

Abstract
Background
There is a growing attention on the role of patients and stakeholders in resilience, but there is lack of knowledge and methods on how to support collaborative learning between stakeholders and co-creation of resilient healthcare. The aim of this article was to demonstrate how the methodological process of a consensus process for exploring aspects of next of kin involvement in hospital cancer care can be replicated as an effort to promote resilient healthcare through co-creation with multiple stakeholders in hospitals.
Methods
The study applied a modified nominal group technique process developed by synthesizing research findings across 4 phases of a research project with a mixed-methods approach. The process culminated in a 1-day meeting with 20 stakeholder participants (5 next of kin representatives, 10 oncology nurses, and 5 physicians) from 2 Norwegian university hospitals.
Results
The consensus method established reflexive spaces with collective sharing of experiences between the 2 hospitals and between the next of kin and healthcare professionals. The method promoted collaborative learning processes including identification and reflection upon new ideas for involvement, and reduction of the gap between healthcare professionals’ and next of kin experiences and expectations for involvement. Next of kin were considered as important resources for resilient performance, if involved with a proactive approach. The consensus process identified both successful and unsuccessful collaborative practices and resulted in a co-designed guide for healthcare professionals to support next of kin involvement in hospital cancer care.
Conclusions
This study expands the body of knowledge on methods development that is relevant for collaborative learning and co-creation of resilient healthcare. This study demonstrated that the consensus methods process can be used for creating reflexive spaces to support collaborative learning and co-creation of resilience in cancer care. Future research within the field of collaborative learning should explore interventions that include a larger number of stakeholders.
There is a growing attention on the role of patients and stakeholder involvement and collaborative learning in resilient healthcare.1–11 However, there is still a lack of knowledge and methods on how to support collaborative learning among healthcare stakeholders to promote the co-creation of resilient healthcare.12,13 The objective of this article is to demonstrate and reflect on how a consensus methods process was developed to explore next of kin involvement in resilient healthcare and collaborative learning among stakeholders in hospital cancer care in 2 Norwegian university hospitals. Based on the lessons learned, we suggest ways for others to replicate our methodological approaches in their effort to promote resilient healthcare.
Collaborative Learning and Co-creation of Resilient Healthcare
Resilient healthcare can be defined as “a healthcare system’s ability to adjust its functioning before, during, or following changes and disturbances, so that it can sustain required performance under both expected and unexpected conditions.”14(pXXV) Resilient performance in organizations depends on 4 resilience potentials suggested by Hollnagel15: anticipation (knowing what to expect), monitoring (knowing what to look for), responding (knowing what to do and how to adjust), and learning (knowing what has happened and how to improve).15 The capacity to learn and adapt is a fundamental part of resilience thinking, including learning from what went wrong and from innovative practices or changes.16–18 Collaborative learning, which happens in teams and as part of organizational dynamics and change, is a natural consequence of learning at work.19,20 Collaborative learning consists of adaptations, adjustments, improvization, and flexibility, all of which are key characteristics of resilient healthcare. The literature on resilient healthcare uses the terminology of learning potential to reflect how organizations use previous knowledge, errors, and successes to learn and improve their practice.15 However, this literature still lacks a closer connection to the way in which collaborative learning occurs, from both success and failure, and as part of everyday work.3,21–23 Moreover, with a few exceptions,24,25 there is a lack of knowledge about how healthcare providers can apply specific methods in their practice to promote certain types of learning processes in resilience. These methods include patient and stakeholder involvement and how they can be used as a source of resilience and be integrated into collaborative learning processes, either as part of the treatment team, as part of improvement projects, or as part of service development and delivery on a general basis.26–29
Aim and Research Questions
The aim of this study is to explore collaborative learning and user involvement as 2 prerequisites for conceptualization and operationalization of resilience to maintain quality in healthcare.3 This includes acknowledging the role of stakeholders and their contribution in the co-creation of resilient healthcare.5,10 The following research questions guided this study:
How can the application of consensus process methods be applied to foster collaborative learning and co-creation of resilience in hospital cancer care?
Based on this process, what lessons can be learned for next of kin, researchers, and service providers interested in supporting resilient healthcare processes?
By investigating how the mixed-methods research project “Quality and safety in hospital cancer care: a mixed-methods study of next of kin involvement”30 used results from different project phases5,31,32 and involved the participants from the study hospitals and next of kin representatives in a modified nominal group technique consensus process, this article expands the body of knowledge on methods development that is relevant for collaborative learning and the co-creation of resilient healthcare.
METHODS
Design, Data Collection, and Study Setting
This study builds on and synthesizes findings from a mixed-methods research project consisting of 3 substudies that explored quality and safety in 2 Norwegian hospitals.30,33,34 Substudy one was a qualitative study that explored next of kin involvement and methods used in hospital cancer care from the perspectives of healthcare professionals.5,31 Substudy 2 was a quantitative measurement study involving 238 next of kin in a survey of next of kin satisfaction with cancer care services.32 Substudy 3 was a consensus process where the results of substudies 1 and 2 were merged and presented to a stakeholder group.35 The design of substudy 3 was a multistage modified nominal group technique performed as a collaborative learning forum leading to consensus on specific research questions.36 The process was conducted as a 1-day meeting with 20 stakeholder participants, and the main goal was to develop a next of kin involvement guide for hospital cancer care. The healthcare professionals were recruited from affiliated cancer care departments at the same 2 Norwegian university hospitals, and the next of kin representatives were recruited by the regional health authority and by learning and coping centers in the cities in which the 2 hospitals were located.
