

Abstract
Background:
This systematic review aimed to evaluate the efficacy of casein phosphopeptide-amorphous calcium phosphate (CPP-ACPF) varnish for remineralization of white spot lesions (WSLs) “in vitro” in human teeth.
Materials and Methods:
Literature search included three databases, namely Medline (via PubMed), The Cochrane Controlled Clinical Trials Register, and Google Scholar from 2010 to January 2021. The studies assessing WSL depth, calcium, phosphate ion release, and microhardness due to artificial demineralization or remineralization were considered for review. Reference articles were retrieved, and a customized risk assessment tool was used. The Cochrane risk of bias assessment tool was used to generate the risk of bias summary graph. Meta-analysis was performed using RevMan 5.4. Heterogeneity was evaluated by Cochrane's test, and random effects model was used to pool estimate of effect and its 95% confidence intervals (CIs) for surface microhardness.
Results:
Eighteen studies were selected for review based on the eligibility criteria. Four studies showed superior remineralizing effect of CPP-ACPF compared to fluoride varnishes. Four studies involving 120 human permanent teeth samples were included in the meta-analysis. Efficacy of CPP-ACPF varnish was equivalent to other fluoride varnishes in improving surface microhardness after remineralization during 7-day period (mean surface microhardness: 3.94, 95% CI [−9.08–1.21], I2: 75%, P = 0.13). Major risks of bias associated with the studies included in the review were inadequate sample size, improper sample preparation, and unexplained blinding.
Conclusion:
CPP-ACPF varnish appears to be equally effective as other fluoride varnishes in remineralizing artificially induced WSLs, but quality of evidence is low.
Key Words: Casein phosphopeptide-amorphous calcium phosphate, meta-analysis, remineralization, varnish
INTRODUCTION
The development of caries involves a dynamic biological process where acids produced by bacterial glycolysis of dietary carbohydrates cause demineralization of dental hard tissues. Noncavitated white spot lesions (WSLs) are indicative of early stage of dental caries. These lesions are considered reversible if detected early.[1] Topical application of fluoride-releasing materials has been used over three decades to combat dental caries.[2,3] They are considered important adjuvants in clinical practice, particularly when the patient's level of cooperation is low.[4] The major mechanism of fluoride ions in preventing enamel demineralization is by promoting the formation of fluorapatite in enamel in the presence of calcium and phosphate ions produced by plaque bacterial organic acids.[5,6] Fluoride ions can also drive the remineralization of previously demineralized enamel if enough salivary or plaque calcium and phosphate ions are available when the fluoride is applied.[7] Therefore, on topical application of fluoride ions, the availability of calcium and phosphate ions can be the limiting factor for net enamel remineralization to occur.[7] To overcome the limited bioavailability of calcium and phosphate ions, calcium phosphate-based remineralization systems such as amorphous calcium phosphate (ACP), calcium sodium phosphosilicate bioactive glass, and casein phosphopeptide-stabilized ACP were developed. The remineralizing potential of casein phosphopeptide-ACP (CPP-ACP) in cariogenic studies on animals, was demonstrated by researchers in 1995, and only in 2009 was it used for the treatment of WSLs.[8] CPP-ACP nanocomplexes is a technology based on ACP stabilized by casein phosphopeptides (CPP).[7] CPPs stabilize high concentrations of calcium and phosphate ions, together with fluoride ions, at the tooth surface by binding to pellicle and plaque. These ions are freely bioavailable to diffuse down concentration gradients into enamel subsurface lesions, thereby effectively promoting remineralization in vivo.[7]
Varnishes allow for the delivery of high concentrations of fluoride in small amounts.[9] The effectiveness, the relative safety, high fluoride uptake, and the ease of application, offer significant advantages over other professionally applied topical fluoride treatments such as fluoride gels, foams, and mouthrinses.[9] CPP-ACPF varnish is unique in that it uses Recaldent (CPP-ACP) technology incorporated with 5% sodium fluoride. The inclusion of CPP-ACP in MI varnish® (GC America Inc., Alsip, IL, USA) has been proven to inhibit enamel demineralization to a much greater extent than fluoride varnishes without CPP-ACP.[10,11] Literature search revealed three systematic reviews on CPP-ACP, with one focusing on effectiveness of MI paste and the other two reviewing effect of all formulations of CPP-ACP in human randomized clinical trials.[12,13,14] Review of in vitro studies comparing remineralizing potential of CPP-ACPF varnish with other fluoride varnishes has not been done. Hence, this systematic review aimed to evaluate the efficacy of CPP-ACPF varnish in remineralizing WSLs in vitro on human teeth.
MATERIALS AND METHODS
The Cochrane Handbook for Systematic Reviews of Interventions[15] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines were followed for review.[16] The Population, Intervention, Comparison, Outcome, and Study design method as applicable is presented in Table 1. The protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42021237900).
Table 1.
Population, Intervention, Comparison, Outcome, and Study design format of study
| Component | Description |
|---|---|
| Population | Human permanent and primary molars or premolars |
| Intervention | CPP-ACPF varnish |
| Comparison | fluoride varnishes other than CPP-ACPF |
| Outcome | Lesion depth, microhardness and calcium and phosphate release, and mineral loss/gain |
| Study design | In vitro studies |
CPP-ACPF: Casein phosphopeptide-amorphous calcium phosphate fluoride
Search strategy for article identification
An extensive electronic search for in vitro clinical trials via three databases, namely Medline (via PubMed), The Cochrane Controlled Clinical Trials Register, and Google Scholar, till January 29, 2021, was done. The outcomes of the search and Medical Subject Headings are summarized in Table 2. Hand searching was performed for relevant journals and the reference lists of all eligible studies for additional relevant studies. No restrictions on the language or date of publication were applied during the search. Reference articles were retrieved and exported to the Mendeley Desktop 1.13.3 software (Elsevier. Mendeley Ltd, London, United Kingdom).[17] The authors were not blinded to country or journal names.
Table 2.
Search strategy of the study
| Database | Search strategy | Articles retrieved |
|---|---|---|
| PubMed | (“Casein Phosphopeptide-Amorphous Calcium Phosphate nanocomplex”[Supplementary Concept] OR “Casein Phosphopeptide-Amorphous Calcium Phosphate nanocomplex”[All Fields] OR “CPP ACP”[All Fields]) AND (“paint”[MeSH Terms] OR “paint”[All Fields] OR “varnish”[All Fields])) AND Remineralization [All Fields] AND (Invitro[All Fields] AND Study[All Fields]) | 55 |
| Cochrane Central Library | MI varnish “CPP ACP varnish” AND remineralization | 16 |
| Google Scholar | MI varnish “CPP ACP varnish” AND remineralization, MI varnish “CPP ACP varnish” | 839 |
CPP-ACP: Casein phosphopeptide amorphous calcium phosphate
Selection of studies
The review included in vitro studies on human teeth from 2010 to January 2021. The studies assessing depth of WSL, microhardness due to artificial demineralization or remineralization and calcium, phosphate ion release, and mineral loss/gain were considered for review. Case reports, abstracts, editorials, review articles, non-English articles, animal studies, and studies testing formulations of CPP-ACP, such as sugar-free gums, lozenges, fluoridated gels, mouth rinse, paste, and antibacterial gels, were excluded from review.
