenblas & Downs, 2001; Smolak et al., 2000). Third, we hypothesized that there would be a large amount of heterogeneity across studies, with moderator analysis indicating that certain sub-groups of athletes would report higher rates of ED psychopathology. More specifically, we hypothesized that sport type (aesthetic/leanness sports vs. non-aesthetic/non-leanness sports), age, and level of sport participation (elite/expert vs. collegiate vs. high school/club) would moderate effect sizes. Sport type was hypothesized to moderate effect sizes because of the unique risk that aesthetic/leanness sports may have on ED psychopathology compared to non-aesthetic/non-leanness sports (Joy et al., 2011; Krentz & Warschburger, 2013; Kong & Harris, 2015; Thompson & Sherman, 2010). Age was hypothesized to influence effect size due to the large variation of ages included. Level of sport participation was hypothesized to influence effect sizes due to findings that elite athletes reported more ED psychopathology than non-elite athletes (Smolak et al., 2000).
Method
The current study followed meta-analytic procedures published in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Reporting Guidelines (Page et al., 2021). Methods for the systematic search, study selection, data extraction, and analyses are described in the following sections.
Information Sources & Search Terms
Our systematic search was designed to identify any study published, including dissertations, that included a measure of ED psychopathology among female athletes and non-athletes. Information sources included PubMed and PsycINFO. Specific search terms in PsycINFO were: (su(“athlet*”) OR AB,TI(“team”) OR AB,TI(“sport*”) OR AB,TI(“athlet*”) OR su(“team”) OR su(“sport*”)) AND (AB,TI(“bulimia”) OR AB,TI(“anorexia*”) OR AB,TI(“binge eating”) OR AB,TI(“eating attitude*”) OR AB,TI((“eating behavior” OR “eating behaviors” OR “eating behaviour”)) OR AB,TI(“eating concern*”) OR AB,TI((“eating disorder” OR “eating disorders”)) OR su(“eating attitude*”) OR su(“anorexia*”) OR su(“bulimia”) OR su(“binge eating”) OR su(“eating behav*”) OR su(“eating concern*”) OR su(“eating disorder*”)). Filters were applied to identify articles (not books), humans (not animals), studies published in English, and studies including a female sample. Study information (e.g., title, authors, publication date, etc.) and abstracts were extracted from PubMed and PsycINFO into separate Zotero files prior to the study selection process (described below). The search was completed on January 18, 2022. We completed additional searches to ensure that we were not missing any possible studies by examining eligible study reference sections (i.e., snowballing).
Study Inclusion and Exclusion Criteria
Eligible studies were required to: 1) compare a sample of female athletes and a sample of female non-athletes and 2) include mean differences on a published measure of ED psychopathology. Studies that included mixed-gender samples were included, if they reported means separately for females and males. When mixed-sample studies reported only combined means and when studies reported only the proportion of individuals above and below a specific cut-point, we contacted the corresponding author to request means and standard deviations for the female athlete and non-athlete groups. We defined athletes as individuals who competed in organized sports or dance. Recreational sports without competition and recreational fitness activities like exercising at a gym did not meet criteria. We defined non-athletes as individuals who were not participating in organized sports; however, participation in recreational sport, fitness, and recreational dance was permissible for the non-athlete group. The definition of ED psychopathology was broad, and any measure that assessed overall ED psychopathology, body dissatisfaction, drive for thinness, restricting, or loss-of-control eating were included.
Studies were excluded if they: 1) were published in a language other than English, 2) specifically sampled participants into the study based on high or low ED psychopathology levels, 3) sampled participants into the study based on ED diagnostic status or on a characteristic that could be indicative of an ED in athletes according to RED-S criteria (e.g., irregular menstrual functioning), 4) reported national norms for the non-athlete group rather than sampling a non-athlete group, 5) created their own items to assess ED psychopathology that were not previously validated or published, 6) reported only the proportion of individuals who scored above or below a specific cut-score. We did not include studies that sampled their athlete or non-athlete groups for high vs. low ED psychopathology (or ED status) because this procedure could artificially influence results given that the aim of the current study was to compare naturally occurring levels of ED psychopathology between athlete and non-athlete groups. We chose not to include studies that compared athletes to national norms of ED psychopathology because we wanted the non-athlete group to be sampled similarly to the athlete group to limit artificial differences that could arise from different sampling procedures. Moreover, we did not include studies that created their own measure of ED psychopathology because we wanted to ensure that results were not influenced by the inclusion of unvalidated measures or measures using only single items to assess ED psychopathology.
Study Selection Process
PubMed and PsycINFO Zotero files were combined and duplicates were removed. Studies were examined for possible inclusion based on the following step-by-step process: 1) titles were examined, 2) abstracts were read, and 3) manuscripts were read. Studies that did not meet the proposed eligibility criteria were removed at each step. The first author (DC) and second author (SJ) completed the study selection process.
Data Extraction Process
The first author (DC) and a team of coders (second-seventh authors) completed data extraction. Included studies were coded by two independent coders for all extracted variables using a pre-defined Excel spreadsheet and detailed coding protocol. Study information variables extracted included: authors, publication type, year of publication, year data were collected, country data collected in, age range, mean age, sport type(s), sport level(s), whether the sport(s) was aesthetic/lean, and the number of years of sport participation. Aesthetic/lean sports included sports that emphasized thinness/leanness or utilized weight classes including, marital arts, judo, CrossFit, distance running/cross-country running, cycling, dance, gymnastics, cheerleading, baton twirling, synchronized swimming, swimming, diving, aerobics, and ice-skating/figure skating, triathlon, and rowing. Non-aesthetic/non-lean sports included sports that did not emphasize thinness/leanness or utilize weight classes, including volleyball, soccer, basketball, softball, hockey, and tennis. Sports were categorized aesthetic/lean or non-aesthetic/non-lean based on previous studies (Martinsen et al., 2010). Some sport categories (e.g., CrossFit) were not explicitly categorized in Martinsen et al. (2010), and in these instances we categorized these sports as aesthetic/lean and non-aesthetic/non-lean based on our general definition. For example, to be consistent with our categorization of other weight-based sports, we categorized CrossFit as an aesthetic/lean sport. The elite/expert level was defined as competing or performing at the national, international, or professional level. Collegiate athletes competed at the collegiate level in any division, DI, DII, or DIII. Club/Regional athletes competed in sport locally or regionally outside of high school. High school athletes competed at the high school level.
Effect size information variables that were extracted included: total sample size, sample size of athletes, sample size of non-athletes, page number with effect size information, means and standard deviations for athletes and non-athletes on all ED psychopathology outcome measures, additional data needed to calculate effect sizes when means and standard deviations were not reported (e.g., t-score, confidence intervals, etc.), and internal consistency reliability as measured by Cronbach’s Alpha for each self-report measure included. When there was missing data needed for effect size calculation for any particular study, the corresponding author was contacted via email with one week between contacts (maximum of three contacts). Following the data extraction process, the level-of-agreement between the two independent raters was calculated using two-way mixed intraclass correlation coefficient (ICC) for continuous variables and kappa for categorical variables. Interrater reliability ranged from moderate to almost perfect agreement (average interrater reliabilities for study information were K = .836 for categorical variables and ICC = .957 for continuous variables; average interrater reliability for effect size variables were ICC = .955. Any discrepancies in data extraction/coding were discussed among the two coders and resolved leading to a final data extraction file to be used for statistical analyses.
Synthesis of Results
The ‘metafor’ package in R (Viechtbauer, 2010) was used to complete all analyses. The principal summary measure was the difference in means between athletes and non-athletes. We calculated Hedge’s g effect sizes using standardized mean differences. Hedges’ g was used to summarize standardized mean differences as some studies included small sample sizes in each group (e.g., n < 20), and Hedges’ g is corrected to be an unbiased estimator of effect size in small samples (Hedges, 1981). General guidelines for Hedges’ g interpretation are similar to the interpretation of Cohen’s d as the estimates are nearly identical if sample sizes are larger than 20, .2 for a small effect, .5 for a medium effect, and .8 for a large effect (Cohen, 1992). When studies included multiple groups of athletes of the same type and only one control group (e.g., multiple aesthetic/lean sport groups compared to one control group) or multiple measures of the same ED construct (e.g., means and standard deviations on EDI-BD and another measure of body dissatisfaction), the means and standard deviations were averaged using a weighted averaging approach to avoid issues of interdependence. When studies reported on aesthetic/lean athletes and/or non-aesthetic/non-lean athletes separately, we retained an effect size for those groups to inform our hypothesis about aesthetic/lean vs. non-aesthetic/non-lean athletes. Similarly, when studies reported on various sport levels separately (e.g., elite/expert athletes, collegiate athletes, high school, and club athletes), we retained an effect size for those groups to inform our hypothesis about sport levels. Using a multilevel model of within- and between-study random-effects methods, we investigated the amount of heterogeneity among different studies using the Q test. The Q test was used due to research highlighting similarities between Q and other heterogeneity tests like I2 (Augusteijn et al., 2019; Huedo-Medina et al., 2006). The null hypothesis of the Q test is homogeneity, and significant p-values on this test indicate that there is support for heterogeneity. If a large amount of heterogeneity existed, which was hypothesized, we completed additional sub-group analysis using a multilevel approach to test if sport type, age, sport level, and nationality moderated the observed effect sizes. Publication bias was evaluated by examining funnel plots and Begg’s test.
To assess risk of bias within the included studies, we modified the Joanna Briggs Institute’s (JBI) Critical Appraisal Checklist for Analytical Cross-Sectional Studies (Joanna Briggs Institute, 2017) to be relevant and consistent with the design of the current meta-analysis (please see online supplement for details). Two independent raters completed the modified JBI checklist for each included study, and discrepancies were discussed and resolved as a team. Average interrater reliability on the JBI checklist ratings was .621.
Results
We contacted the corresponding author for 44 articles to request additional information that would be necessary to meet study inclusion criteria (e.g., means and standard deviations, women/girl data separate from men/boy data, etc.). Our contacts were unsuccessful for 21 of these articles, and authors did not have access to raw data to provide additional information for an additional 17 articles. Data were available for six articles; two of these six articles contained duplicate data that were already represented in another included article. Thus, an additional four articles were included after contacting authors. A total of 56 studies and k = 208 effect sizes were included in the final meta-analysis (see Figure 1 for a Flow Diagram). Detailed effect size information for each study can be found in Table 1 and information on race, ethnicity, and SES for each study can be found in Table 2.
Figure 1.
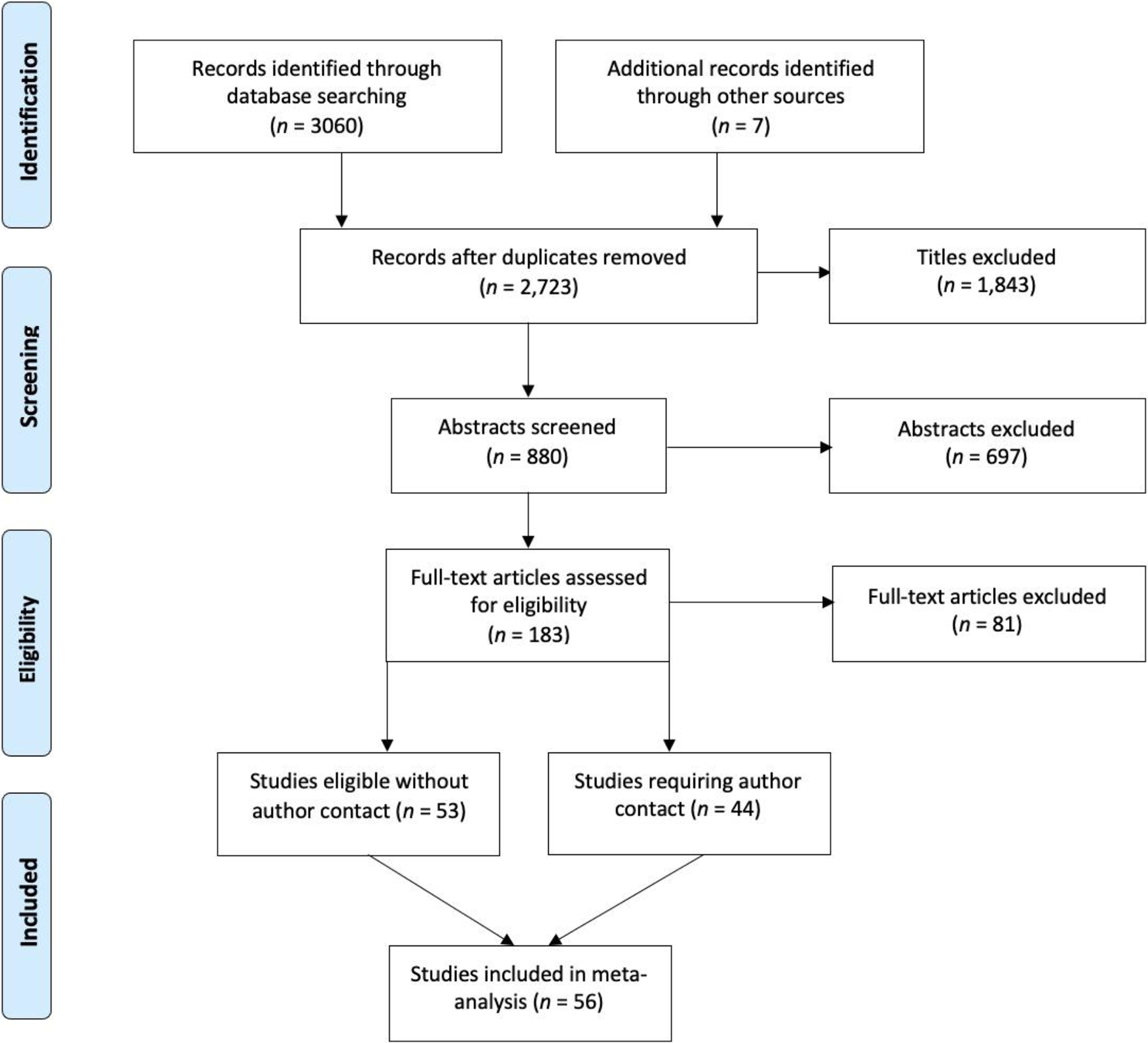
Flow Diagram
Table 1.
