

Abstract
Introduction:
Different techniques have been developed over the years for achieving mandibular nerve anesthesia. Many methods have been proposed back and forth in order to perform effective anaesthesia.
Aims and Objective:
The main aim of our study was to carry out comparison of clinical efficacy of mandibular nerve anaesthesia by Kurt Thoma technique with that of Vazirani-Akinosi nerve block technique.
Materials and Methods:
10 adult patients requiring bilateral mandibular teeth extraction were selected randomly to receive Kurt Thoma technique and Vazirani-Akinosi technique for nerve block randomly.
Results:
There is no statistically difference between two techniques in terms of need of additional injection, pain, complications, onset of action.
Conclusions:
By this study we conclude that both the techniques are equally effective and all the oral and maxillofacial surgeons should learn these techniques so that they can use in various patients where conventional mandibular nerve block techniques are not feasible.
Keywords: Closed mouth mandibular nerve block, conventional mandibular nerve block, Kurt-Thoma technique, mandibular anesthesia, Vazirani-Akinosi technique
INTRODUCTION
Achieving excellence in pain control is an intrinsic, yet challenging, goal of dentistry. Oral and Maxillofacial surgery largely depends on local anesthesia for painless day-to-day practice and different techniques are available to achieve the same.[1] The most commonly used techniques are infiltration and blocks such as Inferior Alveolar Nerve Block (IANB), Posterior Superior Alveolar (PSA), infraorbital and greater palatine nerve.
Classical IANB is the most commonly administered nerve block technique to achieve mandibular anesthesia both in children and in adults undergoing exodontia, endodontic procedures, minor oral surgical procedures, etc.[2]
IANB is the most widely practiced mandibular local anesthesia (LA) nerve block in dentistry. “Halstead or Standard technique,” “Vazi-rani-Akinosi or Closed Mouth Technique” and “Gow-Gates or Open Mouth Technique” are the various techniques for achieving IANB. Infiltration and blocks such as IANB, PSA, infraorbital, and greater palatine nerve are the most widely used techniques.[3]
A procedure for blocking the inferior alveolar nerve (IAN) using cocaine as the local anesthetic was identified by Dr. William Stewart Halstead on December 6, 1884, and since then, it has been the most frequently used method for blocking the IAN. However, this technique's performance rate is significantly smaller than that of most other nerve blocks.[3]
The classical technique relies on the presence of certain anatomical landmarks. Anatomical variability and accessory innervations are, often the biggest challenge, in successfully providing mandibular anesthesia, thereby contributing to the reported failure rates of up to 20%–25%[4] of Classical IANBs. The value of the alternative mandibular nerve block techniques is their ability to address these reasons for IANB failure and situations where classical techniques are not feasible.
Modification of the classical IANB has decreased the failure rate and drastically enhanced the success rates of 95% with IANB. These include modifications by Thangavelu et al., Boonsiriseth et al., Suazo Galdames et al., Nooh and Abdullah, and Takasugi et al.
Several alternative approaches to the technique of IAN bock have been identified in the literature, both of which seek to achieve a high rate of effectiveness, reduce the likelihood of intravascular injections and eventually, prevent nerve injury.
