

INTRODUCTION
Chronic rhinosinusitis with nasal polyps (CRSwNP) is an inflammatory disease of the nasal and paranasal sinuses that displays a predominantly type 2 inflammatory signature and is associated with a high symptom burden, poor health‐related quality of life (HRQoL), and high economic burden. 1 , 2 , 3 , 4 Dupilumab is a fully human monoclonal antibody that blocks interleukin (IL)‐4 receptor‐α, the shared receptor component for IL‐4 and IL‐13, which are key and central drivers of type 2 inflammation. In the randomized, placebo‐controlled, phase 3 SINUS‐24 (NCT02912468) and SINUS‐52 (NCT02898454) studies in adults with severe CRSwNP, dupilumab significantly improved endoscopic, radiographic, clinical, and patient‐reported symptoms as well as HRQoL, including in subgroups with prior sinonasal surgery and comorbid asthma or nonsteroidal anti‐inflammatory drug‐exacerbated respiratory disease (NSAID‐ERD). 5
To optimize shared decision‐making it is important for clinicians and patients to know when one might expect improvements in symptoms after initiating treatment and how long improvements might be expected to last. Similarly, it is important to know whether the presence of common comorbidities affects the onset of action or the magnitude and time course of treatment effects. Here, we investigate the onset of action, magnitude, and time course of treatment effects of dupilumab across CRSwNP disease measures and HRQoL in the SINUS‐24 and SINUS‐52 studies. Results are presented for all patients and for those with and without prior sinonasal surgery, asthma, NSAID‐ERD, and allergic rhinitis (AR).
PATIENTS AND METHODS
The study designs have been described. 5 In brief, eligible patients had severe CRSwNP with bilateral nasal polyp score (NPS) ≥5 (maximum 8), nasal congestion/obstruction (NC), and either loss of smell (LoS) or nasal discharge despite intranasal corticosteroids, and either systemic corticosteroids in the preceding 2 years or prior sinonasal surgery. History of surgery, asthma, NSAID‐ERD, and AR were self‐reported by patients at study entry. Dupilumab or matching placebo was administered subcutaneously every 2 weeks for 24 weeks (SINUS‐24) or 52 weeks (SINUS‐52). Patients recorded symptoms of NC, LoS, and rhinorrhea (anterior and posterior) daily using an eDiary with a score of 0−3 for each symptom. Total symptom score (TSS) was the sum of these symptom scores, with anterior and posterior rhinorrhea being averaged for a total possible score of 9. Patients also recorded peak nasal inspiratory flow (PNIF) daily. NPS, University of Pennsylvania Smell Identification Test (UPSIT; scale 0−40), and the 22‐item Sino‐Nasal Outcome Test (SNOT‐22) were assessed at scheduled clinic visits. Both studies met their primary objectives of reduction in co‐primary endpoints of NPS and NC at 24 weeks. Statistical and imputation methods have been described. 3 Data for placebo and dupilumab 300 mg once every 2 weeks (q2w) are presented from pooled SINUS‐24/SINUS‐52 studies for onset and from SINUS‐52 for results to week 52.
RESULTS
In total, 724 patients were randomized in the two trials, with mean ± standard deviation (SD) CRSwNP duration 11.0 ± 9.45 years and baseline NPS 5.97 ± 1.25, NC 2.40 ± 0.58, and LoS 2.74 ± 0.53 (Supplementary Table S1). Overall, 63% of patients had prior sinonasal surgery, 59% had comorbid asthma, 28% NSAID‐ERD, and 58% AR.
