

ABSTRACT
Retail food environments (RFEs) are complex systems with important implications for population health. Studying the complexity within RFEs comes with challenges. Complex systems models are computational tools that can help. We performed a systematic scoping review of studies that used complex systems models to study RFEs for population health. We examined the purpose for using the model, RFE features represented, extent to which the complex systems approach was maximized, and quality and transparency of methods employed. The PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) guidelines were followed. Studies using agent-based modeling, system dynamics, discrete event simulations, networks, hybrid, or microsimulation models were identified from 7 multidisciplinary databases. Fifty-six studies met the inclusion criteria, including 23 microsimulation, 13 agent-based, 10 hybrid, 4 system dynamics, 4 network, and 2 discrete event simulation models. Most studies (n = 45) used models for experimental purposes and evaluated effects of simulated RFE policies and interventions. RFE characteristics simulated in models were diverse, and included the features (e.g., prices) customers encounter when shopping (n = 55), the settings (e.g., restaurants, supermarkets) where customers purchase food and beverages (n = 30), and the actors (e.g., store managers, suppliers) who make decisions that influence RFEs (n = 25). All models incorporated characteristics of complexity (e.g., feedbacks, conceptual representation of multiple levels), but these were captured to varying degrees across model types. The quality of methods was adequate overall; however, few studies engaged stakeholders (n = 10) or provided sufficient transparency to verify the model (n = 12). Complex systems models are increasingly utilized to study RFEs and their contributions to public health. Opportunities to advance the use of these approaches remain, and areas to improve future research are discussed. This comprehensive review provides the first marker of the utility of leveraging these approaches to address RFEs for population health.
Keywords: food environment, healthy retail, nutrition interventions, systematic review, agent-based modeling, system dynamics, simulation, microsimulation, networks
Statement of Significance: This is the first review to synthesize and evaluate the use of complex systems models (e.g., agent-based, system dynamics, network, and discrete event simulation models) to study retail food environments for addressing population health.
Introduction
Unhealthy diet is a leading cause of mortality worldwide (1), and federal and private budgets are burdened by growing health care expenditures for diet-related chronic disease (2). Pronounced disparities in access to healthy, affordable foods have been documented in retail food environments (RFEs) of economically deprived, Black, indigenous, and people of color (BIPOC), and other marginalized communities (3–7). Some evidence also suggests associations between health behaviors and unhealthy RFE neighborhoods (8–10) as well as links between consumer-level RFE features, such as product placement, and the healthfulness of customer purchases (11–15). However, inconsistent relations between RFEs and health in the literature exist (16–18), which may reflect a limited consideration of the complexity of RFEs in prior research.
Local RFEs and their impact on health have historically been investigated using observational research designs and analytic methods such as regression modeling. Although customary, such approaches are limited when examining both the complexity of RFEs as well as their impacts on health. In particular, RFEs are multilayered, bridge numerous disciplines, and span an array of settings (e.g., grocery stores), modalities (e.g., online ordering), products, and other characteristics (e.g., prices) (19). Underlying these complexities are also a multitude of interrelations between factors, which may be dynamic, reciprocal, and interdependent, and together may be better understood as a system (20, 21). Although traditional statistical approaches are useful for many research questions, they often prioritize identifying average effects of an isolated relation (22–24), making them ineffective in capturing the holistic interconnectedness within a system. Further, as complex systems are not easily explained by studying their individual parts (25), additional methods are necessary to study the links between RFEs and health.
A set of methods that has received growing attention in this area is complex systems computational modeling. Complex systems modeling involves a series of diverse computational tools that capture the nature of a system, including its processes, behavior, and evolution (20, 26). These approaches are well-suited for capturing various dimensions of dynamic systems and population-level patterns that emerge from them (20, 21, 23), and their use is increasingly encouraged by health and scientific authorities (27, 28). In addition, as many of these approaches involve the use of simulations, they can be leveraged to estimate future effects of proposed policies and interventions (29), augmenting the retrospective (i.e., “has happened”) knowledge gained from traditional study designs. Examining such “what if” scenarios and other forms of complexity could help facilitate additional insights necessary to inform policy and health efforts to improve RFEs and address diet-related chronic disease.
In this review, we focused on 6 specific approaches of complex systems computational modeling. Although variation remains in what is considered the core approaches (22, 24–26, 29–32), for this review we considered complex systems approaches to include agent-based models (ABM), system dynamics (SD), discrete event simulations (DESs), networks, and any hybrid of the above. We also include the approach of microsimulation, given its similarities to ABM (22, 26, 29). Both similarities and differences exist in the ways each approach handles complex systems, which are described in Table 1.
TABLE 1.
Descriptions of the modeling approaches included in the review of studies using complex systems models to study retail food environments for population health
| Model approach | Description |
|---|---|
| System dynamics models | An aggregate- (versus individual-) level modeling approach that uses specific techniques (e.g., differential equations, state variables, stocks and flows) to capture and understand endogenous sources of complex system behavior. It centers on the principles of feedbacks and accumulation and is well-suited to simulating and capturing a macroscopic view of system behavior in large populations (24–26, 30, 31) |
| Discrete event simulations | Simulations with individual actors that are passive entities whose behavior is modeled as a sequence of discrete events in a setting over time. In this approach, events are the priority over the individual entities. Models are commonly used to examine resources and system constraints in meeting a target, and health sciences often use these to determine patient flows through clinical care settings (25, 26, 31) |
| Network analyses | Models with individual entities (e.g., people, organizations) that measure and analyze the relations and/or flows among them. Models can be used to analyze the network structure as well as how the transfer of information, behaviors, or diseases across connections change as relations for each individual entity change (23–25, 30) |
| Agent-based models | Simulations with individual actors (i.e., agents) that are active entities which make decisions and/or behave based on a set of rules. Individual actors may interact with each other and their environment and can adapt to these interactions producing emergent properties of the system that make them effective at capturing complex social phenomena (22–24, 31) |
| Microsimulations | Simulations with individual actors that are passive entities without interactions. Experiments often modify the attribute(s) of individual actors to understand the effect the change has on an individual over time. Common method in the economics field and tends to focus on estimating the detailed predictions of a specific policy/intervention on a target outcome as well as determining its cost-effectiveness (22, 23) |
| Hybrid models | Combined use of 2 or more model approaches in the same simulation. Offers the advantage of balancing the strengths and shortfalls of each approach to improve the effectiveness of a model in capturing aspects of a complex system (26, 31) |
Prior reviews have examined the use of complex systems methods to study noncommunicable chronic disease, obesity, and health behavior (25, 33–35). Yet, to our knowledge, no prior review has examined the contributions of these approaches to understanding the specific role of RFEs in population health. Thus, the purpose of this systematic review was to examine research to date that used a complex systems computational modeling approach to study the RFE for population health. We focused on addressing the following questions: why was the model used (i.e., model purpose); what RFE characteristics were included in the model and to what breadth; to what extent were use of complex systems approaches maximized (i.e., models included complexity characteristics, such as feedback loops, that distinguish them from statistical models); and what was the quality of modeling methods employed? We conclude by summarizing the strengths observed in the use of these approaches and by identifying areas of improvement for nutrition research to fully benefit from them when investigating how RFEs could improve population health.
Methods
We performed a systematic scoping review due to the multidisciplinary nature of studying RFEs and our broad research questions. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Guidelines for Scoping Reviews (36) to conduct the review and analysis. Prior to executing our search strategies, we developed a review protocol (Supplemental Methods A), including objectives, inclusion criteria, and methods. Investigators agreed upon iterative changes to the methodology, and we present the final strategy below.
Search strategy
Guided by the team, a university public health librarian (SH) created the search strategy for 7 databases: MEDLINE via Ovid, PsycINFO, AGRICOLA, CAB Abstracts, Business Source Premier, PAIS Index, and Scopus. These databases represent literature from multiple relevant disciplines, such as medicine, public health, psychology, agriculture/food, business, and public policy. The searches were run from March to April 2020, and there were no publication date restrictions used in the search.
Supplemental Methods B details the full electronic search strategies. The final search strategy was developed based on results of preliminary searches in MEDLINE via Ovid, team input, and keywords and phrases from relevant articles known in the literature (37–47). Terminology focused on 2 concepts: retail food environment and complex systems approaches. The search was designed to be specific to identify the 6 complex systems modeling approaches, while more comprehensive to identifying RFE concepts.
