

Abstract
Background Acute facial nerve iatrogenic or traumatic injury warrants rapid management with the goal of reestablishing nerve continuity within 72 hours. However, reconstructive efforts should be performed up to 12 months from the time of injury since facial musculature may still be viable and thus facial tone and function may be salvaged.
Methods Data of all patients who underwent facial nerve repair following iatrogenic or traumatic injury were retrospectively collected and assessed. Paralysis etiology, demographics, operative data, postoperative course, and outcome were examined.
Results Twenty patients underwent facial nerve repair during the years 2004 to 2019. Data were available for 16 of them. Iatrogenic injury was the common category ( n = 13, 81%) with parotidectomy due to primary parotid gland malignancy being the common surgery ( n = 7, 44%). Nerve repair was most commonly performed during the first 72 hours of injury ( n = 12, 75%) and most of the patients underwent nerve graft repair ( n = 15, 94%). Outcome was available for 12 patients, all of which remained with some degree of facial paresis. Six patients suffered from complete facial paralysis (50%) and three underwent secondary facial reanimation (25%). There were no major operative or postoperative complications.
Conclusion Iatrogenic and traumatic facial nerve injuries are common etiologies of acquired facial paralysis. In such cases, immediate repair should be performed. For patients presenting with facial paralysis following previous surgery or trauma, nerve repair should be considered up to at least 6 months of injury. Longstanding paralysis is best treated with standard facial reanimation procedures.
Keywords: facial palsy, facial nerve injury, facial nerve trauma
Introduction
Facial nerve paralysis is a devastating condition with possible physical and psychosocial consequences. 1 2 3 4 5 The most common cause of acquired paralysis is Bell's palsy in which partial or complete recovery is expected in most cases. 1 Mechanical, irreversible damage to the facial nerve or its branches appears in iatrogenic and traumatic injuries and together these constitute the second most common cause of acquired facial paralysis. 6 7 8 This population of patients is highly heterogenous in terms of medical background, extent of paralysis, and accompanying facial insult (e.g., adjuvant radiotherapy or concomitant soft tissue damage). Such cases of acute disruption of the facial nerve have the possible advantage of direct repair of an anatomic disturbance allowing for preservation and restoration of facial nerve function. 9
Acute disruption of the facial nerve warrants rapid management with the primary goal of immediate repair. 6 9 10 11 Such injury is divided to acute (up to 72 hours), subacute (72 hours to 12–18 months), and longstanding (beyond 12–18 months). 1 6 Restoration of facial nerve continuity should optimally be performed in the acute phase; however, reconstruction may still be successfully performed up to 12 months from injury, since, during this period, facial muscles may still reanimate with neural stimulation. Longstanding damage is generally not amendable to nerve repair due to atrophy of the target facial musculature. The reconstructive approach is dictated by multiple factors including etiology and mechanism of injury, duration since palsy onset, patient age, comorbidities, risk factors, and patient's subjective needs and wishes.
In this article, we describe our experience with the management of acute facial nerve injury and assess operative and postoperative courses and outcome.
Methods
The study was approved by our Institutional Review Board (no. 0727–19-TLV). During 2004 to 2109, a total of 20 patients were treated for acute or subacute facial nerve injury at our department. All patients granted informed consent for the operative treatment. All reconstructions were performed by the senior author (E.G.). The majority of cases were treated in the framework of our collaboration with the ENT (ear–nose–throat) team at our institution. A retrospective cohort study was performed and data regarding demographic details, oncological background, etiology of facial nerve injury, timing of reconstruction, duration of follow-up, complications and outcome were assessed. Data were extracted from the medical center's computerized database. The authors declare conforming to the Declaration of Helsinki. Patients presented in this article granted informed consent for publication of their photographs.
