

Accessible Summary
What is known on the subject?
The Safewards model has been introduced to forensic mental health wards with mixed results.
Research has identified a need to consider the addition of factors that may be relevant to forensic mental health services to enhance the introduction of Safewards.
What the paper adds to existing knowledge?
This study elicits factors specific to forensic mental health settings missing from the original Safewards model, which have the potential to enhance nursing care, improve safety and improve adherence to Safewards in a forensic mental health setting.
What are the implications for practice?
This study provides the adaptation required in a forensic mental health setting to enhance the implementation of the Safewards model of care, originally developed to assist nurses to prevent and manage conflict and containment in acute general mental health settings.
The development of Safewards Secure has incorporated perspectives from expert Safewards and forensic mental health nurse leaders and healthcare clinicians and is inclusive of consumer and carer perspectives to ensure the model is applicable and broadly acceptable.
Abstract
Introduction
Safewards is a model designed specifically for acute mental inpatient wards. Research investigating the introduction of Safewards has identified a need to consider factors relevant in forensic mental health services, such as offence and risk issues.
Aim
To identify adaptations needed to address gaps in the Safewards model to assist forensic mental health nurses to prevent and manage conflict and containment.
Method
A Delphi study was employed to engage a group of international Safewards and forensic mental health experts (n = 19), to elucidate adaptation of the Safewards model.
Results
Experts identified necessary elements and reached consensus on key considerations for Safewards interventions. To ensure the Safewards Secure model was robust and developed on a platform of research, all items suggested by Delphi experts were cross‐referenced and dependent on empirical evidence in the literature.
Discussion
This study identified a number of key differences between civil and forensic mental health services, which informed the development of Safewards Secure, an adjunct to the original Safewards model.
Implications for Practice
The development of person‐centred models of nursing care adapted to specific settings, such as forensic mental health, provides a potential solution to preventing and managing conflict and containment, and improving consumer outcomes.
Relevance Statement
Managing conflict and containment in mental health services remains an ongoing challenge for mental health nurses. Safewards is a model of care designed for acute mental health inpatient settings to prevent conflict and containment. To date, there has been mixed results when introducing Safewards in forensic mental health settings, and reported reluctance and scepticism. To address these issues, this study employed a Delphi design to elicit possible adaptions to the original Safewards model. From this study, Safewards Secure was developed with adaptations designed for forensic services, to enhance the management of conflict and containment, assist implementation and improve consumer outcomes.
Keywords: acute mental health, aggression, forensic, restraint, violence
1. INTRODUCTION
Safewards is a model of care that provides a framework for nurses to prevent conflict (events that threaten staff or consumer safety, e.g. aggression, self‐harm, suicide and absconding) and containment events (interventions staff undertake to prevent conflict from occurring, e.g. the use of restrictive interventions, such as restraint and seclusion) (Bowers et al., 2014). The Safewards model was designed specifically for acute mental health wards in civil mental health services, where the introduction of Safewards has produced positive findings in the reduction of conflict and containment events (Bowers et al., 2014; Fletcher et al., 2017; Stensgaard et al., 2018). Despite success in civil mental health wards, research related to forensic mental health service introduction of the Safewards model has reported challenges with implementation and acceptance (Cabral & Carthy, 2017; Maguire et al., 2018; Price et al., 2016; Whitmore, 2017).
2. BACKGROUND
Forensic mental health services provide assessment and treatment within a secure environment, for people who have a mental illness and a history of violent offending or are considered to be at high risk of such offending (Maguire & McKenna, 2020). In this setting, nurses work with individuals to treat symptoms of mental illness, address offending behaviour, enhance quality of life, reduce the likelihood of future offending and, where possible, support reintegration into the community (Martin et al., 2012).
Historically, the development of forensic mental health services has been marred by care practices delivered via compulsory treatment, and at times in authoritarian, custodial and coercive environments, which were often not person‐centred (Gillespie & Flowers, 2009). Contemporary mental health policies in many countries have endorsed the need for mental health services, and the workforce to practice person‐centred, recovery‐oriented care (Hornik‐Lurie et al., 2018; Shera & Ramon, 2013), including in forensic mental health services (Maguire & McKenna, 2020).
There are a number of challenges to the establishment of recovery‐oriented care in forensic mental health settings, related to inherent restrictions due to compulsory admission and detainment in a secure setting (Livingston et al., 2012; Simpson & Penney, 2011). The presence of challenging behaviours, which can place others at serious risk of harm (Sturmey & McMurran, 2011), and higher use of restrictive interventions (Maguire, Ryan, et al., 2020) can result in psychological, emotional and physical harm for staff and consumers. This in turn can negatively influence the therapeutic milieu (Brophy et al., 2016; Pelto‐Piri et al., 2020; Whitmore, 2017). Yet, services should provide care in the least restrictive manner, while working to reduce aggression and use of restrictive practices (Department of Health, 2013; O'Rourke et al., 2018). Safewards is directed towards this intent. It was developed for acute mental health wards to explore the relationship between conflict and containment, identify opportunities to intervene and generate ideas for change that have the potential to prevent and reduce conflict and containment (Bowers et al., 2014).
Safewards has been introduced to acute mental health, and forensic mental health services in many countries including the UK, Australia, Canada and Germany (see Baumgardt et al., 2019; Fletcher et al., 2017; James et al., 2017; Whitmore, 2017). Safewards is a multidisciplinary model, though resonates in particular with nursing practice, as many of the interventions are based on sound mental health nursing principles (Price et al., 2016).
The model covers six domains (the physical environment, the staff team, the service user characteristics, influences outside the hospital, the inpatient community and the regulatory framework mandating care). The model identifies key influences in each of the six domains, and these key influences can give rise to conflict and containment events. For example in the inpatient community domain, a key influence is discord among the consumer group, which can lead to conflict between consumers, which may then result in staff use of containment measures to prevent or minimize the conflict (Bowers, 2014).
