

Abstract
A 45-year-old Japanese man underwent esophagogastroduodenoscopy, which revealed spotty redness at the gastric fornix, mucosal swelling, diffuse redness in the corpus, and mucosal atrophy in the gastric angle and antrum. Histological examination showed rod-shaped bacteria that appeared larger than Helicobacter pylori. The patient tested positive for rapid urease test, and serum anti-H. pylori IgG antibody test results were negative. Further examination of the bacteria revealed that H. suis antibody test was positive, and the presence of H. suis was confirmed using H. suis-specific real-time PCR. H. suis was successfully eradicated after triple therapy with vonoprazan, amoxicillin, and clarithromycin. This case reinforces the notion that non-H. pylori Helicobacter species such as H. suis and H. heilmannii may be involved in the pathogenesis of active gastritis in patients who test negative for H. pylori antibodies.
1. Introduction
Since its discovery in 1982, Helicobacter pylori has been widely recognized as a pathogenic organism that causes gastritis, peptic ulcer disease, and gastric cancer [1]. In addition to H. pylori, various spiral-shaped organisms have been identified in humans and other animals. Helicobacter species other than H. pylori are known as non-Helicobacter pylori Helicobacter, which include H. suis, H. heilmannii, H. bizzozeroni, H. salomonis, and H. felis. Among these, H. suis is the primary human pathogenic organism [2].
Although H. suis infection in the human stomach causes gastritis, the clinicopathological features of H. suis-associated gastritis have long been uninvestigated because its isolation and cultivation are technically difficult [3]. Herein, we report the case of a patient with H. suis-associated gastritis, who showed endoscopic features similar to those of conventional H. pylori-associated atrophic gastritis.
2. Case Presentation
A 45-year-old Japanese male underwent upper gastrointestinal series and was diagnosed with chronic gastritis. Subsequently, the patient underwent esophagogastroduodenoscopy, which revealed spotty redness at the gastric fornix (Figure 1(a)), mucosal swelling, diffuse redness in the corpus (Figure 1(b)), and mucosal atrophy at the gastric angle (Figure 1(c)) and antrum (Figure 1(d)). Regular arrangement of collecting venules was scarcely identified throughout the stomach. Thus, atrophic gastritis and current infection of H. pylori were suspected. However, the serum anti-H. pylori IgG antibody test results were negative. Histological examination revealed rod-shaped bacteria that appeared larger than H. pylori (Figure 2, arrows). Infection of non-H. pylori Helicobacter species, such as H. suis and H. heilmannii, was then suspected, and the patient was referred to our hospital for further investigation.
Figure 1.
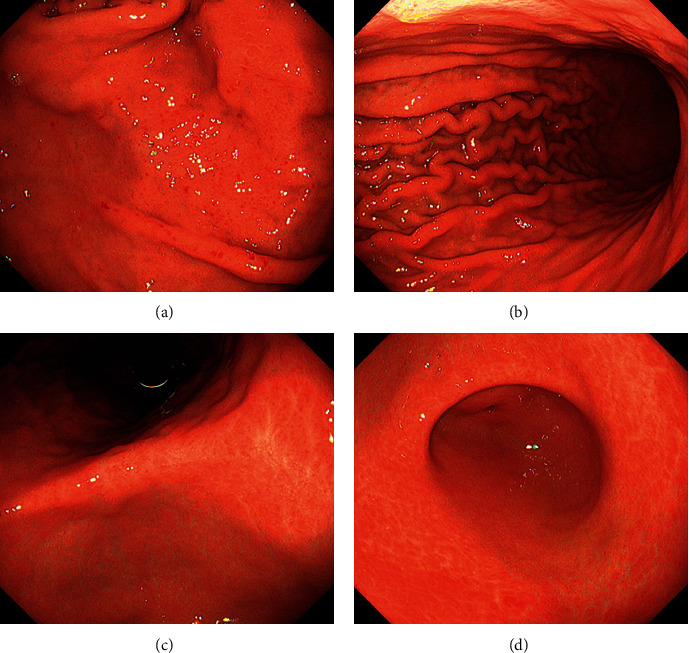
Esophagogastroduodenoscopy images. Endoscopy reveals spotty redness at the gastric fornix (a), mucosal swelling with diffuse redness in the corpus (b), and mucosal atrophy in the gastric angle (c) and antrum (d).
Figure 2.