To capture citations missed by electronic searches, we performed hand searching methods in October–November 2020. We reviewed reference lists (backward search) and performed citation searches (forward search) of all included studies, and reviewed reference lists of key literature reviews (33, 34, 48–53).
Study selection
Studies were included if: 1) published in English; 2) empirical in nature (i.e., an empirical research study with results); 3) published in an academic journal; 4) implemented or developed an SD, DES, network, ABM, hybrid, or microsimulation model that included an aspect of the local or regional RFE; 5) studied the RFE aspect in a high-income (54) and/or Organization for Economic Co-operation and Development (OECD) country (55); and 6) studied a diet-related behavior or noncommunicable disease (e.g., food purchases, obesity) or otherwise were explicitly specified as related to population health. We limited studies to high-income and/or OECD countries to capture RFEs operating in similar economic and trade environments. Concepts from the Retail Food Environment and Customer Interaction framework (19) were used to guide the RFE aspects that met inclusion criteria. These included RFE settings where people purchase food/beverage products (e.g., stores, restaurants); the RFE features customers experience once at a setting (e.g., price, product availability, promotion); and/or the people who make decisions that influence the RFE (e.g., store managers, distributors) (19).
Studies were excluded if they: 1) only studied food safety (e.g., acute foodborne illness) or alcohol retail; 2) did not study the RFE separately from other environments (e.g., examined an overall built environment); 3) were the wrong publication type (i.e., literature review); or 4) involved nonhuman research.
Duplicate studies were removed, and items were uploaded to Rayyan (56), a web application for independent title/abstract screening. Screeners (MW, YM, MT) first tested screening agreement and then completed independent title/abstract screening once adequate agreement was reached (i.e., 85% on 20 records). Each title/abstract record was independently screened by 2 reviewers, and disagreements were resolved through discussion. Two screeners, then, independently reviewed full texts against eligibility criteria and resolved discrepancies through discussion. Figure 1 presents the study selection flow and reasons for exclusion.
FIGURE 1.
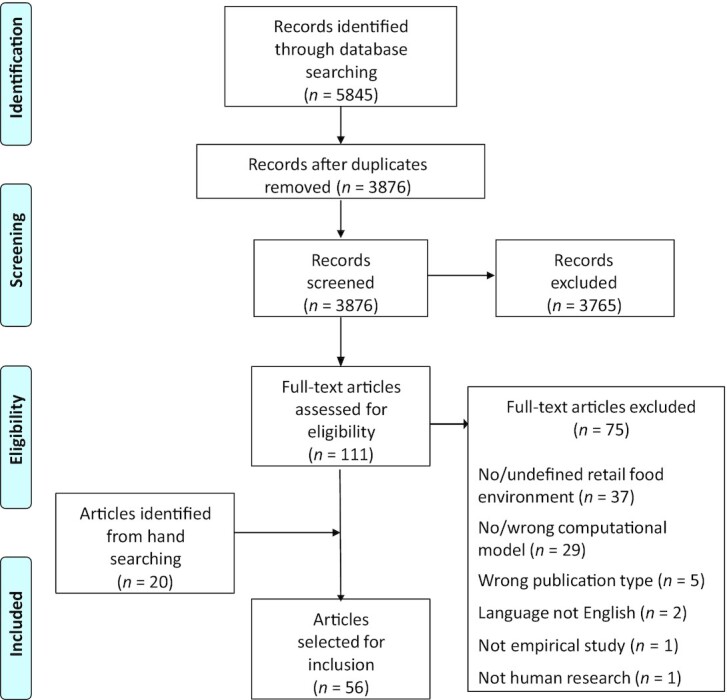
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) study selection flow diagram of studies using complex systems models to study retail food environments for population health.
Data extraction and transparency evaluation
Data were extracted from included articles and their published supplemental materials. Data were charted into a matrix using Microsoft Excel, following a list of definitions and guidelines for all items (Supplemental Methods C). Initial documents were informed by prior systems science literature reviews (23, 34) and then trialed by MW, YM, and MT on 5 articles that used different modeling approaches. Documents were refined based on inconsistencies and additional feedback sought and incorporated from the study team. Reviewers then assessed independent data extraction agreement, and once adequate (i.e., 85% across 5 additional articles), independently extracted the remaining articles with a second person verifying.