Study and Effect Size Information
| Author(s) | Effect Size(s) g | Athlete Group(s) n | Control Group(s) n | Sport Level | Mean Age | ED Measures |
|---|---|---|---|---|---|---|
| Abbott et al. (2021) | −0.36e (NA) |
70 | 138 | Elite/Expert | 24.5 | EAT26e |
| Ashley et al. (1996) | −.238a
−.034b −.116e |
145 | 14 | Collegiate | 19.2 | EDI2-BDa EDI2-DTb EDI2-Be |
|
Bachner-Melman et al. (2006)
|
−.173a (A) −.083b (A) −.058e (A) −.451a −.350b −.181e |
111 (A) 68 |
248 | NR | 21.17 | EDI2-BDa EDI2-DTb, SATAQ-TIb EAT26e |
| Bert et al. (2019) | −.371c | 82 | 57 | NR | 26.70 | EHQc, ORTO15c |
| Brooks-Gunn et al. (1988) | .421c (A) .514e (A) |
161(A) | 424 | Combined | 15.66 | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Byrne & McLean (2002) | .004a (A) .836b (A) .939c (A) .632e (A) .115a (NA) .272b (NA) .423c (NA) .255e (NA) |
93 (A) 61 (NA) |
154 | Elite/Expert Elite/Expert |
18.05 | EDI2-BDa EDI2-DTb TFEQ-Rc EDI2-Be, BUILTRe |
| Carvalhais et al. (2019)* | −.108a .322c .143d .049e |
372 | 372 | Elite/Expert | 21.00 | EDEQ-Sa, EDEQ-Wa EDEQ-Rc EDEQ-ECd EDEQe |
| Costarelli & Stamou (2009) | .094a (A) .134e (A) |
14 (A) | 32 | Elite/Expert | 19.67 | MBSRQ-OPa EAT26e |
| Darcy et al. (2013a) | −.062a .020c −.092d .054e |
544 | 429 | Combined | 20.82 | EDEQ-Sa, EDEQ-Wa
EDEQ-Rc EDEQ-ECd EDEQe |
| Davis & Cowles (1989) | −.323a (A) .163b (A) −.109e (A) −.903a (NA) −.366b (NA) −.445e (NA) |
64 (A) 62 (NA) |
64 | Combined | 20.67 | EDI-BDa EDI-DTb EDI-Be |
| Davison et al. (2002) | .201a (A) −.311a |
174 (A) 57 |
158 | NR | 6.00 | WCa |
| de Oliveira Coelho et al. (2013)* | −.638a (NA) −.321e (NA) |
24 (NA) | 21 | Combined | 15.09 | BSQa BITEe, EAT26e |
| DiBartolo & Shaffer (2002) | −.688a
−.560e |
94 | 115 | Collegiate | 19.10 | EDI-BDa EAT26e |
| Doyle-Lucas et al. (2010) | .549c (A) .652d (A) .460e (A) |
15 (A) | 15 | Elite/Expert | 24 | TFEQ-Rc TFEQ-Dd EAT26e |
| Ferrand et al. (2009) | 1.244e (A) |
103 (A) | 49 | Elite/Expert | 16.10 | EAT26e |
| Fortes et al. (2014)* | −.876c 1.524e |
116 | 199 | Combined | 13.64 | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Francisco et al. (2013) | .230a (A) .439c (A) .530d (A) .362e (A) |
60 (A) | 82 | Elite/Expert | 14.78 | EDEQ-Sa, EDEQ-Wa EDEQ-Rc EDEQ-ECd EDEQe |
| Gaines & Burnett (2014) | −6.336e | 58 | 196 | Collegiate | 20.8 | EATe |
| Goldfield (2009) | −.130a (A) .183b (A) .647e (A) |
20 (A) | 25 | NR | 26.80 | EDI-BDa EDI-DTb EDI-Be |
| Goodwin et al. (2016) | −.393a −.212b −.126e |
123 | 126 | Combined | 14.80 | EDI2-BDa EDI2-DTb EDI2-Be |
| Grupski (2010) | −.220a −.149b |
178 | 361 | Combined | 20.43 | SPASa DISb, EDI2-DTb |
| Haase & Prapavessis (2001) | −.112a (A) .517e (A) −.381a (NA) −.159e (NA) |
123 (A) 75 (NA) |
53 | Elite/Expert |
19.04 | SPASa EATe |
| Hausenblas & Mack (1999) | −.796a (A) −.444b (A) 0e (A) −.145a (NA) .092b (NA) .079e (NA) |
36 (A) 39 (NA) |
39 | Combined |
17.02 | EDI2-BDa, SPASa EDI2-DTb EDI2-Be |
| Hausenblas & McNally (2004) | −.724a
−.374b −.397e |
140 | 95 | Combined | 20.28 | EDI2-BDa EDI2-DTb EDI2-Be |
| Heradstveit et al. (2020)* | −.116e | 2716 | 2416 | NR | NR | EDS5e |
| Hoch et al. (2009) | −.161e |
80 | 80 | HS/Club | 16.50 | EAT26e |
| Holm-Denoma et al. (2009) |
Collegiate .365a −.029b .232e HS/Club .597a −.090b .223e |
43 60 |
171 | Collegiate HS/Club |
19.00 | EDI-BDa EDI-DTb EDI-Be |
| Hulley et al. (2007) |
United Kingdom −.372a (A) −.119c (A) −.148d (A) −.272e (A) Kenya −.391a (A) −.057c (A) −.353d (A) −.068e (A) |
82 (A) 75 (A) |
97 101 |
Elite/Expert | 20.80 | EDEQ-Sa, EDEQ-Wa EDEQ-Rc EDEQ-ECd EDEQe |
| Jankauskiene & Baceviciene* (2019) | .152a .001e |
108 | 191 | NR | 17.2 | MBSRQ-OPa EAT26e |
| Jankauskiene et al. (2020)* | 0a
.257b .254e |
136 | 252 | NR | 16.9 | EDI3-BDa EDI3-DTb EDEQe |
| Jeong et al. (2011) | .030a (A) −.034b (A) .429c (A) .296d (A) .222e (A) .071a (NA) −.082b (NA) −.018c (NA) −.096d (NA) −.023e (NA) Elite .064a −.073b .214c .118d .114e Collegiate −.012a −.041b .276c .139d .104e |
211 (A) 167 (NA) 284 94 |
567 | Combined Combined Elite Collegiate |
20.1 | KEDEQ-Sa, EDEQ-Wa, EDI2-BDa EDI2-DTb, SATAQ-Ib KEDEQ-Rc KEDEQ-ECd KEDEQe |
|
Kong & Harris (2015)
|
Elite .614c (A) .594e (A) .156c (NA) .077e (NA) Combined .216c (A) .138e (A) .046c (NA) −.086e (NA) |
80 (A) 48 (NA) 59 (A) 53 (NA) |
35 45 |
Elite Combined |
21.7 | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Krane et al. (2001) | −.325a (NA) −.322b(NA) −.108e (NA) −.300a −.272b −.034e |
114 (NA) 81 |
177 | Collegiate | 19.65 | EDI-BDa, SPASa EDI-DTb EDI-Be |
| Latu (2021) | −.296a (A) .024c (A) .519e (A) |
53 (A) | 253 | NR | 32.68 | MBSRQ-OPa EAT26-Dc, EAT26-OCc EAT26-Be |
| Mathisen et al. (2020) | .261e (A) |
25 (A) | 26 | Elite/Expert | 28.9 | EDEQe |
| Michou & Costarelli (2011) | .057c (NA) .029e (NA) |
74 (NA) | 80 | Elite/Expert | 25.07 | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Monthuy-Blanc et al. (2012) | .278a (A) .449b (A) −.176e (A) −.007a (NA) .112b (NA) −.234e (NA) |
50 (A) 41 (NA) |
47 | Combined Combined | 14.11 | EDI-BDa EDI-DTb EDI-Be |
| Morringson et al. (2006) | −.039a | 143 | 100 | Combined | 15.76 | MBSRQ- OPa |
| Muia et al. (2016) | .056b (A) .295c (A) |
61 (A) | 49 | Combined | NR | EDI3-DTb TFEQ-Rc |
| Okano et al. (2005) |
Japan .558c (A) .702e (A) China .179c (A) .095e (A) |
238 (A) 272 (A) |
593 147 |
Combined | NR | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Ozedengul et al., (2021) | .038c | 46 | 312 | Elite | 29.12 | ORTO-Rc |
| Palermo & Rancout (2021)* |
Study 1 −.421a −.069c −.270d −.324e Study 2 −.530a −.266c −.176d |
200 89 |
240 136 |
NR | 20.94 | EDEQ-Sa, EDEQ-Wa EPSI-BDa EDEQ-Rc EPSI-CR, EPSI-Rc EDEQ-Ed EPSI-BEd EDEQe |
| Petisco-Rodriguez et al. (2020) | −.361c (A) −.408e (A) −.282c (NA) −.331e (NA) |
40 (A) 40 (NA) |
40 | Elite/Expert | 17.2 | EAT40-Dc, EAT40-OCc EAT40-Be, SCOFFe |
| Pritchard et al. (2007) | .020a .755e |
106 | 206 | Collegiate | 21.36 | BSQa EAT26e |
| Reinking & Alexander (2005) | .255a (A) .149b (A) −.188e(A) −.603a (NA) −.500b (NA) −.538e (NA) |
16 (A) 68 (NA) |
62 | Collegiate | 19.95 | EDI2-BDa EDI2-DTb EDI2-Be |
| Rhea et al. (1999) | −.159a −.056b −.032e |
477 | 383 | HS/Club | 15.5 | EDI-BDa EDI-DTb EDI-Be |
| Robinson & Ferraro (2004) | −.880a (NA) −.784b (NA) −.009e (NA) −.938a −.566b .215e |
16 (NA) 37 |
55 | Collegiate | 19.90 | EDI-BDa EDI-DTb EDI-Be |
| Rosendahl et al. (2009)* | −.339e
|
210 | 171 | Combined | 15.80 | EAT26e |
| Rouveix et al. (2007) | .139c (A) .863e (A) |
12 (A) | 14 | Elite/Expert | 18.70 | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Schwarz et al. (2005) | −.517a | 55 | 48 | Collegiate | 20.53 | EDI-BDa |
| Somasundaram & Burgess (2008) | .016a (A) −.086e (A) −.157a 0e |
44 (A) 230 |
204 | NR | 19.31 | EDI-BDa EAT26e |
| Steinfeldt et al. (2011) | −.374b
|
78 | 65 | Collegiate | 19.74 | CFNI45-Tb |
| Thiemann et al. (2015) | −.106a (A) .569b (A) .348e (A) −.148a (NA) −.156b (NA) −.233e (NA) |
46 (A) 57 (NA) |
46 57 |
Elite/Expert |
19.58 | EDI2-BDa EDI2-DTb EDEQe |
| Torstveit & Sundgot-Borgen (2005)* | −.396a −.204b |
623 | 569 | Elite/Expert | 24.3 | EDI-BDa EDI-DTb |
| Wollenberg et al. (2015) | −.429c −.376e |
151 | 376 | Collegiate | 19.67 | EAT26-Dc, EAT26-OCc EAT26e, EAT26-Be |
| Zucker et al. (1999) | .109a (A) .522b (A) .124e (A) −.754a −.299b −.106e |
37 (A) 33 |
62 | Collegiate | 20.3 | BSQa, EDI2-BDa EDI2-DTb EDI2-Be |
Note. EAT= eating attitudes test; EAT-D= eating attitudes test- dieting; EAT-OC= eating attitudes test- oral control ; EAT-B= eating attitudes test- bulimia and food preoccupation; EDI= eating disorder inventory; EDI-BD= eating disorder inventory- body dissatisfaction ;EDI-DT= eating disorder inventory- drive for thinness; EDI-B= eating disorder inventory- bulimia; SATAQ-TI= social attitudes toward appearance scale- thin internalization; EHQ= eating habits questionnaire; TFEQ-R= three-factor eating questionnaire- dietary restraint; TFEQ-D= three factor eating questionnaire- disinhibition; BUILTR= bulimia test- revised; BUILTR-WC= bulimia test-revised- weight concern; BUILTR-DF= bulimia test-revised-dieting frequency; EDEQ= eating disorder examination- questionnaire; EDEQ-S= eating disorder examination questionnaire- shape concern; EDEQ-W= eating disorder examination questionnaire- weight concern; EDEQ-EC= eating disorder examination questionnaire- eating concern; EDEQ-R= eating disorder examination questionnaire- restraint; WC= weight concern scale; BITE= bulimia investigatory test edinburgh; BSQ= body shape questionnaire; SPAS= social physique anxiety scale; DIS= dietary intent scale; EDS= eating disorder symptoms; MBSRQ-OP= multidimensional body-self relations questionnaire- overweight preoccupation; EPSI-BD= eating pathology symptoms inventory; EPSI-CR= eating pathology symptoms inventory-cognitive restraint; EPSI-BE = eating pathology symptoms inventory- binge eating; CFNI45-T= confirmatory to feminine norms inventory- thin internalization; A= aesthetic athletes; NA= non-aesthetic athletes.
body dissatisfaction measure or effect size
drive for thinness measure or effect size
restricting measure or effect size
loss-of-control eating measure or effect size
overall eating-disorder psychopathology measure or effect size
Table 2.