The alternate procedure identified by Thangavelu et al., in 2012.[5] The needle is inserted 6–8 mm above an imaginary midpoint between the upper and lower occlusal planes and 8–10 mm behind the anterior boundary of the ramus with the patient's mouth completely extended, while the syringe barrel is between the canine and premolar. The needle is relocated to the bone and then the barrel is shifted to the midline, keeping the needle very close to the ramus's medial surface. During penetration, the creator of this procedure recommends several touches on the bone of the medial surface of the ramus. The suggested depth for penetration ranges from 21 to 24 mm. By switching the barrel once more, on the opposite side, the needle position is changed closer to the mandibular foramen. During the use of this procedure, the studies observed no problems and no positive expectations, and claim a 95% success rate
The Thangavelu et al., in 2012 procedure using the internal oblique ridge.[6] The use of the internal oblique ridge was also stated by Thangavelu et al. as the only landmark for another alternative approach to the technique of the lower alveolar nerve block. The thumb is positioned over the retromolar region in this technique and its edge shows the location of the internal oblique ridge. The needle penetration point would then be 6–8 mm higher than the thumb midpoint and 2 mm higher than the inner oblique ridge. The syringe barrel is located on the opposite side of the lower premolar teeth in the region of the lower premolar teeth on the opposite side of the syringe. The penetration depth is 15–20 mm, and the bone is reached at that point. During the treatment, the lingual nerve is anesthetized, and it is confirmed that the success rate is 95%
The innovative Boonsiriseth et al. procedure, 2012[7] This technique uses a long 30 mm needle whose insertion point is the same as that used in the traditional process, but the syringe barrel is positioned on the same side of the injection at the occlusal surface of the teeth. A rubber stop on the needle limits the penetration depth. The needle has no bony interaction with the ramus and the procedure is primarily based on the point and depth of penetration. The benefits of this approach include a reduction in pain and the possibility of nerve traumatization. The authors of this technique say that it reduces the risk of systemic complications, although in some cases there were optimistic aspirations (5%), a fact which means that the use of this technique does not rule out the incidence of systemic complications
Palti et al., 2011s latest approach to IANB[8] This procedure seeks to recognize several easy-to-find landmarks for the site of the mandibular foramen and requires the identification of the mesiobuccal groove and the middle point of the distolingual cusp of the main second molar or first molar permanent mesial slope. In this procedure, two wires are used, one passing through the mesiobuccal groove and the midpoint of the mesial slope on one side of the mandible, while the other is passing through the occlusal plane on the opposite side; the direction of the mandibular foramen is indicated by the junction of the two wires. This technique needs further clinical studies to confirm its effectiveness
Suazo Galdames et al., IANB through the retromolar triangle[9] This procedure involves the deposition at the retromolar triangle of a local anesthetic solution, a triangular region near the distal side of the lower third molar, created by a fork in the temporal crest situated on the inner surface of the mandibular ramus and the distal surface of the mandibular ramus. A variable number of holes of differing sizes perforate the bone in this area, allowing the passage of the buccal artery that anastomoses with the inferior alveolar arteries in the mandibular canal. Through this connection with the retromolar triangle and the mandibular canal, local anesthetic solution deposition in this region will enter the IAN. With an onset time of 10 min, the success rate of this approach was stated to be 72%. In patients with blood diseases where the use of the traditional IANB can present complications, this procedure is stated to be useful
Modified indirect technique by Nooh and Abdullah[10] This technique is a modified variant of the indirect technique by Malamed. The needle is placed 1.5 cm above the occlusal plane with a syringe barrel located at the opposite location of the premolar region in this technique. The syringe is then moved to the same side of the injection after contacting the bone, and the needle then moves when it is in contact with the bone at a distance of 30–34 mm. The authors claimed that this approach has a lower failure rate (1%), lower positive aspiration, and lower complication occurrence
Injection into the domain of a pterygomandibular. Takasugi et al. technique[11] This technique is based on the presence of a space between the medial pterygoid muscle and the deep temporal muscle tendon near the anterior boundary of the mandible ramus. The procedure is often referred to as the technique of the anterior IANB. The needle is inserted at a point on the lateral side of the pterygomandibular raphe, about 10 mm above the occlusal plane, in this procedure. The syringe barrel is located on the opposite side of the first mandibular molar. The position of the barrel is based on the mean angles of the computed tomography (CT) images expected. The position of the barrel is based on the mean angles of the CT images expected. Just 10 mm is the diameter of needle penetration. The advantages of this procedure include a decline in the risk of nerve damage or intravascular injection; however, the success rate is estimated to be only 75% and the time of onset varies from 4 to 9 min. Radiographic research by Okamoto et al. on the anterior technique diffusion of local anesthetic showed that the local anesthetic solution spread rapidly throughout the pterygomandibular area and even entered the IAN, a zone lacking large arteries or nerves, from the site anterior to the mandibular foramen[12,13]
Other alternative techniques: Other available techniques target the branches of the mandibular nerve rather than just the lower alveolar nerve; these include methods mentioned by Gow-Gates, the closed mouth of Vazirani/Akinosi, and the three-stage technique of Fischer;[5,6] all three techniques involve a highly skilled operator and are rarely used in Saudi Arabia by dentists, but may be a common procedure in other countries.
