

Abstract
Background
During the COVID-19 pandemic, several home monitoring programs have described the success of reducing hospital admissions, but only a few studies have investigated the experiences of patients and health care professionals.
Objective
The objective of our study was to determine patients’ and health care professionals’ experiences and satisfaction with employing the COVID-box.
Methods
In this single-center, retrospective, observational study, patients and health care professionals were asked to anonymously fill out multiple-choice questionnaires with questions on a 5-point or 10-point Likert scale. The themes addressed by patients were the sense of reassurance and safety, experiences with teleconsultations, their appreciation for staying at home, and the instructions for using the COVID-box. The themes addressed by health care professionals who treated patients with the COVID-box were the characteristics of the COVID-box, the technical support service and general satisfaction, and their expectations and support for this telemonitoring concept. Scores were interpreted as insufficient (≤2 or ≤5, respectively), sufficient (3 or 6-7, respectively), or good (≥4 or ≥8, respectively) on a 5-point or 10-point Likert scale.
Results
A total of 117 patients and 25 health care professionals filled out the questionnaires. The median score was 4 (IQR 4-5) for the sense of safety, the appreciation for staying at home, and experiences with teleconsultations, with good scores from 76.5% (88/115), 86% (56/65), and 83.6% (92/110) of the patients, respectively. Further, 74.4% (87/117) of the patients scored the home monitoring program with a score of ≥8. Health care professionals scored the COVID-box with a minimum median score of 7 (IQR 7-10) on a 10-point scale for all domains (ie, the characteristics of the COVID-box and the technical support service and general satisfaction). For the sense of safety, user-friendliness, and additional value of the COVID-box, the median scores were 8 (IQR 8-10), 8 (IQR 7-9), and 10 (IQR 8-10), respectively, with good scores from 86% (19/22), 75% (15/20), and 96% (24/25) of the health care professionals, respectively. All health care professionals (25/25, 100%) gave a score of ≥8 for supporting this home monitoring concept, with a median score of 10 (IQR 10-10).
Conclusions
The positive experiences and satisfaction of involved users are key factors for the successful implementation of a novel eHealth solution. In our study, patients, as well as health care professionals, were highly satisfied with the use of the home monitoring program—the COVID-box project. Remote home monitoring may be an effective approach in cases of increased demand for hospital care and high pressure on health care systems.
Keywords: COVID-19, digital health, eHealth, telemedicine, telemonitoring, hospital admission, health care professional, thematic analysis, user satisfaction, usability, home monitoring, health care system
Introduction
The COVID-19 pandemic resulted in an increased demand for hospital care. To keep up with this surging demand, home monitoring was implemented in many countries to avoid unnecessary hospital admissions and detect clinical deterioration in patients at an earlier stage to allow for timely admission and readmission [1].
At the Leiden University Medical Center (LUMC), the Netherlands, we developed the COVID-box project, which is a home monitoring program for patients with (suspected) COVID-19. After a hospital or emergency department visit, patients with (suspected) COVID-19 receive Bluetooth-connected devices (blood pressure monitor, pulse oximeter, and thermometer) and instructions for monitoring their vital parameters 3 times per day, combined with daily teleconsultations carried out by a health care professional. Once the patients get home, the COVID-box team calls the patients to help with the installation of devices and answer questions. The COVID-box team is reachable during office hours for solving logistics issues and answering questions from patients and health care professionals. A detailed description of the telemonitoring program was published previously [2].
The implementation of several home monitoring programs has resulted in a reduction in hospital admissions by allowing for the safe survey of clinical symptoms and vitals [3-9]. Although many observational studies have studied the effectiveness of home monitoring, few studies have reported on patients’ and doctors’ experiences with telemonitoring [5,10-13]. We focused on the COVID-box experiences of patients and health care professionals.
Methods
Ethics Approval
Central ethical approval was obtained for this study from the medical ethics committee of the LUMC.