Although assessing study quality is not generally part of scoping reviews (36), insights from complex systems computational approaches may be most useful if trustworthy practices are used in the modeling process and made transparent in the publication (57–60). Thus, we assessed the transparency of each study using 10 items inspired by Jalali et al. (58, 59) (Supplemental Table 1). All included articles were appraised by one reviewer and verified by a second. We examined the presence of each item across studies as well as by a total score; the number of “Yes” answers was divided by the number of applicable criteria to derive a total percentage score. As the criteria only examined presence and not quality or extent, we ran the risk of overestimating the transparency of studies; thus, we selected a stricter qualitative assessment of overall transparency with <70% of items present defined as low, 70–89% as adequate, and ≥90% as high transparency.
Data synthesis
Synthesis included both quantitative and qualitative approaches, which were finalized once the relevant content from all included studies was extracted. We used a priori definitions from our data extraction guide (Supplemental Methods C) and the Retail Food Environment and Customer Interaction model (19) to categorize the model purpose and the RFE characteristics included in models, and then used a thematic approach to identify inductive patterns within categories. We also performed simple counts to summarize information across our areas of interest—model purpose, RFE characteristics included, complexity characteristics represented, and model methods employed. Given the enormous diversity in research questions, we did not synthesize study findings and instead prioritized the utilization, benefits, and limitations of employing these models to study the RFE for population health.
Results
Description of included studies
Our initial database searches identified 5845 records (Figure 1). We screened 3876 unique records and assessed 111 full-text articles for eligibility. An additional 75 articles were excluded after full-text review, and we identified 20 additional articles from hand searching. The final 56 articles that met our review criteria were published between 2010 and 2020 with the number of publications increasing over time (Figure 2).
FIGURE 2.
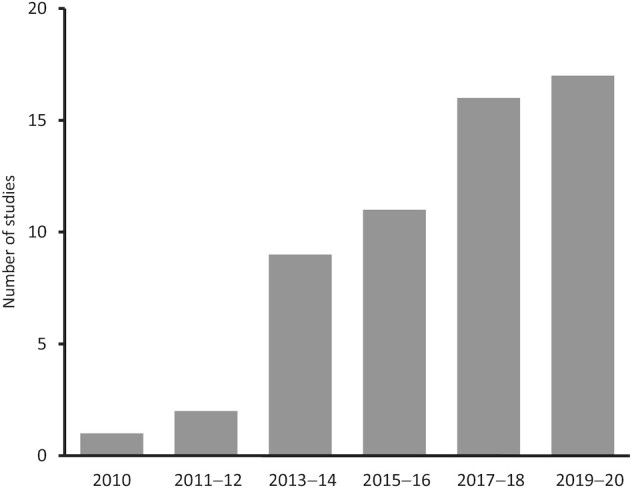
Publication year of studies (n = 56) using a complex systems model to study retail food environments for population health.
Eight OECD countries were represented across studies, though most studied populations in the USA (n = 46) (37, 40–47, 61–97). All 6 complex systems modeling approaches were represented with 23 microsimulations (74–91, 98–102), 13 ABMs (37–39, 41, 44, 47, 67–73), 10 hybrid models using ABM coupled with DES or networks (40, 42, 43, 61–66, 103), 4 SDs (95–97, 104), 4 network models (45, 92, 93, 105), and 2 DESs (46, 94). We also identified 25 studies that used the same model or a modified version (Supplemental Table 2), which included 6 microsimulation models used across 17 studies (75–79, 81, 83, 85–90, 99–102), 2 hybrid models used across 6 studies (40, 42, 43, 62–64), and 1 ABM used across 2 studies (47, 68).
Why was the model used?
Across a wide range of research questions (Supplemental Table 2), studies implemented complex systems models for 3 primary purposes—descriptive (n = 4) (45, 92, 93, 105), mechanistic (n = 7) (41, 47, 66, 71–73, 97) (i.e., to understand the system's etiology), and experimental (n = 45) (37–40, 42–44, 46, 61–65, 67–70, 74–91, 94–96, 98–104). Studies with descriptive purposes employed network models and aimed to characterize relations among supply chains (45, 92), product label messages (105), or procurement locations used by food assistance program participants (93). Seven studies used models for only mechanistic purposes, including ABM (n = 5) (41, 47, 71–73), hybrid (n = 1) (66), and SD (n = 1) (97). The mechanisms of interest ranged widely and depended on the specific research question [e.g., understanding the effects of neighborhood income segregation on healthy food access (72), understanding customer and producer features that make alternative food hubs sustainable (41)].
Implementing models for experimental purposes, including evaluating potential effects of proposed policies and interventions, was most common (n = 45), and all types of complex systems models were used for this purpose except network models (Supplemental Table 2). Some investigations only examined interventions or policies specific to the RFE, such as Wong et al. (46) which only simulated the effects of cooler and shelf placement on customer purchasing of nonsugar-sweetened beverages (non-SSBs); whereas, others examined interventions targeting RFEs as well as individuals [e.g., modifying resident's willingness-to-walk (61), product bans for food assistance benefits (75, 76, 87, 88)] or other environmental features [e.g., increased transportation options (44), improved school quality (43)]. Of the 42 studies (37–40, 43, 44, 46, 61, 64, 65, 67–70, 74–91, 94–96, 98–104) examining ≥1 proposed RFE policy or intervention, over half (n = 24) (38–40, 64, 65, 68, 70, 74–76, 78, 81, 84, 85, 87, 88, 90, 91, 94–96, 98, 101, 104) included scenarios that involved modifying food prices (e.g., SSB taxes, reducing produce prices); 11 examined scenarios resulting in product reformulation (67, 77, 79, 80, 83, 86, 89, 99–102); 7 studied scenarios involving product labels (e.g., SSB health warning) (37, 81–83, 86, 101, 104); 6 simulated scenarios that added neighborhood retail sources (e.g., increase supermarket density) (40, 43, 44, 61, 64, 103); 5 included scenarios that increased healthy food availability within sources (e.g., increase produce offerings in convenience stores) (44, 69, 81, 95, 104); 1 examined in-store product placement scenarios (46); and 1 examined product marketing scenarios (104). Most studies examined multiple scenarios to either understand the dose of a particular intervention [e.g., food industry compliance with sodium reformulation targets under optimal, modest, and pessimistic scenarios (89)] or to facilitate comparisons among different interventions [e.g., compare effects of adding farmer's market vendors to mobile markets (44)].
In addition, although all studies explicitly contextualized their study purpose as relevant to health, there was variation in the primary outcomes of interest (Figure 3). Forty-five studies (37–40, 42–44, 46, 47, 62–68, 70, 71, 73–91, 95, 96, 98–102, 104) used models to examine health and/or behavior outcomes (e.g., obesity, dietary intake) of which 6 (38, 39, 42, 43, 66, 70) were primarily interested in disparities between population groups. Other outcomes of interest included the cost-effectiveness of proposed policies (n = 15) (74, 75, 78–81, 83, 85–90, 95, 102), business interests like revenue and store survivability (n = 5) (41, 72, 94, 103, 104), food security and access (n = 4) (61, 69, 72, 75), RFE supply networks (n = 2) (45, 92), or other factors [n = 3 (93, 97, 105), e.g., implementation and maintenance of a restaurant intervention (97)]. Seventeen studies (72, 74, 75, 78–81, 83, 85–90, 95, 102, 104) examined more than one of these outcomes, mostly health and cost-effectiveness.
FIGURE 3.