Race, Ethnicity, and SES Information
| Author(s) | Race | Ethnicity | SES |
|---|---|---|---|
| Abbott et al. (2021) | NR | NR | NR |
| Ashley et al. (1996) | 84.9% White, 15.1% Black | NR | NR |
| Bachner-Melman et al. (2006) | NR | NR | NR |
| Bert et al. (2019) | NR | NR | NR |
| Brooks-Gunn et al. (1988) | Non-athletes- NR Athletes- 96.3% White, 1.9% Black, 1.9% Asian |
NR | middle- to upper-middle class |
| Byrne & McLean (2002) | 97% White, 3% Asian | NR | NR |
| Carvalhais et al. (2019)* | NR | NR | NR |
| Costarelli & Stamou (2009) | NR | NR | NR |
| Darcy et al. (2013) | 74.2% White, 11.2% Asian, 5.4% Black, 1.6% Biracial/Multiracial, 1% Other, .1% Native Hawaiian/Pacific Islander | 6.1% Hispanic |
NR |
| Davis & Cowles (1989) | NR | NR | NR |
| Davison et al. (2002) | 100% White |
0% Hispanic |
66.7% of mothers had an education above a high school diploma. Equal proportions of families reported incomes below $35K, $35K-$50K and above $50K |
| de Oliveira Coelho et al. (2013)* | NR | NR | NR |
| DiBartolo & Shaffer (2002) | Non-athletes- 69% White, 14% Asian, 10% Other/NR, 4% Black Athletes- 84% White, 7% Asian, 6% Other/NR, 2% Black |
Non-athletes- 1% Hispanic Athletes- 0% Hispanic |
NR |
| Doyle-Lucas et al. (2010) | NR | NR | NR |
| Ferrand et al. (2009) | 100% White | NR | 100% middle to upper-class |
| Fortes et al. (2014)* | NR | NR | NR |
| Francisco et al. (2013) | NR | NR | NR |
| Gaines & Burnett (2014) | 24% White, 5.9% Black, 1.2% Other Other races NR |
68.9% Hispanic | NR |
| Goldfield (2009) | NR | NR | NR |
| Goodwin et al. (2016) | 92.9% ‘White-British’ Other races NR |
NR | Assessed based on location of schools through the United Kingdom’s Office for National Statistics. Sample included individuals who had average to low levels of economic deprivation. |
| Grupski (2010) | 74.5% White, 8.5% Black, 1.5% Asian, 1.9% Biracial, .7% NR | 12.8% Latina | NR |
| Haase & Prapavessis (2001) | NR | NR | NR |
| Hausenblas & Mack (1999) | NR | NR | NR |
| Hausenblas & McNally (2004) | 72.1% White, 19.2% Black | NR | 66.8% upper-middle class, 22.8% lower-middle class |
| Heradstveit | NR | NR | Perceived economic well-being as compared to others was reported as: 7.9% poorer than others, 22% better than others, 70.1% equal to others Maternal education was reported as: 10.8% primary school, 40.3% high school, 48.9% college/university Paternal education was reported as: 10.9% primary school, 43.3% college/university, 45.8% high school |
| Hoch et al. (2009) | Non-Athletes- 95% White, 2.5% Black Athletes- 100% White |
Non-Athletes- 2.5% Hispanic Athletes- 0% Hispanic |
NR |
| Holm-Denoma et al. (2009) | 58.4% White, 21.2% Black, 2.2% Asian, 3% Other |
15.3% Hispanic/Latina |
NR |
| Hulley et al. (2007) | NR | NR | NR |
| Jankauskiene & Baceviciene (2019) | NR | NR | NR |
| Jankauskiene et al. (2020) | NR | NR | NR |
| Jeong et al. (2011) | NR | NR | NR |
| Kong & Harris (2015) | NR | NR | NR |
| Krane et al. (2001) | NR | NR | NR |
| Latu (2021) | Non-Athletes- 77.9% White, 5.1% Native American, 2% Black, 2% Asian American/Pacifica Islander, 2% Biracial Athletes- 77.4% White, 5.7% Asian American/Pacifica Islander, 3.8% Biracial, 1.9% Black, 1.9% Native American |
Non-athletes- 6.7% Hispanic/Latina Athletes- 9.4% Hispanic/Latina |
Non-athletes- 8.7% less than $20K, 5.9% $20K-$30K, 8.3% $30K-$40K, 5.9% $40K-$50K, 9.5% $50K-$60K, 9.9% $60K-$70K, 13% $70K-$80K, 35.2% above 80K Non-athletes- 0% did not complete high school, 5.1% high school degree, 5.1% AA degree, 32.8% undergraduate degree, 53.4% graduate degree Athletes- 3.8% less than $20K, 3.8% $20K-$30K, 7.5% $30K-$40K, 9.4% $40K-$50K, 9.4% $50K-$60K, 18.9% $60K-$70K, 13.2% $70K-$80K, 34% above 80K Athletes- 50.9% graduate degree, 37.7 undergraduate degree, 7.5% high school degree, 1.9% did not complete high school, 1.9% AA degree |
| Mathisen et al. (2020) | NR | NR | NR |
| Michou & Costarelli (2011) | NR | NR | NR |
| Monthuy-Blanc et al. (2012) | NR | NR | NR |
| Morringsonet al., 2005 | Non-athletes- 50.9% White, 21.7% Asian, 6.6% Black, .9% Pakistani, .9% Arab-Palestinian Athletes: 56% White, 12% Asian, 6.7% Black, 2% Pacific Islander, .7% Iranian |
Non-athletes- 18.9% Hispanic Athletes- 22.7% Hispanic |
Non-athletes- 1.1% less than $10K, 1.1% $10K-$25K, 15.6% $25K-$50K, 42.2% $50K-$100K, 40% above $100K Athletes- .7% less than $10K, 2.9% $10K-$25K, 16.8% $25K-$50K, 44.5% $50K-$100K, 35% above $100K |
| Muia et al. (2016) | NR | NR | NR |
| Okano et al. (2005) | NR | NR | NR |
| Ozedengul et al., (2021) | NR | NR | Highest Education Completed- 65.7% university, 25.5% master’s degree, 5.2% high school, 1.8% elementary, 1.8% doctorate Employment- 52.1% student, 34.7% employed, 13.2% unemployed |
| Palermo & Rancout (2021) | Study 1- 75.6% Non-Hispanic/Non-Latinx- 66.7% White, 16.3% Black, 13.8% Asian, 7.9% Other, 1.6% American Indian or Alaska Native, .9% Native Hawaiian or Other Pacific Islander Study 2- 75.1% Non-Hispanic- 66.7% White, 11.6% Black, 11.6% Asian, 4% Other, .9% American Indian or Alaska Native |
Study 1- 24.4% Hispanic/Latinx- 72% White, 19.6% Other, 14% Black, 1.9% American Indian or Alaska Native, 1.9% Asian, .9% Native Hawaiian or Other Pacific Islander Study 2- 24.9% Hispanic/Latinx- 76.4% White, 9.1% Other, 9.1% Black |
NR |
| Petisco-Rodriguez et al. (2020) | NR | NR | NR |
| Pritchard et al. (2007) | 90% White Other races NR |
NR | NR |
| Reinking & Alexander (2005) | NR | NR | NR |
| Rhea et al. (1999) | 34% Black, 22% White, 8% Other, 6% Asian, 2% Native American | 28% Hispanic |
NR |
| Robinson & Ferraro (2004) | NR | NR | NR |
| Rosendahl et al. (2009)* | NR | NR | NR |
| Rouveix et al. (2007) | NR | NR | NR |
| Schwarz et al. (2005) | 83% White, 10% Black, 1% Asian, 1% Native American |
NR | NR |
| Somasundaram & Burgess (2008) | 70.3% White, 13.3% Asian/Pacific Islander, 5% Black, 4.4% Other, .4% American Indian, | 6.6% Hispanic/Latino |
NR |
| Steinfeldt et al. (2011) | 75% White, 11% Black, 6% Multiracial, 4% Asian, 3% Other/NR |
1% Hispanic |
NR |
| Thiemann et al. (2015) | NR | NR | NR |
| Torstveit & Sundgot-Borgen (2005) | NR | NR | NR |
| Wollenberg et al. (2015) | NR | NR | NR |
| Zucker et al. (1999) | NR | NR | NR |
Note. NR= not reported.
Overall ED Psychopathology
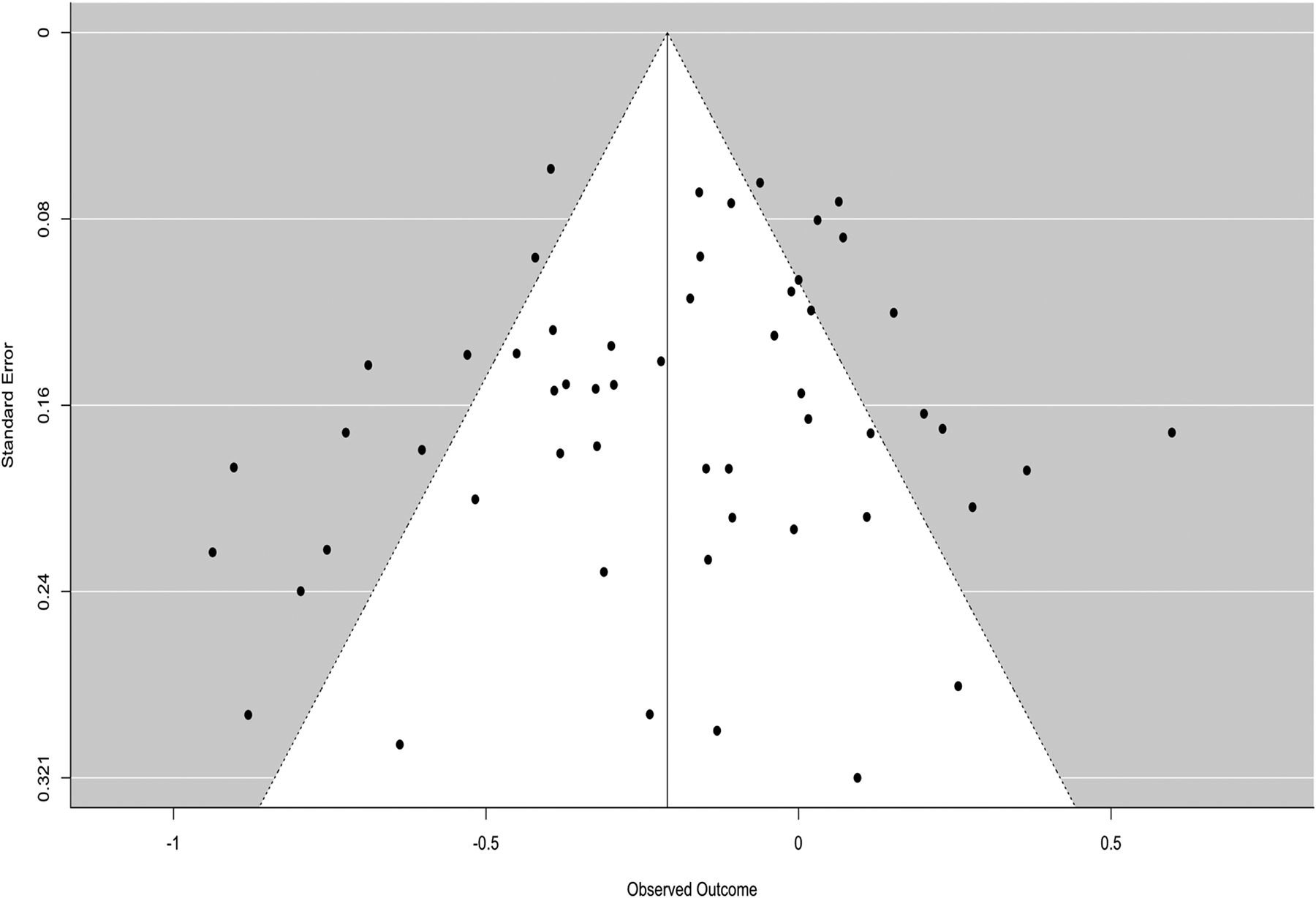
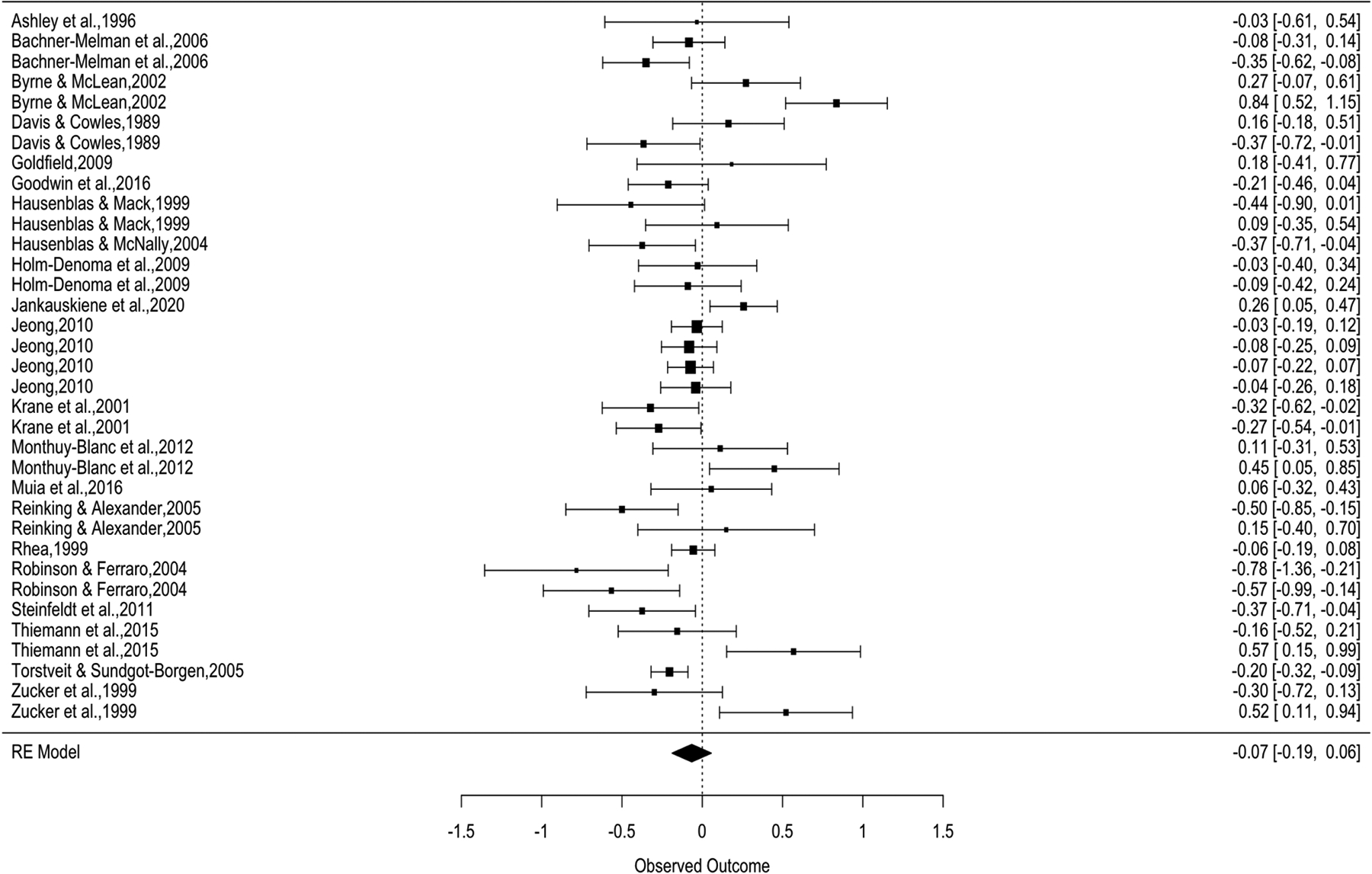
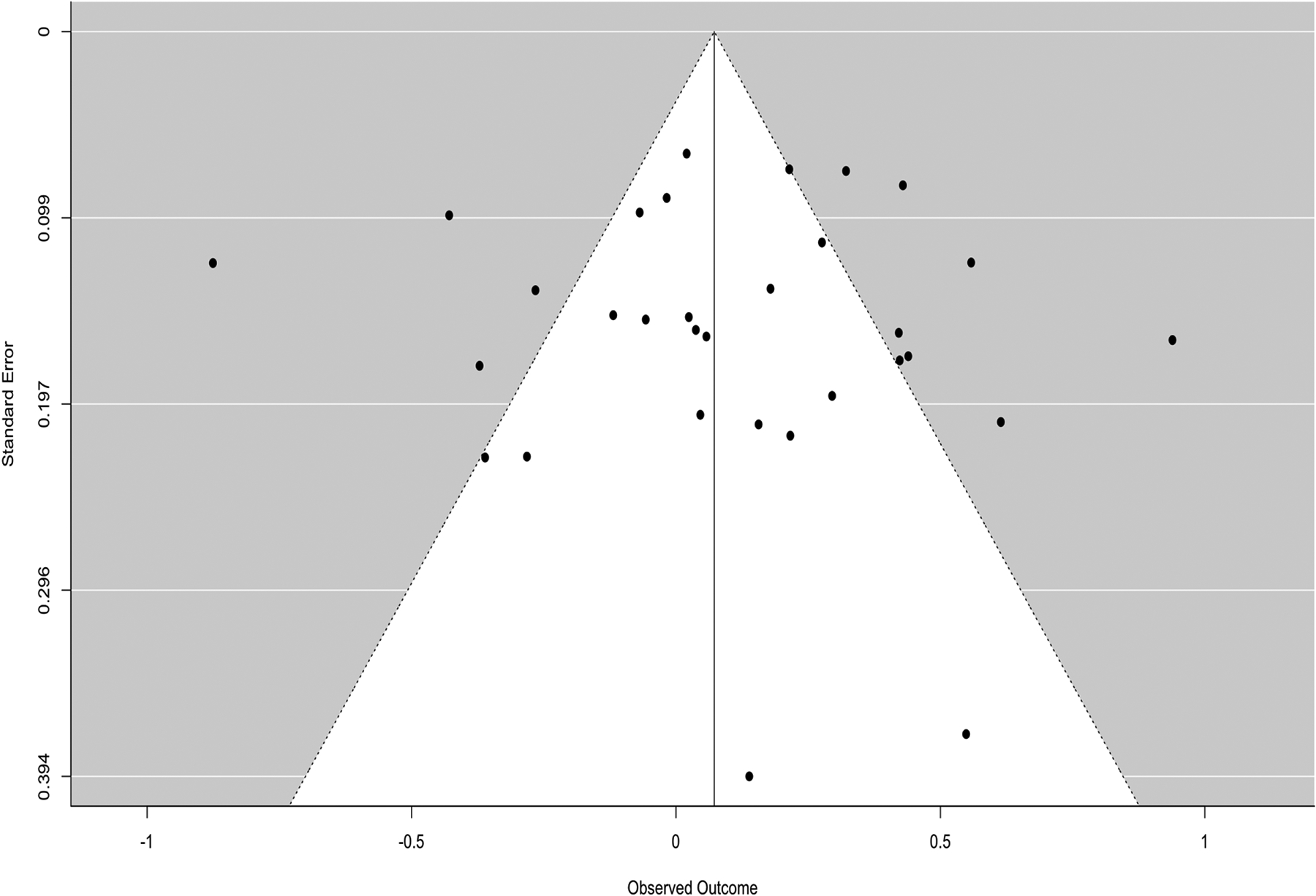
There were k = 70 effect sizes used to test mean differences in overall ED psychopathology (e.g., EDE Global, EAT-26 Total, etc.) between athletes and non-athletes. The overall effect size (g = −.035, 95% CI [−.31, .24]) was non-significant (t = −.255, p = .8), suggesting that athletes and non-athletes reported similar levels of overall ED psychopathology on average. There was a substantial amount of within-group heterogeneity, Q(69) = 814.639, p < .0001 (see Figure 2). An examination of a funnel plot (see Figure 3) and Begg’s test for asymmetry (tau = .024, p = .777) suggested that publication bias was unlikely.