Study Design
This retrospective observational study was conducted as part of the COVID-box project, which was initiated at the LUMC in May 2020 upon the first wave of the pandemic. A detailed operational description of the COVID-box project was previously reported [2]. In this study, we evaluated patients with COVID-19 and their experiences with telemonitoring by surveying patients after the completion of the telemonitoring phase and full recovery. Patients were asked to anonymously fill out questionnaires regarding the sense of reassurance and safety, experiences with teleconsultations, their appreciation for staying at home, and the instructions for the COVID-box. Health care professionals who treated patients with the COVID-box were given separate questionnaires regarding the characteristics of the COVID-box, the technical support service and general satisfaction (estimated patient satisfaction), and their expectations and support for this telemonitoring concept. All questions were multiple-choice questions on a 5-point or 10-point Likert scale. For this study, scores were interpreted as follows: on a 5-point Likert scale, scores of ≤2 were insufficient scores, scores of 3 were sufficient scores, and scores of ≥5 were good scores; on a 10-point scale, scores of ≤5 were marked as insufficient, scores of 6 to 7 were marked as sufficient, and scores of ≥8 were marked as good. Unvalidated questionnaires were developed by members of the Department of the Directorate of Quality and Patient Safety and clinicians from the Department of Internal Medicine. The questionnaires were web-based and anonymous.
Statistics
Descriptive statistics were used to summarize the results. The scores given by patients and health care professionals are presented as medians with IQRs, and the number of patients and health care professionals are presented as absolute numbers and percentages. We used IBM SPSS Statistics Version 25 (IBM Corporation).
Results
Patients
Of the first 300 patients who were monitored in the COVID-box project from June 2020 to March 2021, a total of 117 (39%) responded to a web-based survey (Multimedia Appendix 1). All of these patients underwent actual telemonitoring with at least 1 contact with a health care professional by using the COVID-box as a home monitoring tool. The results are summarized in Figure 1.
Figure 1.
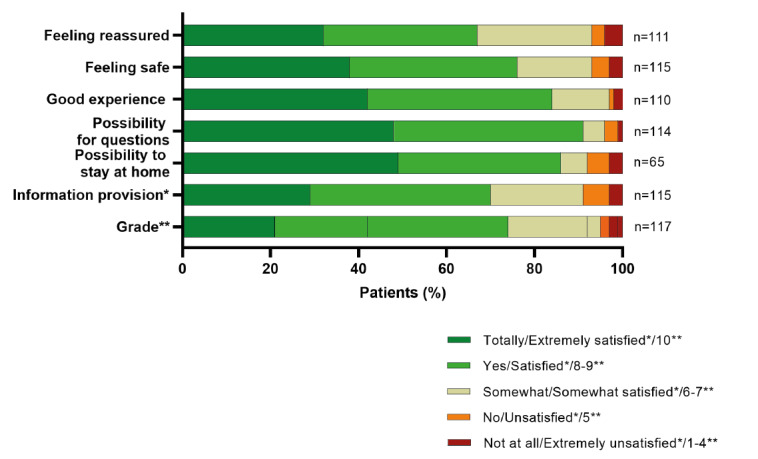
Patients' valuation. *"Information provision" ratings; **"Grade" ratings.
The median score for the sense of reassurance and for the instructions of the COVID-box was 4 (IQR 3-5), with good scores from 67.6% (75/111) and 70% (80/115) of patients, respectively. For the sense of safety, experiences with teleconsultations, the appreciation for staying at home, and the ability to ask questions about the disease and disease course, the median score was 4 (IQR 4-5); good scores were given by 76.5% (88/115), 83.6% (92/110), 86% (56/65), and 91.2% (104/114) of patients, respectively. Overall, 74.4% (87/117) of patients scored the home monitoring program with the COVID-box as good, with a score of 8 or higher.
Health Care Professionals
Overview
Of the 60 health care professionals approached, 25 (42%) filled out the questionnaire (Multimedia Appendix 2). Of these, 6 (24%) were specialists who worked at the emergency department, 5 (20%) were specialists from the Department of Internal Medicine (20%), 12 (48%) were residents, and 2 (8%) were nurse practitioners. The results are summarized in Figure 2.
Figure 2.