Alternative techniques have been introduced and adopted for circumventing most of the problems encountered with the classical IANB; particularly, the requirement of adequate mouth opening; which is not feasible in all cases such as oral submucous fibrosis, trismus, or Temporomandibular Joint ankylosis or swelling. They include the Gow-Gates technique introduced in 1973 and the Akinosi technique introduced in 1977, and also extraoral approach by Kurt Thoma. Gow-gates technique cannot be administered in patients with trismus, as the technique requires a wide opening of the mouth by the patient during admission. In patients with trismus, The Akinosi mandibular block technique, a closed-mouth intraoral approach, and extraoral mandibular nerve block techniques are often indicated.
Aims and objectives
The aim of the present study was to evaluate the efficacy and applicability of the VA nerve block technique in comparison with Kurt-Thoma technique for IANB technique.
MATERIALS AND METHODS
After receiving necessary approvals from the institutional ethics committee, the study began on patients requiring extraction of mandibular teeth and satisfying the inclusion criteria. Ten patients were selected from among the patients who reported to the Department of Oral and Maxillofacial Surgery, K. M. Shah Dental College and Hospital, Vadodara, who required bilateral extraction of mandibular teeth in a split-mouth study design.
Inclusion criteria
Any age group
Participants of both the gender
Patients requiring extraction of bilateral mandibular teeth.
Exclusion criteria
Patients with active infections or swelling or abscess
Patients with systemic diseases in whom the administration of LA and minor oral surgery is contraindicated
Patients who failed to give consent.
Methodology
All cases were operated by the author and extraction was performed under aseptic conditions. All the patients are done by a single operator in both groups and with the same local anesthetic solution (Lignocaine 2% w/v with Adrenaline 0.001% w/v).
Ethical review approval number
Approval No.: SVIEC/ON/DENT/SRP/15041 Completion No.: SVIEC/ON/DENT/SRP/15082.
Vazirani Akinosi technique[14]
The patient's teeth are closed into occlusion, and the cheek is retracted to expose the posterior teeth. The needle is positioned at the level of and parallel to the mucogingival line of the maxillary molars. The needle is inserted as closely as possible to the medial surface of the ramus and is advanced to a depth of 2.5–3.0 cm into the area between the maxillary tuberosity and the mandibular ramus. After negative aspiration, the contents of standard dental anesthetic solutions are deposited [Figures 1 and 2].[10]
Figure 1.

Demonstration on the human dried skull for the area of insertion and needle position for Vazirani-Akinosi Technique. (a) frontal view, (b) lateral view
Figure 2.
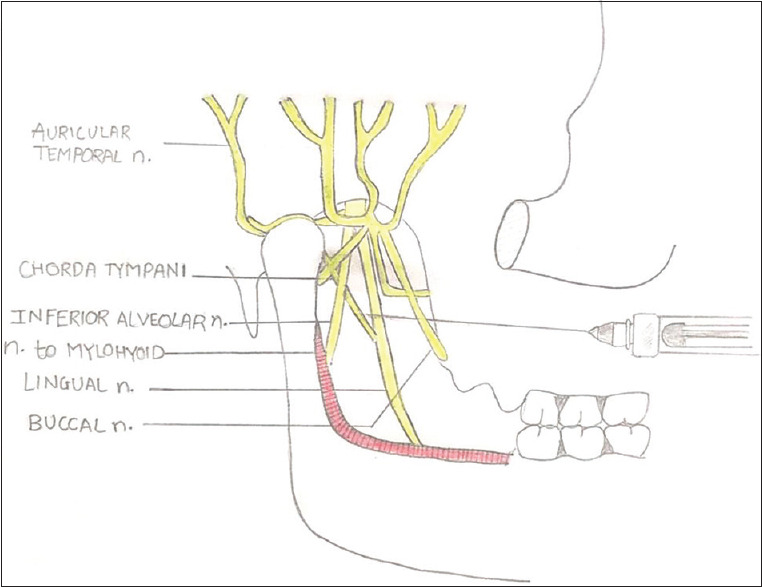
A schematic diagram showing the relationship of the main branches of the mandibular nerve and the relationship of the needle during injection
Extra oral technique Kurt Thoma[15]
Extraoral nerve block method has been attributed to Professor, Kurt Thoma. First, the anterior border of the masseter is located by getting the patient to clench the teeth. The operator's finger is then run down this border until its lowest point is found. This point is marked and a line drawn connecting this with the tragus of the ear. The midpoint of this line is noted as it marks externally the position of the mandibular foramen.
