

Abstract
Purpose
Low magnetic field systems provide an important opportunity to expand MRI to new and diverse clinical and research study populations. However, a fundamental limitation of low field strength systems is the reduced SNR compared to 1.5 or 3T, necessitating compromises in spatial resolution and imaging time. Most often, images are acquired with anisotropic voxels with low through‐plane resolution, which provide acceptable image quality with reasonable scan times, but can impair visualization of subtle pathology.
Methods
Here, we describe a super‐resolution approach to reconstruct high‐resolution isotropic T2‐weighted images from a series of low‐resolution anisotropic images acquired in orthogonal orientations. Furthermore, acquiring each image with an incremented TE allows calculations of quantitative T2 images without time penalty.
Results
Our approach is demonstrated via phantom and in vivo human brain imaging, with simultaneous 1.5 × 1.5 × 1.5 mm3 T2‐weighted and quantitative T2 maps acquired using a clinically feasible approach that combines three acquisition that require approximately 4‐min each to collect. Calculated T2 values agree with reference multiple TE measures with intraclass correlation values of 0.96 and 0.85 in phantom and in vivo measures, respectively, in line with previously reported brain T2 values at 150 mT, 1.5T, and 3T.
Conclusion
Our multi‐orientation and multi‐TE approach is a time‐efficient method for high‐resolution T2‐weighted images for anatomical visualization with simultaneous quantitative T2 imaging for increased sensitivity to tissue microstructure and chemical composition.
Keywords: child brain development, low field MRI, magnetic resonance imaging, pediatric neuroimaging
1. INTRODUCTION
Quantitative measurement of the transverse magnetic relaxation time constant (T2) is a valuable tool in both clinical and research MRI imaging applications. Clinically, these uses include visualizing spinal disc degeneration, 1 diagnosis of cardiomyopathy, 2 liver iron quantification, 3 and evaluation of articular cartilage health and degeneration. 4 In the research context, quantitative (q)T2 imaging has been used to investigate white matter maturation and myelination during neurodevelopment, 5 white and gray matter microstructure degeneration associated with aging and cognitive decline (including Alzheimer disease), 6 brain iron changes associated with neurological disorders (e.g., Parkinson disease), 7 and quantifying hypoxic–ischemic injury in neonates 8 among other uses.
Conventionally, qT2 imaging is performed with a multi‐echo fast or turbo spin‐echo (FSE or TSE) approach, with T2 calculated at each voxel or region‐of‐interest from two or more images acquired with different effective echo times, TE, 9 the time at which the central k‐space lines are acquired. Under ideal conditions, i.e., single‐species relaxation and full suppression of stimulated or indirect echoes, T2 can be calculated from two acquired images at different TEs using a linearized fit to the signal equation
| (1) |
Past work has eloquently shown that many tissues, including brain white matter, are more accurately modeled as the summation of multiple T2 species that reflect distinct tissue components (i.e., myelin vs the intra‐ and extra‐cellular water in brain white matter). 10 , 11 In these tissues, the calculated two‐point T2 will depend on the chosen TEs and will be biased toward the faster‐relaxing myelin‐associated water or the slower‐relaxing intra‐ and extra‐cellular water. 12 However, even under these conditions, a single‐component qT2 measurement can still provide useful information on tissue change and damage with high intra‐ and inter‐site reproducibility provided matched acquisition parameters. 13 , 14
Widespread adoption of quantitative imaging has been limited in part by the lengthy acquisition times needed to reliably calculate high‐resolution qT2 maps. This limitation is magnified at lower field strengths (e.g., 50–200 mT) where the SNR of the acquired T2‐weighted images is further reduced. Here, images are often acquired with non‐isotropic voxels with large through‐plane dimensions (e.g., 1.5 mm × 1.5 mm × 5 mm) to reduce imaging time while maintaining acceptable SNR. Lower field strength systems, such as the Hyperfine Swoop (64 mT) and others, offer the potential for a new approach to clinical and research imaging in which the scanner is brought to the patient or participant. 15 Portable neuroimaging could be transformative for clinical studies of neonatal hypoxic–ischemic encephalopathy, in which unstable infants are difficult to transport between the neonatal intensive care and radiology units; or population‐based studies of Alzheimer disease, in which many interested individuals are unable to participate due to challenges with mobility and transportation to an imaging center.
Currently, available product sequences on the Hyperfine system are set to a default spatial resolution of (1.5 mm × 1.5 mm × 5 mm). A research agreement with the manufacturer has allowed us to adjust this base resolution but, unfortunately, higher resolution isotropic images yield lengthy acquisition times (e.g., ∼12–15 min for a single 2 mm × 2 mm × 2 mm T2‐weighted image). Thus, acquisition of even just two differing TEs may be prohibitively long in many clinical settings or in sensitive (infant or elderly populations). The inability to remain motionless for this entire scan and exam will result in likely motion‐related artifact corruption in non‐sedated infants and all but the most exceptionally compliant clinical populations.
