

Abstract
Introduction
This study was conducted to examine the impact of a group cognitive rehabilitation program for people with dementia on everyday memory function and quality of life.
Methods
Participants included in the study were community‐dwelling adults with a diagnosis of dementia. The intervention was a 5‐week occupational therapy lead group cognitive rehabilitation program delivered once a week for 1.5 h. Outcome measures included standardised memory tests, subjective everyday memory function and quality of life ratings. The measures were completed at baseline, post‐intervention and 3‐month post‐intervention.
Results
Outcome measures were completed with 58 participants. Statistically significant improvements in standardised memory scores were noted following the intervention. Similarly, self‐rated everyday memory function and quality of life scores significantly improved following the intervention. All standardised scores and subjective ratings were maintained at 3‐month follow‐up.
Conclusion
Group‐based cognitive rehabilitation programs can positively impact the quality of life and everyday memory function among people with dementia.
Keywords: cognitive rehabilitation, dementia, group intervention, memory, occupational therapy
Key Points for Occupational Therapy.
Group‐based occupational therapy cognitive interventions are successful in improving subjective everyday memory function among people with early dementia.
Client‐centred goal‐setting measures like COPM can be used successfully to identify and measure meaningful goals.
Occupational therapy involvement in post‐diagnostic supports is important to maintain everyday functional memory performance.
1. INTRODUCTION
Dementia is a major global health concern and is one of the significant causes of disability and dependency among older people, with an estimated prevalence of 50 million people living with dementia worldwide and approximately 10 million new cases annually (World Health Organisation [WHO], 2019). In Europe, the number of people with dementia is projected to increase from 7.5 million in 2015 to 14.3 million people by 2050 (Prince et al., 2015). In Ireland, the prevalence of dementia is estimated at approximately 55,000 people living with dementia. Ireland, like many other countries, has an ageing population and based on the current profile in Ireland, it is estimated that the number of people with dementia will increase significantly in the coming years (O'Shea et al., 2017). Memory impairments are among the most prominent cognitive deficits noted among people with dementia due to Alzheimer's disease (de Werd et al., 2013). Other symptoms alongside memory deterioration include impaired thinking, poor concentration, language and behaviour that can affect an individual's performance with everyday tasks (Health Service Executive, 2021; Prince et al., 2014; WHO, 2021).
Post‐diagnostic supports for people diagnosed with dementia include a variety of interventions, therapeutic treatment and activities that build on strengths and abilities that help maintain and enhance quality of life. The Irish National Dementia working group, in consultation with the National Dementia Post‐Diagnostic Support Project, identified that peer support, cognitive rehabilitation therapies, social contact and sharing information are essential after diagnosis (Gibb et al., 2019). Although cognitive interventions focused on memory training have been found to be successful for people with mild cognitive impairment and Alzheimer's disease (Cotelli et al., 2012), the focus of these interventions is often on training isolated components of memory function. The cognitive rehabilitation approach on the other hand emphasises a personalised approach that helps individuals and their families set realistic and meaningful goals to help with functioning in everyday life (Clare et al., 2019; Wilson, 2002). The approach is not focussed on cognitive training but instead aims to improve or maintain everyday function, utilising the person's strengths as a compensatory technique to address areas of deficit, focusing on supporting independence (National Institute for Health and Care Excellence, 2018). As such, the approach is very relevant in the treatment of dementia as it has been found to facilitate performance and optimise the (re)‐learning of skills rather than focussing purely on the restoration of the impaired memory function (de Vreese et al., 2001; Viola et al., 2011). Cognitive rehabilitation may be effective for improving learning, memory, executive functioning, and performance of activities of daily living, general cognitive problems and ameliorating depression in people with Alzheimer's disease (Sitzer et al., 2006). Studies have shown that people with dementia can continue to (re)acquire (some) valuable skills and relevant daily life activities (de Werd et al., 2013). Studies using a cognitive rehabilitation based approach have shown that people with dementia can maintain and even improve their scores on standardised memory tests as well as improvement in the utilisation of functional compensatory memory strategies (Bahar‐Fuchs et al., 2013; Clare et al., 2010, 2019; Coe et al., 2019; McGrath & Passmore, 2009).
Occupational therapists are concerned with addressing the management of functional deficits as a result of an illness or condition and have a skill set to address cognitive deficits that negatively affect the daily lives of individuals through a consideration of the dynamic interconnections between the person, environment and daily occupations (American Occupational Therapy Association, 2021). Occupational therapy theory and research support the principle that cognition is essential to performing everyday tasks (Toglia & Kirk, 2000). Occupational therapists embed principles of cognitive rehabilitation into their interventions where the emphasis is not necessarily on ameliorating the underlying memory deficit and is instead focused on the careful and individualised implementation of compensatory and rehabilitation strategies. This aims to reduce the negative impact of the memory deficit on everyday functioning.