The model articulates “flashpoints” as circumstances, which arise in each of the six domains that signal the potential for conflict (e.g. in the inpatient community domain, flashpoints include crowding, queuing and instability associated with staff and service user turnover) (Bowers, 2014). The model also describes staff modifiers, “features of the staff as individuals or teams that have the ability to impact on the occurrence of conflict and/or containment” (Bowers, 2014, p. 500). The model includes interventions designed to reduce conflict and containment by acting on flashpoints (Fletcher, Hamilton, et al., 2019). While a range of interventions are identified, there are ten interventions that were tested in the development of the model, and commonly used in practice (“clear mutual expectations,” “soft words,” “talk down,” “positive words,” “bad news mitigation,” “know each other,” “mutual help meetings,” “calm down methods,” “reassurance” and “discharge messages”).
The model has been subject to a randomized controlled trial (RCT), where a significant reduction in both conflict (15%) and containment rates (26%) were reported, as compared to the wards that received the control intervention (Bowers et al., 2015). Since the initial RCT, there have been a number of studies published on Safewards indicating a positive impact on reducing conflict and containment, and improvement in ward atmosphere (Baumgardt et al., 2019; Fletcher et al., 2017 ; Fletcher, Buchanan‐Hagen, et al., 2019; Fletcher, Hamilton, et al., 2019; Hottinen et al., 2020; Stensgaard et al., 2018). Ward atmosphere refers to the social climate of the ward and is influenced by staff and consumers, social conditions and events that occur on the ward (Efkemann et al., 2019).
There have also been studies evaluating the introduction of Safewards in forensic mental health services. Some studies have reported an improvement in ward atmosphere (Cabral & Carthy, 2017; Maguire et al., 2018); however, some did not find any indication of a significant reduction in conflict and containment events (Maguire et al., 2018; Price et al., 2016). Furthermore, some studies have reported resistance, scepticism, frustration, sabotage, fracture occurring in teams and anxiety when introducing Safewards, along with resistance and/or poor adherence to the interventions (Cabral & Carthy, 2017; Price et al., 2016). In particular, the “discharge messages” intervention (whereby positive messages of the inpatient stay, and helpful pieces of advice are posted for others to see, when a consumer is discharged from the ward) has been highlighted as problematic to introduce, where there may be few discharges (Maguire et al., 2018; Price et al., 2016).
To give the optimum opportunity for Safewards to function effectively in forensic mental health services, consideration needs to be given to the adaptation of the key influences in the six domains, the corresponding flashpoints and relevant interventions in forensic mental health inpatient settings (Maguire et al., 2018; Whitmore, 2017). The aim of this study was to engage Safewards and forensic mental health experts in identifying potential adaptations that may be needed to address gaps in the Safewards model, and develop a model for forensic mental health services, incorporating the essence of the Safewards model, to enhance adherence, acceptability and implementation of the model in forensic mental health services.
3. METHOD
3.1. Study design
This study employed a Delphi design, a systematic communication technique, to seek responses from a panel of Safewards and forensic mental health international experts. The Delphi method has been used widely in social science research (Keeney et al., 2001), and employs experts in a multistage approach, with each Delphi round, building on the results of the previous round, as the experts work towards consensus (McKenna, 1994). Important considerations in the selection of experts include, having a diverse range of experience, the ability of the Delphi members to be able to make their decisions independently (Jorm, 2015).
In this study, the researchers sought experts from a range of disciplines, though primarily nurses, and experts with significant experience in forensic mental health and/or Safewards. Consumer and carer consultants were also included to ensure diverse perspectives (Jorm, 2015) and to ensure the consumer and carer voice were represented in the Safewards model for forensic mental health services. The researchers all have experience in forensic mental health practice and research, and Safewards research.
Experts were engaged in the study through a series of questionnaires sent by the researchers via email. For each round, Delphi members were presented with contextual information and questions (see detail below), which they were asked to respond to, and return to the researchers. The data were collated and sent back to the experts in a summarized form. The Delphi experts then reviewed the summary independently and sent back their response to the researchers. The researchers then provided further feedback in the form of a summary. This process of feedback and refinement continued until there was consensus among the Delphi members. For the purpose of reporting this study, the Standards for Reporting Qualitative Research (SRQR) was used (O'Brien et al., 2014). The SRQR was designed to provide clear standards for reporting qualitative research (O'Brien et al., 2014).
3.2. Participants
Participants in this study included a combination of identified experts in forensic mental health and Safewards, across a range of disciplines (n = 19). An expert in forensic mental health was defined as a person working in a leadership role (e.g. Director of Nursing, forensic psychiatric consultant and senior consumer consultant). An expert in Safewards was defined as someone with experience in implementing, teaching or researching Safewards.
Expertise in Safewards was also confirmed by consultation with an international Safewards expert, who was involved in developing Safewards, and has since worked to disseminate Safewards to services. A snowball method of sampling was employed, whereby the initial group of experts invited participation to people they identified as a forensic mental health and/or Safewards expert.
3.3. Data collection
An open‐ended questionnaire was distributed in the first Delphi round. Delphi members were invited to provide a brief summary of their experience in Safewards and/or forensic mental health. The members were then asked to identify any key influences missing from the six domains, and corresponding flashpoints in a forensic mental health setting. Members were also asked to consider whether there was a need for any adjustments of Safewards interventions for forensic mental health services, and if they had experienced any difficulties when introducing the model or interventions.
In subsequent rounds, the researchers provided an anonymous summary of the experts’ suggestions from the previous round, and a summary of the rationale group members provided for their judgments. Delphi members were encouraged to revise their earlier replies in the light of a summary of participant's responses. During this iterative process, the range of diversity in responses decreased, and the group converged towards the selection of a preferred Safewards Secure model, and suggestions for the implementation of the Safewards interventions in a forensic mental health setting. This occurred after three Delphi rounds.
3.4. Data analysis
Data from each expert in round one were coded, tabulated, themed by the first author and then discussed with the research team, before being presented back to participants to initiate consideration of possible gaps in the Safewards model, and issues identified in the implementation of interventions for forensic mental health services. Participants were given the opportunity to provide commentary and justification throughout the Delphi process, and this information was taken into account during the thematic analysis. In subsequent Delphi rounds, descriptive statistics were used to present and describe the level of agreement among the experts for adaptations to the domains, flashpoints and interventions as suggested by the Delphi members. Reasons for divergent views were listed from the explanations provided by participants. Consensus was considered to be achieved when Delphi members were over 70% in agreeance.
3.5. Ethical considerations
Approval for this study was granted by the Forensicare Operational Research Committee and ethical approval to conduct the study was granted by the Swinburne Human Research Ethics Committee (SHREC Project 20191008–15). The study was conducted in compliance with the ethical guidelines of the Declaration of Helsinki (World Medical Association, 2001).