The dupilumab treatment effect was rapid, with significant improvement across all daily assessed measures within 4 days of initiating treatment: by day 3 for LoS, day 2 for NC, day 2 for TSS, and day 4 for PNIF; all p < 0.05 versus placebo (Figure 1). Onset of treatment effect with dupilumab was similar regardless of prior surgery, asthma, NSAID‐ERD, or AR (Supplementary Figures S1–S4). In clinic‐assessed measures, significant improvements versus placebo were observed at the first scheduled postbaseline assessments: week 2 in pooled studies for UPSIT (least squares [LS] mean difference vs. placebo [all patients] 5.53 (95% confidence interval [CI], 4.38–6.69); p < 0.0001), week 4 in SINUS‐52 for NPS (−1.15; 95% CI, −1.40 to −0.91; p < 0.0001), week 8 in SINUS‐24 for NPS (−1.42; 95% CI, −1.75 to −1.10; p < 0.0001), and week 8 in pooled studies for SNOT‐22 (−14.8; 95% CI, −17.4 to −12.2; p < 0.0001). Improvements with dupilumab continued and were sustained to the end of treatment in both studies (Figure 2; Supplementary Table S2). The onset of action, magnitude, and maintenance of treatment effect were similar regardless of prior surgery, or comorbid asthma, NSAID‐ERD, or AR.
FIGURE 1.
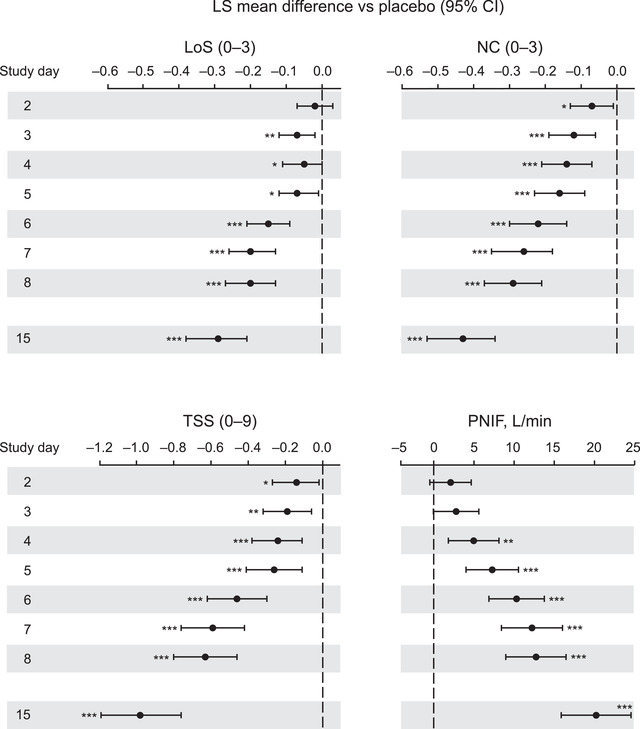
Treatment effect of dupilumab versus placebo in daily‐assessed symptoms of CRSwNP over the first dosage interval (2 weeks; SINUS‐24 and SINUS‐52 pooled). Nominal p value versus placebo: *p <0.05, **p <0.01, ***p <0.001. LoS and NC were scored on a scale of 0−3 with 0 = no symptom and 3 = severe symptom. TSS was the sum of symptom scores for LoS, NC, and rhinorrhea. Each of the imputed complete data were analyzed by fitting an ANCOVA model with the corresponding baseline value, treatment group, asthma/NSAID‐ERD status, prior surgery history, region, and study indicator as covariates. Abbreviations: ANCOVA, analysis of covariance; CRSwNP, chronic rhinosinusitis with nasal polyps; LoS, loss of smell; NC, nasal congestion; NSAID‐ERD, nonsteroidal anti‐inflammatory drug‐exacerbated respiratory disease; PNIF, peak nasal inspiratory flow; TSS, total symptom score
FIGURE 2.