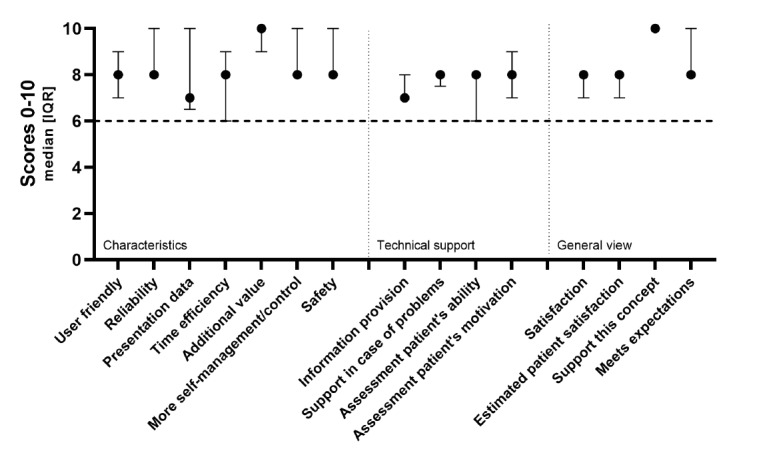
Health care professionals' valuation.
Characteristics of the COVID-box
The median score for the sense of safety, reliability, and more self-management/control in patients was 8 (IQR 8-10), with good scores from 86% (19/22), 89% (8/9), and 92% (22/24) of health care professionals, respectively. For user-friendliness, data presentation, and time efficiency, the median scores were 8 (IQR 7-9), 7 (IQR 7-10), and 8 (IQR 6-9), respectively; good scores were given by 75% (15/20), 44% (4/9), and 55% (6/11) of health care professionals, respectively. The additional value of the COVID-box had a median score of 10 (IQR 8-10), with good scores from 96% (24/25) of health care professionals.
Technical Support Service (COVID-box Team)
For information provision and technical support for problems, the median scores were 7 (IQR 7-8) and 8 (IQR 7.5-8), respectively, with good scores from 37% (8/22) and 76% (13/17) of health care professionals, respectively. The median scores for the assessment of a patient’s ability and motivation were 8 (IQR 6-8) and 8 (IQR 7-9), respectively. A total of 57% (13/23) and 76% (16/21) of health care professionals, respectively, scored these items as good.
General Satisfaction
The general satisfaction of health care professionals and estimated patient satisfaction had a median score of 8 (IQR 7-8), and 60% (15/25) and 95% (18/19) of health care professionals scored these items as good, respectively. With regard to meeting the expectations for this home monitoring concept, good scores were given by 92% (22/24) of health care professionals, with a median score of 8 (IQR 8-10). With regard to supporting this home monitoring concept, the median score was 10 (IQR 10-10), with good scores from all health care professionals (25/25, 100%).
Discussion
Principal Findings
Our study demonstrates that the home monitoring of patients with COVID-19 is well appreciated by patients as well as health care professionals. Previous observational studies have shown the safety of the remote telemonitoring of patients with (suspected) COVID-19 and its efficacy in reducing hospitalization. Few studies have addressed user experience and patients’ and health care professionals’ satisfaction with telemonitoring. It is well established that the successful implementation of novel eHealth solutions is critically dependent on the positive experiences and satisfaction of involved users.
Comparison With Prior Work
During the extraordinary situation of the COVID-19 pandemic, remote telemonitoring has been quickly implemented in different ways [5-7,10-13]. In general, many patients and health care professionals are very positive about this concept. Remote telemonitoring is used for conducting disease triage; reducing hospital admissions; and providing reassurance, disease and disease course information, and psychological support to clinically stable patients at home. Several studies have reported that patients appreciate all forms of remote telemonitoring (eg, the measuring of vital parameters, symptom recording, and daily teleconsultations) in various settings (eg, in primary care and after an emergency department visit or hospital admission) [5-7,10-13]. The important aspects are easy access to the program, good information provision, and the good quality of the service for the onboarding process. Importantly, older age does not seem to be a problem, as different studies have successfully included patients aged >50 years [5,7,11]. Patients have pointed out that video consultations are also highly appreciated. Self-evidently, the adherence of patients to telemonitoring is critical to its success. Nonadherence to telemonitoring among patients with COVID-19 has been reported when they feel too sick, forget to measure vital parameters, feel insufficiently informed, or experience quick improvements in disease symptoms [13]. Health care professionals are largely convinced of the benefits of remote telemonitoring, as long as a program is easy to use and it is possible to receive patient data correctly.