Results
During 2004 to 2019, a total of 20 patients were treated for acute or subacute facial nerve damage ( Table 1 ). Data were available for 16 of them. The majority of patients were males ( n = 11, 69%), mean age at surgery was 44 years (range: 0.7–81 years), and paralysis was equally distributed between right and left sides ( n = 8, 50% each). Etiology of paralysis was iatrogenic injury in 13 cases (81%) and traumatic injury in 3 cases (19%). In the iatrogenic injury group, the most common surgery and indication were parotidectomy due to primary parotid gland tumor ( n = 7, 44%). These included five radical parotidectomies, one total parotidectomy, and one superficial parotidectomy. Other surgeries involved with iatrogenic facial nerve injury were microsurgical resection of acoustic schwannoma ( n = 2, 12%), mastoidectomy ( n = 1, 6%), hemimandibulectomy ( n = 1, 6%), resection of lymphangioma ( n = 1, 6%), and facelift ( n = 1, 6%). The cause of facial trauma was motor-vehicle accident in two patients (12%) and stab wound in one (6%). Operative and postoperative details are presented in Table 2 . Immediate repair (up to 72 hours of injury) was performed in 12 cases (75%), while repair was performed in the subacute phase (72 hours–6 months) in the reminder ( n = 4, 25%). The majority of repairs were performed using cable nerve graft/s ( n = 15, 94%) with the sural nerve being the most common donor nerve ( n = 12, 75%). Other donor nerves in this study included the greater auricular nerve ( n = 1, 6%), nerve to vastus lateralis ( n = 1, 6%), and an unnamed cervical nerve ( n = 1, 6%). One patient underwent immediate primary repair of the facial nerve ( n = 1, 6%). Four patients (25%) were treated with postoperative adjuvant radiation to the head and neck. There were no cases of intraoperative or postoperative major complications.
Table 1. Demographic and clinical details.
| n | % | Mean | Range | |
|---|---|---|---|---|
| Number of patients | 16 | 100 | ||
| Male gender | 11 | 69 | ||
| Side of paralysis: right | 8 | 50 | ||
| Age at insult/nerve repair (y) | 44.6 | 0.7–81 | ||
| Over 50 years old at nerve repair | 7 | 44 | ||
| Smoking a | 1 | 6 | ||
| Etiology of paralysis | ||||
| Head and neck oncologic surgery | 12 | 69 | ||
| Parotidectomy b | 7 | 44 | ||
| Acoustic schwannoma c | 2 | 12 | ||
| Mastoidectomy | 1 | 6 | ||
| Mandibulectomy d | 1 | 6 | ||
| Resection of lymphangioma | 1 | 6 | ||
| Facial trauma | 3 | 19 | ||
| Facelift | 1 | 6 | ||
| Indication for head and neck surgery | ||||
| Pleomorphic adenoma of parotid gland | 2 | |||
| Mucoepidermoid carcinoma of parotid gland | 2 | |||
| Schwannoma | 2 | |||
| Undetermined parotid malignancy | 1 | |||
| Merkel cell carcinoma | 1 | |||
| Squamous cell carcinoma | 1 | |||
| Lymphangioma | 1 | |||
| Osteoradionecrosis of mandible | 1 | |||
| Cholesteatoma | 1 | |||
| Facial paralysis a | ||||
| Complete | 8 | 53 | ||
| Incomplete | 7 | 47 | ||
| Previous head and neck radiotherapy a | 3 | 20 | ||
Data available for 15 patients.
Five radical parotidectomies, one total parotidectomy, and one superficial parotidectomy.
1 microsurgical resection, 1 microsurgical resection with superficial parotidectomy.
Extended hemimandibullectomy.
Table 2. Operative and postoperative courses.