4. RESULTS
4.1. Description of participants
In the first round, n = 22 Delphi members were invited to participate in the initial questionnaire, of which n = 19 responded (86% response rate). In round two, n = 15 of 19 (79%) of Delphi members responded (however one expert responded late, so their response was not included, though they were not excluded from the third round). In round three, the final round, all 15 participants responded and responses were included in the analysis).
Out of the initial 19 experts who responded (n = 14), 74% were nurses, the remaining representatives were from social work (5%, n = 1), psychiatry (5%, n = 1), and the consumer and carer workforce (16%, n = 3). The experts were from Australia, Canada, Great Britain and New Zealand. Three participants were not forensic mental health experts; however, they had experience in teaching and consultation of Safewards in forensic mental health settings. Experience in forensic mental health among the remainder of participants included working directly with consumers in locations such as inpatient services, courts, community settings and prisons.
All forensic mental health experts had been employed (currently or recently) in either corporate or leadership roles (2%, n = 4,), research roles (3%, n = 3) practice development and/or educational roles (47%, n = 9), and/or family, carer and consumer consultant positions (16%, n = 3). All experts had a broad range of experience with Safewards including teaching, implementation, oversight, evaluation and mentoring consumers in Safewards.
4.2. Delphi rounds
4.2.1. Six Safewards domains
In round one, Delphi members identified a number of key influences. The key influences were then grouped or collapsed by the authors where possible. Following this process, a total number of 29 key influences were identified. The number of additional influences identified in each domain was as follows: physical environment (n = 2), the staff team (n = 5), the service user characteristics (n = 10), influences outside the hospital (n = 4), the inpatient community (n = 6) and the regulatory framework mandating care (n = 2).
In round two, Delphi members were then asked to indicate their support for these analyses applied to the identified key influences (Table 1). Delphi members reached a level of agreement of 70% and above on all but one key influence, which was “taking away hope” (57%), identified in the “staff team” domain, which was then excluded as a key influence on this basis. A literature search (using CINHAL and PsychINFO databases) was then conducted on each of the key influences, as suggested by the Delphi members to determine whether there was evidence in the literature (including evidence‐based frameworks) to support inclusion. Following the literature search, six key influences were removed due to the search producing little, to no empirical evidence, or where the evidence suggested no difference between forensic mental health and civil mental health. Following this process 23 key influences remained that were supported by evidence in the literature (Table 1). One of the 23 influences was reworded in line with the literature.
TABLE 1.
Additional domain key influences with level of consensus
| Safewards domain | Additional key influences | Consensus | |
|---|---|---|---|
| n of 14 | % | ||
| Physical environment |
|
12 | 86 |
| 12 | 86 | ||
| Staff team |
|
13 | 93 |
| 13 | 93 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| 8 | 57 | ||
| Service users characteristics |
|
12 | 86 |
| 10 | 71 | ||
| 11 | 79 | ||
| 12 | 86 | ||
| 12 | 86 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| 12 | 86 | ||
| Outside hospital |
|
13 | 93 |
| 13 | 93 | ||
| 100 | |||
| 100 | |||
| Inpatient community |
|
12 | 86 |
| 11 | 79 | ||
| 12 | 86 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| 13 | 93 | ||
| Regulatory framework mandating care |
|
100 | |
| 11 | 79 | ||
Key influences with no or little empirical evidence.
Key influences and flashpoints reworded in line with literature.
4.3. Flashpoints
In round one, Delphi members identified 14 additional flashpoints for the six Safewards domains. In round two, Delphi members were asked to indicate their support for these additional flashpoints. The Delphi members reached over 70% consensus on all of the flashpoints, with two reaching unanimous agreement (Table 2). After the second round, a literature search was also conducted on the flashpoints as suggested by the Delphi participants, to determine whether there was evidence in the literature to support inclusion. There was scholarly evidence in the literature to support all flashpoints; however, three flashpoints were reworded to reflect the language used in the literature. Many of the flashpoints were related to tension and the impact of various index offences/offending behaviour, interpersonal communication and the inherent restrictions present in forensic mental health settings, which is reflected in the forensic mental health literature.
TABLE 2.
Additional flashpoints identified with level of consensus
| Domain | Flashpoint | Consensus | |
|---|---|---|---|
| n of 14 | % | ||
| Physical environment |
|
12 | 86 |
| Staff team |
|
10 | 71 |
| 13 | 93 | ||
| 13 | 93 | ||
| Service users characteristics |
|
13 | 93 |
| 13 | 93 | ||
| 11 | 79 | ||
| Outside hospital |
|
13 | 93 |
| Inpatient community |
|
13 | 93 |
| 13 | 93 | ||
| 14 | 93 | ||
Flashpoints reworded in line with the literature.
4.4. Safewards interventions
In round one, Delphi members provided a range of issues and observations regarding the use of the Safewards interventions in a forensic mental health setting. Comments for each intervention were grouped together and collapsed where possible. In the second round, Delphi members were presented with these analyses, along with comments for divergent views, and asked to indicate whether they agreed or disagreed (Table 3). The issues and observations on the interventions that did not achieve consensus (over 70%) after round 2 were disregarded. Six of the issues/observations were below 70% agreement, four reached unanimous agreement, and the remainder reached consensus.
TABLE 3.
Safewards interventions with level of consensus agreement and decision
| Safewards intervention | Issues/observations identified | n of 14 | % |
|---|---|---|---|
| Soft words |
|
9 | 64 |
| 8 | 57 | ||
| Positive words |
|
9 | 64 |
| Calm down methods |
|
14 | 100 |
| 8 | 57 | ||
| Talk down |
|
10 | 71 |
| Discharge messages |
|
13 | 93 |
| 13 | 93 | ||
| 6 | 43 | ||
| 2 | 14 | ||
| Mutual help meeting |
|
13 | 93 |
| Clear mutual expectations |
|
14 | 100 |
| Reassurance |
|
12 | 86 |
| Bad news mitigation |
|
13 | 93 |
| 14 | 100 | ||
| Know each other |
|
14 | 100 |
The final list of considerations when introducing the Safewards interventions into a forensic mental health service developed from the Delphi study is shown in Table 4, which were also agreed on by the Delphi members.