Figure 2.
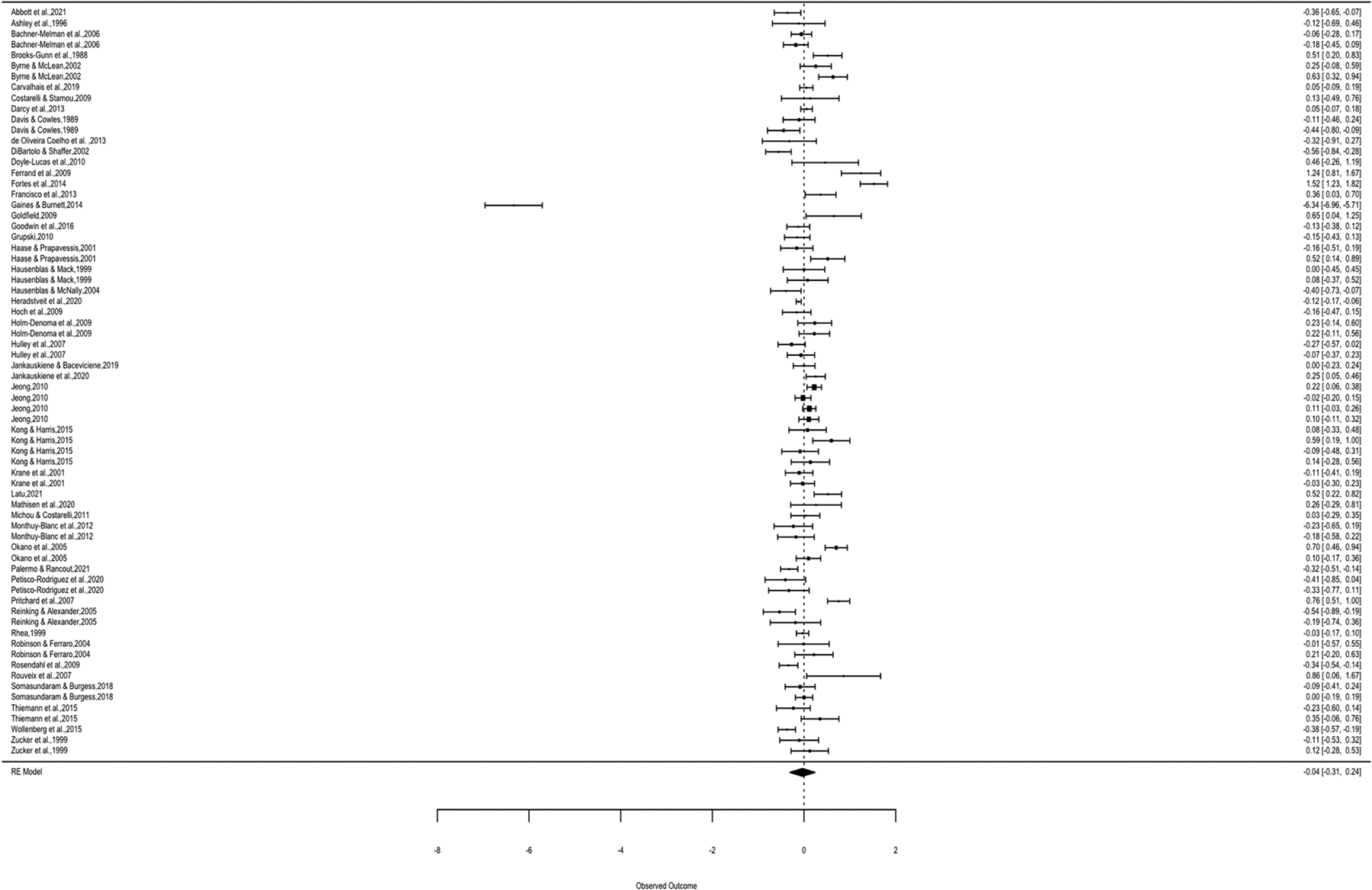
Global Eating-Disorder Psychopathology Forest Plot
Figure 3.
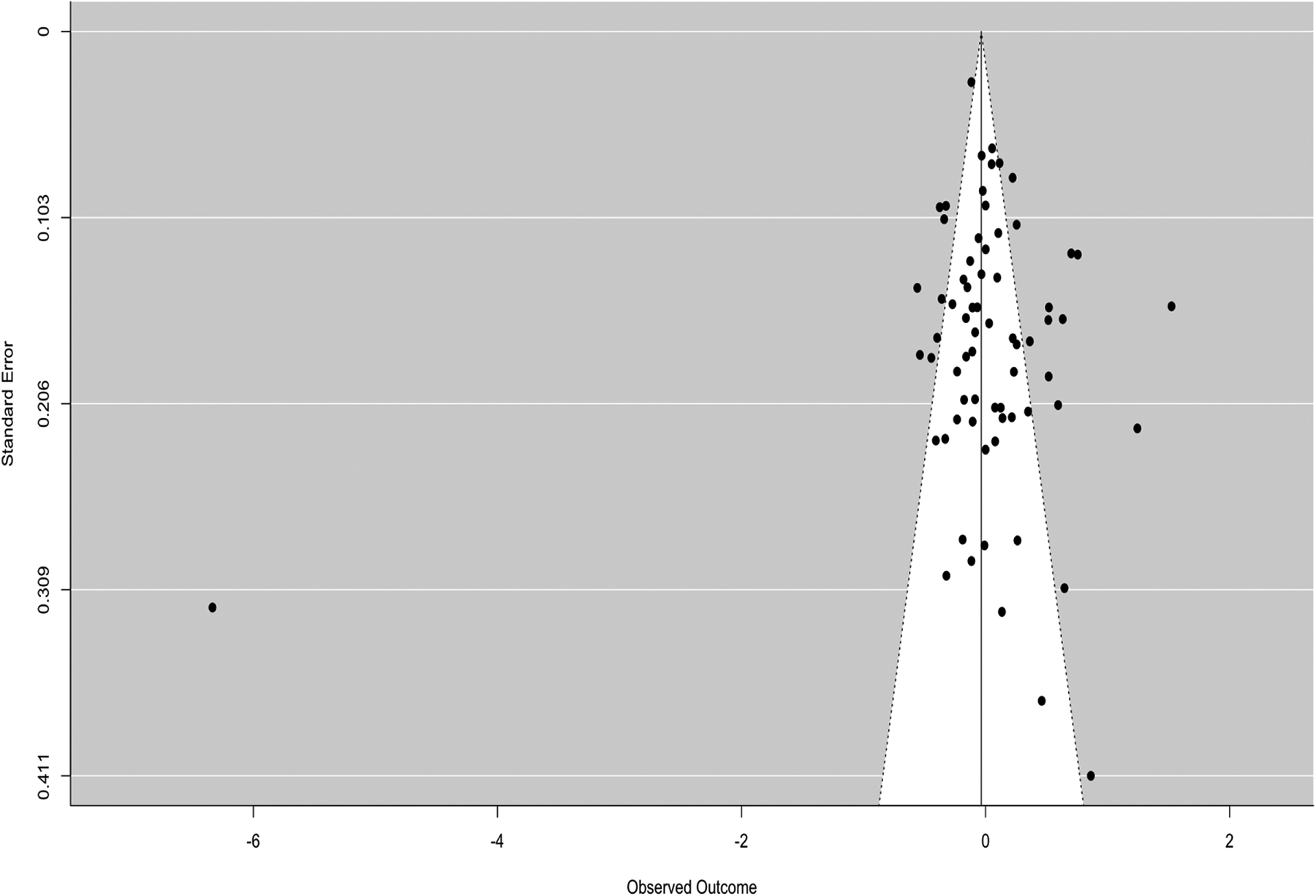
Global ED Psychopathology Funnel Plot
We evaluated the potential moderating effects of participant sport type (aesthetic/lean vs. non-aesthetic/non-lean), age, sport level (elite/expert vs. collegiate vs. high school/club), and nationality (western country vs. non-western country). Sport type was a significant moderator, F(2, 66) = 7.517, p = .001, of overall ED psychopathology differences between athletes and non-athletes, such that effect sizes were larger in studies with aesthetic/lean sports. The average effect size observed in athletes participating in non-aesthetic/non-lean sports relative to non-athletes was g = −.224, 95% CI [−.524, .076] which was not significant (t = −1.493, p = .14), suggesting that athletes participating in non-aesthetic/non-lean sports reported similar levels of overall ED psychopathology compared to non-athletes. In studies with aesthetic/lean-sport athletes, the observed differences in overall ED psychopathology between athletes and non-athletes were significantly different compared to studies with non-aesthetic/non-lean sports (t = 3.869, p < .001, g = .074). Athletes participating in aesthetic/lean sports reported more overall ED psychopathology compared to athletes participating in non-aesthetic/non-lean sports, relative to non-athletes. Participant age (F(1, 65) = .067, p = .797), sport level (F(3, 56) = .761, p = .521), and nationality (F(1, 68) = .529, p = .469) were non-significant moderators.
Body Dissatisfaction
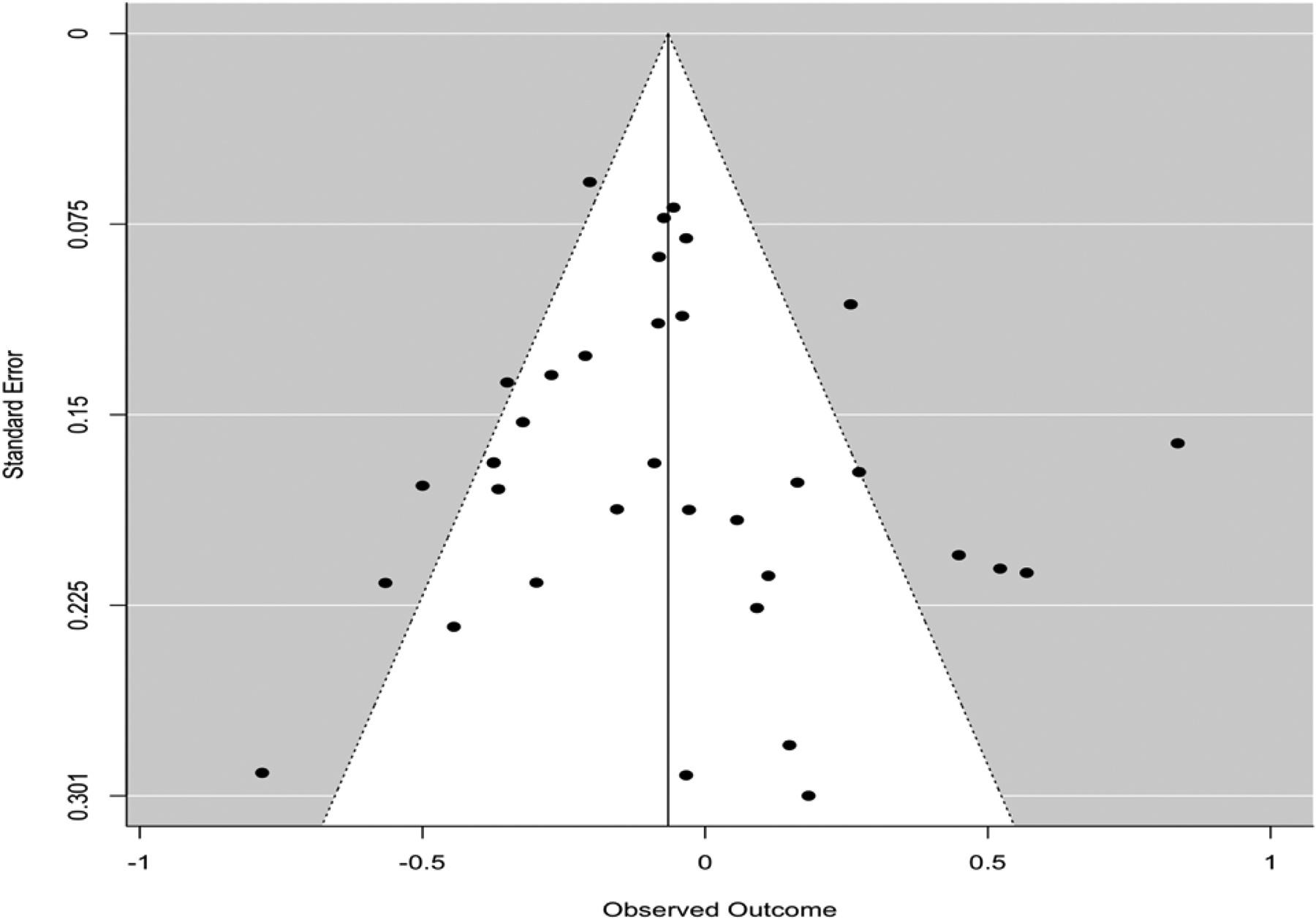
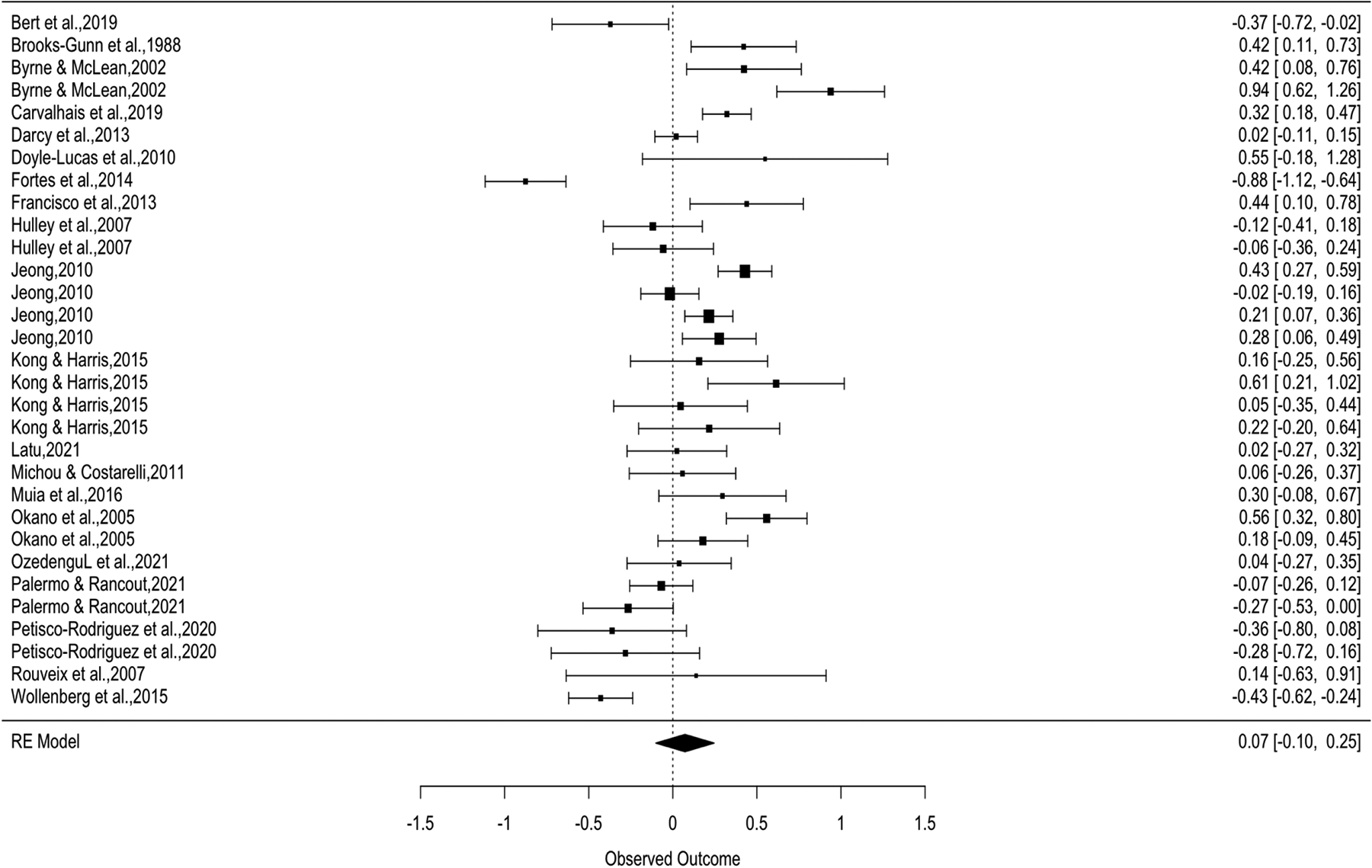
There were k = 55 effect sizes used to test mean differences in body dissatisfaction between athletes and non-athletes. The overall effect size (g = −.21, 95% CI [−.306, −.114]) was significant (t = −4.385, p <.0001) demonstrating that athletes reported lower levels of body dissatisfaction compared to non-athletes on average. There was a substantial amount of within-group heterogeneity, Q(54) = 223.14, p < .0001 (see Figure 4). An examination of a funnel plot (see Figure 5) and Begg’s test for asymmetry (tau = −.125, p = .183) suggested that publication bias was unlikely.