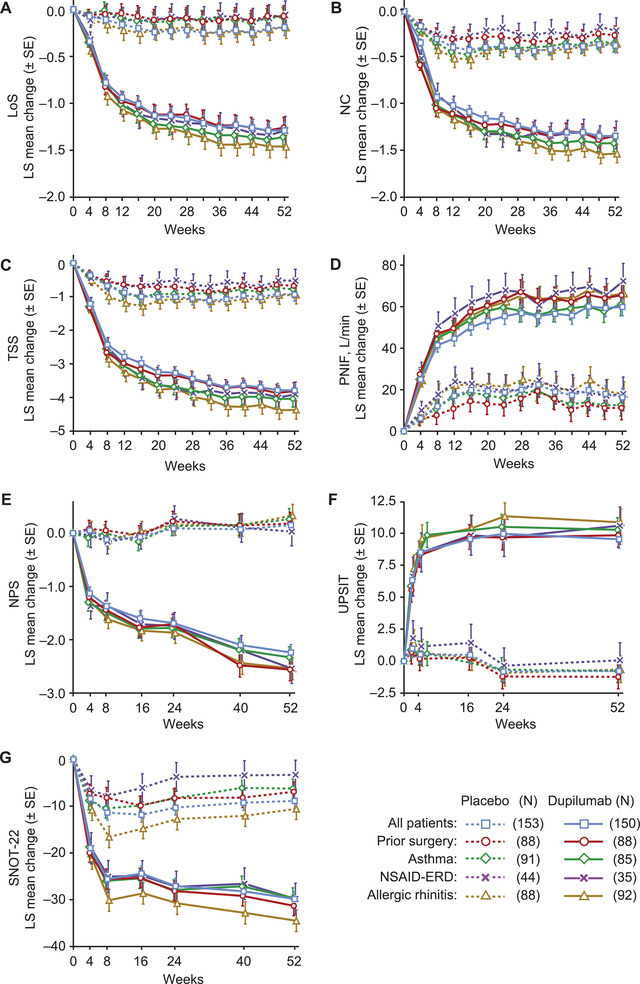
LS mean change in CRSwNP disease measures to week 52 in SINUS‐52 in all patients and in subgroups with prior surgery, asthma, NSAID‐ERD, and allergic rhinitis: (A) LoS†, (B) NC†, (C) TSS†, (D) PNIF†, (E) NPS, (F) UPSIT, and (G) SNOT‐22 total score. †Data points are monthly averages (mean of the previous 28 days). Each of the imputed complete data was analyzed by fitting an ANCOVA model with the corresponding baseline value, treatment group, asthma/NSAID‐ERD status, prior surgery history, region, and study indicator as covariates. Abbreviations: ANCOVA, analysis of covariance; CRSwNP, chronic rhinosinusitis with nasal polyps; LoS, loss of smell; LS, least squares; NC, nasal congestion; NSAID‐ERD, nonsteroidal anti‐inflammatory drug‐exacerbated respiratory disease; PNIF, peak nasal inspiratory flow; SNOT‐22, 22‐item Sino‐Nasal Outcome Test; TSS, total symptom score
DISCUSSION
Rapid onset of effect is an important feature of treatment, providing early symptom relief to patients and assurance to their physicians that the treatment is effective. This report shows that dupilumab treatment was associated with rapid onset of improvement in CRSwNP across multiple outcomes in a population with an average disease duration of 11 years. Onset of symptom improvement was similar in patients with prior sinonasal surgery, asthma, NSAID‐ERD, and AR, who may have more severe disease and be more difficult to treat. In SINUS‐52, improvements with dupilumab were sustained up to week 52 across all outcome measures regardless of prior sinonasal surgery, asthma, NSAID‐ERD, or AR. Notably, no plateau of treatment effect was observed up to week 52 in LoS, NC, TSS, PNIF, NPS, and SNOT‐22, which suggests that 52 weeks of follow‐up may not capture the full potential treatment effect.
Limitations of this study include that it was a post hoc analysis and that ascertainment of comorbidities was based on patient‐reported medical history rather than documented physician diagnosis. It should be noted that the rapid improvements shown here are mean group values that do not provide information on the percentage of patients achieving a threshold of response. Responder analyses are reported elsewhere. 5 , 6 Assessment of response with biologic therapies for CRSwNP is recommended after 6 months in European Forum for Research and Education in Allergy and Airway Diseases (EUFOREA) guidance and after 16 weeks in European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) guidance. 7 , 8
In conclusion, dupilumab produced rapid and sustained improvements in the co‐primary and secondary outcome measures of CRSwNP in SINUS‐24 and SINUS‐52, with improvements versus placebo observed as early as the second day of treatment and sustained over 52 weeks of treatment. Rapid and sustained improvement was observed irrespective of prior sinonasal surgery, comorbid asthma, NSAID‐ERD, or AR.