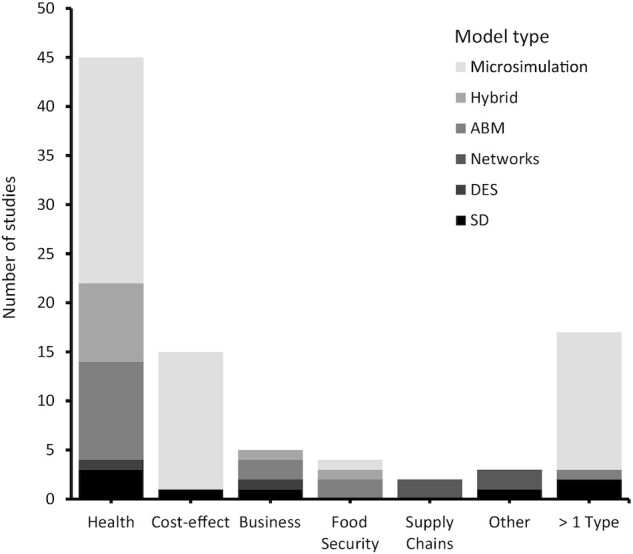
Primary outcome of interest across studies (n = 56) by model type. Categories of the primary outcomes are not mutually exclusive; studies with >1 primary outcome of interest are represented within each applicable category. >1 Type, studies with multiple primary outcomes of interest; ABM, agent-based model; Business, retail outcomes including store revenue and survivability; Cost-effect, cost-effectiveness of simulated policy or intervention; DES, discrete event simulations; Health, population health behavior or outcome; Hybrid, >2 model approaches used; SD, system dynamic models.
What RFE characteristics were included in models?
We identified a diverse breadth of RFE characteristics that were represented and simulated in model scenarios (Supplemental Table 2). We grouped characteristics using concepts from the Retail Food Environment and Customer Interaction model (19), including characteristics related to the customer retail experience, retail sources (e.g., grocery stores, fast food), and retail actors (e.g., managers) (Figure 4).
FIGURE 4.

Number of studies that examined different retail food environment (RFE) characteristics and incorporated customers in model scenarios. Upstream indicates RFE features that are more distal to customers for which they have limited control, interaction, or influence; downstream indicates RFE features that are proximal to customers.
Customer retail characteristics
Customer retail characteristics comprised features customers encounter when they acquire a product (19), such as price, product availability, and promotion, and 55 models (37–47, 61–92, 94–105) included ≥1 customer retail characteristic (Figure 4). Product characteristics were represented in nearly all models (n = 54) (37–47, 61–64, 66–92, 94–105), which varied from general characterizations of product healthfulness [e.g., “healthy” (45, 95)] to specific products [e.g., SSBs (94), fruits and vegetables (44, 78)] and nutrients [e.g., added sugars (83)]. Price was also a common feature represented in models (n = 32) (38–41, 47, 62–65, 68–72, 74–76, 78, 81, 84, 85, 87, 88, 90, 91, 94–96, 98, 101, 103, 104) varying from general classifications [e.g., “inexpensive” or “expensive” food store prices (39)] to specific values [e.g., 1-peso-per-liter beverage tax (98)]. Promotion features, like product labels and in-store marketing, were less common (n = 7) (37, 81–83, 97, 104, 105), whereas product placement (n = 1) (46) and other customer features, like service (n = 1) (103), were rarely represented.
Retail sources
Retail sources involved the settings where customers purchased food and beverages (e.g., restaurants), which were included in 30 models (37–46, 61–64, 66, 69, 71–74, 77, 81, 86, 87, 92–94, 96, 97, 103) (Figure 4). Across these studies, the presence of grocery stores, supermarkets, and discount clubs were most commonly represented (n = 12) (37, 38, 42–44, 61, 69, 72, 87, 92, 93, 103) followed by convenience or corner stores (n = 10) (37, 44–46, 61, 69, 87, 93, 94, 103), restaurants (n = 6) (37, 73, 77, 81, 86, 92), farmers’ markets/produce vendors (n = 5) (38, 44, 92, 93, 103), fast food/carry-outs (n = 4) (37, 38, 87, 97), and other sources [e.g., community-supported agriculture (74, 92), food hubs (41), vending (71, 81)]. Seven models (39, 40, 62–64, 66, 77) included a generic classification of “food stores,” though additional specification was provided by assigning customer retail features (e.g., store prices, products available).
