An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
. 2021 May 1;2021:205.
Improvements in Air Quality and Health Outcomes Among California Medicaid Enrollees Due to Goods Movement Actions
Improvements in Air Quality and Health Outcomes Due to Goods Movement Actions in California
This Statement, prepared by the Health Effects Institute, summarizes a research project funded by HEI and conducted by Dr. Ying-Ying Meng at the University of California, Los Angeles, and colleagues. Research Report 205 contains both the detailed Investigators’ Report and a Commentary on the study prepared by the Institute’s Review Committee.
The 2006 California Goods Movement Plan sought to decrease emissions related to the movement of goods through ports and highways via numerous mandatory and voluntary actions.
This cohort study examined the impact of the plan on air quality and healthcare utilization among 23,000 adults with chronic health conditions who were continuously enrolled in Medi-Cal, a low-income healthcare program.
To disentangle the impact of this plan from other simultaneous emissions regulations, investigators compared changes from the pre-policy period (2004–2007) to the post-policy period (2008–2010) in three areas based on proximity to major goods movement transit routes: areas near ports and freeways with truck traffic, near freeways without truck traffic, and control areas.
Larger improvements in nitrogen dioxide (-2.43 ppb) and fine particulate matter (-1.58 μg/m3) exposures were observed near ports and truck-permitted freeways versus control areas during the first-year post-policy compared with pre-policy years.
Greater reductions in emergency room visits were observed among Medi-Cal beneficiaries with asthma (-170 per 1,000 beneficiaries per year) or COPD (-180 per 1,000 beneficiaries per year) who lived near ports and freeways with truck traffic versus control areas three years post-policy compared with pre-policy years.
Results from this study demonstrated that actions to reduce emissions related to goods movement may be effective in improving local air quality levels and healthcare utilization among disadvantaged people.
BACKGROUND
Air pollution accountability research evaluates the extent to which policies aimed at improving air quality produce the intended reductions in pollutant concentrations and improvements to public health. A major challenge in this research field is isolating improvements that can be attributed to the policy in question from improvements that may be due to other unrelated regulations or secular trends. This is a particular concern when policies target numerous pollutant sources, affect large geographical regions, and take several years to fully implement.
Dr. Ying-Ying Meng of the University of California, Los Angeles, and colleagues proposed to evaluate one such policy, the 2006 Emission Reduction Plan for Ports and Goods Movement in California (herein referred to as “Goods Movement Plan”). This complex set of regulations and voluntary actions targeted emissions from various marine as well as on-road and off-road vehicles used to transport traded goods into, out of, and across the entire state of California, and was implemented over several years. They assessed whether this policy resulted in reduced ambient concentrations of three air pollutants and decreased emergency healthcare utilization. To help isolate reductions attributable to this policy alone, the investigators devised exposure groupings based on proximity to goods-movement-related traffic corridors versus other traffic areas.
APPROACH
Meng and colleagues implemented a quasi-experimental design to study the effects of the Goods Movement Plan on air quality and health outcomes. They focused on vulnerable populations living within 10 California counties that contained dense urban areas and three major ports. Specifically, they studied an existing cohort of adult Medi-Cal beneficiaries (California’s Medicaid healthcare program for low-income individuals) with at least one of the following chronic conditions: asthma, chronic obstructive pulmonary disease (COPD), diabetes, and heart disease. The analysis was limited to 23,000 beneficiaries with continuous Medi-Cal enrollment during the study period.
The investigators examined three air pollutants directly and indirectly targeted by the plan, including nitrogen dioxide (NO2), fine particulate matter (PM2.5), and ozone (O3). Using EPA and supplemental air quality monitoring data, they first estimated annual exposure levels to these pollutants based on the home address of each beneficiary. Addresses were further assigned to three categories based on proximity to three traffic zones: (1) goods movement corridors — areas within 500 m of ports or freeways where trucks were allowed; (2) non-goods movement corridors — areas within 500 m of truck-prohibited freeways or within 300 m of freeway-connecting roads; and (3) control areas, which included all other areas away from the goods and non-goods movement corridors in the studied counties.
Meng and colleagues used these traffic zones to evaluate whether air quality and health outcomes had improved more in the areas with major truck traffic where the Goods Movement Plan was expected to have greater impacts. By comparing the three areas, they hoped to tease out the specific effects of the Goods Movement Plan compared with other regional and national regulations aimed at traffic-related pollution from cars, or that may have been due to other factors leading to reduced emissions of pollutants.
Changes in air pollutant exposure levels among those living in the three zones were compared between the pre-policy period (2004–2007) and the post-policy period (2008–2010) using difference-indifferences regression, a method commonly used for observational research on policy-related interventions to mimic experimental designs. In addition, Meng and colleagues used the difference-in-differences approach to examine subsequent changes in healthcare utilization among the Medi-Cal beneficiaries to assess whether the policy-related air quality improvements were effective in improving health. They adjusted the analysis for numerous individual-level health risk factors, neighborhood-level socioeconomic factors, and census-tract-level economic indicators to account for the 2008 global recession, both at baseline and over time. Ninety-five percent confidence intervals (95% CIs) were reported. The investigators hypothesized that compared with control areas, reductions in the selected air pollutants and healthcare utilization would be greatest in goods movement corridors that were targeted by the policy actions, followed by non-goods movement corridors, which may have shown improvements due to more general statewide and national air pollution regulations.
KEY RESULTS AND INTERPRETATION
Compared with the pre-policy period, Meng and colleagues reported statistically significant reductions in NO2 and PM2.5 concentrations across all 10 counties in the post-policy period. Results from the difference-in-differences analyses showed the greatest reductions in NO2 and PM2.5 when comparing goods movement to control areas for all beneficiaries and among those with each chronic condition. For example, among beneficiaries with asthma, NO2 and PM2.5 exposures were 2.43 ppb (95% CI = -2.51, -2.34) and 1.58 μg/m3 (95% CI = -1.63, -1.52) lower, respectively, for those living in the goods movement versus control areas in the first-year post-policy compared with average levels in pre-policy years. Similar, but smaller, reductions in NO2 and PM2.5 were observed when comparing non-goods movement to control areas, with the smallest reductions observed when comparing goods movement areas to non-goods movement areas. In contrast, O3 concentrations demonstrated the opposite trend during the post-policy period, which is consistent with the known inverse relationship between O3 and NO2 concentrations. The largest changes for all three pollutants were observed in the first year of the post-policy period.
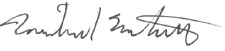
Investigators reported statistically significantly greater improvements in health outcomes for Medi-Cal beneficiaries suffering from respiratory-related chronic conditions who were living in goods movement and non-goods movement corridors when compared with control areas. For example, the number of emergency visits among the 8,636 beneficiaries with asthma (Statement Figure) and 8,900 beneficiaries with COPD was reduced by 170 (95% CI = -290, -50) and 180 (95% CI = -300, -50) visits per 1,000 beneficiaries per year, respectively, in the goods movement areas compared with control in the third year following the goods movement policy actions. Post-policy reductions in emergency room visits among all beneficiaries and among beneficiaries with either diabetes or heart disease were not significantly different for goods movement and non-goods movement corridors when compared with controls, however. There were also no significant differences in emergency visits (for all causes, asthma, COPD, diabetes, or heart disease) among any of the beneficiary groups living in goods movement compared with non-goods movement corridors. Investigators reported that the difference-indifferences estimates for hospitalizations showed a downward trend in the post-policy period but were not significantly different for those living in goods and non-goods movement corridors versus controls.
Average number of emergency room visits among Medi-Cal beneficiaries with asthma before and after policy implementation in 2007. Reductions were greater for goods movement corridors compared with control areas and were related to reductions in exposure to NO2. The counterfactual line shows the expected trend if the Goods Movement Plan had not been implemented. (Adapted from Figure 5 in Investigators’ Report.)
HEI REVIEW COMMITTEE EVALUATION
In its independent evaluation of the study, the HEI Review Committee appreciated that this study used a quasi-experimental design to assess the effectiveness of the 2006 California Goods Movement Plan on air pollution and health outcomes near major ports and freeways permitting trucks. They generally agreed with the investigators that there were greater reductions in NO2 and PM2.5 levels during the post-policy period in goods movement areas compared with control areas. They also agreed that the post-policy reductions in air pollution subsequently were associated with lower emergency healthcare utilization among Medi-Cal beneficiaries with respiratory-related chronic conditions. Smaller reductions were observed when comparing non-goods movement with control areas, and the smallest reductions were observed when comparing goods movement with non-goods movement areas. Overall, the Committee found the study results to be useful and clearly presented, and they considered them to be of particular interest to policymakers who are planning goods movement policy interventions in other jurisdictions. However, the Committee thought that the investigators’ stated conclusions were too strong because the changes in health outcomes could not be definitively linked to the Goods Movement Plan since various other air pollution regulations and economic changes that happened during the same time frame could have also contributed to improvements.
The Committee noted several strengths of this study, including a robust study design that mimics a randomized trial, the use of unique datasets linking detailed air quality measurements with a large longitudinal Medi-Cal claims dataset, and exposure assessment at the individual home address level. Of note, this study targeted people who may be more vulnerable to the health effects of air pollution, a population that is often inadequately included in many other studies. The Committee also appreciated the inclusion of an intermediate non-goods movement area. This allowed the investigators to attempt to tease out the effects attributable to the Goods Movement Plan from the effects of other regional and national regulations involving vehicle emissions that would impact both the goods movement and non-goods movement corridors, but which were expected to affect the control areas to a much smaller extent. The three different traffic zones also allowed investigators to compare changes by approximate distance from goods movement traffic. In fact, the difference-in-differences results comparing these three zones were suggestive of a gradation in responses, with goods movement corridors showing the greatest improvement in air quality and healthcare utilization, a smaller improvement shown for non-goods movement corridors, and minimal or no improvement in control areas.
However, the Committee noted several limitations. First, the exclusion of beneficiaries without continuous Medi-Cal enrollment greatly reduced the sample size. Although this was necessary to ensure individuals were followed throughout the study period, the investigators did not characterize demographic differences between those excluded and the study cohort in their Investigators’ Report. Therefore, it is unclear whether findings from this study generalize to all Medi-Cal beneficiaries with chronic conditions. It is also unknown whether external secular trends, such as the 2006 diesel fuel standard change or the 2008 global economic recession may have affected the results for the goods movement, non-goods movement, and control areas differentially. Although investigators attempted to control for the 2008 recession in their statistical analysis of pollutant exposures, this information could not all be included in the health effect models. Finally, the Goods Movement Plan included many rules that took time to implement. Thus, if the Goods Movement Plan were largely responsible for air quality improvements, the Committee would have expected NO2 and PM2.5 improvements to accumulate over time. However, results showed the greatest improvements during the first-year post-policy period, with incrementally smaller improvements in the second and third years. The Committee would have preferred a more detailed interpretation of these results.
Overall, this study provided evidence that regulatory actions to limit emissions from goods-movement-related traffic may decrease emergency care utilization among disadvantaged people who live nearby, in particular among those who suffer from respiratory-related chronic conditions. Further research is needed to understand whether continued improvements are seen during the decade(s) following the start of the implementation of the Goods Movement Plan in 2006, given that it takes many years to implement such an ambitious program and that vehicle turnover is generally slow. It will also be useful to evaluate whether similar improvements are observed elsewhere when goods movement actions are implemented, targeting ports and other major distribution hubs. The most difficult and pressing challenge remains to disentangle the effects of individual regulations. Although it is useful to study the effectiveness of a broad program of regulations, such as the Goods Movement Plan, governing authorities would ultimately like to know which of the individual actions has been most effective.
Res Rep Health Eff Inst. 2021 May 1;2021:205.
Improvements in Air Quality and Health Outcomes Among California Medicaid Enrollees Due to Goods Movement Actions
1
UCLA Center for Health Policy Research, University of California, Los Angeles
2 Division of Environmental Health Sciences, School of Public Health, University of California, Berkeley
3 School of Biological and Population Health Sciences, Oregon State University, Corvallis
4 Department of Environmental Health Sciences, Fielding School of Public Health, University of California, Los Angeles
5 Center for Occupational and Environmental Health, Fielding School of Public Health, University of California, Los Angeles
This Investigators’ Report is one part of Health Effects Institute Research Report 205, which also includes a Commentary by the Review Committee and an HEI Statement about the research project. Correspondence concerning the Investigators’ Report may be addressed to Dr. Ying-Ying Meng, UCLA Center for Health Policy Research, University of California, Los Angeles, California; yymeng@ucla.edu. No potential conflict of interest was reported by the authors.
Although this document was produced with partial funding by the United States Environmental Protection Agency under Assistance Award CR– 83467701 to the Health Effects Institute, it has not been subjected to the Agency’s peer and administrative review and therefore may not necessarily reflect the views of the Agency, and no official endorsement by it should be inferred. The contents of this document also have not been reviewed by private party institutions, including those that support the Health Effects Institute; therefore, it may not reflect the views or policies of these parties, and no endorsement by them should be inferred.
In 2006, the California Air Resources Board (CARB*) and local air quality management districts implemented an Emission Reduction Plan for Ports and Goods Movement program (referred to hereinafter as GM policy actions) (CARB 2006). The GM policy actions comprise approximately 200 actions with an estimated investment value of $6 to $10 billion. These actions targeted the major sources and polluters related to goods movements, such as highways; ports and railyard trucks; ship fuel and shore power; cargo equipment; and locomotives. These actions aimed to reduce total statewide domestic GM emissions to 2001 levels or lower by the year 2010; to reduce the state-wide diesel particulate matter (DPM) health risk from GM by 85% by the year 2020; and to reduce the nitrogen oxides (NOx) emissions from international GM in the South Coast Air Basin by 30% from projected 2015 levels and 50% from projected 2020 levels. The years 2006 and 2007 marked an important milestone in starting to regulate GM polluters and adopting stricter standards for traffic-related air pollution.
This project aimed to examine the impact of the GM policy actions on reductions in ambient air pollution and subsequent improvements in health outcomes of Medi-Cal fee-for-service (FFS) beneficiaries with chronic conditions in 10 counties in California. Specifically, we examined whether the GM policy actions reduced air pollution near GMC corridors more than in control areas. We subsequently assessed whether there were greater decreases in emergency room (ER) visits and hospitalizations for enrollees with chronic conditions who lived in the GM corridors (GMCs) than for those who lived in other areas.
METHODS
The study used a quasi-experimental design. We defined areas within 500 m of truck-permitted freeways and ports as GMCs. We further defined non-goods movement corridors (NGMCs) as locations within 500 m of truck-prohibited freeways or 300 m of a connecting roadway, and areas out of GMCs and NGMCs as controls (CTRLs). We defined years 2004–2007 as the pre-policy period and years 2008–2010 as the post-policy period. We developed linear mixed-effects land use regression models and created annual air pollution surfaces for nitrogen dioxide (NO2), fine particulate matter (PM2.5 ), and ozone (O3) across California for years 2004–2010 at a spatial resolution of 30 m, then assigned them to enrollees’ home addresses.
We used a retrospective cohort of 23,000 California Medicaid (Medi-Cal) FFS adult beneficiaries living in 10 California counties with six years of data (September 1, 2004, to August 31, 2010). Cohort beneficiaries had at least one of four chronic conditions, including asthma, chronic obstructive pulmonary disease (COPD), diabetes, and heart disease.
We used a difference-in-differences (DiD) model to assess whether air pollutant concentration and health care utilization (ER visits and hospitalizations) for cohort beneficiaries declined more for those living in intervention corridors (GMCs, NGMCs) than those living in CTRLs. All the models controlled for age, sex, language spoken, race/ethnicity, number of comorbidities in baseline years, county, time-varying health indicator variables, and several neighborhood variables.
To facilitate interpretation, we calculated the DiD estimates in each of the three years after the policy intervention. The DiD was used to assess the causal impact of regulatory policy on reductions of air pollution, as well as for the improvements in health outcomes.
We explored whether improvements in health outcomes were due to the air pollution reduction by using a multilevel mediation model, in which the effect of GM actions on health outcomes was mediated through the effect of actual air pollution reductions in the post-policy years. We used the Generalized Structural Equation Models for the estimation and combined the effects of NO2 and PM2.5 in the model. To further verify the causal inferences of the GM actions on reductions of exposures and improvements in health outcomes, we performed sensitivity analyses with propensity score weighting.
RESULTS
We observed statistically significant reductions in pollutant NO2 and PM2.5 concentrations for enrollees in all 10 counties. The enrollees in GMCs experienced greater reductions in NO2 and PM2.5 from the pre- to the post-policy periods than those in CTRLs. Greater reductions were also observed among beneficiaries living in NGMCs versus those in CTRLs, but those reductions were smaller than among beneficiaries living in GMCs. For O3 concentrations, an opposite trend was observed.
Furthermore, we observed significantly greater reductions in ER visits for patients with asthma and COPD living in GMCs than those in CTRLS in the post-policy years. For example, we saw in the DiD modeling results there were 170 fewer ER visits for 1,000 beneficiaries with asthma per year in GMCs if the regionwide trend in the CTRL group was considered not related to the GM policy. Similarly, among the beneficiaries with COPD, there were 180 fewer ER visits per 1,000 patients estimated in the GMCs for the third year after the implementation of the policy.
We also observed greater reductions in ER visits among those with asthma, when comparing NGMCs with CTRLs, but reductions were smaller than comparisons between GMCs and CTRLs. The ER visits for those with COPD, diabetes, and the total sample in NGMCs also had downward trends in the post-policy year in comparison with those in CTRLs but the differences were not statistically significant; similar phenomena were also observed for the ER visits among those with diabetes and heart diseases and in the total sample when GMCs versus CTRLs and GMCs versus NGMCs were compared. Although hospitalizations also decreased more in GMCs than in NGMCs and more in NGMCs than in CTRLs in the post-policy period, results were not statistically significant.
Using the mediation models, we observed 0.129 more reductions in the expected number of ER visits among individuals with asthma for a composite reduction in one unit NO2 and one unit PM2.5 (DiD = -0.129, P < 0.05) from the pre-policy years to the post-policy years. The reductions in NO2 and PM2.5 due to policy change estimated by the mediation model are essentially the same as shown in the respective DiD models. Mediation analyses suggested that the effects of GM policy interventions on health improvements were largely due to exposure reductions. Finally, sensitivity analyses with propensity scores produced similar DiD results.
CONCLUSIONS
This project has produced empirical evidence that air pollution control actions reduced pollution exposures among disadvantaged and susceptible populations. More importantly, our findings suggest that the reductions in air pollution led to health outcome improvements among low-income people with chronic conditions. Our investigation also contributed to scientific methods for assessing the health effects of long-term, large-scale, and complex regulatory actions with routinely collected pollutants and Medi-Cal claims data. Therefore, the results strongly support both short-term and long-term efforts to improve air quality for all members of society and future studies on the impact of air pollution control policies.
INTRODUCTION
California has the world’s eighth-largest economy and is home to one of eight Americans. The state also has four major ports, with three of them among the top five in the United States. The adjacent Los Angeles and Long Beach Ports are the two busiest container ports in the United States and the fifth busiest in the world, moving more than $260 billion in goods each year. Moving these goods to and from the ports to their ultimate destinations across the United States and the world involves diesel-powered vehicles and equipment at each step of transport. Goods movement (GM) thus creates high air pollution exposures and worsens health in nearby communities, especially for those living in the state’s four “port-to-border” GM corridors, including Los Angeles–Long Beach/Inland Empire, San Francisco Bay Area, San Diego/Border, and the Central Valley. The CARB and local air quality management districts’ Emission Reduction Plan for Ports and Goods Movement program (referred to hereinafter as GM policy actions) launched in 2006 and comprises approximately 200 actions with an estimated investment of $6 to $10 billion. These actions targeted the major sources and polluters related to GM, such as highways, ports, rail-yard trucks, ship fuel, shore power, cargo equipment, and locomotives.
This project aimed to examine reductions in ambient air pollution from the implementation of the 2006 emission reduction plan and subsequent improvements in health outcomes in some 23,000 Medi-Cal FFS beneficiaries with chronic conditions — including asthma, COPD, diabetes, and heart disease (i.e., atherosclerotic heart disease, coronary artery disease, and congestive heart failure). Our project is a retrospective cohort study using six years of Medi-Cal and pharmacy claims data from September 1, 2004, to August 31, 2010, of FFS adult Medi-Cal enrollees, 22 years of age and older residing in the California counties of Los Angeles, Riverside, San Bernardino, San Diego, Alameda, San Francisco, Santa Clara, San Joaquin, Fresno, and Sacramento. This study area contains the state’s four “port-to-border” GMCs. Unlike other U.S. studies that use administrative Medicare data at the ZIP code resolution (Di et al. 2017), we were able to obtain data with the residential home address, which allowed us to estimate their fine-scale variations in pollution exposures and their closeness to GM areas. Specifically, we divided the study populations into three location categories (i.e., domains): goods movement corridors (GMCs), non-goods movement corridors (NGMCs), and control areas (CTRLs). We defined GMCs as locations within 500 m of truck-permitted freeways, or ports (HEI 2010). We defined NGMCs as locations within a 500-m buffer of a truck-prohibited roadway or within 300 m of connecting roadways. The NGMC location category provided measurements on roadways that have high impacts from traffic other than trucks, which helped us understand the policy effects on reductions of air pollution from diesel-fueled machines and vehicles. Areas outside of the two mentioned corridors served as CTRLs (measuring mainly background impact) for comparing changes in air pollutant concentrations and health effects in general. This design allowed us to ascertain whether any improvements in health outcome measures are attributable to air quality interventions related to GM regulations and not to other secular trends. For example, by comparing changes in pollutant concentrations in NGMCs versus CTRLs, we were able to identify the effects of broader mobile emission reduction policies; it also helped us account for the effects of other determinants of health outcomes in this population, such as new medications and changes in access to health care. The distribution of the three location categories is displayed in Appendix 2, Figure A2-1 (available on the HEI website). Because of time lags between the promulgation of air quality regulations and subsequent impacts on air quality and health effects, we used the end of 2007 as a cut-point for policy intervention, with 2004–2007 defined as a pre-policy period and 2008– 2010 as a post-policy period.