Occupational therapy interventions effectively address memory rehabilitation among people with memory difficulties in both individual and group settings (Coe et al., 2019; Kim, 2015; McGrath & Passmore, 2009). An individualised home‐based occupational therapy memory rehabilitation program using cognitive rehabilitation principles was beneficial to people with early‐stage dementia and their caregivers and showed positive long term benefits (McGrath & Passmore, 2009). A small randomised controlled study completed by Kim (2015) indicated that cognitive rehabilitation is an effective intervention for improving performance and satisfaction with activities of daily living for people with Alzheimer's dementia.
A randomised controlled trial demonstrated the effectiveness of a home‐based, goal‐orientated cognitive rehabilitation intervention program for people with early‐stage Alzheimer's disease (Clare et al., 2010). The findings of this study resulted in significant improvement in performance and satisfaction with everyday activities among people with Alzheimer's related memory impairment. Subsequently, the GREAT trial, a randomised controlled trial completed by Clare et al. (2019), indicated that individualised cognitive rehabilitation enabled people with early‐stage dementia to improve their everyday functioning relating to individual goals targeted in therapy. Similar positive outcomes were reported in a recent Irish study of occupational therapy group‐based interventions among a clinical sample of people with subjective memory impairment, mild cognitive impairment and mild dementia (Coe et al., 2019). This 6‐week group cognitive rehabilitation program found significant improvements in the use of functional memory aids and increased scores on standardised memory tests immediately following the intervention.
This current study was conducted to examine the outcomes on everyday functioning following a 5‐week occupational therapy lead group cognitive rehabilitation program. The Specialised Memory and Attention Rehabilitation Therapy (SMART) program was set up specifically to target the subgroup of patients diagnosed with dementia in a large urban acute teaching hospital. This study was conducted to examine the impact of the SMART program on reducing the negative effect of memory deficit on everyday function and quality of life, improving satisfaction and performance with daily tasks and maintaining everyday functional memory for people living with dementia.
2. METHODS
2.1. Design
The study was executed using a pre‐test–post‐test design with a 3‐month follow‐up to measure the impact of the SMART program on the person's everyday memory function. Participants completed individual assessments with the occupational therapist prior to attending the SMART program. Participants were re‐assessed upon completion of the 5‐week SMART program and again at 3‐month post‐intervention follow‐up.
2.2. Participants
Participants with a diagnosis of dementia were referred to the occupational therapy SMART program via the hospital‐based memory clinic, outpatient geriatric clinics, multidisciplinary day hospital staff and the frailty team in the emergency department of the hospital site. To be eligible to participate in the occupational therapy SMART program (and subsequently the research study), participants had to be community‐dwelling adults diagnosed with dementia and score 18 or above on the Mini Mental State Examination (Folstein et al., 1975). The participant had to be able to get to and from the hospital each week, and they had to have adequate hearing and eyesight to engage in a group setting. After receiving a referral to the SMART program, participants provided written consent allowing their data to be used for the research study. Participation in the occupational therapy SMART program was not impacted by a person's decision to allow their data to be used in the research or not. Data were collected over a 15‐month period, from January 2019 to March 2020. Consecutive referrals for the occupational therapy SMART program over this 15‐month time period and who consented to participate in the study were recruited.
2.3. SMART program intervention
The occupational therapy SMART program is a 5‐week group cognitive rehabilitation program delivered on an outpatient basis. Although the SMART program is a group‐based intervention, each participant is seen individually by the occupational therapist to complete the assessments. During these individual appointments, the occupational therapist also works with each participant to identify individual memory‐related functional goals they wish to work on during the group sessions.
The program was delivered within the occupational therapy department in an acute care hospital. Group sessions were delivered on the same day and time each week, and each session lasted 1.5 hours. The group size was limited to a maximum of six participants per group based on the group size reported in research of similar interventions (Coe et al., 2019). Following each group session, participants were encouraged to complete tasks at home and implement strategies discussed during the session. Participants were encouraged to be accompanied by a family member/caregiver during the group sessions as they may assist the participant in implementing the memory strategies discussed within the intervention in their everyday lives. Participants were also supplied with a handbook outlining key content from each of the five sessions to refer to at home (see an overview of the five sessions in Table 1).
TABLE 1.
Overview of the 5‐week SMART program
|
Week 1 ‘An introduction to dementia, brain health and attention’ |
|
|
Week 2 ‘Understanding memory’ |
|
|
Week 3 ‘Understanding memory’ |
|
|
Week 4 ‘Home environment, driving and future planning’ |
|
|
Week 5 ‘Session recap’ |
|
2.4. Data collection tools
Data were collected at three time points; individual assessments were completed at baseline prior to commencing the SMART program, repeat assessment was completed at the end of the 5‐week program, and a final follow‐up assessment 3 months later.
The outcome measures used in the study included the Rivermead Behavioural Memory Test 3rd edition (RBMT‐3) (Wilson et al., 2008); dementia quality of life (DEMQOL) measure (Smith et al., 2005); Canadian Occupational Performance Measure (COPM) (Law et al., 2014); and the Functional Independence Measure and the Functional Assessment Measure (FIM + FAM) (Turner‐Stokes et al., 1999).