Three questions guided the consensus process: What can we learn from next of kin experiences with hospital cancer care? How can these experiences be valued more systematically to improve the quality and safety of cancer care? What methods or tools are appropriate for collecting experiences and for next of kin involvement locally, regionally, and nationally? The consensus process had a 2-fold aim: to establish consensus on the 3 questions that informed the development of a guide for next of kin involvement in cancer care and to bring together stakeholders from 2 hospitals in a collaborative learning process to reflect on research findings from their own hospitals5,31,32,35 and learn from each other’s and from next of kin representatives’ experiences and practices. Results from the development of the guide, including methodological details, have been published elsewhere.35 This article reports on the second aim of the consensus process: focusing on lessons learned from the entire process and how to model methods for collaborative learning and co-creation of resilient healthcare.
Ethics Approval and Consent to Participate
The study is approved by the regional committee for medicine and health research ethics in Norway (2015/1488). Participation was based on voluntary recruitment and informed consent. The study governance was also approved by data protection officers at the 2 hospitals.
Modeling Methods–Research Phases and Analysis
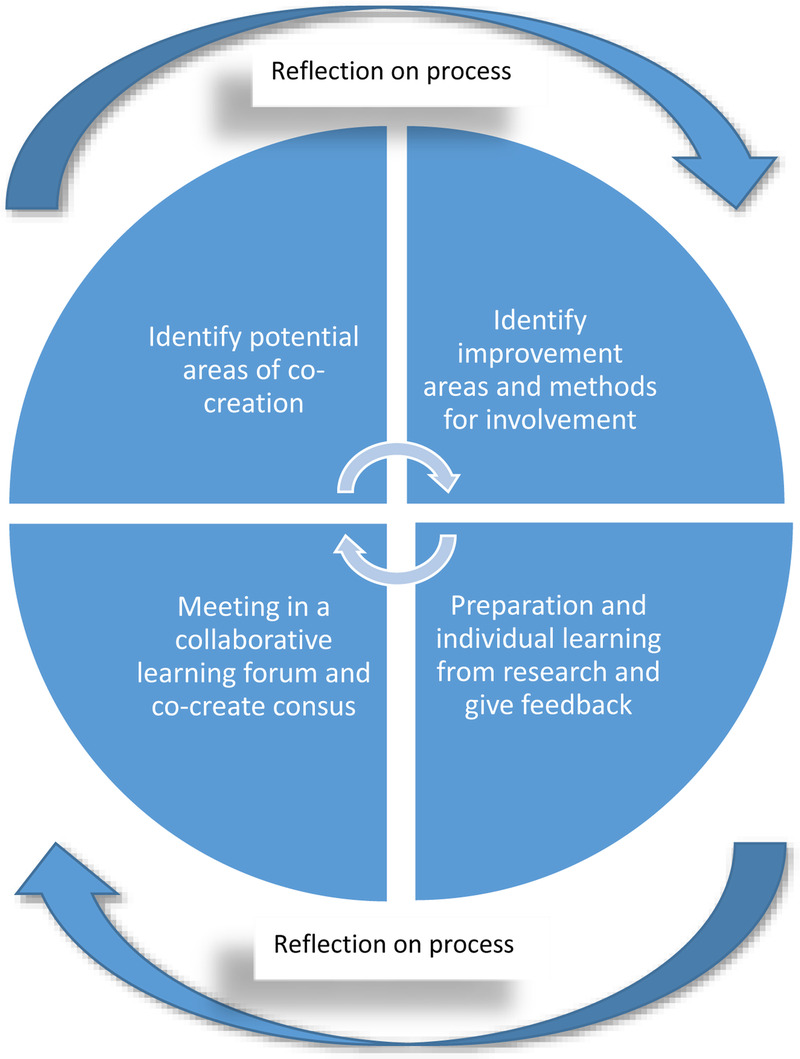
The consensus process was informed by 4 steps of the research project,35 before the actual consensus meeting, as illustrated in Figure 1.
FIGURE 1.
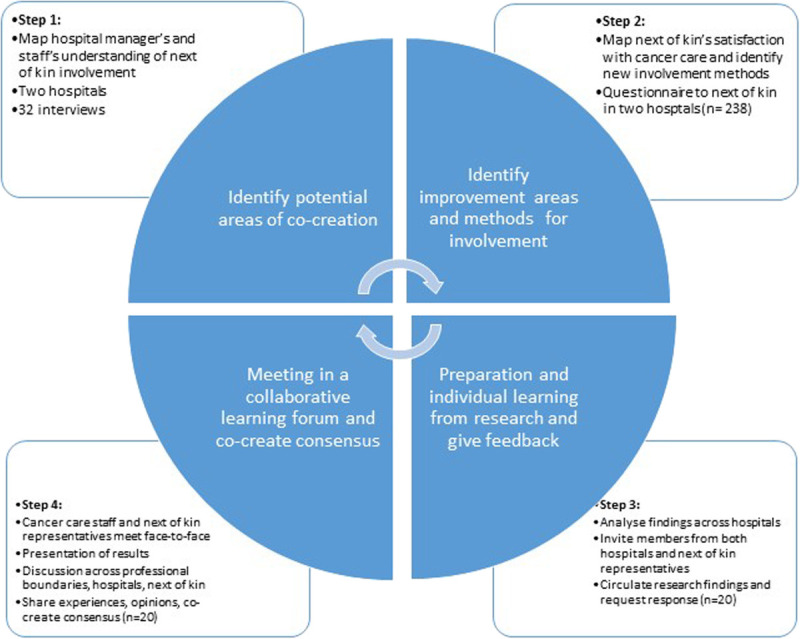
Modeling methods for collaborative learning and co-creation of resilience.
Step 1—Identify Potential Areas of Co-creation
In step 1, we identified how 32 cancer care managers and staff in 2 Norwegian university hospitals experienced the role of next of kin in cancer care quality and safety and potential areas of co-creation (information, pain treatment, transitions, observation, motivation and emotional support, physical activity and rehabilitation, daily care, nutrition, and palliative and terminal care31). The voluntary informants in this step were recruited by their nearest manager with close collaboration with appointed local coordinators in both hospitals.30,31 The sample consisted of 8 nurses, 12 oncology nurses, 7 consultants, and 1 quality manager. Thirteen of the participants were managers and 19 were healthcare professionals. The participants had desired variation in different positions, age, service levels, and experience.30
Step 2—Identify Improvement Areas and Methods for Involvement
In step 2, we surveyed 238 next of kin to cancer care patients. A consecutive sampling strategy was used to identify participants for this step.37 The sample comprised 59% women and 41% men. The most frequent cancer diagnoses for the patient was hematologic cancer, gastrointestinal cancer, and breast cancer.32 Participants reported on satisfaction with cancer care using the 20-item FAMCARE Scale.38,39 In addition, many of the survey respondents (n = 100) answered a question in free text about their preferred methods for involving next of kin in cancer care.32 Results showed that hospital cancer care should provide next of kin involvement through a 2-sided approach by balancing the next of kin needs with the patient perspective.32
Step 3—Preparation and Individual Learning From Research and Giving Feedback
In step 3, all results from step 1 and 2 were analyzed across hospitals with a mixed-methods apporach.30,33,34 At this stage, we recruited 20 participants for participation in the consensus process with the purpose of creating a collaborative learning forum between the 2 hospitals and next of kin representatives. A purposive sampling strategy was used to recruit participants for the consensus meeting.30,35,37 The participants were 2 local and 1 regional next of kin representatives, 2 next of kin representatives form coping centers, 5 physicians, and 10 oncology nurses.30,35
We circulated 2 published research articles5,31 and a summary of the results in step 2 to the participants, in preparation for the consensus meeting. All participants replied with sending in one written page of their individual feedback about the 3 questions guiding the consensus process. The author team, with I.J.B. in the lead, completed a qualitative content analysis of the written material inspired by Graneheim and Lundman.40
Step 4—Meeting in a Collaborative Learning Forum and Co-create Consensus
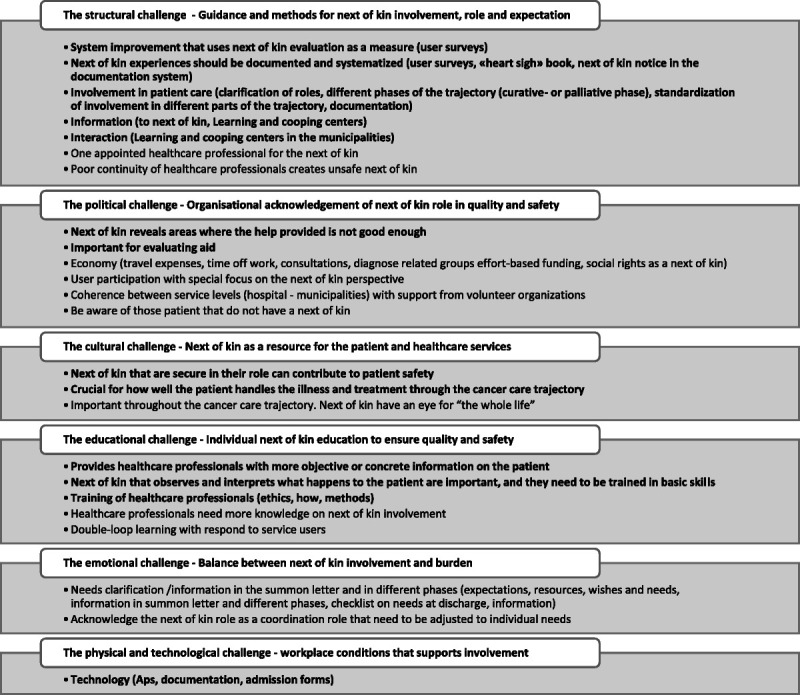
In step 4, we gathered all the participants in a 1-day consensus meeting. The day started with an informal introduction and welcome session with all participants and the 5 researchers who facilitated the process. I.J.B. presented a summary of the findings and the results of the content analysis from step 3 to set the scene, before breaking participants into 2 working groups. The 2 groups included healthcare professionals and next of kin representatives from both hospitals. Each group discussed separate questions and reached agreement on codes. After each group reached agreement, the researchers brought the 2 groups together in a plenary session, where they both presented their codes. We continued with further input and discussion with all participants. The day ended with all participants voting anonymously on their top 5 priorities for the questions of both groups. A minor change was made to only one of the codes in the list. The results of the consensus process have been integrated into a guide for healthcare professionals in next of kin involvement in cancer care (Fig. 2). This is a co-created reflexive tool for hospital managers and staff.35
FIGURE 2.