One approach that has found considerable success in addressing the challenge of time‐efficient high‐resolution imaging is super‐resolution (SR) reconstruction from multiple lower resolution anisotropic images acquired in three or more rotated orientations (i.e., axial, sagittal, and coronal). 16 , 17 While this does not necessarily reduce total imaging time, each individual acquisition is shorter and potentially more tolerable in motion‐sensitive populations (and each can be repeated independently without requiring the full exam to be restarted).
In conventional SR, each image is acquired with similar acquisition parameters except for orientation. However, varying the TE of each acquisition may further allow qT2 calculation without loss of image quality or increase in imaging time. Such an approach has been previously demonstrated for qT1 imaging. 18
The aim of this work, therefore, was to investigate the feasibility of this simultaneous multi‐TE and multi‐orientation approach for the concurrent collection of high‐resolution isotropic T2‐weighted and qT2 imaging at low field (64 mT) on a Hyperfine Swoop system. We show that reliable isotropic qT2 imaging is possible with a clinically tolerable 12‐min scan time and with quantitative values that agree well with gold‐standard reference measures. While further work is needed to improve overall image quality, these results represent an important advance for low field neuroimaging.
2. METHODS
2.1. Approach
Super‐resolution and related algorithms aim to improve the spatial resolution of an image by combining information from one or more lower‐resolution images. While the initial applications of SR to MRI dates back almost two decades, 19 its use has accelerated over the past 3–5 y with the development of new deep learning techniques (e.g., Refs. [20, 21, 22]) In many of the original MRI implementations, the lower resolution images were acquired with subtle shifts in one or more directions. 23 , 24 , 25 In more recent implementations, often associated with fetal MRI, 16 , 26 , 27 the lower resolution images are acquired from different orientations—often chosen as the three principal axes (axial, sagittal, and coronal). To reconstruct a high‐resolution image, the general approach follows an initial registration of the low‐resolution images to each other in a common registration space to create a template image with the desired spatial resolution with a maximum likelihood approach used to interpolate the high‐resolution image intensities. 24 , 28 Iterative affine and non‐linear transformations are then performed between the source data and the template, with the template improved at each step.
A simplified approximation to SR can be achieved through repeated multi‐resolution registration as implemented in the Advanced Normalization Tools (ANTS) multivariate template construction tool 29 as described in Ref. [30]. Here, the low‐resolution images are aligned using linear and diffeomorphic registration with symmetric normalization. This approach provides not only the combined high‐resolution isotropic image but also the forward and inverse transformations for each low‐resolution image to the combined result (Figure 1).
FIGURE 1.
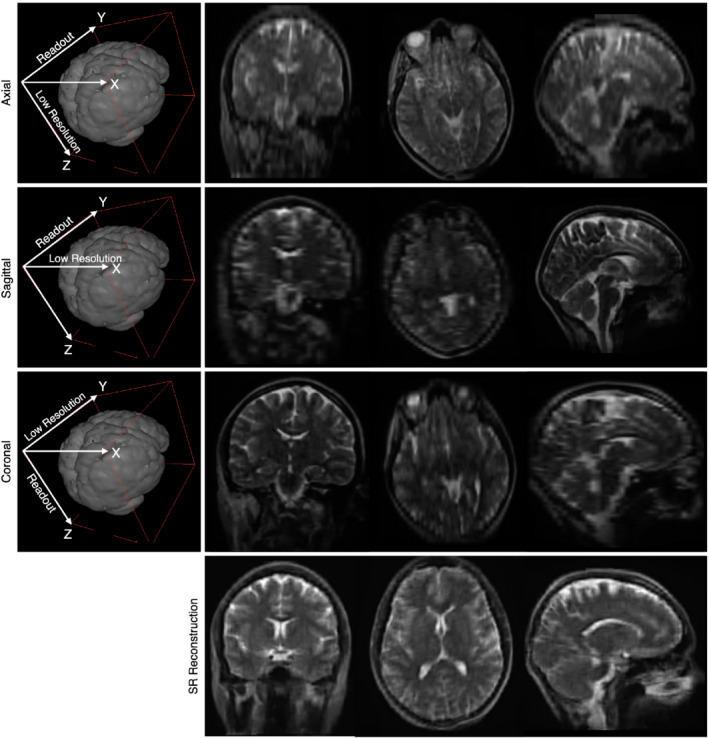
Example illustration of SR image reconstruction using images acquired in the axial, sagittal, and coronal orientations (the frequency encoding/readout and lower resolution directions are labeled) and the final reconstructed image
For our proposed approach, anisotropic T2‐weighted axial, sagittal, and coronal images are acquired with incremented TEs. In‐plane resolution for each image is 1.5 mm × 1.5 mm with a through‐plane resolution of 5 mm (like shown in Figure 1). Using the approach described, these data are first combined into a single (1.5 × 1.5 × 1.5) mm3 T2‐weighted image for anatomical visualization. A conventional non‐linear exponential fit for T2 is then performed using the three registered images in the high‐resolution space to generate the qT2 image.
2.2. Data collection
To validate our approach, a series of phantom and in vivo human imaging data were acquired on a 64 mT Hyperfine Swoop system. All human data were acquired following informed consent as part of an approved study monitored by our institution's ethical review board. Phantom measurements were acquired of the commercially available CaliberMRI phantom that is closely modeled on the NIST “Phannie” phantom 31 and provides a range of T1 and T2 values. In vivo data were acquired of five healthy female adult volunteers with a mean age of 24 ± 3 y.
Three datasets were acquired of the phantom and each volunteer (described in Table 1):
“Gold Standard” Hyperfine multi‐TE T2: single‐orientation FSE approach with five incremented TEs.
-
Single orientation multi‐TE FSE approach with data collected at three incremented TEs of approximately 123, 182, and 242 ms (rounded to the nearest ms).
and
Our proposed multi‐orientation and multi‐TE approach with FSE images acquired with the same three TEs as 2 but acquired in the axial, coronal, and sagittal orientations, respectively.
TABLE 1.
Acquisition parameters for the three sets of data collected phantom and each human volunteer
| Hyperfine multi‐TE T2 | TE #1 | TE #2 | TE #3 | TE #4 | TE #5 |
|---|---|---|---|---|---|
| Axial FOV (X × Y × Z)cm3 | 16.8 × 20.4 × 18.0 | 16.8 × 20.4 × 18.0 | 16.8 × 20.4 × 18.0 | 16.8 × 20.4 × 18.0 | 16.8 × 20.4 × 18.0 |
| Matrix (X × Y × Z) | 112 × 136 × 36 | 112 × 136 × 36 | 112 × 136 × 36 | 112 × 136 × 36 | 112 × 136 × 36 |
| Readout direction | Y (AP) | Y (AP) | Y (AP) | Y (AP) | Y (AP) |
| In‐plane resolution (mm × mm) | 1.5 × 1.5 | 1.5 × 1.5 | 1.5 × 1.5 | 1.5 × 1.5 | 1.5 × 1.5 |
| Slice thickness (mm) | 5 | 5 | 5 | 5 | 5 |
| TR (ms) | 2200 | 2200 | 2200 | 2200 | 2200 |
| TE (ms) | 60 | 100 | 150 | 200 | 300 |
| ETL | 12 | 20 | 30 | 40 | 60 |
| Acquisition time (min) | 13:37 | ||||
| Single‐orientation multi‐TE | TE #1 | TE #2 | TE #3 | ||
| Axial FOV (X × Y × Z) cm3 | 18.0 × 21.9 × 18.0 | 18.0 × 21.9 × 18.0 | 18.0 × 21.9 × 18.0 | ||
| Matrix (X × Y × Z) | 120 × 146 × 36 | 120 × 146 × 36 | 120 × 146 × 36 | ||
| Readout direction | Y (AP) | Y (AP) | Y (AP) | ||
| In‐plane resolution (mm × mm) | 1.5 × 1.5 | 1.5 × 1.5 | 1.5 × 1.5 | ||
| Slice thickness (mm) | 5 | 5 | 5 | ||
| TR (ms) | 2000 | 2000 | 2000 | ||
| TE (ms) | 122.8 | 182.4 | 241.6 | ||
| ETL | 20 | 30 | 40 | ||
| Acquisition time (min) | 5:58 | 4:00 | 3:00 | 12:58 | |
| Multiple‐orientation multi‐TE | TE #1 | TE #2 | TE #3 | ||
| Axial FOV (X × Y × Z) cm3 | 18.0 × 21.9 × 18.0 | ||||
| Sagittal FOV (X × Y × Z) cm3 | 18.0 × 21.9 × 18.0 | ||||
| Coronal FOV (X × Y × Z) cm3 | 18.0 × 18.0 × 20 | ||||
| Matrix (X × Y × Z) | 120 × 146 × 36 | 120 × 146 × 36 | 120 × 120 × 40 | ||
| Readout direction | Y (AP) | Y (AP) | Z (SI) | ||
| In‐plane resolution (mm × mm) | 1.5 × 1.5 | 1.5 × 1.5 | 1.5 × 1.5 | ||
| Slice thickness (mm) | 5 | 5 | 5 | ||
| TR (ms) | 2000 | 2000 | 2000 | ||
| TE (ms) | 122.8 | 182.4 | 241.6 | ||
| ETL | 20 | 30 | 40 | ||
| Acquisition time (min) | 4:11 | 4:00 | 3:30 | 11:41 | |
In all cases, the T2 data were collected using a fully 3D sequence with a Cartesian k‐space trajectory. The built in image reconstruction pipeline was used that includes gradient non‐linearity correction and noise compensation using external magnetic field monitors. For the Hyperfine multi‐TE approach (#1), the data are acquired sequentially with the qT2 map calculated using an exponential fit. For approaches #2 and #3 in which each TE image was acquired and reconstructed independently and then the qT2 map calculated, the deep learning reconstruction approach (similar to that described in Ref. [32]) was turned off in favor of a conjugate gradient least square method (e.g., Ref. [33]) to avoid unknown scaling and manipulation of the signal values between the different TE acquisitions. To vary the TEs, the echo train length (ETL) was changed from 20 for the shortest TE, 30 for mid‐length TE, and 40 for the longest TE. Given the low field strength and low risk of high energy deposition (specific absorption rate, SAR), the excitation and refocusing pulses were 90 and 180 degrees, respectively.
Image orientations for the short, mid, and long TE acquisitions were chosen to minimize overall acquisition time, yielding a total scan time of just under 12 min.
2.3. Data analysis and comparison
For the Hyperfine multi‐TE approach, the qT2 maps were automatically calculated using on‐scanner software that consisted of an initial linearized least squares estimation to provide an initial estimate of the model parameters, and then a single exponential fit to the data (assuming Equation (1)).
For the single orientation multi‐TE approach, linear image alignment was first performed to account for any subject movement between images followed by T2 calculations at each imaging voxel using a similar approach of an initial linearized least squares estimation with a non‐linear fit to the exponential model using a Nelder–Mead Simplex method with 100 sequential iterations. For the multiple orientation multi‐TE approach, SR reconstruction was first used to calculate the isotropic spatial resolution images, and then T2 values were estimated using linearized least squares and non‐linear exponential fit using a Nelder–Mead Simplex. Example analysis code for these steps is provided as supporting Information Appendix S1.
Given the low SNR of the acquired images, we sought to evaluate the use of anisotropic noise filtering 34 to improve map quality. For the multiple‐orientation multi‐TE approach we applied the spatially adaptive denoising approach of Manjon et al. 35 to the aligned high spatial resolution multi‐TE source images after SR reconstruction but prior to T2 calculation and then followed the same steps as above to calculate the qT2 image.
Following calculation of the qT2 images from each of the three datasets, mean measures were obtained from 10 phantom elements and six in vivo brain regions: right and left anterior internal capsule white matter, right and left posterior white matter, cerebellar white matter, and body of the corpus callosum. In vivo region masks were first manually drawn on the MNI template, which was then non‐linearly aligned to each participant's T2‐weighted image and superimposed onto their corresponding qT2 image. Agreement between the measures obtained with the different approaches was then assessed via the intra‐class correlation, ICC.
3. RESULTS
Figure 2 provides an overview of collected data, processing workflow, and calculated qT2 images using each of the acquisition approaches for one of the healthy volunteers. No significant B0‐field related distortion effects are noted between the multi‐orientation images, except in the posterior of the sagittal image, which appears to be handled during the non‐linear reconstruction process. A visual comparison of in vivo T2 values derived from the noise‐filtered multi‐orientation + multi‐TE data are provided in Figure 3, with the values calculated using the Hyperfine five‐TE approach assumed as reference values. Overall, we note strong alignment between the multi‐orientation + multi‐TE and reference T2 values, with an ICC of 0.93. For comparison, the ICC between the non‐noise filtered multi‐orientation + multi‐TE and reference T2 values is 0.85.
FIGURE 2.
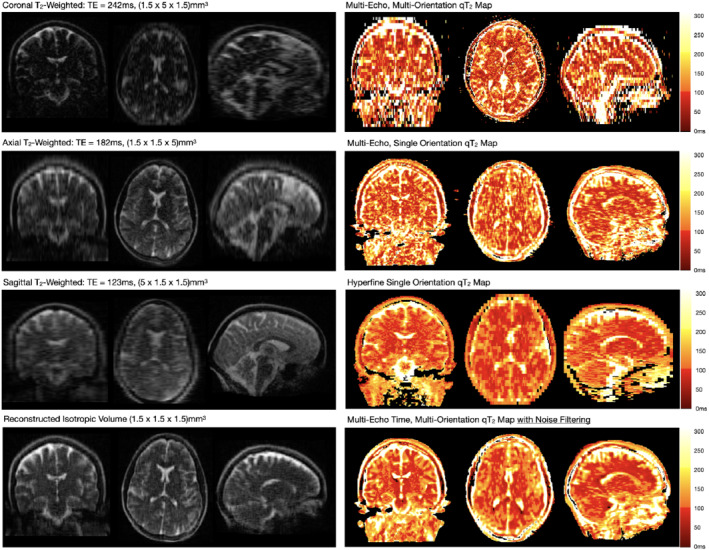
Analysis workflow from the acquisition of the source anisotropic T2‐weighted data with coronal, axial, and sagittal orientations (left panel); SR reconstruction of an isotropic T2‐weighted image from the acquired data (bottom, left panel); and calculation of qT2 maps from the aligned and resampled multi‐orientation data (top, right panel). For comparison, qT2 maps calculated from multiple TEs acquired in a single orientation and using Hyperfine‐provided five‐TE approach (middle, right panel) are also shown. As well, we show a multi‐orientation + multi‐TI qT2 calculated from data that was preprocessed using adaptive denoising (bottom, right panel)
FIGURE 3.