Figure 4.
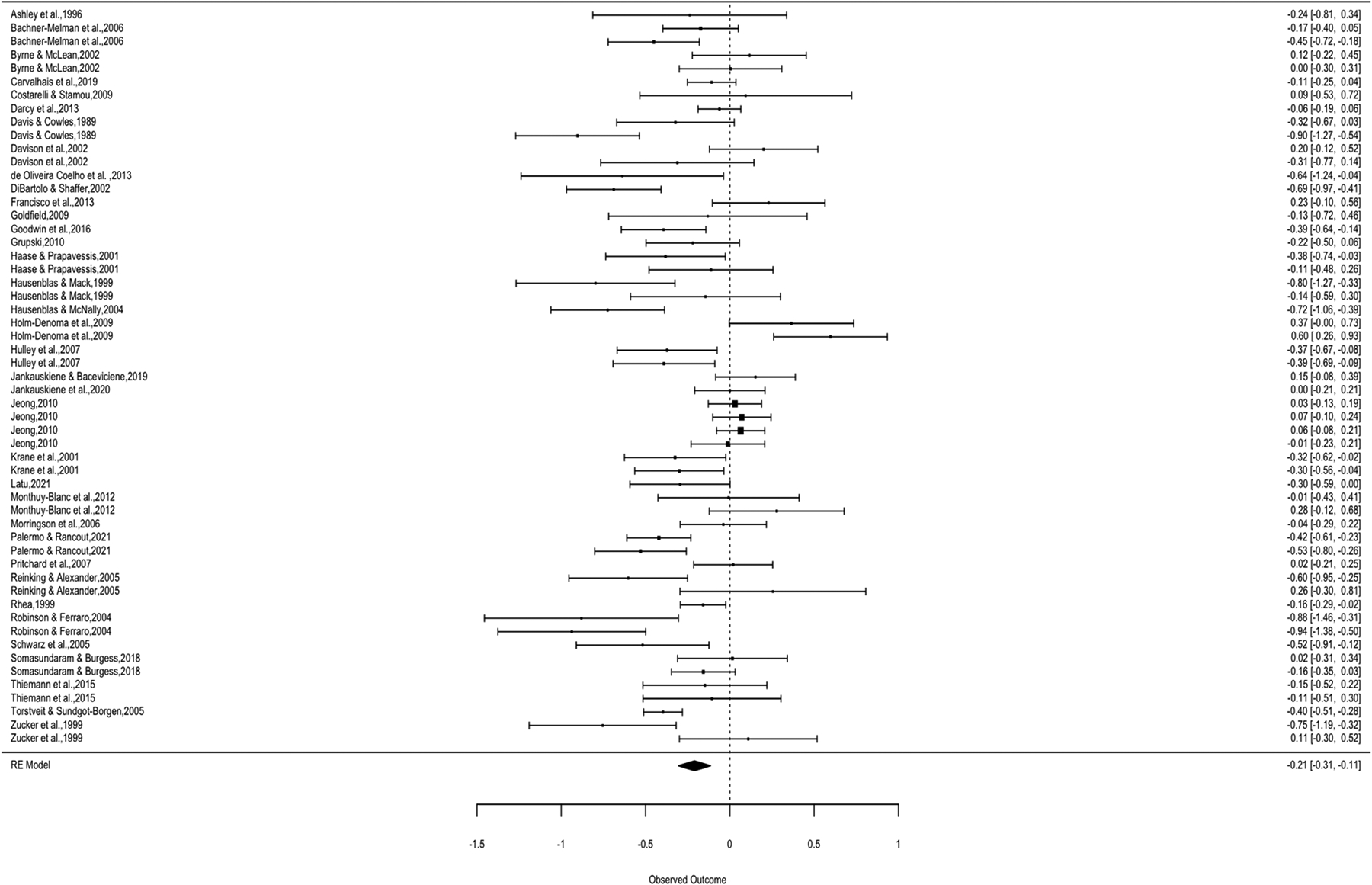
Body Dissatisfaction Forest Plot
Figure 5.
Body Dissatisfaction Funnel Plot
We evaluated the moderating effects of sport type (aesthetic/lean vs. non-aesthetic/non-lean), age, sport level (elite/expert vs. collegiate vs. high school/club), and nationality (western country vs. non-western country). Sport type was a significant moderator, F(2, 51) = 5.806, p = .005, of body dissatisfaction differences between athletes and non-athletes, such that effect sizes were larger in studies with aesthetic/lean sports. The average effect size observed in athletes participating in non-aesthetic/non-lean sports relative to non-athletes was g = −.273, 95% CI [−.433, −.112] which was significant (t = −3.408, p = .001) suggesting that athletes participating in non-aesthetic/non-lean sports reported significantly less body dissatisfaction compared to non-athletes. In studies with aesthetic/lean-sport athletes, the observed differences in body dissatisfaction between athletes and non-athletes were significantly different compared to studies with non-aesthetic/non-lean sports (t = 2.198, p = .033, g = −.094). Athletes participating in aesthetic/lean sports reported more body dissatisfaction compared to athletes participating in non-aesthetic/non-lean sports, relative to non-athletes. Participant age (F(1, 53) = 2.615, p = .112), sport level (F(3, 39) = 1.443, p = .245), and nationality (F(1, 53) = .039, p = .845) were non-significant moderators.
Drive for Thinness
There were k = 35 effect sizes used to test mean differences in drive for thinness between athletes and non-athletes. The overall effect size (g = −.066, 95% CI [−.188, .057]) was non-significant (t = −1.087, p = .285) suggesting that athletes and non-athletes reported similar levels of drive for thinness on average. There was a substantial amount of within-group heterogeneity, Q(34) = 118.678, p < .0001 (see Figure 6). An examination of a funnel plot (see Figure 7) and Begg’s test for asymmetry (tau = .045, p = .714) suggested that publication bias was unlikely.
Figure 6.
Drive for Thinness Forest Plot
Figure 7.
Drive for Thinness Funnel Plot
We evaluated the moderating effects of sport type (aesthetic/lean vs. non-aesthetic/non-lean), age, sport level (elite/expert vs. collegiate vs. high school/club), and nationality (western vs. non-western). Sport type was a significant moderator, F(2, 32) = 6.001, p = .006, of drive for thinness differences between athletes and non-athletes, such that effect sizes were larger in studies with aesthetic/lean sports.. The average effect size observed in athletes participating in non-aesthetic/non-lean sports relative to non-athletes was g = −.181, 95% CI [−.361, −.002] which was significant (t = −2.059, p = .048) suggesting that athletes participating in non-aesthetic/non-lean sports reported significantly less drive for thinness compared to non-athletes. In studies with aesthetic/lean-sport athletes, the observed differences in drive for thinness between athletes and non-athletes were significantly different compared to studies with non-aesthetic/non-lean sports (t = 3.461, p = .002, g = .166). Athletes participating in aesthetic/lean sports reported more drive for thinness compared to athletes participating in non-aesthetic/non-lean sports, relative to non-athletes. Participant age (F(1, 32) = 1.298, p = .263), sport level (F(3, 27) = 2.021, p = .135), and nationality (F(1, 33) = .025, p = .875) were non-significant moderators.
Restricting
There were k = 31 effect sizes used to test mean differences in restricting between athletes and non-athletes. The overall effect size was g = .072, 95% CI [−.101, .246] and non-significant (t = .851, p = .402) suggesting that athletes and non-athletes reported similar levels of restricting. There was a substantial amount of within-group heterogeneity, Q(30) = 215.937, p < .0001 (see Figure 8). An examination of a funnel plot (see Figure 9) and Begg’s test for asymmetry (tau = .019, p = .893) suggested that publication bias was unlikely.
Figure 8.
Restricting/Restraint Forest Plot
Figure 9.
Restricting/Restraint Funnel Plot
We evaluated the moderating effects of sport type (aesthetic/lean vs. non-aesthetic/non-lean), age, sport level (elite/expert vs. collegiate), and nationality (western country vs. non-western country). Sport type was a significant moderator, F(2, 28) = 7.444, p = .003, of restricting differences between athletes and non-athletes, such that effect sizes were larger in studies with aesthetic/lean sports.. The average effect size observed in athletes participating in non-aesthetic/non-lean sports relative to non-athletes was g = −.141, 95% CI [−.373, .092] which was not significant (t = −1.241, p = .225) suggesting that athletes participating in non-aesthetic/non-lean sports reported similar levels of restricting compared to non-athletes. In studies with aesthetic/lean-sport athletes, the observed differences in restricting between athletes and non-athletes were significantly different compared to studies with non-aesthetic/non-lean sports (t = 3.623, p = .001, g = .231). Athletes participating in aesthetic/lean sports reported more restricting compared to athletes participating in non-aesthetic/non-lean sports, relative to non-athletes. Participant age (F(1, 26) = .016, p = .899), sport level (F(2, 24) = .576, p = .57), and nationality (F(1, 29) = .748, p = .394) were non-significant moderators.
Loss-of-Control Eating/Binge Eating
There were k = 12 effect sizes used to test mean differences in loss-of-control eating or binge eating between athletes and non-athletes. The overall effect size (g = .049, 95% CI [−.184, .281]) was non-significant (t = .459, p = .656) suggesting that athletes and non-athletes reported similar levels of loss-of-control eating and binge eating. There was a substantial amount of within-group heterogeneity, Q(11) = 52.016, p < .0001 (see Figure 10). An examination of a funnel plot (see Figure 11) and Begg’s test for asymmetry (tau = .03, p = .947) suggested that publication bias was unlikely.
Figure 10.
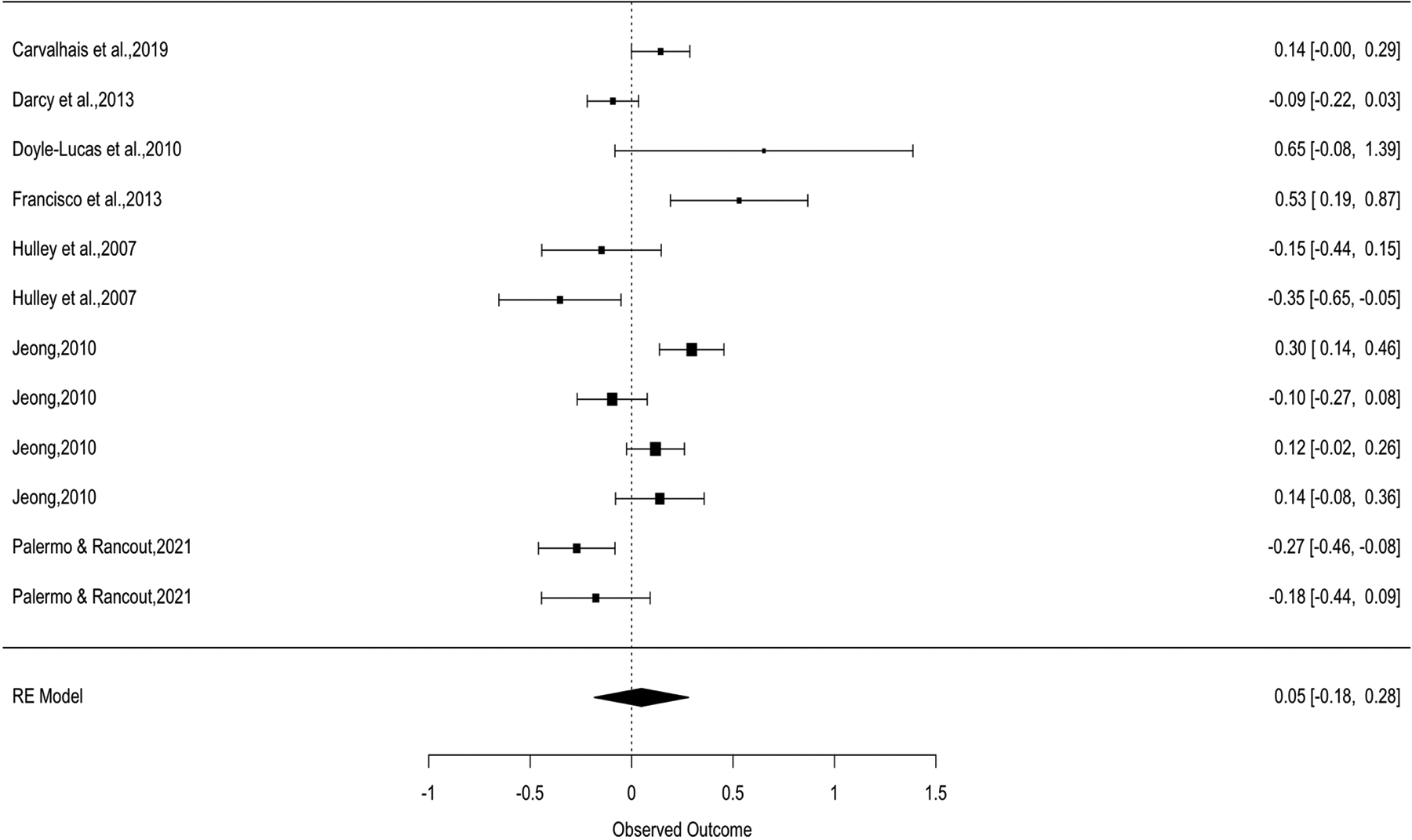
Binge Eating Forest Plot
Figure 11.