TABLE 4.
Considerations when introducing the Safewards interventions into a FMH service
| Safewards intervention | Considerations in a fmh setting |
|---|---|
| Soft words | Soft Words is a flexible intervention designed to adjust the culture of the unit and can improve relationships in any environment including FMHS |
| Positive words | Positive words requires some cognitive flexibility on behalf of staff. It is crucial FMHS professionals remain clinically focused and provide accurate and balanced information during handovers free from personal frustrations. Positive words also create an opportunity to understand behaviour that may be related to illness, trauma and offence issues |
| Calm down methods | There is a need for creativity in regard to what people can have access to with and without supervision, and possibly the language used to describe calm down methods |
| Talk down | Consideration of interpersonal styles that are hostile‐dominant, and how to engage best with this style of interaction may be helpful to consider when teaching and using talk down in practice |
| Hope messages | Given that in some services consumers may be rarely discharged from wards, messages about progress maybe more helpful in a FMH setting |
| Mutual help meeting | Staff need to remain involved in mutual help meetings in any setting, and in FMHS it is also very important for staff to get to know the consumer group, see the positive aspects of the consumer group, and to support consumers who may be more vulnerable in the community |
| Clear mutual expectations | Clear mutual expectations may be enhanced in FMHS as the community is together longer |
| Reassurance | The reassurance intervention may change as consumer's progress through the FMHS. For example, consumers in the initial stages of admission may need more reassurance when the consumer group and environment is new to them. Reassurance may also be crucial later on in the pathway, especially if progress is slow |
| Bad new mitigation | In FMHS, there is the increased possibility of criminal justice decisions being made with lack of consumer or staff control. There is a need for an increased awareness of additional restrictions on consumers and the impact of these on the future and hope, e.g. longer length of stay, less access to the outside world (community, community activity, family etc.) |
| Know each other | FMHS may be more conscious about sharing information, and this may result in a greater resistance towards this intervention from staff and consumers. However, there is information that can be shared that will not cross non‐negotiable boundaries. It should also be noted that the community is together for longer periods of time and consumers may get to know a lot of information about individual staff members over time as a consequence. This is also an important intervention that signals a move away from custodial settings |
4.5. Development of the Safewards Secure Model
The Delphi members were asked to consider how to best integrate the identified key influences and flashpoints. The decision by the Delphi group (71% consensus) was to retain the original model and add an appendage to the model to create Safewards Secure. Therefore, three models of a potential Safewards Secure model were suggested, and participants were asked to indicate their preference with a rationale. The three depictions of the model were 1) the original Safewards model located in the centre of a Safewards Secure model; 2) the Safewards model on the left hand side with a plus symbol, and the Safewards Secure model located on the right‐hand side; and 3) the Safewards model in the centre, with the six domains from the Safewards Secure model feeding into the original Safewards model. The Safewards Secure model selected by the majority (73%) was model three (Figure 1).
FIGURE 1.
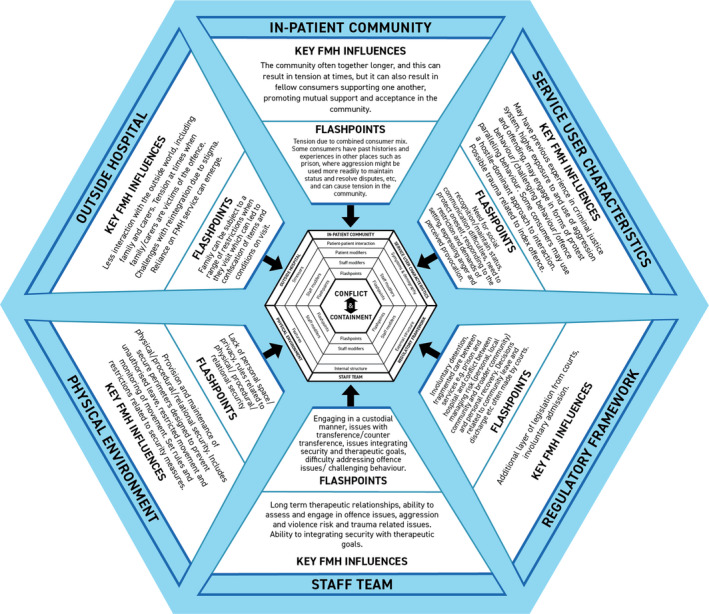
Safewards Secure Model
5. DISCUSSION
The aim of this study was to identify adaptations needed to address current gaps in the Safewards model for forensic mental health services and to develop a model for forensic mental health services to use in conjunction with the original Safewards model (Safewards Secure). Employing a Delphi method with forensic mental health and Safewards experts facilitated the identification of a number of key influences and flashpoints specific to forensic mental health care, not present in the original Safewards model. The Delphi members also identified a number of considerations for forensic mental health services when implementing the ten commonly used Safewards interventions. Findings from this study support a desire for adaption of Safewards for forensic mental health services.
5.1. Key influences
Delphi members were able to identify key influences for each Safewards domain, specific to forensic mental health. The identification of these influences offers some insight into key differences between civil mental health and forensic mental health services, while also signalling some potential challenges for forensic services when implementing the original Safewards model. The key influences related to a range of consumer factors (e.g. prisoner status, offence issues, use of aggression and experience of trauma) and contextual factors (e.g. extended length of stay, issues integrating security into therapeutic care, assessment and engagement in addressing offence issues), and these findings contribute to a clearer understanding of the unique challenges present in forensic mental health settings.
As identified by the Delphi members, many consumers who are admitted to forensic mental health services have spent time in prison prior to admission, where hostile behaviour and conflict with others are often resolved by aggression and may also be used to gain or enhance status (Daffern et al., 2005, 2007). Use of aggression and violence is also often the very reason people are admitted to forensic mental health services (Cabral & Carthy, 2017). While forensic mental health services acknowledge the inherent tension in working with a consumer group that presents with high risk of engaging in aggression and violence (Maguire, Carroll, et al., 2020), in practice this often means staff (most often nurses) are working in unpredictable and stressful environments, where many of the consumers are also presenting with persisting complex mental health needs and high risk behaviours (Barr et al., 2019; Maguire et al., 2012). Forensic mental health services are also challenged with increasing numbers of people within prison services with serious mental health issues, and increasing bed pressure (Fazel et al., 2016; Jansman‐Hart et al., 2011; Priebe et al., 2005). Nurses working in such settings need to be trained and supported to work with forensic consumers confidently and safely (Barr et al., 2019). The inclusion and acknowledgement of forensic mental health‐specific influences in Safewards Secure may assist nurses and other staff in this complex task.