Bergerød et al’s revised organizing for quality framework model31(p10) inspired by Bate et al.41
In the consensus meeting, 2 researchers facilitated each of the groups during the group work and all researchers contributed to facilitating the discussions during the plenary sessions if needed. Researchers consisted of 2 cancer nurses, 2 doctors, and 1 safety scientist. One of the researchers observed the entire process and took notes. In this article, we use the observation notes, data from the consensus meeting, and researchers’ experiences, to reflect on the method in light of a resilient healthcare perspective to derive the lessons learned and suggest tips for success.
RESULTS
Creating Reflexive Spaces Between Stakeholders
The consensus process contributed to the establishment of reflexive spaces4 for face-to-face dialogical practices. This involved the sharing of experiences and suggestions between the 2 hospitals and between next of kin and healthcare professionals. New ideas were generated and debated. The participants agreed that next-of-kin stakeholders can be important resources for the patient and healthcare professionals in terms of hospital quality and safety, if they take an appropriate proactive approach.
The 1-day consensus meeting consisted of several reflexive spaces. First, the collective setting of the agenda and presentation to the participants created an important starting point. On the neutral ground of a hotel conference room, all participants could introduce themselves and tell others about their background and expectations for the day. The participants briefly spoke about their workplace, occupation, background, and expectations. No one behaved in a condescending manner or appeared superior to others. Second, presentation of the results by the researchers opened dialog, allowing opportunity for clarifications, and prepared all participants for group discussions. Third, group discussions with reflections around the learning from next of kin and ways of using their experiences, and identification of appropriate involvement methods, demonstrated a wide variety of perspectives, ideas, and challenges to make this happen. The mix of participants in the groups and the heterogeneous group design ensured that no hospital or professional group was overrepresented. Here, we observed a high degree of sharing of ideas, suggestions, and reflections. Although next of kin representatives were a minority in the 2 groups, they contributed and were invited to participate either by the facilitators or by the other participants. Fourth, the following plenary session to discuss and finalize the voting of the top priorities also constituted a reflexive space where the groups shared their results and met for a plenary discussion and additional input. However, we observed less debate and fewer suggestions in the group sessions. In the plenary session, all 20 participants and the 5 researchers were present, and we observed less eagerness and interest in speaking than in the smaller group sessions. Still, everyone contributed and added new ideas and discussed the results to ensure a common understanding of the topics before the voting. Moreover, the final plenary session constituted an arena where all participants were given the opportunity to ask questions, evaluate the meeting, and obtain the same information about the finalization of the consensus process. This resulted in all participants leaving the 1-day meeting with a shared understanding of the further progress of completing the next of kin involvement guide (Fig. 2). Establishing reflexive spaces has been suggested as a way of incorporating resilience into management and regulation.4 Our approach also demonstrated its relevance for groups of different patients and stakeholders.
Identifying and Reflecting Upon New Involvement Methods
The participants in the 1-day consensus meeting had prepared for the session by reading and reflecting on involvement (Fig. 1). The consensus meeting identified what worked well for both next of kin and healthcare professionals and areas where types and methods of involvement either could be improved or were lacking. Also important was the articulation of work-as-done by healthcare professionals and work-as-experienced by next of kin. This articulation identified work processes in the cancer care trajectory and how these might or might not benefit from next of kin involvement and where such involvement might be of utter importance and therefore in need of stronger acknowledgement and support.
We experienced a large interest in new ideas for involvement methods but also suggestions for how involvement could be better systematized by the healthcare professionals and providers (e.g., prompted and documented in medical record). In addition, the requirements for success, both from the healthcare professionals’ and from the next of kin’s point of view, were identified (e.g., time, money, training, IT registration systems). Although no representatives from the primary care services participated in the consensus process (e.g., from general practitioners, home care, nursing homes, municipal decision offices), several of the methods and suggestions also related to these service providers, because cancer patients often receive services from all levels of the healthcare service.
Some of the suggested involvement initiatives in the next-of-kin involvement guide (Fig. 2)35 were a system improvement that uses next of kin evaluation as a measure (user surveys), closer interaction with external support bodies in cancer care, systematic involvement in the cancer care trajectory, and training for healthcare professionals in next of kin involvement. In addition, the participants pinpointed that the way in which next of kin experiences are used for improvement can be of importance for how well a patient manages the illness and treatment through the cancer care trajectory.35 Both next of kin and healthcare professionals agreed that next of kin may contribute with essential information and play a key role in patient transitions between service levels, in medication management, and in foreseeing possible deteriorations and treatment consequences. However, neither of the hospitals’ participants nor the next of kin representatives had experienced these contributions being taken into account in a systematic way. Therefore, they suggested specific methods for registration and reminders to follow up and document the next of kin involvement, to ensure double loop learning and improvement in their organizations.35
Co-designing a Guide to Improve Involvement