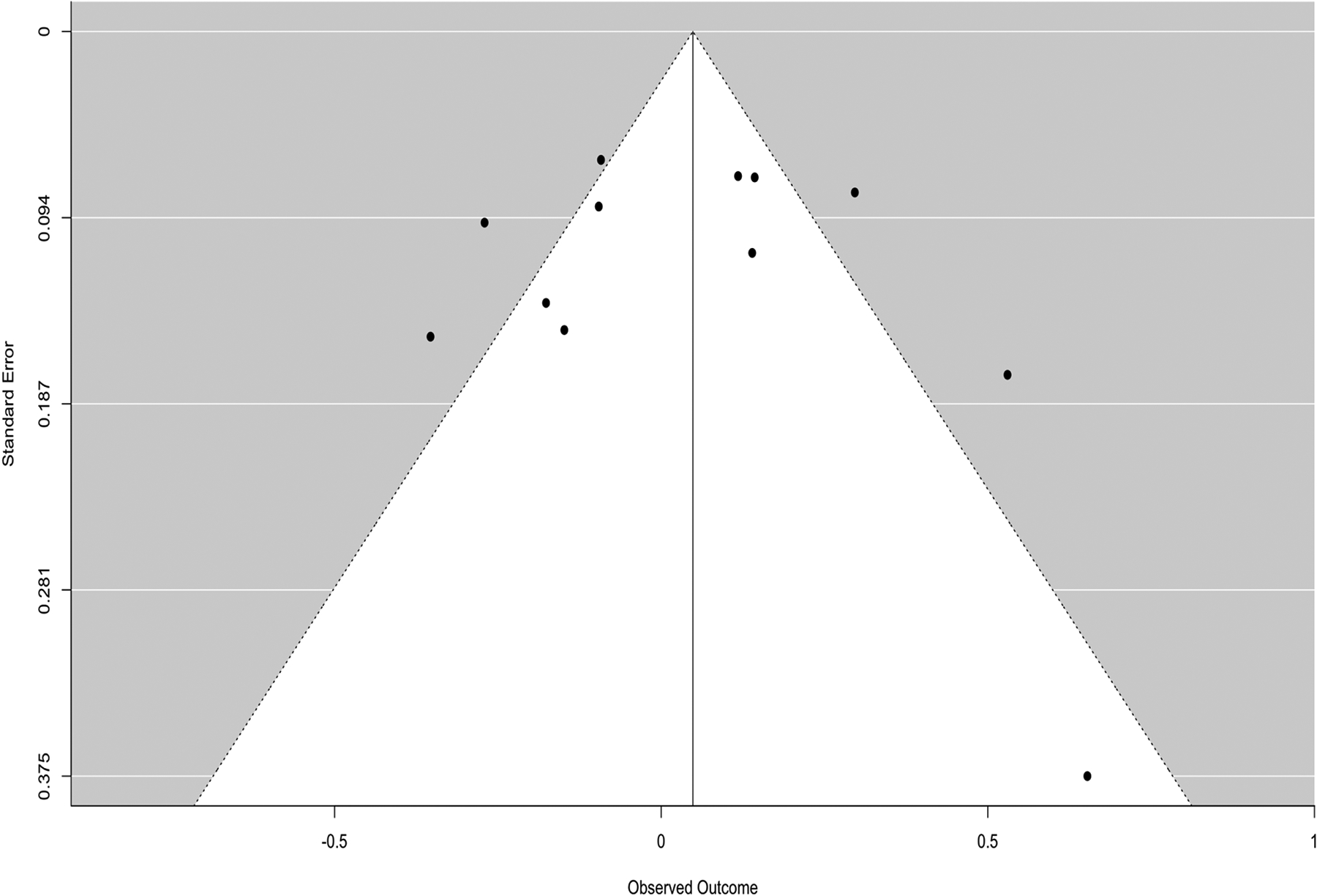
Binge Eating Funnel Plot
We evaluated the moderating effects of sport type (aesthetic/lean vs. non-aesthetic/non-lean), age, sport level (elite/expert vs. collegiate), and nationality (western country vs. non-western country). Sport type was a significant moderator, F(2, 9) = 5.901, p = .023, of loss-of-control eating differences between athletes and non-athletes, such that effect sizes were larger in studies with aesthetic/lean sports.. The average effect size observed in athletes participating in non-aesthetic/non-lean sports relative to non-athletes was g = −.218, 95% CI [−.544, .108] which was not significant (t = −1.515, p = .164) suggesting that athletes participating in non-aesthetic/non-lean sports reported similar levels of loss-of-control eating compared to non-athletes. In studies with aesthetic/lean-sport athletes, the observed differences in loss-of-control eating between athletes and non-athletes were significantly different compared to studies with non-aesthetic/non-lean sports (t = 3.388, p = .008, g = .177). Athletes participating in aesthetic/lean sports reported more loss-of-control eating and binge eating compared to athletes participating in non-aesthetic/non-lean sports, relative to non-athletes. Participant age (F(1, 10) = 2.022, p = .186), sport level (F(2, 7) = .121, p = .888), and nationality (F(1, 10) = .556, p = .473) were non-significant moderators.
Risk of Bias
Descriptive results from our JBI risk of bias assessment found that 77.2% of the included articles included adequate information describing the athlete and non-athlete groups, and 73.7% included adequate information describing the objective criteria utilized to categorize participants as athletes or non-athletes. However, only 10.5% of the papers explicitly implemented matching procedures to ensure that athletes and non-athletes were similar on demographic characteristics, and only 43.9% of the papers provided evidence for adequate internal consistency (i.e., defined as Cronbach’s alpha greater than .7) reliability for the measures used to assess ED psychopathology.
Discussion
The purpose of this paper was to provide an updated meta-analysis on mean levels of ED psychopathology among female athletes and non-athletes. First, we hypothesized that female athletes would experience more overall ED psychopathology, drive for thinness, restricting, and loss-of-control eating compared to non-athletes based on previous research (Smolak et al., 2000). Second, we hypothesized that athletes would report lower body dissatisfaction compared to non-athletes consistent with past meta-analytic reviews (Hausenblas & Downs, 2001; Smolak et al., 2000. Finally, we expected effects to be small with significant heterogeneity, and we hypothesized that mean age, sport level, and sport type would emerge as significant moderators of observed effect sizes. We expected that a greater level of ED psychopathology would be reported among athletes participating in aesthetic/lean sports (compared to non-aesthetic/non-lean sports) and athletes participating in sports at an elite/expert level (compared to lower level).
Results from our meta-analysis of 56 eligible studies (k = 208) did not support our first hypothesis. We expected that athletes would report higher mean levels of overall ED psychopathology, drive for thinness, restricting, and loss-of-control eating compared to non-athletes. However, the effect sizes testing for mean differences between athletes and non-athletes on overall ED psychopathology and specific measures of drive for thinness, restricting, and loss-of-control eating were non-significant. Similar to the small and heterogenous overall effect sizes observed in a previous meta-analysis (Smolak et al., 2000), a large amount of heterogeneity was observed in the current study.
Our second hypothesis was supported. Athletes reported less body dissatisfaction compared to non-athletes (g = −.21), similar to effects found in a meta-analysis comparing body image (g = −.27) in a mixed-sex sample of athletes (Hausenblas & Downs, 2001) and a meta-analysis (d = −.31) in female athletes (Smolak et al., 2000). A systematic review of body-image concerns among collegiate, female athletes also found that involvement in collegiate athletics provided some protection from body-image problems. However, in a study by Varnes et al. (2013), some sports (e.g., gymnastics) and competition levels (e.g., DI) had less protection from body-image concerns than other types of sports and lower levels of competition. A possible explanation for this finding may be that athletes, relative to non-athletes, may have increased appreciation for the physical functionality of their bodies (Lunde & Gattario, 2017; Soulliard et al., 2021). In turn, appreciation for what one’s body can do may serve as a protective factor that non-athletes do not necessarily experience. Consistent with the idea that participation in sports may increase appreciation for one’s body, Menzel and Levine (2011) proposed a theoretical model for the development of positive body image through engagement in embodying activities. Embodying activities are defined as activities that facilitate feelings such as competence, self-expression, and respect for one’s body. In support of Menzel and Levine’s hypothesis (2011), other studies have found that participation in a sport may protect against the development of higher body dissatisfaction (Darcy et al., 2013; Zhan et al., 2020).
Our third hypothesis was supported. Aesthetic/lean sport participation was associated with more overall ED psychopathology, drive for thinness, restricting, and loss-of-control eating compared to non-aesthetic/non-lean athletes, relative to non-athletes. Our findings are consistent with past research that found increased ED psychopathology among athletes in aesthetic/lean sports (Joy et al., 2016; Krentz & Warscburger, 2011; Krentz & Warschburger, 2013; Kong & Harris, 2015; Smolak et al., 2000; Thompson & Sherman, 2010). Results from the current study suggested that individuals who participated in aesthetic/lean sports were at increased risk compared to non-athletes for most measures of ED psychopathology, with the exception of body dissatisfaction. Increased dieting in aesthetic/lean sports may be due to the salience of weight and shape in sport culture, including conversations with coaches and teammates and the belief that smaller and lighter bodies outperform different bodies in sport. Participating in an aesthetic/lean sport also blunted certain protective factors for the development of an ED observed for athletes. For example, aesthetic/lean-sport athletes reported body dissatisfaction levels that were similar to non-athletes. The finding that sport type moderated differences in body dissatisfaction between athletes and non-athletes is similar to research studies that found evidence that athletes participating in aesthetic/lean sports may have higher levels of body dissatisfaction compared to non-aesthetic/non-lean sports (Swami et al., 2009; Varnes et al., 2013)
Contrary to our hypothesis, mean age and elite/expert athlete status did not moderate study results. We included mean age as a potential moderator due to the large age range of participants included in different studies, because some studies included young children, adolescents, adults, or mixed samples. Our findings suggest that mean differences between athletes and non-athletes on measures of ED psychopathology are similar across age groups. Status as an elite/expert athlete (i.e., athletes competing at a professional, national, or international level) also did not emerge as a moderator of our results. Thus, ED psychopathology may be mostly similar to athletes and non-athletes regardless of involvement in high-level competition. Similarly, research comparing elite and non-elite gymnasts found that organizational pressures to be thin within the gymnastics club were more predictive of ED psychopathology compared to competition level (Francisco et al., 2012). This could suggest that athletes, even at lower levels of competition, may experience pressures and personality traits that could contribute to increased or lowered risk for ED psychopathology. Overall, however, the results of our meta-analysis suggest that pressures associated with increased ED psychopathology are not directly related to the level of sport or how competitive the level is.
Results identifying aesthetic/lean sports as a significant moderator of ED psychopathology highlight that there may be some subgroups of athletes who experience higher levels of ED psychopathology compared to non-athletes. For example, we found that aesthetic/lean sport participants were more susceptible to ED psychopathology. Athletes participating in aesthetic/lean sports may benefit from increased education, prevention, and treatment efforts prior to and during sport participation. Additionally, attempting to change coaching behaviors and culture within aesthetic/lean sport organizations could be an important target. For example, Piran (1999) provided an intervention aimed at changing the coaching and staffing environment within the National Ballet of Canada, and this program led to a decrease in disordered eating among ballet students. It is important to note, however, that the standardized mean difference between athletes and non-athletes was small, even after including sport type as a moderator. Results from this meta-analysis identified small effects and large amounts of heterogeneity in standardized mean differences between athletes and non-athletes; thus, research efforts should aim to go beyond simply identifying and comparing levels of ED psychopathology between athletes and non-athletes at a cross-sectional level. Instead, athletes may be better served if future studies focus on understanding sport-related risk factors (i.e., risk factors that are specific to participating in sport) that trigger the onset of an ED or maintain a pre-existing ED in athletes using longitudinal designs. For example, Krentz et al. (2013) completed a longitudinal study in adolescent aesthetic-sport athletes; results found that a self-reported desire to be lean to improve sport performance predicted increases in disordered eating (Krentz et al., 2013). Similarly, longitudinal research identifying maintenance factors of disordered eating over time during the sport season and during off-season could further inform already promising eating-disorder intervention programs, like the Female Athlete Body Project (Gorrell et al., 2021; Stewart et al., 2019). Thus, more information about sport-related risk factors could contribute critical information to better adapt and tailor prevention and intervention efforts for the athlete community.
Several limitations of this study are worth noting. First, there was a large amount of heterogeneity that was unexplained after controlling for sport type in the meta-analytic model. This heterogeneity highlights that there may be other important moderating factors that we were unable to model in this meta-analysis (e.g., sport positions, uniforms, and person-specific factors). Within a particular sport, some positions may place a higher importance on weight-status than other positions (e.g., coxswains in rowing). There is some evidence to suggest that certain positions in sport may be at higher risk for disordered eating compared to other positions (Compte et al., 2018; Torres-McGehee et al., 2012). Uniforms vary considerably across different types of sports, ages, and levels of competition, and these differences could alter associated ED risk (Thompson & Sherman, 2014; Torres-McGehee et al., 2012). For example, volleyball, a ball-game sport that is classified as a non-aesthetic/non-lean sport, typically has more revealing uniforms in the form of spandex shorts for older female athletes and less revealing uniforms in the form of standard-sized shorts for younger athletes and in men of all ages. Person-specific factors, such as levels of perfectionism (e.g., concern over mistakes), could be important to model given the link between perfectionism and eating disorders in the general population and in athletes specifically (Bulik et al., 2003; Forsberg & Lock, 2006; Madigan et al., 2017; Thompson & Sherman, 1999).
Second, the current study was limited to females and results can only be generalizable to that group. Chapman & Woodman (2016) provide a meta-analytic review of male athletes and non-athletes. Similar to findings in Chapman & Woodman (20016), the current meta-analysis found non-significant differences in overall ED psychopathology between female athletes and female non-athletes with sport type moderating the observed mean differences between athletes and non-athletes. However, there is a considerable gap in the literature as none of the included studies seemed to include transgender athletes. Transgender athletes may be at higher risk for ED symptoms and RED-S due to the intersectionality of gender and holding an athletic identity. A case study of a person who was a distance runner and identified as a transgender male highlighted the relationship between energy availability, energy expenditure through sport, and desires to avoid menstruation and secondary sex characteristics that were inconsistent with the person’s experienced gender (Holtzman et al., 2021).
Third, the results of our meta-analysis were limited by the methods used in past research investigating ED psychopathology in athletes and non-athletes. Many studies did not report data related to the race/ethnicity and socioeconomic status of their participants. Of the available demographic information of included studies, it appeared that many studies lacked representation across race, ethnicity, and socioeconomic status. Fourth, there were few studies that assessed loss-of-control eating, purging, and compulsive/maladaptive exercise. Flatt et al. (2020) assessed differences between athletes and non-athletes on self-reported ED behavior and found that athletes reported significantly more maladaptive exercise episodes. Our study was unable to test for differences between athletes and non-athletes on maladaptive exercise because few studies included a measure of maladaptive exercise or athletic overtraining.
Fifth, the measures most frequently used, including the EAT, EDI, and the Eating Disorder Examination- Questionnaire (Fairburn & Beglin, 1994), were not created in athlete samples. Sixth, findings from this meta-analysis were based on self-report assessments. Studies using clinical interviews and diagnostic assessments among athletes suggested that athletes may underreport ED psychopathology on self-reports (Martinsen & Sundgot-Borgen, 2013; Sundgot-Borgen, 1993). There is also data to suggest that individuals may report higher levels of ED psychopathology on self-report versus a clinical interview, perhaps due to feeling less embarrassed when completing a self-report (Keel et al., 2002). If athletes do under-report ED psychopathology on self-reports, results from this study may be an underestimate of true levels of ED psychopathology in athletes. Future research on the topic of EDs in athletes and non-athletes should consider utilizing clinical interviews in addition to self-reports to assess the extent to which differences may exist between methods. Finally, only the first author entered the search terms into PubMed and PsycInfo. However, both the first and second authors independently reviewed and screened all study titles, abstracts, and articles for possible inclusion in the current meta-analysis.