For participants in this study, the inclusion of offending issues as a key influence for forensic mental health services in Safewards Secure was considered important. The original Safewards model does not include offending behaviour, and nor should it, as the model was designed for acute civil mental health wards. The presence and need to address offending issues are features that distinguish forensic mental health nursing practice, from nurses working in civil mental health settings (Martin, 2010; Martin et al., 2012). The inclusion of offending behaviour reflects the practice reality in forensic mental health nursing, where care and treatment needs to include attention to offending issues. Forensic mental health nurses are required to establish trusting relationships with consumers to assess risk; develop strategies for interventions that address offending behaviour; and evaluate the effectiveness of these interventions (Carton, 1998; Hammarström et al., 2019). While offending is not the only factor nurses need to address, it is important that offending is included as part of holistic care, as failing to address offending behaviour results in a significant part of the persons experience not being addressed (Martin, 2010; Martin et al., 2012).
Despite recognition in the literature that addressing offending behaviour is an expected role in the therapeutic process of reducing and managing risk (Martin et al., 2012; Woods et al., 2002), forensic mental health nursing has been criticized for not fully incorporating assessment, intervention and documentation of offending behaviour into practice (Martin & Street, 2003). Furthermore, despite the need to attend to offending behaviour, as evidenced in the literature, there is currently no nursing model of care that integrates interventions that address offending. Inclusion of offending in Safewards Secure may assist in this endeavour, as offending behaviour was considered to have an influence on each of the key domains in Safewards Secure. For example, in the staff team domain, offending requires staff to have the skills and knowledge to address the offending behaviour. In the consumer characteristics domain, consumers may have experienced trauma in relation to their offending. While in the hospital domain, there may be tensions when families/carers have been the victim of the offence. Inclusion of the role of offending behaviour in Safewards Secure may prompt related assessment and intervention.
Consideration of these unique key influences may be helpful in providing a more comprehensive understanding of conflict and containment in forensic mental health settings and may resonate with staff, especially given that previous studies have identified staff resistance and anxiety regarding the introduction of Safewards. This may then impact on uptake and adherence to the interventions (Cabral & Carthy, 2017; Price et al., 2016). This study has identified a need to consider relevant factors specific to forensic mental health settings, rather than assuming there will be no necessary adaptions required for forensic mental health services (Price et al., 2016).
5.2. Flashpoints
The Delphi members also identified specific flashpoints as they relate to the key influences across the Safewards Secure domains. The flashpoints included consumer and contextual related events and/or situations considered most likely to trigger conflict or containment events in a forensic mental health setting.
Consumer‐related flashpoints included expression of anger, perceived provocation and the need to maintain status. These personal factors have also been identified in the literature related to prison and forensic mental health settings (Daffern & Howells, 2002; Maguire et al., 2012; Maguire, Carroll, et al., 2020). While it is important to identify consumer‐related factors, it is also important to highlight that consumer characteristics comprises one domain out of the six Safewards domains. Price et al. (2016) noted that staff tend to attribute conflict due to consumer factors, rather than contextual factors, and recommend Safewards education and implementation would benefit from emphasis on relevant contextual factors. Importantly, the Delphi members also identified a diverse range of contextual factors inherent in forensic mental health settings that are likely to trigger conflict and containment events, as evidenced in the extant literature. The flashpoints identified by the Delphi members were related to restrictions related to perceived risk and forensic consumer status; a range of physical, procedural and relational security measures; involuntary (and sometime prolonged) containment; and the inability of members of the team to work with consumers to address issues such as offending and challenging behaviour to integrate security requirements with therapeutic care.
5.3. Issues implementing Safewards interventions
Delphi members indicated that challenges in implementing the Safewards interventions reflected environments in which restrictions, long‐term detention and consumer‐related factors such as hostile‐dominant ways of responding were part of the everyday reality. Such challenges are not insurmountable and collaboration between staff and consumers could be used to refine the interventions to suit the context. An example of such collaboration might involve the examination of discharge messages with attention given to the intention of the intervention. As such, discharge messages intend to “imbue hope and convey authoritative messages about the purpose and benefit of an admission” (Safewards 2021). Collective discussion and consideration about how the intent can be retained, when discharge rates are low, may result in adaptation of the intervention, to better suit the needs and inherent issues in a forensic mental health setting. There may be opportunity to substitute “discharge” with “progression” through the forensic mental health service, together with celebration of completion of other short‐term goals that accumulate towards discharge or transfer to lesser restrictive environments.
It is also important to note that while there may be challenges in implementing Safewards interventions, there are also opportunities inherent in the forensic mental health setting. For example, while lengthy hospital stays for consumers can create tension, and potentially lead to flashpoint, spending longer periods of time together may actually enhance some of these interventions, as forensic mental health wards generally do not experience the constant churn of admissions and discharges, allowing more time for staff to build a therapeutic alliance with consumers, and for the consumer group to get to know each other. For example, mutual help meetings may be enhanced by having a stable consumer and staff team and may better facilitate consumers positively appreciate each other in the longer term.
5.4. Strengths and limitations of this study
A key strength of this study was the broad selection of international Delphi experts, with the inclusion of consumer consultants/experts by experience and family carer consultant representation. The expertise of the Delphi members enabled insight into the clinical reality, and difficulties encountered when introducing Safewards in forensic mental health settings.
One potential limitation is the arbitrary setting of the consensus measure at 70% of the participants; however, there is evidence to suggest that agreement at 70% and above is sufficient (Feo et al., 2018; Hsu & Sandford, 2007). Furthermore, the number of participants was small, with a total of 15 responding in the final round. It is also possible there are other Safewards and forensic mental health experts, who were not captured in the snowball sampling, from the four countries represented in this study, who may arrive at different consensus conclusions. However, checking out the consensus decisions in relation to evidence‐based literature did offset the potential for the consensus to be influenced by the unique characteristics of the actual Delphi participants.
The decision to only include adaptations for Safewards Secure that were supported by evidence in the literature was made on the basis that the original Safewards model was developed in a similar way (Bowers et al., 2014). Replicating this process for Safewards Secure resulted in suggestions for change by the Delphi members either being removed, or reworded in line with the literature. While some suggestions from Delphi experts could not be located within the scholarly literature, this does not indicate that these suggestions are not indeed valid. There are some areas in forensic mental health practice that have received very little research attention, especially in regard to the consumer, family/carer experience and perspective.
6. CONCLUSION
The findings from this Delphi study supported the development of a potentially robust Safewards Secure model, which includes key influences and flashpoints, and some considerations for implementation of interventions, all of which are unique to the forensic mental health setting. Safewards Secure was derived from a broad range of international experts in the field and validated by the inclusion of items supported by empirical evidence. It is important to highlight Safewards Secure is not to be used without the original Safewards model, rather as an adjunct to the original model. Further research is required to test Safewards Secure, evaluate the impact in forensic mental health settings and further refine the interventions.
7. RELEVANCE TO PRACTICE
Findings from this study can be used to enhance the implementation of Safewards in forensic mental health settings in several ways. The addition of Safewards Secure can provide a framework for discussion regarding key differences from civil mental health services. In particular, the identification of offending issues and unique contextual factors is important for forensic mental health services to consider, to assist training, implementation and acceptance in this setting (Bowers, 2014; Price et al., 2016). When implementing Safewards Secure, we suggest that it may be helpful for the training to spend some time discussing offence/risk issues and how they influence care and treatment in forensic mental health settings, and consideration of local contextual factors and the influence they have on the six Safewards domains and flashpoints. Furthermore, the suggestions from the Delphi experts outlining the interventions provide some direction for forensic mental health staff in how these might be best implemented in a forensic mental health setting.
The areas identified by Delphi experts that were not included in the model could signal potential research opportunities. It is also worth noting that some of the suggestions such as forensic mental health nurses experiencing higher rates of trauma as compared to civil mental health nurses were not supported in the literature. To be included in the model, there needed to be clear differences from civil mental health services. Evidence suggests that forensic mental health nurses may display similar levels of post‐traumatic stress reactions and general distress, to civil mental health nurses (Lee et al., 2015). This in no way negates the impact of trauma or post‐traumatic stress in forensic mental health nurses, rather it signals this is an issue across many settings, and not unique to forensic mental health nursing.
The introduction of Safewards and Safewards Secure may offer a significant shift from authoritarian custodial practice often associated with forensic mental health services and instead provide a recovery‐oriented and person‐centred framework. The findings from this study also have implications for future research in regard to test the model, the need for further work to establish staff and consumer modifiers, and to establish whether Safewards Secure enhances motivation of staff and consumers to engage with the model. The work undertaken to establish suitable additions for forensic mental health services might signal an approach for other specialized areas such as aged care, children and adolescent mental health settings and prison services, when introducing Safewards.
CONFLICT OF INTEREST
The authors report no conflict of interest.
ACKNOWLEDGEMENTS
The authors wish to thank Ms Katie Richardson for her effort and contribution into the design of the Safewards Secure model. All authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, where all authors contributed to study design, data collection, data analysis and write up. All authors are in agreement with the manuscript. Open access publishing facilitated by Swinburne University of Technology, as part of the Wiley ‐ Swinburne University of Technology agreement via the Council of Australian University Librarians. [Correction added on 18 May 2022, after first online publication : Funding statement has been added.]
Maguire, T. , Ryan, J. , Fullam, R. , & McKenna, B. (2022). Safewards Secure: A Delphi study to develop an addition to the Safewards model for forensic mental health services. Journal of Psychiatric and Mental Health Nursing, 29, 418–429. 10.1111/jpm.12827
Funding information
The authors received no financial support for the research, authorship and/or publication of this article
DATA AVAILABILITY STATEMENT
Data are available on request due to privacy/ethical restrictions. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
- Barr, L. , Wynaden, D. , & Heslop, K. (2019). Promoting positive and safe care in forensic mental health inpatient settings: Evaluating critical factors that assist nurses to reduce the use of restrictive practices. International Journal of Mental Health Nursing, 28(4), 888–898. 10.1111/inm.12588 [DOI] [PubMed] [Google Scholar]