2.5. Rivermead Behavioural Memory Test 3rd edition (RBMT‐3)
The RBMT‐3 measures everyday memory function, designed to assess everyday memory problems and monitor change over time. The RBMT‐3 includes 14 subtests assessing visual, verbal, recall, recognition, immediate and delayed everyday memory, prospective memory and new learning. The RBMT‐3 is available in parallel versions to allow repeat assessment. The RBMT is commonly used in occupational therapy practice and has been shown to be appropriate and sensitive to detect a change in memory function among people with dementia (Coe et al., 2019).
2.6. Dementia quality of life (DEMQOL)
DEMQOL is a patient‐reported outcome measure designed to assess health‐related quality of life for people with dementia. The DEMQOL consists of 28 items reported on a Likert scale (a lot, quite a bit, a little, not at all). The DEMQOL can be used with all types of dementia and was developed from a five domain conceptual framework—health and well‐being, cognitive functioning, social relationships, daily activities and self‐concept. Higher scores indicate better quality of life (Mulhern et al., 2013). DEMQOL was found to have high internal consistency and test–re‐test reliability in mild and moderate dementia (Smith et al., 2005, 2007).
2.7. Canadian Occupational Performance Measure (COPM)
The COPM is an occupational therapy outcome measure that enables client‐centred goal setting. The COPM, conducted through a semi‐structured interview, allows individuals to identify occupational performance problems experienced in everyday living. A 10‐point scale is used to rate the level of performance and satisfaction with identified occupational performance problems—one indicates poor performance and low satisfaction, respectively, whereas 10 indicates excellent performance and high satisfaction. The COPM is used to detect changes in a client's self‐perception of occupational performance over time. For the SMART program, participants were asked to identify memory‐related everyday functions that they wished to address within the SMART program. Family members/caregivers could assist with identifying these everyday problems, and the occupational therapist guided the process.
2.8. Functional Independence Measure (FIM) and the Functional Assessment Measure (FAM)
The FIM is an 18 item global measure of disability with rating scales for everyday tasks. The FAM does not stand alone but adds 12 FAM items to the FIM, specially addressing cognitive and psychosocial function. Each item receives a score from 1 to 7 that evaluates the independence level in completing the daily task. The higher the score, the higher the level of independence.
2.9. Analysis
Descriptive analysis was used to analyse the demographic data, and non‐parametric analysis was used to complete the comparative analysis. Wilcoxon signed ranks test was used to test for differences between the pre‐test and post‐test scores on the outcome measures, and Mann Whitney U test was used for subgroup comparisons; significant levels were set at P < 0.05. Analysis was completed using IBM SPSS Version 25.
Ethical approval was received from the Joint Research Ethics Committee (JREC), St James’s Hospital (REC Reference: 2017‐08) to conduct the research.
3. RESULTS
Over the 15 months of the study, 58 participants (36 female and 22 male) completed the SMART program and the 3‐month follow‐up assessment. The median age of the participants was 76 years of age (range 58–91 years), all were community‐dwelling, and the median FIM score at baseline was 116 (range 92–124). Each participant had a diagnosis of dementia and the time since diagnosis was known for 47 participants (median, 4 months; range, 1–37 months).
A statistically significant improvement was found in RBMT scores post completion of the 5‐week SMART Program (P < 0.001); no change in RBMT scores was noted during the 3‐month follow‐up period (P = 0.353). However, the 3‐month follow‐up score was significantly higher than the pre‐SMART score at baseline (P = 0.001), indicating that memory scores were maintained over the follow‐up period (see Table 2).
TABLE 2.
Comparison of baseline pre‐SMART scores, post‐SMART scores and 3‐month follow‐up scores tested with Wilcoxon signed ranks test
| Pre‐SMART | Post‐SMART | Three‐month follow‐up | P value | |
|---|---|---|---|---|
| N = 58 (except DEMQOL, n = 57) | N = 57 | N = 49 | Pre‐SMART – Post SMART Post SMART – Follow‐up PRE‐SMART – Follow‐up | |
| Mean (SD) Median (range) | Mean (SD) Median (range) | Mean (SD) Median (range) | ||
| RBMT (raw scores) | 69.7 (24.5) | 82.2 (28.1) | 80 (27.9) | <0.001 |
| 67.5 (28–140.5) | 80 (35–156) | 80 (32–165) | 0.353 | |
| 0.001 | ||||
| DEMQOL | 93.9 (14.4) | 97.3 (13.1) | 97.4 (13.7) | 0.002 |
| 96 (56–115) | 99 (64–116) | 102 (55–116) | 0.930 | |
| 0.012 | ||||
| COPM‐P | 4.7 (1.7) | 6.6 (1.6) | 6.6 (1.4) | <0.001 |
| 4.5 (1–9) | 6.5 (3.5–10) | 6.5 (3.5–9.5) | 0.340 | |
| <0.001 | ||||
| COPM‐S | 4.4 (1.9) | 6.5 (1.7) | 6.5 (1.7) | <0.001 |
| 4.5 (0–9) | 6.5 (2.5–10) | 6 (2.5–9.5) | 0.323 | |
| <0.001 |
Abbreviations: COPM‐P, Canadian Occupational Performance Measure – Performance; COPM‐S, Canadian Occupational Performance Measure – Satisfaction; DEMQOL, dementia quality of life measure; RBMT, Rivermead Behavioural Memory Test; SMART, Specialised Memory and Attention Rehabilitation Therapy.