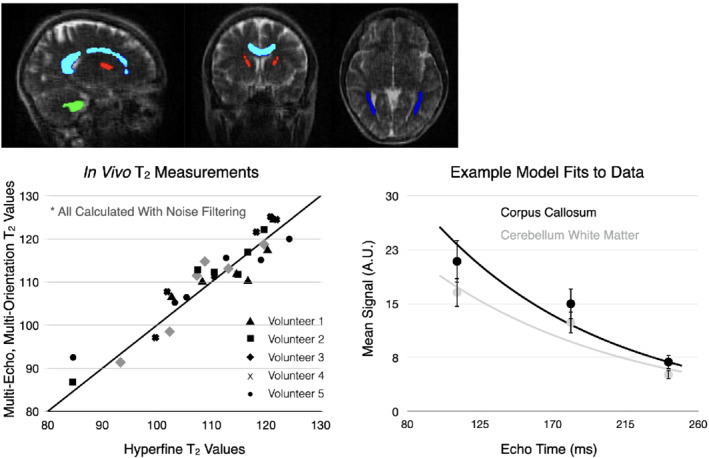
Comparison of qT2 values from four brain regions of interest (top) in each healthy volunteer. Brain regions included cerebellar white matter (green), corpus callosum (light blue), anterior internal capsule (red), and posterior thalamic radiations (dark blue). The ICC between the noise filtered multi‐orientation + multi‐TE and reference Hyperfine 5‐TE qT2 values was 0.93. Example monoexponential fits to the corpus callosum and cerebellar white matter data from one of the healthy volunteers is also shown
Examining the Hyperfine and non‐noise filtered images (Figure 2) we note the multi‐orientation + multi‐TE images suffer from significantly reduced SNR, likely owing to the reduced acquisition time (13:37 vs 11:41) and smaller voxel volume (11.25 mm3 vs 3.38 mm3) of the multi‐orientation + multi‐TE data. Based on conventional associations, these differences should translate to an SNR reduction of approx. 400%, which agrees well with the measured difference in white matter T2‐to‐noise ratio of 9.4 in the reference map and 3.2 in the multi‐orientation + multi‐TE map. However, making use of spatially adaptive denoising substantially improves the visual appearance of the qT2 maps, despite subtle loss of image detail.
Building on the in vivo results in Figures 2 and 3, Figure 4 displays a comparison of the Hyperfine five‐TE and noise‐filtered multi‐orientation + multi‐TE qT2 maps and mean phantom element T2 values. As with the in vivo data, we find agreement between the values, with an ICC of 0.96.
FIGURE 4.
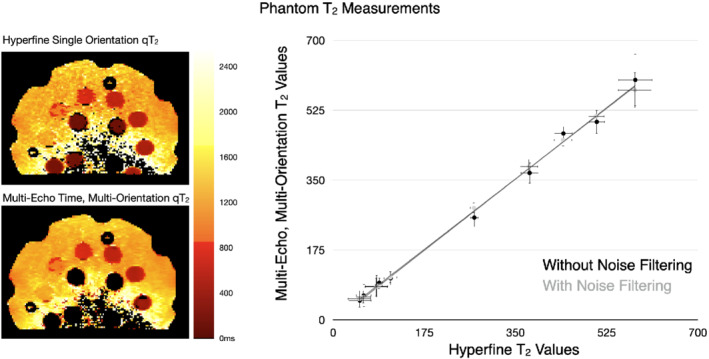
(Left) Comparison of qT2 images through the multi‐element phantom and (Right) Mean phantom multi‐orientation + multi‐TE and reference Hyperfine 5‐TE qT2 values. The solid line corresponds to the line of unity, and errors bars in the phantom measurements denote 1 SD. ICC values for the phantom data were 0.97 (with denoising) and 0.96 (without denoising)
From the in vivo data, mean T2 values for the different regions of interest were: cerebellar white matter, 110 ± 19 ms; corpus callosum, 112 ± 7 ms; left frontal white matter, 114 ± 3.5 ms; right frontal white matter, 118 ± 6 ms; left posterior white matter, 98 ± 7 ms; and right posterior white matter, 102 ± 9 ms. These measures are in general agreement with those previously reported at 1.5 and 3 T (ranging from 60 to 130 ms), 36 as well as with prior measurements at lower field strengths (80–130 ms at 50–150 mT). 37 , 38 The relative invariance of in vivo T2 measures with field strength is theoretically predicted. 39
4. DISCUSSION
In past work, our group investigated the use of portable low field MRI for pediatric neuroimaging, 40 demonstrating the ability to reliably image and quantify total and regional brain volumes. That analysis, however, used the conventional raw anisotropic T2‐weighted images provided by the Hyperfine system, and volumes were over‐estimated relative to higher field strength isotropic images. The approach proposed here offers important advantages over this earlier work. Specifically, the reconstruction of isotropic resolution images may help address this estimation bias and improve overall comparisons with high field strength data. Recently, a joint SR and image synthesis approach has been proposed to allow reconstruction of high‐resolution 1 mm isotropic images from anisotropic and low‐resolution data, such as that acquired with Hyperfine. 41 We speculate that improved image synthesis will be possible from the higher resolution low field images provided through our approach. Of note, the open‐source SynthMR package makes use of low field T1 and T2 images to reconstruct the synthetic high‐resolution T1 weighted image using the predict_command_line_hyperfine.py module. The acquisition time for these is approximately 11‐min—approximately the same as for our approach.
