

Abstract
Background:
To emphasize treatment speed for time-sensitive conditions, emergency medicine has developed not only the concept of the “golden hour,” but also the “platinum half-hour”. Acute stroke patients treated within the first half-hour of onset have not been previously characterized.
Methods:
In this cohort study, we analyzed patients enrolled in the Field Administration of Stroke Therapy–Magnesium (FAST-MAG) trial, testing paramedic prehospital start of neuroprotective agent ≤2h of onset. The features of all acute cerebral ischemia (ACI), and intracranial hemorrhage (ICH) patients with treatment starting at ≤30m of last known well (LKW) were compared with later-treated patients.
Results:
Among 1680 patients, 203 (12.1%) received study agents within 30 minutes of LKW. Among platinum half-hour patients, median onset-to-treatment time was 28 mins (IQR 25-30), and final diagnoses were: ACI in 71.8% (ischemic stroke 61.5%, TIA 10.3%); ICH in 26.1%; and mimic in 2.5%. Clinical features among platinum half-hour patients were largely similar to later-treated patients, and included age 69 (IQR 57-79), 44.8% women, prehospital Los Angeles Motor Scale median 4 (3-5), and early-post-arrival NIHSS deficit 8 (IQR 3-18). Platinum half-hour ACI patients did have more severe prehospital motor deficits and younger age; platinum half-hour ICH patients had more severe motor deficits, were more often female, and less often of Hispanic ethnicity. Outcomes at 3m in platinum half-hour patients were comparable to later-treated patients and included freedom-from-disability (mRS 0-1) in 35.5%, functional independence (mRS 0-2) in 53.2%, and mortality in 17.7%.
Conclusions:
Prehospital initiation permits treatment start within the platinum half-hour after LKW in a substantial proportion of acute ischemic and hemorrhagic stroke patients, accounting for more than 1 in 10 enrolled in a multicenter trial. Hyperacute platinum half-hour patients were largely similar to later-treated patients and are an attainable target for treatment in prehospital stroke trials.
Graphical Abstract

It is well-known that timely treatment in stroke is essential to improve patient functional outcomes.(1) For acute ischemic stroke, reperfusion therapy with intravenous thrombolysis and with endovascular thrombectomy are both highly time dependent and in preclinical models neuroprotective agents also show a strong time dependency.(2-5) For intracerebral hemorrhage, substantial clinical trial evidence suggests that blood pressure lowering and start of prothrombotic agents are also beneficial in only a short time window and, within this window, the sooner the better for treatment start.(6,7)
Stroke is one of several emergency conditions in which patient outcome is heightened by accelerated treatment initiation; others include trauma, shock, status epilepticus, and cardiac arrest. To emphasize the importance of treatment speed for time-sensitive conditions, Emergency Medicine has developed several rubrics for different treatment time windows. The concept of the “golden hour” - the first 60 minutes after illness onset - is the most well-known,(8-10) but other useful time labels have also been promulgated. The terms “platinum 30 minutes” and “platinum 10 minutes” have been advanced for the most challenging and most beneficial time windows for intervention, when disease processes are least advanced and most reversible.(11-14)
For stroke patients, sparse, but at least some, studies have delineated the clinical characteristics and treatment outcomes of golden hour patients. However, to our knowledge, the frequency, characteristics, and outcomes of platinum 30 minute patients has not been previously well characterized. These patients are generally not captured in studies of patients evaluated and treated in the Emergency Department. Even at the optimal attainable speed, the cumulative time intervals of symptom detection to 911 call (3-7 minutes), dispatcher phone assessment leading to ambulance activation (1-2 minutes), ambulance travel to scene (5-10 minutes), paramedic assessment and stabilization of patient and loading of patient into ambulance (10-20 minutes), ambulance travel from scene to Emergency Department door (5-10 minutes), and initial physician assessment in the ED (0-10 minutes) results in almost all acute stroke patients arriving and assessed in the ED beyond the platinum 30 minutes.(15) Prehospital assessment and treatment is the only practical approach to achieving interventions for stroke patients within the first 30 minutes after onset. Further, given the time needed to perform and review brain imaging, even Mobile Stroke Units are generally not able to achieve treatment times within the first 30 minutes.(16)
In contrast, standard ambulances staffed by paramedics are a widely available resource for potentially delivering stroke therapy in the platinum 30 minutes. However, stroke patients assessed and treated by paramedics with neurovascular-targeted agents in the platinum 30 minutes have not been previously well-delineated. Understanding this population better is essential to the design of future trials focused upon the hyperacute period and to planning for implementation of trial-based treatments in practice. Accordingly, to achieve this objective, we analyzed this population in the NIH Field Administration of Stroke Therapy - Magnesium (FAST-MAG) Phase 3 trial, a large, multicenter randomized trial assessing start of a potentially neuroprotective agent by paramedics in the field prior to hospital arrival.
METHODS
Data Availability
Anonymized data and materials have been made publicly available at the National Institute of Neurological Disorders and Stroke and can be accessed at: www.ninds.nih.gov/Current-Research/Research-Funded-NINDS/Clinical-Research/Archived-Clinical-Research-Datasets
Study design
This cohort study is an exploratory analysis of the Field Administration of Stroke Therapy - Magnesium (FAST-MAG) Trial, a multicenter, randomized, double-blind, placebo-controlled, phase 3 clinical trial which assessed magnesium sulfate initiated in the prehospital setting in acute stroke patients within 2 hours of last known well time (LKWT). The study database was originated and validated by an independent, outcome-blinded data collection and analysis team. The study was performed from January 2005 to March 2013 by a consortium including 40 emergency medical system agencies, 315 ambulances, 60 acute care receiving hospitals in Los Angeles and Orange counties in California. Details of study design and primary trial results have been presented in prior reports.(17-19) The study protocol was approved by the institutional review board at each emergency medical services agency and hospital study site. Enrollment occurred using explicit informed consent obtained via cellphone conversation between patients on the scene or their legally authorized representatives and enrolling physician-investigators off the scene or under exception from informed consent regulations.
At the first encounter in the prehospital setting, paramedics recorded vital signs, the severity of the stroke motor deficit on the Los Angeles Motor Scale (LAMS), level of consciousness on the Glasgow Coma Scale (GCS). After Emergency Department arrival, study coordinators assessed repeated vital sign, LAMS, and GCS assessments and also recorded multidomain neurologic deficits on the National Institute of Health Stroke Scale (NIHSS), demographics, past medical history, and medications taken prior to stroke onset.
The lead efficacy outcome at 3 months was non-disabled status/excellent outcome (modified Rankin Scale score 0-1). Secondary efficacy outcomes were functional independence (mRS score 0-2) and the distribution of global disability across all 7 mRS levels. All-cause mortality (mRS=6) was the lead safety endpoint. All mRS score assessments were performed by physician- and nurse-raters certified in the validated Rankin Focused Assessment method.
Patients were placed in time categories based on the time interval from last known well time (LKWT) to time of initiation of the prehospital study agent. Two analytic approaches were taken. In a granular analysis of time windows, patients were placed in five time categories: 15-30 minutes (platinum group); 31-45 minutes; 46-60 minutes; 61-120 minutes; and over 120 minutes. In a broad analysis of time windows, patients were placed in two categories: 15-30 minutes (platinum group) and greater than 30 minutes. For the platinum group, the lower limit of 15 minutes was used because trial entry criteria required patient deficit to have lasted at least 15 minutes prior to enrollment.
Statistical Analysis
Descriptive statistics were used to characterize demographic, clinical, and outcomes characteristics of the study population. Numbers and percentages were used for binary variables and medians and interquartile ranges for continuous and ordinal variables. For scales with 15 or less levels, means and standard deviations are additionally reported. Three populations of patients were analyzed: 1) acute cerebral ischemia (ACI) patients, consisting of all patients with a final diagnosis of ischemic stroke or transient ischemic attack; 2) intracranial hemorrhage (ICH) patients; and 3) all enrolled patients, including ACI patients, ICH patients, neurovascular mimic patients, and patients unable to be classified combined.
Features distinguishing platinum half hour patients and later-treated patients were analyzed bivariately and using multivariable monitoring. The 17 baseline covariates analyzed were: age, sex, race, Hispanic ethnicity, hypertension, diabetes, hyperlipidemia, atrial fibrillation, prior stroke or transient ischemic attack, tobacco use, alcohol use, motor deficit severity on the prehospital Los Angeles Motor Scale (LAMS), laterality of prehospital LAMS motor weakness, level of consciousness on the Glasgow Coma Scale (GCS), time of day of onset, prehospital SBP, and prehospital DBP. For the prehospital LAMS score, the lead analysis was nonparametric (median, interquartile range, Kruskal Wallis, and Mann Whitney) reflecting its ordinal character. However, as the LAMS scores had only 5 levels, limiting the informativeness of the median value in indicating group differences, for descriptive purposes the LAMS was also analyzed using parametric analysis (mean, standard deviation, ANOVA, and t-test), an approach appropriate for ordinal data in large sample sizes per the Central Limit Theorem.
In the bivariate analyses of platinum half hour patients vs all later-treated patients, Mann Whitney and Chi-squared tests were used to compare patient groups, as appropriate. In the analyses comparing the 5 granular OTT groups (15-30m, 31-45m, 46-60m, 61-120m, >120m), Kruskall Wallis tests were used for continuous outcomes. For dichotomized outcomes, Chi-squared tests were used for binary predictor variables and Fisher Exact Test for categorical predictor variables.
For the multivariable monitoring of features associated with platinum half-hour treatment, the 17 potential predictors were simultaneously assessed using logistic regression, classification tree (recursive partitioning) models and gradient boosting models. The boost analysis was used primarily to find nonlinear relationships and interactions among variables that could be used to refine the logistic model.20 Model accuracy was summarized by the concordance (C) statistic; model performance was considered: excellent, 0.80 to 1.00; good, 0.70 to 0.79; fair, 0.60 to 0.69; and poor, 0.50 to 0.59.21 Model accuracy was also summarized by the sensitivity, specificity, and overall accuracy. 21
The relation of platinum half-hour treatment and treatment in later time epochs with functional outcomes was analyzed bivariately and multivariately, separately for acute cerebral ischemic patients and ICH patients, for 3 month endpoints of freedom-from-disability (mRS 0-1), functional independence (mRS 0-2), and mortality. Multivariate logistic regression modeling incorporated baseline features related bivariately to outcomes with p<0.20 plus platinum half-hour vs later treatment. In addition, onset to treatment time as a continuous variable and the distribution of 3 month modified Rankin Scale outcomes in the acute cerebral ischemia and in the intracranial hemorrhage patients was analyzed using the Spearman correlation coefficient.
Two-tailed significance was considered at P<0.05. Statistical analysis was performed through SPSS, version27 (SPSS Inc)
RESULTS
Among the overall 1700 patients enrolled in the FAST-MAG Trial, 1680 (98.8%) had confirmed valid data for both last known well time and study agent prehospital start time. Final diagnosis among the patients was: acute cerebral ischemia in 1229 [73.15%, including acute ischemic stroke in 1028 (61.2%) and transient ischemic attack in 201 (12.0%)]; intracranial hemorrhage in 385 (22.9%); and neurovascular mimic in 64 (3.81%). Demographic and clinical characteristics of this all-patient population are presented in Supplemental Results Text S1, Supplemental Table S1, and Supplemental Figure S1). Platinum half hour treatment occurred with comparable frequencies among ICH and ACI patients, 13.8% vs 11.7%, RR 1.17 (95%CI 0.88-1.58). Calls to EMS were placed earlier among platinum half-hour than later-treated patients, 5 (IQR 2-6) vs 19 (IQR 10-39), p < 0.001.
Among the 1299 acute cerebral ischemia patients, median age was 73 (IQR, 61-82), 44.5 % were women, and prehospital LAMS was median 4 (IQR 3-5). (Table 1) The interval from last known well to study agent start was median 48 minutes (IQR 36-68.8 minutes). The detailed distribution of onset-to-treatment times is shown in Figure 1A. The characteristics of patients in the binary categories of 1-30 mins and >30 mins and in each of the 5 more granular OTT categories are shown in Table 2. In the bivariate comparison of platinum half-hour treated patients vs later-treated patients, features strongly distinguishing the groups were: age (lower in the platinum 30 minutes patients) and LAMS (more severe motor deficits in the platinum 30 minutes patients).
Table 1.
Descriptive characteristics of platinum half-hour and later -treated acute cerebral ischemia patients
| 15-30m (N=144) |
31-45m (N=424) |
46-60m (N=281) |
61-120m (N=336) |
>120m (N=44) |
P value (comparing 5 groups) |
>30m (N=1085) |
P value comparing 15- 30m & >30m |
|
|---|---|---|---|---|---|---|---|---|
| Age, median (IQ) y | 71(59-80) | 70.5(59-81) | 75(62-83) | 73(62.3-81.8) | 75(65.3-85.8) | 0.01 | 73(61-82) | 0.03 |
| Sex, No. (%) | ||||||||
| Female | 59(41.0) | 182(42.9) | 135(48.0) | 153(45.5) | 24(54.5) | 0.38 | 494(45.5) | 0.34 |
| Race, No. (%) | 0.71 | 0.48 | ||||||
| White | 115(79.9) | 326(76.9) | 221(78.7) | 26(77.4) | 33(75.0) | 840(77.4) | ||
| Black/African American | 19(13.2) | 52(12.3) | 41(14.6) | 51(15.2) | 7(15.9) | 151(13.9) | ||
| Asian | 7(4.9) | 43(10.1) | 18(6.4) | 22(6.6) | 4(9.1) | 87(8.0) | ||
| Other | 2(1.4) | 3(0.7) | 2(0.7) | 3(0.9) | 0(0.0) | 25(2.3) | ||
| Hispanic Ethnicity, No. (%) | 25(17.4) | 78(18.4) | 60(21.4) | 76(22.6) | 9(20.5) | 0.57 | 223(20.6) | 0.39 |
| Medical Hx, No. (%) | ||||||||
| Hypertension | 103(71.5) | 334(78.8) | 216(76.9) | 265(78.9) | 36(81.9) | 0.43 | 851(78.4) | 0.09 |
| Diabetes | 32(22.2) | 80(18.9) | 66(23.5) | 91(27.1) | 14(31.8) | 0.06 | 251(23.1) | 0.84 |
| Hyperlipidemia | 78(54.2) | 201(47.4) | 140(49.8) | 181(53.9) | 22(50.0) | 0.39 | 544(50.1) | 0.32 |
| Atrial Fibrillation | 42(29.2) | 113(26.7) | 85(30.3) | 80(23.9) | 11(25.0) | 0.45 | 289(26.6) | 0.48 |
| Prior Stroke/TIA | 23(16) | 72(17) | 63(22.4) | 54(16.1) | 9(20.5) | 0.27 | 198(18.3) | 0.55 |
| Tobacco use | 18(12.5) | 82(19.3) | 45(16.0) | 60(17.9) | 11(25.0) | 0.23 | 198(18.3) | 0.095 |
| Any alcohol use | 53(36.8) | 171(40.3) | 88(31.3) | 127(37.8) | 16(36.4) | 0.19 | 402(37.1) | 0.99 |
| LKWT, No (%) ** | <0.001 | 0.39 | ||||||
| 0001-0400 | 0(0) | 3(0.7) | 7(2.5) | 7(2.1) | 3(6.8) | 0.01 | 20(1.8) | 0.16 |
| 0401-0800 | 6(4.2) | 15(3.5) | 20(7.1) | 32(9.5) | 9(20.5) | <0.001 | 76(7) | 0.21 |
| 0801-1200 | 40(27.8) | 113(26.7) | 71(25.3) | 94(28.0) | 8(18.2) | 0.66 | 286(26.4) | 0.65 |
| 1201-1600 | 42(29.2) | 114(26.9) | 73(26.0) | 81(24.1) | 6(13.6) | 0.26 | 274(25.3) | 0.27 |
| 1601-20:00 | 31(21.5) | 112(26.4) | 57(20.3) | 67(19.9) | 11(25.0) | 0.19 | 247(22.8) | 0.8 |
| 20:01-24:00 | 23(16.0)) | 66(15.6) | 54(19.2) | 55(16.4) | 7(15.9) | 0.79 | 182(16.8) | 0.86 |
| SBP, median (IQ),mmHg | ||||||||
| Prehospital | 151(136-178) | 154(138-174) | 150(136-176) | 158(140-174) | 152.5(141-177) | 0.44 | 155(138-175) | 0.51 |
| DBP, median (IQ),mmHg | ||||||||
| Prehospital | 89(22) | 89(76-100) | 84(74-96) | 89.5(76-100) | 82(77-95) | 0.058 | 88(76-100) | 0.85 |
| Presenting Stroke Features | ||||||||
| LAMS-Prehospital, median (IQ) | 4(3-5) | 4(3-5) | 4(3-5) | 3(2-5) | 4(2.3-5) | <0.001 | 4(3-5) | 0.007 |
| LAMS-Prehospital, mean (SD) | 4.0(1.2) | 3.8(2) | 3.6(1.3) | 3.4(1.4) | 3.6(2.3) | <0.001 | 3.6(1.3) | 0.003 |
| GCS-Prehospital, median (IQ) | 15(13-15) | 15(13-15) | 15(14-15) | 15(15-15) | 15(14.3-15) | 0.043 | 15(14-15) | 0.24 |
| GCS-Prehospital, mean (SD) | 13.9(2.1) | 13.8(2.2) | 14.1(1.6) | 14.2(1.7) | 14.2(1.6) | 0.05 | 14(1.9) | 0.37 |
| NIHSS-Early Hospital, median (IQ) | 6(2-15) | 9(3-16) | 7(2-15) | 6(2-13) | 8.8(4-14.8) | 0.003 | 7(3-15) | 0.17 |
| NIHSS-Aphasia, No.(%) | 41(28.5) | 131(3.9) | 81(28.8) | 8(23.8) | 15(34.1) | 0.21 | 307(28.3) | 0.79 |
| NIHSS-Neglect, No. (%) | 43(29.9) | 150(35.4) | 85(30.3) | 72(21.4) | 14(31.8) | 0.002 | 321(29.6) | 0.72 |
| Side of weakness | 0.80 | 0.67 | ||||||
| Right | 59(41.0) | 163(38.4) | 115(40.9) | 139(41.4) | 18(40.9) | 435(40.1) | ||
| Left | 82(56.9) | 260(61.3) | 164(58.4) | 193(57.4) | 26(59.1) | 643(59.3) | ||
| Both*** | 2(1.4) | 1(0.2) | 3(1.1) | 4(1.2) | 0(0) | 8(0.7) | ||
| Final Diagnosis, No. (%) | 0.77 | 0.58 | ||||||
| Ischemic Stroke | 123 (85.4) | 356 (84.0) | 234 (83.3) | 276 (82.1) | 39(88.6) | 905(83.4) | ||
| TIA | 21 (14.58) | 68 (16.0) | 47(16.7) | 60 (17.9) | 5(11.4) | 180(16.6) |
Abbreviations: TIA, Transient Ischemic Attack; LKWT, Last Known Well Time; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; LAMS, Los Angeles Motor Scale; GSC, Glasgow Coma Scale; NIHSS, National Institutes of Health Stroke Scale.
Number and proportion of patients with last known well times at different times of 24-hour day, in 4 hours increments.
The uncommon patients with bilateral weakness are shown for descriptive purposes but were not included in the statistical calculation for laterality.
Figure 1.

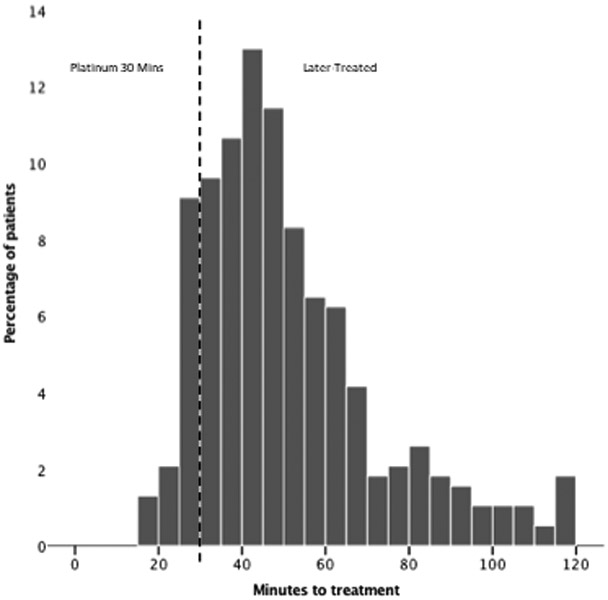
Histogram showing proportions of patients treated in 5 minute intervals from 0-120 minutes. A) Acute cerebral ischemia patients; B) Intracranial hemorrhage patients
Table 2.
Descriptive characteristics of platinum half-hour and later- treated intracranial hemorrhage patients
| 15-30m (N=53) |
31-45m (N=132) |
46-60m (N=96) |
61-120m (N=96) |
>120m (N=8) |
P value (comparing 5 groups) |
>30m (N=332) |
P value (comparing 15-30m& >30m) |
|
|---|---|---|---|---|---|---|---|---|
| Age, median (IQ) y | 66(55.5-74.5) | 63.5 (55-77) | 64(52.3-75) | 66.5 (55-77.8) | 60.5(52.3-77.3) | 0.69 | 64(54-76) | 0.64 |
| Sex, No. (%) | ||||||||
| Female | 28 (52.8) | 37 (28) | 37 (38.5) | 26 (27.1) | 0(0) | 0.001 | 100(30.1) | 0.001 |
| Race, No. (%) | 0.44 | 0.84 | ||||||
| White | 44 (83.0) | 105 (79.6) | 77 (79.4) | 71 (74) | 8(100) | 261(78.6) | ||
| Black/African American | 3 (5.7) | 14 (10.6) | 5 (5.2) | 14(14.6) | 0 | 33(9.9) | ||
| Asian | 5 (9.4) | 12 (8.4) | 13 (13.4) | 8 (8.3) | 0 | 33(9.9) | ||
| Other | 1 (1.9) | 1 (0.8) | 1 (1) | 3 (3.1) | 0 | 5(1.5) | ||
| Hispanic Ethnicity, No. (%) | 11(20.8) | 41(31.1) | 36(37.5) | 35(36.5) | 6(75) | 0.02 | 118(35.5) | 0.03 |
| Medical Hx, No. (%) | ||||||||
| Hypertension | 40 (75.5) | 103 (78) | 75 (78.1) | 81 (84.4) | 4(50) | 0.19 | 263(79.2) | 0.54 |
| Diabetes | 8 (15.1) | 21 (15.9) | 21 (21.9) | 19 (19.8) | 3(37.5) | 0.45 | 64(19.3) | 0.47 |
| Hyperlipidemia | 18 (34.0) | 58 (43.9) | 35(36.5) | 28 (29.2) | 1(13.5) | 0.11 | 122(36.8) | 0.70 |
| Atrial Fibrillation | 4 (7.6) | 10 (7.6) | 7 (7.3) | 9 (9.4) | 0 | 0.98 | 26(7.8) | 0.60 |
| Prior Stroke/TIA | 3 (5.7) | 17 (12.9) | 10 (10.4) | 12 (12.5) | 0 | 0.68 | 39(11.8) | 0.33 |
| Tobacco use | 9(17) | 20(15.2) | 18(18.8) | 17(17.7) | 1(12.5) | 0.96 | 56(16.9) | 0.98 |
| Any alcohol use | 23(43.4) | 53(40.2) | 51(53.1) | 43(44.8) | 2(25) | 0.27 | 149(44.9) | 0.85 |
| LKWT, No (%) ** | 0.44 | 0.55 | ||||||
| 0001-0400 | 1(1.9) | 2(1.5) | 3(3.1) | 4(4.2) | 0(0) | 0.73 | 9(2.7) | 0.59 |
| 0401-0800 | 3(5.7) | 10(7.6) | 15(15.6) | 11(11.5) | 2(25) | 0.12 | 38(11.5) | 0.15 |
| 0801-1200 | 12(22.6) | 34(25.8) | 24(25) | 31(32.3) | 1(12.5) | 0.60 | 90(27.1) | 0.61 |
| 1201-1600 | 11(20.8) | 27(20.5) | 16(16.7) | 19(19.8) | 1(12.5) | 0.94 | 63(19) | 0.85 |
| 1601-20:00 | 19(35.9) | 40(30.3) | 19(19.8) | 21(21.9) | 3(37.5) | 0.11 | 83(25) | 0.13 |
| 20:01-24:00 | 7(13.2) | 18(13.6) | 19(19.8) | 9(9.4) | 1(12.5) | 0.35 | 47(14.2) | 0.52 |
| SBP, median (IQ), mmHg | ||||||||
| Prehospital | 174(154-196) | 178 (160-194) | 177 (160-195) | 172.5 (160-192) | 156.5(142-205) | 0.73 | 176(160-194) | 0.18 |
| DBP, median (IQ), mmHg | ||||||||
| Prehospital | 100(89-111) | 100(86-114) | 100(82-110) | 100(88-110) | 98(85-126) | 0.24 | 100(86-110) | 0.38 |
| Presenting Stroke Features | ||||||||
| LAMS-Prehospital, median (IQ) | 4 (4-5) | 5(3-5) | 4(3-5) | 4 (3-5) | 3(2-3.8) | 0.007 | 4(3-5) | 0.16 |
| LAMS-Prehospital, mean (SD) | 4.41.2 | 4.15(1.2) | 4.1(1.1) | 3.9(1.1) | 2.75(1) | 0.004 | 4.1(1.2) | 0.08 |
| GCS-Prehospital, median (IQ) | 15(15-15) | 15(14-15) | 15(15-15) | 15(15-15) | 15(15-15) | 0.19 | 15(15-15) | 0.36 |
| GCS-Prehospital, mean (SD) | 14.6(1.2) | 14.2(1.6) | 14.3(1.6) | 14.5(1.3) | 14.9(0.4) | 0.20 | 14.3(1.5) | 0.28 |
| NIHSS-Early Hospital, median (IQ) | 15(9.5-24) | 18.5(11-29) | 15(9-26.8) | 16.5(7-25) | 13(11.3-21.8) | 0.66 | 16(9-2) | 0.93 |
| NIHSS-Aphasia, No. (%) | 18(34) | 62(47) | 37(38.5) | 35(36.8) | 5(62.5) | 0.23 | 139(41.9) | 0.28 |
| NIHSS-Neglect, No. (%) | 29(54.7) | 67(51.2) | 50(52.1) | 43(45.3) | 3(37.5) | 0.70 | 163(49.1) | 0.45 |
| Side of weakness | 0.67 | 0.31 | ||||||
| Right | 17(32.1) | 60(45.5) | 34(35.4) | 38(39.6) | 4(50) | 136(41) | ||
| Left | 35(66) | 71(53.8) | 61(63.5) | 58(60.4) | 4(50) | 194(58.4) | ||
| Both*** | 1(1.9) | 1(0.8) | 1(1) | 0(0) | 0(0) | 2(0.6) | ||
| Final Diagnosis, No. (%) | 0.34 | 0.32 | ||||||
| Intracerebral Hemorrhage | 53(100) | 128(97) | 94(97.9) | 96(100) | 8(100) | 326(98.2) | ||
| Intracranial Hemorrhage | 0(0) | 4(3) | 2(2.08) | 0(0) | 0(0) | 6(1.8) |
Abbreviations: TIA, Transient Ischemic Attack; LKWT, Last Known Well Time; SBP, Systolic Blood Pressure; DBP, Diastolic Blood Pressure; LAMS, Los Angeles Motor Scale; GSC, Glasgow Coma Scale; NIHSS, National Institutes of Health Stroke Scale.
Number and proportion of patients with last known well times at different times of 24-hour day, in 4 hours increments.
The uncommon patients with bilateral weakness are shown for descriptive purposes but were not included in the statistical calculation for laterality.
The results of multivariate models to distinguish platinum half hour patients from the later-treated patients among individuals with acute cerebral ischemia are shown in Supplemental Table S2. The multivariate additive logistic regression model incorporating all 17 baseline covariates to distinguish platinum half hour patients showed fair predictive accuracy, with c statistic 0.66. A multivariate additive logistic regression model incorporating just the 7 baseline covariates identified as most predictive in the gradient boost analysis (LAMS, GCS, race, time of day of onset, SBP, and DBP) performed similarly, c statistic 0.65. The classification tree modeling yielded 8 nodes incorporating 7 variables (LAMS, GCS, sex, history of hypertension, atrial fibrillation, alcohol,and DBP). The classification tree model also showed fair predictive performance, with c statistic of 0.63.
Among the 385 patients with ICH, median age was 64 (IQR 55-76), 42.4% were women, and prehospital motor deficit severity on the Los Angeles Motor Scale (LAMS) was median 4 (IQR 3-5). The median time from last known well to study agent start was 47 minutes (IQR 37-62.5). The detailed distribution of onset-to-treatment times is shown in Figure 1B. The characteristics of patients in the binary categories of 1-30 mins and >30 mins and in the five more granular OTT categories are shown in Table 3. In the binary comparison of platinum half-hour patients vs later-treated patients, features distinguishuing the groups were sex (more frequent in the platinum 30 minutes patients) and Hispanic ethnicity (less frequent in the platinum group).
Table 3.
90-day outcomes in platinum half-hour and later-treated groups
| Acute Cerebral Ischemia | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Final 3m Outcome |
15-30m (N=144) |
31-45m (N=424) |
46-60m (N=281) |
61-120m (N=336) |
>120m (N=44) |
P value (comparing 5 groups) |
>30m (N=1085) |
Unadjusted P value comparing 15-30 v 31-120 |
Adjusted P value comparing 15-30 v 31-120 |
| mRS 0-1 (Non Disabled), No. (%) | 61(42.4) | 197(46.5) | 119(42.3) | 155(46.1) | 10(22.7) | 0.03 | 481(44.3) | 0.73 | 0.92 |
| mRS 0-2 (Independent), No. (%) | 89(61.8) | 248(58.5) | 158(56.2) | 199(59.2) | 20(45.5) | 0.27 | 625(57.6) | 0.26 | 0.17 |
| mRS, median (IQ) | 2(0-4) | 2 (0-4) | 2 (0-4) | 2(1-4) | 3(2-4.8) | 0.10 | 2(0-4) | 0.31 | -- |
| mRS, mean (SD) | 2.19(2.1) | 2.33(2.1) | 2.39(2.1) | 2.28(2) | 3.05(1.9) | 0.18 | 2.36(2.1) | 0.37 | -- |
| Mortality, No. (%) | 19(13.2) | 53(12.5) | 37(13.2) | 37(11) | 8(18.2) | 0.72 | 135(12.4) | 0.76 | 0.76 |
| Intracranial Hemorrhage | |||||||||
| Final 3m Outcome |
15-30m (N=53) |
31-45m (N=132) |
46-60m (N=96) |
61-120m (N=96) |
>120m (N=8) |
P value (comparing 5 groups) |
>30m (N=332) |
Unadjusted P value comparing 15-30 v 31-120 |
Adjusted P value comparing 15-30 v 31-120 |
| mRS 0-1 (Non-Disabled), No. (%) | 8(15.1) | 11(8.3) | 9(9.4) | 7(7.3) | 0(0) | 0.48 | 27(8.1) | 0.11 | 0.09 |
| mRS 0-2 (Independent), No. (%) | 15(28.3) | 38(28.8) | 33(34.4) | 24(25) | 4(50) | 0.45 | 99(29.8) | 0.78 | 0.53 |
| mRS, median (IQ) | 5(2-6) | 4(2-6) | 4(2-5) | 4(2-6) | 3(2-5) | 0.57 | 4(2-6) | 0.53 | -- |
| mRS, mean (SD) | 4(1.9) | 3.9(1.8) | 3.7(1.8) | 4(1.7) | 3.4(1.5) | 0.68 | 3.9(1.8) | 0.53 | -- |
| Mortality, No. (%) | 16 (30.2) | 36 (27.3) | 23 (24) | 28 (29.2) | 0(0) | 0.37 | 87(26.2) | 0.58 | 0.89 |
Abbreviations: mRS, modified Rankin Scale.
For ACI, adjustment variables were: age, hypertension, prehospital LAMS, tobacco. For ICH, adjustment variables were: sex, Hispanic ethnicity, systolic blood pressure, prehospital LAMS
The results of multivariate models to distinguish platinum half hour patients among ICH patients are shown in Supplemental Table S2. The multivariate additive logistic regression model incorporating all 17 baseline covariates showed good predictive accuracy, with c statistic 0.72. In this model, sex, race, and ethnicity were statistically significant covariates. The classification tree model yielded 3 nodes incorporating 2 variables (GCS and sex). The classification tree model showed fair predictive performance, with c statistic of 0.63.
The global disability outcomes on the mRS at 90 days in the platinum half hour and later treated patients, for acute cerebral ischemia patients and for intracranial hemorrhage patients, are shown in Table 3 and Figure 2. (The mRS outcomes for the all-patient population are shown in Supplemental Table S3 and Supplemental Figure S2.) In all populations, global disability outcomes at 3 months were similar in platinum half hour and in later-treated patients in both bivariate and multivariate analysis.. Among the ACI patients, the overall correlation between OTT and 90d mRS was r = −0.06; among the ICH patients, r = 0.01.
Figure 2.
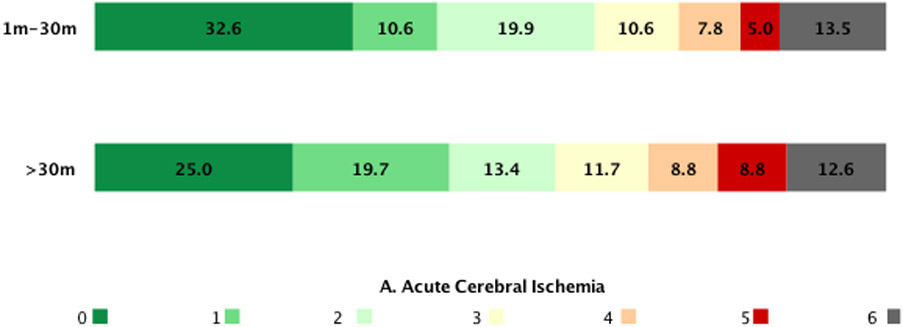
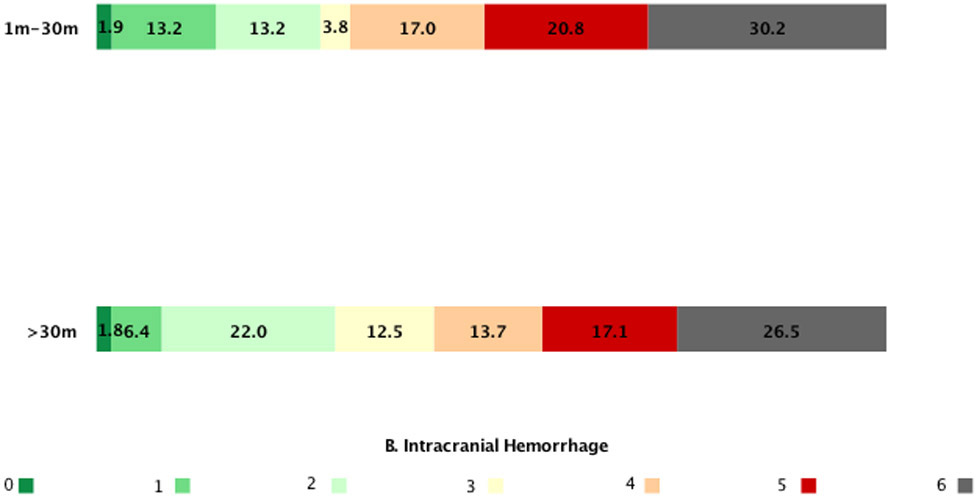
Global disability mRS outcome distributions at 90 days in platinum half-hour and later-treated patients. A) Acute cerebral ischemia patients; B) Intracranial hemorrhage patients
DISCUSSION
This study finds that, with a strategy of prehospital initiation in a large multicenter trial, platinum half hour start of a potential neuroprotective agent was able to be achieved in a substantial proportion of acute ischemic and hemorrhagic stroke patients, accounting for more than 1 in 10 patients of all enrolled patients. Among patients with acute cerebral ischemia, the strongest determinants of platinum half hour treatment status were more severe motor deficits on first prehospital assessment and younger age. Among intracranial hemorrhage patients, the strongest associations with platinum half hour status were female sex, not being of Hispanic ethnicity, and more severe motor deficits prehospital. Global disability outcomes at 3 months on the modified Rankin Scale were similar among patients with onset to treatment times within versus beyond the platinum half hour.
These patient features associated with platinum half hour status are biologically and clinically plausible. The association of more severe motor deficits with platinum half hour treatment in both acute cerebral ischemic and hemorrhagic stroke patients indicates that speed of call to the EMS system by patients or on-scene witnesses is driven in part by deficit severity. The stronger association of deficit severity with platinum half hour presentation for acute cerebral ischemia patients than intracranial hemorrhage patients likely reflects that early EMS contact in hemorrhage patients is also driven by discomforting symptoms of headache and nausea. Among acute cerebral ischemia patients, the association of younger age with platinum half hour treatment may reflect greater social engagement (more opportunity for witnesses to observe onset) and less baseline cognitive disturbance and pre-existing disability interfering with patient symptom recognition. Among intracerebral hemorrhage patients, the association of female sex with increased platinum half hour treatment is speculative but may reflect earlier onset of headache in ICH patients with a background disposition to migraine, with headache prompting earlier EMS contact. The association of Hispanic ethnicity with reduced platinum half-hour treatment may reflect lack of awareness of cerebrovascular disease and the need to activate the EMS system, hesitancy to incur healthcare costs by activating EMS, and language communication barriers. 22,23
However, the variables associated with platinum half hour status among acute cerebral ischemia patients had only modest determinative value, with multivariable model predictive performance only in the fair range. These results indicate that platinum half hour acute cerebral ischemia patients are broadly similar in demographic and clinical variables to later presenting patients, even though they almost certainly differ in having more favorable penumbral profiles.24,25 This finding suggests that treatments found beneficial in platinum half hour patients are likely also to be of benefit for later-presenting patients harboring salvageable tissue, rather than being limited by distinctive demographic and clinical patient features. In contrast, the variables associated with platinum half hour status among intracranial hemorrhage patients showed good multivariate determinative value. As Hispanic ethnicity was an important factor in late presentation, this finding highlights the need to address ongoing disparities in early access to the medical system.
It is noteworthy that 3 month outcomes did not differ among platinum half-hour patients and later-treated patients. This result indicates that platinum half-hour presentation, compared with slightly later presentation, has only limited prognostic value regarding final outcome. However, once a beneficial therapy able to be started in ambulances becomes available, platinum half hour treatment is likely to be associated with maximal intervention benefit. Platinum half hour status would then be a biomarker that is predictive but not prognostic.26
This study has limitations. Our analysis included only those patients who were enrolled in a clinical trial. Though the trial entry criteria were broad in age, stroke severity, and comorbidities,(17) the study did exclude patients with uncommon features such as prestroke disability and systolic blood pressure higher than 220 mm Hg. Such patients may have different frequencies of platinum-half hour presentation. Early vessel imaging after hospital arrival was not obtained routinely in studied patients, so the effect of presence or absence of large vessel occlusion upon platinum-half hour presentation in acute cerebral ischemic could not be explored. While initial brain imaging was obtained in all \patients, follow-up imaging was not mandated and varied in timing and components with local practice. As a result, the study did not address the frequencies of postarrival infarct growth or hematoma expansion in platinum half-hour compared with later-treated patients.
CONCLUSION
Paramedic prehospital initiation of neuroprotection study agent permits treatment start within the platinum first 30 minutes in a substantial proportion of acute ischemic and hemorrhagic stroke patients, accounting for more than 1 in 10 patients enrolled in a multicenter trial. Hyperacute platinum half hour patients were largely similar to later-treated patients and are an attainable target for treatment in prehospital stroke trials.
Supplementary Material
Funding:
The FAST-MAG Trial was supported by a grant from NIH-NINDS.
NON-STANDARD ABBREVIATIONS AND ACRONYMS
- ACI
Acute cerebral ischemia
- DBP
Diastolic blood pressure
- FAST-MAG
Field Administration of Stroke Therapy–Magnesium
- GCS
Glasgow Coma Scale
- ICH
Intracranial hemorrhage
- LAMS
Los Angeles Motor Scale
- LKW
Last Known well time
- mRS
modified Rankin Scale
- NIHSS
NIH Stroke Scale
- OTT
Onset to treatment
- SBP
Systolic blood pressure
Footnotes
Disclosures:
JLS: Outside the submitted work: Contracted hourly payments for services on clinical trial steering committees, advising on rigorous study design and conduct, from Cerenovus, Medtronic, BrainsGate, BrainQ. Contracted stock options for service on clinical trial steering committees, advising on rigorous study design and conduct, from Rapid Medical.
DSL: Outside the submitted work: Genentech, Cerenovus, Medtronic, Stryker
ASR, FPV, SStar, NS, GA, SStra, JG, LS, LRJ, MVS, MJT, PV, RC, SH: None
REFERENCES
- 1.Saver JL. Time is brain—quantified. Stroke. 2006;37:263–266. [DOI] [PubMed] [Google Scholar]
- 2.Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, Brott T, Cohen G, Davis S, Donnan G, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. The Lancet. 2014;384:929–935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Saver JL, Fonarow GC, Smith EE, Reeves MJ, Grau-Sepulveda MV, Pan W, Olson DM, Hernandez AF, Peterson ED, Schwamm LH. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. Jama. 2013;309:480–488. [DOI] [PubMed] [Google Scholar]
- 4.Saver JL, Goyal M, Van der Lugt AA, Menon BK, Majoie CB, Dippel DW, Campbell BC, Nogueira RG, Demchuk AM, Tomasello A, et al. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. Jama. 2016;316:279–289. [DOI] [PubMed] [Google Scholar]
- 5.Jahan R, Saver JL, Schwamm LH, Fonarow GC, Liang L, Matsouaka RA, Xian Y, Holmes DN, Peterson ED, Yavagal D, et al. Association between time to treatment with endovascular reperfusion therapy and outcomes in patients with acute ischemic stroke treated in clinical practice. Jama. 2019;322:252–263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Carcel C, Wang X, Sato S, Stapf C, Sandset EC, Delcourt C, Arima H, Robinson T, Lavados P, Chalmers J, et al. Degree and timing of intensive blood pressure lowering on hematoma growth in intracerebral hemorrhage: intensive blood pressure reduction in acute cerebral hemorrhage trial-2 results. Stroke. 2016;47:651–653. [DOI] [PubMed] [Google Scholar]
- 7.Mayer SA, Davis SM, Skolnick BE, Brun NC, Begtrup K, Broderick JP, Diringer MN, Steiner T. Can a subset of intracerebral hemorrhage patients benefit from hemostatic therapy with recombinant activated factor VII?. Stroke. 2009;40:833–840. [DOI] [PubMed] [Google Scholar]
- 8.Wyen H, Lefering R, Maegele M, Brockamp T, Wafaisade A, Wutzler S, Walcher F, Marzi I, TraumaRegister DGU. The golden hour of shock–how time is running out: prehospital time intervals in Germany—a multivariate analysis of 15, 103 patients from the TraumaRegister DGU®. Emergency Medicine Journal. 2013;30:048–055 [DOI] [PubMed] [Google Scholar]
- 9.Nasr A, Saavedra Tomasich F, Collaço I, Abreu P, Namias N, Marttos AC (eds). The Trauma Golden hour: A Practical Guide. Springer; 2020. [Google Scholar]
- 10.Kim JT, Fonarow GC, Smith EE, Reeves MJ, Navalkele DD, Grotta JC, Grau-Sepulveda MV, Hernandez AF, Peterson ED, Schwamm LH, et al. Treatment with tissue plasminogen activator in the golden hour and the shape of the 4.5-hour time-benefit curve in the National United States Get With The Guidelines-Stroke Population. Circulation. 2017;135:128–139. [DOI] [PubMed] [Google Scholar]
- 11.Volpi NM. Motor vehicle collisions and the GOLDEN Hour, Platinum 10. EMS1. https://www.ems1.com/vehicle-crashes/articles/motor-vehicle-collisions-and-the-golden-hour-platinum-10-38qe0oGsT0GS98Xt/. November 14, 2018. Accessed August 4, 2021.