Improvements were also noted on the subjective/self‐reported measures at the post‐SMART assessment. A statistically significant improvement in scores was noted on the self‐reported quality of life (DEMQOL) upon completion of the SMART program (P = 0.002). Similarly, participants rated both their performance and satisfaction with their performance on everyday functional memory activities significantly higher upon completion of the SMART program (COPM‐P, P < 0.001, and COPM‐S, P < 0.001) (see Figure 1).
FIGURE 1.
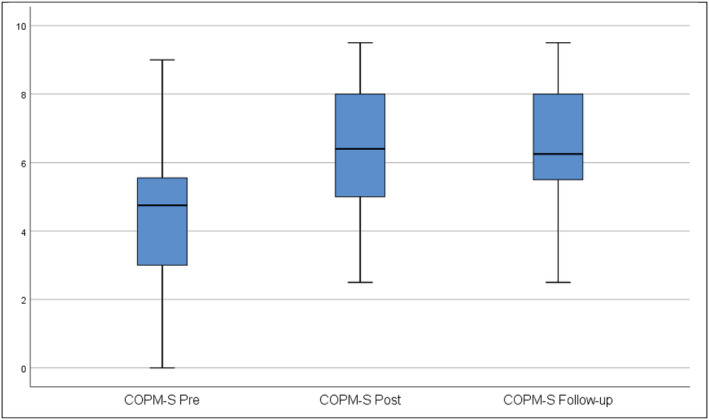
Box plot of COPM‐S scores at baseline pre‐SMART, at post‐SMART and 3‐month follow‐up. COPM‐S, Canadian Occupational Performance Measure – Satisfaction; SMART, Specialised Memory and Attention Rehabilitation Therapy
These self‐rated measures of quality of life, performance and satisfaction with performance were maintained over the 3‐month follow‐up period following completion of the SMART program, and at the follow‐up, self‐ratings on all three measures remained significantly better than at baseline pre‐SMART (DEMQOL, P = 0.012; COPM‐P, P < 0.001; COPM‐S, P < 0.001) (see Table 2). Some examples of everyday memory goals set by participants included remembering people's names, remembering what they did yesterday, knowing what day of the week it is, and remembering where items (i.e., keys) were left to minimise time spent searching for items.
There was a high level of family/caregiver attendance over the SMART program, with 44 (75.9%) family/caregivers attending two or more SMART sessions and 33 (56.9%) family/caregivers attending all five sessions. A smaller number of participants (N = 14, 24.1%) did not have family/caregiver attendance at any SMART session. No definite pattern emerged as to any participant characteristics that may have been linked to family/caregiver attendance throughout the SMART program. The only trend noted was that participants whose family/caregiver attended were slightly older than those who did not have any family/caregiver attending the program (median age 78 years' vs. median age 74.5 years). This age difference was close to statistical significant (P = 0.05). A slightly greater magnitude of improvement in DEMQOL scores was noted among the participants whose family/caregiver attended the SMART program than those who did not have a family/caregiver in attendance, but this difference was not significant (P = 0.517). Subgroup analysis did not show any significant differences in the other outcome measure scores among those who did and those who did not have family/caregivers attending the SMART program. Subgroup analysis also showed that neither age nor time because diagnosis was found to have any statistically significant impact on any outcome measures.
4. DISCUSSION
This study examined the impact of a 5‐week SMART, occupational therapy group, cognitive rehabilitation program for people with dementia. The program was delivered for people who were recently diagnosed with dementia. Participants attended the weekly group session on an outpatient basis and were encouraged to have a family/caregiver attend the sessions if they wished. The participants in this study reflected a typical demographic of people with dementia with all bar two of the participants aged 65 or older and over 60% were aged 75 or older. This age demographic matches the projected age profile of people with dementia in Ireland (Cahill et al., 2012) and would reflect the demographic of persons being diagnosed with dementia in Ireland.
The 5‐week SMART program showed significant improvement in memory scores on standardised testing among the participants, which was maintained at 3‐month follow‐up. The immediate improvement in standardised memory scores after the SMART program mirrors Coe et al. (2019) following their 6‐week memory strategy education group intervention. Participants in our study maintained their memory scores at 3‐month follow‐up, whereas the subgroup of participants with dementia in the Coe et al. (2019) study had a drop in objective memory scores. This difference in follow‐up scores may be attributable to the smaller number of participants with dementia in the Coe et al. (2019) study. The findings from the current study support the findings of previous studies indicating that people with dementia have the potential to learn new strategies to improve their memory functioning following cognitive rehabilitation interventions (Clare et al., 2019; Clare & Woods, 2004; McGrath & Passmore, 2009).
An important finding to emerge from this study is that the participants themselves reported subjective improvement in their everyday memory function alongside improved scores on standardised memory tests. The use of the COPM enabled participants to set their own individualised memory‐related goals and rate their performance on these everyday memory goals and their satisfaction with their performance. Examples of goals set by participants include knowing what day of the week it is, remembering conversations, remembering where glasses are placed, and remembering appointments. The COPM has been used in previous studies (Clare et al., 2010; Coe et al., 2019) and highlights the importance of including some self‐reported measures when delivering such interventions to customise the intervention to the individual. Using these self‐reported measures also ensures that changes in objective memory tests reflect improved memory function in everyday life from the person's perspective.
We also found significant improvement in quality of life scores measured by the DEMQOL upon completion of the 5‐week SMART program that was maintained at follow‐up. Our finding contrasts somewhat with the findings of Coe et al. (2019) in the DEMQOL scores. Coe et al. (2019) reported maintenance of DEMQOL scores among their subgroup of participants with dementia, whereas, in the current study, we found continued improvement in median DEMQOL scores among the participants upon completion of the program and at 3‐month follow‐up. One reason that may explain this finding is that Coe et al. (2019) included a mix of participants with memory impairment in their study and found that participants with subjective memory impairment and mild cognitive impairment showed more significant improvement following their intervention, whereas in the current study, the SMART program was delivered exclusively to participants who were recently diagnosed with dementia and possibly the content may have been more tailored to this particular group of participants. This may explain the greater positive outcome in quality of life ratings following the intervention. This improvement in quality of life as measured by the DEMQOL is perhaps also matched by the improvement in the participant's subjective ratings of their satisfaction (COPM‐S) with their performance on daily memory function following the SMART program, again highlighting the importance of using self‐rating measures to evaluate the impact of these types of intervention programs for people with dementia.
Overall, there was an excellent level of attendance to the SMART program, with 94% of participants attending all or 4/5 of the sessions. In addition, family/caregivers were encouraged to attend the program with the participant and over half of the family/caregivers attended all five SMART sessions. Family/caregivers are generally recommended to attend hospital appointments with people with dementia as they can support the person during the appointment and encourage person‐centred care (Griffin et al., 2020). Research shows the importance of having caregivers involved in care delivery to help improve the quality of life for the person with dementia (Brodaty & Donkin, 2009; Wolff et al., 2017). The reason for encouraging family/caregiver attendance during the SMART program was that family/caregivers might be able to help translate SMART content into everyday life and assist the person with dementia to implement the cognitive rehabilitation strategies at home. Similarly, caregiver attendance has been encouraged in other programs for people with dementia (Coe et al., 2019; Graff et al., 2006; Moebs et al., 2017; Wenborn et al., 2021) to assist with the implementation of strategies and caregivers also benefit from the education and support offered in such programs, although, in this study, we did not find any significant changes in outcomes if the family/caregiver were present for the intervention sessions or not, the presence of family/caregivers was important for the carryover and implementation of advice at home between sessions and family/caregiver attendance will be continued in the further roll‐out of the SMART program.
The SMART group interventions described in this paper were delivered once weekly over a consecutive 5‐week period. The sessions were of 1.5‐h duration and were designed and delivered by an occupational therapist. A similar duration of occupational therapy lead outpatient‐based cognitive rehabilitation programs has been reported (Coe et al., 2019). Other group‐based interventions have been delivered over 9 weeks (Moebs et al., 2017), although some individualised home‐based interventions for people with dementia involving caregivers have often been delivered over a more extended period of up to 10 weeks (Clare et al., 2019; Graff et al., 2006; McGrath & Passmore, 2009; Wenborn et al., 2021). Attendance is usually limited to approximately six people per group to allow for personalised components such as the individualised goal setting, and, if caregivers are attending, keeping a limit on numbers is essential. The high level of attendance among participants and family/caregivers in the SMART program may also indicate the perceived relevance of the program's content. Subjective feedback from both participants and family/caregivers emphasised the benefits of the intervention and the peer support gained during attendance, similar to the findings of Moebs et al. (2017). The findings from the current study add to the previous research on similar types of programs that such interventions can effectively improve everyday functional memory performance for people with dementia.
In contrast to some previous studies, the current study focussed on people who were recently formally diagnosed with dementia. This may explain the positive changes noted on the outcome measures compared to some of the previous studies that may have been targeting people with more established dementia. The Next Steps guidelines (Gibb et al., 2019) recommend that cognitive rehabilitation be offered as a post‐diagnostic support to people diagnosed with dementia. Findings from the current study indicate that group‐based cognitive rehabilitation programs may be beneficial for those in the early stages following a dementia diagnosis.
4.1. Limitations
The current study was conducted as a pilot study of an occupational therapy clinical intervention. The study's design was a pre‐test–post‐test study design, and there was no control group for comparison. Recruitment was dependent on consecutive referrals for occupational therapy intervention over the period of the study, and the study was not designed or powered to definitively test effectiveness of the intervention. This was not a funded study, and no additional resources were available. The treating therapist took the outcome measures, and there was no blinding. However, standardised test administration was adhered to, and the participants themselves completed the self‐rating measures without input from the treating therapist.
4.2. Implications for practice
The study was conducted among a clinical sample and reflected the typical caseload of patients referred to occupational therapy soon after formal diagnosis of dementia. Similar to previous research, an occupational therapy‐led group‐based intervention following cognitive rehabilitation principles seems effective in contributing to subjective and objective improvement in functional everyday memory performance among people with early dementia. This type of program delivered over 5 weeks appears adequate to enhance everyday memory function among people with dementia. In addition to enhancing outcomes for participants, completing this type of intervention in a group setting is time effective for the therapist involved and does not require the same intensity of intervention as a one‐to‐one intervention.
5. CONCLUSION
In conclusion, the study adds to the existing body of evidence that occupational therapy led cognitive rehabilitation programs positively impact objective and subjective everyday memory function and quality of life. Customising the content of such programs through individualised goal setting and self‐rating measures ensures that the content of these programs is relevant at an individual level. Evidence from the study supports previous research showing that people with dementia can benefit from such programs and have the potential to learn new strategies to maintain and improve day‐to‐day memory function.
FUNDING INFORMATION
This research received no specific grant from any funding agency in the public, commercial or not‐for‐profit sectors.
CONFLICT OF INTEREST
The authors have no conflict of interest to declare.
AUTHOR CONTRIBUTIONS
All authors were involved in various stages of the design and development of the intervention, ethics board approval, recruitment, and delivery of the SMART program, analysis of findings, review of findings and drafting of the final manuscript for publication. Aislinn Griffin was responsible for the design and delivery of the SMART program, ethics application, data collection and analysis, and final write up of the manuscript. Aoife O`Gorman was responsible for the coordination of the design and delivery of the SMART intervention, ethics application, analysis review, and final manuscript write‐up. David Robinson was responsible for the consultation on the design of the SMART program, recruitment of participants to the SMART program, review of analysis, drafting and writing the final manuscript. Matthew Gibb was responsible for the consultation on the design of the SMART program, recruitment of participants to the SMART program, review of analysis, drafting and writing the final manuscript. Tadhg Stapleton was responsible for the consultation on the design of the research component of the SMART program, completion of all analyses of data, co‐authored final drafts of the manuscript.
ACKNOWLEDGEMENTS
The researchers sincerely thank the patients who consented to participate in the study. The researchers would also like to acknowledge the support provided by consultant geriatricians, memory clinic staff, occupational therapy department and other multidisciplinary colleagues. Open access funding provided by IReL. [Correction added on 24 May 2022, after first online publication: IReL funding statement has been added.].
Griffin, A. , O`Gorman, A. , Robinson, D. , Gibb, M. , & Stapleton, T. (2022). The impact of an occupational therapy group cognitive rehabilitation program for people with dementia. Australian Occupational Therapy Journal, 69(3), 331–340. 10.1111/1440-1630.12795
DATA AVAILABILITY STATEMENT
Research data are not shared.
REFERENCES
- American Occupational Therapy Association . (2021). The role of occupational therapy in adult cognitive disorders. American Occupational Therapy Association. https://www.aota.org/About-Occupational-Therapy/Professionals/PA/Facts/Adult-Cognitive-Disorders.aspx
- Bahar‐Fuchs, A. , Clare, L. , & Woods, B. (2013). Cognitive training and cognitive rehabilitation for mild to moderate Alzheimers's disease and vascular dementia (review). Cochrane Database of Systematic Reviews, 6, 1465–1858. 10.1002/14651858.CD003260.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brodaty, H. , & Donkin, M. (2009). Family caregivers of people with dementia. Dialogues in Clinical Neuroscience, 11(2), 217–228. 10.31887/DCNS.2009.11.2/hbrodaty [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cahill, S. , O'Shea, E. , & Pierce, M. (2012). Creating excellence in dementia care: A research review for Ireland's National Dementia Strategy. DSIDC's living with dementia research programme. Irish Centre for Social Gerontology; National University of Ireland. [Google Scholar]