The participants in the consensus meeting knew upfront that the research process was intended to develop and co-design an experience-based guide for next of kin involvement for healthcare professionals in hospital cancer care. Some healthcare professionals from both hospitals had participated in the early-phase interviews, but all participants acquired insight into the research process leading up to the consensus meeting. The consensus voting process included 2 rounds of voting to agree on: (1) methods or tools appropriate for collecting experiences and for involvement of next of kin and (2) what can be learned from next of kin experiences and how these experiences can be valued more systematically to improve cancer care quality and safety. The top 5 priorities (e.g., document next of kin experiences; clarify involvement in patient care) in both voting rounds resulted in more than 5 topics, because several topics received equal scores (e.g., provide healthcare professionals with objective information; next of kin need to be trained in basic treatment skills). We included all items in the guide and did not run an additional round of voting to exclude topics, because we found the suggestions relevant and anchored in the group.35
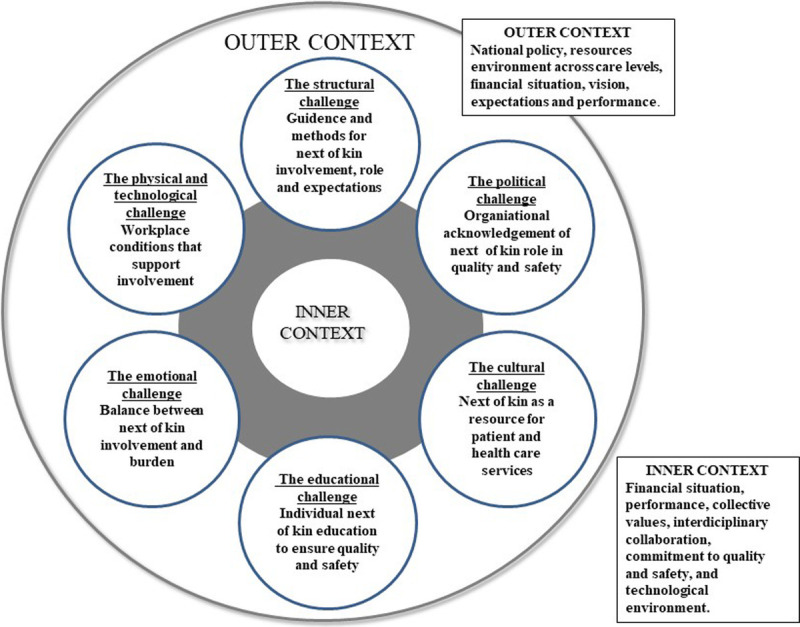
The next of kin involvement guide35 is structured around the organizing for quality framework, developed by Bate and Roberts.41 The foundation for the framework is based on large studies of hospitals in Europe and the Unites States showing the need to resolve 6 challenges to ensure quality and safety in healthcare: structure, culture, emotions, education, politics, and physical and technical challenges. In step 1 of the research process (Fig. 1), we analyzed the results according to the organizing for quality framework, suggested adaptations, and developed the theoretical framework to increase its relevance for the cancer care context,31 depicted in Figure 3.
FIGURE 3.
“Organizing for quality and safety: a next of kin involvement guide.”35(p8)
We used the model in Figure 3 as a basis for the next of kin involvement guide and added the participants’ topics to each of the 6 challenges to operationalize these into practical tasks or ideas for healthcare professionals. The final guide (Fig. 2) includes the 6 challenges and several items for each challenge to guide everyday involvement in cancer care.35 The guide is oriented around reflection and support for successful involvement, rather than as a basis for identifying gaps, failures, and malpractice.
DISCUSSION
In this article, we have illustrated how a consensus process was used to link 4 phases of a research project and bring together stakeholders (doctors, nurses, and next of kin representatives) from 2 university hospitals. In the following section, we discuss lessons learned for service providers, next of kin, and for research with a resilient healthcare perspective.
Lessons Learned for Service Providers and Next of Kin
In the literature, reflexive spaces can be understood as physical or virtual platforms where reflexive dialogical practices happen among stakeholders.42 The consensus process generated reflexive spaces and supported learning processes between hospitals and between stakeholders.42–44 It also constituted an arena for learning from within hospitals, because professional groups that often tend to learn within professional silos45 were brought together to discuss and share experiences. Although our research project was conducted over a longer period than a typical improvement process in a hospital or primary care service provider, we argue that the approach is not time-sensitive and constitutes process-based tips for other service providers whether this is a large- or small-scale process in a short- or long-term perspective. It is essential to bring healthcare professionals and other stakeholders together to learn and close the gap between work-as-imagined and work-as-done,24,46 and the consensus process proved successful.
As demonstrated by Ellis and colleagues,47 resilience research needs new methods for investigating resilience and for identifying interventions to support resilient healthcare. This is also supported by others4,46,48; however, an intervention in resilience in healthcare is not a tool, technology, or rule to be implemented. Instead, we argue that interventions should be designed to foster work conditions and work processes under which resilient performance is more likely to occur. Resilience is not something an organization has; it is an adaptive capacity in organizations depending on the potentials to anticipate, monitor, respond, and learn.15 Here, learning processes are key because learning is always involved in everyday work.20,43,44 By investing time in bringing together healthcare professionals, managers, and other stakeholders, we were able to create reflexive spaces42 that promoted a shared understanding and mental models of what were experienced as best work practices (e.g., specific meeting with next of kin, systematic questions to next of kin during cancer care trajectory; organize and cover of all transport costs) and work-as-done14,49 (e.g., irregular meetings, limited option for individual conversation without patient present). Thereby, the process supported learning from successful involvement practices, while also identifying practices that should be improved or avoided. We hold that other service providers could take advantage of this approach in their effort to promote resilient performance and co-design services with next of kin, healthcare professionals, and managers. All of these stakeholders are playing a key role in the healthcare service provision,12,50 and next of kin in particular in co-creating resilience as they support resilience potentials and complement the healthcare professionals at times of peak demand, low staffing, and care transitions.1,5
Thinking in practical terms of how such a consensus process could take place in, for example, a hospital or nursing home setting, our tip for service providers is to treat the process as integral to ongoing improvement work.51 In Figure 4, we provide an example of how this might be implemented, inspired by the Formative Evaluation Feedback Loops (FEFLs) method proposed by Braithwaite and colleagues.52,53 The FEFL method is based on the Plan-Do-Study-Act approach, which consists of a 4-stage learning approach to improvement: (1) determining the nature and scope of the problem, (2) deciding the changes to be made, (3) implementing the changes, and (4) assessing the results. Action should then be advanced with the FEFL cycle resuming. As depicted in Figure 4, we recommend testing on a small scale and start by identifying the area of interest for care quality (e.g., medication administration, investigations, adverse events, success stories) and reveal the diverse perspectives from stakeholders (patient, next of kin, healthcare professionals, managers). Similar to our process, the next step could be to disseminate aggregated information to the involved stakeholders about the different views and ask stakeholders to reflect individually, before bringing all participants together to discuss and establish consensus on the best way forward. This could, for example, be translated into practice by implementing ideas in pilot testing of a new work practice in a ward or clinic and assess development over time; or by establishing new joint meeting arenas for sharing of knowledge between stakeholders. Over time the process could be repeated to continuously improve work practices, as shown in Figure 4 where loops move upwards and to the right.
FIGURE 4.
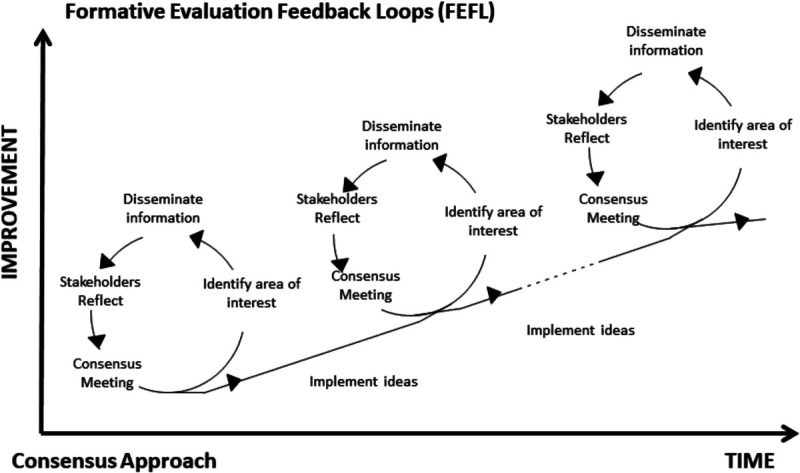
Formative evaluation feedback loops—integrating consensus processes into quality improvement. Adapted from Braithwaite et al.52
Lessons Learned for Resilient Healthcare Research
Lessons learned for resilient healthcare research highlight the value of analyzing research results across phases of research projects and synthesize results from different research methods. We argue that this could increase the value of the current research tradition in resilient healthcare studies, which have been based on single-case studies, often at the sharp end of the healthcare system.7,47,54 Mixed-methods designs are lacking in studies of resilient healthcare, but our study shows the added value of combining interviews, surveys, and consensus methods. Not only does a mixed-methods design support the application of different methods, but it also contributes to the collection of data from healthcare professionals, managers, and next of kin at the micro, meso, and macro levels of the system, as is required to understand how resilience is created and co-created in healthcare.7,55
As mentioned, developing interventions is an area of interest in resilient healthcare research.47,48 Our study has illustrated how the thinking around interventions could be extended. Designing a consensus process that includes several stakeholders may in itself be an intervention and a way to create arenas for reflection, co-creation, and knowledge sharing. Such arenas are vital to establish in addition to an environment that supports psychological safety and a work climate that cultivates resilience in healthcare.56 We suggest further studies to develop and test resilience interventions focusing on supporting reflexive spaces in different healthcare contexts.4
Finally, we argue that creating an opportunity for the participants in the consensus process to reflect on the entire research process has the potential to foster second-order learning processes as depicted in Figure 5.57–59
FIGURE 5.
Modeling methods for second-order learning processes in resilience.
In our study, organizational learning was highlighted as a reason for establishing structures and processes for more systematic next of kin involvement. By bringing the participants together, the consensus process was a way of creating the time and space for taking a step back and considering how the organizations can use the knowledge provided by the entire research process, not only to correct deviant work practices but also to make changes that solve everyday problems and support functional work practices. We believe that there is a potential for additional testing and developing similar research activities in resilient healthcare studies.
CONCLUSIONS
Methods for collaborative learning and co-creation of resilient healthcare with multiple stakeholders in healthcare services are rare.3,22,23 This study demonstrated how a consensus method can be used to create reflexive spaces that support collaborative learning and co-creation of resilient hospital cancer care. The methodology presented could identify potential areas for co-creation in hospitals and improvement efforts (methods, areas) and integrate learning in collaboration with multiple stakeholders in collaborative learning forums. This methodological approach has future implications for clinical practice by leveraging the healthcare system toward more systematic involvement of key stakeholders in resilient healthcare.
Limitations
First, the consensus meeting was conducted as a 1-day meeting. Because of the extensive process, it could benefit from being conducted over 2 days.35 Second, healthcare professionals comprised the largest group of the participants in the meeting, and an increased number of user representatives (patient and next of kin) might have contributed to an even greater understanding of the result of the study.35 Third, there is a possibility that the participants reading and reflection on published articles of the study (step 1, Fig. 1) might have affected their view. However, this is a key step in the modified nominal group technique (Fig. 1) and a way to ensure and use stakeholder involvement in the study.30,35
ACKNOWLEDGMENTS
The authors thank all the stakeholders and the moderators in the consensus meeting for sharing their time, valuable experience, and expert opinions.