Retail actors
Retail actors are individuals (e.g., store managers, suppliers) that behave and make decisions which create the RFEs experienced by customers and were included in 25 models (38–41, 45, 62, 63, 67, 72, 77, 79, 80, 83, 85, 86, 89, 90, 92, 94, 97, 99–102, 104) (Figure 4). The majority (n = 17) (41, 45, 67, 77, 79, 80, 83, 85, 89, 90, 92, 94, 99–102, 104) represented food producers and/or suppliers, largely by examining scenarios of product reformulation or supply chain relations. Managers and owners were less commonly included (n = 10) (38–40, 45, 62, 63, 72, 86, 94, 97) and typically represented via decisions to modify prices or products sold at a source or whether to close a store site. In contrast, nearly all models (n = 51) (37–44, 46, 47, 61–91, 93, 95, 96, 98–104) included customers (Figure 4 and see Supplemental Table 2 for study population details).
Breadth of RFE characteristics
As RFEs are complex, multilayered entities, we also examined the breadth of RFE features incorporated into the same model scenario, which allows the dynamics and interdependencies between RFE features to be simulated. Overall, 35 studies (37–41, 44, 45, 47, 61–64, 66–69, 72, 73, 83, 85, 86, 88, 90, 92–97, 99–104) simulated >1 RFE feature in the same scenario (Figure 5), which was performed among all SD (n = 4) (95–97, 104) and most ABM (n = 11) (37–39, 41, 44, 47, 67–69, 72, 73) models. For example, Struben et al. (104) used SD to simulate scenarios that examined changes in the prices and promotion of both healthy and unhealthy products; whereas Gouri Suresh et al. (72) used ABM to simulate multiple retailer behaviors, such as choosing where to locate a new store and the prices of store products. In contrast, the majority of microsimulation studies (74–82, 84, 87, 89, 91, 98) only examined a single RFE feature (Figure 5), such as Pitt et al. (91) that simulated price changes for a single product category (i.e., meat).
FIGURE 5.
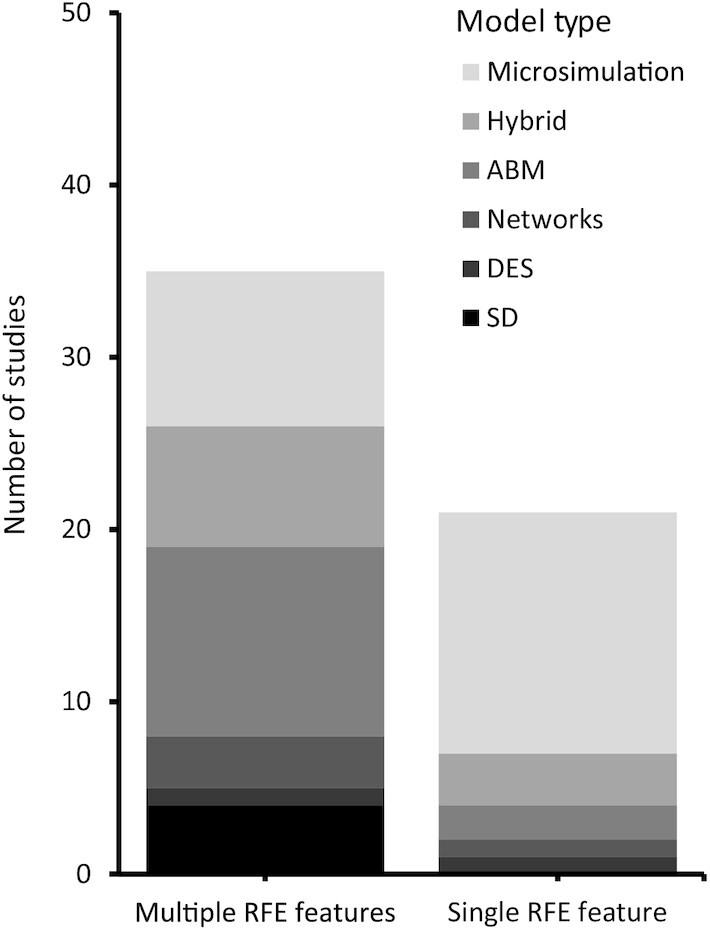
Studies that simulated a single retail food environment (RFE) feature or multiple RFE features in the same scenario by model type. ABM, agent-based model; DES, discrete event simulation; Hybrid, >2 model approaches used; RFE, retail food environment; SD, system dynamic model.