| n | % | Mean | Median | |
|---|---|---|---|---|
| Timing of repair | ||||
| < 72 hours | 12 | 75 | ||
| 72 hours–6 months | 4 | 25 | ||
| > 6 months | 0 | 0 | ||
| Repair | ||||
| Nerve graft | 15 | 94 | ||
| Sural nerve graft | 12 | 75 | ||
| Other a | 3 | 18 | ||
| Primary repair | 1 | 6 | ||
| Number of nerve grafts | ||||
| One | 6 | 37 | ||
| One graft split to two | 3 | 18 | ||
| One graft split to three | 1 | 6 | ||
| Two | 1 | 6 | ||
| Three or more | 5 | 31 | ||
| Three grafts split to four | 2 | 12 | ||
| Missing data | 2 | 12 | ||
| Intraoperative complications | 0 | 0 | ||
| Follow-up (mo) b | 39 | 6–111 | ||
| Postoperative radiation b | 4 | 33 | ||
| Postoperative complications b | 0 | 0 | ||
| Postoperative facial paralysis b | ||||
| Incomplete | 6 | 50 | ||
| Complete | 6 | 50 | ||
| Synkinesis b | 6 | 50 | ||
| Secondary facial reanimation b | 3 | 25 | ||
One greater auricular nerve, one cervical unnamed nerve, and one nerve to vastus lateralis.
Available for 12 patients.
Documentation of clinical outcome was available for 12 patients ( Table 3 ). In this subgroup, mean duration of follow-up was 44 months (range: 12–111 months). Average age at reconstruction was 38.7 years (range: 7 months–70 years). The majority of patients underwent repair using nerve grafts ( n = 11, 92%). The average number of facial nerve branches repaired was 3.5 (range: 1–6) and average gap length was 7.7 cm (range: 4–14 cm). Postoperative outcome showed some degree of restoration of facial nerve function in six patients (50%). This ranged from near-normal activity in one patient (8%) and some degree of incomplete facial paralysis in five (42%). Synkinesis was observed in six patients (50%). In the reminder of patients, complete facial paralysis was observed, however, with fair static facial symmetry ( n = 6, 50%). In total, three patients underwent secondary facial reanimation with free muscle transfer (25%).
Table 3. Breakdown of operative data and patient outcome.
| No. | Gender | Side | Etiology | Extent of paralysis/damage | Timing of reconstruction | Age (y) | Injured territory | Type of repair | Number of segments reconstructed | Gap length (cm) | Result | Synkinesis | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | Left | Iatrogenic | Radical parotidectomy | Incomplete | Immediate | 34 | BZ | Nerve grafting | 2 | Middle trunk of FN coapted to two BZ branches via one nerve graft split to two | Missing | Incomplete facial paralysis | Yes |
| 2 | Male | Left | Iatrogenic | Radical parotidectomy | Complete | Immediate | 10 | Complete | Nerve grafting | 4 | Four branches reconstructed with four nerve grafts | 4 | Incomplete facial paralysis | Yes |
| 3 | Male | Right | Iatrogenic | Lymhpangioma resection | Complete | Immediate | 0.7 | Complete | Nerve grafting | 2 | Proximal FN stump coapted to two main FN trunks via one nerve graft split to two | 7 | Complete facial paralysis with good static symmetry | No |
| 4 | Female | Left | Iatrogenic | Radical parotidectomy | Complete | Immediate | 44 | Complete | Nerve grafting | 4 | Proximal FN stump coapted to four distal FN branches: TP, BZ, MM territory | Missing | Complete facial paralysis with good static symmetry | No |
| 5 | Female | Left | Iatrogenic | Schwannoma resection and partial parotidectomy | Complete | Immediate | 36 | Complete | Nerve grafting | 1 | Proximal FN stump coapted by nerve graft | 5 | Incomplete facial paralysis | Yes |
| 6 | Male | Right | Iatrogenic | Radical parotidectomy | Complete | Immediate | 69 | Complete | Nerve grafting | 2 | Proximal FN stump coapted to two distal branches | Missing | Complete facial paralysis with good static symmetry | No |
| 7 | Male | Left | Iatrogenic | Radical parotidectomy | Complete | Immediate | 59 | Complete | Nerve grafting | 3 | Proximal FN stump coapted to four distal FN branches: TP and BZ territory | 12 | Complete facial paralysis with good static symmetry | No |
| 8 | Male | Left | Trauma | Motor vehicle accident | Incomplete | Immediate | 8 | BZ | Nerve grafting | Missing | Missing | Missing | Complete facial paralysis with good static symmetry | No |
| 9 | Male | Right | Trauma | Motor vehicle accident | Incomplete | Immediate | 16 | BZ, FR | Nerve grafting | 6 | Six branches reconstructed with six nerve grafts | 4 | Near normal facial nerve function | Yes |
| 10 | Male | Left | Iatrogenic | Microsurgical resection of acoustic schwannoma | Incomplete | Subacute: 12 weeks | 70 | BZ, MM | Nerve grafting | 5 | Five branches reconstructed with five nerve grafts | 14 | Complete facial paralysis with good static symmetry | Yes |
| 11 | Male | Right | Iatrogenic | Extended hemimandibulectomy | Complete | Subacute: 24 weeks | 51 | Complete | Nerve grafting | 4 | Two proximal FN trunks coapted to four distal branches | 8 | Incomplete facial paralysis | Yes |
| 12 | Female | Right | Iatrogenic | Facelift | Incomplete | Subacute: 24 weeks | 67 | BZ | Primary repair | 5 | Five BZ FN branches reconstructed with five nerve grafts | NA | Incomplete facial paralysis | No |
Abbreviations: BZ, buccozygomatic; FN, facial nerve; FR, frontal; MM, marginal mandibular; NA, nonapplicable; TP, temporal.