Despite these limitations, the current study has several strengths. First, this study provided an updated meta-analysis on studies measuring ED psychopathology in female athletes and non-athletes over the past 20 years. Second, this study followed PRIMSA guidelines and best practices for meta-analytic reviews. Third, the current study utilized broad inclusion criteria, which increases the generalizability of our results and provides a snapshot of the relationship between sport participation and mean levels of ED psychopathology in female athletes. We included the “grey literature” by incorporating data that came from dissertation studies and data that were not published in original articles following our correspondence with authors. Fourth, the current meta-analysis explored several potential moderators to help better understand differential effects among different subgroups of female athletes.
In conclusion, this meta-analysis found that mean level differences in ED psychopathology between female athletes and non-athletes vary depending on sport type. Athletes participating in aesthetic/lean sports reported more overall ED psychopathology, drive for thinness, restricting, and loss-of-control eating compared to non-aesthetic/non-lean sports. Athletes reported significantly less body dissatisfaction compared to non-athletes, although this effect was less pronounced for individuals participating in aesthetic/lean sports. Findings from the current meta-analysis could inform future ED prevention and treatment in female athletes by highlighting subgroups of female athletes who may be at higher risk for drive for thinness, restricting, and loss-of-control eating (athletes in aesthetic/lean sports) and subgroups of female athletes who may be at lower risk for body dissatisfaction (athletes in non-asethetic/non-lean sports).
Supplementary Material
Public Significance Statement.
The current meta-analysis summarized findings from 56 studies that assessed levels of disordered eating, body dissatisfaction, dietary restricting, and loss-of-control eating in female athletes and non-athletes. Athletes reported lower levels of body dissatisfaction compared to non-athletes, highlighting that participation in sport could have some protective factors.
Athletes participating in sports that require weight categories (e.g., judo) and sports that emphasize thinness/leanness (e.g., gymnastics and distance running) had higher levels of disordered eating relative to athletes participating in other types of sports that do not emphasize thinness/leanness (e.g., volleyball and basketball).
Acknowledgments
DANC is supported by a R36 grant from NIMH (5R36MH120943). KAC and SNJ are supported by a CTSA grant from NCATS through Frontiers: University of Kansas Clinical and Translational Science Institute (#TL1TR002368). The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the NIH, NCATS, or NIMH.
Data Availability:
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- *.Abbott W, Brett A, Brownlee TE, Hammond KM, Harper LD, Naughton RJ, Anderson L, Munson EH, Sharkey JV, Randell RK, & Clifford T (2021). The prevalence of disordered eating in elite male and female soccer players. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 26(2), 491–498. 10.1007/s40519-020-00872-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arcelus J, Witcomb GL, & Mitchell A (2014). Prevalence of eating disorders amongst dancers: A systemic review and meta-analysis. European Eating Disorders Review, 22(2), 92–101. 10.1002/erv.2271 [DOI] [PubMed] [Google Scholar]
- *.Ashley CD, Smith JF, Robinson JB, & Richardson MT (1996). Disordered eating in female collegiate athletes and collegiate females in an advanced program of study: A preliminary investigation. International Journal of Sport Nutrition and Exercise Metabolism, 6(4), 391–401. 10.1123/ijsn.6.4.391 [DOI] [PubMed] [Google Scholar]
- Augusteijn HE, van Aert R, & van Assen MA (2019). The effect of publication bias on the Q test and assessment of heterogeneity. Psychological Methods, 24(1), 116–134. 10.1037/met0000197 [DOI] [PubMed] [Google Scholar]
- *.Bachner-Melman R, Zohar AH, Ebstein RP, Elizur Y, & Constantini N (2006). How anorexic-like are the symptom and personality profiles of aesthetic athletes?. Medicine &Science in Sports & Exercise, 38(4), 628–636. 10.1249/01.mss.0000210188.70295.c0 [DOI] [PubMed] [Google Scholar]
- *.Bert F, Gualano MR, Voglino G, Rossello P, Perret JP, & Siliquini R (2019). Orthorexia nervosa: A cross-sectional study among athletes competing in endurance sports in Northern Italy. PloS one, 14(8), e0221399. 10.1371/journal.pone.0221399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Brooks-Gunn J, Burrow C, & Warren MP (1988). Attitudes toward eating and body weight in different groups of female adolescent athletes. International Journal of Eating Disorders, 7(6), 749–757. https://doi.org/.1002/1098-108X(198811)7:6<749::AIDEAT2260070604>3.0.CO;2-M [Google Scholar]
- Bulik CM, Tozzi F, Anderson C, Mazzeo SE, Aggen S, & Sullivan PF (2003). The relation between eating disorders and components of perfectionism. American Journal of Psychiatry, 160(2), 366–368. 10.1176/appi.ajp.160.2.366 [DOI] [PubMed] [Google Scholar]
- *.Byrne S, & McLean N (2002). Elite athletes: Effects of the pressure to be thin. Journal of Science and Medicine in Sport, 5(2), 80–94. 10.1016/S14402440(02)80029-9 [DOI] [PubMed] [Google Scholar]
- *.Carvalhais A, Araújo J, Jorge RN, & Bø K (2019). Urinary incontinence and disordered eating in female elite athletes. Journal of Science and Medicine in Sport, 22(2), 140–144. 10.1016/j.jsams.2018.07.008 [DOI] [PubMed] [Google Scholar]
- Chapman J, & Woodman T (2016). Disordered eating in male athletes: A meta-analysis. Journal of Sports Sciences, 34(2), 101–109. 10.1080/02640414.2015.1040824 [DOI] [PubMed] [Google Scholar]
- Cohen J (1992). A power primer. Psychological Bulletin, 112(1), 155–159. 10.1037/0033-2909.112.1.155 [DOI] [PubMed] [Google Scholar]
- Compte EJ, Murray SB, Sepúlveda AR, Schweiger S, Bressan M, & Torrente F (2018). What position do you play? Eating disorder pathology among rugby players, and the understudied role of player position. International Journal of Eating Disorders, 51(8), 1015–1019. 10.1002/eat.22933 [DOI] [PubMed] [Google Scholar]
- *.Costarelli V, & Stamou D (2009). Emotional intelligence, body image and disordered eating attitudes in combat sport athletes. Journal of Exercise Science & Fitness, 7(2), 104–111. 10.1016/S1728-869X(09)60013-7 [DOI] [Google Scholar]
- *.Darcy AM, Hardy KK, Crosby RD, Lock J, & Peebles R (2013). Factor structure of the Eating Disorder Examination Questionnaire (EDE-Q) in male and female college athletes. Body Image, 10(3), 399–405. 10.1016/j.bodyim.2013.01.008 [DOI] [PubMed] [Google Scholar]
- *.Davis C, & Cowles M (1989). A comparison of weight and diet concerns and personality factors among female athletes and non-athletes. Journal of Psychosomatic Research, 33(5), 527–536. 10.1016/0022-3999(89)90060-3 [DOI] [PubMed] [Google Scholar]
- *.Davison KK, Earnest MB, & Birch LL (2002). Participation in aesthetic sports and girls’ weight concerns at ages 5 and 7 years. International Journal of Eating Disorders, 31(3), 312–317. 10.1002/eat.10043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Bruin AK, & Oudejans RR (2018). Athletes’ body talk: The role of contextual body image in eating disorders as seen through the eyes of elite women athletes. Journal of Clinical Sport Psychology, 12(4), 675–698. 10.1123/jcsp.2018-0047 [DOI] [Google Scholar]
- *.de Oliveira Coelho GM, de Farias MLF, de Mendonça LMC, de Mello DB, Lanzillotti HS, Ribeiro BG, & de Abreu Soares E (2013). The prevalence of from Rio de Janeiro, Brazil. Appetite, 64, 39–47. 10.1016/j.appet.2013.01.001 [DOI] [PubMed] [Google Scholar]
- *.DiBartolo PM, & Shaffer C (2002). A comparison of female college athletes and nonathletes: Eating disorder symptomatology and psychological well-being. Journal of Sport and Exercise Psychology, 24(1), 33–41. 10.1123/jsep.24.1.33 [DOI] [Google Scholar]
- *.Doyle-Lucas AF, Akers JD, & Davy BM (2010). Energetic efficiency, menstrual irregularity, and bone mineral density in elite professional female ballet dancers. Journal of Dance Medicine & Science, 14(4), 146–154. [PubMed] [Google Scholar]
- Fairburn CG, & Beglin SJ (1994). Assessment of eating disorders: Interview or self-report questionnaire?. International Journal of Eating Disorders, 16(4), 363–370. 10.1002/1098-108X(199412)16:4<363::AID-EAT2260160405>3.0.CO;2# [DOI] [PubMed] [Google Scholar]
- *.Ferrand C, Champely S, & Filaire E (2009). The role of body-esteem in predicting disordered eating symptoms: A comparison of French aesthetic athletes and non-athletic females. Psychology of Sport and Exercise, 10(3), 373–380. 10.1016/j.psychsport.2008.11.003 [DOI] [Google Scholar]
- Flatt RE, Thornton LM, Fitzsimmons-Craft EE, Balantekin KN, Smolar L, Mysko C, Wilfley DE, Taylor CB, DeFreese JD, Bardone-Cone AM, & Bulik CM (2021). Comparing eating disorder characteristics and treatment in self-identified competitive athletes and non-athletes from the National Eating Disorders Association online screening tool. International Journal of Eating Disorders, 54(3), 365–375. 10.1002/eat.23415 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forsberg S, & Lock J (2006). The relationship between perfectionism, eating disorders and athletes. Minerva Pediatr, 58, 525–536. [PubMed] [Google Scholar]
- *.Fortes LDS, Kakeshita IS, Almeida SS, Gomes AR, & Ferreira MEC (2014). Eating behaviours in youths: A comparison between female and male athletes and non athletes. Scandinavian Journal of Medicine & Science in Sports, 24(1), e62–e68. 10.1111/sms.12098 [DOI] [PubMed] [Google Scholar]
- Francisco R, Narciso I, & Alarcão M (2012). Specific predictors of disordered eating among elite and non-elite gymnast and ballet dancers. International Journal of Sport Psychology, 43, 479–502. 10.7352/IJSP2012.43.015 [DOI] [Google Scholar]
- *.Francisco R, Narciso I, & Alarcão M (2013). Parental influences on elite aesthetic athletes’ body image dissatisfaction and disordered eating. Journal of Child and Family Studies, 22(8), 1082–1091. 10.1007/s10964-006-9159-x [DOI] [Google Scholar]
- *.Gaines SA, & Burnett TBS (2014). Perceptions of eating behaviors, body image, and social pressures in female Division ii college athletes and non-athletes. Journal of Sport Behavior, 37(4), 351–369. [Google Scholar]
- Galli N, Petrie T, & Chatterton J (2017). Team weigh-ins and self-weighing: Relations to body-related perceptions and disordered eating in collegiate male athletes. Psychology of Sport and Exercise, 29, 51–55. 10.1016/j.psychsport.2016.12.004 [DOI] [Google Scholar]
- Garner DM (1991). Eating disorder inventory-2 (pp. 48–48). Odessa, FL: Psychological Assessment Resources. [Google Scholar]
- Garner DM, & Garfinkel PE (1979). The Eating Attitudes Test: An index of the symptoms of anorexia nervosa. Psychological Medicine, 9(2), 273–279. 10.1017/s0033291700030762 [DOI] [PubMed] [Google Scholar]
- *.Goldfield GS (2009). Body image, disordered eating and anabolic steroid use in female bodybuilders. Eating Disorders, 17(3), 200–210. 10.1080/10640260902848485 [DOI] [PubMed] [Google Scholar]
- Gorrell S, Schaumberg K, Boswell JF, Hormes JM, & Anderson DA (2021). Female athlete body project intervention with professional dancers: A pilot trial. Eating Disorders, 29(1), 56–73. 10.1080/10640266.2019.1632592 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Goodwin H, Haycraft E, & Meyer C (2016). Disordered eating, compulsive exercise, and sport participation in a UK adolescent sample. European Eating Disorders Review, 24(4), 304–309. 10.1002/erv.2441 [DOI] [PubMed] [Google Scholar]
- *.Grupski A (2010). Classifying exercise activities according to motivation, self-objectification, and disordered eating: How can we target change?. (Publication No. 3392054) [Doctoral dissertation, University of Illinois at Urbana Champaign]. ProQuest Dissertations and Theses Global. [Google Scholar]
- Gurevitch J, Koricheva J, Nakagawa S, & Stewart G (2018). Meta-analysis and the science of research synthesis. Nature, 555(7695), 175–182. 10.1038/nature25753 [DOI] [PubMed] [Google Scholar]
- *.Haase AM, & Prapavessis H (2001). Social physique anxiety and eating attitudes in female athletic and non-athletic groups. Journal of Science and Medicine in Sport, 4(4), 396–405. 10.1016/S1440-2440(01)80049-9 [DOI] [PubMed] [Google Scholar]
- Hagmar M, Hirschberg AL, Berglund L, & Berglund B (2008). Special attention to the weight-control strategies employed by Olympic athletes striving for leanness is required. Clinical Journal of Sport Medicine, 18(1), 5–9. 10.1097/JSM.0b013e31804c77bd [DOI] [PubMed] [Google Scholar]
- Hausenblas HA, & Downs DS (2001). Comparison of body image between athletes and nonathletes: A meta-analytic review. Journal of Applied Sport Psychology, 13(3), 323–339. 10.1080/104132001753144437 [DOI] [Google Scholar]
- *.Hausenblas HA, & Mack DE (1999). Social physique anxiety and eating disorder correlates among female athletic and nonathletic populations. Journal of Sport Behavior, 22(4), 502–513. [Google Scholar]
- *.Hausenblas HA, & McNally KD (2004). Eating disorder prevalence and symptoms for track and field athletes and nonathletes. Journal of Applied Sport Psychology, 16(3), 274–286. 10.1080/10413200490485630 [DOI] [Google Scholar]
- Hedges LV (1981). Distribution theory for Glass’s estimator of effect size and related estimators. Journal of Educational Statistics, 6(2), 107–128. [Google Scholar]
- *.Heradstveit O, Hysing M, Nilsen SA, & Bøe T (2020). Symptoms of disordered eating and participation in individual-and team sports: A population-based study of adolescents. Eating Behaviors, 39, 101434. 10.1016/j.eatbeh.2020.101434 [DOI] [PubMed] [Google Scholar]
- *.Hoch AZ, Pajewski NM, Moraski L, Carrera GF, Wilson CR, Hoffmann RG, Schimke JE, & Gutterman DD (2009). Prevalence of the female athlete triad in high school athletes and sedentary students. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine, 19(5), 421–428. 10.1097/JSM.0b013e3181b8c136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Holm-Denoma JM, Scaringi V, Gordon KH, Van Orden KA, & Joiner TE Jr (2009). Eating disorder symptoms among undergraduate varsity athletes, club athletes, independent exercisers, and nonexercisers. International Journal of Eating Disorders, 42(1), 47–53. 10.1002/eat.20560 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holtzman B, O’Brien KH, Reece LM, & Ackerman KE (2021). Menstrual dysfunction and athletic performance in a transgender runner: A case study. Current Sports Medicine Reports, 20(11), 588–590. 10.1249/JSR.0000000000000905 [DOI] [PubMed] [Google Scholar]
- Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, & Botella J (2006). Assessing heterogeneity in meta-analysis: Q statistic or I2 index?. Psychological Methods, 11(2), 193–206. 10.1037/1082-989X.11.2.193 [DOI] [PubMed] [Google Scholar]