A line is drawn down from this point parallel with the posterior border of the mandible toward the lower border. This line is now measured and a spinal 21-gauge needle of 7–8 cm length is marked to a similar length by means of a piece of rubber dam or another suitable method. After the cleaning the skin with disinfectant.[16] An infiltration injection is made in the area with a fine gauge needle to obtain local analgesia. The long needle is now inserted on the inner aspect of the lower border of the mandible, care being taken to keep it as near bone as possible throughout the injection. The needle is gradually inserted, taking great care to keep it parallel with the line marked on the skin of the external surface of the mandible. When it has reached the depth indicated by marker that is opposite the point marked on the skin overlying the position of foramen the solution is slowly injected. In this technique, there is no such complication [Figures 3 and 4].[15]
Figure 3.

Foramen upon the skin. Draw a line from the tragus of the ear to the point where the anterior border of the masseter meets the inferior border of the mandible. Divide into halves. The point of division marks the location of the foramen
Figure 4.

Shows the needle about to be inserted for the extraoral pterygomandibular injection
RESULTS
A total of ten adult patients were enrolled in the study that required bilateral mandibular posterior teeth extraction, both the technique one on either side used which was randomly selected. The values for the onset of anesthesia, pain during injecting the LA solution, positive aspiration of the blood, supplementary injections, and complications are shown in Tables 1-5, respectively. There was no statistically significant difference found between the two techniques.
Table 1.
Onset of anesthesia
| Time (min) | Vazirani Akinosi | Kurt Thoma | χ2 (P) |
|---|---|---|---|
| 2-3 | 7 | 4 | 0.219 |
| 3.1-4 | 2 | 3 | |
| Above 4.1 | 1 | 3 | |
| Total | 10 | 10 |
Table 5.
Complications
| Vazirani Akinosi | Kurt Thoma | χ2 (P) | |
|---|---|---|---|
| Yes | 0 | 1 | 0.343 |
| No | 10 | 9 | |
| Total | 10 | 10 |
Table 2.
Pain on Visual Analog Scale
| Vazirani Akinosi | Kurt Thoma | χ2 (P) | |
|---|---|---|---|
| 0-1 | 5 | 5 | 1 |
| <1 | 5 | 5 | |
| Total | 10 | 10 |
Table 3.
Positive aspiration of blood
| Vazirani Akinosi | Kurt Thoma | χ2 (P) | |
|---|---|---|---|
| Yes | 1 | 1 | 1 |
| No | 9 | 9 | |
| Total | 10 | 10 |
Table 4.
Supplemental injection needed
| Vazirani Akinosi | Kurt Thoma | χ2 (P) | |
|---|---|---|---|
| Yes | 2 | 3 | 0.591 |
| No | 8 | 7 | |
| Total | 10 | 10 |
DISCUSSION
Classical IANB is the most commonly administered nerve block technique to achieve mandibular anesthesia both in children and in adults undergoing exodontia, endodontic procedures, minor oral surgical procedures, etc., to anesthetics the mandible there are various intaoral and extraoral techniques available. To reanalyze a lost forgotten technique in the present clinical scenario and various conditions such as trismus, tumor of the retromandibular region.
In our study, the evaluation of pain experience during injection suggested that Vazirani-Akinosi and Kurt-Thoma technique had the same perception of pain. No significant difference was seen. Although patient anxiety was more in Kurt-Thoma technique.