Discussion
Video 1 Preoperative video of the patient presented in Fig. 2 . Note incomplete right facial nerve paralysis involving mainly temporal and buccozygomatic branches.
Video 2 Postoperative video of the patient presented in Fig. 2 . Note improved facial nerve function and facial symmetry.
The two main etiological groups of facial nerve injury leading to nerve disruption are traumatic and iatrogenic damage 8 10 ( Figs. 1 and 2 ). Traumatic facial paralysis may result from blunt or penetrating trauma and is usually secondary to motor-vehicle accidents or assault (e.g., stab or gunshot wounds and animal bites). 6 10 The incidence of iatrogenic facial nerve injury varies widely between reports and is dependent on multiple factors (e.g., type of surgical procedure, previous intervention or insult, anatomical variants, and others). Surgical procedures that put the facial nerve in risk include oral and maxillofacial surgery, head and neck oncologic surgery, temporomandibular joint surgery, otologic surgery, Mohs surgery, and cosmetic facial surgery. 2 3 7 8 9 12
Fig. 1.
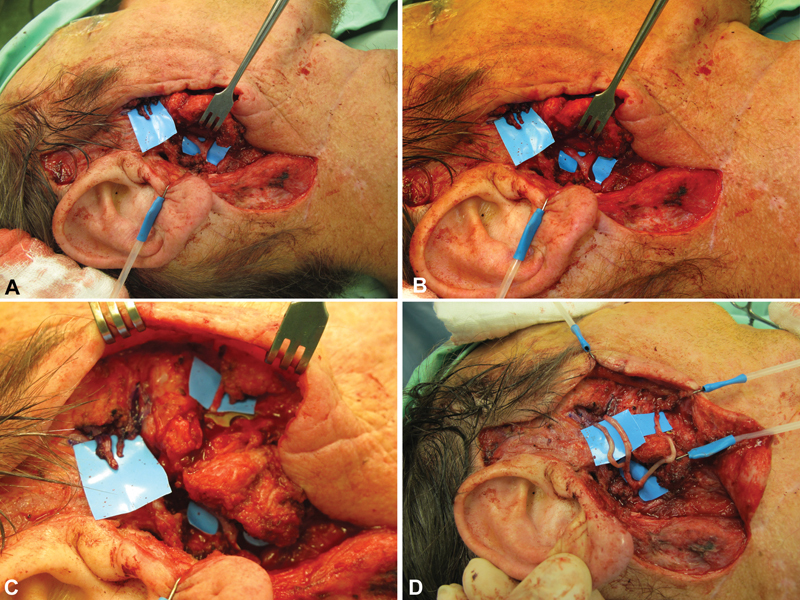
A 51-year-old male with iatrogenic facial nerve injury following hemimandibulectomy. Facial nerve repair was performed 24 weeks following injury. A sural nerve graft was harvested and used as three interpositional nerve grafts for reconstruction of temporal and buccozygomatic branches. ( A–C ) Facial nerve's division into two main trunks with the parotid gland where it was found cut, and three distal branches. ( D ) Following facial nerve repair using nerve grafts.