Data extraction
One author searched the studies, screened the titles and abstracts of each study based on the criteria, and extracted data. Two authors independently rechecked the full text of the screened studies. Any disagreement between the two authors, was resolved by a third reviewer. Data collected for each study included information pertaining to year of publication, authorship, sample size, study characteristics like intervention, comparison, follow-up period, examination methods, and results.
Assessment of risk of bias
A customized risk assessment tool was prepared using Office of Health Assessment and Translation risk-of-bias tool[18] and checklist for reporting in vitro studies guidelines.[19] The domains evaluated are listed in Figure 1. All included studies were assessed independently by two review authors who were not blinded to identifying details of articles. Each domain was classified as having a low, high, or unclear risk of bias. The Cochrane risk of bias assessment tool was used to generate the risk of bias summary graph.[20]
Figure 1.
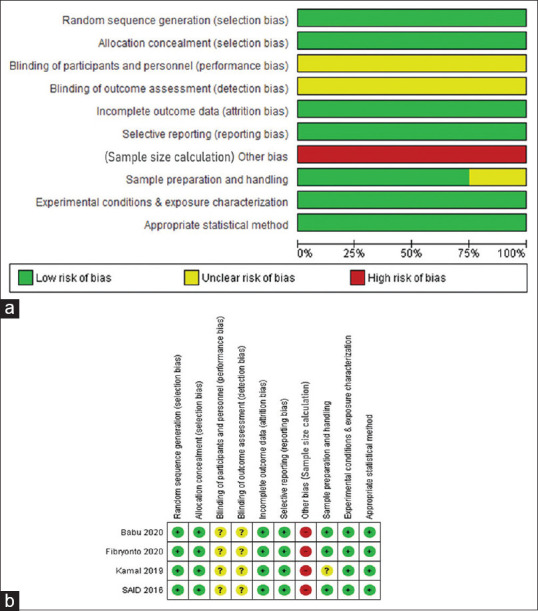
Cochrane risk of bias of the included studies (a) graph, (b) summary.
Statistical analysis
Data were analyzed using RevMan 5.4.[21] Heterogeneity between the estimates was evaluated by Cochrane's test (I2 test) at α = 0.10.[22] I2>50% indicated a high heterogeneity.[22] Furthermore, the statistical significance for testing the hypothesis was set at P value (two-tailed) < 0.05. Studies assessing the effect of CPP-ACPF versus fluoride varnishes on surface microhardness of artificially created WSLs in permanent teeth over a period of 1 week were included in the meta-analysis. The treatment effect for each study was summarized using mean differences and standard deviations. Random effects model was used to combine the studies due to the clinical and methodological heterogeneity existing in the studies.[23] A pooled estimate of effect and its 95% confidence intervals (CIs) for surface microhardness was calculated. Data from eligible studies were extracted into RevMan software and forest plot was generated for graphic presentation. Meta-analysis was not performed for the parameters lesion depth and mineral loss/gain due to dissimilarity in outcome measurements.
RESULTS
Study selection and description
Through the literature search, 913 studies were identified, including 822 duplicates. Seventy-four articles were identified after excluding duplications. A total of 17 articles evaluating the efficacy of MI paste were excluded after reading abstract. Full-text articles were retrieved for 57 relevant studies. Thirty-nine articles were excluded after full-text reading. Finally, 18 studies which met the inclusion criteria were considered [Figure 2]. Review evaluated three different outcomes: lesion depth, surface microhardness, and mineral loss/gain. Studies assessing the remineralization effect of CPP-ACP varnish over a period of 7 days in comparison to other fluoride varnish were pooled. Results of four studies measuring surface microhardness were synthesized using forest plot.
Figure 2.
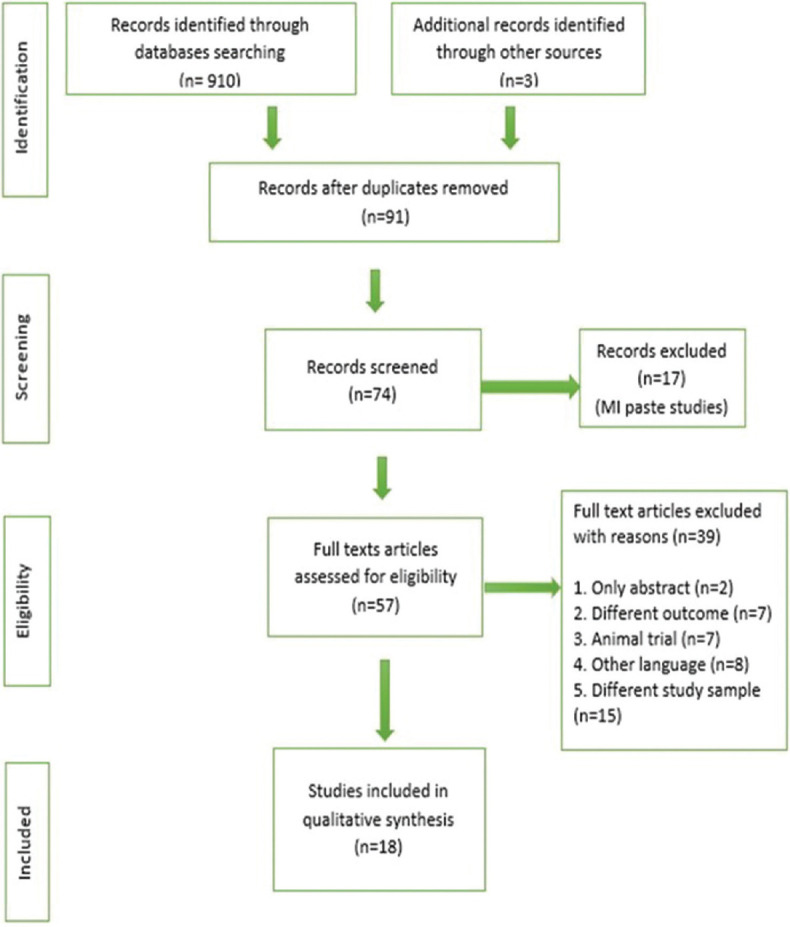
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of review methodology.