Comparison of three techniques done by Roy and Talukdar[2] concluded that aspiration tests were positive in 14% of total cases of Classical IANB while for Vazirani it was 6%. In our study aspiration tests were positive in 10% of total cases. The incidence of Positive aspiration encountered was same in Vaziraniakinosis and Kurt Thoma technique. The P value was statistically not significant. A study was done by Jendi and Thomas study compared two techniques in 140 patients; Vazirani-Akinosi and Halstead's technique'; observed that in the Vazirani-Akinosi group only one patients had positive aspiration while in other group 11 patients got positive aspiration.[3] The success rate achieved in this study was 97.14% with single injection for VA with highly significant difference when compared to the success rate of Halstead's standard inferior alveolar nerve block (SIANB) technique (81.42%). VA technique has a lower incidence of positive aspiration (<10%) when compared to the SIANB which is about 10%–15%. The incidence of positive aspiration with VA has been reported to be 1.43% by B Sarat Ravi Kiran et al.[17]
Kurt Thoma technique is especially beneficial when there is severe limitation of the opening of jaws. Although not preferred for usual purposes compared with other extraoral techniques, this technique may be advantageous in cases of severe limitation of mouth opening and having swellings in relation to retromolar area. One disadvantage of the technique is that anesthesia spreads slowly as compared to other intraoral techniques of IANB. Yu et al.[18] a meta-analysis found that the VA method has a faster onset of action than SIANB with significantly lower incidence of positive aspiration, and there was no significant difference in success rate between these two techniques. Comparison of three techniques done by Roy and Talukdar[2] concluded that onset of anesthesia recorded with classical IANB technique was 2.81 min. The onset of anesthesia as recorded for the Akinosi technique was 3.02 min. In our study, onset of anesthesia recorded with Vazirani-Akinosi was 2.96 min and Kurt Thoma was 3.72 min. The onset of anesthesia was slower in Kurt-Thoma technique compare to Vaziraniakinosis this may be explained on the basis that exact identification of mandibular foramen may not be possible with extra oral Kurt-Thoma technique and solution may require more time to diffuse to the nerve. A study done by Vadlamudi et al. Speed of anesthesia was moderate in Group I consisting of open mouth intraoral and Group II closed mouth intraoral and slow in Group III Kurt-Thoma technique.[19] Closed technique does come with the advantage of locating the anatomical landmarks but requires a more skilled approach as compared to other intraoral techniques. Hence, most of clinicians prefer conventional intraoral techniques as they are less technique sensitive. In Vadlamudi study, patient anxiety and clinical expertise required were also high in the Kurt Thoma Group and results were comparable with our study.
The weaknesses of VA technique cannot be forgotten. Where the maxillary tuberosity is deformed or some tumor occurs in the region of insertion of needle, it is inconvenient to conduct VA process. This approach becomes difficult to use if teeth in the maxillary arch are missing, particularly the posterior teeth. However, instead of using the gingival margin as a guideline, the alveolar ridge may be used. In children, this approach is unreliable.[20]
Other extraoral techniques will block whole the nerve while this technique will block only IAN but it is more accurate technique while other techniques are blind technique.
Vazirani akinosi technique[21]
Advantages
Relatively less patient apprehension
Relatively painless
Single-injection blocks buccal and lingual nerves as well.
Easy to perform
Complications are less likely
Very useful in trismus condition.
Disadvantages
No bony contact
Difficult to visualize the path and depth of needle penetration.
Kurt H. Thoma technique[15]
Advantage
This technique is especially beneficial when there is severe limitation of the opening of jaws
When other techniques are not possible.
Disadvantage
Extraoral skin must be cleansed properly before injecting.
CONCLUSION
Kurt Thoma and Vazirani-Akinosi techniques are good to be in one's armamentarium as all patients cannot be treated with only the IANB technique. These techniques for mandibular anesthesia should be taught to dental students. A larger sample size comparison may be done in future to emphasize our results.
Declaration of patient consent