Fig. 2.

A 16-year-old male with facial nerve traumatic injury following a motor vehicle accident. The patient arrived at our department 24 hours following the injury and was operated on immediately. On admission he presented with incomplete right facial paralysis involving mainly temporal and buccozygomatic branches. Due to extensive soft tissue and facial nerve damage, primary repair was not possible. A sural nerve graft was harvested and used for 6 interpositional nerve grafts. ( A ) Preoperative photo. ( B, C ) Intraoperative photos following debridement and exploration. Several facial nerve branches were found and marked with a surgical pen. ( D, E ) Following multiple cable graft repair and wound closure.
Immediate nerve repair (up to 72 hours of injury) should be considered whenever facial nerve continuity is disrupted, either in planned oncologic resections, unplanned damage during surgery, or in the acute setting of facial trauma. This is said to provide the best chance of preserving facial form and function. 1 2 6 8 9 13 14 During the acute phase, repair may be performed by primary neurorrhaphy or via interpositional nerve graft/s according to the mechanism of injury and other local considerations (e.g., soft tissue damage, extent of nerve damage, hardware, and others). This allows for early reestablishment of facial tone and aids to preserve static symmetry. In our cohort, the majority of cases of immediate repair were reconstructed using nerve grafts since the ablative surgery required partial excision of the nerves thus not allowing tension-free primary repair. The sural nerve is most commonly used as donor nerve; however, other options exist including the greater auricular nerve, medial or lateral cutaneous antebrachial nerves, thoracodorsal nerve, and nerve to vastus lateralis. 2 13 Subacute injury to the facial nerve is ill defined and includes a timeframe between 72 hours and up to 18 months as of injury. During this period, intraoperative assessment of distal facial nerve branches is difficult due to the Wallerian degeneration; however, facial target muscle may still be viable. 6 15 Nerve repair during the subacute phase may not be amendable to primary repair due to scarring and remodeling of surrounding tissue and interposition nerve graft/s are used, taking into account the zone of injury, gap length, and distance from nerve to muscle. 6
In our cohort, the most common etiology for paralysis was iatrogenic injury during surgery for parotid gland malignancy. The incidence of permanent facial nerve paralysis following parotidectomy ranges between 0 and 17% in most reports and is dependent on various factors including tumor size, location, and preoperative facial paresis and/or pain. 16 17 Radical parotidectomy includes sacrifice of the facial nerve by definition and is reserved for advanced parotid malignancies. However, the facial nerve may also be injured in total or superficial parotidectomies. In such cases, immediate repair using nerve grafts has been shown to produce good results with high degree of movement restoration following the inevitable facial weakness that appears after surgery. 2 7 13 18 19 Facial nerve injury during otologic surgery is rare (0.5–3.5%) and early exploration and repair is performed according to the principals described above. 12 Microsurgical resection of vestibular schwannomas is associated with 8 to 10% incidence of permanent facial nerve paralysis or paresis. In cases of intraoperatively identified facial nerve transection, immediate nerve grafting is said to provide the best long-term outcome. 20 In some cases, facial weakness may be observed postoperatively without intraoperative evidence of injury. Early exploration within 72 hours is recommended and repair performed if nerve disruption is identified. In case the facial nerve is found to be intact, close follow-up is advised as facial function may recover; however, if not, facial reanimation procedures designed to preserve the native facial musculature should be performed within a 6-month timeframe. 21 Adjuvant radiotherapy may be indicated following head and neck oncological surgery and, to date, there is no evidence that such treatment interferes with neural regeneration. Therefore planned postoperative irradiation should not exclude patients from immediate nerve repair or grafting, and facial nerve repair should not postpone adjuvant treatment. 2 8 18 22