- Clare, L. , Kudlicka, A. , Oyebode, J. R. , Jones, R. W. , Bayer, A. , Leroi, I. , Kopelman, M. , James, A. A. , Culverwell, A. , Pool, J. , Brand, A. , Henderson, C. , Hoare, Z. , Knapp, M. , & Woods, B. (2019). Individual goal‐orientated cognitive rehabilitation to improve everyday functioning for people with early stage dementia: A multicentre randomised controlled trial (the GREAT trial). International Journal of Geriatric Psychiatry, 34, 709–721. 10.3310/hta23100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clare, L. , Linden, D. E. , Woods, R. T. , Whitaker, R. , Evans, S. J. , Parkinson, C. H. , Paasschen, J. , Nelis, S. M. , Hoare, Z. , Yuen, K. S. L. , & Rugg, M. D. (2010). Goal‐oriented cognitive rehabilitation for people with early‐stage Alzheimer's disease: A single‐blind randomised controlled trial of clinical efficacy. The American Journal of Geriatric Psychiatry, 18(10), 928–939. 10.1097/JGP.0b013e3181d5792a [DOI] [PubMed] [Google Scholar]
- Clare, L. , & Woods, R. T. (2004). Cognitive training and cognitive rehabilitation for people with early‐stage alzheimer's disease: A review. Neuropsychological Rehabilitation, 14(4), 385–401. [Google Scholar]
- Coe, A. , Martin, M. , & Stapleton, T. (2019). Effects of an occupational therapy memory strategy education group intervention on Irish older adult's self‐management of everyday memory difficulties. Occupational Therapy in Health Care, 33(1), 37–63. 10.1080/07380577.2018.1543911 [DOI] [PubMed] [Google Scholar]
- Cotelli, M. , Manenti, R. , Zanetti, O. , & Miniussi, C. (2012). Non‐pharmacological intervention for memory decline. Frontiers in Human Neuroscience, 6(46), 1–17. 10.3389/fnhum.2012.00046 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Vreese, L. P. , Neri, M. , Fioravanti, M. , Belloi, L. , & Zanetti, O. (2001). Memory rehabilitation in Alzheimer's disease: A review of progress. International Journal of Geriatric Psychiatry, 16(8), 794–809. 10.1002/gps.428 [DOI] [PubMed] [Google Scholar]
- de Werd, M. , Boelen, D. , Olde Rikkert, M. , & Kessels, R. (2013). Errorless learning of everyday tasks in people with dementia. Clinical Interventions in Aging, 13(8), 1177–1190. 10.2147/CIA.S46809 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Folstein, M. F. , Folstein, S. E. , & McHugh, P. R. (1975). Mini‐mental state: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research, 12(3), 189–198. 10.1016/0022-3956(75)90026-6 [DOI] [PubMed] [Google Scholar]
- Gibb, M. , O'Caheny, D. , Craig, C. , & Begley, E. (2019). The Next Steps: Dementia post diagnostic guidance. National Dementia Office.
- Graff, M. J. , Vernooij‐Dassen, M. J. , Thijssen, M. , Dekker, J. , Hoefnagels, W. H. , & Rikkert, M. G. (2006). Community based occupational therapy for patients with dementia and their care givers: Randomised controlled trial. British Medical Journal, 333, 1196–1199. 10.1136/bmj.39001.688843.BE [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin, J. M. , Riffin, C. , Havyer, R. D. , Biggar, V. S. , Comer, M. , Frangiosa, T. L. , & Bangerter, L. R. (2020). Integrating family caregivers of people with Alzheimer's disease and dementia's into clinical appointments: Identifying potential best practices. Journal of Applied Gerontology, 39(11), 1184–1194. 10.1177/0733464819880449 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health Service Executive . (2021). Dementia signs and symptoms. Dementia understand together. https://www.understandtogether.ie/about-dementia/what-is-dementia/signs-and-symptoms/
- Kim, S. (2015). Cognitive rehabilitation for elderly people with early‐stage Alzheimer's disease. Journal of Physical Therapy Science, 27, 543–546. 10.1589/jpts.27.543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Law, M. , Baptiste, S. , Carswell, A. , McColl, M. A. , Polatajko, H. , & Pollock, N. (2014). Canadian Occupational Performance Measure (COPM) (5th ed.). COAT Publications ACE. https://eprovide.mapi-trust.org/instruments/canadian-occupational-performance-measure [Google Scholar]
- McGrath, M. , & Passmore, P. (2009). Home‐based memory rehabilitation programme for persons with mild dementia. Irish Journal of Medical Science, 178(8), 267–338. 10.1007/s11845-009-0409-2 [DOI] [PubMed] [Google Scholar]
- Moebs, I. , Gee, S. , Miyahara, M. , Paton, H. , & Croucher, M. (2017). Perceptions of a cognitive rehabilitation group by older people living with cognitive impairment and their caregivers: A qualitative interview study. Dementia, 16(4), 513–522. 10.1177/1471301215609738 [DOI] [PubMed] [Google Scholar]
- Mulhern, B. , Rowen, D. , & Brazier, J. (2013). Development of DEMQOL‐U and DEMQOL‐PROXY‐U: Generation of preference based indices from DEMQOL and DEMQOL‐PROXY for use in economic evaluation. Health Technology Assessment, 17(5), 1–140. 10.3310/hta17050 [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute for Health and Care Excellence (NICE) . (2018). Dementia: Assessment, management and support for people living with dementia and their carers. https://www.nice.org.uk/guidance/ng97 [PubMed]