Footnotes
The authors disclose no conflict of interest.
Contributor Information
Robyn Clay-Williams, Email: robyn.clay-williams@mq.edu.au.
Siri Wiig, Email: siri.wiig@uis.no.
REFERENCES
- 1.O’Hara JK, Aase K, Waring J. Scaffolding our systems? Patients and families ‘reaching in’ as a source of healthcare resilience. BMJ Qual Saf. 2019;28:3–6. [DOI] [PubMed] [Google Scholar]
- 2.O’Hara JK, Canfield C, Aase K. Patient and family perspectives in resilient healthcare studies: a question of morality or logic? Saf Sci. 2019;120:99–106. [Google Scholar]
- 3.Wiig S Aase K Billett S, et al. Defining the boundaries and operational concepts of resilience in the resilience in healthcare research program. BMC Health Serv Res. 2020;20:330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Wiig S, Aase K, Bal R. Reflexive spaces: leveraging resilience into healthcare regulation and management. J Pat Saf. 2021;17:e1681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bergerod IJ, Braut GS, Wiig S. Resilience from a stakeholder perspective: the role of next of kin in cancer care. J Patient Saf. 2020;16:e205–e210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fylan B Armitage G Naylor D, et al. A qualitative study of patient involvement in medicines management after hospital discharge: an under-recognised source of systems resilience. BMJ Qual Saf. 2018;27:539–546. [DOI] [PubMed] [Google Scholar]
- 7.Berg SH Akerjordet K Ekstedt M, et al. Methodological strategies in resilient health care studies: an integrative review. Saf Sci. 2018;110:300–312. [Google Scholar]
- 8.Hollnagel E, Sujan M, Braithwaite J. Resilient health care—making steady progress. Saf Sci. 2019;120:781–782. [Google Scholar]
- 9.Wears RL, Hollnagel E, Braithwaite J. Resilient Health Care, Volume 2: The Resilience of Everyday Clinical Work. Resilience of everyday clinical work. Farnham: Ashgate Publishing Ltd; 2015. [Google Scholar]
- 10.Wiig S Haraldseid-Driftland C Zachrisen RT, et al. Next of kin involvement in regulatory investigations of adverse events that caused patient death: a process evaluation (part I—the next of kins’ perspective). J Pat Saf. 2021;17:e1713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wiig S Schibevaag L Tvete Zachrisen R, et al. Next of kin involvement in regulatory investigations of adverse events that caused patient death: a process evaluation (part II—the inspectors’ perspective). J Patient Saf. 2021;17:e1707–e1712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Elwyn G Nelson E Hager A, et al. Coproduction: when users define quality. BMJ Qual Saf. 2020;29:711–716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Batalden M Batalden P Margolis P, et al. Coproduction of healthcare service. BMJ Qual Saf. 2016;25:509–517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hollnagel E, Braithwaite J, Wears RL. Resilient health care. In: Ashgate studies in resilience engineering. Farnham, Ashgate; 2013. [Google Scholar]
- 15.Hollnagel E. Safety-II in Practice: Developing the Resilience Potentials. New York: Taylor & Francis; 2017. [Google Scholar]
- 16.Comfort LK, Boin A, Demchak CC, eds. Designing resilience: preparing for extreme events. Pittsburgh, PA: University of Pittsburgh Press; 2010. [Google Scholar]
- 17.Hollnagel E. In: Hollnagel E Pariès J Woods D, et al., eds. Resilience Engineering in Practice A Guidebook.2011To learn or not to learn, that is the question. England: Ashgate Publishing Group, Ltd; 2011:193–198. [Google Scholar]
- 18.Wildavsky A. Searching for Safety. Vol 10. New York: Transaction Publisher Books, 1988. [Google Scholar]
- 19.Billett SR. Securing intersubjectivity through interprofessional workplace learning experiences. J Interprof Care. 2014;28:206–211. [DOI] [PubMed] [Google Scholar]
- 20.Billett S. Learning through health care work: premises, contributions and practices. Med Educ. 2016;50:124–131. [DOI] [PubMed] [Google Scholar]
- 21.Serrat O. Knowledge Solutions: Tools, Methods, and Approaches to Drive Organizational Performance. New York: SpringerOpen; 2017. [Google Scholar]
- 22.Aase K Guise V Billett S, et al. Resilience in healthcare (RiH): a longitudinal research programme protocol. BMJ Open. 2020;10:e038779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Anderson JE Aase K Bal R, et al. Multilevel influences on resilient healthcare in six countries: an international comparative study protocol. BMJ Open. 2020;10:e039158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Clay-Williams R, Hounsgaard J, Hollnagel E. Where the rubber meets the road: using FRAM to align work-as-imagined with work-as-done when implementing clinical guidelines. Implement Sci. 2015;10:125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lawton R Taylor N Clay-Williams R, et al. Positive deviance: a different approach to achieving patient safety. BMJ Qual Saf. 2014;23:880–883. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Donetto S Pierri P Tsianakas V, et al. Experience-based co-design and healthcare improvement: realizing participatory design in the public sector. Des J. 2015;18:227–248. [Google Scholar]
- 27.Fisher KA, Mazor KM. Patient and family complaints in cancer care: what can we learn from the tip of the iceberg? Jt Comm J Qual Patient Saf. 2017;43:495–497. [DOI] [PubMed] [Google Scholar]
- 28.Greene J Farley D Amy C, et al. How patient partners influence quality improvement efforts. Jt Comm J Qual Patient Saf. 2018;44:186–195. [DOI] [PubMed] [Google Scholar]