Traumatic facial nerve injuries may be more difficult to manage, as the exact location and magnitude of injury is difficult to determine. Blunt trauma due to fracture of the temporal bone is the most common cause of traumatic facial nerve injury. 6 10 In cases of acute extracranial facial nerve trauma with intact facial musculature, primary neurorrhaphy is the treatment of choice. Tension-free nerve coaptation is critical for successful facial nerve recovery and when a gap of more than 2 cm between nerve endings exists, interposition nerve grafting is indicated. When there is no proximal facial nerve stump to act as donor nerve (intracranial or severe proximal injury), immediate reanimation of facial musculature may be attempted using regional nerve transposition. If concomitant facial musculature damage is observed, reestablishing facial nerve continuity is not expected to salvage facial mimetic function and these cases usually render secondary facial reanimation procedures. Static procedures may be performed at initial exploration to conserve facial symmetry at this early point. 10 23 Some cases of acute traumatic facial nerve injury may be initially managed by expectant observation and these include incomplete paralysis, delayed onset of paralysis, paralysis following blunt facial injury, and distal damage (e.g., medial to the lateral canthus). Such cases may represent type I (neuropraxia) or type II (axonotmesis) nerve injury, and spontaneous recovery is possible. Close medical follow-up is appropriate with surgical intervention reserved for patients not improving within 6 months of injury. 10 24
Our results provide a view of the wide range of patients and clinical scenarios in which facial nerve disruption may be encountered. Such injury creates inevitable facial weakness and the main goal of early intervention is to preserve as much of the native neural course and facial mimetic function as possible. Outcome was assessed for 12 patients since several patients were oncologically treated and followed in other medical centers. Moreover, we could not perform objective facial function assessment due to the retrospective nature of the study, and since these were not routinely documented for all patients. Outcome is therefore based on the subjective description of the senior author during follow-up visits. All patients in our cohort suffered from some degree of facial paralysis following repair; however, static symmetry and facial tone were satisfactory in all patients. This is most probably due to the rapid reestablishment of facial muscles' neurotization which prevented facial muscle atrophy and in turn provided better postoperative esthetics and some degree of salvaged facial function. We feel that this by itself justifies the reconstructive efforts for repair up to at least 6 months postinjury, as it may also prevent some of the facial paralysis symptomatology such as drooling, eating disturbances, and lack of corneal protection. One patient regained near-normal facial function ( Fig. 2 ; Videos 1 and 2 ). This was a 16-year-old male who suffered from acute transection of frontal, zygomatic and buccal branches of the facial nerve due to facial trauma in a motor-vehicle accident. He underwent repair 24 hours following injury with six interpositional nerve grafts. Nerve grafts were used instead of primary repair since the nerve endings were injured and large gaps were created following debridement of nonviable tissue. Of note, three of the patients who were followed-up underwent repair in the subacute phase. Two of them remained with incomplete paralysis (66%) and one with a complete paralysis (33%). Among the nine patients who underwent immediate repair, four patients regained some degree of facial nerve function ranging from near-normal activity to incomplete facial paralysis (45%) and five remained with complete facial paralysis (55%). This small sample size does not allow to compare the clinical outcome between the groups; however, it suggests that salvage of facial nerve function may be achieved up to at least 24 weeks postinjury. A total of three patients underwent secondary dynamic facial reanimation with a free gracilis muscle transfer, two of which due to complete facial paralysis and one due to incomplete facial paralysis. Synkinesis is a common problem in facial nerve repair and indeed 50% of the patients who underwent assessment had documented synkinesis. These are the same patients who showed improved facial function, so in fact all patients who regained or preserved facial function did have postoperative synkinesis. This appears due to aberrant nerve sprouting and is more severe in proximal defects. This problem is difficult to prevent, and in our institution is mainly dealt by postoperative botulinum toxin injections. Our results demonstrate that facial nerve repair is safe, as no operative or postoperative complications were seen.
Our study has several limitations. This is a retrospective chart review examining a relatively small number of patients, highly heterogenous in demographics and operative data. Patients had no objective facial paralysis scoring, thus outcome was assessed primarily by a retrospective review of medical documents with subjective assessment of facial function.