The impact studies that have investigated and documented the effects of regulations on reductions in air pollution and subsequent improvements in health remain limited (Boogaard et al. 2017; Burns et al. 2019; Henneman et al. 2016; Rich 2017). Due to the considerable challenges inherent in such research, most impact studies were based on “natural experiments,” not on actual targeted policies and programs nor on the consequences of shorter-term or relatively small-scale actions, such as the Dublin coal ban and traffic and pollution controls implemented during the Atlanta and Beijing Olympic Games (Binder 1983; Carle 2009; van Erp and Cohen 2009). Emerging research in the field shows that the improvements in air quality improved lung development in children (Gilliland et al. 2017), reduced ER visits (Russell et al. 2018), and mortality in Medicare populations (Di et al. 2017). However, these studies lack the specificities of a particular regulation on improving air quality and health. Some studies have contributed to statistical method development in this area (Zigler et al. 2016), but further development of appropriate epidemiological and statistical approaches remains important to support the evaluation of air quality actions.
Our investigation was one of the first studies that assess specific long-term, large scale, and complex regulatory actions. Our study also took into consideration concomitant changes in weather and population and economic factors (e.g., an economic recession). Structuring our analyses within three well-defined study areas (GMCs, NGMCs, and CTRLs) allowed us to compare concentration differences along GMCs that are mostly attributable to GM policies versus changes in concentrations that occurred on non-truck freeways (where trucks are prohibited). Those changes would most likely be attributable to broader mobile emission reduction policies versus changes in concentrations that have occurred in control areas likely due to regional emissions reductions policies.
The project was conducted in two phases. In Phase I, to adequately address possible concerns over using sparse government monitoring sites to identify GM regulation effects, we conducted two new rounds of field sampling focusing on nitrogen oxides (including NO2) in Los Angeles and Alameda counties in 2012–2013 and integrated them with government monitoring to model their greater spatiotemporal variations that cannot be typically uncovered from one type of monitoring. Using these data and previously collected Ogawa saturation monitoring data for 2004–2005 (Alameda) and 2006–2007 (Los Angeles), we identified improvements in air quality measured by NO2 and NOx concentrations in GMCs and NGMCs that were significantly greater than those in CTRLs after controlling for potential confounders such as truck/vehicle kilometers traveled, cargo volume, meteorological conditions, and other factors (Su et al. 2016). In Phase II of the project, we investigated associations of long-term (i.e., pre- and post-policy periods) and intermediate-term (e.g., annual) pollutant levels with health outcomes to determine whether regulatory actions contributed to reductions in air pollution exposures and subsequent improvements in health outcomes using the small-area variation (i.e., 30 m) exposure assessment modeling results. Similar efforts were also made on identifying whether the Medi-Cal (California’s Medicaid program) beneficiaries had greater improvements in air pollution exposures and health in GMCs and NGMCs than those in CTRLs, as well as in GMCs versus NGMCs.
We chose Medicaid beneficiaries as the study population because Medicaid is the largest provider of health insurance for low-income and minority populations and about 60% of those beneficiaries are racial/ethnic minorities. Medi-Cal health insurance is paid for with federal and state tax revenues. At the state level, the Department of Health Services administers the Medi-Cal program. In 2004, Medi-Cal program provided health care services to welfare recipients and other qualified low-income persons, primarily pregnant women and families with children, and the aged, blind, or disabled with incomes up to 133% of the poverty level. Medi-Cal is among the largest in the nation, both in terms of the number of beneficiaries and total expenditures (Legislative Analyst’s Office 2004). Medi-Cal provides health care through two basic types of payment arrangements — FFS and managed care. FFS is the traditional arrangement in which providers are paid for each examination, procedure, or other services that they provide. Beneficiaries generally obtain services from any provider who has agreed to accept Medi-Cal payments. The provider submits the claims to receive the payment for their services. Managed care is generally provided by prepaid health plans. The health plans receive monthly “capitation” payments from the Medi-Cal program for each enrollee in return for providing all of the covered care needed by those enrollees. Since payments to the plan do not vary with the amount of service provided, there are many fewer incentives for providers or health plans to submit information (or claims) on the services provided. As a result, the FFS population has more complete utilization data since all records are based on claims (Howell 1996). More than half (3.3 million of the total of 6.4 million Medi-Cal eligibles in July 2003) were enrolled in managed-care plans, but most enrolled in managed care after October 2010. In November 2010, the state extended mandatory managed care to seniors and people with disabilities enrolled in Medi-Cal.
The Medi-Cal program had a $46.6 billion budget in 2009 and 82% of those expenditures were for FFS beneficiaries. More than 36% of adult Medi-Cal beneficiaries have one or more chronic conditions. Hypertension, COPD, heart disease, and diabetes are among the 10 highest-expenditure conditions within the FFS Medi-Cal population (Asparouhov 2006). The rationale for focusing on a Medicaid population with chronic disease conditions was that they are potentially more susceptible to air pollution exposures, have worse symptoms, and therefore are more likely to need treatment. For example, individuals with COPD have been shown to be more susceptible to adverse health effects from fine particles because such particles are more likely to deposit in their lungs than in the lungs of healthy people (Kim and Kang 1997; Svartengren et al. 1991). The same phenomenon was also observed among people with asthma (Chalupa et al. 2004). In addition to being more susceptible to air pollution due to their chronic disease conditions, the Medicaid population has relatively lower socioeconomic status (SES); and low SES has shown to be more affected by pollutants due to greater vulnerability or higher exposures (Clark et al. 1999; Mortimer et al. 2002; Ostro et al. 2001; Ou et al. 2008; Perera et al. 2002). This creates two problems: socially disadvantaged groups face higher exposures and are also likely to be more susceptible to the adverse effects of air pollution due to higher rates of chronic disease, and higher levels of psychosocial stresses (Lipfert 2004; O’Neill et al. 2003; Sexton and Adgate 1999). A previous study by the principal investigator and coauthors showed that the high prevalence of frequent asthma symptoms among low-income Californians was related to both higher traffic-related pollution exposures and increased susceptibility due to differences in overall health status and access to care. Additionally, those in poverty appeared to be more strongly affected by heavy traffic near their residences than those above poverty (Meng et al. 2008). Therefore, it is expected that the Medi-Cal population with pre-existing conditions would be more responsive to air quality improvements due to their higher relative exposure reductions and higher susceptibility to adverse effects of air pollution.
SPECIFIC AIMS
In Phase I of the project, we developed annual pollutant concentration models for criteria pollutants NO2, PM2.5, and O3 across the state of California. In Phase II of the project, we developed and assigned the modeled annual concentration surfaces at a spatial resolution of 30 m for years 2004–2010 to the subjects’ home addresses to investigate associations of long-term (i.e., pre- and post-policy periods) and intermediate-term (e.g., annual) pollutant levels with health outcomes to determine whether or not regulatory actions contributed to reductions in air pollution and subsequent improvements in health outcomes. The specific aims were as follows:
Develop annual land use regression (LUR) models and associated surfaces for pollutants NO2, PM2.5, and O3 for years 2004–2010 across California at a spatial resolution of 30 m;
Assess reductions in air pollution exposure measures among Medi-Cal enrollees living in GMCs, NGMCs, and CTRLs by assigning the annual pollutant concentration measures to their home addresses and comparing the degrees of reduction in pollutant concentrations among the three location categories from the pre-policy period to the post-policy period;
Develop and evaluate measures for health effects (e.g., ER visits and hospitalizations) and time-varying confounding factors (e.g., change in disease severity) to support our proposed research;
Identify whether improvements in air quality were greater in GMCs and NGMCs than in CTRLs from the pre-policy period to the post-policy period;
Examine whether regulatory policies (GM policy actions) resulted in improvements in health outcomes, including reductions in the number of ER visits and hospitalizations among Medi-Cal beneficiaries with asthma, heart disease, COPD, and diabetes by estimating the difference-in-differences using generalized linear multilevel models;
Conduct sensitivity and verification analyses (e.g., propensity scores) and, using a multilevel mediation model, examine whether improvements in health outcomes were due to the mediation effect of regulatory policies on reductions in air pollution.
The team had obtained both Institutional Review Board approvals from the Committee for the Protection of Human Subjects under the California Health and Human Services Agency and UCLA for the study.
PART 1: GOODS MOVEMENT POLICIES AND AIR QUALITY IMPROVEMENTS
GOODS MOVEMENT ACTIONS
In 2006, CARB and local air quality management districts approved and implemented an Emission Reduction Plan for Ports and Goods Movement program (GM policy actions) (CARB 2006). The GM policy actions aimed to protect public health by cutting emissions from the big polluters in the state through five main goals:
Reduce total statewide international and domestic GM emissions to the greatest extent possible and, at a minimum, back to 2001 levels by the year 2010.
Reduce the statewide DPM health risk from international and domestic GM by 85% by the year 2020.
Reduce emissions of nitrogen oxides (NOx) from international GM in the South Coast by 30% from the projected year 2015 levels and 50% from the projected year 2020 levels based on preliminary targets for attaining federal air quality standards.
Apply the emission reduction strategies for ports and GM statewide to aid all regions in attaining air quality standards.
Make every feasible effort to reduce localized risk in communities adjacent to GM facilities as expeditiously as possible.
CARB’s pollutant reduction plan covers emissions from five major sectors associated with ports or the distribution channels of international and domestic goods, including ocean-going vessels (OGV), harbor craft (HC), cargo handling equipment (CHE), rail locomotives, and heavy-duty vehicles (HDV) (CARB 2006). The detailed strategies for emission controls are in Table 1 and summarized as follows:
Table 1.
Goods Movement Actions: Summary for Four Port-to-Border Transportation Corridors, including Los Angeles– Long Beach/Inland Empire, San Francisco Bay Area, San Diego/Border, and the Central Valleya,b
Public Health and Environmental Mitigation — Air Quality
Immediate Actions
Short-Term Actions (0–3 years)
Intermediate-Term Actions (4–10 years)
Ships
Support for ratification of MARPOL Annex 6 for international shipping.
Implement vessel speed reduction MOU in Southern California.
Abbreviations: CARB, California Air Resources Board; MARPOL, International Convention for the Prevention of Pollution from Ships; MOU, memorandum of understanding; OAL, Office of Administrative Law; SECA, sulfur emission control area; U.S. EPA, U.S. Environmental Protection Agency.
a Adapted from “Emission Reduction Plan for Ports and Goods Movement” (CARB 2006).
b “CA low sulfur diesel” is defined as an action that states that starting June 2006 in accordance with the phase-in schedule, no person shall sell, offer for sale, supply or offer for supply any vehicular diesel fuel having a sulfur content exceeding 15 parts per million by weight in California.
For OGV, the primary strategies for emission reductions are fuel switching, shore power, Port’s Environmental Ship Index Incentive Program, and Vessel Speed Reduction compliance. The International Maritime Organization North American Emission Control Areas augmented the CARB OGV Fuel Regulation by extending the compliance zone from 24 nautical miles (nm) to 200 nm from the shore. All engines for OGV continued to use fuel with 0.1% sulfur or lower and the At-Berth Regulation (i.e., requirement for ships at berth to use shore power).
For HC (e.g., tugs, ferries, and fishing vessels), the emission reductions are due to the repowering the equipment with a compliant engine that have occurred as required by the CARB Harbor Craft Regulation or funding incentives, removal of older equipment due to attrition, and more efficient operations.
For CHE, implementation of Clean Air Action Plan measures and CARB’s Cargo Handling Equipment Regulation, along with funding incentives, resulting in the replacement of older equipment with cleaner units, retrofits, and repowers, which when combined with efficiency in operations led to lower emissions.
For locomotives, the decreases in fleet-wide emissions from line-haul locomotives are due to meeting the terms of the memorandum of understanding with CARB, and the replacement of older switching locomotives with new low-emission and ultralow emission switchers.
For HDV, the implementation of the Port’s Clean Truck Program resulted in a significant turnover of older trucks to newer and cleaner trucks as compared with 2005.
These strategies have been successfully implemented and reduced pollutant emissions. The years 2006 and 2007 marked an important milestone in regulating big polluters and adopting stricter standards for traffic-related air pollution. In 2007, the 1-hour average state standard for NO2 — a traffic pollution marker (Andersen et al. 2011; Roorda Knape et al. 1999; Studnicka et al. 1997; World Health Organization 2013) — was lowered from 250 ppb to 180 ppb and a new annual average state standard was established for NO2 at 30 ppb. These efforts have led to overall emission reductions in PM, including PM2.5 and DPM, by 69%, and NOx by 50% in the Port of Los Angeles from 2005 to 2010 (Port of Los Angeles 2019). Taking the busiest port in California, the Long Beach Port, as an example, the Port exceeded the 2014 NOx mass emission reduction standard of 22% in 2010 and is more than three-quarters of the way towards meeting the 2023 NOx emission reduction standard of 59%. The primary strategies for reducing NOx emissions for the Port include Clean Air Action Plan measures, the Clean Trucks Program, the Vessel Speed Reduction Program, shore power, and the use of slide valves. In addition to these measures, CARB’s OGV shore power regulation and the implementation of more stringent NOx standards for vessels as required by the International Maritime Organization significantly helped in meeting these standards despite the increases in cargo volumes.
Based on Long Beach Port NOx emission reduction inventory between 2005 and 2010, HDV had achieved the largest emission reduction at 78%; then rail, 43%; CHE, 38%; OGV, 26%; and HC, 24%. In 2010, the Port met the 2014 diesel particulate matter (DPM) mass emission reduction standard of 72%. The DPM emission reductions are the result of the implementation of Clean Air Action Plan measures, including vessel speed reduction, shore power, and the Clean Trucks Program. CARB’s OGV marine fuel regulation, which was in effect for the full year in 2010, also contributed to the overall reduction of DPM emissions. Between 2005 and 2010, the largest DPM reductions were HDV, 90%; OGV, 72%; rail, 48%; CHE, 47%; and HC, 22% (Starcrest Consulting Group July 2011)
AIR QUALITY IMPROVEMENTS DUE TO GOODS MOVEMENT ACTIONS (PHASE I)
The project was designed to be conducted in two phases. During Phase I of the project (9/2012–12/2014), we determined that improvements in air quality in GMCs are statistically significantly greater than in CTRLs after controlling for truck/vehicle kilometers traveled, cargo volume, meteorological conditions, and other factors. Detailed methods and findings of Phase I are presented in Appendix 1(available on the HEI website). In the fall of 2012 and spring of 2013, we deployed two rounds of Ogawa NOx and NO2 fixed-site saturation monitors in the counties of Los Angeles and Alameda. The purpose of saturation monitoring was to identify the small area variations (i.e., 30 m) in traffic-related air pollution and potential improvements in air quality due to GM regulatory policies. We chose Los Angeles and Alameda as locations of saturation sampling for the following reasons: (1) they are within the two biggest urban regions in California; (2) we have historical high-density air pollution monitoring data for the pre-GM policy period; and (3) they contain three major U.S. ports: Los Angeles, Long Beach, and Oakland.
We hypothesized that areas near GMCs would experience greater reductions in traffic-related air pollutants than areas away from the GM areas, which were defined in our study as control (CTRL) areas. Using the 2012 and 2013 saturation monitoring data and the previously collected Ogawa saturation monitoring data for 2004–2005 (Alameda) and 2006– 2007 (Los Angeles), we observed significantly greater declines in air pollution near GMCs and port facilities compared with CTRL areas, with GMCs experiencing the greatest reductions in NO2 and NOx concentrations, followed by NGMCs, and the lowest in CTRLs (Su et al. 2016). In Los Angeles, compared with the pre-policy period, the reductions of median pollutant concentrations for NO2 and NOx in GMCs were 6.4 and 21.7 ppb, respectively, whereas the reductions were smaller in NGMCs, 5.9 and 16.3 ppb, respectively, and smallest in CTRLs, 4.6 and 12.1 ppb, respectively. The reductions of NOx concentrations in GMCs were more than twofold those of corresponding reductions in CTRLs. These relationships were largely maintained for the Bay Area, where concentrations for NO2 and NOx were lower compared with those of Los Angeles.
At the time California implemented the CARB GM policy actions, the global economy was experiencing a decline (in December 2007) and took a particularly sharp downward turn in September 2008, this downward turn is referred to as the Great Recession (Catalano 2009). This severe economic recession and financial crisis originated in the United States and rapidly spread to other countries, which created widespread impacts on various industrial sectors including housing, stock, and import and export business (Bagliano and Morana 2012). Bagliano and Morana argued that the import and export business was the key transmission mechanism of real economic shocks. These economic dynamics also impacted the amount of GM and transportation in the United States and California. To investigate the CARB regulatory policy effect on reductions in air pollution at GMCs, we controlled for the impacts of economic downturn and meteorological conditions, including truck/vehicle kilometers traveled, cargo volume, and meteorological factors such as temperature, atmospheric pressure, and relative humidity. It is appropriate to use total traffic (98.6% of which are non-commercially registered vehicles) and weighted cargo volumes to control for potential confounding from impacts of the economic downturn. Even though these measures are related to levels of exposure, it is still appropriate to adjust for them to observe reductions in concentration due to the policy impact. For example, one can interpret the results from these adjusted models as the impact of the policy that is not due to the reductions in total vehicle miles traveled on roadways or the reductions in overall cargo movement (two factors most closely related to the economic downturn) but to other changes that influenced pollution levels (such as cleaner trucks, etc.).
After taking into consideration the interaction between location category (GMCs, NGMCs, and CTRLs) and policy period (pre- and post-), the adjusted mean pollutant concentrations were found to be 4.8 (± 0.4) and 15.5 (± 1.8) ppb lower in the post-policy period compared with the pre-policy period for NO2 and NOx, respectively. In GMCs and NGMCs, the pollutant concentrations of NO2 and NOx were significantly higher than in CTRLs, with respective differences of 6.2 (± 0.9) and 3.0 (± 0.9) ppb for NO2 and of 30.6 (± 4.3) and 9.1 (± 4.4) ppb for NOx. The interaction terms showed that reductions of both NO2 (mean = 1.3 ppb and [standard error] SE = 0.5 ppb) and NOx (mean = 10.2 ppb and SE = 2.4 ppb) from the pre- to post-policy period were statistically significantly larger in GMCs than reductions in CTRLs while controlling for those potential confounding factors. Although we also observed reductions in NGMCs from the pre- to the post-policy period, the interaction term between NGMCs and policy period, however, was not statistically significant (P = 0.1 for NO2 and for NOx). These research findings have been published in Environmental Science & Technology (Su et al. 2016). Because these findings served as a justification for Phase II and have already been summarized in the scholarly literature, we have summarized the findings here as background to the main focus of the report that uses quasi-experimental DiD models for assessing reductions in exposures and improvements in health potentially resulting from the GM policy actions.
PART 2: CONCENTRATION MODELING, ASSIGNMENTS, AND TRENDS
LAND-USE REGRESSION MODELING METHODS
In LUR modeling, we applied the Deletion/Substitution/Addition algorithm to develop annual air pollution models (Beckerman et al. 2013; Su et al. 2015b). This algorithm is an aggressive model search algorithm that iteratively generates polynomial generalized linear models based on the existing terms in the current “best” model and the following three steps: (1) a deletion step which removes a term from the model, (2) a substitution step which replaces one term with another, and (3) an additional step which adds a term to the model. The search for the “best” estimator starts with the base model specified with “formula” typically the intercept model, except when the user requires a number of terms to be forced in the final model. Before searching through the statistical model space of polynomial functions, the dataset for a specific year and a specific type (e.g., saturation or government continuous monitoring) are assigned randomly into v-folds with roughly equal numbers of observations in each fold. Data in one fold is used for validation, while the data in the remaining folds are used for prediction/model training. This process repeats for v-times until all the folds are used for validation. The polynomial within the search space that minimizes the cross-validated risk is selected as the prediction algorithm. The v-fold randomization of sample cross-validation helped us avoid model overfitting. In our practice, we limited the predictors to be only on linear terms (the maximum sum of powers in each variable to be 1) and disallowed any interaction except corridor by year. Further, we modeled the repeated measures in our annual models to take into consideration that one site might be measured multiple times during the 2004–2010 period.
Corresponding covariates (see the detailed covariate list in Appendix 1) were developed for LUR modeling, included both non-buffer variables and buffer variables. For each variable with buffer statistics, 40 buffers were created, generating 40 buffered covariates (50–2000 m with an interval of 50 m). Because of this, the total number of covariates in a single LUR model was close to 600. To reduce the number of covariates and avoid high correlations between them for LUR modeling, we first created a correlation coefficient matrix between a pollutant and all the covariates. The covariate of the highest correlation with the pollutant was used to calculate absolute correlation coefficients with all the remaining covariates and those covariates with an absolute correlation coefficient greater than or equal to 0.9 with the covariate of highest correlation with pollutant were removed. The covariate in the remaining covariates with the highest correlation with the pollutant was used to remove those remaining covariates who had a correlation coefficient greater than 0.9 with the covariate. This process continued until no absolute correlation coefficient was greater than 0.9 between any remaining covariates.
In modeling NO2, we developed an annual LUR model that incorporated the data from the saturation monitoring (for years in 2004–2005, 2006–2007, and 2012–2013 in Alameda and Los Angeles counties) (Appendix 2, Table A2-1, available on the HEI website) and governmental continuous monitoring (years 2004–2010) into a single modeling framework. The data from saturation monitoring were used to estimate small-area variations and the data from the governmental continuous monitoring helped us identify temporal variations. For each year of the study period, if there was saturation monitoring, we randomly separated those saturation monitoring data into 10-folds of equal size (after removing those co-located with government monitoring). The government’s continuous monitoring data for years 2004, 2006, and 2012 were also randomly separated into 10-folds of equal size for each year. These 10-folds of data were merged together to form a dataset of 10-folds for all the years across all the sampling types. Repeated measures were taken into consideration by adding a random effect intercept in site ID number, which represented either government or our own research designed saturation air quality monitors, during modeling. To help identify the general trends of pollutant concentrations throughout the years, we also included the variable year in the models as a predictor. Due to our research finding (Su et al. 2016) that the reductions in pollutant concentrations in NOx were greater in GMCs and NGMCs than in CTRLs from the pre- to the post-policy period, we created a three-way interaction term between a corridor, policy period, and year. The three-way interaction identified differences in air pollutant concentrations across the three location categories for policy periods and years of study.
LAND-USE REGRESSION RESULTS
Through analysis of distance curves of predictors in correlation with measured NO2 concentrations (Appendix 2, Figure A2-2), we found that percentage of impervious surface had the greatest positive contributions to the levels of NO2. High- and medium-intensity land development also had positive contributions. Both total vehicle kilometers traveled and total truck kilometers traveled had positive impacts on NO2. By contrast, vegetation (including trees/forest, shrubland, and grassland) showed negative associations with NO2. Developed open space, barren land, and bodies of water also showed negative associations with NO2. Using these buffered variables plus those non-buffer statistics (e.g., meteorological conditions) we developed a LUR model with effective power (adjusted R2 = 0.74) (Table 2) to predict annual NO2 concentrations throughout California at a spatial resolution of 30 m for years 2004–2010. The interaction between GMCs, the policy period, and the year was found to be statistically significant (P < 0.05).
Table 2.
Land-Use Regression Model Predicting Annual Pollutant Concentrations of NO2 for Californiaa
a The first set of parentheses for a predictor represents the unit of measure, and the second set, if any, represents the buffer distance. Table 1 presents only the fixed effects associated with the LUR model. A repeated measure of site ID was also used for the modeling process.
Using the fixed-effects model coefficients, we generated annual NO2 surfaces at a spatial resolution of 30 m across California for years 2004–2010 (Figure 1 and Appendix 2, Figure A2-3). Figure 1 shows the predicted surfaces for years 2004, 2006, 2008, and 2010 for the San Francisco Bay area (top) and the Los Angeles Metro (bottom). The statewide surfaces are included in Appendix 1. We identified dramatic reductions in NO2 concentrations for both San Francisco Bay and Los Angeles from 2004 to 2010, especially for locations near GMCs and after policy regulation.
The annual NO2 surfaces generated for San Francisco Bay (top) and Los Angeles (bottom) using the deletion/substitution/addition modeling approach. (Source: From Su et al. 2020; licensed under CC-BY-NC-ND 4.0.)
Similar to model annual NO2 concentrations, we randomized the data from governmental monitoring and divided them into 10 folds of equal size separately for years 2004, 2006, 2008, 2010, and 2012 in modeling PM2.5 and O3, and repeated measures were taken into consideration. Through analysis of distance curves of predictors in correlation with measured PM2.5 concentrations (Appendix 2, Figure A2-4), we found that the associations were similar to those found for NO2. The percentage of impervious surface had the greatest positive contribution to the levels of PM2.5 . High and medium intensity land development also had positive contributions. Both total vehicle kilometers traveled and total truck kilometers traveled had positive impacts on PM2.5 . By contrast, vegetation (including trees/forest, shrubland, and grassland) showed negative associations with PM2.5 . Developed open space, barren land, and bodies of water also showed negative associations with PM2.5. Using these buffered variables plus those non-buffer statistics (e.g., meteorological conditions) we developed a LUR model with a prediction power (R2 = 0.64) similar to other research findings (Table 3). The interactions between GMCs, the policy period, and year, and between NGMCs, the policy period, and year were found to be statistically significant (P < 0.05). Using the annual PM2.5 model, we generated PM2.5 concentration surfaces throughout California also at a spatial resolution of 30 m for years 2004–2010 (Figure 2 and Appendix 2, Figure A2-5).
Table 3.
Land-Use Regression Model Predicting Annual Pollutant Concentrations of PM2.5 for Californiaa
a The first set of parentheses for a predictor represents the unit of measure, and the second set, if any, represents the buffer distance. Table 2 presents only the fixed effects associated with the LUR model. A repeated measure of site ID was also used for the modeling process.
The annual PM2.5 surfaces generated for San Francisco Bay (top) and Los Angeles (bottom) using the deletion/substitution/addition modeling approach.
In modeling O3 concentrations (Table 4), we found that the predictors with positive impacts on NO2 and PM2.5 concentrations had negative impacts on O3. Greater vegetation cover in grass was associated with higher O3 concentrations whereas the greater proportion in impervious surface was associated with lower O3 levels. The annual O3 model had GMC being lowest in concentrations and the model had a prediction power similar to PM2.5 with 66% variance being explained.
Table 4.
Land-Use Regression Model Predicting Annual O3 Concentrations for Californiaa
a The first set of parentheses for a predictor represents the unit of measure, and the second set, if any, represents the buffer distance. Only the fixed effects were shown with the LUR model. A repeated measure of site ID was also used for the modeling process.
CONCENTRATION ASSIGNMENTS AND TRENDS AMONG BENEFICIARIES
The annual pollution surface data were delivered via secure FTP from the University of California, Berkeley (UC Berkeley) to the University of California, Los Angele (UCLA). The concentration surfaces were assigned to the home addresses of the subjects included in this project, for years 2004–2010. The home address of the study subjects in 2004 was geocoded via SAS/GRAPH 9.2 software with built-in U.S. street lookup data for specific Census Bureau’s Topologically Integrated Geographic Encoding and Referencing (TIGER) database released by the Census Bureau of the year 2012, then assigned the appropriate annual exposures. We had only the subjects’ addresses at the beginning of the study and had to assume that they lived in the same addresses during the study period.
We observed significant reductions in pollutant concentrations for enrollees living in 10 counties based on the pre- and post-policy averages for NO2 and PM2.5 using the annual air pollution surfaces developed for years 2005–2010. Figure 3 and Appendix 3, Table 3-1 display average NO2, PM2.5, and O3 concentration levels among study subjects for the pre-policy and post-policy periods summarized by domain. The average NO2 exposures decreased in ppb from 24 to 19.3, from 22.4 to 18.7, and from 20.1 to 17.3 for those living in GMC, NGMC, and CTRL areas, respectively. The enrollees living in GMCs experienced the greatest reductions in NO2 concentration. Their levels were approaching those of NGMCs and CTRLs in the post-policy periods. For PM2.5, reductions in μg/m3 were seen from 13.9 to 11.8, from 12.9 to 10.9, and from 12.3 to 10.4 in GMC, NGMC, and CTRL areas, respectively. However, the O3 exposures showed an opposite trend with relatively low concentration in GMCs, and trends are identical among the three study domains.
Air pollution concentration trends among all beneficiaries by domain.
PART 3: POLLUTANT EXPOSURE REDUCTION AND HEALTH IMPACT ANALYSES
METHODS
Medi-Cal Data and Outcome and Time-Varying Covariate Measures
To examine whether pollutant reductions from regulatory actions resulted in improvements in health outcomes among Medi-Cal beneficiaries with asthma, heart disease, COPD, and diabetes, we used six years of Medi-Cal claim data to create the study sample and define the outcome and covariate measures. The data for evaluating the impact of the pollutant reduction on health outcomes is part of California Medicaid data for ten counties from September 1, 2004, to August 31, 2010. The data was originally obtained by the UCLA Center for Health Policy Research to evaluate the Disease Management Pilot Program project conducted by the California Department of Health Care Services. The goal of this Disease Management Pilot Program was to test the efficacy of providing a disease management benefit to Medi-Cal FFS beneficiaries with chronic conditions. The original inclusion criteria for the program included: being 22 years of age or older under certain aid codes (excluding Medicare eligible) and having at least one paid claim between March 1, 2004, and October 2010, for any of the six following conditions: asthma, COPD, diabetes, atherosclerotic heart disease, coronary artery disease, and congestive heart failure (the later three were grouped into heart disease). The study populations were mostly under 65 years of age because when participants reached the age of 65 years most of them would be eligible for Medicare coverage. And once they are enrolled in Medicare, most of their care is reimbursed through Medicare even if they are still eligible for Medicaid. The impact of the exclusion of children and the elderly in the study sample is unknown because no studies show the elderly or children to be more or less responsive than adults to air quality improvements. However, other studies indicated that improvements in air quality led to better health outcomes among children and the elderly (Di et al. 2017; Gilliland et al. 2017). The study period ended in October 2010 because that is when the Disease Management Pilot Program projects ended and most of the Medi-Cal–eligible started to enroll in managed care plans.
To assure data completeness for the study cohort, we aimed at identifying patients with six years of continuous Medi-Cal enrollments between 2004 and 2010 and at least one presence in the claims data per year. Continuous enrollment was defined to be at least 11 months enrolled within a year. We started with the claims data of a total of 172,334 patients and applied basic exclusion rules. The exclusion criteria included long-term care patients, cancer patients, and HIV patients defined by specific International Classification of Diseases Ninth Revision (ICD-9) codes and place of service code. For this study, we further limited our study subjects to those who had a valid home address (e.g., not a post office box number or ZIP code only) with pollutant assignments. Based on those conditions, we created a cohort of 23,377 enrollees for the study. We went through the following six steps to create the analytical sample for data analyses (Figure 4):
The steps implemented in the study to select the final sample for the project.
We created subsets of enrollees using only the four chronic conditions that were targeted by this study: COPD, asthma, diabetes, and heart disease. The conditions were defined as any appearance of the respective diagnostic codes in the first three years (pre-policy period).
We identified patients who have been continuously enrolled in the entire six-year period by using the Medi-Cal eligibility file. This step drastically reduced the sample size because most Medi-Cal enrollees in the sample were not retained for all six years, due to changes in the status of Medi-Cal eligibility and churning in general.
Since we needed to assign to each patient the environmental variables, such as corridor, and pollutant level, we kept only those patients with valid geocodes based on their addresses provided to UCLA at the beginning of the study by the California Department of Health Care Services. Those with post office box numbers or ZIP Codes only were excluded from analyses.
Some patients might not have used any Medi-Cal services even though they had been continuously enrolled with one of the four required chronic conditions in any given year. We included only those enrollees who had used the Medi-Cal service at least once each year. This is equivalent to requiring the presence of the enrollee in every year of the claims data.
The corridor (GMC, NGMC, and CTRL) shapefile was done by the air pollution modeling team at UC Berkeley and was based on the corridor-designation criteria described above. That information was then merged with the Medi-Cal patient data using ArcGIS software via interpolating the corridor surface to the geocoded locations of the beneficiaries. Some Medi-Cal beneficiaries might not have provided addresses within California and were removed from analyses.
Similarly, the annual pollutant concentration surfaces of NO2, PM2.5, and O3 created by the UC Berkeley team were assigned to each individual based on their respective geocoded home address. The individual pollutant concentration data were then merged with health data for analyses.
The biggest drop in the sample size happened when the six-year continuous enrollment requirement was imposed. We decided to use a cohort instead of the whole study population and only allowed for the one-month gap each year due to the nature of the program. The evidence suggests that a sizable number of people in the Medicaid program are unable to maintain their coverage over a long period, despite remaining eligible for the program (Seifert et al. 2010; Sommers et al. 2013). For instance, a study showed that about 43% of newly enrolled adults in Medicaid experienced a gap in coverage during their initial 12 months of coverage (Sommers 2009). There are two types of coverage disenrollment: (1) dropping out of the program completely and (2) “churning,” or “enrollment interruptions,” referring to case closings followed by re-openings (Seifert et al. 2010). Research has shown that interruptions in Medicaid coverage can result in greater ER use as well as significant increases in hospitalization for conditions that can be managed on an ambulatory basis (Bindman et al. 2008; Cassedy et al. 2008; Hall et al. 2008; Kasper et al. 2000; Ku et al. 2009; Paradise and Garfield 2013). As a result, if we used the whole study population, it might be hard to distinguish whether the changes in the study outcomes (e.g., reduction in ER visits) are due to GM policy actions or to the turnover of Medicaid enrollees.
We developed and tested annual health outcome measures using a combination of diagnostic codes (up to two ICD-9 codes for each encounter), claim type (e.g., outpatient, inpatient, pharmacy, Medi-Cal/physician, and dental), place of service (e.g., emergency room, doctor office, outpatient/inpatient hospital) and date of service to define each measure. The actual Year 1 was from September 1, 2004, to August 31, 2005, based on the California fiscal year, and was referred to as 2005 for this project. Similar patterns were followed for other study years through the whole study period.
The specific outcome measures for all causes were developed as follows.
Annual number of ER visits: actual number of ER visits (e.g., 0, 1, 2) each year per beneficiary with the post-policy period in years 2008, 2009, and 2010 compared with the 2004–2007 average (pre-policy baseline years).
Annual number of hospital admissions: the actual number of hospital admissions (e.g., 0, 1, 2) each year per beneficiary with the post-policy period in years 2008, 2009, and 2010 compared with the 2004–2007 average (baseline years).
We also took advantage of the Medi-Cal enrollment and claims data and accounted for common risk or modifying factors (listed below) when examining associations between improvement in air quality and decreases in adverse health outcomes. We constructed individual-level socioeconomic variables that included age groups, sex, race/ethnicity (white, Latino, African American, Asian and Pacific Islander, and others), and spoken languages (English and non-English speaking). Additionally, we developed and tested measures of other confounding or time-varying factors (e.g., access to primary care, changes in disease severity, or development of comorbidities) that may influence changes in health outcomes. The details for each of these variables are as follows:
Disease severity: We used a Chronic Illness and Disability Payment System (CDPS) scale, which Kronick and colleagues (2000) developed to assess illness severity (http://cdps.ucsd.edu/). Specifically, an annual score for severity of illness was created for the study population using a CDPS software combining codes from diagnostic codes (ICD-9-Clinical Modification) and pharmacy codes that occurred for a patient during the measurement year. In the statistical model, it is lagged and transformed on a logarithmic scale based on previous-year claims. We chose the CDPS severity scale because, using analysis of Medicaid claims from six states, Kronick and colleagues (2000) showed that for disabled adults on Medi-Cal, the CDPS model is more predictive of future health care needs (e.g., next year) than both the diagnostic cost group/hierarchical condition category model and the pharmaceutical reimbursement model. We used a CDPS score in each year to reflect any changes in an enrollee’s disease severity.
Comorbidities (including depression): We used the number of preexisting comorbidities as one of the major factors. For instance, for a patient with heart disease, comorbidity of asthma or COPD may make them even more sensitive to air quality changes. To sufficiently control for the influence of comorbidities, all diagnoses in a claims record (up to two diagnoses in each encounter) were used to identify subjects with these comorbidities. One claim record with more than one diagnosis of the diseases under study (e.g., asthma, heart disease, COPD, and diabetes) each year (from September 2004–August 2007) was defined as the presence of comorbidity in the baseline year and actual accounts were used to indicate the number of comorbidities. For depression, we searched depression-related ICD-9 codes in the claims for each year to identify those with depression.
Smoking behavior: We searched smoking-related ICD9 codes in the claims (e.g., 305.1 for Tobacco use disorder) to identify beneficiaries who smoke. By only accessing primary and second diagnosis codes, we identified 3,321 (14.2%) unduplicated ever-smoking beneficiaries in the study period. This was comparable with the percentage of adult who reported smoking, 14.9% and 14.1%, respectively, reported in the 2005 and 2011 California Health Interview Surveys. We used smoking percentages in pre- and post-policy years. Specifically, if someone has a smoking diagnosis in a year, they were defined as smoking in the year. Correspondingly, if someone had no smoking diagnosis in later years, they were defined as non-smoking in that year. Due to the incompleteness of doctor’s records of smoking status (e.g., doctor might only add the diagnostic code only if the patient was undergoing a related treatment, such as cessation), we may under- or over-estimate the changes in smoking status
Access to primary care: Most of the chronic diseases investigated in our study may benefit from appropriate management of these conditions in the primary care setting (Porter et al. 2007). In other words, timely and appropriate access to primary care can reduce the likelihood of ER use or inpatient admission by delaying disease progression and avoiding acute episodes (Billings et al. 1993; Porter et al. 2007). Given that we do not have the direct measures for access to care, we used a year-specific number of primary doctor visits in the study period as a proxy for access to primary care in each pre- and post-policy year as was done in other studies (Institute of Medicine [U.S.] 1993; Lambrew et al. 1996).
Neighborhood Socioeconomic Status (Census Tract Level)
We used the census-tract-level Social Vulnerability Index (SVI) (Flanagan et al. 2011) data developed by the U.S. Centers for Disease Control and Prevention to control for socioeconomic changes at the neighborhood level. The SVI ranks each census tract on 14 social factors, including poverty, lack of vehicle access, and crowded housing, and groups them into four related themes. Each census tract receives a separate ranking for each of the four themes such as a percentile ranking for a socioeconomic theme, household composition theme, minority status/language theme, and housing/transportation theme as well as an overall ranking. The SVIs are only available for 2000, 2010, and 2014. We used the 2000 SVI for the pre-policy period and the 2010 SVI for the post-policy period as the variables to control for neighborhood SES changes due to economic downturns or other factors.
Statistical Analyses
To examine whether the GM policy actions led to reductions in ambient air pollution exposures and subsequent improvements in health outcomes among Medi-Cal beneficiaries in 10 counties in California, we estimated the predicted outcomes for enrollees in GMCs with and without policy intervention by using the control group as the counterfactual. To facilitate interpretation, we calculated DiD estimates in the first, second, and third year after the policy intervention, respectively. We explored whether parts of the improvements in health outcomes were due to the air pollution reduction by using a multilevel mediation model, in which the effect of GM policy actions on health outcomes was mediated through the effect of actual air pollution reductions in the post-policy years. To further verify the causal inferences of the GM policy actions on the improvement of exposures and health outcomes, we performed several sensitivity analyses, including conducting DiD analyses as described above using inverse probability of treatment weighting derived from propensity scores. All the models control for sex, language speaking, age groups (21–45, 46–55, and 56+years), race/ethnicity (White, Black, Asian and Pacific Islander, Latino, Other or Unknown), number of comorbidities in baseline years (0, 1 or 2, 3+), the county as fixed effects, and time-varying variables including year-specific smoking status, depression status, number of doctor visits, and log-transformed CDPS scores. We also controlled for several census track-level variables: census track level percentage of unemployed (age 16+), the percentage of persons below poverty estimates, percentage of minority, and percentage of households with no vehicle available. Because we only have two years of those census-track level variables, we used the data in 2000 for the pre-policy period and 2010 for the post-policy period.
DiD Models with a Parallel Trends Assumption
To examine whether reductions in air pollution led to improvements in health outcomes such as decreases in the number of ER visits or hospitalizations for beneficiaries with asthma, heart disease, COPD, and diabetes, we implemented several modeling techniques to establish their possible associations. First, we assessed whether the enrollees living within the three types of location categories described above had improved pollution exposures and health outcomes in the post-compared with the pre-policy intervention period. We then identified whether those living inside the GMCs experienced greater improvements in concentration and health than those living in CTRL areas. For health effect analyses, we assumed that the interventions of air pollution reduction are exogenous to health outcomes. With this assumption in mind, we took full advantage of the longitudinal data to evaluate the causal effect of the interventions by estimating the DiD using a multilevel modeling approach.
To examine whether the emission reduction plan led to decreases in NO2 level, we estimated a DiD model using a linear mixed model with random intercepts for beneficiaries to examine temporal changes in outcomes by comparing intervention corridors with control corridors (e.g., GMCs with CTRLs) before and after the policy intervention. The model controls for potential differential pre-trends between the two groups and allows the health impact to evolve over time. We estimated the following equation:
where GMCi is a dummy variable; 1 = GMC and 0 = CTRL. Xi represents sex, language spoken, age groups, race/ ethnicity, number of comorbidities in baseline years, the county as fixed effects, time-varying variables including year-specific smoking status, depression status, number of doctor visits, and log-transformed CDPS scores, and census track-level variables, including percentage of unemployed (age 16+), the percentage of persons below poverty estimates, percentage of minority, and percentage of households with no vehicle available. The coefficients (γk) of the interactions between year dummy variables and the group dummy during the post-policy years indicates DiD estimates in year k.
To evaluate the effect of emission reduction plan on ER visits or hospitalizations, we used a multilevel generalized linear model with a negative binomial distribution and random intercepts for beneficiaries to examine temporal changes of ER visits or by comparing GMCs with CTRLs. The model accounts for the skewed distribution of ER visits and serial correlation for beneficiaries across study periods. For example, the equation we use to estimate for ER visits is specified below:
where Yit denotes the number of ER visits for patient i at time t. GMCi is an indicator variable that equals 1 for patients from GMCs; 0 for those from CTRLs. There are a total of six time points corresponding to six years of annual data, and they are grouped as pre-intervention period (t = 1, 2, 3) and post-intervention period (t = 4, 5, 6). Note that the outcome in equation 1 is on the natural scale whereas for equation 2 the outcome is on the log scale (more on this below). Coefficients for β2, β3, …, β6 represent the trend of the outcome without policy regulation for a respective specific time. Coefficients γ4, γ5, γ6 describe the difference in the outcome variable between GMC and CTRL corridors in the post-intervention period. In the equation, 1() is an indicator function, and 1(t = k) = 1 if t = k; otherwise, 1(t = k) = 0. Xit is a vector of covariates.
Based on the parallel assumption, the DiD was used to assess the causal impact of regulatory policy on reductions of air pollution, as well as for the causal impact on improvements in health outcomes. Since the coefficients from the above nonlinear model are on the log scale, it is difficult to interpret the coefficients directly. To facilitate interpretation, we used the margins command in Stata (Version 15.1) to get the predicted number of ER visits for GMC and NGMC over the study period. It is worth noting here that the margins command incorporates both fixed effects and random effects into the predicted values. Based on these predicted numbers of ER visits, we calculated DiD estimates in the first year (2008), the second year (2009), and the third year (2010) after the policy intervention, respectively. Similarly, separate models were developed for different chronic condition-specific subsamples.
In addition, the parallel assumption has been imposed on the transformed log-linear scale, and the coefficients (γk) on the interaction terms capture changes on a log scale. As an alternate way to interpret the results, we computed a new estimate as 100(eγk-1), which indicates the percent change in the expected number of ER visits due to the intervention of policy.
Sensitivity Analyses Tests To Assess Parallel-Trends Assumption
We conducted several tests to assess the adequacy of the parallel-trends assumption, which includes the investigation of parallel assumptions in the pre-policy period and inclusion of interaction terms between the intervention group (GMCs) and time dummy variables in the pre-policy period. The details are as follows:
Parallel Trends Assumption in the Pre-Policy Period
Because we used a multilevel model with a negative binomial distribution and log link function, the parallel trends assumption is on the log scale of ER visits. We were unable to create meaningful graphs of empirical ER averages to estimate the trends for ER visits because there are too many zero values. Instead, we investigated the parallel trends assumption by estimating the following model that allows different pre-trends in the three baseline years (t = 1,2,3) between GMCs and CTRLs.
where γit denotes the number of ER visits for patient i at time t. GMCi is an indicator variable that equals 1 for patients from GMCs; 0 for those from CTRLs. The first baseline year (t = 1) is considered as the reference group, and γk tests for the “parallel trends” assumption on the log scale. ζi denotes the random intercept for individual i. We fitted a multilevel model with individual random intercepts, a negative binomial distribution, and a loglink function. As shown in Appendix 3, Table A3-6, coefficients on these interaction terms were not statistically significant, which suggests that the “parallel trends” assumption is reasonable.
DiD Estimates with Full Interactions Between Group and Year Dummy Variables
To further assess the robustness of our estimates to the parallel trends assumption, we re-estimated our main specification including interaction terms between the intervention group (GMCs) and time dummy variables in the pre-policy period. In this way, it allows differential trends in the number of ER visits between GMCs and CTRLs. If we can get similar DiD estimates as those from the primary model, we can further confirm that the parallel trends assumption, on the log scale, holds. Specifically, we fitted the following model that allows unstructured time trends to vary between GMCs and CTRLs before and after the implementation of the “Emission Reduction Plan for Ports and Goods Movement” policy:
where Yit denotes the number of ER visits for patient i at time t. GMCi is an indicator variable that equals 1 for patients from GMCs; 0 for those from CTRLs. The first base-line year (t = 1) is considered as the reference group. Xit is a vector of covariates as introduced in the main statistical model ζi denotes the random intercept for individual i.
Multilevel DiD Models with Mediation Through Air Pollution Reduction
Also, we explored whether improvements in health outcomes (the number of ER visits) were due to the air pollution reduction by using a multilevel mediation model, in which the effect of the GM policy actions on health outcomes was mediated through the air pollution reduction. Such an effect was estimated using the generalized structural equation models.
where variable t in the equation ranges from 1 to 6 and represents the years after the baseline year. Li is a latent variable accounting for heterogeneity across individuals (Greene 2003). Equation 5a (level 1) estimates the cross-sectional effect of pollutants on ER visits by using the outcome ER at time 3 predicted by ER at time 2 and NO2 at time 2. The equations 5b and 5c (level 2) are longitudinal, and the same DiD models used to assess air pollutant changes in Equation 1. The random effects are individual level variables, and we allow the random effects of equations 5b and 5c to be correlated with the latent variable in the equation 5a. The vector Xit includes the same covariates as those in the DiD model described above.
Such a model allows us to estimate the indirect effect of policy through the effect of NO2 and PM2.5, as follows. The policy effect on NO2 is encoded in the coefficients of γk. For instance, the change in NO2 due to policy in program year one is γ4, the program year two γ5 and so on. Therefore, the indirect effect of policy through NO2 on ER will be τ1 × γ4 on the log scale. In other words, the expected change in the log of ER due to policy change is τ1 × γ4. We then exponentiated them to get the change in the change in the count. We can also estimate the joint effects of PM2.5 and NO2 on ER visits in program year one as exp (τ1 × γ4 + τ1 × λ4 )-1, which is the percent change in the number of ER visits due to the total counterfactual change in NO2 and PM2.5 due to policy intervention.
DiD Models with Inverse Probability of Treatment Weighting
As sensitivity analyses, we performed similar analyses described above with inverse probability of treatment weighting derived from propensity scores. The propensity scores were calculated from a logit model to estimate the probability of being in the GMC group relative to the control group as a function of sex, age group (21–45, 46–55, and 56+), number of comorbidities in baseline years (0, 1 or 2, 3+), and annual log-transformed CDPS score. Using the predicted probabilities from this model, average treatment effect weights (ATEWT) for GMC and CTRLs samples was created.
These weights were truncated at the 99th percentile for dichotomous metrics to avoid overly large weights. These were subsequently used as probability weights in the regression models. In this way, we reduced bias in the estimates of the pollutant effect, which could be confounded with other unobserved factors.
RESULTS
Descriptive Statistics
The study sample included 23,377 FFS Medi-Cal beneficiaries residing in 10 California counties. There were 8,636 enrollees with asthma, 8,900 enrollees with COPD, 13,337 enrollees with diabetes, and 8,684 enrollees with heart disease (including atherosclerotic heart diseases, coronary artery disease, and congestive heart failure) (Table 5). These enrollees were distributed in the following way across our study areas: 22.4% (5,232) in GMCs, 57.2% (13,377) in NGMCs, and 20.4% (4,768) in CTRL areas, respectively. The number of enrollees with each chronic condition may not add to the total since enrollees may have multiple diseases and they could be double-counted by disease. However, within each disease subgroup, a person can only be assigned to one domain (GMCs, NGMCs, or CTRLS). There were slightly more African Americans and Latinos in the GMCs than in the CTRLs (18% vs. 14% and 15% vs. 12%, respectively. At the neighborhood levels, the unemployment rates increased in CTRL areas from 2000 to 2010 (9.2% to 11.7%); and percentage of minorities also increased from 60.1% to 68. 6%, but the percentage of households with no vehicles decreased from 10% to 7.7% in the post-policy years.
DiD Results for Improvements in Pollution Exposures
To test the hypotheses that the GM policy actions have led to reductions in air pollutant concentrations and also the improvements in health outcomes (such as decreases in the number of ER visits or hospitalizations for beneficiaries with asthma, heart disease, COPD, and diabetes ), we evaluated the causal effect of the interventions by estimating the DiD using a multilevel modeling approach.
DiD-based models utilize an observed control group (or more precisely, a “quasi-control” group), which should exhibit similar trends when compared to the intervention group in the absence of a policy intervention. Such natural or quasi-experimental designs aid in establishing causality when randomization is not practical or ethical. Specifically, we examined temporal changes of NO2 and ER visits or hospitalizations by comparing GMCs with CTRLs and NGMCs with CTRLs, respectively. We estimated the predicted outcomes for enrollees in GMCs with and without the policy intervention by using the CTRL group as the counterfactual. To facilitate interpretation, we calculated DiD estimates in the first, second, and third year after the policy intervention. To verify the parallel assumption, we visualized the empirical time trend and tested the differential trends statistically (Figure 5).
The predicted values for NO2 (ppb) and ER visits from difference-in-differences models with parallel trends assumption. (Source: First panel [NO2 for all patients] reproduced from Su et al. 2020. Licensed under CC-BY-NC-ND 4.0.)
Concentration Improvements
We observed statistically significant reductions in NO2 and PM2.5 concentrations for enrollees in 10 counties. The reductions in NO2 concentrations were greater for beneficiaries living in GMCs than in CTRLs in the post-policy years, including all beneficiaries with different chronic conditions (DiD = -2 to -2.4, P < 0.01 (Table 6 and Figure 5). More reductions in NO2 concentrations were also observed among beneficiaries living in NGMCs than those in CTRLs in the post-policy years. However, the reductions in NO2 concentrations in NGMCs were smaller than in GMCs in comparison to CTRL (DiD= -1 to -1.44, P < 0.01). The reductions in NO2 concentrations were even smaller when GMCs were compared with NGMCs (DiD= -1, P < 0.01) (Table 6).
Table 6.
Difference-in-Differences Estimates for NO2 (ppb) between GMCs and CTRLs, GMCs and NGMCs, and NGMCs and CTRLs
a The model was adjusted for age groups, sex, race/ethnicity, language speaking, number of comorbidities in baseline years, the county, year-specific smoking, depression, number of doctor visits, and CDPS scores, plus census track-level SVI variables: percentage of unemployed (age 16+), persons below poverty estimates, minority, and households with no vehicle available.
b Numbers are difference-in-differences (DiD) estimates comparing changes between corridors each post-policy year vs. the baseline years (3 years before the implementation of GM actions). Post3rd Year denotes the policy effect three years after GM actions; 95% CI entries refer to 95% confidence intervals.
Similar patterns of the reductions of PM2.5 concentrations were also observed, but the magnitudes of reductions were smaller in comparison with NO2. The reductions in PM2.5 concentrations were greater for beneficiaries living in GMCs than in CTRLs in the post-policy years, including all beneficiaries with different chronic conditions (DiD = -1.32 to -1.51, P < 0.01 [Table 7]). Reductions in PM2.5 concentrations were also observed among beneficiaries living in NGMCs versus those in CTRLs in the post-policy years. However, the reductions in PM2.5 concentrations in NGMs were smaller than in GMCs (DiD = -.80 vs. DiD = -.91, P < 0.01) in comparison to CTRLs. The reductions in PM2.5 concentrations were the smallest when GMCs were compared with NGMCs (DiD = -0.47 to DiD = -0.60, P < 0.01) (Table 6). Additionally, the O3 concentrations showed an opposite trend with a slight increase for beneficiaries living in GMCs than for those in CTRLs, as well as in NGMCs and CTRLs in the post-policy years, but no changes were observed among those in GMCs and NGMCs (Appendix 3, Table A3-2, available on the HEI website).
Table 7.
Difference-in-Differences Estimates for PM2.5 (μg/m3) between GMCs and CTRLs, GMCs and NGMCs, and NGMCs and CTRLs
a The model was adjusted for age groups, sex, race/ethnicity, language speaking, number of comorbidities in baseline years, the county, year-specific smoking, depression, number of doctor visits, and CDPS scores, plus census track-level SVI variables: percentage of unemployed (age 16+), persons below poverty estimates, minority, and households with no vehicle available.
b Numbers are difference-in-differences (DiD) estimates comparing changes between corridors each post-policy year vs. the baseline years (3 years before the implementation of GM actions). Post 3rd year denotes the policy effect three years after GM actions; 95% CI entries refer to 95% confidence intervals.
DiD Results for Improvements in Health Outcomes
ER Visits Reductions
We observed statistically significantly greater reductions in ER visits for those in the GMCs than those in the CTRLs in post-policy years.
Specifically, those with asthma living in GMCs experienced a larger reduction in the number of ER visits compared with their counterparts living in CTRLs in the second year (DiD = -0.17, P < 0.01) and third year (DiD = -0.17, P < 0.01) after the policy intervention (Table 8). The number of ER visits for those with COPD in GMCs also decreased more than for those living in CTRLs in the second year (DiD = -0.13, P < 0.05) and third year (DiD = -0.18, P < 0.01). For those with diabetes and heart disease and the total sample, we observed greater downward trends in ER visits in post-policy years for those living in GMCs than those in CTRLs but the differences were not statistically different. We also observed that the number of ER visits for those beneficiaries with asthma living in NGMCs decreased more than for those living in CTRLs in the second year (DiD = -0.11,P < 0.05) and third year (DiD = -0.16, P < 0.01) after the policy (Table 8). The number of ER visits for those with COPD, diabetes, and the total sample in NGMCs also had downward trends in the post-policy year in comparison with those in CTRLs but the differences were not statistically significant. Similar downward trends were observed in the number of ER visits in post-policy years for those living in GMCs than those in NGMCs, but the differences were also not statistically different (Table 8).
Table 8.
Difference-in-Differences Estimates for ER Visits, between GMCs and CTRLs, GMCs and NGMCs, and NGMCs and CTRLs
a The model was adjusted for age groups, sex, race/ethnicity, language speaking, number of comorbidities in baseline years, the county, year-specific smoking, depression, number of doctor visits, and CDPS scores, plus census track-level SVI variables: percentage of unemployed (age 16+), persons below poverty estimates, minority, and households with no vehicle available.
b Numbers are difference-in-differences (DiD) estimates comparing changes between corridors each post-policy year vs. the baseline years (3 years before the implementation of GM actions). Post3rd Year denotes the policy effect three years after GM actions; 95% CI entries refer to 95% confidence intervals.
Table 8 documents the main DiD estimates of the GM action on the number of ER visits. To interpret the DiD estimates, the DiD estimate of -0.17 in the third year after the policy implementation comparing GMCs with CTRL among asthma patients means -0.17 reductions in ER visits per person that year. It implies that for 1,000 beneficiaries with asthma, the GM regulations could contribute to a reduction of 170 ER visits per year in GMCs when compared with CTRLs. Similarly, when comparing GMCs with CTRLs among 1,000 beneficiaries with COPD, an increased reduction of 180 ER visits was estimated for the third year after the implementation of the GM policy.
Using the multilevel generalized linear model with a log link function and a negative binomial distribution, we also computed a new estimate as, 100(eγk -1)which indicates the percent change in the expected number of ER visits due to the intervention of policy. We found that the number of ER visits for those with asthma living in GMCs decreased 11.8% (95% CI, -21.4% to -1.1%) more than with those living in CTRLs in the second year and decreased 14.8% in the third-year (95% CI, -24.0 to -4.4%) after the policy (Appendix 3, Table A3-3). The numbers of ER visits for those with COPD in GMCs also decreased more than for those living in CTRLs in the third year (percent change = -11.8, 95% CI, -21.2% to -1.2%).
We also used the DiD models to further control for pollutant impacts such as PM2.5 and O3. Further controlling for pollutant concentrations such as NO2, PM2.5, and O3 in addition to covariates in the primary models produced results that were similar to the original DiD results in Table 8. For example, the number of ER visits for those with asthma living in GMCs decreased more than for those living in CTRLs in the second year (DiD = -0.17, P < 0.01) and third year (DiD = -0.17, P < 0.01) after the policy (Appendix 3, Table A3-4). To estimate the impact of potential time-varying variables, such as disease severity, we did analyses to lag disease severity (CDPS scores) for a year (Appendix 3, Table A3-5) so that we could estimate whether the disease severity in the previous year had any impact on the use of ER service. The findings showed results that were identical to those of the original DiD tests (Appendix 3, Table A3-5).
DiD Estimates with Parallel Trends Assumption and Tests
We used DiD estimates with parallel-trends assumption, which assumed that the control group exhibited the same exposure or health trajectory as the intervention group before and after the intervention in the absence of policy. We visualized the empirical time trend for NO2 concentrations and ER visits for those with asthma and COPD and total study samples (Figure 5). The red line (bottom) indicated observed rates of the CTRL group, the blue line (middle) indicated observed rates of the intervention group, and the gray line (top) indicated the expected rates of the intervention group without policy intervention, which was parallel with the control group. Here we observed significant improvements in the intervention group in the GMCs compared to CTRL living in areas largely removed from ports or trucking activities. The results showed that the GM policy actions led to measurable changes in NO2 concentrations for those in GMCs compared with those in CTRLs in the post-policy years: the reductions in exposure to NO2 were significantly greater for those in GMCs, including all beneficiaries with different chronic conditions. We also observed significantly greater decreases in the numbers ER visits for those with respiratory diseases in the GMCs than those in the CTRLS in post-policy years. Specifically, the average number of ER visits among those with asthma living in GMCs was reduced from 1.23 to 1.11 and to 1.13 in the second year and third year, respectively, post policy. Nevertheless, the number of ER visits for those living in CTRLs increased from 0.90 to 0.94 and 0.99 in the same time periods as was expected due to aging or the natural course of the development of their chronic conditions (Agarwal et al. 2017). The numbers of ER visits for those with COPD in GMCs also decreased when compared with those living in CTRLs in the second year and third year post policy. For those in the total sample, we observed greater downward trends in numbers of ER visits in post-policy years for those living in GMCs than those in CTRLs, but the differences were not statistically different.
We conducted several tests to assesses the adequacy of the parallel-trends assumption, which assumes that the control group should exhibit the same exposure or health trajectory as the intervention group before and after the intervention in the absence of policy. The findings further confirmed that no empirical evidence from the data showed violations of the parallel assumptions. The details are as follows:
Test of Parallel-Trends Assumption in the Pre-Policy Period for ER Visits for Those with Asthma and COPD
As we used a multilevel model with a log-link function, the parallel-trends assumption is on the log scale of ER visits. We examined the assumption based on the pre-policy trends for GMCs and CTRLs and conducted separate analyses for asthma patients and COPD patients. As shown in Table A3-6 in Appendix 3 (available on the HEI website), coefficients on these interaction terms were not statistically significant, which suggests that the parallel-trends assumption is reasonable.
Estimates with Full Interactions Between Group and Year Dummy Variables for ER Visits for Those with Asthma and COPD
To further assess the robustness of our estimates to the parallel-trends assumption, we re-estimated our main specification including interaction terms between the intervention group (GMCs) and time dummy variables in the pre-policy period. In this way, it allows differential trends in the number of ER visits between GMCs and CTRLs. If we can get similar DiD estimates as those from the primary model, we can further confirm that the parallel-trends assumption, on the log scale, holds. Table A3-7 of Appendix 3 shows the results for asthma patients and COPD patients, respectively. All of these estimates are fairly consistent with those from our main model specifications. It is reassuring and further suggests that the parallel trends assumption is plausible in our study.
Mediation Modeling Results
We explored whether improvements in health outcomes are due to the air pollution reduction by using a multilevel mediation model, in which the effect of GM policy actions on health outcomes was mediated through the effect of actual air pollution reductions in the post-policy years. We combined the effects of NO2 and PM2.5 in the model. We observed a greater decrease of 0.129 in ER visits among asthma patients for a composite change of one unit reduction in NO2 and one unit reduction in PM2.5 (DiD = -0.129, P < 0.05) from the pre-policy years to the post-policy years (Table 9). The reductions in NO2 and PM2.5 due to policy change estimated by the mediation model are essentially the same as shown in Tables 6 and 7. Mediation analyses suggested that the effects of GM policy interventions on health improvements were largely due to exposure reductions. For all other beneficiaries, there were greater downward trends in GMCs, but the magnitudes of reductions were smaller and not statistically significant.
Table 9.
Results from the Mediation Analysesa for ER Visits between GMCs and CTRLs
a The model was adjusted for age groups, sex, race/ethnicity, language speaking, number of comorbidities in baseline years, the county, year-specific smoking, depression, number of doctor visits, and CDPS scores, plus census track-level SVI variables: percentage of unemployed (age 16+), persons below poverty estimates, minority, and households with no vehicle available.
b Numbers are estimates comparing changes in ER visits between corridors each post-policy year vs. the baseline years (3 years before the implementation of the policy) for a composite change of one unit reduction in NO2 and one unit reduction in PM2.5 from the pre-policy years to the post-policy years. Post 3rd year denotes the policy effect three years after GM actions. CI entries refer to 95% confidence intervals.
Causal Inference Results Via DiD Models with Inverse Probability of Treatment Weighting
To further verify the causal inferences of the GM regulations on the improvement of concentrations and health outcomes, we performed similar analyses described above inverse probability of treatment weights obtained from propensity scores. The weights effectively balance the intervention and comparison groups based on their baseline characteristics, including sex, age groups, number of comorbidities in baseline years, and annual log-transformed CDPS scores (Appendix 3, Table A3-8). Propensity score methods (e.g., weighting) are often used in quasi-experimental research to reduce selection bias that could create differences between the intervention and the control groups in key characteristics that might be associated with both the intervention and the outcome. Without propensity score methods, the validity of inference from the models specified in the equations could be compromised because of failure to account for key confounders at baseline. Inverse probability weighting balances the treatment with the control group by giving more weight to those predicted to be less likely to be in the treatment group, and less weight to those predicted to be more likely to be in the treatment group. Estimates from this method are consistent with other bias-adjusted weighting estimators as well.
The propensity score weighting created a relative balance of key baseline characteristics in the GMCs and CTRLs. The details of descriptive statistics after the propensity score weighting for all beneficiaries and by asthma and COPD status are shown in Table A3-8 in Appendix 3. After the weighting, the results from the DiD models are consistent with the DiD results without weighting (Table 10 vs. Table 8).
Table 10.
Difference-in-Differences Estimates for ER Admissions between GMCs and CTRLs, after Propensity Score Weightinga
a Estimates are from the primary DiD model after propensity score weighting.
Changes in Hospitalization
There were also some downward trends for hospitalization for those living in GMCs than those in CTRLs in the post-years, but the magnitude of reductions was small (up to less than 4%) and the reductions were not statistically significant (Appendix 3, Table A3-9). There were also similar downward trends of hospitalization for those living in GMCs than for those in NGMCs in the post-years (up to less than 6%); for those living in NGMCs than for those CTRLs in the post-years (up to less than 3%) and they were all not statistically significant (Appendix 3, Table A3-9). We also did DiD analyses with additional controls for PM2.5, NO2, and O3. The results are identical (Appendix 3, Table A3-10).