- 29.Gagliardi AR Berta W Kothari A, et al. Integrated knowledge translation (IKT) in health care: a scoping review. Implement Sci. 2016;11:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bergerød IJ. Quality and Safety of Cancer Care: A Mixed Methods Study of Next of Kin Involvement [dissertation]. Norway: University of Stavanger; 2021. [Google Scholar]
- 31.Bergerod IJ Gilje B Braut GS, et al. Next-of-kin involvement in improving hospital cancer care quality and safety—a qualitative cross-case study as basis for theory development. BMC Health Serv Res. 2018;18:324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bergerød IJ Dalen I Braut GS, et al. Measuring next of kin satisfaction with hospital cancer care: using a mixed-method approach as basis for improving quality and safety. J Adv Nurs. 2020;76:1232–1246. [DOI] [PubMed] [Google Scholar]
- 33.Creswell JW. A Concise Introduction to Mixed Methods Research. Thousand Oaks, CA: SAGE; 2015. [Google Scholar]
- 34.Creswell JW. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. London, United Kingdom: SAGE Publications; 2014. [Google Scholar]
- 35.Bergerød IJ Braut GS Fagerdal B, et al. Developing a next-of-kin involvement guide in cancer care—results from a consensus process. Cancer Nurs. 2020;44:E447–E457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Delbecq AL, Van de Ven AH. A group process model for problem identification and program planning. J Appl Behav Sci. 2016;7:466–492. [Google Scholar]
- 37.Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice. 8th ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2014. [Google Scholar]
- 38.Ringdal GI, Jordhoy MS, Kaasa S. Family satisfaction with end-of-life care for cancer patients in a cluster randomized trial. J Pain Symptom Manage. 2002;24:53–63. [DOI] [PubMed] [Google Scholar]
- 39.Ringdal GI, Jordhoy MS, Kaasa S. Measuring quality of palliative care: psychometric properties of the FAMCARE Scale. Qual Life Res. 2003;12:167–176. [DOI] [PubMed] [Google Scholar]
- 40.Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–112. [DOI] [PubMed] [Google Scholar]
- 41.Bate P, Mendel P, Robert G. Organizing for Quality: The Improvement Journeys of Leading Hospitals in Europe and the United States. Oxford: Radcliffe; 2008. [Google Scholar]
- 42.Cunliffe A. Reflexive dialogical practice in management learning. Manag Learn. 2002;33:35–61. [Google Scholar]
- 43.Gherardi S, Nicolini D. The organizational learning of safety in communities of practice. J Manag Inq. 2000;9:7–18. [Google Scholar]
- 44.Gherardi S, Nicolini D. Practice-based theorizing on learning and knowing in organisations. J Manag Inq. 2000;7:211–223. [Google Scholar]
- 45.Aase I. Interprofessional Teamwork Training for Nursing and Medical Students in Norway [dissertation]. Norway: University of Stavanger; 2016. [Google Scholar]
- 46.Wiig S, Fahlbruch B. Exploring resilience—an introduction. In: Wiig S, Fahlbruch B, eds. Exploring Resilience. Cham: Springer International Publishing; 2019:1–5. [Google Scholar]
- 47.Ellis LA Churruca K Clay-Williams R, et al. Patterns of resilience: a scoping review and bibliometric analysis of resilient health care. Saf Sci. 2019;118:241–257. [Google Scholar]
- 48.Righi AW, Saurin TA, Wachs P. A systematic literature review of resilience engineering: research areas and a research agenda proposal. Reliability Eng Sys Saf. 2015;141:142–152. [Google Scholar]
- 49.Anderson JE Ross AJ Back J, et al. Implementing resilience engineering for healthcare quality improvement using the CARE model: a feasibility study protocol. Pilot Feasibility Stud. 2016;2:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Guise V Aase K Chambers M, et al. Patient and stakeholder involvement in resilient healthcare: an interactive research study protocol. BMJ Open. 2021;11:e049116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Johannessen T Ree E Strømme T, et al. Designing and pilot testing of a leadership intervention to improve quality and safety in nursing homes and home care (the SAFE-LEAD intervention). BMJ Open. 2019;9:e027790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Braithwaite J Westbrook M Nugus P, et al. A four-year, systems-wide intervention promoting interprofessional collaboration. BMC Health Serv Res. 2012;12:99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hillman KM, Chen J, Jones D. Rapid response systems. Med J Aust. 2014;201:519–521. [DOI] [PubMed] [Google Scholar]
- 54.Bergström J, van Winsen R, Henriqson E. On the rationale of resilience in the domain of safety: a literature review. Reliability Eng Sys Saf. 2015;141:131–141. [Google Scholar]
- 55.Kislov R Waterman H Harvey G, et al. Rethinking capacity building for knowledge mobilisation: developing multilevel capabilities in healthcare organisations. Implement Sci. 2014;9:166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Edmondson A. The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth. New Jersey: Wiley; 2019. [Google Scholar]
- 57.Argyris C, Schön DA. Organizational Learning II: Theory, Method, and Practice. Boston, MA: Addison-Wesley Publishing Company; 1996. [Google Scholar]
- 58.Argyris C. Double-loop learning, teaching, and research. Acad Manag Learn Edu. 2002;1:206–218. [Google Scholar]
- 59.Tucker AL, Nembhard IM, Edmondson AC. Implementing new practices: an empirical study of organizational learning in hospital intensive care units. Manag Sci. 2007;53:894–907. [Google Scholar]