One of the principal limitations of our approach is the relatively low SNR of the calculated T2 map. For clinical studies, this may translate to a need for larger samples sizes to identify subtle differences in neurodevelopment, accelerated degeneration, increased iron accumulation, or other examples. Improvements to the qT2 map quality may be possible by down‐sampling the raw data used for the qT2 map calculation, although at the obvious cost of resolution. Our use of noise filtering and reduction, however, also provides a significant improvement in image quality without degrading T2 measurement accuracy. Additional alternatives, image synthesis and deep‐learning may also offer methods to not only improve the single‐component qT2 images presented here but also model multi‐component relaxometry and myelin water imaging. 42
A second limitation of our approach is the relatively long TEs used relative to the TRs of the tissue we are measuring. Ideally, we would aim to sample the decay curve more completely, including shorter TEs. 43 Unfortunately, we are relatively limited in terms of available sequence modifications on the Hyperfine system and balancing the range of TEs with acquisition time yielded the values used here (approximately 123, 182, and 242 ms). While the mean fits to the data (examples shown in Figure 3) appear valid, it is hoped that greater access to pulse sequence design will allow greater flexibility in chosen TEs, further improving the qT2 accuracy and image quality.
Greater sequence design access may also allow for additional subtle control of FOV positioning, which is currently performed automatically. By varying not only orientation, as done here, but also adding sub‐voxel shifts along the other image dimensions may further improve the SR reconstruction, allowing further reduction of voxel dimensions below the (1.5 × 1.5 × 1.5) mm3 achieved here. 19
While our presented results are preliminary and are demonstrated in adult subjects only, they illustrate the potential of low field imaging as a viable complement to high field systems. Furthermore, they offer the potential for imaging studies of neurodevelopment or neurodegeneration in many low‐ and middle‐income settings where disease, malnutrition, psychosocial adversities, and other environmental exposures may profoundly affect brain structure and function, but where access to MRI is significantly limited.
5. CONCLUSIONS
It is increasingly clear that portable low field imaging offers a new paradigm in neuroimaging. Not only allowing increased access to clinical and research populations in the “global north,” but affording the opportunity for accessible imaging in low‐ and middle‐income settings. At present, however, commercial low field strength devices are limited in the range of available image contrasts and acquisition methods. Here, we have taken an initial step toward acquiring higher resolution T2‐weighted imaging for anatomical visualization with simultaneous qT2 imaging for increased sensitivity to tissue microstructure and chemical composition, all performed within a clinically manageable 12 min. It is envisaged that, as low field devices become more commonplace, and imaging data are shared across the research community, improvements to the described technique will allow for increased performance, lower noise, and more rapid acquisition—further enhancing the diagnostic capability of these devices.
CONFLICT OF INTEREST
The authors report no significant financial conflicts of interest with respect to the subject matter of this manuscript.
Supporting information
Appendix S1.
Deoni SCL, O'Muircheartaigh J, Ljungberg E, Huentelman M, Williams SCR. Simultaneous high‐resolution T2‐weighted imaging and quantitative T 2 mapping at low magnetic field strengths using a multiple TE and multi‐orientation acquisition approach. Magn Reson Med. 2022;88(3):1273‐1281. doi: 10.1002/mrm.29273
Funding information Environmental Influences on Child Health Outcomes (ECHO) National Institutes of Health (SCD UG3OD023313). National Institutes of Health (SCD R34‐DA050284). Bill and Melinda Gates Foundation (INV‐005774 and INV‐005798). JOM is supported by a Sir Henry Dale Fellowship jointly funded by the Wellcome Trust and the Royal Society (Grant Number 206675/Z/17/Z). SW and JOM are supported in part by the Medical Research Council Centre for Neurodevelopmental Disorders, King's College London (MR/N026063/1), and SCRW by Wellcome Trust/EPSRC Centre for Medical Engineering and the National Institute for Health Research (NIHR) Maudsley Biomedical Research Centre (BRC).