DISCUSSION AND CONCLUSIONS
CHANGES IN AIR QUALITY AND HEALTH DUE TO GM POLICY ACTIONS
We observed significant reductions in pollutant concentrations for enrollees in 10 California counties for NO2 and PM2.5 for all three location domains. The GM policy actions, however, led to the largest reduction in and PM2.5 concentrations for those in GMCs versus those in CTRLs; followed by those in NGMCs versus in CTRLs. The differences between GMCs and NGMCs were the smallest in the post-policy years. As a result, the levels of exposure to NO2 for those living in GMCs were similar to those of NGMCs and CTRLs in the post-policy periods. The magnitudes of PM2.5 reductions were smaller in comparison with NO2 across all two-way corridor comparisons. The explanations for our findings are threefold. One is that the NGMCs are geographically closer to the GMCs, so there are more spill-over effects of the GM policy actions. The second is that in addition to GM policy actions, there are other regulatory policies and emissions reduction strategies developed to address California’s air quality during this period, including the low-emission vehicle (LEV) program, which will drastically reduce emissions from passenger cars, light-duty trucks, and medium-duty trucks. The fuel reformulation programs in the 2000s may have been especially important in this period. The LEV program, fuel reformulations, and other measures targeting light-duty vehicle (LDV) emissions and large stationary sources may all play a role in the air quality improvement in the NGMCs and CTRLs (Gilliland et al. 2017; Lurmann et al. 2015). Third, NO2 is emitted largely by roadway traffic (CARB 2020a; Cox 1999). NO is produced in much greater quantities than NO2, but it oxidizes to NO2 quickly in the atmosphere (Cox 1999; U.S. EPA 2016). The levels of NO2 generally decrease to background level 200–500 m away from major roadways (Brugge et al. 2015; Hagenbjörk-Gustafsson 2014; Pasquier and André 2017). NO2 is much higher in the vicinity of major roadways than in regional background locations (Cox 1999). The regulatory policy implemented by CARB significantly reduced NO2 emissions from roadway traffic and directly resulted in the overall reductions in regional NOx levels. In California, the source contribution of ambient PM2.5 is mainly roadway traffic (CARB 2020b; Hodan and Barnard 2004). There are other point or regional source contributions, such as residential cooking, smoke from wood burning, power plants, wildfires, agricultural burning, and dusts (CARB 2020b). The majority of PM2.5 mass is formed via secondary reactions in the atmosphere (Hodan and Barnard 2004). These secondary particles typically produce a more homogeneous spatial distribution pattern (Pasquier and André 2017) than primary particles, such as those emitted directly from roadway combustion sources. The spatial gradients of PM2.5 are much less pronounced than those for NOx. The significant reductions in roadway primary PM2.5 emissions from the CARB regulatory policy implementation were likely partially offset by the contributions from the secondary reactions and other sources of emissions and did not result in immediate significant reductions in the regional levels of PM2.5 (Pasquier and André 2017). Continued implementation of the regulatory policy gradually brought the secondary PM2.5 levels down by reducing the primary sources of PM2.5 emissions from roadway traffic and by reducing precursors to secondary PM formation such as NOx.
Various statistical modeling methods used in our study all consistently showed significantly greater reductions in ER visits for those with asthma and COPD living in GMCs compared with those living in CTRLs. Given that the study population is comprised of adults with chronic conditions, it is expected that the study participants might have higher health services usage due to aging and the natural course of development of their chronic conditions as we observed in the CTRL groups (Agarwal et al. 2017). In contrast, for those in GMCs, we observed statistically significant reductions. These results suggest that beneficiaries with asthma and COPD in GMCs benefited from the pollution reductions due to GM policy actions. It indicates that the GM regulations contributed to a greater reduction in the number ER visits for participants living in GMCs. For example, we saw in the DiD modeling results there were 170 fewer ER visits for 1,000 beneficiaries with asthma per year in GMCs if the regionwide trend in the CTRL group was considered not related to the GM policy. Similarly, among the beneficiaries with COPD, there were 180 fewer ER visits per 1,000 patients estimated in the GMCs for the third year after the implementation of the policy. Using the mediation models, we observed 129 fewer ER visits for 1,000 beneficiaries with asthma in all post-policy years per unit reductions in NO2 and PM2.5. Although GM and other interventions can theoretically affect health outcomes in a myriad of ways, the mediation modeling results provided empirical evidence that the effects of GM policy interventions on health improvements are largely due to exposure reductions. In other words, the findings have contributed to the scientific evidence regarding causal relationships between GM policy actions and the reductions in air pollution that led to subsequent improvements in health.
Few previous studies evaluated whether reductions in air pollution levels led to reductions in ER visits or hospitalizations. However, numerous studies have established the links between adverse health effects and traffic-related pollutant exposures among individuals with chronic respiratory diseases (e.g., asthma and COPD) (Cirera et al. 2012; Hesterberg et al. 2009). Such pollutants are more likely to be deposited in the lungs of those with asthma or COPD than in the lungs of healthy people, which makes them more susceptible to the exposures (Chalupa et al. 2004; Kim and Kang 1997; Svartengren et al. 1991). Compared with changes in the number of ER visits for asthma and COPD patients, we did not see the statistically significant changes in ER visits for those with diabetes and heart disease, although the general trend toward reduced admissions was present in these groups as well. There are emerging evidence for a connection between type 2 diabetes and air pollution (Bhatnagar 2009; Brook et al. 2008; Eze et al. 2015) and death for those with cardiovascular diseases.
These findings also showed that reducing air pollution might have an additional beneficial effect on reducing health inequalities between more- and less-advantaged groups. Although all of our study subjects were of low income (a requirement to qualify for Medi-Cal), those living in the CTRLs and NGMCs generally had lower exposures and lower rates of ER visits at the beginning of the study than those subjects living in the GMCs. As the effects of the policy persisted into years 2 and 3 of the post-intervention period, both the exposure and health disparities among the control groups and the GMC intervention group tended to decrease. These observed phenomena are promising to shed a light on eliminating health inequities by reducing unequal exposures to environmental hazards. Our study population is more susceptible to air pollution due to chronic disease conditions than the general population, and their low SES probably made them more susceptible to pollutants due to greater vulnerability resulting from higher co-exposures, higher rates of obesity, potentially less nutritious diets, and worse access to quality Medi-Cal care (Bravo et al. 2016; Clark et al. 1999; Hajat et al. 2015; Morello-Frosch et al. 2011; Mortimer et al. 2002; Ostro et al. 2001; Ou et al. 2008; Perera et al. 2002; Su et al. 2012). Previous studies have shown that low SES is a twofold problem; it is associated with living in areas with increased pollution, and it makes individuals more susceptible to pollutant effects (Lipfert 2004; O’Neill et al. 2003; Sexton and Adgate 1999). A previous study by the principal investigator and coauthors showed that the high prevalence of frequent asthma symptoms among low income Californians was related to both higher traffic-related pollution exposures and increased susceptibility due to differences in overall health status and access to care. Additionally, those living in poverty appeared to be more strongly affected by heavy traffic near their residences than those living above poverty (Meng et al. 2008). The findings of this study, however, indicated that those more exposed and susceptible or vulnerable also potentially benefit the most from the exposure reductions, such as those living in GMCs. The findings suggest that significant health benefits accrued for disadvantaged groups by targeting GM as a key source of emissions reduction. As a corollary, GM regulations may serve to reduce persistent health disparities among different social groups, which result in part from the unequal distribution of exposures to air pollution and other environmental stressors.
STRENGTH AND LIMITATIONS OF THE STUDY
A need exists for a systematic approach to evaluate the impact of air quality regulations and policies on public health, especially when focusing on susceptible and vulnerable populations. The concurrent availability of geocoded Medi-Cal claims data for a large vulnerable population (Medi-Cal enrollees with chronic diseases), an extensive air monitoring network, and rich supplementary data for the targeted counties (especially in Los Angeles and Alameda counties), as well as our LUR models, made it possible for us to assess changes in pollutant exposures and related health impacts due to air quality regulations.
One strength of the study is that we built annual LUR models and associated surfaces to coincide with the annual health outcomes. It is well known that typical LUR models predict long-term pollutant concentrations with a single surface and those LUR models tend to overfit (Su et al. 2015a). We used a v-fold cross-validation strategy in our deletion/substitution/addition modeling to improve reduce overfitting, that is, using a subset of the original dataset model development (Beckerman et al. 2013; Su et al. 2015a), and we considered the repeated measure effects. To adequately address possible concerns over using sparse government monitoring sites to identify GM regulation effects, we also conducted two new rounds of field sampling focusing on NOx in the counties of Los Angeles and Alameda in Phase I. The LUR modeling process integrated data from both government regulatory monitoring and the research-oriented saturation monitoring into a single modeling framework. All these efforts improved our model for out-of-sample prediction locations, which enabled us to accurately predict annual concentrations of the pollutant of interest in the study region.
The second strength of our study is that we used longitudinal claims data to create a study cohort with six years of data to examine the health effects of air pollution reduction programs. More importantly, unlike other U.S. studies that used administrative data at the ZIP code resolution (Di et al. 2017), we were able to obtain data with the residential home address, which allowed us to estimate fine-scale variations in pollution and proximity to GM areas. We were able to structure our analyses within three well defined study areas that realistically reflected exposure gradients (GMCs, NGMCs, and CTRLs), which allowed us to compare changes in concentrations/exposures and health outcomes in all three domains. The classification of GMCs allowed us to identify changes in subregions that were closely related to GM policies versus changes in NGMCs that have occurred on non-truck freeways that would be most likely attributable to broader mobile emission reduction policies versus changes that have occurred in control areas likely due to regional emissions reductions policies.
The third strength is that by using Medi-Cal enrollment and claims data we created a cohort to account for common risk or modifying factors when examining associations between air quality improvement and the decrease in adverse health outcomes. We developed and tested confounding or time-varying variables (e.g., access to primary care, changes in disease severity, or development of comorbidities, depression and smoking) that may influence changes in health outcomes. In addition to those variables, we constructed individual-level socioeconomic variables that included age, sex, race/ethnicity (white, Latino, African American, Asian and Pacific Islander, and others), and spoken languages (English and non-English speaking). Our study also took into consideration concomitant changes in population and economic factors (e.g., economic downturn using unemployment rates and percentages of populations below poverty) at the neighborhood levels. The design increased the internal validity of the findings.
Furthermore, we used more modern and forward thinking statistical approaches for accountability studies, specifically including a quasi-experimental design with well-defined intervention and control groups, which has not been commonly done before in accountability studies for the air pollution regulatory literature; (2) directly assessing whether the difference in pollution is attributable to the policy intervention and contributing to specific health improvements in the intervention group compared with the controls; and (3) comparing the results generated in methods (1) and (2) with more conventional causal mediation methods. We established causality in our observational studies by evaluating natural experiments via DiD-based models with parallel-trends assumption. We utilized an observed control group (or more precisely, a “quasi-control” group), which should exhibit similar health trends when compared to the intervention group in the absence of policy intervention. Such natural or quasi-experimental designs aid in establishing causality when randomization is not practical or ethical, such as in GM policy actions.
Ideally, one would establish causality by conducting a randomized control trial, where, for example, individuals would be randomly assigned to live in an exposed (intervention) area such as GMCs or an unexposed (control) area for an extended period of time. We could then observe changes in health for the two groups. If the more highly exposed group showed greater changes related to a particular health parameter, such as ER visits, one might infer that the associated elevated exposures were the cause. Due to randomization, we would expect the two groups to be the same with regard to confounder variables, with the only difference being due to “intervention” or exposure levels. Such randomization, however, would be unethical given the likely harm that could be caused and extremely impractical and expensive to implement. In the absence of such a randomized design, we fit regression-based models in with a quasi-experimental design, which “adjust” for a variety of confounders in an attempt to tease out the effect of the exposure-based variables of interest by relying on the parallel trend assumption. Given that all participants were Medi-Cal beneficiaries we can assume any Medi-Cal related policy changes or public health interventions may affect those in three corridors equally. If there are any county-level interventions, the inclusion of county as a fixed effect may help adjust for unmeasured exogenous factors at the county level. We also controlled for neighborhood SES (e.g., economic downturn using unemployment rates and percentages of populations below poverty) . With all these efforts, we may still not be able to control all other exogenous factors. There might be potential unmeasured confounding remaining, especially at the neighborhood or household level (e.g., installing air filters for the public housings near freeways), which might distort the results by violating the parallel trends assumption though we are not aware of these kinds of interventions.
We are aware of current concerns regarding the use and misuse of P values to make binary statements regarding the “statistical significance” of interventions, especially with regard to the rejection of infeasible “straw man” null hypotheses (Amrhein et al. 2019). These concerns are relevant to our work, as a statistically significant effect refers to the rejection of a null hypothesis of zero policy effect, and it is difficult to imagine that a policy intervention would have absolutely zero effect on exposure–health reduction. As such much of our work includes graphs and confidence intervals that address questions related to the extent to which policy interventions cause changes in concentration levels and the extent to which such interventions improve health, as opposed to binary, yes/no questions regarding effect versus no-effect. Further efforts — especially with regard to the development of methods to examine spatially varying causal effects — need to be developed as this would allow for a more targeted policy-based approach to pollutant concentration reduction and health improvement.
This study also takes advantage of the completeness of FFS claim data, which has already been thoroughly vetted and combined with real-time eligibility and demographic data. However, we only had up to two diagnostic codes for each encounter, so we might not have had a complete picture of comorbidities. Nevertheless, that limitation may have affected the intervention and control groups in similar ways. We also had the beneficiaries’ addresses at the beginning of the study. Based on data from the California Health Interview Survey 2009, 54% of Medi-Cal respondents have lived at current residence for 5 years or more in our study counties. It is unknown whether they moved within the corridors or out of the corridors, so the impact on our results is unknown. We mainly relied on residence-based air pollution exposure estimates, which allowed us to conduct the small-area analyses, but we lacked information on other potentially important micro-environments because the claims data did not collect information on beneficiaries’ work locations or time spent in other environments. Thus, similar to most observational studies of air pollution health effects, our exposure measures did not consider interindividual variability in exposures due to personal mobility, indoor, commuting, and occupational exposures. Previous cohort studies, however, that included multiple communities assigned exposure based on community-average pollution concentrations and considered long-term health effects have shown that the results are relatively unaffected by a lack of personal exposure measures (Berhane et al. 2004). People in high income countries tend to spend the majority of their time indoors, and thus exposure to outdoor air pollution is modified by time spent indoors. One important factor influencing indoor and personal exposures to pollutants is the fraction of outdoor air that penetrates indoors, which is a function of pollutant type and home ventilation characteristics, including the use of air conditioning. The use of air conditioning depends heavily on meteorology and topographic conditions of an area; for example, residents of coastal areas are less likely to use air conditioning. Indoor pollutant exposures may be elevated in low-income housing due to multiple sources, such as cigarette smoking, mold, and gas appliance combustion, and small apartment sizes (Zota et al. 2005). For example, levels of NO2 and CO were substantially higher in low income, inner-city residences relative to the U.S. average (Schwab 1990). Additionally, exposures to cockroaches, dust mites, and fungal allergens that are believed to induce asthma symptoms (Zhong 1996) are more common in households with generally poor living conditions (Sarpong et al. 1996). In addition, we did not have data on all the other possible asthma triggers, such as the age of housing, mold, dust mites, and the use of gas appliances. As a result, we could not control for these possible triggers in this study, but this would only affect statistical inference if these indoor exposures differed substantially across the three study domains.
IMPLICATIONS OF FINDINGS
Our findings indicated that the adoption and implementation of emission control strategies specific to the GM sector have resulted in significant emissions reductions, which resulted in the reductions of NO2 exposures for vulnerable populations. The proportionately higher reductions in the GMCs suggest the potential for regulatory actions to benefit all groups, but particularly those in high exposure areas. This finding suggests that properly targeted regulations may also reduce environmental exposure inequalities in traffic-related air pollution.
Our findings add to empirical evidence that air pollution control actions reduce pollution exposures. More importantly, our findings suggest that the reductions in air pollution led to health outcome improvements among the vulnerable population with chronic conditions in the state with some of the largest goods-movement corridors in the world. The findings have strengthened the evidence for the reduction of adverse health effects through air pollution control, supporting the case for further regulatory actions. The findings can be generalized to the similar vulnerable populations in other parts of the country and world because some pollutants (e.g., NOx, NO2, and PM2.5) will likely have similar effects across the populations. California has one of the largest, most ethnically diverse populations in the United States and covers geographic areas with both high and low air pollution levels in comparison with the rest of the nation. Therefore, the observed associations between pollutant reductions and improvements in health outcomes of the vulnerable population with chronic conditions may apply to different parts of the country and the world.
Our investigation also contributed to scientific methods for assessing the health effects of long-term, large scale, and complex regulatory actions with routinely collected pollutants and Medi-Cal claims data. Few studies to date have used geocoded longitudinal claims data to examine health effects from air pollution reduction programs. The study also contributed to the development of methods for conducting such evaluations. This study also showed the adequacy of using routinely and continuously collected Medi-Cal claims data to identify and monitor chronic diseases and to correlate them with policy, environmental, behavioral, health access, and demographic factors; that is, to evaluate the usefulness of Medi-Cal claims data as a surveillance and policy assessment tool in public health. The results can also help identify important confounders to adjust for when developing these outcome indicators, for example, access to care and severity of the disease.
ER visits are usually very costly. The reductions in ER visits could greatly reduce costly Medi-Cal expenditures. The health care delivery system can use this information to help providers identify opportunities for interventions. Understanding the independent contribution of air pollution compared with other patient-level risk factors will be crucial for managing high-risk populations through better care coordination and case management as well as developing a risk-based payment system. Most Medicaid beneficiaries are likely to still reside in similar locations examined in this study and face the same issues, such as air pollution exposures. Therefore, the health of the beneficiaries with chronic conditions is still compromised due to air pollution exposures or lack of access to quality care. This study provides pertinent information that Medi-Cal can leverage to promote enhanced risk management and care coordination for beneficiaries with complex health care needs; thus, managed care plans and providers can use this information to improve the effectiveness of care for these patients at high risk. Health care authorities, such as the Centers for Medicare & Medicaid Services, can set additional guidelines for health plans to add pollution profile (geography) in the care of beneficiaries at high-risk of adverse outcomes. This will lead to better risk assessments and management for potential “hot spots” of utilization, such as areas with higher ER visits or hospitalization. They can also use this information to educate providers for improving the effectiveness of care for these patients at high risk.
This project has produced empirical evidence that air pollution control actions reduced pollution exposures among disadvantaged and susceptible populations. More importantly, our findings suggest that the reductions in air pollution led to health outcome improvements among low-income people with chronic conditions. Our investigation also contributed to scientific methods for assessing the health effects of long-term, large-scale, and complex regulatory actions with routinely collected pollutants and Medi-Cal claims data. Therefore, the results strongly support both short-term and long-term efforts to improve air quality for all members of society and future studies on the impact of air pollution control policies.
ACKNOWLEDGMENTS
This project was performed under a contract with the Health Effects Institute (# 4950-RFA11-1/16-1). We thank the families, staff, and administrators at the UCLA Center for Health Policy Research, without whom this project would not have been possible. We especially thank the staff of the California Department of Health Services and CARB for their efforts in providing us the data. We also thank the HEI staff and Research Committee Members for their guidance and support during the project. The authors have considered their activities and report no conflicts of interest. The contents of this report are solely the responsibility of the authors and do not necessarily represent the official views of the funding agencies who have provided the support.
Footnotes
* A list of abbreviations and other terms appears at the end of this volume.
HEI QUALITY ASSURANCE STATEMENT
The “Improvements in air quality and health outcomes among California Medicaid enrollees due to goods movement actions” study contains a unique dataset for investigating the health effects of air pollution in a state with some of the largest goods-movement corridors in the world. The conduct of this research project was subject to independent quality assurance (QA) oversight by an audit team from Sonoma Technology, Inc., and the University of Washington. The audit team consisted of Dr. Michael McCarthy with expertise in quality assurance planning and exposure assessment; Dr. Adam Szpiro who was the primary biostatistician and environmental epidemiologist; and Mr. Fred Lurmann with expertise in exposure modeling and land-use regression modeling. Mr. Bryan Penfold also assisted in GIS processing of land-use data in the final off-site audit. The QA oversight consisted of an on-site meeting and an audit of the Draft Final Report and underlying methodology. The dates of the audits and reviews are listed below.
Onsite Audit, June 2018
The audit team conducted an on-site audit at the University of California, Los Angeles, on June 20, 2018. McCarthy and Lurmann of the audit team visited in person, and Szpiro attended remotely via conference call. The audit team reviewed the following study components: study protocol, Institutional Review Board (IRB) documents, data management and storage standard operating procedure, statement of work, progress reports, study presentations, feedback letters from site visits, and a methods letter. Data security, management, and transfer protocols were extremely well considered. Study investigators demonstrated the file structure in the secure workstation room. Network structures were clear, well organized, and self-documenting. Ownership of files was clear through the network file-naming protocols implemented. Review procedures for displaying health data were clear and also self-documenting. The audit team had no recommendations for the team regarding the data security or data management protocols at UCLA. The audit team reviewed methods for land use regression and statistical modeling, but no interim or final code or datasets were provided for review during the on-site audit. No errors were noted, but recommendations were made for documenting organizational roles and QA/QC procedures and clarifying methodological steps.
Final Remote Audit (October 2020–March 2021)
The final remote audit consisted of three parts: (a) multiple calls with study investigators to document source data and codes, (b) audit of data-processing steps, and (c) review of the UCLA Draft Final Report for the project. The final remote audit focused on documenting the steps to demonstrate reproducibility and transparency of processing steps used to produce primary tables and figures supporting the findings of the final study. Not all portions of the study could be remotely accessed and so the audit team focused on code review of the sections of the Draft Final Report.
The audit of the data included study documentation; review of SAS, STATA, and R scripts; land-use regression modeling audits; and statistical review. The code review included reviewing scripts for data import, processing, reduction, modeling, and analysis. Due to the limited on-site audit of the scripts in 2018, this remote audit reviewed each of the sections of code for the first time. The audit focused on key steps for selecting data participants, linking pollutant information, reproducing subsets of the land-use regression modeling results, checking the statistical codes and outputs and matching them to Draft Final Report results, and identifying any gaps between steps. Due to restrictions on health data, it was not possible to reproduce or independently audit the portions of the study involving participants.
No major quality issues were discovered in the final remote audit. A few minor discrepancies and typos were identified and communicated to study investigators. Minor corrections or changes were recommended to clarify these discrepancies. Written reports of each audit were provided to HEI. These quality assurance audits demonstrate that appropriate steps were taken to validate, audit, and review the study procedures. To the extent possible, the audit team is confident that the final remote audit demonstrates that the study followed a valid, transparent, and reproducible set of procedures. The UCLA Draft Final Report appears to be an accurate representation of the underlying procedures and methods used to generate the findings and conclusions.
Ying-Ying Meng, DrPH, the principal investigator on this project, is a senior research scientist and codirector of the Chronic Disease Program at the University of California, Los Angeles Center for Health Policy Research. Meng received doctoral and master’s degrees in health policy and administration from the University of California, Berkeley. She has focused her research on disparities in health and healthcare among vulnerable populations, such as the elderly and children, women, racial/ethnic minorities, and those with low income or chronic disease. She has been a principal investigator for numerous multiyear epidemiological studies on the health effects of air pollution and a lead evaluator for intervention projects funded by federal and state agencies. In these epidemiological and intervention studies, she examined the relationship of social positions (e.g., low income and minority status), neighborhood factors (e.g., traffic/air pollutants near homes and access to care), and health behavior (e.g., smoking) with morbidity of chronic conditions such as asthma, diabetes, and obesity. Meng has led and published research in scholarly publications, including studies with cutting-edge methodologies, such as hierarchical models, small-area estimations, and using geographic information systems for health service research. As codirector of the Chronic Disease Program, Meng has established the Center as a recognized source of important analysis of population-based data to understand the relationship between physical and social environments and chronic disease morbidity.
Jason G. Su, PhD, an associate researcher at the University of California, Berkeley, received a postdoctoral fellowship in exposure assessment and environmental health at UC, Berkeley and a postdoctoral fellowship in exposure assessment and environmental health at the University of British Columbia, Vancouver, Canada. He received a PhD in human and economic geography (minor GIS) from the Chinese Academy of Sciences, Beijing, China, and a PhD in rangeland and wildlife resources management (minor remote sensing of environment) from the University of Alberta, Edmonton, Canada. Su applies multi-petabyte catalogs of satellite imagery and geospatial datasets for planetary-scale analysis of Earth’s surface environments, including air pollution, weather, and climate; land use; and land cover through Google Earth Engine. He developed land-use regression modeling algorithms that incorporate multiple types of measurements into a single modeling frame for the purpose of creating high spatial (e.g., 30 m) and temporal (e.g., daily, monthly, and annual) resolution air pollution surfaces. Su has also conducted biostatistics and machine learning analyses investigating associations of adverse health outcomes, especially respiratory diseases with harmful environmental exposures.
Xiao Chen, PhD, is the associate director of the Health Economics and Evaluation Program at the University of California, Los Angeles Center for Health Policy Research. Her doctoral degree is in mathematics from the University of Virginia. She manages data analysis for the UCLA Center’s Health Economics and Evaluation Research Program and provides support in statistical programming, data management, and statistical modeling in the area of health economics and program evaluation. Before joining the Center, Chen was a senior statistical consultant and the manager of the UCLA/ATS Statistical Consulting Group. She worked with many UCLA researchers on various data management issues and statistical modeling techniques, including linear and generalized linear multilevel models, structural equation modeling, latent variable models, multiple imputations and Monte Carlo simulation. Chen wrote numerous web pages for the well-known ATS/Stat group website on various topics including statistical computing and modeling, as well as many SAS and Stata programs for UCLA researchers.
John Molitor, PhD, is a tenured associate professor at Oregon State University. He is originally from the Greater St. Louis area and received his doctoral degree in mathematical statistics from the University of Missouri, Columbia, in 1999. Since then he worked as a senior statistical programmer at Muthén & Muthén, a small software firm in Los Angeles (2001), as a post-doctoral fellow and researcher at the University of Southern California (2001– 2006), as a lecturer (U.S. assistant professor) at Imperial College, London (2006–2011), and as an associate professor at Oregon State University since 2010. Molitor’s research interests involve Bayesian analysis, computational statistics, spatial modeling of air pollution exposures, genetic epidemiology, and causal inference. He has been lead author, near-lead author, or senior author on important high-impact publications in such journals as Hypertension, American Journal of Human Genetics, Proceedings of the National Academy of Sciences, Environmental Health Perspectives, and others. He has also been lead principal investigator on large grants related to issues such as the development of the statistical methodology to analyze multiple air pollution exposures and to examine their effects on human health.
Dahai Yue, PhD, is a health economist and assistant professor in the Department of Health Policy and Management at the University of Maryland, College Park. He received his doctoral degree in health policy and management (economics cognate) from the University of California, Los Angeles. His research focuses on deploying medicine, economic theories, and rigorous methods to understand better how social factors shape health and healthcare-seeking behaviors. The overarching goal of his research is to integrate social determinants of health into the study of healthcare delivery systems to improve care efficiency and reduce health disparities. His work has been supported by the Gilbert Foundation Research Grant and featured in top journals, including Health Affairs and Health Services Research.
Michael Jerrett, PhD, is an internationally recognized expert in geographic information science for exposure assessment and in spatial epidemiology. He is a full professor in the Department of Environmental Health Sciences, Director of the Center for Occupational and Environmental Health, and codirector of the Center for Healthy Climate Solutions, Fielding School of Public Health, University of California, Los Angeles. Jerrett earned his Ph.D. in geography from the University of Toronto. Over the past 23 years, he has researched how to characterize population exposures to air pollution and built environmental variables, the social distribution of these exposures among different groups (e.g., poor vs. wealthy), and how to assess the health effects from environmental exposures. He has worked for many years on how the built environment affects exposures and health, particularly the roles parks and green spaces play on physical activity promotion and obesity prevention. He has also published extensively on air pollution and climate change, including wildfires, vulnerability to heat stress, and public health co-benefits of climate change mitigation. He has published some of the most widely cited papers in the fields of exposure assessment and environmental epidemiology in leading journals, including The New England Journal of Medicine, The Lancet, Proceedings of the National Academy of Science of the United States of America, and Nature. He serves as a standing member of the Health Effects Institute Review Committee and as an editorial board member for the Annual Review of Public Health and Environmental Research. He recently completed a 3-year term on the Geographical Sciences Committee of the U.S. National Academy of Sciences.
OTHER PUBLICATIONS RESULTING FROM THIS RESEARCH
Su JG, Meng YY, Pickett M, Seto E, Ritz B, Jerrett M. 2016. Identification of effects of regulatory actions on air quality in goods movement corridors in California. Environ Sci Tech 50:8687–8696.
Su JG, Meng YY, Chen X, Molitor, J. Yue D, Jerrett M. 2020. Predicting differential improvements in annual pollutant concentrations and exposures for regulatory policy assessment Environment Intl 143:105942.
Meng YY, Yue D, Molitor J, Chen X, Su JG, Jerrett M. Air quality and health improvements resulting from goods movement policies in California: A quasi-experimental study. Submitted to Lancet Planetary Health (in review).
REFERENCES
Agarwal P, Bias TK, Sambamoorthi U. 2017. Longitudinal patterns of emergency department visits: A multistate analysis of Medicaid beneficiaries. Health Serv Res
52:2121–2136. [DOI] [PMC free article] [PubMed] [Google Scholar]
Amrhein V, Greenland S, McShane B. 2019. Scientists rise up against statistical significance. Nature
567:305–307. [DOI] [PubMed] [Google Scholar]
Andersen ZJ, Hvidberg M, Jensen SS, Ketzel M, Loft S, Sørensen M, et al. 2011. Chronic obstructive pulmonary disease and long-term exposure to traffic-related air pollution: A cohort study. Amer J Res Crit Care Med
183:455–461. [DOI] [PubMed] [Google Scholar]
Asparouhov T. 2006. General multi-level modeling with sampling weights. Comm Stat — Theory Meth:439–460. [Google Scholar]
Bagliano FC, Morana C. 2012. The great recession: US dynamics and spillovers to the world economy. J Bank Financ
36:1–13. [Google Scholar]
Beckerman BS, Jerrett M, Serre M, Martin RV, Lee S-J, van Donkelaar A, et al. 2013. A hybrid approach to estimating national scale spatiotemporal variability of PM2.5 in the contiguous United States. Environ Sci Tech
47:7233–7241. [DOI] [PMC free article] [PubMed] [Google Scholar]
Berhane K, Gauderman WJ, Stram DO, Thomas DC. 2004. Statistical issues in studies of the long-term effects of air pollution: The Southern California Children’s Health Study. Stat Sci
19:414–449. [Google Scholar]
Bhatnagar A. 2009. Could dirty air cause diabetes?
Circulation
119:492–494. [DOI] [PubMed] [Google Scholar]
Billings J, Zeitel L, Lukomnik J, Carey TS, Blank AE, Newman L. 1993. Impact of socioeconomic status on hospital use in New York City. Health Aff (Millwood)
12:162– 173. [DOI] [PubMed] [Google Scholar]
Binder DA. 1983. On the variances of asymptotically normal estimators from complex surveys. International Statistica Review/Revue Internationale de Statistique
51:279–292. [Google Scholar]
Bindman AB, Chattopadhyay A, Auerback GM. 2008. Interruptions in Medicaid coverage and risk for hospitalization for ambulatory care-sensitive conditions. Ann Intern Med
149:854–860. [DOI] [PubMed] [Google Scholar]
Blaszczak RJ. 1999. Nitrogen Oxide (NOx), Why and How They Are Controlled. Technical Bulletin, US Environmental Protection Agency. [Google Scholar]
Boogaard H, van Erp A, Walker K, Shaikh R. 2017. Accountability studies on air pollution and health: The HEI experience. Curr Environ Health Rep
4:1–9. [DOI] [PubMed] [Google Scholar]
Bravo MA, Anthopolos R, Bell ML, Miranda ML. 2016. Racial isolation and exposure to airborne particulate matter and ozone in understudied US populations: Environmental justice applications of downscaled numerical model output. Environ Int
92:247–255. [DOI] [PubMed] [Google Scholar]
Brook RD, Jerrett M, Brook JR, Bard RL, Finkelstein MM. 2008. The relationship between diabetes mellitus and traffic-related air pollution. J Occup Environ Med
50:32–38. [DOI] [PubMed] [Google Scholar]
Brugge D, Patton AP, Bob A, Reisner E, Lowe L, Bright OJM, et al. 2015. Developing community-level policy and practice to reduce traffic-related air pollution exposure. Environ Justice
8:95–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
Burns J, Boogaard H, Polus S, Pfadenhauer LM, Rohwer AC, van Erp AM, et al. 2019. Interventions to reduce ambient particulate matter air pollution and their effect on health. Cochrane Database Syst Rev
5(5):CD010919; doi:10.1002/14651858.CD010919.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Carle AC. 2009. Fitting multilevel models in complex survey data with design weights: Recommendations. BMC Med Res Meth
9.1:49. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cassedy A, Fairbrother G, Newacheck PW. 2008. The impact of insurance instability on children’s access, utilization, and satisfaction with health care. Ambulatory Pediatrics
8(5);321–328. [DOI] [PubMed] [Google Scholar]
Catalano R. 2009. Health, Medi-Cal care, and economic crisis. N Engl J Med
360:749–751. [DOI] [PubMed] [Google Scholar]
Chalupa DC, Morrow PE, Oberdörster G, Utell MJ, Frampton MW. 2004. Ultrafine particle deposition in subjects with asthma. Environ Health Perspect
112:879–882. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cirera L, García-Marcos L, Giménez J, Moreno-Grau S, Tobías A, Pérez-Fernández V, et al. 2012. Daily effects of air pollutants and pollen types on asthma and COPD hospital emergency visits in the industrial and Mediterranean Spanish city of Cartagena. Allergologia et Immunopathologia
40:231–237. [DOI] [PubMed] [Google Scholar]
Clark N, Brown R, Parker E, Robins T, Remick DJ, Philbert M, et al. 1999. Childhood asthma. Environ Health Perspect
107:421–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
Di Q, Dominici F, Schwartz JD. 2017. Air pollution and mortality in the Medicare population. N Eng J Med
377:1498–1499. [DOI] [PubMed] [Google Scholar]
Eze IC, Hemkens LG, Bucher HC, Hoffmann B, Schindler C, Künzli N, et al. 2015. Association between ambient air pollution and diabetes mellitus in Europe and North America: Systematic review and meta-analysis. Environ Health Perspect
123:381–389. [DOI] [PMC free article] [PubMed] [Google Scholar]
Flanagan BE, Gregory EW, Hallisey EJ, Heitgerd JL, Lewis B. 2011. A social vulnerability index for disaster management. J Homeland Security Emergency Management
8(1). doi: 10.2202/1547-7355.1792 [Google Scholar]
Gilliland F, Avol E, McConndell R, Berhane K, Gauderman W, Lurmann F. 2017. The Effects of Policy-Driven Air Quality Improvements on Children’s Respiratory Health. Research Report 190. Boston, MA:Health Effects Institute. [PMC free article] [PubMed] [Google Scholar]
Greene WH. 2003. Econometric Analysis. Pearson Education India. [Google Scholar]
Hagenbjörk-Gustafsson A. 2014. Validation of diffusive samplers for nitrogen oxides and applications in various environments. Umeå, Sweden:Umeå University. [Google Scholar]
Hajat A, Hsia C, O’Neill MS. 2015. Socioeconomic disparities and air pollution exposure: A global review. Curr Environ Health Rep
2:440–450. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hall AG, Harman JS, Zhang J. 2008. Lapses in Medicaid coverage: Impact on cost and utilization among individuals with diabetes enrolled in Medicaid. Med Care
46:1219–1225. [DOI] [PubMed] [Google Scholar]
HEI Panel on the Health Effects of Traffic-Related Air Pollution. 2010. Traffic-Related Air Pollution: A Critical Review of the Literature on Emissions, Exposure, and Health Effects. Special Report 17. Boston, MA:Health Effects Institute. [Google Scholar]
Henneman LRF, Liu C, Mulholland JA, Russell AG. 2016. Evaluating the effectiveness of air quality regulations: A review of accountability studies and frameworks. J Air Waste Manage Assoc
67:144–172. [DOI] [PubMed] [Google Scholar]
Hesterberg TW, Bunn WB, McClellan RO, Hamade AK, Long CM, Valberg PA. 2009. Critical review of the human data on short-term nitrogen dioxide (NO2) exposures: Evidence for NO2 no-effect levels. Crit Rev Toxicol
39:743– 781. [DOI] [PubMed] [Google Scholar]
Hodan WM, Barnard WR. 2004. Evaluating the contribution of PM2.5 precursor gases and re-entrained road emissions to mobile source PM2.5 particulate matter emissions. MACTEC Federal Programs, Research Triangle Park, NC. [Google Scholar]
Howell EM. 1996. Medicaid managed care encounter data: What, why, and where next?
Health Care Financ Rev
17:87–95. [PMC free article] [PubMed] [Google Scholar]
Institute of Medicine (U.S.). 1993. Chapter 2. A model for monitoring access. In; Access to Health Care in America. (Millman M, ed). Washington, DC:National Academies Press. [PubMed] [Google Scholar]
Kasper JD, Giovannini TA, Hoffman C. 2000. Gaining and losing health insurance: Strengthening the evidence for effects on access to care and health outcomes. Med Care Res Rev.
57(3):298–318. [DOI] [PubMed] [Google Scholar]
Kim CS, Kang TC. 1997. Comparative measurement of lung deposition of inhaled fine particles in normal subjects and patients with obstructive airway disease. Am J Respir Crit Care Med
155:899–905. [DOI] [PubMed] [Google Scholar]
Kronick R, Gilmer T, Dreyfus T, Lee L. 2000. Improving health-based payment for Medicaid beneficiaries: CDPS. Health Care Financ Rev
21:29–64. [PMC free article] [PubMed] [Google Scholar]
Ku L, MacTaggart P, Pervez F, Rosenbaum S. 2009. Improving Medicaid’s continuity of coverage and quality of care. Washington, D.C.: Association for Community Affiliated Plans. [Google Scholar]
Lambrew JM, DeFriese GH, Carey TS, Ricketts TC, Biddle AK. 1996. The effects of having a regular doctor on access to primary care. Med Care
34:138–151. [DOI] [PubMed] [Google Scholar]
Lipfert FW. 2004. Air pollution and poverty: Does the sword cut both ways?
J Epidemiol Comm Health
58:2–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lurmann F, Avol E, Gilliland F. 2015. Emissions reduction policies and recent trends in Southern California’s ambient air quality. J Air Waste Manag Assoc
65:324–335. [DOI] [PMC free article] [PubMed] [Google Scholar]
Meng YY, Wilhelm M, Rull RP, English P, Nathan S, Ritz B. 2008. Are frequent asthma symptoms among low-income individuals related to heavy traffic near homes, vulnerabilities, or both?
Ann Epidemiol
18:343–350. [DOI] [PubMed] [Google Scholar]
Morello-Frosch R, Zuk M, Jerrett M, Shamasunder B, Kyle AD. 2011. Understanding the cumulative impacts of inequalities in environmental health: Implications for policy. Health Aff
30:879–887. [DOI] [PubMed] [Google Scholar]
Mortimer KM, Neas LM, Dockery DW, Redline S, Tager IB. 2002. The effect of air pollution on inner-city children with asthma. Eur Respir J
19:699–705. [DOI] [PubMed] [Google Scholar]
O’Neill MS, Jerrett M, Kawachi I, Levy JI, Cohen AJ, Gouveia N, et al. 2003. Health, wealth, and air pollution: Advancing theory and methods. Environ Health Perspect
111:1861–1870. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ostro B, Lipsett M, Mann J, Braxton-Owens H, White M. 2001. Air pollution and exacerbation of asthma in African American children in Los Angeles. Epidemiology
12:200– 208. [DOI] [PubMed] [Google Scholar]
Ou CQ, Hedley AJ, Chung RY, Thach TQ, Chau YK, Chan KP, et al. 2008. Socioeconomic disparities in air pollution associated mortality. Environ Res
107:237–244. [DOI] [PubMed] [Google Scholar]
Paradise J, Garfield R. 2013. What Is Medicaid’s Impact on Access to Care, Health Outcomes, and Quality of Care?
Setting the Record Straight on the Evidence. Kaiser Family Foundation. [Google Scholar]
Pasquier A, André M. 2017. Considering criteria related to spatial variabilities for the assessment of air pollution from traffic. Transportation Research Procedia
25:3354–3369. [Google Scholar]
Perera FP, Illman SM, Kinney PL, Whyatt RM, Kelvin EA, Shepard P, et al. 2002. The challenge of preventing environmentally related disease in young children: Community-based research in New York City. Environ Health Perspect
110:197–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
Porter J, Herring J, Lacroix J, Levinton C. 2007. Avoidable admissions and repeat admissions: What do they tell us?
Healthc Q
10:26–28. [DOI] [PubMed] [Google Scholar]
Rich DQ. 2017. Accountability studies of air pollution and health effects: Lessons learned and recommendations for future natural experiment opportunities. Environ Int
100:62–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
Roorda-Knape MC, Janssen NA, de Hartog J, Van Vliet PH, Harssema H, Brunekreef B. 1999. Traffic-related air pollution in city districts near motorways. Sci Total Environ
235:339–341. [DOI] [PubMed] [Google Scholar]
Russell A, Tolbert P, Henneman L, Abrams J, Liu C, Klein M, et al.2018. Impacts of Regulations on Air Quality and Emergency Department Visits in the Atlanta metropolitan area. Research Report 195. Boston, MA:Health Effects Institute. [PMC free article] [PubMed] [Google Scholar]
Sarpong SB, Hamilton RG, Eggleston PA, Adkinson NF, Jr. 1996. Socioeconomic status and race as risk factors for cockroach allergen exposure and sensitization in children with asthma. J Allergy Clin Immunol
97:1393–1401. [DOI] [PubMed] [Google Scholar]
Schwab M. 1990. An examination of the intra-SMSA distribution of carbon monoxide exposure. J Air Waste Manag Assoc
40:331–336. [DOI] [PubMed] [Google Scholar]
Seifert R, Kirk G, Oakes M. 2010. Enrollment and Disenrollment in MassHealth and Commonwealth Care. Boston, MA:Massachusetts Medicaid Policy Institute. [Google Scholar]
Sexton K, Adgate JL. 1999. Looking at environmental justice from an environmental health perspective. J Expo Anal Environ Epidemiol
9:3–8. [DOI] [PubMed] [Google Scholar]
Sommers BD, Buchmueller T, Decker SL, Carey C, Kronick R. 2013. The Affordable Care Act has led to significant gains in health insurance and access to care for young adults. Health Aff
32:165–174. [DOI] [PubMed] [Google Scholar]
Studnicka M, Hackl E, Pischinger J, Fangmeyer C, Haschke N, Kuhr J, et al. 1997. Traffic-related NO2 and the prevalence of asthma and respiratory symptoms in seven year olds. Euro Respir J
10:2275–2278. [DOI] [PubMed] [Google Scholar]
Su JG, Hopke PK, Tian YL, Baldwin N, Thurston SW, Evans K, et al. 2015a. Modeling particulate matter concentrations measured through mobile monitoring in a deletion/substitution/addition approach. Atmos Environ
122:477–483. [Google Scholar]
Su JG, Jerrett M, Meng YY, Pickett M, Ritz B. 2015b. Integrating smart-phone based momentary location tracking with fixed site air quality monitoring for personal exposure assessment. Sci Total Environ
506:518–526. [DOI] [PubMed] [Google Scholar]
Su JG, Jerrett M, Morello-Frosch R, Jesdale BM, Kyle AD. 2012. Inequalities in cumulative environmental burdens among three urbanized counties in California. Environ Inter
40:79–87. [DOI] [PubMed] [Google Scholar]
Su JG, Meng YY, Chen X, Molitor J., Yue D, Jerrett M. 2020. Predicting differential improvements in annual pollutant concentrations and exposures for regulatory policy assessment
Environ Intl
143:105942. [DOI] [PubMed] [Google Scholar]
Su JG, Meng YY, Pickett M, Seto E, Ritz B, Jerrett M. 2016. Identification of effects of regulatory actions on air quality in goods movement corridors in California. Environ Sci Tech
50:8687–8696. [DOI] [PubMed] [Google Scholar]
Svartengren M, Anderson M, Bylin G, Philipson K, Camner P. 1991. Regional deposition of 3.6-micron particles and lung function in asthmatic subjects. J Appl Physiol
71:2238–2243. [DOI] [PubMed] [Google Scholar]
van Erp A, Cohen AJ. 2009. HEI’s Research Program on the Impact of Actions to Improve Air Quality: Interim Evaluation and Future Directions. Communication 14. Boston, MA:Health Effects Institute. [Google Scholar]
WHO (World Health Organization). 2013. Review of Evidence on Health Aspects of Air Pollution — REVIHAAP Project: Technical Report. Copenhagen, Denmark:WHO Regional Office for Europe. [PubMed] [Google Scholar]
Wooldridge JM. 2010. Econometric Analysis of Cross Section and Panel Data. Cambridge, MA: MIT Press. [Google Scholar]
Zhong NS. 1996. New insights into risk factors of asthma. Respirology
1:159–166. [DOI] [PubMed] [Google Scholar]
Zigler C, Kim C, Choirat C, Hansen J, Wang Y, Hund L, et al. 2016. Causal Inference Methods for Estimating Long-Term Health Effects of Air Quality. Research Report 187. Boston, MA:Health Effects Institute. [PubMed] [Google Scholar]
Zota A, Adamkiewicz G, Levy JI, Spengler JD. 2005. Ventilation in public housing: Implications for indoor nitrogen dioxide concentrations. Indoor Air
15:393–401. [DOI] [PubMed] [Google Scholar]
Res Rep Health Eff Inst.
Commentary by Review Committee
Research Report 205, Improvements in Air Quality and Health Outcomes Among California Medicaid Enrollees Due to Goods Movement Actions, Y-Y Meng et al.
Dr. Meng’s 4-year study, “Improvements in Air Quality and Health Outcomes Among California Medicaid Enrollees Due to Goods Movement Actions,” began in September 2012. Total expenditures were $750,867. The draft Investigators’ Report from Meng and colleagues was received for review in January 2020. A revised report, received in October 2020, was accepted for publication in December 2020. During the review process, the HEI Review Committee and the investigators had the opportunity to exchange comments and to clarify issues in both the Investigators’ Report and the Review Committee’s Commentary. As a co-investigator of the Meng report, Dr. Michael Jerrett was not involved in its evaluation by the Review Committee.
This document has not been reviewed by public or private party institutions, including those that support the Health Effects Institute; therefore, it may not reflect the views of those parties, and no endorsements by them should be inferred.
Governmental regulation is essential for protecting environmental quality and human health, but also typically incurs an economic cost. For example, the U.S. Clean Air Act and its amendments are credited with the drastic improvements in ambient air quality over the last four decades, including large reductions in lead, particulate matter, and carbon monoxide. Yet the U.S. Environmental Protection Agency (U.S. EPA*) estimates that implementation and compliance costs totaled $588 billion between 1970 and 2010 (U.S. EPA 1997, 2011). It is therefore essential to understand whether environmental policies result in the intended improvements, comparing the predicted benefits to air quality and health with those that are actually achieved. This area of research is known as accountability, and it evaluates the extent to which environmental regulations yield improved air quality and public health.
Over the past two decades the Health Effects Institute (HEI) has emerged as a leader in air pollution accountability research, contributing to research design, funding, and study oversight. In 2003, an HEI working group developed a conceptual framework for conducting air pollution accountability research and outlined methods and opportunities for future research (HEI Accountability Working Group 2003). More details on HEI’s involvement in accountability research is reviewed in the Preface. Through a series of Requests for Applications (RFAs) over the past two decades, HEI has now funded over a dozen studies that assessed a wide variety of regulations targeting both point and mobile sources of air pollution. For practical reasons, earlier studies tended to focus on local-level actions that were implemented over a relatively short time frame. HEI later solicited research that evaluated actions with a larger geographical scope and were implemented over longer periods of time.
In its 2011 RFA 11-1, “Assessing the Health Outcomes of Air Quality Actions,” HEI aimed to fund research studies that would (1) evaluate regulatory and other actions at the national or regional level that were implemented over multiple years; (2) evaluate complex sets of actions aimed at improving air quality in large urban areas, including those in the vicinity of major ports; or (3) develop methods to support such health outcomes research. In response, Meng and colleagues proposed to study the impact of the 2006 Emission Reduction Plan for Ports and Goods Movement in California on air pollution exposures and healthcare utilization among more than 20,000 low-income residents of port-adjacent communities. They would first estimate changes before and after the implementation of the plan in individual-level exposures to three pollutants primarily emitted from diesel engines by leveraging existing governmental air quality monitoring data and additional sampling in cities near California’s largest ports. Then they would evaluate whether emergency room visits and hospitalizations decreased after implementation of the plan to a greater extent for people living near ports and major highways in comparison with people living in areas further away and less likely to be impacted by the plan.
The HEI Research Committee recommended the proposal by Meng and colleagues for funding due to its strong focus on disadvantaged communities living near ports and major roadways, because this was an area of great interest to HEI’s industry and governmental sponsors and yet the subject of limited existing research. A key strength of the proposed study design was the comparison of different areas based on proximity to major goods movement transportation routes (i.e., ports and highways leading to ports), which would help differentiate the goods movement policy actions under study versus other regulations that may affect pollution from other forms of road traffic. The Research Committee also appreciated the substantial sample size and focus on large urban regions, as well as the air pollution modeling expertise among the investigators. The study was conducted in two phases, with air pollutant and health outcome assessments commencing in 2012 and 2015, respectively.
This Commentary provides the HEI Review Committee’s evaluation of the study. It is intended to aid the sponsors of HEI and the public by highlighting both the strengths and limitations of the study and by placing the Investigators’ Report into scientific and regulatory context.
SCIENTIFIC AND REGULATORY BACKGROUND
The U.S. economy relies heavily on international trade, with approximately $4 trillion worth of goods imported and exported annually, including raw materials, agricultural supplies, and consumer products (U.S. Census Bureau and U.S. Bureau of Economic Analysis 2021). Three-quarters of these goods by weight are transported into and out of the United States via oceangoing vessels, largely funneled through only a handful of ports (Tomer and Kane 2015). These ports are vital to U.S. economic prosperity, accounting for a quarter of gross domestic product and generating more than 30 million jobs (Martin Associates 2019). Yet just 4% of traded goods start or end their journey within local port communities — instead, they travel an average of 1,000 miles, mainly via truck or rail, to their final destinations across the country (Tomer and Kane 2015). This goods movement transport network is operated by a sequence of ships, cargo-handling machinery, locomotives, and trucks that are primarily powered by diesel engines.
However, goods movement–related diesel emissions, especially from older diesel engines, can contribute to locally elevated air pollution, exposing the nearly 40 million Americans who live near ports, and the 11 million who live near major highways, to harmful contaminants such as particulate matter and nitrogen oxides (Boehmer et al. 2013; U.S. EPA 2016). The International Agency for Research on Cancer classifies diesel emissions as carcinogenic to humans (Benbrahim-Tallaa et al. 2012), and exposure has been associated with increased risks of adverse respiratory symptoms, hospitalizations related to heart and lung illnesses, and premature death (U.S. EPA 2016). In addition, the people that live near ports and thus have higher exposure to diesel emissions tend to consist of low-income and racial- and ethnic-minority households (Rosenbaum et al. 2011). Compared with those from higher socioeconomic backgrounds, these households may be more susceptible to air pollution-related health effects due to higher rates of comorbidities and less access to primary Medi-Cal care (Daw 2017; National Association of Community Health Centers 2007).
California represents a microcosm of these issues. The state has the largest economy of any state (U.S. Census Bureau and U.S. Bureau of Economic Analysis 2021), and its eleven ports connect U.S. trade with countries across the Pacific Ocean. The Port of Los Angeles is the busiest container port in the Western Hemisphere, moving $276 billion in goods per year. Together with the adjacent Port of Long Beach, the port complex handles 30% of national cargo volumes (Port of Los Angeles 2019). In residential neighborhoods surrounding the port complex and nearby roadways, diesel-related pollutant exposures were previously estimated to be five times greater than non-impacted locations (Kozawa et al. 2009), with higher exposures disproportionately impacting communities of color (Houston et al. 2014). Further, research undertaken by the California Environmental Protection Agency’s Air Resource Board (CARB) had found that people living in those communities were likely to suffer pollution-related economic loss, including restricted activity and missed work, and poorer health, including increased risk of asthma attacks, cancer, and premature death (Di 2006).
Recognizing that goods movement–related emissions were the primary contributor to transportation emissions in the State of California (Di 2006) and that controlling those emissions was critical to protecting public health, CARB and local air quality management districts implemented the Emission Reduction Plan for Ports and Goods Movement in California (herein referred to as Goods Movement Plan) in 2006 (CARB 2006). The plan had five major goals:
Decrease California’s overall emissions from international and domestic goods movement to 2001 levels or lower by year 2010.
Achieve an 85% reduction in CARB-estimated statewide health effects due to diesel particulate matter emissions from international and domestic goods movement by 2020.
Reduce nitrogen oxide emissions from international goods movement within four counties surrounding the Los Angeles–Long Beach port complex to prescribed levels by 2020, putting the region on track for meeting state and federal air quality standards.
Implement a comprehensive set of emission-reduction strategies for ports and goods movement across the state to help all regions achieve state and federal air quality standards.
Prioritize implementation of all feasible strategies to reduce health risks to communities adjacent to goods movement facilities.
The Goods Movement Plan consisted of a multi-year rollout of emission reduction strategies targeting five modes of goods movement transport including ships, commercial harbor craft, cargo handling equipment, heavy duty trucks, and locomotives. Strategies comprised state and federal regulations, international agreements, and voluntary incentive programs primarily designed to reduce diesel particulate matter and nitrogen oxide pollution. The Commentary Table summarizes selected strategies from the Goods Movement Plan by transportation mode and approximate period of implementation. Note that there were numerous previously and concurrently implemented strategies not shown in the Commentary Table, including certain emissions standards, fuel rules, and violation reporting; those additional strategies were expected to have an ongoing contribution to emission reductions.
Commentary Table.
Summary of the Goods Movement Plan Strategies to Reduce Emissions from Ports and Goods Movement by Transport Mode and Estimated Implementation Timeline
Implementation of the Goods Movement Plan provided an unprecedented natural experiment in which a well-defined network of goods movement-related roads and freeways would undergo immediate and ongoing interventions to reduce emissions. Research was also essential to evaluate whether the estimated $6–10 billion investment required to implement the plan was effective in reducing ambient air pollution and improving public health, particularly within communities adjacent to ports and other goods movement transportation corridors. However, major challenges of this research would be to assemble a cohort representative of the population residing in near-port communities and to identify any air quality and public health improvements that were attributable to the Goods Movement Plan versus other regulations that may have similar effects.
In their research report, Improvements in Air Quality and Health Outcomes Among California Medicaid Enrollees Due to Goods Movement Actions, Meng and colleagues describe a study designed to meet these challenges. The investigators assessed changes in air pollutant concentrations and healthcare utilization before and after the 2006 Goods Movement Plan implementation within ten counties surrounding California’s major ports. They set out to investigate potential health benefits in an existing cohort of racially diverse adults enrolled in Medi-Cal, a Medi-Cal care program for low-income individuals. To help differentiate potential improvements attributable to the Goods Moment Plan versus other regulations impacting vehicle emissions, investigators compared three exposure groups defined by their proximity to goods movement transportation routes and other high vehicle traffic areas. Their findings will help inform future regulations to control goods movement emissions across the country.
SUMMARY OF THE STUDY
OBJECTIVES
Meng and colleagues studied the effects of the 2006 California Goods Movement Plan on air quality and health outcomes by focusing on vulnerable populations living in three areas: neighborhoods close to the ports and major highways with heavy-duty truck traffic driving to and from the ports (referred to as “goods movement corridors”), neighborhoods close to highways where truck traffic was banned (“non-goods movement corridors”), and neighborhoods located away from the ports and highways (“control areas”). They evaluated whether air quality had changed more in the areas where the Goods Movement Plan was expected to have greater effects and whether any observed air quality improvements had led to improved health outcomes. By comparing the three areas they hoped to tease out the specific effects of the Goods Movement Plan as compared with other regional and national regulations aimed at traffic-related pollution from cars or other factors that also lead to reduced emissions of pollutants. The investigators studied three criteria pollutants directly and indirectly targeted by the plan — nitrogen dioxide (NO2), fine particulate matter (PM2.5), and ozone (O3) — in relation to health outcome data for Medi-Cal beneficiaries (California’s Medicaid program) with chronic health conditions. They focused their analyses on comparing air quality and healthcare utilization before and after the plan went into effect and on comparing the results among people living in those three areas. Specific study objectives included the following:
Develop annual land use regression models and associated surfaces for pollutants NO2, PM2.5, and O3 for years 2004–2010 across California at a spatial resolution of 30 m.
Assess reductions in air pollution exposure measures among Medi-Cal enrollees living in goods movement, non-goods movement, and control areas by assigning the annual pollutant concentrations to their home addresses and comparing their reductions among the three location categories from the pre- to the post-policy period.
Develop and evaluate measures for health effects (e.g., emergency room visits and hospitalization) and time-varying confounding factors (e.g., change in disease severity) to support the analysis.
Identify whether improvements in air quality were greater in goods movement and non–goods movement areas than those in control areas from the pre- to the post-policy period.
Examine whether changes in exposure resulted in improvements in health outcomes, including reductions in the number of emergency room visits and hospitalizations among Medi-Cal beneficiaries with asthma, heart disease, chronic obstructive pulmonary disease (COPD), and diabetes by estimating the difference-in-differences using generalized linear multilevel models.
Conduct sensitivity analyses (e.g., propensity score methods) and analyses using a multilevel mediation model to examine whether improvements in health outcomes were due to the effect of regulatory policies on reductions in air pollution.
Meng and colleagues first estimated annual NO2, PM2.5, and O3 concentrations across California for each year from 2004 to 2012. These pollutant estimates were then assigned to the home addresses of the Medi-Cal beneficiaries with at least one of the following chronic conditions: asthma, COPD, diabetes, and heart disease. Each address was further assigned to one of three location categories based on proximity to specific traffic zones: goods movement corridors — areas within 500 m of a port or freeway where trucks were allowed; non–goods movement corridors — areas within 500 m of truck-prohibited freeways or within 300 m of freeway-connecting roads; and control areas, which included all areas other than goods movement and non-goods movement corridors. Changes in pollutant exposure among those living in the three zones were compared between the pre- and post-policy periods. Although the Goods Movement Plan was approved in 2006, rollout was slow. Therefore, Meng and colleagues defined 2004–2007 as the pre-policy period and 2008– 2010 as the post-policy period. Finally, the investigators examined subsequent changes in healthcare utilization among these Medi-Cal beneficiaries to assess whether the policy-related air quality improvements were effective in improving health. The investigators hypothesized that compared with control areas, reductions in the selected air pollutants and healthcare utilization would be greatest in goods movement corridors that were targeted by the policy actions, followed by non–goods movement corridors, which may show improvements due to more general statewide and national air pollution regulations.
STUDY DESIGN AND METHODS
Design
This study implemented a quasi-experimental design among a previously established cohort of Medi-Cal enrollees to identify whether 2006 goods movement policy actions were effective in improving ambient air pollution and health outcomes among disadvantaged populations living near California ports or freeways where trucks were permitted. Meng and colleagues compared reductions in pollutant exposure levels and healthcare utilization from the pre-policy (2004–2007) to early post-policy (2008– 2010) periods among people residing in areas designated as goods movement, non–goods movement, and control areas (see sidebar) to identify whether policies had a greater impact in goods movement corridors compared with other high and low traffic areas. The post-policy study period was meant to capture goods movement actions that were implemented immediately and during the first three years of the Goods Movement Plan multiyear rollout (see Commentary Table).
ABOUT GOODS MOVEMENT CORRIDORS
Meng and colleagues focused on evaluating changes in post-policy air pollution and healthcare utilization among zones classified by proximity to goods movement transport routes to identify changes attributable to the Goods Movement Plan versus other regulations and unrelated secular trends.
Goods Movement Corridors were areas within 500 m of ports or freeways where trucks are permitted. This zone was expected to experience the greatest benefit from the Goods Movement Plan because it included the policy-targeted transportation modes involved in the international and domestic goods movement through ports, such as drayage trucks, transport refrigerator units, and tractor trailers.
Non-Goods Movement Corridors were areas within 500 m of truck-prohibited freeways or within 300 m of freeway-connecting roads. This zone was expected to benefit from ongoing air pollution policy changes implemented at the regional and national level that imposed emissions limits on passenger cars and light-duty vehicles, but to a lesser extent than goods movement corridors given the exclusion of major goods movement transportation modes.
Control Areas, located away from the ports and freeways, served as the comparison group. Post-policy changes here were considered background shifts related to other policies affecting traffic-related emissions, but less likely to be affected by the Goods Movement Plan.
Study Population
The cohort was assembled with Medi-Cal fee-for-service claims data from the California Department of Health Care Services. Medi-Cal is California’s Medicaid system, a needs-based healthcare program for low income and disabled persons. The cohort was part of a disease management program evaluation conducted by the University of California, Los Angeles Center for Health Policy from 2004–2010. The claims data included both inpatient (e.g., hospitalization) and outpatient (e.g., emergency room visit, doctor visit, and pharmacy) Medi-Cal service encounters, with up to two diagnoses listed per encounter. Beneficiaries resided in 10 California counties including Los Angeles, Riverside, San Bernardino, San Diego, Alameda, San Francisco, Santa Clara, San Joaquin, Fresno, and Sacramento (Commentary Figure 1). Original inclusion criteria for the disease management program limited the cohort to adults 22 years and older who were Medicare ineligible and had at least one paid Medi-Cal claim for one of four chronic conditions. These conditions included asthma, COPD, diabetes, and heart disease (which included atherosclerotic heart disease, coronary artery disease, and congestive heart failure). Most beneficiaries in the source Medi-Cal claims dataset were middle-aged because persons who are 65 and older typically enroll in Medicare, the national Medi-Cal program for elderly individuals.
Dr. Meng limited the study population to beneficiaries in the healthcare program evaluation with continuous Medi-Cal enrollment over the 2004–2010 study period and at least one claim per year. Enrollees were excluded if they had been diagnosed with human immunodeficiency virus or cancer, were long-term care patients, or they did not have a valid home address that could be linked with pollution data. Of the approximately 172,000 enrollees in the original claims dataset, about 23,000 remained after exclusions.
Approach
The project was conducted in two phases. In Phase I, Meng and colleagues estimated annual levels of pollutants NO2, PM2.5, and O3 across the state of California by developing land use regression model surfaces for calendar years 2004 to 2012. In Phase II of the study, home addresses for each Medi-Cal beneficiary were assigned NO2, PM2.5, and O3 exposure levels and categorized into the goods movement, non–goods movement, and control areas (see sidebar and Commentary Figure 1). Health outcome measures included annual number of all-cause emergency room visits and hospitalizations per beneficiary from September 1, 2004, to August 31, 2010. To detect potential incremental improvements over time, the pollutant exposure levels and healthcare utilization for each year in the early post-policy period (2008, 2009, and 2010) were compared with the average annual utilization during the pre-policy period (2004–2007).
Statistical Analysis
Estimating Pollutant Levels Across California
Meng and colleagues estimated annual levels of pollutants NO2, PM2.5, and O3 at a 30-m resolution across the state by developing mixed-effects land use regression models for every year of the study period. Air pollution data were merged from two sources. Continuous pollutant concentrations were monitored at more than 100 sites across California by the U.S. EPA for all study years, with approximately 38% of sites located within the 10 counties under study. The investigators conducted additional NO2 monitoring in Alameda and Los Angeles counties because they are home to California’s three largest ports and are part of the two largest urban regions in the state. These NO2 monitoring data were collected in 2004–2005 for Alameda and 2006–2007 for Los Angeles counties. Additional sampling was conducted in 2012–2013 for Alameda and Los Angeles in order to improve land use regression modeling, although this occurred after the time frame when Medi-Cal data were available. The more than 600 NO2 samples were distributed evenly across the goods movement, non–goods movement, and control areas. The statewide data allowed Meng and colleagues to reduce the uncertainty of pollutant exposure estimates in the outer regions of the study areas, while supplemental monitoring in Alameda and Los Angeles counties increased the precision and accuracy of NO2 exposure estimates in key areas.
The optimal land use regression model was chosen using a deletion/substitution/addition algorithm paired with cross-validation. Predictors included numerous variables related to road traffic, distance to ports and coastline, land elevation and use, atmospheric conditions, and the gridded ozone concentrations from the U.S. EPA’s ozone Downscaler (U.S. EPA 2020). The investigators intended for vehicle-kilometers-traveled variables to serve as proxies for changes in economic conditions, including the 2008 economic recession. Phase I of this study culminated with annual NO2, PM2.5, and O3 concentrations predicted at a 30-m spatial resolution across California.
Analysis of Health Data
To test whether goods movement policy actions improved air quality and health outcomes, the investigators applied a difference-in-differences model in Phase II. This method is commonly used in observational research on policy-related interventions to mimic experimental designs and compares the change of an outcome over time in an intervention group to a change in outcome over time in a control (no intervention) group (Dimick and Ryan 2014). In the absence of confounding, if the policy has no effect, then baseline differences between these two groups will remain unchanged over time. But if a policy impacts the intervention group, then the differences between groups may become larger or smaller over time.
Meng and colleagues used the difference-in-differences analysis to compare changes in pollutant exposure levels and healthcare utilization, including both emergency room visits and hospitalizations, among those living in the goods movement, non–goods movement, and control areas. Changes in each of the areas were compared. They analyzed these changes for each of the three post-policy years (2008, 2009, and 2010), evaluating the entire cohort together and among those with each of the four chronic conditions separately. If the Goods Movement Plan had the intended effects, in the absence of confounding investigators would expect to observe greater reductions in pollutant exposure levels and healthcare utilization in the goods movement corridor compared with other areas. Analyses were adjusted for numerous risk factors to control for individual- and neighborhood-level variables that could bias results. To control for differences across the three traffic areas, beneficiary-level variables included age, sex, language spoken, race and ethnicity, number of comorbidities in pre-policy years, and county of residence. To control for changes over time, they also adjusted for annually recorded smoking status, depression, number of doctor visits, and severity of health status using the Chronic Illness and Disability Payment System risk scores. Neighborhood-level factors were derived from the 2000 and 2010 U.S. Census (representing the pre- and post-policy periods, respectively) and included percent minority, unemployed, living in poverty, and households with no vehicle. Results were considered statistically significant at α = 0.05 and reported with both 95% confidence intervals (CI) and P values.
Supplemental Analyses
Investigators conducted additional sensitivity analyses to evaluate the robustness of their findings. To account for the fact that individuals could not be randomized to the goods movement corridor, difference-in-differences analyses with inverse probability weighting was also conducted. This method first uses logistic regression to estimate the predicted probability of each Medi-Cal beneficiary living in the goods movement compared with control areas, given key demographic characteristics. In their report, investigators chose age, sex, number of comorbidities, and severity of health status as their key characteristics. The inverse of these probabilities is then used to create weights for each individual. Thus, individuals living in goods movement areas with characteristics similar to their neighbors will be down-weighted, while those with characteristics more similar to those living in control areas will be upweighted. Compared to an experimental design where the distribution of characteristics is equal across groups due randomization, this method attempts to distribute characteristics equally across groups by re-weighting them (Rosenbaum and Rubin 1983).