In conclusion, facial nerve iatrogenic and traumatic injury is a common cause of acquired facial paralysis. According to our experience and the literature, acute and subacute facial nerve injuries should be treated with immediate exploration and facial nerve repair with the goal of treatment during the first 72 hours of injury. However, reconstructive efforts should be performed up to at least 6 months of injury. This approach improves postoperative facial nerve function and may salvage facial musculature tone. In case facial nerve repair does not provide satisfactory facial function, secondary facial reanimation may still be performed.
Author Contributions
All authors have contributed to the study design, drafting, and reviewing of the manuscript and have approved its submission.
Funding Statement
Funding None.
Conflict of Interest E.G. is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Ethical Statement
The authors declare conforming to the Declaration of Helsinki (local Institutional Review Board no.: 0727–19-TLV).
Patient Consent
All patients granted informed consent for the operative treatment.
References
- 1.Fattah A, Borschel G H, Manktelow R T, Bezuhly M, Zuker R M. Facial palsy and reconstruction. Plast Reconstr Surg. 2012;129(02):340e–352e. doi: 10.1097/PRS.0b013e31823aedd9. [DOI] [PubMed] [Google Scholar]
- 2.Ciolek P J, Prendes B L, Fritz M A. Comprehensive approach to reestablishing form and function after radical parotidectomy. Am J Otolaryngol. 2018;39(05):542–547. doi: 10.1016/j.amjoto.2018.06.008. [DOI] [PubMed] [Google Scholar]
- 3.Yawn R J, Wright H V, Francis D O, Stephan S, Bennett M L. Facial nerve repair after operative injury: impact of timing on hypoglossal-facial nerve graft outcomes. Am J Otolaryngol. 2016;37(06):493–496. doi: 10.1016/j.amjoto.2016.05.001. [DOI] [PubMed] [Google Scholar]
- 4.Roy M, Corkum J P, Shah P S et al. Effectiveness and safety of the use of gracilis muscle for dynamic smile restoration in facial paralysis: a systematic review and meta-analysis. J Plast Reconstr Aesthet Surg. 2019;72(08):1254–1264. doi: 10.1016/j.bjps.2019.05.027. [DOI] [PubMed] [Google Scholar]
- 5.Saadi R, Shokri T, Schaefer E, Hollenbeak C, Lighthall J G. Depression rates after facial paralysis. Ann Plast Surg. 2019;83(02):190–194. doi: 10.1097/SAP.0000000000001908. [DOI] [PubMed] [Google Scholar]
- 6.Brown S, Isaacson B, Kutz W, Barnett S, Rozen S M. Facial nerve trauma: clinical evaluation and management strategies. Plast Reconstr Surg. 2019;143(05):1498–1512. doi: 10.1097/PRS.0000000000005572. [DOI] [PubMed] [Google Scholar]
- 7.Hohman M H, Bhama P K, Hadlock T A. Epidemiology of iatrogenic facial nerve injury: a decade of experience. Laryngoscope. 2014;124(01):260–265. doi: 10.1002/lary.24117. [DOI] [PubMed] [Google Scholar]
- 8.Györi E, Mayrhofer M, Schwaiger B M, Pona I, Tzou C H. Functional results after facial reanimation in iatrogenic facial palsy. Microsurgery. 2019;40(02):145–153. doi: 10.1002/micr.30478. [DOI] [PubMed] [Google Scholar]
- 9.Owusu J A, Stewart C M, Boahene K. Facial nerve paralysis. Med Clin North Am. 2018;102(06):1135–1143. doi: 10.1016/j.mcna.2018.06.011. [DOI] [PubMed] [Google Scholar]
- 10.Lee L N, Lyford-Pike S, Boahene K D. Traumatic facial nerve injury. Otolaryngol Clin North Am. 2013;46(05):825–839. doi: 10.1016/j.otc.2013.07.001. [DOI] [PubMed] [Google Scholar]