AUTHOR CONTRIBUTIONS
Peter W. Hellings acquired data; all authors contributed to the conception and design of the study and participated in the interpretation of the data, provided critical feedback and final approval for submission, and took responsibility for the accuracy, completeness, and protocol adherence of data and analyses.
CONFLICT OF INTERESTS
Peter W. Hellings: Regeneron Pharmaceuticals, Inc., Sanofi – advisory board member. Anju T. Peters: Regeneron Pharmaceuticals, Inc., Sanofi – advisory board member; AstraZeneca – research support and advisory board member; Optinose – consultant and research support. Adam M. Chaker: Technical University Munich (TUM) – research/clinical study grants: ALK Abello, Allergopharma, ASIT Biotech, AstraZeneca, Bencard/Allergen Therapeutics, European Institute of Technology (EIT), GlaxoSmithKline, LETI, Roche; ALK Abello, AstraZeneca, Bencart/Allergen Therapeutics, GlaxoSmithKline, Immunotek, LETI, Lofarma, Novartis, Regeneron Pharmaceuticals, Inc., Sanofi‐Genzyme, Zeller advisory board member and/or speaker – all via TUM. Enrico Heffler: AstraZeneca, GlaxoSmithKline, Novartis, Sanofi – advisory board member. Yamo Deniz, Scott Nash, Shahid Siddiqui, and Haixin Zhang: Regeneron Pharmaceuticals, Inc. – employees, may hold stock and/or stock options in the company. Asif H. Khan, Juby A. Jacob‐Nara, Amy Praestgaard, and Paul J. Rowe: Sanofi – employees, may hold stock and/or stock options in the company.
Supporting information
Supplementary information
ACKNOWLEDGMENTS
We thank Matt Lewis, PhD, of Adelphi Group, Macclesfield, UK, for medical writing/editorial assistance funded by Sanofi‐Genzyme and Regeneron Pharmaceuticals, Inc., in accordance with Good Publications Practice (GPP3) guidelines.
Hellings PW, Peters AT, Chaker AM, et al. Rapid and sustained effects of dupilumab in severe chronic rhinosinusitis with nasal polyps. Int Forum Allergy Rhinol. 2022;12:958–962. 10.1002/alr.22944
Funding information
Research sponsored by Sanofi and Regeneron Pharmaceuticals, Inc. ClinicalTrials.gov Identifiers: NCT02912468 (SINUS‐24) and NCT02898454 (SINUS‐52).
REFERENCES
- 1. Khan A, Vandeplas G, Huynh TMT, et al. The Global Allergy and Asthma European Network (GALEN rhinosinusitis cohort: a large European cross‐sectional study of chronic rhinosinusitis patients with and without nasal polyps. Rhinology. 2019;57:32–42. [DOI] [PubMed] [Google Scholar]
- 2. Bachert C, Bhattacharyya N, Desrosiers M, Khan AH. Burden of disease in chronic rhinosinusitis with nasal polyps. J Asthma Allergy. 2021;14:127–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Khan A, Huynh TMT, Vandeplas G, et al. The GALEN rhinosinusitis cohort: chronic rhinosinusitis with nasal polyps affects health‐related quality of life. Rhinology. 2019;57:343–351. [DOI] [PubMed] [Google Scholar]
- 4. Bhattacharyya N, Villeneuve S, Joish VN, et al. Cost burden and resource utilization in patients with chronic rhinosinusitis and nasal polyps. Laryngoscope. 2019;129:1969–1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bachert C, Han JK, Desrosiers M, et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS‐24 and LIBERTY NP SINUS‐52): results from two multicentre, randomised, double‐blind, placebo‐controlled, parallel‐group phase 3 trials. Lancet. 2019;394:1638–1650. [DOI] [PubMed] [Google Scholar]
- 6. Chuang CC, Guillemin I, Bachert C, et al. Dupilumab in CRSwNP: responder analysis using clinically meaningful efficacy outcome thresholds. Laryngoscope. Published online November 24, 2021. 10.1002/lary.29911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bachert C, Han JK, Wagenmann M, et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: definitions and management. J Allergy Clin Immunol. 2021;147:29–36. [DOI] [PubMed] [Google Scholar]
- 8. Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary information