

Abstract
Kyphoplasty is a well-established method to treat symptomatic vertebral compression fractures. Reported local cement leakage rates are high, but clinically relevant leakages are rare. A fatal complication is the extravasation of cement to the venous system with cardiopulmonary manifestation. We report a case with right ventricular perforation caused by leaked cement fragments. (Level of Difficulty: Beginner.)
Key Words: cardiac perforation, cement leakage, embolism, kyphoplasty
Abbreviations and Acronyms: CT, computed tomography; PCE, pulmonary cement embolism
Central Illustration

Next to percutaneous vertebroplasty, kyphoplasty is a well-established, minimally invasive method to treat symptomatic vertebral compression fractures. In kyphoplasty, percutaneous bone cement, like polymethylmethacrylate, is inserted into the cancellous bone of the affected vertebral body. Treatment aims are pain relief and prevention of further loss of vertebral body height. Impaired viscosity of the cement, meaning low viscosity of polymethylmethacrylate, or high pressure of injection are related to cement leakages.1 The rate of local leakage of bone cement is high,2 but symptomatic leakage of cement after kyphoplasty is rarely reported. A rare but feared complication is the leakage of cement in the spinal canal or the venous system. The extravasation of cement into the spinal canal can cause neurologic damage, including paraplegia; symptomatic pulmonary emboli can occur if cement enters the venous system. A cardiopulmonary manifestation of the cement embolus can lead to a life-threatening course.
Learning Objectives
-
•
To emphasize the risk of delayed clinical manifestations of cardiac and pulmonary cement leakage after kyphoplasty.
-
•
To recommend routine thoracic imaging after kyphoplasty to prevent serious delayed cardiopulmonary failures.
History of Presentation
An 83-year-old woman who underwent kyphoplasty for T12 and L2 fractures 2 months earlier was admitted to the emergency department with increasing dyspnea on exertion. The patient’s examination revealed signs of a survived deep venous thrombosis. Upon discharge, 3 weeks before her readmission, a chest x-ray film showed signs of a radiopaque disseminated reticular proliferation, leading to high suspicion of cement leakage after kyphoplasty (Figure 1).
Figure 1.

First Chest X-Ray After Operation With Multiple Pulmonary Emboli of Bone Cement
The red arrows show pulmonary emboli of bone cement.
Past Medical History
Apart from the kyphoplasty that had taken place 2 months before and the survived venous thrombosis, there were no previous illnesses.
Differential Diagnosis
The differential diagnosis included pulmonary embolism, pneumonia, and heart failure.
Investigations
A thoracic computed tomography (CT) scan was performed, as was transthoracic echocardiography (Figures 2, 3, 4, 5, and 6), which revealed an elongated mass in the right atrium and right ventricle with suspected perforation of the right heart’s apex (10 mm above the myocardial wall) (Figures 2, 3, 4, 5, and 6, Videos 1, 2, and 3). Furthermore, the CT scan showed a peripheral pulmonary embolism.
Figure 2.

Chest Computed Tomography Scan (Sagittal Plane) Showing Polymethylmethacrylate Fragment Penetrating the Heart's Apex
The red arrow shows the polymethylmethacrylate fragment.
Figure 3.

Chest Computed Tomography Scan (Transverse Plane) Showing Polymethylmethacrylate Fragment Penetrating the Heart's Apex
The red arrow shows the polymethylmethacrylate fragment.
Figure 4.

Chest Computed Tomography Scan (Transverse Plane) Showing Polymethylmethacrylate Fragment Crossing the Right Ventricle and Atrium
The red arrow shows the polymethylmethacrylate fragment.
Figure 5.
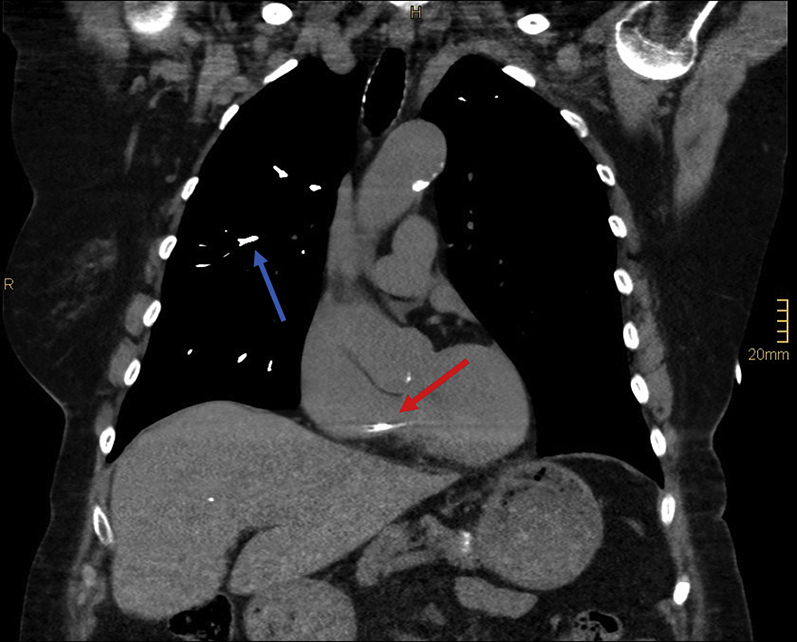
Chest Computed Tomography Scan (Coronal Plane) Showing Polymethylmethacrylate Fragment in the Right Heart and Multiple Pulmonary Emboli of Bone Cement
The red arrow shows the polymethacrylate fragment and the blue arrow shows multiple pulmonary emboli of bone cement.
Figure 6.

Echocardiogram of the Right Ventricle Showing a Hyperechogenic Polymethylmethacrylate Fragment
Thered arrow shows the cement fragment.
Management
The patient remained under stable hemodynamics. Because of the high risk of hemopericardium with pericardial tamponade and the possibility of injuring the tricuspid and pulmonary valves with the cement spike and carryover of the cement material into the pulmonary arteries, a transfer to our department of cardiothoracic surgery was realized, and an operation was performed.
Consequently, operative cement resection was done using full median sternotomy. After full heparinization, venous cannulation for the heart-lung machine was achieved by cannulation of the superior and inferior vena cava and arterial cannulation of the ascending aorta. Subsequent to cross-clamping, cardioplegic arrest was induced by using Buckberg’s solution.
After opening of the right atrium, an 8.5-cm-long and 2-mm-thick cement-like foreign body with loose contact to the tricuspid valve was exposed. It was removed entirely from the right atrium and chamber in 2 pieces (Figures 7, 8, and 9). Also, surgical closing of the right ventricle was performed with 4-0 Teflon-felt sutures (Serapren, Serag Wiessner). The bypass time was 42 minutes, with a cross-clamp time of 19 minutes. Following surgery, the patient was transferred to the intensive care unit, her hemodynamics remained stable, and she was weaned from the respirator on the same day. The further course was without any complications. Because of the increased thromboembolic risk after cardiopulmonary cement embolism and the overcome deep vein thrombosis, an anticoagulation with rivaroxaban 15 mg once daily was initiated. The patient was discharged 2 weeks after surgery.
Figure 7.

Polymethylmethacrylate Fragment Penetrating the Heart's Apex of the Right Ventricle
The red arrow shows the right ventricle.
Figure 8.

Cement Fragment From the Opened Right Atrium
The red arrow shows the cement fragment.
Figure 9.

Polymethylmethacrylate Fragment 8.5 cm in Length Removed From the Right Ventricular Cavity
Discussion
In this case, a cardiopulmonary manifestation of cement leakage occurred 2 months after kyphoplasty. The reported incidence of pulmonary cement embolism (PCE) ranges widely, from 2.1% to 26% for percutaneous vertebroplasty or kyphoplasty.3 Eck et al4 describe a prevalence of symptomatic cement embolism in 3 of 963 (0.3%) for kyphoplasty. Cardiopulmonary findings of cement are a rarely reported complication of this commonly used surgical procedure. By performing follow-up CT scans after kyphoplasty, the incidence of asymptomatic cement leakages was increased. There might be a higher incidence than what is currently reported in the literature. CT scans are not routinely performed after kyphoplasty.1 Therefore, the clinical significance of cardiopulmonary microemboli might be underestimated.2 However, there is no significant impact on all-cause mortality if PCE is found incidentally.5 Because of the possibility of a life-threatening course, a more accurate exclusion of cement leakage—for example, by chest x-ray film or thoracic CT scan—should be considered after kyphoplasty. In the case of a peripheral and asymptomatic PCE, a wait-and-see strategy with renewed control is recommended. For peripheral symptomatic or central asymptomatic PCEs, anticoagulation should be established because of the high thromboembolic risk. In the case of symptomatic and central PCE or possible cardiac involvement, a surgical embolectomy with postoperative anticoagulation should be performed.1
Follow-Up
The 1-year follow-up was performed at the referring hospital. The patient had no cardiopulmonary complaints. In the further course, the patient was lost to follow-up.
Conclusions
This case emphasizes the risk of delayed clinical manifestations of cardiac and pulmonary cement leakage after kyphoplasty and the need for cardiac surgery to prevent a life-threatening course. Suggesting that the risk of such an embolism might be underestimated, we propose routine thoracic imaging after kyphoplasty to prevent serious delayed cardiopulmonary failures.
Footnotes
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the Author Center.
Appendix
For supplemental videos, please see the online version of this paper.
Appendix
Transthoracic Echocardiography Modified 4-Chamber View: Elongated Mass in the Right Atrium and Right Ventricle
Transthoracic Echocardiography Modified 4-Chamber View: Elongated Mass in the Right Atrium and Right Ventricle
Transthoracic Echocardiography Modified 2-Chamber View—Right Ventricle: Elongated Mass in the Right Atrium and Right Ventricle
References
- 1.Krueger A., Bliemel C., Zettl R., Ruchholtz S. Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: a systematic review of the literature. Eur Spine J. 2009;18(9):1257–1265. doi: 10.1007/s00586-009-1073-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lee I.J., Choi A.L., Yie M.-Y., et al. CT evaluation of local leakage of bone cement after percutaneous kyphoplasty and vertebroplasty. Acta Radiol. 2010;51(6):649–654. doi: 10.3109/02841851003620366. [DOI] [PubMed] [Google Scholar]
- 3.Wang L-j, Yang H-l, Shi Y.-X., Jiang W.-M., Chen L. Pulmonary cement embolism associated with percutaneous vertebroplasty or kyphoplasty: a systematic review. Orthop Surg. 2012;4(3):182–189. doi: 10.1111/j.1757-7861.2012.00193.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Eck J.C., Nachtigall D., Humphreys S.C., Hodges S.D. Comparison of vertebroplasty and balloon kyphoplasty for treatment of vertebral compression fractures: a meta-analysis of the literature. Spine J. 2008;8(3):488–497. doi: 10.1016/j.spinee.2007.04.004. [DOI] [PubMed] [Google Scholar]
- 5.Kang H.-R., Kim T.-H., Chung C.-K., Lee C.-H. The impact of incidental pulmonary cement embolism on mortality risk. J Thromb Thrombolysis. 2020;49(3):468–474. doi: 10.1007/s11239-019-02027-0. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Transthoracic Echocardiography Modified 4-Chamber View: Elongated Mass in the Right Atrium and Right Ventricle
Transthoracic Echocardiography Modified 4-Chamber View: Elongated Mass in the Right Atrium and Right Ventricle
Transthoracic Echocardiography Modified 2-Chamber View—Right Ventricle: Elongated Mass in the Right Atrium and Right Ventricle