The authors declare that they have obtained consent from patients. Patients have given their consent for their images and other clinical information to be reported in the journal. Patients understand that their names will not be published and due efforts will be made to conceal their identity but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Haas DA. Alternative mandibular nerve block techniques: A review of the Gow-Gates and Akinosi-Vazirani closed-mouth mandibular nerve block techniques. J Am Dent Assoc. 2011;142(Suppl 3):8S–12. doi: 10.14219/jada.archive.2011.0341. [DOI] [PubMed] [Google Scholar]
- 2.Roy D, Talukdar B. Comparison between conventional inferior alveolar nerve block with Vazirani-Akinosi technique and Gow-Gates technique of the mandibular nerve block. Int J Res Rev. 2019;6:364–8. [Google Scholar]
- 3.Jendi SK, Thomas BG. Vazirani-Akinosi nerve block technique: An asset of oral and maxillofacial surgeon. J Maxillofac Oral Surg. 2019;18:628–33. doi: 10.1007/s12663-019-01183-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Khalil H. A basic review on the inferior alveolar nerve block techniques. Anesth Essays Res. 2014;8:3–8. doi: 10.4103/0259-1162.128891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thangavelu K, Kannan R, Kumar NS. Inferior alveolar nerve block: Alternative technique. Anesth Essays Res. 2012;6:53–7. doi: 10.4103/0259-1162.103375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Thangavelu K, Sabitha S, Kannan R, Saravanan K. Inferior alveolar nerve block using internal oblique ridge as landmark. SRM Univ J Dent Sci. 2012;3:15–8. [Google Scholar]
- 7.Boonsiriseth K, Sirintawat N, Arunakul K, Wongsirichat N. Comparative study of the novel and conventional injection approach for inferior alveolar nerve block. Int J Oral Maxillofac Surg. 2013;42:852–6. doi: 10.1016/j.ijom.2012.11.017. [DOI] [PubMed] [Google Scholar]
- 8.Palti DG, Almeida CM, Rodrigues Ade C, Andreo JC, Lima JE. Anesthetic technique for inferior alveolar nerve block: A new approach. J Appl Oral Sci. 2011;19:11–5. doi: 10.1590/S1678-77572011000100004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Suazo Galdames IC, Cantín López MG, Zavando Matamala DA. Inferior alveolar nerve block anesthesia via the retromolar triangle, an alternative for patients with blood dyscrasias. Med Oral Patol Oral Cir Bucal. 2008;13:E43–7. [PubMed] [Google Scholar]
- 10.Nooh N, Abdullah W. Incidence of complications of inferior alveolar nerve block injection. J Med Biomed Sci. 2010;1:52–6. [Google Scholar]
- 11.Takasugi Y, Furuya H, Moriya K, Okamoto Y. Clinical evaluation of inferior alveolar nerve block by injection into the pterygomandibular space anterior to the mandibular foramen. Anesth Prog. 2000;47:125–9. [PMC free article] [PubMed] [Google Scholar]
- 12.Khoury JN, Mihailidis S, Ghabriel M, Townsend G. Applied anatomy of the pterygomandibular space: Improving the success of inferior alveolar nerve blocks. Aust Dent J. 2011;56:112–21. doi: 10.1111/j.1834-7819.2011.01312.x. [DOI] [PubMed] [Google Scholar]
- 13.Okamoto Y, Takasugi Y, Moriya K, Furuya H. Inferior alveolar nerve block by injection into the pterygomandibular space anterior to the mandibular foramen: Radiographic study of local anesthetic spread in the pterygomandibular space. Anesth Prog. 2000;47:130–3. [PMC free article] [PubMed] [Google Scholar]
- 14.Malamed SF. Handbook of Local Anesthesia. St. Louis, Missouri: Elsevier; 2013. [Google Scholar]
- 15.Thoma KH. Extraoral Conductive Anaesthesia for Oral Surgical Operations. Louisville, KY: Read before the Joint Meeting of the Interstate Association of Anesthetists and the National Dental Association; 1916. [Google Scholar]
- 16.Hutin Y, Hauri A, Chiarello L. Best infection control practices for intradermal, subcutaneous, and intramuscular needle injections. Bull World Health Organ. 2003;81:491–500. [PMC free article] [PubMed] [Google Scholar]
- 17.Kiran BS, Kashyap VM, Uppada UK, Tiwari P, Mishra A, Sachdeva A. Comparison of efficacy of halstead, vazirani akinosi and gow gates techniques for mandibular anesthesia. J Maxillofac Oral Surg. 2018;17:570–5. doi: 10.1007/s12663-018-1092-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yu F, Xiao Y, Liu H, Wu F, Lou F, Chen D, et al. Evaluation of three block anesthesia methods for pain management during mandibular third molar extraction: A meta-analysis. Sci Rep. 2017;7:40987. doi: 10.1038/srep40987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vadlamudi A, Marripudi M, Dev SP, Vivek A, Gongura H, Krishna BS. Evaluation of efficacy and pain in intra oral versus extra oral inferior alveolar nerve block technique for third molar extraction: An original research. J Adv Med Dent Sci Res. 2020;8:66–9. [Google Scholar]
- 20.Akinosi JO. A new approach to the mandibular nerve block. Br J Oral Surg. 1977;15:83–7. doi: 10.1016/0007-117x(77)90011-7. [DOI] [PubMed] [Google Scholar]
- 21.Jendi S, Thomas B. Vazirani-Akinosi nerve block technique: An asset of oral and maxillofacial surgeon. J Maxillofac Oral Surg. 2019;18:628–33. doi: 10.1007/s12663-019-01183-3. [DOI] [PMC free article] [PubMed] [Google Scholar]