Finally, investigators conducted a multi-level mediation analysis to test whether the way in which the Goods Movement Plan reduced healthcare utilization was through reduced air pollution. This is important because the policy intervention could improve health outcomes directly but be due to outside influences. In their modeling approach, investigators tested whether the policy-related reductions in both NO2 and PM2.5 mediated the reduction in emergency visits among those living in goods movement corridors compared with controls. Only NO2 and PM2.5 were included in the mediation analysis because preliminary results showed these pollutants, but not O3, were related to the intervention.
SUMMARY OF KEY RESULTS
Population Characteristics
In this study population of Medi-Cal beneficiaries, 13,337 (57%) had been diagnosed with diabetes, 8,900 (38%) with COPD, 8,636 (37%) with asthma, and 8,684 (37%) with heart disease. Beneficiaries were not evenly distributed across the three areas, with most residing in non–goods movement corridors (57%), followed by goods movement (22%), and control areas (20%). Demographic characteristics were similar across zones; however, those residing in goods and non–goods movement areas were more likely to be African American and Latino compared with control areas. At the neighborhood-level higher rates of unemployment, poverty, and households without vehicles were observed in goods movement corridors, followed by non–goods movement corridors, compared with control areas.
Air Quality Improvements
Compared with the pre-policy period, Meng and colleagues reported statistically significant reductions in NO2 and PM2.5 concentrations across all 10 counties in the post-policy period. Results from the difference-in-differences analyses showed the greatest reductions in NO2 and PM2.5 when comparing goods movement to control areas for all Medi-Cal beneficiaries together and when stratifying by beneficiaries with each of the four chronic conditions. For example, the average annual estimated exposures to NO2 and PM2.5 were 2.43 ppb (95% CI =-2.51, -2.34) and 1.58 μg/m3 (95% CI = -1.63, -1.52) lower, respectively, among beneficiaries with asthma living in the goods movement corridor versus the control area during the first-year post-policy compared with average levels in pre-policy years. Commentary Figure 2(A) shows the decreasing NO2 exposure levels among all beneficiaries, and beneficiaries with asthma and COPD, across the study period with greater reductions for those living in goods movement corridors compared to control areas during the post-policy period. The investigators reported that the higher NO2 concentrations in goods movement corridors during the pre-policy period decreased by 19.5% and approached the lower concentrations observed in non–goods movement and control areas during the post-policy period.
Average NO2 exposure levels (A) and emergency room visits (B) among all beneficiaries, those with asthma, and those with COPD from the pre-policy (2005-2007) to post-policy (2008-2010) study periods. After 2007 policy implementation, reductions were greater for goods movement corridors (solid blue line) compared with control areas (long-dashed red line). The counterfactual (gray short-dashed line) indicates the expected trend for the goods movement corridor if the Goods Movement Plan had not been implemented. (Adapted from Figure 5 in Investigators’ Report.)
Similar, but smaller reductions in NO2 and PM2.5 were observed when comparing non–goods movement to control areas, with the smallest reductions observed when comparing goods movement areas to non–goods movement areas. For example, among beneficiaries with asthma, during the first-year post-policy average annual estimated exposure to NO2 and PM2.5 was 1.31 ppb (95% CI = -1.39, -1.24) and 0.90 μg/m3 (95% CI = -0.95, -0.86) lower, respectively, among beneficiaries living in the non-goods movement corridor versus control, and 1.11 ppb (95% CI = -1.18, -1.05) and 0.68 μg/m3 (95% CI = -0.72, -0.63) lower, respectively, among beneficiaries living in the goods movement versus non-goods movement corridors. Reductions in NO2 and PM2.5 were generally largest in the first year following policy changes, with smaller reductions in years two and three. For example, the average annual exposures among all beneficiaries living in the goods movement corridor versus control areas during the first, second, and third years post-policy were 2.35, 2.21, and 1.98 ppb lower, respectively, for NO2, and 1.49, 1.34, and 1.37 μg/m3 lower, respectively, for PM2.5.
In contrast, O3 concentrations demonstrated the opposite trend during the post-policy period, where greater increases were observed for goods and non–goods movement corridors when compared with controls. This finding is consistent with the known inverse relationship between O3 and NO2. O3 concentrations showed similar changes across the study period in goods and non–goods movement corridors.
Health Outcome Improvements
Investigators reported statistically significantly greater improvements in health outcomes for Medi-Cal beneficiaries suffering from respiratory-related chronic conditions who were living in goods and non–goods movement corridors when compared with controls in the second and third years post-policy. For example, difference-in-differences estimates indicated that in year three following the goods movement policy actions, an additional 170 (95% CI = -290, -50) emergency visits among those with asthma, and an additional 180 (95% CI = -300, -50) emergency visits among those with COPD, were avoided annually for every 1,000 beneficiaries in the goods movement areas compared with control areas. Estimates were smaller when comparing non-goods movement corridors with control areas. For example, in post-policy year three, an additional 160 (95% CI = -260, -60) emergency visits among those with asthma, and an additional 90 (95% CI = -200, -10) emergency visits among those with COPD, were avoided annually for every 1,000 beneficiaries in the non-goods movement compared with control areas. There were no significant differences between goods and non-goods movement corridors. Commentary Figure 2(B) shows the emergency room visits among all beneficiaries, as well as those suffering from asthma and COPD, across the study period. Although emergency visits decreased for beneficiaries living in goods movement corridors, they increased for those living in control areas during the post-policy period.
Results from the mediation analysis indicated that the reductions in emergency room visits among beneficiaries with asthma in goods movement compared with control areas were mediated through reductions in NO2 and PM2.5 in the post-policy period. This suggests that reductions in emergency room visits among those with asthma were at least partially a downstream effect of the policy-related air quality improvements.
Post-policy reductions in emergency room visits among all beneficiaries and those with diabetes and heart disease were not significantly different for goods and non–goods movement corridors when compared with controls, and post-policy reductions among each beneficiary group was not significantly different for goods compared with non– goods movement corridors. Investigators posited that the observed ER reductions in asthma and COPD, but not diabetes and heart disease, were due to an increased biological susceptibility when air pollutants are deposited in the lungs of persons with chronic respiratory diseases.
Investigators reported that the difference-in-differences estimates for hospitalizations showed a downward trend in the post-policy period but were not significantly different for those living in goods and non–goods movement corridors versus controls or for goods movement versus non– goods movement corridors. Similar results were observed in supplemental difference-in-differences analyses of health outcomes with inverse probability weighting.
HEI REVIEW COMMITTEE EVALUATION
In its independent evaluation of the study, the Review Committee appreciated that this study used a quasi-experimental design to assess the effectiveness of the 2006 California Goods Movement Plan on air pollution and health outcomes near major ports. In the absence of confounding, this study design enabled investigators to establish cause and effect from observational data (Dominici et al. 2014). They generally agreed with the interpretation of results as reported by the investigators. First, there were greater reductions in NO2 and PM2.5 levels during the post-policy period in goods movement areas compared with control areas (for a description of the goods movement areas, see the sidebar). Furthermore, the post-policy reductions in air pollution subsequently led to lower emergency healthcare utilization among Medi-Cal beneficiaries with respiratory-related chronic conditions, but not among those beneficiaries with diabetes or heart disease. Finally, smaller reductions were observed when comparing non–goods movement with control areas, and the smallest reductions were observed when comparing goods movement with non-goods movement areas.
Overall, the Committee found the study results to be useful and clearly presented and considered them to be of particular interest to policymakers who are planning goods movement policy interventions in other jurisdictions. However, the Committee thought that the conclusions were too strong because the changes in health outcomes could not be definitively linked to the policy actions due to various other regulations and economic changes that happened during the same time frame. Below, we highlight strengths and limitations of the study.
STUDY DESIGN
The Committee noted that the robust study design enabled assessment of regulatory impacts on public health and was applied to unique datasets linking detailed air quality measurements and models with longitudinal Medi-Cal claims. In addition, the investigators were able to obtain individual home addresses, allowing them to estimate finer variation in pollution exposure by small-scale proximity to goods movement areas. However, the observational nature of this study design meant that it was not possible to randomly assign people to goods movement corridors and therefore inherent differences between beneficiaries living in the three areas at baseline and over time may have influenced the results. To account for this, investigators used a difference-in-differences model and inverse probability weighting to control for dissimilar socioeconomic and health characteristics between Medi-Cal beneficiaries in the goods movement and control areas. They reported that trajectories in pollutant exposures and healthcare utilization for the goods movement and control areas were parallel over time, indicating that potential biases due to unobserved confounding should be minimized, and similar results were obtained with and without inverse-probability weighting. Although these methods aim to replicate randomized experimental trials by balancing characteristics of the intervention and control groups at baseline and over time, residual and unmeasured differences cannot be completely ruled out.
Another major strength of this study was that the analysis was structured within three goods movement traffic zones. In particular, the Committee appreciated the inclusion of an intermediate non–goods movement area. This allowed the investigators to tease out effects attributable to the Goods Movement Plan from the effects of other regional and national regulations affecting vehicle emissions that would impact both the goods movement and non–goods movement corridors but were expected to affect the control areas to a much smaller extent. The difference-in-differences estimates comparing these three areas were suggestive of a gradation in responses, with goods movement corridors showing the greatest improvement in air quality and healthcare utilization, a smaller improvement shown for non–goods movement corridors, and minimal or no improvement in control areas.
Finally, the Committee appreciated that the investigators evaluated three air pollutants and were therefore able to compare results for a traffic-related air pollutant (i.e., NO2); a pollutant largely related to traffic, regional transport, and shipping emissions (i.e., PM2.5); and a secondary air pollutant (i.e., O3). Meng and colleagues reported that goods movement actions reduced concentrations of NO2, with smaller reductions in concentrations of PM2.5. Consistent with the known inverse relationship between NO2 and O3, O3 concentrations increased during the post-policy period. Therefore, the results from this study can be built upon so that future regulations can better target specific pollutants that are most likely to be affected by the goods movement sector.
STUDY POPULATION
Investigators limited the cohort to beneficiaries with six years of continuous Medi-Cal enrollment. Enrollment interruptions, known as churning, are common due to intermittent eligibility changes (e.g., inconsistent income level). They justified this choice because those with disrupted coverage generally have higher emergency-care utilization that may be difficult to differentiate from policy-related utilization changes. The Review Committee noted that characterization of those excluded from this cohort, including demographic information and which traffic corridor or control area they resided in, would have been helpful to include in the Investigators’ Report to identify potential selection bias affecting the results and aid our understanding of how the results may be generalized. Currently it is unclear whether results from this study suggesting that goods movement policies improve health outcomes would apply to the overall Medi-Cal population with chronic conditions. The Committee acknowledged that including churning beneficiaries may have made the results more difficult to interpret but would have preferred additional sensitivity analysis.
Another limitation was the time frame of available Medi-Cal data. The study period was limited to only three years post-policy because in 2010 the Medi-Cal fee-for-service reimbursement system, where healthcare providers are paid for each service performed, transitioned to a managed-care system, where providers are regularly paid a predetermined amount to monitor and manage a patient’s health. This transition can alter healthcare utilization (Kern et al. 2019; Toseef et al. 2019, 2020; Yamaki et al. 2019) and providers’ claim submission behaviors, with uncertain changes to this Medi-Cal population with chronic conditions. Although the transition to managed care was gradually implemented beginning in 2003, the investigators state that all members of the cohort were fee-per-service patients and that the changes would not affect the inclusion of participants in the cohort. The Committee thought that it was unfortunate that the study population could not be followed for a longer period but agreed that the change in the data due to the change in reimbursement system would have been too large for reasonable comparisons after 2010. Overall, the Committee appreciated that the study targeted people who may be more vulnerable to the health effects of air pollution, a population that is often inadequately included in many other studies.
ALTERNATIVE EXPLANATIONS FOR THE RESULTS
Although the results suggested that the Goods Movement Plan improved some aspects of air quality and health, the Review Committee acknowledged the possibility that other factors may have contributed to the observed results due to inherent limitations to the design. However, they felt these limitations were not adequately addressed in the discussion. Although the investigators controlled for numerous confounding variables in their analysis, some bias may nonetheless persist. Population changes, additional public health interventions, and secular trends occurring over the study period may have influenced the results if they disproportionately affected some locations or population subgroups, but not others. The investigators argued that such changes would be accounted for using the difference-in-differences model; Medi-Cal policy changes would impact the entire study population equally; and local interventions would be partially controlled for by adjusting for county and neighborhood poverty levels in the regression models. However, these assumptions cannot be comprehensively tested.
Of particular concern, it is unclear whether a 2006 diesel fuel standard change or the 2008 global economic recession affected the goods movement, non–goods movement, and control areas differently. In 2006 the U.S. EPA began phasing in regulations requiring all highway vehicles, locomotives, and marine engines and equipment to transition to ultra-low-sulfur diesel fuel, which reduces both nitrogen oxide and particulate matter emissions (Zhu et al. 2010). The economic recession also severely impacted port and road traffic. For example, between 2007 and 2009, the number of shipping containers moving through the Ports of Los Angeles and Oakland declined 19% and 14%, respectively (Port of Los Angeles; Port of Oakland). Although annual traffic and cargo volumes were included in the statistical analyses of pollutant exposures, the investigators reported that this information could not be meaningfully assigned to beneficiaries and therefore could not be included in the health outcome models. Alternatively, the investigators adjusted for pre- and postintervention census-tract-level unemployment, poverty, and vehicle ownership to help control for the economic downturn. Notably, results showed that NO2 levels and emergency room visits markedly decreased in 2008. Therefore, the Committee thought that the decline could not be fully attributed to the Goods Movement Plan.
Another result that was not discussed in the report was that NO2 and PM2.5 levels showed the greatest improvement in the first year post-policy, with incrementally smaller improvements in the second and third years. However, the Goods Movement Plan included many rules, such as electrification of ships and drayage vehicles in the ports that took time to implement, as did rules that affected vehicle emissions that happen over several years due to slow fleet turnover (see the Commentary Table for summary of Goods Movement Plan strategies and timelines). Thus, changes in air quality due to the Goods Movement Plan were expected to accumulate over time and extend well beyond the study period. If the policy intervention were directly and primarily responsible for greater reductions in NO2 and PM2.5 levels in the goods movement corridor compared with the control area, the Committee would have expected to observe greater improvements in the second and third years.
The Committee concluded that the results were consistent with the investigators’ interpretation that changing air pollution was responsible for the changes in health outcomes, but not sufficient to prove there was a causal relationship given the uncertain influence of extrinsic factors. In addition, the investigators were not able to fully tease apart air quality changes that could be attributed to the goods movement regulations from those resulting from other regulations to reduce emissions or other changes in society that happened over the same time period. Given the infeasibility of exploring all possible alternative explanations, the Review Committee believed that the investigators may have been too strong in their conclusions without completely acknowledging the limitations.
SUMMARY AND CONCLUSIONS
Meng and colleagues assessed the effectiveness of the 2006 California Goods Movement Plan on air quality and healthcare utilization among Medi-Cal beneficiaries with chronic conditions living near ports or freeways over a 6year period. They classified neighborhoods into three zones based on proximity to goods movement transportation routes: goods movement corridors were adjacent to ports or freeways, non–goods movement corridors with high levels of non-truck traffic, and control areas with comparably low traffic. Using a difference-in-differences analysis, they compared changes in ambient NO2, PM2.5, and O3 exposure, and changes in emergency room visits and hospitalizations, from the pre-policy (2004–2007) to post-policy (2008–2010) periods among the three zones.
The investigators hypothesized that goods movement corridors would receive the greatest benefit because the Goods Movement Plan targeted the major transportation modes within and through ports. They reported greater reductions in NO2 and PM2.5 concentrations during the three-year post-policy period among those living in the goods movement areas compared with those living outside of those areas. Furthermore, the post-policy reductions in air pollution were associated with fewer emergency room visits among Medi-Cal beneficiaries with asthma and COPD. However, there was no improvement in O3 exposures, hospitalizations, or emergency room visits among beneficiaries with diabetes and heart disease.
The Review Committee commented on the strong quasi-experimental study design addressing an important research topic of great interest to policymakers. They agreed with the investigators that the evidence supported the conclusions that the Goods Movement Plan was related to greater reductions in NO2 and PM2.5 exposures and greater reduction in emergency care utilization among beneficiaries with asthma and COPD living in goods movement corridors compared with other areas. Yet they thought some study limitations were not fully addressed. The Committee would have preferred additional results demonstrating similarities and differences between the current cohort and those excluded so that selection bias and generalizability could be adequately evaluated. They would have also preferred a more detailed discussion of alternative explanations, including other regulations and secular trends, which may have contributed to observed findings.
Overall, this study provided evidence that regulatory actions to limit emissions from goods movements in and around major ports and freeways may decrease emergency care utilization among disadvantaged people who live close to those locations and also suffer from respiratory-related chronic conditions. Further research is needed to understand whether continued improvements are seen during the decade(s) following the start of the implementation of the Goods Movement Plan in 2006, given that it takes many years to implement such an ambitious program and that vehicle turnover is generally slow. It will also be useful to evaluate whether similar improvements are observed elsewhere when goods movements actions are implemented, targeting ports and other major distribution hubs. The most difficult and pressing challenge remains to disentangle the effects on emissions, air quality, and health of individual regulations. Whereas it is useful to study the effectiveness of a broad program of regulations, such as the Goods Movement Plan, governing authorities would ultimately like to know which of the individual actions have been most effective. Further research and development of statistical approaches is needed to provide further insight into these issues.
ACKNOWLEDGMENTS
The Review Committee thanks the ad hoc reviewers for their help in evaluating the scientific merit of the Investigators’ Report. The Committee is also grateful to Hanna Boogaard and Annemoon van Erp for their oversight of the study, to Eva Tanner and Allison Patton for their assistance in preparing its Commentary, to Mary K. Brennan for editing of this Report and its Commentary, and to Hope Green, Fred Howe, Hilary Selby Polk, and Ruth Shaw for their roles in preparing this Research Report for publication.
Footnotes
* A list of abbreviations and other terms appears at the end of this volume.
REFERENCES
Benbrahim-Tallaa L, Baan RA, Grosse Y, Lauby-Secretan B, El Ghissassi F, Bouvard V, et al. 2012. Carcinogenicity of diesel-engine and gasoline-engine exhausts and some nitroarenes. Lancet Oncol
13:663–664; doi:10.1016/s14702045(12)70280-2. [DOI] [PubMed] [Google Scholar]
Boehmer TK, Foster SL, Henry JR, Woghiren-Akinnifesi EL, Yip FY. 2013. Residential proximity to major highways — United States, 2010. MMWR
62:46–50. [PubMed] [Google Scholar]
Daw J. 2017. Contribution of four comorbid conditions to racial/ethnic disparities in mortality risk. Am J Prev Med
52:S95–S102; doi:10.1016/j.amepre.2016.07.036. [DOI] [PubMed] [Google Scholar]
Dimick JB, Ryan AM. 2014. Methods for evaluating changes in health care policy: The Difference-in-Differences Approach. JAMA
312:2401–2402; doi:10.1001/jama.2014.16153. [DOI] [PubMed] [Google Scholar]
HEI Accountability Working Group. 2003. Assessing Health Impact of Air Quality Regulations: Concepts and Methods for Accountability Research. Communication 11. Boston, MA: Health Effects Institute. [Google Scholar]
Houston D, Li W, Wu J. 2014. Disparities in exposure to automobile and truck traffic and vehicle emissions near the Los Angeles–Long Beach port complex. Am J Public Health
104:156–164; doi:10.2105/AJPH.2012.301120. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kern LM, Rajan M, Pincus HA, Casalino LP, Stuard SS. 2019. Changes in ambulatory utilization after switching from Medicaid fee-for-service to managed care. Am J Manag Care
25:e254–e260. [PubMed] [Google Scholar]
Kozawa KH, Fruin SA, Winer AM. 2009. Near-road air pollution impacts of goods movement in communities adjacent to the Ports of Los Angeles and Long Beach. Atmos Environ
43:2960–2970; doi:10.1016/j.atmosenv.2009.02.042. [Google Scholar]
Martin Associates. 2019. 2018 National Economic Impact of the U.S. Coastal Port System. Lancaster, PA:Martin Associates. [Google Scholar]
Rosenbaum A, Hartley S, Holder C. 2011. Analysis of diesel particulate matter health risk disparities in selected US harbor areas. Am J Public Health 101 Suppl
1:S217–223; doi:10.2105/AJPH.2011.300190. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rosenbaum P, Rubin D. 1983. The central role of the propensity score in observational studies for causal effects. Biometrika
70:41–55; doi:10.1093/biomet/70.1.41. [Google Scholar]
Toseef MU, Jensen GA, Tarraf W. 2019. Is enrollment in a Medicaid health maintenance organization associated with less preventable hospitalizations?
Prev Med Rep
16:100964; doi:10.1016/j.pmedr.2019.100964. [DOI] [PMC free article] [PubMed] [Google Scholar]
Toseef MU, Jensen GA, Tarraf W. 2020. Medicaid managed care and preventable emergency department visits in the United States. F. Fischer, ed.
PLoS ONE
15:e0240603; doi:10.1371/journal.pone.0240603. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yamaki K, Wing C, Mitchell D, Owen R, Heller T. 2019. The impact of Medicaid managed care on health service utilization among adults with intellectual and developmental disabilities. Intellect Dev Disabil
57:289–306; doi:10.1352/1934-9556-57.4.289. [DOI] [PubMed] [Google Scholar]
Zhu L, Zhang W, Liu W, Huang Z. 2010. Experimental study on particulate and NOx emissions of a diesel engine fueled with ultra-low sulfur diesel, RME-diesel blends and PME-diesel blends. Sci Total Environ
408:1050–1058; doi:10.1016/j.scitotenv.2009.10.056. [DOI] [PubMed] [Google Scholar]