Study characteristics
Eighteen relevant studies were found published from 2011 to 2021 (January). Ten studies were reported from Asia, three from the Middle East, two each from America and Australia, and one from Europe. All the studies were conducted on extracted human permanent teeth. These studies reported intervention on permanent molars, premolars, and anterior teeth. Examination methods for surface microhardness assessment included microhardness tester machine expressing Knoop hardness number and Vickers microhardness number. For evaluating lesion depth, polarized light microscope, FluorCam, transverse microradiography, stereomicroscope, micro-computed tomography analysis, and Diagnodent were used. To measure calcium and phosphate ion release, ion chromatography and scanning electron microscope were utilized and transverse microradiography was used for assessing mineral content. Test group considered was only ACP-CPPF varnish compared with one or more control groups such as no treatment, fluoride varnish, and other varnishes. The follow-up period ranged from 4 to 84 days [Table 3].
Table 3.
Characteristics of included studies
| Author/Year/Country | Sample teeth/surface | Intervention group(n) | Comparison group(n) | Follow-up period | Examination methods |
|---|---|---|---|---|---|
| Attiguppe etal., 2019, India[10] | Premolars/buccal and the lingual surfaces | Group1-CPP-ACPF varnish(24) | Group2-Fluor protector varnish(24) | 1. Lesion depth-30days 2. Frelease(2 and 4weeks) |
1. Polarized light microscope-Lesion depth 2. Fluoride-specific ion electrode-Fluoride release |
| Abufarwa etal., 2019, Texas[24] | Premolars and Molars/buccal surface | Group1-CPP-ACPF varnish(21) | Group2-Laser(21) Group3-Control group(21) |
10days | 1. KNH number-surface microhardness 2. FluoreCam-lesion depth |
| Abufarwa etal., 2019, Texas[25] | Premolars and Molars/buccal surface | Group1-CPP-ACPF varnish(40) | Group2-Control group(40) | 2, 4, 8, and 12weeks | 1. FluoreCam system-area 2. Polarized light microscopelesion depth |
| Girish Babu etal., 2018, India[26] | Premolars/buccal surface | Group1-CPP-ACPF varnish(25) | Group2-Fluor protector(25) Group3-Control window-no varnish |
6days | 1. Polarized light microscope-Lesion depth |
| Babu etal., 2020, India[27] | Premolars/buccal surface | Group1-CPP-ACPF varnish(30) | Group2-Fluor protector(30) Group3-No varnish(30) |
8days | 1. Microhardness tester machine-Surface microhardness |
| Bakry and Abbassy 2018, Saudi Arabia[28] | Third molars/buccal and lingual surfaces | Group3-CPP-ACPF varnish(25) | Group1-MI paste(25) Group2-MI paste+bond(25) Group4-Control(25) |
7days | 1. Vickers microhardness-surface microhardness 2. Transverse microradiography analysis-lesion depth, mineral loss |
| Bapat etal. 2020, India[29] | Premolars/buccal surface | Group1-CPP-ACPF varnish(10) | Group2-Embrace Varnish(10) Group3-Control(10) |
10days | 1. Vickers microhardness method-surface microhardness |
| Fibryanto etal., 2020, Indonesia[30] | Premolars/buccal surface | Group1-CPP-ACPF varnish(10) | Group2-Bifluorid(10) Group3-Clinpro XT varnish(10) |
7thand 14thdays | 1. Vickers microhardness method-surface microhardness |
| Kamal etal., 2020, Egypt[31] | Molars/buccal surface | Group1-CPP-ACPF varnish(10) | Group2-Control(10) Group3-Fluoride(10) |
1stand 4thweeks | 1. Vickers microhardnessmethod-Surface microhardness |
| Majithia etal., 2016, Malaysia[32] | Premolars/buccal surface | Group4-CPP-ACPF Varnish(10) | Group1-No varnish(10) Group2-Flor-Opal® Varnish White(10) Group3-Premier Enamel Pro Varnish(10) |
5days | 1. Vickers microhardness-surface microhardness 2. SEM-EDAX testing-Calcium/phosphorus ratio |
| Ramadevi etal., 2020, India[33] | Anteriors/buccal surface | Group2: CPP-ACPF Varnish(10) | Group1: NaF(10) | 5days | 1. Polarized light micro-scopelesion depth |
| Mohd Said etal., 2017, China[34] | 3rd molars/buccal surface | Group2: CPP-ACPF Varnish(10) | Group0: Control (no varnish),(10) Group1: Duraphat,(10) Group3: Embrace Varnish,(10) Group4: Enamel Pro-Varnish,(10) Group5: Clinpro-White Varnish.(10) |
8days | 1. Knoop surface microhardness-surface microhardness 2. Transverse microradiography-lesiondepth and change in mineral loss |
| Shen etal., 2016, Australia[11] | 3rd molars/buccal and lingual surfaces | Group3-CPP-ACPF varnish(12) | Group1-Enamel Pro(12) Group2-Clinpro(12) Group4-Duraphat(12) Group5-Profluorid(12) Group6-Control(12) |
4days | 1. Transverse microradiography lesiondepth 2. Ion chromatography-ions release |
| Sleibi etal., 2018, UK[35] | Premolar roots/buccal surface | Group1-CPP-ACPF varnish(12) | Group2-Bioglass(12) Group3-5% NaF(12) Group4-Control(12) |
5days | 1. XMT-change in mineral concentration |
| Shen etal., 2020, Australia[36] | 3rd molars/gingival or occlusal | Group1-CPP-ACPF varnish(10) | Group2-Duraphat varnish(10) Group3-Control group(10) |
14days | 1. Ion chromatography-Ions release 2. Transverse microradiography mineral content |
| Thakkar etal., 2017, India[37] | Molars/buccolingually, and mesiodistally (4sections) | Group3-CPP-ACPF varnish(20) | Group1-CPP-ACP paste(20) Group2-Tooth Mousse plus(20) Group4-Control group(20) |
Demineralization=12 days Remineralization=19 days |
1. Stereomicroscope -lesional depth |
| Üstün and Aktören 2019, Istanbul[38] | 3rd Molars/buccal and lingual surfaces | Group1-CPP-ACPF varnish(8) | Group2-Duraphat varnish(8) Group3-Artificial saliva(8) |
30days | 1. Diagnodent-lesional depth 2. μCT analysis-Lesion depth, surface area |
| Varma etal., 2019, India[39] | Premolars/buccal surface | Group1-CPP-ACPF varnish(10) | Group2-Clinpro XT varnish(10) Group3-Control group(10) |
7days | 1. Diagnodent-lesional depth. |
Control group - Untreated, (n) - sample size. CPP-ACPF: Casein phosphopeptide-amorphous calcium phosphate fluoride, F: Fluoride, KNH: Knoop hardness, XMT: X-ray microtomography, SEM-EDAX: Scanning electron microscopy with an energy dispersive X-ray analysis attachment, NaF: Sodium fluoride
Risk of bias assessment
Score of 1 was given for each risk of bias item, if mentioned. The overall level of risk for each study was subsequently classified as low risk, “moderate risk/unclear risk,” and “high risk” (if score was 7 or more, 3 or more, and <3 out of the nine categories, respectively). The scores were averaged for each included study. Score was not given when individual risk of bias item was not mentioned clearly. For example: no mention of sample size calculation;[19] blinding and multiple samples prepared from the same specimen.[19] Risk of bias item randomization and allocation concealment were considered low risk as the samples (human teeth enamel) used were homogenous.[18] Overall, 7[26,31,32,34,38] of the 18 included studies had unclear risk of bias and rest 11[10,11,24,27,29,30,33,35,36,37,39] had low risk of bias. The risks of bias of the included studies are summarized in Table 4 [Figure 3]. Major risks of bias associated with these studies included inadequate sample size, improper sample preparation, and unexplained blinding.
Table 4.
Summary of risk of bias of the included studies
| Author/year/country | Sample size calculation | Sample preparation and handling-S/MS⁋ | Randomization | Allocation concealment | Blinding (M/NM) | Experimental conditions and exposure characterization similar(yes/no) | Outcome data-attrition/exclusion (M/NM) | Reported - measured outcome (Yes/No) | Appropriate statistical method (Yes/No) | Risk of bias score |
|---|---|---|---|---|---|---|---|---|---|---|
| Attiguppe etal., 2019, India[10] | M | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 7/9 |
| Abufarwa etal., 2019, Texas[24] | M | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 7/9 |
| Abufarwa etal., 2019, Texas[25] | M* | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 6/9 |
| Girish Babu etal., 2018, India[26] | NM | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 6/9 |
| Babu etal., 2020, India[27] | NM | S | NM | NM | NM | Yes | M | Yes | Yes | 7/9 |
| Bakry and Abbassy 2018, Saudi Arabia[28] | M* | MS⁋ | M | NM | NM | No | M | Yes | Yes | 5/9 |
| Bapat etal., 2020, India[29] | NM | S | M | NM | NM | Yes | M | Yes | Yes | 7/9 |
| Fibryanto etal., 2020, Indonesia[30] | NM | S | M | NM | NM | Yes | M | Yes | Yes | 7/9 |
| Kamal etal., 2020, Egypt[31] | NM | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 6/9 |
| Majithia etal., 2016, Malaysia[32] | NM | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 6/9 |
| Ramadevi etal., 2020, India[33] | NM | MS⁋ | NM | NM | M | Yes | M | Yes | Yes | 7/9 |
| Mohd Said etal., 2017, China[34] | NM | MS⁋ | M | M | NM | Yes | M | Yes | Yes | 6/9 |
| Shen etal., 2016, Australia[11] | NM | MS⁋ | M | M | M | Yes | M | Yes | Yes | 7/9 |
| Sleibi etal., 2018, UK[35] | M | MS⁋ | M | M | NM | Yes | M | Yes | Yes | 7/9 |
| Shen etal., 2020, Australia[36] | NM | MS⁋ | M | NM | M | Yes | M | Yes | Yes | 7/9 |
| Thakkar etal., 2017, India[37] | M | MS⁋ | M | NM | M | Yes | M | Yes | Yes | 8/9 |
| Üstün and Aktören 2019, Istanbul[38] | M* | MS⁋ | M | NM | NM | Yes | M | Yes | Yes | 6/9 |
| Varma etal., 2019, India[39] | M | S | NM | NM | NM | Yes | M | Yes | Yes | 8/9 |
Unclear/moderate risk - Yellow, Low risk – Green. M: Mentioned; NM: Not mentioned; M*: Mentioned but less samples used, MS⁋: Multiple sample from same specimen, S: Single sample from the specimen
Figure 3.

Forest plot summary of included studies.
Synthesis of results – Effect of interventions
Surface microhardness
Out of six studies, five studies[27,30,31,32,34] showed no significant difference in surface microhardness between the intervention and fluoride groups after an interval of 7 days. CPP-ACPF varnish groups recorded significantly harder enamel than no treatment groups [Table 5].[24,27,28,29,31,32,34]
Table 5.
Summary of findings of review related to surface microhardness, mineral loss/gain, ion release, and lesion depth
| Author | Summary of findings |
|---|---|
|
| |
| Surface microhardness | |
| Babu etal.[27] | There was statistically significant difference between control and experimental windows(P<0.001). No significant difference was seen between CPP-ACPF varnish and fluoride group |
| Abufarwa etal.[24] | The fluoride group showed statistically significant harder enamel than the control at 20, 40, and 60 μm depths |
| Bakry and Abbassy[28] | Percent surface microhardness recovery for CPP-ACPF varnish group was significantly higher compared to control |
| Bapat etal.[29] | The CPP-ACPF Varnish group showed significantly high value of enamel surface microhardness as compared to pulpdent embrace group and control group |
| Kamal etal.[31] | No statistically significant difference was found between fluoride and CPP-ACPF |
| Majithia etal.[32] | Microhardness values were statistically significant from those of the control group. But no significant difference was seen between varnish groups |
| Mohd Said etal[34] | Varnish groups post remineralization microhardness values and(% SHR) were statistically significant from those of the control group. No significant difference was reported between varnishes groups |
| Fibryanto etal.[30] | Day seven remineralization showed no significant difference in microhardness between CPP-ACP and 5% calcium fluoride group |
| Mineral loss/gain and Ions release from varnish | |
|
| |
| Majithia etal.[32] | Varnish groups post remineralization Ca and Pvalues, Ca/P ratio were statistically significant from those of the control group. No significant difference was seen between the different varnish groups |
| Mohd Said etal.[34] | Mean change in mineral loss in CPP-ACPF group was significantly higher when compared with the control group |
| Shen etal.[11] | CPP-ACPF Varnish released the highest levels of calcium, phosphate fluoride ions. Showed significantly lower reduction in mineral loss compared to fluoride alone varnishes |
| Sleibi etal.[35] | The mineral gain was superior in fluoride groups than CPP-ACPF and there was no significant difference |
| Shen etal.[36] | Mineral gain was significantly higher in CPP-ACPF varnish than fluoride group. Significantly higher levels of all ions(Ca, PO4, F) in the CPP-ACPF varnish group than fluoride varnish group |
| Lesion depth | |
|
| |
| Attiguppe etal.[10] | Demineralization inhibitory effect was higher in CPP-ACPF varnish grp and showed a high statistically significant difference between the groups |
| Girish Babu etal.[26] | There was statistically significant difference between control and experimental windows in both groups. No significant difference was seen between varnish groups |
| Abufarwa etal. [24] | The area of enamel demineralization in the CPP-ACPFgroup was significantly smaller than control |
| Abufarwa etal. [25] | Demineralization inhibitory effect was higher in CPP-ACPF varnish group than control |
| Lesion depth | |
|
| |
| Bakry and Abbassy28 | CPP-ACPF varnish groups recorded significant decrease in lesion depth than control group |
| Mohd Said etal.[34] | Significant difference in lesion depth postremineralization was seen between different varnishes and control. No difference was reported between the varnish groups |
| Shen etal.[11] | The CPP-ACPF varnish inhibited demineralization significantly better than when compared with the Duraphat fluoride-alone control |
| Thakkar etal.[37] | Difference in the mean lesional depth of sections from CPP-ACPF varnish was significantly lower compared to control group after demineralization cycle. Samples from CPP-ACPF showed significant remineralization effect when compared to control group |
| Üstün and Aktören etal.[38] | There was no significant difference between CPP-ACFP/NaF for all time intervals. Statistically significant differences were found for varnish groups when compared to the control group |
| Varma etal.[39] | CPP-ACPF varnish had significantly better remineralization effect than others |
| Shen etal.[36] | The CPP-ACP/F varnish promoted significantly greaterremineralization than the fluoride-alone Duraphat varnish |
| Ramadevi etal[33] | CPP-ACPF varnish had statistically significant reduction in the mean lesion depth compared to 5% sodium fluoride varnish alone |
%SHR: Percent surface hardness recovery, F: fluoride, NaF: Sodium fluoride, Ca/P: Calcium/phosphorus, PO4: Phosphate, CPP-ACPF: Casein phosphopeptide - amorphous calcium phosphate fluoride
For meta-analysis, we pooled data of four studies[27,30,31,34] involving 120 human permanent teeth samples. CPP-ACPF varnish compared to fluoride varnish did not significantly favor improvement of surface microhardness after remineralization during 7-day period (SMH: 3.94, 95% CI [−9.08–1.21], P = 0.13), and there was substantial heterogeneity (tau = 19.2, Chi-squared = 10.7, I2= 72%) across the studies [Figure 1].
Mineral loss/gain
Three studies evaluated calcium and phosphate ions release. Two studies[11,36] reported calcium and phosphate ion release to be significantly higher in CPP-ACPF varnish group than fluoride group, whereas in one study, there was no significant difference.[32] The mean change in mineral gain after remineralization was superior in CPP-ACPF varnish group over control.[34,35,36] The mineral gain was highest in CPP-ACPF varnish than fluoride groups in a study,[36] but two studies did not report significant result.[34,35] Reduced mineral loss during demineralization was seen in CPP-ACPF group compared to fluoride varnish[11] [Table 5].
Lesion depth
Of the 12 studies, 2 studies[10,11] showed superior demineralizing inhibitory effect of CPP-ACPF varnish over fluoride varnish. CPP-ACPF varnish showed superior remineralizing effect when compared to no treatment.[11,24,25,26,28,34,36,37,38,39] When remineralizing effect of CPP-ACPF varnish was compared to fluoride varnish, superior efficacy was seen in four studies[11,33,36,39] while two studies[34,38] did not report a significant effect [Table 5].
DISCUSSION
This systematic review and meta-analysis underline the significant remineralizing effect of CPP-ACPF varnish compared to fluoride varnishes. Majority of in vitro studies[11,33,36,39] have shown pronounced remineralizing effect of CPP-ACPF varnishes compared with other fluoride varnishes. However, few in vitro[34,38] studies have shown contradictory results. Meta-analysis showed no significant difference between CPP-ACPF varnish and other fluoride varnishes in improving the surface microhardness after remineralization during 7-day period.
Fluoride varnishes are more effective compared to other forms of delivery because of long contact periods resulting in high fluoride uptake and the formation of CaF2 deposits that act as fluoride reservoirs.[40] The CPP-ACP has been shown to interact with fluoride ions to produce an additive anticariogenic effect through the formation of CPP-stabilized amorphous calcium fluoride phosphate (ACFP) phase.[41,42,43,44] The in situ study by Reynolds[45] showed that CPP-ACP plus fluoride formulation not only increased fluoride incorporation into plaque but also in subsurface enamel and substantially increased remineralization of subsurface lesions of enamel compared with fluoride alone. An in vitro study by Duraisamy et al. reported that demineralization inhibitory potential on the additive use of F − varnish + CPP-ACP was superior to fluoride varnish or CPP-ACP applied alone on the enamel of young permanent teeth.[46] The presence of the CPP-ACFP nanocomplexes in MI varnish has shown to be superior to fluoride alone in inhibiting enamel demineralization and promoting remineralization in a number of in situ and in vivo randomized controlled clinical trials.[8,45,47,48,49]
An in vitro study by Thakkar et al. found that CPP-ACPF varnish had significant demineralization inhibitory property compared to CPP-ACP paste and CPP-ACPF paste plus. Remineralizing effect did not differ significantly compared to both groups.[37] A previous study, which evaluated remineralizing efficiency of CPP-ACPF varnish and paste groups, showed increased values of calcium, phosphate contents, higher percent surface microhardness recovery, decrease in lesion depth, and mineral loss compared to paste groups.[28]
In the studies considered for review, fluoride varnishes contained a variety of combinations, which accounted for substantial clinical heterogeneity. CPP-ACPF varnish showed significantly higher demineralization inhibitory effect and greater amount of fluoride release as compared to fluor protector for a period of 1 month.[10] An in vitro study compared calcium phosphate-containing varnishes such as enamel pro, Clinpro, and CPP-ACPF varnish with other fluoride varnishes. The results showed that only CPP-ACPF varnish significantly inhibited demineralization than fluoride alone varnishes such as Duraphat and Profluorid.[11] Furthermore, CPP-ACPF varnish provided 130% greater inhibition when compared with the Duraphat fluoride-alone control.[11] The presence of the CPP-ACFP nanocomplexes and combination with fluoride would explain the superior ability of CPP-ACP varnish in inhibiting demineralization.
Remineralization potential on artificial enamel caries-like lesions in permanent teeth was significantly better with CPP-ACPF varnish compared to 5% sodium fluoride varnish[33,36] and Clinpro varnish.[33] However, CPP-ACPF varnish did not achieve better remineralization of artificial enamel carious lesions when compared with Duraphat varnish.[34,38] In a clinical trial by Obradović et al., CPP-ACPF varnish showed better remineralization of initial smooth surface caries lesions of primary teeth compared to conventional varnish with fluoride.[50] A systematic review and meta-analysis on randomized controlled trials by Tao et al. concluded that fluorides combined with CPP-ACP treatment produce significantly better remineralization of occlusal early caries lesions. For lesions on smooth surfaces, the meta-analysis showed no significant difference between using fluorides with CPP-ACP and using fluorides alone.[13] The CPP-ACFP are amorphous electroneutral nanocomplexes and their hydrodynamic radius allows rapid diffusion out of the varnish and is reported to enter the porosities of an enamel subsurface lesion through intraprismatic spaces favoring remineralization.[51]
Most varnishes in the market contain 5% NaF with an alcohol- and resin-based solution. The evaporation of the alcohol makes the system fast drying, and the resin functions to allow the fluoride to adhere to the teeth.[52] The most common resin additive is colophony, a resin derived from pine tree sap.[52] The main complaint about varnish, “stickiness,” and a noticeable film on the teeth is due to the carrier. The resin base in fluoride varnishes allows them to stick to tooth surfaces and stay for up to 24 h whereby fluoride is gradually released from the varnish and is taken up by the tooth enamel and dentin.[52] The strongly bound fluoride, incorporated onto the surface of the crystals of apatite, can reduce the solubility of the tooth mineral and hence inhibit demineralization due to acids generated by plaque bacteria.[53] Varnishes are preferred over other topical forms since they are user friendly and requires less handling and application time, When compared to gels, they are less likely to be ingested by young children. Varnishes are a successful strategy of prevention of caries in individuals with special requirements, such as those with developmental disabilities, because they stick to the tooth surface for longer lengths of time and requires less patient compliance.[54] A randomized trial by Huang et al. assessed the effectiveness of MI Paste Plus and PreviDent fluoride varnish for treatment of WSLs. The results showed no significant difference between two groups compared to a standard oral hygiene and toothpaste. This result can be attributed to the presentation of material in the form of varnish and not in toothpaste form.[4,55]
A Cochrane review in 2016 suggested the superiority of resin-based fissure sealants over fluoride varnish applications for preventing occlusal caries in permanent molars, but the quality of evidence was low.[56] Fluoride varnish was shown to be less expensive than fissure sealant in a randomized clinical trial that used mobile dental clinics to target children with high caries risk. However, caries prevention was not significantly different when either strategy was used twice a year.[57] A cost-effectiveness analysis based on a clinical decision tree found the application of fluoride varnish as a cost-effective community strategy to prevent early childhood caries among rural children in nonfluoridated areas.[58] Cost-effectiveness of varnish against sealant was assessed over a period of 4 years in a school-based setting. Varnish appeared to be more cost-effective than sealants as the latter required expertise in application.[59] The application of varnish requires very little infrastructure, and it can be more readily applied in nontraditional settings (dental chair with illumination and fluid evacuation to maintain a dry field).[59] Even health-care providers with minimal training can also apply varnish.[59]
In vitro studies make possible the inexpensive and rapid yet sensitive assessment of any new inventions in a highly controlled environment representing a key component of product activity confirmation. However, major limitation is their inability to simulate the complex biological processes involved in caries. And, also the oral conditions that prevail in the mouth.[60] In in-situ and in -vitro investigations, quantitative measurements of mineral loss and lesion depth are regarded as standard primary outcomes for evaluating re and demineralization.[60] Surface microhardness is indirect technique which complements direct measures of mineral gain and loss.[60] There were very few studies which assessed mineral loss/gain in the present review.[11,34,35,36]
Lesion depth defines the magnitude of penetration and damage from acid caused by varnishes. Transverse microradiography and polarized light microscopy are desirable methods[61] for direct assessment of lesion depth which was followed in only a few studies. Some studies had a small sample size. There was heterogeneity in the method of outcome assessment for lesion depth and mineral loss/gain, which limited meta-analysis for these parameters. Future research would benefit from a uniform method of assessment for mineral loss/gain and lesion depth using these products. Being cognizant about heterogeneity in reporting of methodology and evaluation, including the duration of follow-up and assessment, the evidence should be considered with caution. Future studies should be planned overcoming these limitations and dental association bodies should frame guidelines for reporting of efficacy of caries remineralizing agents in scientific studies which will help in review of articles and framing of clinical practice guidelines.
CONCLUSION
CPP-ACPF varnish appears to be equally effective as other fluoride varnishes in remineralizing WSLs, but quality of evidence is low.
Financial support and sponsorship
Nil.
Conflicts of interest
The authors of this manuscript declare that they have no conflicts of interest, real or perceived, financial or nonfinancial in this article.
REFERENCES
- 1.Featherstone JD. The caries balance: The basis for caries management by risk assessment. Oral Health Prev Dent. 2004;2(Suppl 1):259–64. [PubMed] [Google Scholar]
- 2.Marinho VC, Higgins JP, Sheiham A, Logan S. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;2003:CD002278. doi: 10.1002/14651858.CD002278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Marinho VC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013;11(7):CD002279. doi: 10.1002/14651858.CD002279.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pithon MM, Dos Santos MJ, Andrade CS, Leão Filho JC, Braz AK, de Araujo RE, et al. Effectiveness of varnish with CPP-ACP in prevention of caries lesions around orthodontic brackets: An OCT evaluation. Eur J Orthod. 2015;37:177–82. doi: 10.1093/ejo/cju031. [DOI] [PubMed] [Google Scholar]
- 5.Pollick H. The role of fluoride in the prevention of tooth decay. Pediatr Clin North Am. 2018;65:923–40. doi: 10.1016/j.pcl.2018.05.014. [DOI] [PubMed] [Google Scholar]
- 6.ten Cate JM. Current concepts on the theories of the mechanism of action of fluoride. Acta Odontol Scand. 1999;57:325–9. doi: 10.1080/000163599428562. [DOI] [PubMed] [Google Scholar]
- 7.Reynolds EC. Calcium phosphate-based remineralization systems: Scientific evidence? Aust Dent J. 2008;53:268–73. doi: 10.1111/j.1834-7819.2008.00061.x. [DOI] [PubMed] [Google Scholar]
- 8.Bailey DL, Adams GG, Tsao CE, Hyslop A, Escobar K, Manton DJ, et al. Regression of post-orthodontic lesions by a remineralizing cream. J Dent Res. 2009;88:1148–53. doi: 10.1177/0022034509347168. [DOI] [PubMed] [Google Scholar]
- 9.Cecchini-259 J. New Generation of Fluoride Varnish is Coming to You! Oral Health Group. 2021. [Last accessed on 2021 Jul 07]. Available from: https://www.oralhealthgroup. com/features/new-generation-fluoride-varnish-coming/
- 10.Attiguppe P, Malik N, Ballal S, Naik SV. CPP-ACP and fluoride: A synergism to combat caries. Int J Clin Pediatr Dent. 2019;12:120–5. doi: 10.5005/jp-journals-10005-1608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shen P, Bagheri R, Walker GD, Yuan Y, Stanton DP, Reynolds C, et al. Effect of calcium phosphate addition to fluoride containing dental varnishes on enamel demineralization. Aust Dent J. 2016;61:357–65. doi: 10.1111/adj.12385. [DOI] [PubMed] [Google Scholar]
- 12.Indrapriyadharshini K, Madan Kumar PD, Sharma K, Iyer K. Remineralizing potential of CPP-ACP in white spot lesions – A systematic review. Indian J Dent Res. 2018;29:487–96. doi: 10.4103/ijdr.IJDR_364_17. [DOI] [PubMed] [Google Scholar]
- 13.Tao S, Zhu Y, Yuan H, Tao S, Cheng Y, Li J, et al. Efficacy of fluorides and CPP-ACP vs.fluorides monotherapy on early caries lesions: A systematic review and meta-analysis. PLoS One. 2018;13:e0196660. doi: 10.1371/journal.pone.0196660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Imani MM, Safaei M, Afnaniesfandabad A, Moradpoor H, Sadeghi M, Golshah A, et al. Efficacy of CPP-ACP and CPP-ACPF for prevention and remineralization of white spot lesions in orthodontic patients: A systematic review of randomized controlled clinical trials. Acta Inform Med. 2019;27:199–204. doi: 10.5455/aim.2019.27.199-204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions [Internet] Training.cochrane.org. 2021. [cited 29 January 2022]. Available from: https://training.cochrane.org/ handbook .
- 16.Moher D, Liberati A, Tetzlaff J, Altman DG PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009 Jul 21;6(7):336–41. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Patak AA, Naim HA, Hidayat R. Taking Mendeley as multimedia-based application in academic writing. Int J Adv Sci Eng Inf Technol. 2016;6:557–60. [Google Scholar]
- 18.Rooney A. Extending a Risk-of-Bias Approach to Address in vitro Studies. National Toxicology Program Office of Health Assessment and Translation. Bing.com. 2015. [Last accessed on 2021 Feb 09]. Available from: https://www.bing.com/search?q=rooney+andrew%2C+ohat+to ol&cvid=f7e3f48f23674accb19a1f442e6740c1&pglt=43&FOR M=ANNTA1&PC=HCTS .
- 19.Krithikadatta J, Gopikrishna V, Datta M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J Conserv Dent. 2014;17:301–4. doi: 10.4103/0972-0707.136338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi: 10.1136/bmj.d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Review Manager Web (RevMan Web) [Computer Program]. Version 1.22.0. The Cochrane Collaboration; [Internet] 2020. [Last accessed on 2022 Jan 29]. Available from: http://revman.cochrane.org .
- 22.Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods. 2006;11:193–206. doi: 10.1037/1082-989X.11.2.193. [DOI] [PubMed] [Google Scholar]
- 23.Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Abufarwa M, Noureldin A, Azimaie T, Campbell PM, Buschang PH. Preventive effects of carbon dioxide laser and casein phosphopeptide amorphous calcium phosphate fluoride varnish on enamel demineralization: A comparative, in vitro study. J Investig Clin Dent. 2019;10:e12400. doi: 10.1111/jicd.12400. [DOI] [PubMed] [Google Scholar]
- 25.Abufarwa M, Noureldin A, Campbell PM, Buschang PH. The longevity of casein phosphopeptide-amorphous calcium phosphate fluoride varnish's preventative effects: Assessment of white spot lesion formation. Angle Orthod. 2019;89:10–5. doi: 10.2319/021718-127.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Girish Babu KL, Subramaniam P, Teleti S. Remineralization potential of varnish containing casein phosphopeptides-amorphous calcium phosphate with fluoride and varnish containing only fluoride: A comparative study. Saudi J Oral Sci. 2018;5:35–40. [Google Scholar]
- 27.Babu KL, Subramaniam P, Teleti S. Effect of varnish containing casein phosphopeptides-amorphous calcium phosphate and fluoride on surface microhardness of enamel – An in vitro study. Saudi J Oral Sci. 2020;7:29–34. [Google Scholar]
- 28.Bakry AS, Abbassy MA. Increasing the efficiency of CPP-ACP to remineralize enamel white spot lesions. J Dent. 2018;76:52–7. doi: 10.1016/j.jdent.2018.06.006. [DOI] [PubMed] [Google Scholar]
- 29.Bapat SA, Shashikiran ND, Gugawad S, Gaonkar N, Taur S, Hadakar S, et al. In-vitro comparison of anti-microbial efficacy and enamel microhardness after application of two types of fluoride varnishes. J Clin Diag Res. 2020;14:ZC05–8. [Google Scholar]
- 30.Fibryanto E, Elline D, Indah DP, Hidayat A. The effect of topical remineralization agents on surface microhardness of enamel (ex vivo research) J Int Dent Med Res. 2020;13:964–8. [Google Scholar]
- 31.Kamal D, Hassanein H, Elkassas D, Hamza H. Complementary remineralizing effect of self-assembling peptide (P11-4) with CPP-ACPF or fluoride: An in vitro study. J Clin Exp Dent. 2020;12:e161–8. doi: 10.4317/jced.56295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Majithia U, Venkataraghavan K, Choudhary P, Trivedi K, Shah S, Virda M. Comparative evaluation of application of different fluoride varnishes on artificial early enamel lesion: An in vitro study. Indian J Dent Res. 2016;27:521–7. doi: 10.4103/0970-9290.195642. [DOI] [PubMed] [Google Scholar]
- 33.Ramadevi RP, Jayasudha K, Arun E, Madhan CG, Jayanthi M, Aravinth V. An in-vitro comparative evaluation of two different fluoride varnishes in the remineralization of artificial caries lesions on human primary and permanent teeth. Univ J Surg Surg Spec. 2020;6:1–5. [Google Scholar]
- 34.Mohd Said SN, Ekambaram M, Yiu CK. Effect of different fluoride varnishes on remineralization of artificial enamel carious lesions. Int J Paediatr Dent. 2017;27:163–73. doi: 10.1111/ipd.12243. [DOI] [PubMed] [Google Scholar]
- 35.Sleibi A, Tappuni A, Mills D, Davis GR, Baysan A. Comparison of the efficacy of different fluoride varnishes on dentin remineralization during a critical pH exposure using quantitative X-ray microtomography. Oper Dent. 2018;43:E308–16. doi: 10.2341/18-014-L. [DOI] [PubMed] [Google Scholar]
- 36.Shen P, McKeever A, Walker GD, Yuan Y, Reynolds C, Fernando JR, et al. Remineralization and fluoride uptake of white spot lesions under dental varnishes. Aust Dent J. 2020;65:278–85. doi: 10.1111/adj.12787. [DOI] [PubMed] [Google Scholar]
- 37.Thakkar PJ, Badakar CM, Hugar SM, Hallikerimath S, Patel PM, Shah P. An in vitro comparison of casein phosphopeptide-amorphous calcium phosphate paste, casein phosphopeptide-amorphous calcium phosphate paste with fluoride and casein phosphopeptide-amorphous calcium phosphate varnish on the inhibition of demineralization and promotion of remineralization of enamel. J Indian Soc Pedod Prev Dent. 2017;35:312–8. doi: 10.4103/JISPPD.JISPPD_308_16. [DOI] [PubMed] [Google Scholar]
- 38.Üstün N, Aktören O. Analysis of efficacy of the self-assembling peptide-based remineralization agent on artificial enamel lesions. Microsc Res Tech. 2019;82:1065–72. doi: 10.1002/jemt.23254. [DOI] [PubMed] [Google Scholar]