- Baumgardt, J. , Jäckel, D. , Helber‐Böhlen, H. , Stiehm, N. , Morgenstern, K. , Voigt, A. , Schöppe, E. , Mc Cutcheon, A. K. , Lecca, E. , Löhr, M. , Schulz, M. , Bechdolf, A. , & Weinmann, S. (2019). Preventing and reducing coercive measures: An evaluation of the implementation of the Safewards model in two locked wards in Germany. Frontiers in Psychiatry, 10, 340. 10.3389/fpsyt.2019.00340 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowers, L. (2014). Safewards: A new model of conflict and containment on psychiatric wards. Journal of Psychiatric and Mental Health Nursing, 21, 499–508. 10.1111/jpm.12129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowers, L. , Alexander, J. , Bilgin, H. , Botha, M. , Dack, C. , James, K. , Jarrett, M. , Jeffery, D. , Nijman, H. , Owiti, J. A. , Papadopoulos, C. , Ross, J. , Wright, S. , & Stewart, D. (2014). Safewards: the empirical basis of the model and a critical appraisal. Journal of Psychiatric and Mental Health Nursing, 21, 354–364. 10.1111/jpm.12085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bowers, L. , James, K. , Quirk, A. , Simpson, A. , Stewart, D. , & Hodsoll, J. (2015). Reducing conflict and containment rates on acute psychiatric wards: The Safewards cluster randomised controlled trial. International Journal of Nursing Studies, 52, 1412–1422. 10.1016/j.ijnurstu.2015.05.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brophy, L. M. , Roper, C. E. , Hamilton, B. E. , Tellez, J. J. , & McSherry, B. M. (2016). Consumers’ and their supporters’ perspectives on barriers and strategies to reducing seclusion and restraint in mental health settings. Australian Health Review, 40, 599–604. 10.1071/AH15128 [DOI] [PubMed] [Google Scholar]
- Cabral, A. , & Carthy, J. (2017). Can Safewards improve patient care and safety in forensic wards? A pilot study. British Journal of Mental Health Nursing, 6(4), 165–171. 10.12968/bjmh.2017.6.4.165 [DOI] [Google Scholar]
- Carton, G. (1998). Nurse education: Scribes and scriptures. In Mason T., & Mercer D. (Eds.), Critical Perspectives in Forensic Care. Palgrave. 10.1007/978-1-349-26104-8_15 [DOI] [Google Scholar]
- Daffern, M. , Howells, K. , & Ogloff, J. (2007). What's the point? Towards a methodology for assessing the function of psychiatric inpatient aggression. Behaviour Research and Therapy, 45(1), 101–111. 10.1016/j.brat.2006.01.011 [DOI] [PubMed] [Google Scholar]
- Daffern, M. , Howells, K. , Ogloff, J. R. P. , & Lee, J. (2005). Individual characteristics predisposing patients to aggression in a forensic psychiatric hospital. Journal of Forensic Psychiatry and Psychology, 16(4), 729–746. 10.1080/14789940500345595 [DOI] [Google Scholar]
- Daffern, M. , & Howells, K. (2002). Psychiatric inpatient aggression: A review of structural and functional assessment approaches. Aggression and violent behavior, 7(5), 477–497. 10.1016/S1359-1789(01)00073-8 [DOI] [Google Scholar]
- Department of Health (2013). Providing a Safe Environment for All: Framework for Reducing Restrictive Interventions. Mental Health Drugs and Regions Division Department of Health Victorian Government. [Google Scholar]
- Efkemann, S. A. , Bernard, J. , Kalagi, J. , Otte, I. , Ueberberg, B. , Assion, H. J. , Zeiß, S. , Nyhuis, P. W. , Vollmann, J. , Juckel, G. , & Gather, J. (2019). Ward atmosphere and patient satisfaction in psychiatric hospitals with different ward settings and door policies. Results from a mixed methods study. Frontiers Psychiatry, 10, 576. 10.3389/fpsyt.2019.00576 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fazel, S. , Hayes, A. J. , Bartellas, K. , Clerici, M. , & Trestman, R. (2016). Mental health of prisoners: prevalence, adverse outcomes, and interventions. The Lancet Psychiatry, 3(9), 871–881. 10.1016/S2215-0366(16)30142-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feo, R. , Conroy, T. , Jangland, E. , Muntlin Athlin, Å. , Brovall, M. , Parr, J. , Blomberg, K. , & Kitson, A. (2018). Towards a standardised definition for fundamental care: A modified Delphi study. Journal of Clinical Nursing, 27(11–12), 2285–2299. 10.1111/jocn.14247 [DOI] [PubMed] [Google Scholar]
- Fletcher, J. , Buchanan‐Hagen, S. , Brophy, L. , Kinner, S. , & Hamilton, B. (2019). Consumer perspectives of Safewards impact in acute inpatient mental health wards in Victoria Australia. Frontiers in Psychiatry, 10, 461. 10.3389/fpsyt.2019.00461 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fletcher, J. , Hamilton, B. , Kinner, S. A. , & Brophy, L. (2019). Safewards impact in inpatient mental health units in Victoria, Australia: Staff perspectives. Frontiers in Psychiatry, 10, 462. 10.3389/fpsyt.2019.00462 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fletcher, J. , Spittal, M. , Brophy, L. , Tibble, H. , Kinner, S. , Elsom, S. , & Hamilton, B. (2017). Outcomes of the Victorian Safewards trial in 13 wards: Impact on seclusion rates and fidelity measurement. International Journal of Mental Health Nursing, 26, 461–471. 10.1111/inm.12380 [DOI] [PubMed] [Google Scholar]
- Gillespie, M. , & Flowers, P. (2009). From the old to the new: Is forensic mental health nursing in transition? Journal of Forensic Nursing, 5(4), 212–219. 10.1111/j.1939-3938.2009.01056.x [DOI] [PubMed] [Google Scholar]
- Hammarström, L. , Häggström, M. , Devik, S. A. , & Hellzen, O. (2019). Controlling emotions‐nurses’ lived experiences caring for patients in forensic psychiatry. International Journal of Qualitative Studies on Health and Well‐Being, 14(1), 1682911. 10.1080/17482631.2019.1682911 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hornik‐Lurie, T. , Shalev, A. , Haknazar, L. , Epstein, P. G. , Ziedenberg‐Rehav, L. , & Moran, G. S. (2018). Implementing recovery‐oriented interventions with staff in a psychiatric hospital: A mixed‐methods study. Journal of Psychiatric and Mental Health Nursing, 25(9–10), 569–581. 10.1111/jpm.12502 [DOI] [PubMed] [Google Scholar]
- Hottinen, A. , Rytila‐Manninen, M. , Lauren, J. , Autio, S. , Laiho, T. , & Lindberg, N. (2020). Impact of the implementation of the safewards model on the social climate on adolescent psychiatric wards. International Journal of Mental Health Nursing, 29, 399–405. 10.1111/inm.12674 [DOI] [PubMed] [Google Scholar]
- Hsu, C. C. , & Sandford, B. A. (2007). The Delphi technique: Making sense of consensus. Practical Assessment Research and Evaluation, 12(10), 1–8. [Google Scholar]
- James, K. , Quirk, A. , Patterson, K. , Brennan, G. , & Stewart, D. (2017). Quality of intervention delivery in a cluster randomised controlled trial: a qualitative observational study with lessons for fidelity. BioMed Central, 18(548), 10.1186/s13063-017-2189-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jansman‐Hart, E. M. , Seto, M. C. , Crocker, A. G. , Nicholls, T. L. , & Côté, G. (2011). International Trends in Demand for Forensic Mental Health Services. International Journal of Forensic Mental Health, 10(4), 326–336. 10.1080/14999013.2011.625591 [DOI] [Google Scholar]