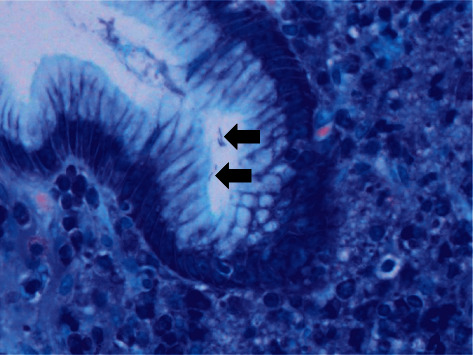
Histological image. Giemsa stain shows rod-shaped bacteria appearing larger than H. pylori (arrows), suggesting a non-Helicobacter pylori Helicobacter infection.
The patient had no history of other diseases and was not taking any medication. Physical examination revealed no abnormalities and no evidence of hepatosplenomegaly or peripheral lymphadenopathy. All laboratory findings, including lactate dehydrogenase and soluble interleukin-2 receptor levels, were within the normal ranges. Repeat esophagogastroduodenoscopy and biopsy showed rod-shaped bacteria that seemed larger than H. pylori. The patient tested positive in the rapid urease test. The serum anti-H. pylori IgG antibody test was negative, whereas the in-house ELISA test for the H. suis antibody was positive. The presence of H. suis was further confirmed using H. suis-specific real-time polymerase chain reaction (PCR) targeting ureA and outer membrane protein genes (Figure 3) [4, 5]. H. pylori was negative on PCR test. Consequently, the patient was diagnosed with H. suis-associated gastritis. H. suis was successfully eradicated after triple therapy with vonoprazan, amoxicillin, and clarithromycin. Esophagogastroduodenoscopy performed two months after eradication therapy showed that spotty redness remained at the gastric fornix (Figure 4(a)), while mucosal swelling and diffuse redness in the corpus disappeared (Figure 4(b)).
Figure 3.
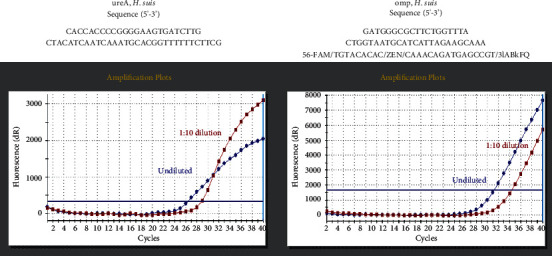
PCR analysis. The presence of H. suis is confirmed using H. suis-specific real-time PCR, targeting ureA and outer membrane protein genes.
Figure 4.
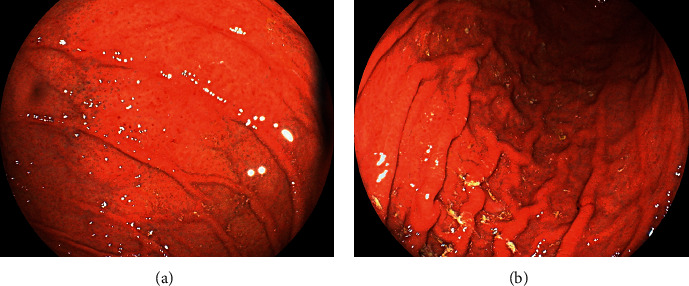
Esophagogastroduodenoscopy images two months after the eradication therapy. Spotty redness still exists at the gastric fornix (a), while mucosal swelling and diffuse redness are not observed in the corpus (b).
3. Discussion
H. suis is a zoonotic pathogen that colonizes the gastric mucosa of 60–95% of pigs at the slaughter age. H. suis primarily infects the fundic and pyloric gland zones of the porcine stomach, leading to gastritis, gastric ulcers, and decreased daily weight gain [6]. Since the first human case of H. suis-associated erosive gastritis was reported in 1994 [7], H. suis infection in humans has been described in only a small number of cases. This is mainly because it is difficult to isolate and cultivate the pathogen. Rimbara et al. reported that H. suis is not viable at neutral pH. Thus, endoscopic biopsy specimens containing H. suis require a low-pH medium for transport and successful isolation [3]. In the present patient, an in-house enzyme-linked immunosorbent assay for the detection of human IgG antibodies to H. suis was positive. In addition, we extracted the DNA from the gastric biopsy specimens and performed nested PCR using the specific primers for H. suis [8], which was also positive. Consequently, the patient was diagnosed with H. suis-associated gastritis.
Although H. suis has urease activity, its activity is generally lower than that of H. pylori [9]. Therefore, the urea breath test and rapid urease test, which are commonly used to detect urease activity in H. pylori, often yield negative results for H. suis [3, 10]. However, the patient tested positive in the rapid urease test. Since both serum H. pylori antibody and PCR assays for H. pylori were negative, co-infection with H. suis and H. pylori was unlikely. Consequently, the urease activity of H. suis detected in the present patient may have been comparable to that of H. pylori. Another explanation is that the bacterial density of H. suis was greater than that of other patients with H. suis infections.