- 39.Varma V, Hegde KS, Bhat SS, Sargod SS, Rao HA. Comparative evaluation of remineralization potential of two varnishes containing CPP-ACP and Tricalcium phosphate: An in vitro study. Int J Clin Pediatr Dent. 2019;12:233–6. doi: 10.5005/jp-journals-10005-1629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Bayrak S, Tuloglu N, Bicer H, Sen Tunc E. Effect of fluoride varnish containing CPP-ACP on preventing enamel erosion. Scanning. 2017;2017:1897825. doi: 10.1155/2017/1897825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Choi HJ, Choi YC, Kim KC, Choi SC. Remineralization depth of CPP-ACP on demineralization human enamel in vitro. J Korean Acad Pediatr Dent. 2008;35:278–86. [Google Scholar]
- 42.Reynolds EC, Cain CJ, Webber FL, Black CL, Riley PF, Johnson IH, et al. Anticariogenicity of calcium phosphate complexes of tryptic casein phosphopeptides in the rat. J Dent Res. 1995;74:1272–9. doi: 10.1177/00220345950740060601. [DOI] [PubMed] [Google Scholar]
- 43.Reynolds EC. Anticariogenic complexes of amorphous calcium phosphate stabilized by casein phosphopeptides: A review. Spec Care Dentist. 1998;18:8–16. doi: 10.1111/j.1754-4505.1998.tb01353.x. [DOI] [PubMed] [Google Scholar]
- 44.Cross KJ, Huq NL, Stanton DP, Sum M, Reynolds EC. NMR studies of a novel calcium, phosphate and fluoride delivery vehicle-alpha (S1)-casein (59-79) by stabilized amorphous calcium fluoride phosphate nanocomplexes. Biomaterials. 2004;25:5061–9. doi: 10.1016/j.biomaterials.2004.01.045. [DOI] [PubMed] [Google Scholar]
- 45.Reynolds EC, Cai F, Cochrane NJ, Shen P, Walker GD, Morgan MV, et al. Fluoride and casein phosphopeptide-amorphous calcium phosphate. J Dent Res. 2008;87:344–8. doi: 10.1177/154405910808700420. [DOI] [PubMed] [Google Scholar]
- 46.Duraisamy V, Xavier A, Nayak UA, Reddy V, Rao AP. An in vitro evaluation of the demineralization inhibitory effect of F(-) varnish and casein phosphopeptide-amorphous calcium phosphate on enamel in young permanent teeth. J Pharm Bioallied Sci. 2015;7:S513–7. doi: 10.4103/0975-7406.163521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Morgan MV, Adams GG, Bailey DL, Tsao CE, Fischman SL, Reynolds EC. The anticariogenic effect of sugar-free gum containing CPP-ACP nanocomplexes on approximal caries determined using digital bitewing radiography. Caries Res. 2008;42:171–84. doi: 10.1159/000128561. [DOI] [PubMed] [Google Scholar]
- 48.Srinivasan N, Kavitha M, Loganathan SC. Comparison of the remineralization potential of CPP-ACP and CPP-ACP with 900 ppm fluoride on eroded human enamel: An in situ study. Arch Oral Biol. 2010;55:541–4. doi: 10.1016/j.archoralbio.2010.05.002. [DOI] [PubMed] [Google Scholar]
- 49.Shen P, Manton DJ, Cochrane NJ, Walker GD, Yuan Y, Reynolds C, et al. Effect of added calcium phosphate on enamel remineralization by fluoride in a randomized controlled in situ trial. J Dent. 2011;39:518–25. doi: 10.1016/j.jdent.2011.05.002. [DOI] [PubMed] [Google Scholar]
- 50.Obradović M, Dolić O, Sukara S, Vojinović J. The role of protective varnishes in the treatment of initial caries. Contemp Mater. 2016;7:93–8. [Google Scholar]
- 51.Cochrane NJ, Cai F, Huq NL, Burrow MF, Reynolds EC. New approaches to enhanced remineralization of tooth enamel. J Dent Res. 2010;89:1187–97. doi: 10.1177/0022034510376046. [DOI] [PubMed] [Google Scholar]
- 52.Picano L. Fluoride Varnishes: What is the Difference, and Which One is Best? Dental Economics. 2020. [Last accessed on 2021 Jul 10]. Available from: https://www.dentaleconomics.com/science-tech/ cosmetic-dentistry-and-whitening/article/14173399/fluoridevarnishes-what-is-the-difference-and-which-one-is-best .
- 53.Tewari A, Chawla HS, Utreja A. Comparative evaluation of the role of NaF, APF & Duraphat topical fluoride applications in the prevention of dental caries – A 2 ½ years study. J Indian Soc Pedod Prev Dent. 1991;8:28–35. [PubMed] [Google Scholar]
- 54.Munshi AK, Reddy NN, Shetty V. A comparative evaluation of three fluoride varnishes: An in-vitro study. J Indian Soc Pedod Prev Dent. 2001;19:92–102. [PubMed] [Google Scholar]
- 55.Huang GJ, Roloff-Chiang B, Mills BE, Shalchi S, Spiekerman C, Korpak AM, et al. Effectiveness of MI Paste Plus and PreviDent fluoride varnish for treatment of white spot lesions: A randomized controlled trial. Am J Orthod Dentofacial Orthop. 2013;143:31–41. doi: 10.1016/j.ajodo.2012.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Kashbour W, Gupta P, Worthington HV, Boyers D. Pit and fissure sealants versus fluoride varnishes for preventing dental decay in the permanent teeth of children and adolescents. Cochrane Database Syst Rev. 2020;11:CD003067. doi: 10.1002/14651858.CD003067.pub5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Chestnutt IG, Hutchings S, Playle R, Morgan-Trimmer S, Fitzsimmons D, Aawar N, et al. Seal or Varnish.A randomised controlled trial to determine the relative cost and effectiveness of pit and fissure sealant and fluoride varnish in preventing dental decay? Health Technol Assess. 2017;21:1–256. doi: 10.3310/hta21210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Zaror C, Muñoz-Millán P, Espinoza-Espinoza G, Vergara-González C, Martínez-Zapata MJ. Cost-effectiveness of adding fluoride varnish to a preventive protocol for early childhood caries in rural children with no access to fluoridated drinking water. J Dent. 2020;98:103374. doi: 10.1016/j.jdent.2020.103374. [DOI] [PubMed] [Google Scholar]
- 59.Neidell M, Shearer B, Lamster IB. Cost-effectiveness analysis of dental sealants versus fluoride varnish in a school-based setting. Caries Res. 2016;50(Suppl 1):78–82. doi: 10.1159/000439091. [DOI] [PubMed] [Google Scholar]
- 60.White DJ. The application of in vitro models to research on demineralization and remineralization of the teeth. Adv Dent Res. 1995;9:175–93. doi: 10.1177/08959374950090030101. [DOI] [PubMed] [Google Scholar]
- 61.White DJ, Faller RV, Bowman WD. Demineralization and remineralization evaluation techniques-added considerations. J Dent Res. 1992;71:929–33. doi: 10.1177/002203459207100S28. [DOI] [PubMed] [Google Scholar]