- *.Hulley A, Currie A, Njenga F, & Hill A (2007). Eating disorders in elite female distance runners: Effects of nationality and running environment. Psychology of Sport and Exercise, 8(4), 521–533. 10.1016/j.psychsport.2006.07.001 [DOI] [Google Scholar]
- *.Jankauskiene R, & Baceviciene M (2019). Body image and disturbed eating attitudes and behaviors in sport-involved adolescents: The role of gender and sport characteristics. Nutrients, 11(12), 3061. 10.3390/nu11123061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Jankauskiene R, Baceviciene M, & Trinkuniene L (2020). Examining body appreciation and disordered eating in adolescents of different sports practice: Cross-sectional study. International Journal of Environmental Research and Public Health, 17(11), 4044. 10.3390/ijerph17114044 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Jeong C (2010). Differentiation in eating behaviors between Korean female collegiate athletes and non-athletes. (Publication No. 3413898) [Doctoral dissertation, Purdue University]. ProQuest Dissertations and Theses Global. [Google Scholar]
- Joanna Briggs Institute. (2017). The Joanna Briggs Institute Critical Appraisal Tools for Use in JBI Systematic Reviews Checklist for Analytical Cross Sectional Studies. North Adelaide, Australia, The Joanna Briggs Institute. [Google Scholar]
- Joy E, Kussman A, & Nattiv A (2016). 2016 update on eating disorders in athletes: A comprehensive narrative review with a focus on clinical assessment and management. British Journal of Sports Medicine, 50(3), 154–162. 10.1136/bjsports-2015-095735 [DOI] [PubMed] [Google Scholar]
- Keel PK, Crow S, Davis TL, & Mitchell JE (2002). Assessment of eating disorders: Comparison of interview and questionnaire data from a long-term follow-up study of bulimia nervosa. Journal of Psychosomatic Research, 53(5), 1043–1047. 10.1016/S0022-3999(02)00491-9 [DOI] [PubMed] [Google Scholar]
- *.Kong P, & Harris LM (2015). The sporting body: Body image and eating disorder symptomatology among female athletes from leanness focused and nonleanness focused sports. The Journal of Psychology, 149(2), 141–160. 10.1080/00223980.2013.846291 [DOI] [PubMed] [Google Scholar]
- *.Krane V, Stiles-Shipley JA, Waldron J, & Michalenok J (2001). Relationships among body satisfaction, social physique anxiety, and eating behaviors in female athletes and exercisers. Journal of Sport Behavior, 24(3), 247–264. [Google Scholar]
- Krentz EM, & Warschburger P (2011). Sports-related correlates of disordered eating in aesthetic sports. Psychology of Sport and Exercise, 12(4), 375–382. 10.1016/j.psychsport.2011.03.004 [DOI] [Google Scholar]
- Krentz EM, & Warschburger P (2013). A longitudinal investigation of sports-related risk factors for disordered eating in aesthetic sports. Scandinavian Journal of Medicine & Science in Sports, 23(3), 303–310. 10.1111/j.1600-0838.2011.01380.x [DOI] [PubMed] [Google Scholar]
- *.Latu JR (2021). Psychological Characteristics of Female Competitive Crossfit Athletes [Doctoral dissertation, Alliant International University; ]. ProQuest Dissertations and Theses Global. [Google Scholar]
- Lunde C, & Gattario KH (2017). Performance or appearance? Young female sport participants’ body negotiations. Body Image, 21, 81–89. 10.1016/j.bodyim.2017.03.001 [DOI] [PubMed] [Google Scholar]
- Madigan DJ, Stoeber J, & Passfield L (2017). Athletes’ perfectionism and reasons for training: Perfectionistic concerns predict training for weight control. Personality and Individual Differences, 115, 133–136. 10.1016/j.paid.2016.03.034 [DOI] [Google Scholar]
- Martinsen M, & Sundgot-Borgen J (2013). Higher prevalence of eating disorders among adolescent elite athletes than controls. Medicine & Science in Sports & Exercise, 45(6), 1188–1197. 10.1249/MSS.0b013e318281a939 [DOI] [PubMed] [Google Scholar]
- Martinsen M, Bratland-Sanda S, Eriksson AK, & Sundgot-Borgen J (2010). Dieting to win or to be thin? A study of dieting and disordered eating among adolescent elite athletes and non-athlete controls. British Journal of Sports Medicine, 44(1), 70–76. 10.1136/bjsm.2009.068668 [DOI] [PubMed] [Google Scholar]
- *.Mathisen TF, Heia J, Raustøl M, Sandeggen M, Fjellestad I, & Sundgot-Borgen J (2020). Physical health and symptoms of relative energy deficiency in female fitness athletes. Scandinavian Journal of Medicine & Science in Sports, 30(1), 135–147. 10.1111/sms.13568 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mehler PS, Birmingham LC, Crow SJ, & Jahraus JP (2010). Medical complications of eating disorders. The treatment of eating disorders: A clinical handbook (p. 66–80). New York, NY: The Guilford Press. [Google Scholar]
- Menzel JE, & Levine MP (2011). Embodying experiences and the promotion of positive body image: The example of competitive athletics. In Calogero RM, Tantleff-Dunn S, & Thompson JK (Eds.), Self-objectification in women: Causes, consequences, and counteractions (pp. 163–186). American Psychological Association. 10.1037/12304-008 [DOI] [Google Scholar]
- *.Michou M, & Costarelli V (2011). Disordered eating attitudes in relation to anxiety levels, self-esteem and body image in female basketball players. Journal of Exercise Science & Fitness, 9(2), 109–115. 10.1016/S1728-869X(12)60006-9 [DOI] [Google Scholar]
- Moher D, Liberati A, Tetzlaff J, Altman DG, & Group TP (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Annals of Internal Medicine, 151(4), 264–269. 10.7326/0003-4819-151-4-200908180-00135 [DOI] [PubMed] [Google Scholar]
- *.Monthuy-Blanc J, Maïano C, Morin AJ, & Stephan Y (2012). Physical self-concept and disturbed eating attitudes and behaviors in French athlete and non-athlete adolescent girls: Direct and indirect relations. Body Image, 9(3), 373–380. 10.1016/j.bodyim.2012.04.005 [DOI] [PubMed] [Google Scholar]
- *.Morrison CD (2006). The impact of sport involvement on adolescent girls’ body image (Publication No. 3209635) [Doctoral dissertation, Alliant International University, Fresno; ]. ProQuest Dissertations and Theses Global. [Google Scholar]
- Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, Lebrun C, Lundy B, Melin A, Meyer NL, Sherman R, Tenforde AS, Torstveit MK, & Budgett R (2018). IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. British Journal of Sports Medicine, 52(11), 687–697. 10.1136/bjsports-2018-099193 [DOI] [PubMed] [Google Scholar]
- *.Muia EN, Wright HH, Onywera VO, & Kuria EN (2016). Adolescent elite Kenyan runners are at risk for energy deficiency, menstrual dysfunction and disordered eating. Journal of Sports Sciences, 34(7), 598–606. [DOI] [PubMed] [Google Scholar]
- *.Okano G, Holmes RA, Mu Z, Yang P, Lin Z, & Nakai Y (2005). Disordered eating in Japanese and Chinese female runners, rhythmic gymnasts and gymnasts. International Journal of Sports Medicine, 26(06), 486–491. 10.1055/s-2004-821058 [DOI] [PubMed] [Google Scholar]
- *.Özdengül F, Yargic MP, Solak R, Yaylali O, & Kurklu GB (2021). Assessment of orthorexia nervosa via ORTO-R scores of Turkish recreational and competitive athletes and sedentary individuals: A cross-sectional questionnaire study. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 26(4), 1111–1118. 10.1007/s40519-020-01006-2 [DOI] [PubMed] [Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, … Moher D (2021). The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. International Journal of Surgery, 88, 105906. 10.1016/j.ijsu.2021.105906 [DOI] [PubMed] [Google Scholar]
- *.Palermo M, & Rancourt D (2021). Understanding athletic and exercise identity in relation to disordered eating behaviors. Eating and Weight Disorders-Studies on Anorexia, Bulimia and Obesity, 26(7), 2301–2308. 10.1007/s40519-020-01092-2 [DOI] [PubMed] [Google Scholar]
- *.Petisco-Rodríguez C, Sánchez-Sánchez LC, Fernández-García R, Sánchez-Sánchez J, & García-Montes JM (2020). Disordered eating attitudes, anxiety, self-esteem and perfectionism in young athletes and non-athletes. International Journal of Environmental Research and Public Health, 17(18), 6754. 10.3390/ijerph17186754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piran N (1999). Eating disorders: A trial of prevention in a high risk school setting. Journal of Primary Prevention, 20(1), 75–90. [Google Scholar]
- *.Pritchard ME, Milligan B, Elgin J, Rush P, & Shea M (2007). Comparisons of risky health behaviors between male and female college athletes and non-athletes. Athletic Insight, 9(1), 67–78. [Google Scholar]
- *.Reinking MF, & Alexander LE (2005). Prevalence of disordered-eating behaviors in undergraduate female collegiate athletes and nonathletes. Journal of Athletic Training, 40(1), 47–51. [PMC free article] [PubMed] [Google Scholar]
- *.Rhea DJ (1999). Eating disorder behaviors of ethnically diverse urban female adolescent athletes and non-athletes. Journal of Adolescence, 22(3), 379–388. 10.1006/jado.1999.0229 [DOI] [PubMed] [Google Scholar]
- *.Robinson K, & Ferraro FR (2004). The relationship between types of female athletic participation and female body type. The Journal of Psychology, 138(2), 115–128. 10.3200/JRLP.138.2.115-128 [DOI] [PubMed] [Google Scholar]
- *.Rosendahl J, Bormann B, Aschenbrenner K, Aschenbrenner F, & Strauss B (2009). Dieting and disordered eating in German high school athletes and non-athletes. Scandinavian Journal of Medicine & Science in Sports, 19(5), 731–739. 10.1111/j.1600-0838.2008.00821.x [DOI] [PubMed] [Google Scholar]
- *.Rouveix M, Bouget M, Pannafieux C, Champely S, & Filaire E (2007). Eating attitudes, body esteem, perfectionism and anxiety of judo athletes and nonathletes. International Journal of Sports Medicine, 28(04), 340–345. 10.1055/s-2006-924334 [DOI] [PubMed] [Google Scholar]
- Scott CL, Haycraft E, & Plateau CR (2019). Teammate influences and relationship quality are associated with eating and exercise psychopathology in athletes. Appetite, 143, 104404. 10.1016/j.appet.2019.104404 [DOI] [PubMed] [Google Scholar]
- *.Schwarz HC, Gairrett RL, Aruguete MS, & Gold ES (2005). Eating attitudes, body dissatisfaction, and perfectionism in female college athletes. North American Journal of Psychology, 7(3), 345–352. [Google Scholar]
- Smink FR, Van Hoeken D, & Hoek HW (2012). Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Current Psychiatry Reports, 14(4), 406–414. 10.1007/s11920-012-0282-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smolak L, Murnen SK, & Ruble AE (2000). Female athletes and eating problems: A meta-analysis. International Journal of Eating Disorders, 27(4), 371–380. 10.1002/(SICI)1098-108X(200005)27:4<371::AID-EAT1>3.0.CO;2-Y [DOI] [PubMed] [Google Scholar]
- *.Somasundaram P, & Burgess AM (2018). The role of division iii sports participation in the relationship between perfectionism and disordered eating symptomology. Journal of Clinical Sport Psychology, 12(1), 57–74. 10.1123/jcsp.2017-0013 [DOI] [Google Scholar]
- Soulliard ZA, Fitterman-Harris HF, Perry JE, Poe LM, & Ross MJ (2021). Differences in Body Appreciation and Functionality Appreciation Outside of and Directly Following Sport Among Collegiate Student-Athletes. The Sport Psychologist, 35(4), 320–328. 10.1123/tsp.2020-0175 [DOI] [Google Scholar]
- *.Steinfeldt JA, Zakrajsek R, Carter H, & Steinfeldt MC (2011). Conformity to gender norms among female student-athletes: Implications for body image. Psychology of Men & Masculinity, 12(4), 401. 10.1037/a0023634 [DOI] [Google Scholar]
- Stewart TM, Pollard T, Hildebrandt T, Wesley NY, Kilpela LS, & Becker CB (2019). The Female Athlete Body project study: 18-month outcomes in eating disorder symptoms and risk factors. International Journal of Eating Disorders, 52(11), 1291 1300. 10.1002/eat.23145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sundgot-Borgen J, & Torstveit MK (2004). Prevalence of eating disorders in elite athletes is higher than in the general population. Clinical Journal of Sport Medicine, 14(1), 25–32. 10.1097/00042752-200401000-00005 [DOI] [PubMed] [Google Scholar]
- Swami V, Steadman L, & Tovée MJ (2009). A comparison of body size ideals, body dissatisfaction, and media influence between female track athletes, martial artists, and non-athletes. Psychology of Sport and Exercise, 10(6), 609–614. 10.1016/j.psychsport.2009.03.003 [DOI] [Google Scholar]
- Tayne S, Hrubes M, Hutchinson MR, & Mountjoy M (2019). Female athlete triad and RED-S. In Piedade S. Rocha, Imhoff A, Clatworthy M, Cohen M, Espregueira-Mendes J (Eds), The Sports Medicine Physician (pp. 395–411). Cham, Switzerland: Springer. [Google Scholar]
- *.Thiemann P, Legenbauer T, Vocks S, Platen P, Auyeung B, & Herpertz S (2015). Eating disorders and their putative risk factors among female German professional athletes. European Eating Disorders Review, 23(4), 269–276. 10.1002/erv.2360 [DOI] [PubMed] [Google Scholar]
- Thompson RA, & Sherman RT (1999). “Good athlete” traits and characteristics of anorexia nervosa: Are they similar?. Eating Disorders, 7(3), 181–190. 10.1080/10640269908249284 [DOI] [Google Scholar]
- Thompson RA, & Sherman RT (2010). Eating disorders in sport. New York, NY: Routledge. 10.4324/9780203879856 [DOI] [Google Scholar]
- Thompson RA, & Sherman R (2014). Reflections on athletes and eating disorders. Psychology of Sport and Exercise, 15(6), 729–734. 10.1016/j.psychsport.2014.06.005 [DOI] [Google Scholar]
- Torres-McGehee TM, Monsma EV, Dompier TP, & Washburn SA (2012). Eating disorder risk and the role of clothing in collegiate cheerleaders’ body images. Journal of Athletic Training, 47(5), 541–548. 10.4085/1062-6050-47.5.03 [DOI] [PMC free article] [PubMed] [Google Scholar]
- *.Torstveit MK, & Sundgot-Borgen J (2005). The female athlete triad: Are elite athletes at increased risk?. Medicine & Science in Sports & Exercise, 37(2), 184–193. 10.1249/01.MSS.0000152677.60545.3A [DOI] [PubMed] [Google Scholar]
- Varnes JR, Stellefson ML, Janelle CM, Dorman SM, Dodd V, & Miller MD (2013). A systematic review of studies comparing body image concerns among female college athletes and non-athletes, 1997–2012. Body Image, 10(4), 421–432. 10.1016/j.bodyim.2013.06.001 [DOI] [PubMed] [Google Scholar]
- Viechtbauer W (2010). Conducting meta-analyses in R with the metafor package. Journal of Statistical Software, 36(3), 1–48. [Google Scholar]
- *.Wollenberg G, Shriver LH, & Gates GE (2015). Comparison of disordered eating symptoms and emotion regulation difficulties between female college athletes and non athletes. Eating Behaviors, 18, 1–6. 10.1016/j.eatbeh.2015.03.008 [DOI] [PubMed] [Google Scholar]
- Zhan C, Heatherington L, & Klingenberg B (2020). Disordered eating- and exercise-related behaviors and cognitions during the first year college transition. Journal of American College Health, 1–12. 10.1080/07448481.2020.1775608. [DOI] [PubMed] [Google Scholar]
- *.Zucker NL, Womble LG, Mlliamson DA, & Perrin LA (1999). Protective factors for eating disorders in female college athletes. Eating Disorders, 7(3), 207–218. 10.1080/10640269908249286 [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.