The typical endoscopic features of non-Helicobacter pylori Helicobacter-associated gastric lesions include spotty redness, crack-like mucosa, nodular gastritis-like appearance, and white marbled appearance. Erosions, ulcers, and even extranodal marginal zone lymphoma of the mucosa-associated lymphoid tissue can be found in the stomach, in association with non-Helicobacter pylori Helicobacter infection [11, 12]. Tsukadaira et al. investigated 50 patients with non-Helicobacter pylori Helicobacter infections in the stomach, including 26 cases of H. suis and two cases of H. heilmannii/H. ailurogastricus [13]. The authors reported that the crack-like mucosa was observed in 45 out of 50 patients (90.0%), which was defined as a mesh-like morphology composed of faded, depressed, and varying width lines on coarse and slightly reddish mucosa extending from the gastric antrum to the angle. Nodular gastritis was noted in 11 out of 50 patients (22.0%). All the patients had a regular arrangement of collecting venules in the gastric corpus (100%). Shiratori et al. reported two patients with non-Helicobacter pylori Helicobacter infection of the stomach [14]. Both patients had a white marble appearance in the lesser curvature of the gastric angle and antrum, and the authors speculated that the white marble appearance is a potential characteristic finding of non-Helicobacter pylori Helicobacter infection gastritis.
Table 1 shows the endoscopic features of the stomach that are characteristic of patients with current H. pylori infection according to the Kyoto classification of gastritis [15]. They include atrophy, diffuse redness, foveolar-hyperplastic polyps, xanthomas, intestinal metaplasia, mucosal swelling, patchy redness, depressive erosions, enlarged and tortuous folds, sticky mucus, spotty redness, and nodularity. In contrast, fundic gland polyps and the regular arrangement of collecting venules are absent or reduced in the stomachs of patients with current H. pylori infection, as opposed to those of people without the infection. Map-like redness is a representative endoscopic feature observed in the stomachs of patients in whom H. pylori infection has been previously eradicated.
Table 1.
Endoscopic features according to the Kyoto classification of gastritis.
| Typical case of active infection with H. pylori | Present patient | |
|---|---|---|
| Entire stomach | ||
| Atrophy | Present | Present |
| Diffuse redness | Present | Present |
| Foveolar-hyperplastic polyp | Present | Absent |
| Xanthoma | Present | Absent |
| Intestinal metaplasia | Present | Absent |
| Mucosal swelling | Present | Present |
| Patchy redness | Present | Absent |
| Depressive erosion | Present | Absent |
| Map-like redness | Absent | Absent |
|
| ||
| Gastric body | ||
| Enlarged and tortuous folds | Present | Present |
| Sticky mucus | Present | Absent |
|
| ||
| Gastric fornix and body | ||
| Spotty redness | Present | Present |
| Fundic gland polyp | Absent | Absent |
|
| ||
| Lower gastric body to antrum | ||
| Nodularity | Present | Absent |
| Regular arrangement of collecting venules | Absent | Absent |
The esophagogastroduodenoscopy performed in the present patient revealed that the crack-like mucosa and white marble appearance were absent, and a regular arrangement of collecting venules was scarcely identified throughout the stomach. Instead, spotty redness at the gastric fornix, mucosal swelling, diffuse redness in the corpus, and mucosal atrophy in the gastric angle were observed (Table 1). In a previous report, the spotty redness in the corpus was found in 4 out of 50 patients (8.0%), and mucosal swelling was observed in only 1 out of 50 patients (2.0%) [13]. The endoscopic features of our patient were indistinguishable from those of conventional H. pylori-induced gastritis. Although the exact cause of the infrequent endoscopic appearance of H. suis-associated gastritis remains unclear, the higher urease activity, which was presumed from the positive results of the rapid urease test, might be involved in the unique endoscopic features of the present patient. However, as this report describes only one patient, this issue must be investigated.
4. Conclusions
This case reinforces the notion that non-H. pylori Helicobacter species, such as H. suis, may be involved in the pathogenesis of active gastritis in patients who tested negative for H. pylori antibodies. It is also noteworthy that H. suis-associated gastritis may present with endoscopic features indistinguishable from those of H. pylori infection.