- 12.Daban JL, Falzone E, Boutonnet M, Peigne V, Lenoir B. Wounded in action: the platinum ten minutes and the golden hour. Soins; la revue de référence infirmière. 2014. Sep 1:14–15. [PubMed] [Google Scholar]
- 13.Galvin B Children's healthcare's new medical helicopter a "flying icu". FOX 5 Atlanta.https://www.fox5atlanta.com/news/childrens-healthcares-new-medical-helicopter-a-flying-icu. August 31, 2016. Accessed August 4, 2021 [Google Scholar]
- 14.Preston C Richie pediatric trauma center - one year later. EMERGIPRESS. 2012; 17:2. [Google Scholar]
- 15.Acker JE III, Pancioli AM, Crocco TJ, Eckstein MK, Jauch EC, Larrabee H, Meltzer NM, Mergendahl WC, Munn JW, Prentiss SM, et al. Implementation strategies for emergency medical services within stroke systems of care: a policy statement from the American Heart Association/American Stroke Association Expert Panel on Emergency Medical Services Systems and the Stroke Council. Stroke. 2007;38:097–115. [DOI] [PubMed] [Google Scholar]
- 16.Ebinger M, Kunz A, Wendt M, Rozanski M, Winter B, Waldschmidt C, Weber J, Villringer K, Fiebach JB, Audebert HJ. Effects of golden hour thrombolysis: a Prehospital Acute Neurological Treatment and Optimization of Medical Care in Stroke (PHANTOM-S) substudy. JAMA neurology. 2015;72:25–30. [DOI] [PubMed] [Google Scholar]
- 17.Saver JL, Starkman S, Eckstein M, Stratton SJ, Pratt FD, Hamilton S, Conwit R, Liebeskind DS, Sung G, Kramer I, et al. Prehospital use of magnesium sulfate as neuroprotection in acute stroke. New England Journal of Medicine. 2015;372:528–536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Saver JL, Starkman S, Eckstein M, Stratton S, Pratt F, Hamilton S, Conwit R, Liebeskind DS, Sung G, Sanossian N, FAST-MAG Investigators and Coordinators. Methodology of the field administration of stroke therapy–magnesium (FAST-MAG) phase 3 trial: Part 1–rationale and general methods. International Journal of Stroke. 2014;9:215–219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Saver JL, Starkman S, Eckstein M, Stratton S, Pratt F, Hamilton S, Conwit R, Liebeskind DS, Sung G, Sanossian N, FAST-MAG Investigators and Coordinators. Methodology of the Field Administration of Stroke Therapy–Magnesium (FAST-MAG) phase 3 trial: part 2–prehospital study methods. International Journal of Stroke. 2014;9:220–225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hastie T, Tibshirani R, Firedman J The Elements of Statistical Learning. Springer; 2021. [Google Scholar]
- 21.Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. Journal of Thoracic Oncology. 2010;5:315–316. [DOI] [PubMed] [Google Scholar]
- 22.Levine DA, Duncan PW, Nguyen-Huynh MN, Ogedegbe OG. Interventions targeting racial/ethnic disparities in stroke prevention and treatment. Stroke. 2020;51:425–432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Seo M, Begley C, Langabeer JR, DelliFraine JL. Barriers and disparities in emergency medical services 911 calls for stroke symptoms in the United States adult population: 2009 BRFSS Survey. Western Journal of Emergency Medicine. 2014;15:251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Campbell BC, Majoie CB, Albers GW, Menon BK, Yassi N, Sharma G, Van Zwam WH, Van Oostenbrugge RJ, Demchuk AM, Guillemin F, White P. Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: a meta-analysis of individual patient-level data. The Lancet Neurology. 2019;18:46–55. [DOI] [PubMed] [Google Scholar]
- 25.Seo WK, Liebeskind DS, Yoo B, Sharma L, Jahan R, Duckwiler G, Tateshima S, Nour M, Szeder V, Colby G, Starkman S. Predictors and functional outcomes of fast, intermediate, and slow progression among patients with acute ischemic stroke. Stroke. 2020;51:553–557. [DOI] [PubMed] [Google Scholar]
- 26.Sechidis K, Papangelou K, Metcalfe PD, Svensson D, Weatherall J, Brown G. Distinguishing prognostic and predictive biomarkers: an information theoretic approach. Bioinformatics. 2018;34:365–376. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Anonymized data and materials have been made publicly available at the National Institute of Neurological Disorders and Stroke and can be accessed at: www.ninds.nih.gov/Current-Research/Research-Funded-NINDS/Clinical-Research/Archived-Clinical-Research-Datasets