Limitations
Given the observational and retrospective nature of our study, which was conducted during the COVID-19 pandemic, our study has several limitations that are noteworthy. First, the patient-reported experience measure questionnaires on telemonitoring a new disease, such as COVID-19, were not validated, and a formal validation of these questionnaires was out of the scope of this study. Second, the questionnaires were completed anonymously; therefore, internal consistency could not be reliably assessed. Lastly, the relatively low response rates (patients: 117/300, 39%; health care professionals: 25/60, 42%) could have introduced unwanted bias to the results of this study.
Conclusion
In conclusion, the home monitoring of patients with COVID-19 is well appreciated by patients as well as health care professionals. This study demonstrated that patients felt safe and reassured with the home monitoring and daily teleconsultations in the COVID-box project. Additionally, health care professionals were satisfied with the safety and user-friendliness of the COVID-box. The acceptation of the COVID-box is critical for the successful implementation and expansion of home monitoring for patients with COVID-19 to relieve the burden on health care systems. Our findings could be especially relevant to the current perspectives on oral antiviral agents for the out-of-hospital treatment of patients with COVID-19.
Abbreviations
- LUMC
Leiden University Medical Center
Questionnaire for patients.
Questionnaire for healthcare professionals.
Footnotes
Conflicts of Interest: None declared.
References
- 1.Vindrola-Padros C, Singh KE, Sidhu MS, Georghiou T, Sherlaw-Johnson C, Tomini SM, Inada-Kim M, Kirkham K, Streetly A, Cohen N, Fulop NJ. Remote home monitoring (virtual wards) for confirmed or suspected COVID-19 patients: a rapid systematic review. EClinicalMedicine. 2021 Jul;37:100965. doi: 10.1016/j.eclinm.2021.100965. https://linkinghub.elsevier.com/retrieve/pii/S2589-5370(21)00245-5 .S2589-5370(21)00245-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Silven AV, Petrus AHJ, Villalobos-Quesada M, Dirikgil E, Oerlemans CR, Landstra CP, Boosman H, van Os HJA, Blanker MH, Treskes RW, Bonten TN, Chavannes NH, Atsma DE, Teng YKO. Telemonitoring for patients with COVID-19: Recommendations for design and implementation. J Med Internet Res. 2020 Sep 02;22(9):e20953. doi: 10.2196/20953. https://www.jmir.org/2020/9/e20953/ v22i9e20953 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Dirikgil E, Roos R, Groeneveld GH, Heringhaus C, Silven AV, Petrus AHJ, Villalobos-Quesada M, Tsonaka R, van der Boog PJM, Rabelink TJ, Bos WJW, Chavannes NH, Atsma DE, Teng YKO. Home monitoring reduced short stay admissions in suspected COVID-19 patients: COVID-box project. Eur Respir J. 2021 Aug 05;58(2):2100636. doi: 10.1183/13993003.00636-2021. http://erj.ersjournals.com/lookup/pmidlookup?view=long&pmid=33795321 .13993003.00636-2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Casariego-Vales E, Blanco-López R, Rosón-Calvo B, Suárez-Gil R, Santos-Guerra F, Dobao-Feijoo MJ, Ares-Rico R, Bal-Alvaredo M, Telea-Covid Lugo Comanagement Team Efficacy of telemedicine and telemonitoring in at-home monitoring of patients with COVID-19. J Clin Med. 2021 Jun 29;10(13):2893. doi: 10.3390/jcm10132893.jcm10132893 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wurzer D, Spielhagen P, Siegmann A, Gercekcioglu A, Gorgass J, Henze S, Kolar Y, Koneberg F, Kukkonen S, McGowan H, Schmid-Eisinger S, Steger A, Dommasch M, Haase HU, Müller A, Martens E, Haller B, Huster KM, Schmidt G. Remote monitoring of COVID-19 positive high-risk patients in domestic isolation: A feasibility study. PLoS One. 2021 Sep 24;16(9):e0257095. doi: 10.1371/journal.pone.0257095. https://dx.plos.org/10.1371/journal.pone.0257095 .PONE-D-21-17053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Drewett GP, Holmes NE, Trubiano JA, Vogrin S, Feldman J, Rose M. COVID-Care - a safe and successful digital self-assessment tool for outpatients with proven and suspected coronavirus-2019. Digit Health. 