Data Availability
The data used to support the findings of this study are restricted in order to protect patient privacy.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1.Bessède E., Mégraud F. Microbiota and gastric cancer. Seminars in Cancer Biology . 2022 doi: 10.1016/j.semcancer.2022.05.001. In press. [DOI] [PubMed] [Google Scholar]
- 2.Padra M., Adamczyk B., Flahou B., et al. Helicobacter suis infection alters glycosylation and decreases the pathogen growth inhibiting effect and binding avidity of gastric mucins. Mucosal Immunology . 2019;12(3):784–794. doi: 10.1038/s41385-019-0154-4. [DOI] [PubMed] [Google Scholar]
- 3.Rimbara E., Suzuki M., Matsui H., et al. Isolation and characterization of Helicobacter suis from human stomach. Proceedings of the National Academy of Sciences of the United States of America . 2021;118(13) doi: 10.1073/pnas.2026337118.e2026337118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liu J., He L., Haesebrouck F., et al. Prevalence of coinfection with gastric non-Helicobacter pylori Helicobacter (NHPH) species in Helicobacter pylori-infected patients suffering from gastric disease in Beijing, China. Helicobacter . 2015;20(4):284–290. doi: 10.1111/hel.12201. [DOI] [PubMed] [Google Scholar]
- 5.Takigawa H., Masaki S., Naito T., et al. Helicobacter suis infection is associated with nodular gastritis-like appearance of gastric mucosa-associated lymphoid tissue lymphoma. Cancer Medicine . 2019;8(9):4370–4379. doi: 10.1002/cam4.2314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.De Bruyne E., Flahou B., Chiers K., et al. An experimental Helicobacter suis infection causes gastritis and reduced daily weight gain in pigs. Veterinary Microbiology . 2012;160(3-4):449–454. doi: 10.1016/j.vetmic.2012.06.031. [DOI] [PubMed] [Google Scholar]
- 7.Tanaka M., Saitoh A., Narita T., et al. Gastrospirillum hominis-associated gastritis: the first reported case in Japan. Journal of Gastroenterology . 1994;29(2):199–202. doi: 10.1007/bf02358683. [DOI] [PubMed] [Google Scholar]
- 8.Matsui H., Takahashi T., Murayama S. Y., et al. Development of new PCR primers by comparative genomics for the detection of Helicobacter suis in gastric biopsy specimens. Helicobacter . 2014;19(4):260–271. doi: 10.1111/hel.12127. [DOI] [PubMed] [Google Scholar]
- 9.De Groote D., Ducatelle R., van Doorn L. J., Tilmant K., Verschuuren A., Haesebrouck F. Detection of ‘Candidatus Helicobacter suis’ in gastric samples of pigs by PCR: comparison with other invasive diagnostic techniques. Journal of Clinical Microbiology . 2000;38(3):1131–1135. doi: 10.1128/jcm.38.3.1131-1135.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Goji S., Tamura Y., Sasaki M., et al. Helicobacter suis-infected nodular gastritis and a review of diagnostic sensitivity for Helicobacter heilmannii-like organisms. Case Reports in Gastroenterology . 2015;9(2):179–187. doi: 10.1159/000431169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kadota H., Yuge R., Miyamoto R., et al. Investigation of endoscopic findings in nine cases of Helicobacter suis-infected gastritis complicated by gastric mucosa-associated lymphoid tissue lymphoma. Helicobacter . 2022;27(3) doi: 10.1111/hel.12887.e12887 [DOI] [PubMed] [Google Scholar]
- 12.Nakagawa S., Shimoyama T., Nakamura M., et al. The resolution of Helicobacter suis-associated gastric lesions after eradication therapy. Internal Medicine . 2018;57(2):203–207. doi: 10.2169/internalmedicine.8971-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tsukadaira T., Hayashi S., Ota H., et al. Prevalence, clinical features, and esophagogastroduodenoscopy (EGD) findings of non-Helicobacter pylori Helicobacter infection: a study of 50 cases at a single facility in Japan. Helicobacter . 2021;26(4) doi: 10.1111/hel.12811.e12811 [DOI] [PubMed] [Google Scholar]
- 14.Shiratori S., Mabe K., Yoshii S., et al. Two cases of chronic gastritis with non-Helicobacter pylori Helicobacter infection. Internal Medicine . 2016;55(14):1865–1869. doi: 10.2169/internalmedicine.55.5891. [DOI] [PubMed] [Google Scholar]
- 15.Hojo M., Nagahara A., Kudo T., et al. Endoscopic findings of Helicobacter pylori gastritis in children and young adults based on the Kyoto classification of gastritis and age-associated changes. JGH Open . 2021;5(10):1197–1202. doi: 10.1002/jgh3.12652. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data used to support the findings of this study are restricted in order to protect patient privacy.