REFERENCES
- 1. Pachowsky ML, Kleyer A, Wegener L, et al. Quantitative T2 mapping shows increased degeneration in adjacent intervertebral discs following Kyphoplasty. Cartilage. 2020;11:152‐159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Thavendiranathan P, Walls M, Giri S, et al. Improved detection of myocardial involvement in acute inflammatory cardiomyopathies using T2 mapping. Circ Cardiovasc Imaging. 2012;5:102‐110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. St Pierre TG, El‐Beshlawy A, Elalfy M, et al. Multicenter validation of spin‐density projection‐assisted R2‐MRI for the noninvasive measurement of liver iron concentration. Magn Reson Med. 2014;71:2215‐2223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Renner N, Kleyer A, Kronke G, et al. T2 mapping as a new method for quantitative assessment of cartilage damage in rheumatoid arthritis. J Rheumatol. 2020;47:820‐825. [DOI] [PubMed] [Google Scholar]
- 5. Deoni SC, Dean DC 3rd, O'Muircheartaigh J, Dirks H, Jerskey BA. Investigating white matter development in infancy and early childhood using myelin water faction and relaxation time mapping. Neuroimage. 2012;63:1038‐1053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Knight MJ, Wearn A, Coulthard E, Kauppinen RA. T2 Relaxometry and diffusion tensor indices of the hippocampus and entorhinal cortex improve sensitivity and specificity of MRI to detect amnestic mild cognitive impairment and Alzheimer's disease dementia. J Magn Reson Imaging. 2019;49:445‐455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Bartzokis G, Cummings JL, Markham CH, et al. MRI evaluation of brain iron in earlier‐ and later‐onset Parkinson's disease and normal subjects. Magn Reson Imaging. 1999;17:213‐222. [DOI] [PubMed] [Google Scholar]
- 8. Bano S, Chaudhary V, Garga UC. Neonatal hypoxic‐ischemic encephalopathy: a radiological review. J Pediatr Neurosci. 2017;12:1‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Bauer CM, Jara H, Killiany R. Alzheimer's disease neuroimaging I. whole brain quantitative T2 MRI across multiple scanners with dual echo FSE: applications to AD, MCI, and normal aging. Neuroimage. 2010;52:508‐514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Laule C, Leung E, Lis DK, et al. Myelin water imaging in multiple sclerosis: quantitative correlations with histopathology. Mult Scler. 2006;12:747‐753. [DOI] [PubMed] [Google Scholar]
- 11. Mac Kay AL, Laule C. Magnetic resonance of myelin water: an in vivo marker for myelin. Brain Plast. 2016;2:71‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Milford D, Rosbach N, Bendszus M, Heiland S. Mono‐exponential fitting in T2‐Relaxometry: relevance of offset and first Echo. PLoS One. 2015;10:e0145255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Deoni SCL, Williams SCR, Jezzard P, Suckling J, Murphy DGM, Jones DK. Standardized structural magnetic resonance imaging in multicentre studies using quantitative T1 and T2 imaging at 1.5 T. Neuroimage. 2008;40:662‐671. [DOI] [PubMed] [Google Scholar]
- 14. Chhetri G, McPhee KC, Wilman AH. Alzheimer's disease neuroimaging I. Bloch modelling enables robust T2 mapping using retrospective proton density and T2‐weighted images from different vendors and sites. Neuroimage. 2021;237:118116. [DOI] [PubMed] [Google Scholar]
- 15. Sarracanie M, Salameh N. Low‐Field MRI: How low can we go? A fresh view on an old debate. Frontiers in Phys Ther 2020;8. doi:10.3389/fphy.2020.00172 [Google Scholar]
- 16. Sui Y, Afacan O, Gholipour A, Warfield SK. Fast and high‐resolution neonatal brain MRI through super‐resolution reconstruction from acquisitions with variable slice selection direction. Front Neurosci. 2021;15:636268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Askin Incebacak NC, Sui Y, Gui Levy L, et al. Super‐resolution reconstruction of T2‐weighted thick‐slice neonatal brain MRI scans. J Neuroimaging. 2022;32:68‐79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Van Steenkiste G, Poot DHJ, Jeurissen B, et al. Super‐resolution T1 estimation: quantitative high resolution T1 mapping from a set of low resolution T1‐weighted images with different slice orientations. Magn Reson Med. 2017;77:1818‐1830. [DOI] [PubMed] [Google Scholar]
- 19. Greenspan H, Oz G, Kiryati N, Peled S. MRI inter‐slice reconstruction using super‐resolution. Magn Reson Imaging. 2002;20:437‐446. [DOI] [PubMed] [Google Scholar]
- 20. Li Z, Yu J, Wang Y, Zhou H, Yang H, Qiao Z. Deep volume: brain structure and spatial connection‐aware network for brain MRI super‐resolution. IEEE Trans Cybern. 2021;51:3441‐3454. [DOI] [PubMed] [Google Scholar]
- 21. Zhao C, Dewey BE, Pham DL, Calabresi PA, Reich DS, Prince JL. SMORE: a self‐supervised anti‐aliasing and super‐resolution algorithm for MRI using deep learning. IEEE Trans Med Imaging. 2021;40:805‐817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Sui Y, Afacan O, Jaimes C, Gholipour A, Warfield SK. Scan‐specific generative neural network for MRI super‐resolution reconstruction. IEEE Trans Med Imaging. 2022. doi: 10.1109/TMI.2022.3142610 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Farsiu S, Robinson MD, Elad M, Milanfar P. Fast and robust multiframe super resolution. IEEE Trans Image Process. 2004;13:1327‐1344. [DOI] [PubMed] [Google Scholar]
- 24. Poot DH, Van Meir V, Sijbers J. General and efficient super‐resolution method for multi‐slice MRI. Med Image Comput Comput Assist Interv. 2010;13:615‐622. [DOI] [PubMed] [Google Scholar]
- 25. Plenge E, Poot DH, Bernsen M, et al. Super‐resolution methods in MRI: can they improve the trade‐off between resolution, signal‐to‐noise ratio, and acquisition time? Magn Reson Med. 2012;68:1983‐1993. [DOI] [PubMed] [Google Scholar]
- 26. Gholipour A, Estroff JA, Warfield SK. Robust super‐resolution volume reconstruction from slice acquisitions: application to fetal brain MRI. IEEE Trans Med Imaging. 2010;29:1739‐1758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Song L, Wang Q, Liu T, et al. Deep robust residual network for super‐resolution of 2D fetal brain MRI. Sci Rep. 2022;12:406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Shilling RZ, Robbie TQ, Bailloeul T, Mewes K, Mersereau RM, Brummer ME. A super‐resolution framework for 3‐D high‐resolution and high‐contrast imaging using 2‐D multislice MRI. IEEE Trans Med Imaging. 2009;28:633‐644. [DOI] [PubMed] [Google Scholar]
- 29. Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. 2011;54:2033‐2044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Niaz MR, Ridwan AR, Wu Y, Alzheimer's Disease Neuroimaging I , Bennett DA, Arfanakis K. Development and evaluation of a high resolution 0.5mm isotropic T1‐weighted template of the older adult brain. Neuroimage. 2022;248:118869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Jiang Y, Ma D, Keenan KE, Stupic KF, Gulani V, Griswold MA. Repeatability of magnetic resonance fingerprinting T1 and T2 estimates assessed using the ISMRM/NIST MRI system phantom. Magn Reson Med. 2017;78:1452‐1457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Koonjoo N, Zhu B, Bagnall GC, Bhutto D, Rosen MS. Boosting the signal‐to‐noise of low‐field MRI with deep learning image reconstruction. Sci Rep. 2021;11:8248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. de Leeuw ML, den Bouter MBG, Remis RF. Conjugate gradient variants for ℓ?‐regularized image reconstruction in low‐field MRI. SN Appl Sci. 2019;1:1736. [Google Scholar]
- 34. Senra Filho AC, Barbosa JH, Salmon CE, Murta LO. Anisotropic anomalous diffusion filtering applied to relaxation time estimation in magnetic resonance imaging. Annu Int Conf IEEE Eng Med Biol Soc. 2014;2014:3893. [DOI] [PubMed] [Google Scholar]
- 35. Manjon JV, Coupe P, Marti‐Bonmati L, Collins DL, Robles M. Adaptive non‐local means denoising of MR images with spatially varying noise levels. J Magn Reson Imaging. 2010;31:192‐203. [DOI] [PubMed] [Google Scholar]
- 36. Wansapura JP, Holland SK, Dunn RS, Ball WS Jr. NMR relaxation times in the human brain at 3.0 tesla. J Magn Reson Imaging. 1999;9:531‐538. [DOI] [PubMed] [Google Scholar]
- 37. Bottomley PA, Foster TH, Argersinger RE, Pfeifer LM. A review of normal tissue hydrogen NMR relaxation times and relaxation mechanisms from 1‐100 MHz: dependence on tissue type, NMR frequency, temperature, species, excision, and age. Med Phys. 1984;11:425‐448. [DOI] [PubMed] [Google Scholar]
- 38. O'Reilly T, Webb AG. In vivo T1 and T2 relaxation time maps of brain tissue, skeletal muscle, and lipid measured in healthy volunteers at 50 mT. Magn Reson Med. 2022;87:884‐895. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Bloembergen N, Purcell EM, Pound RV. Nuclear magnetic relaxation. Nature. 1947;160:475‐476. [DOI] [PubMed] [Google Scholar]
- 40. Deoni SCL, Bruchhage MMK, Beauchemin J, et al. Accessible pediatric neuroimaging using a low field strength MRI scanner. Neuroimage. 2021;238:118273. [DOI] [PubMed] [Google Scholar]
- 41. Iglesias JE, Billot B, Balbastre Y, et al. Joint super‐resolution and synthesis of 1 mm isotropic MP‐RAGE volumes from clinical MRI exams with scans of different orientation, resolution and contrast. Neuroimage. 2021;237:118206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Yu T, Canales‐Rodriguez EJ, Pizzolato M, et al. Model‐informed machine learning for multi‐component T2 relaxometry. Med Image Anal. 2021;69:101940. [DOI] [PubMed] [Google Scholar]
- 43. Shrager RI, Weiss GH, Spencer RG. Optimal time spacings for T2 measurements: monoexponential and biexponential systems. NMR Biomed. 1998;11:297‐305. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1.