2021 Sep 27;7:20552076211047382. doi: 10.1177/20552076211047382. https://journals.sagepub.com/doi/10.1177/20552076211047382?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .10.1177_20552076211047382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Clarke J, Flott K, Crespo RF, Ashrafian H, Fontana G, Benger J, Darzi A, Elkin S. Assessing the safety of home oximetry for COVID-19: a multisite retrospective observational study. BMJ Open. 2021 Sep 14;11(9):e049235. doi: 10.1136/bmjopen-2021-049235. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=34521666 .bmjopen-2021-049235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dinh A, Mercier JC, Jaulmes L, Artigou JY, Juillière Y, Yordanov Y, Jourdain P, AP-HP/Universities/INSERM COVID-19 Research Collaboration Safe discharge home with telemedicine of patients requiring nasal oxygen therapy after COVID-19. Front Med (Lausanne) 2021 Nov 03;8:703017. doi: 10.3389/fmed.2021.703017. doi: 10.3389/fmed.2021.703017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pimlott N, Agarwal P, McCarthy LM, Luke MJ, Hum S, Gill S, Heisey R. Clinical learnings from a virtual primary care program monitoring mild to moderate COVID-19 patients at home. Fam Pract. 2021 Sep 25;38(5):549–555. doi: 10.1093/fampra/cmaa130. https://academic.oup.com/fampra/article/38/5/549/6042205?login=false .6042205 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Panicacci S, Donati M, Lubrano A, Vianello A, Ruiu A, Melani L, Tomei A, Fanucci L. Telemonitoring in the Covid-19 era: The Tuscany Region experience. Healthcare (Basel) 2021 Apr 29;9(5):516. doi: 10.3390/healthcare9050516. https://www.mdpi.com/resolver?pii=healthcare9050516 .healthcare9050516 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McKinstry B, Alexander H, Maxwell G, Blaikie L, Patel S, Guthrie B, Technology Enabled Care TeleCOVID Group The use of telemonitoring in managing the COVID-19 pandemic: Pilot implementation study. JMIR Form Res. 2021 Sep 27;5(9):e20131. doi: 10.2196/20131. https://formative.jmir.org/2021/9/e20131/ v5i9e20131 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lim HM, Abdullah A, Ng CJ, Teo CH, Valliyappan IG, Hadi HA, Ng WL, Azhar AMN, Chiew TK, Liew CS, Chan CS. Utility and usability of an automated COVID-19 symptom monitoring system (CoSMoS) in primary care during COVID-19 pandemic: A qualitative feasibility study. Int J Med Inform. 2021 Nov;155:104567. doi: 10.1016/j.ijmedinf.2021.104567. http://europepmc.org/abstract/MED/34536808 .S1386-5056(21)00193-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kerr C, O' Regan S, Creagh D, Hughes G, Geary U, Colgan MP, Canning C, Martin Z, Merry C, Noonan N, Bergin C. Acceptability of and symptom findings from an online symptom check-in tool for COVID-19 outpatient follow-up among a predominantly healthcare worker population. BMJ Open. 2021 Sep 28;11(9):e050444. doi: 10.1136/bmjopen-2021-050444. https://bmjopen.bmj.com/lookup/pmidlookup?view=long&pmid=34588254 .bmjopen-2021-050444 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Questionnaire for patients.
Questionnaire for healthcare professionals.