- O'Shea, E. , Cahill, S. , & Pierce, M. (2017). Developing and implementing dementia policy in Ireland. The Atlantic Philanthropies. The Atlantic Philanthropies. https://www.atlanticphilanthropies.org/wp-content/uploads/2018/01/Developing-and-Implementing-Dementia-Policy-in-Ireland.pdf [Google Scholar]
- Prince, M. , Albanese, E. , Guerchet, M. , & Prina, M. (2014). World Alzheimer report 2014 dementia and risk reduction: An analysis of protective and modifiable risk factors. Alzheimer's Disease International. https://www.alzint.org/u/WorldAlzheimerReport2014.pdf
- Prince, M. , Wimo, A. , Guerchet, M. , Ali, G. , Wu, Y.‐T. , Prina, M. , & Alzheimer's Disease International . (2015). World Alzheimer report 2015. The global impact of dementia: An analysis of prevalence, incidence, cost and trends. https://www.alzint.org/u/WorldAlzheimerReport2015.pdf
- Sitzer, D. I. , Twamley, E. W. , & Jeste, D. V. (2006). Cognitive training in Alzheimer's disease: A meta‐analysis of the literature. Acta Psychiatrica Scandinavica, 114(2), 75–90. 10.1111/j.1600-0447.2006.00789.x [DOI] [PubMed] [Google Scholar]
- Smith, S. C. , Lamping, D. L. , Banerjee, S. , Harwood, R. H. , Foley, B. , Smith, P. , Cook, J. C. , Murray, J. , Prince, M. , Levin, E. , Mann, A. , & Knapp, M. (2007). Development of a new measure of health‐related quality of life for people with dementia: DEMQOL. Psychological Medicine, 37(5), 737–746. 10.1017/S0033291706009469 [DOI] [PubMed] [Google Scholar]
- Smith, S. C. , Lamping, D. L. , Banerjess, S. , Harwood, R. , Foley, B. , Smith, P. , Cook, J. C. , Murray, J. , Prince, M. , Levin, E. , Mann, A. , & Knapp, M. (2005). Measurement of health‐related quality of life for people with dementia: Development of a new instrument (DEMQOL) and an evaluation of current methodology. Health Technology Assessment, 9(10), 1–93. 10.3310/hta9100 [DOI] [PubMed] [Google Scholar]
- Toglia, J. , & Kirk, U. (2000). Understanding awareness deficits following brain injury. NeuroRehabilitation, 15, 57–70. https://pubmed.ncbi.nlm.nih.gov/11455082/, 10.3233/NRE-2000-15104 [DOI] [PubMed] [Google Scholar]
- Turner‐Stokes, L. , Nyein, K. , Turner‐Stokes, T. , & Gatehouse, C. (1999). The UK FIM + FAM: Development and evaluation; functional assessment measure. Clinical Rehabilitation, 13(4), 277–287. 10.1191/026921599676896799 [DOI] [PubMed] [Google Scholar]
- Viola, L. F. , Nunes, P. V. , Yassuda, M. S. , Aprahamian, I. , Santos, F. S. , Santos, G. D. , Brum, P. S. , Borges, S. M. , Oliveira, A. M. , Chaves, G. F. , Ciasca, E. C. , Ferreira, R. C. , Paula, V. J. , Takeda, O. H. , Mirandez, R. , Watari, R. , Falcao, D. V. , Cachiono, M. , & Forlenza, O. (2011). Effects of a multidisciplinary cognitive rehabilitation program for patients with mild Alzheimer's disease. Clinics, 66(8), 1395–1400. 10.1590/s1807-59322011000800015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wenborn, J. , O'Keeffe, A. G. , Mountain, G. , Moniz‐Cook, E. , King, M. , Omar, R. Z. , Mundy, J. , Burgess, J. , Poland, F. , Morris, S. , Pizzo, E. , Vernooij‐Dassen, M. , Challis, D. , Michie, S. , Russell, I. , Sackley, C. , Graffe, M. , Swinson, T. , Crellin, N. , & Orrell, M. (2021). Community occupational therapy for people with dementia and family carers (COTiD‐UK) versus treatment as usual (valuing active life in dementia [VALID]) study: A single‐blind randomised controlled trial. PLoS Medicine, 18(1), 1–19, 10.1371/journal.pmed.1003433 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson, B. A. (2002). Towards a comprehensive model of cognitive rehabilitation. Neuropsychology Rehabilitation, 12(2), 97–110. 10.1080/09602010244000020 [DOI] [Google Scholar]
- Wilson, B. A. , Greenfield, E. , Clare, L. , Baddeley, A. , Cockburn, J. , Watson, P. , Tate, R. , Sopena, S. , & Nannery, R. (2008). The rivermead behavioural memory test (3rd ed.). Pearson Assessment. [Google Scholar]
- Wolff, J. , Darer, J. , Berger, A. , Clarke, D. , Green, J. , Stametz, R. A. , & Walker, J. (2017). Inviting patients and care partners to read doctors' notes: Open notes and shared access to electronic medical records. Journal of the American Medical Informatics Association, 24(e1), e166–e172. 10.1093/Jamia/Ocw108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organisation . (2019). Risk reduction of cognitive decline and dementia: WHO guidelines. [PubMed]
- World Health Organisation . (2021). Dementia. https://www.who.int/news-room/fact-sheets/detail/dementia
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Research data are not shared.