- 11.Gur E, Stahl S, Barnea Y et al. Comprehensive approach in surgical reconstruction of facial nerve paralysis: a 10-year perspective. J Reconstr Microsurg. 2010;26(03):171–180. doi: 10.1055/s-0029-1242139. [DOI] [PubMed] [Google Scholar]
- 12.Linder T, Mulazimoglu S, El Hadi T et al. Iatrogenic facial nerve injuries during chronic otitis media surgery: a multicentre retrospective study. Clin Otolaryngol. 2017;42(03):521–527. doi: 10.1111/coa.12755. [DOI] [PubMed] [Google Scholar]
- 13.Biglioli F, Tarabbia F, Allevi F et al. Immediate facial reanimation in oncological parotid surgery with neurorrhaphy of the masseteric-thoracodorsal-facial nerve branch. Br J Oral Maxillofac Surg. 2016;54(05):520–525. doi: 10.1016/j.bjoms.2016.02.014. [DOI] [PubMed] [Google Scholar]
- 14.Constantinidis J, Akbarian A, Steinhart H, Iro H, Mautes A. Effects of immediate and delayed facial-facial nerve suture on rat facial muscle. Acta Otolaryngol. 2003;123(08):998–1003. doi: 10.1080/00016480310001853. [DOI] [PubMed] [Google Scholar]
- 15.Salmerón-González E, Simón-Sanz E, García-Vilariño E, García-Sánchez J M, Ruiz-Cases A. Masseter-to-facial nerve transfer for reanimation of a patient with long-term facial paralysis. J Craniofac Surg. 2019;30(01):e43–e45. doi: 10.1097/SCS.0000000000004957. [DOI] [PubMed] [Google Scholar]
- 16.Swendseid B, Li S, Thuener J et al. Incidence of facial nerve sacrifice in parotidectomy for primary and metastatic malignancies. Oral Oncol. 2017;73:43–47. doi: 10.1016/j.oraloncology.2017.07.029. [DOI] [PubMed] [Google Scholar]
- 17.Venkatesh S, Srinivas T, Hariprasad S. Parotid gland tumors: 2-year prospective clinicopathological study. Ann Maxillofac Surg. 2019;9(01):103–109. doi: 10.4103/ams.ams_179_18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hontanilla B, Qiu S S, Marré D. Effect of postoperative brachytherapy and external beam radiotherapy on functional outcomes of immediate facial nerve repair after radical parotidectomy. Head Neck. 2014;36(01):113–119. doi: 10.1002/hed.23276. [DOI] [PubMed] [Google Scholar]
- 19.Volk G F, Pantel M, Streppel M, Guntinas-Lichius O. Reconstruction of complex peripheral facial nerve defects by a combined approach using facial nerve interpositional graft and hypoglossal-facial jump nerve suture. Laryngoscope. 2011;121(11):2402–2405. doi: 10.1002/lary.22357. [DOI] [PubMed] [Google Scholar]
- 20.Kaul V, Cosetti M K. Management of vestibular schwannoma (including NF2): facial nerve considerations. Otolaryngol Clin North Am. 2018;51(06):1193–1212. doi: 10.1016/j.otc.2018.07.015. [DOI] [PubMed] [Google Scholar]
- 21.Yawn R J, Dedmon M M, Xie D et al. Delayed facial nerve paralysis after vestibular schwannoma resection. J Neurol Surg B Skull Base. 2019;80(03):283–286. doi: 10.1055/s-0038-1669941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zhu Y, Zhou S, Xu W, Liu L, Lu H, Yang W. Effects of postoperative radiotherapy on vascularized nerve graft for facial nerve repair in a rabbit model. J Oral Maxillofac Surg. 2019;77(11):2339–2346. doi: 10.1016/j.joms.2019.04.012. [DOI] [PubMed] [Google Scholar]
- 23.White H, Rosenthal E. Static and dynamic repairs of facial nerve injuries. Oral Maxillofac Surg Clin North Am. 2013;25(02):303–312. doi: 10.1016/j.coms.2013.02.002. [DOI] [PubMed] [Google Scholar]
- 24.Sunderland S. The anatomy and physiology of nerve injury. Muscle Nerve. 1990;13(09):771–784. doi: 10.1002/mus.880130903. [DOI] [PubMed] [Google Scholar]