- Jorm, A. F. (2015). Using the Delphi expert consensus method in mental health research. Australian and New Zealand Journal of Psychiatry, 49(10), 887–897. 10.1177/0004867415600891 [DOI] [PubMed] [Google Scholar]
- Keeney, S. , Hasson, F. , & McKenna, H. P. (2001). A critical review of the Delphi technique as a research methodology for nursing. International Journal of Nursing Studies, 38, 195–200. 10.1016/S0020-7489(00)00044-4 [DOI] [PubMed] [Google Scholar]
- Lee, J. , Daffern, M. , Ogloff, J. R. P. , & Martin, T. (2015). Towards a model for understanding the development of post‐traumatic stress and general distress in mental health nurses. International Journal of Mental Health Nursing, 24(1), 49–58. 10.1111/inm.12097 [DOI] [PubMed] [Google Scholar]
- Livingston, J. D. , Nijdam‐Jones, A. , & Brink, B. (2012). A tale of two cultures: Examining patient‐centered care in a forensic mental health hospital. The Journal of Forensic Psychiatry and Psychology, 23(3), 345–360. 10.1080/14789949.2012.668214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maguire, T. , Carroll, A. , McKenna, B. , Dunn, C. , & Daffern, M. (2020). The Model for Understanding Inpatient Aggression: A version for mental health nurses working in prisons. Issues in Mental Health Nursing, 10.1080/01612840.2020.1871134 [DOI] [PubMed] [Google Scholar]
- Maguire, T. , & McKenna, B. (2020). Forensic mental health nursing. In Foster K., Marks P., O'Brien A., & Raeburn T. (Eds.), Mental Health Nursing, 5th ed. (pp. 444–451). Elsevier Australia. [Google Scholar]
- Maguire, T. , Ryan, J. , Fullam, R. , & McKenna, B. (2018). Evaluating the introduction of the Safewards model to a medium to long term forensic mental health ward. Journal of Forensic Nursing, 14(4), 214–222. 10.1097/JFN.0000000000000215 [DOI] [PubMed] [Google Scholar]
- Maguire, T. , Ryan, J. , & McKenna, B. (2020). Benchmarking to reduce restrictive practices in forensic mental health services: a Delphi study. Australasian Psychiatry, 10.1177/1039856220946634 [DOI] [PubMed] [Google Scholar]
- Maguire, T. , Young, R. , & Martin, T. (2012). Seclusion reduction in a forensic mental health setting. Journal of Psychiatric and Mental Health Nursing, 19, 97–106. 10.1111/j.1365-2850.2011.01753.x [DOI] [PubMed] [Google Scholar]
- Martin, T. , Ryan, J. , Bawden, L. , Maguire, T. , Quinn, C. , & Summers, M. (2012). Forensic Mental Health Nursing Standards of Practice 2012. Victorian Institute of Forensic Mental Health. [DOI] [PubMed] [Google Scholar]
- Martin, T. (2010). Psychiatric nurses working with offence paralleling behaviour. In Daffern M., Lawrence J., & Shine J. (Eds.), Offence Paralleling Behaviour (pp. 245–260). West Sussex: John Wiley & Sons LTD. [Google Scholar]
- Martin, T. , & Street, A. F. (2003). Exploring evidence of the therapeutic relationship in forensic psychiatry nursing. Journal of Psychiatric and Mental Health Nursing, 10(5), 543–551. 10.1046/j.1365-2850.2003.00656.x [DOI] [PubMed] [Google Scholar]
- McKenna, H. P. (1994). The Delphi technique: a worthwhile research approach for nursing? Journal of Advanced Nursing, 19, 1221–1225. 10.1111/j.1365-2648.1994.tb01207.x [DOI] [PubMed] [Google Scholar]
- O'Brien, B. C. , Harris, I. B. , Beckman, T. J. , Reed, D. A. , & Cook, D. A. (2014). Standards for reporting qualitative research: a synthesis of recommendations. Academic Medicine, 89(9), 10.1097/ACM.0000000000000388 [DOI] [PubMed] [Google Scholar]
- O'Rourke, M. , Wrigley, C. , & Hammond, S. (2018). Violence within mental health services: how to enhance risk management. Risk Management and Healthcare Policy, 11, 159–167. 10.2147/RMHP.S131834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pelto‐Piri, V. , Warg, L. , & Kjellin, L. (2020). Violence and aggression in psychiatric inpatient care in Sweden: a critical incident technique analysis of staff descriptions. BMC Health Services Research, 20, 362. 10.1186/s12913-020-05239-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Price, O. , Burbery, P. , Leonard, S. , & Doyle, M. (2016). Evaluation of Safewards in forensic mental health: Analysis of a multicomponent intervention intended to reduce levels of conflict and containment in inpatient mental health settings. Mental Health Practice, 19(8), 14–21. 10.7748/mhp.19.8.14.s17 [DOI] [Google Scholar]
- Priebe, S. , Badesconyi, A. , Fioritti, A. , Hansson, L. , Kilian, R. , Torres‐Gonzales, F. , Turner, T. , & Wiersma, D. (2005). Reinstitutionalisation in mental health care: comparison of data on service provision from six European countries. BMJ, 15(330), 123–126. 10.1136/bmj.38296.611215.AE [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shera, W. , & Ramon, S. (2013). Challenges in the implementation of recovery‐oriented mental health policies and services. International Journal of Mental Health, 42(2–3), 17–42. 10.2753/IMH0020-7411420202 [DOI] [Google Scholar]
- Simpson, A. I. F. , & Penney, S. R. (2011). The recovery paradigm in forensic mental health services. Criminal Behaviour and Mental Health, 21, 299–306. 10.1002/cbm.823 [DOI] [PubMed] [Google Scholar]
- Stensgaard, L. , Andersen, M. K. , Nordentoft, M. , & Hjorthøj, C. (2018). Implementation of the safewards model to reduce the use of coercive measures in adult psychiatric inpatient units: An interrupted time‐series analysis. Journal of Psychiatric Research, 105, 147–152. 10.1016/j.jpsychires.2018.08.026 [DOI] [PubMed] [Google Scholar]
- Sturmey, P. , & McMurran, M. (2011). Forensic Case Formulation. Wiley‐Blackwell. [Google Scholar]
- Whitmore, C. (2017). Evaluation of Safewards in forensic mental health: a response. Mental Health Practice, 20(8), 26–29. 10.7748/mhp.2017.e1203 [DOI] [Google Scholar]
- Woods, P. , Collins, M. , & Kettles, A. (2002). Forensic nursing interventions and future directions for forensic mental health practice. In Kettles A., Woods P., & Collins M. (Eds.), Therapeutic Interventions for Forensic Mental Health Nurses (pp. 240–245). Jessica Kingslea Publishers Ltd. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are available on request due to privacy/ethical restrictions. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.