To what extent were use of complex systems approaches maximized?
To understand the extent to which studies maximized their complex systems modeling approach, we examined the presence of specific complexity characteristics in models. Table 2 presents the definition of these characteristics and their existence across studies. Although complexity was present in all studies, it was captured to varying degrees. Variation was driven by investigator modeling decisions and research questions in addition to the constraints of the specific modeling approach selected [e.g., microsimulation does not allow individual actors to interact (22)].
TABLE 2.
Complexity characteristics1 overall and by model type2 across included studies using complex systems models to study retail food environments for population health
| Overall (n = 56) | SD (n = 4) | DES (n = 2) | Networks (n = 4) | ABM (n = 13) | Hybrid (n = 10) | Microsimulation (n = 23) | |
|---|---|---|---|---|---|---|---|
| Complexity characteristic | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) |
| Multilevel: model includes heterogeneous elements that are conceptually aggregated at distinct levels (e.g., individuals, stores, products, neighborhoods) | 54 (96) | 4 (100) | 1 (50) | 3 (75) | 13 (100) | 10 (100) | 23 (100) |
| Multiple levels interact: elements explicitly operationalized at distinct levels connect (e.g., network ties) or influence one another through active or passive interactions (e.g., customers modify travel behavior in neighborhood when food store closes) | 30 (54) | 4 (100) | 1 (50) | 3 (75) | 13 (100) | 9 (90) | 0 (0) |
| Spatial: model includes elements that are located in an explicit definition of space (e.g., graphic or numeric representations) | 21 (38) | 0 (0) | 1 (50) | 1 (25) | 10 (77) | 9 (90) | 0 (0) |
| Dynamic: model includes elements that evolve over time and are not static | 47 (84) | 4 (100) | 0 (0) | 0 (0) | 12 (92) | 10 (100) | 21 (91) |
| Stochastic: model includes elements that are specified probabilistically using random inputs or conditions rather than all elements being deterministically specified | 42 (75) | 0 (0) | 0 (0) | 0 (0) | 12 (92) | 10 (100) | 20 (87) |
| Feedbacks: model includes a sequence of variables or equation functions that form a bidirectional effect or loop of influence | 19 (34) | 3 (75) | 0 (0) | 0 (0) | 6 (46) | 10 (100) | 0 (0) |
| Heterogeneous individual actors: model includes individual entities that are differentiated (e.g., customers with different demographic characteristics) | 51 (91) | 0 (0) | 1 (50) | 4 (100) | 13 (100) | 10 (100) | 23 (100) |
| Actors connect/interact with each other: individual entities within an agent type (e.g., among customers) connect (e.g., network ties) or influence one another through active or passive interactions (e.g., products unavailable to later customers due to prior customers purchasing stock) | 18 (32) | 0 (0) | 0 (0) | 2 (50) | 7 (54) | 9 (90) | 0 (0) |
Nearly all models (n = 54) (37–47, 61–93, 95–104) conceptually represented multiple levels (e.g., RFE features and individual customers); however, only half (n = 30) (37–47, 61–64, 66–73, 92, 93, 95–97, 103, 104) explicitly operationalized those levels in the model and connected them in some way (Table 2). For example, Blok et al. (38) studied various neighborhood and RFE interventions on inequalities in healthy food consumption among residents, which conceptually represent distinct environmental and individual levels; authors then explicitly quantified the interactions between levels, as residents were simulated to select which food stores to shop based on store-to-home distances, and stores were simulated to respond to residents’ purchasing (e.g., store closes if insufficient revenue). Alternatively, Lee et al. (85) examined the effects of various SSB tax policies on cardiovascular disease, which also involve concepts that represent distinct policy and individual levels; however, authors used individual-level SSB intake to quantify the effects of the tax policy as opposed to incorporating environmental price changes of SSBs, for example. A similar pattern was observed among the incorporation of heterogeneous individual actors in models (Table 2), which was common (n = 51) (37–47, 61–93, 98–103, 105), but only one-third (n = 18) (38–43, 62–67, 70–72, 92, 103, 105) had connections or interactions between actors to allow for potential influence [e.g., an individual's behaviors are influenced by peers in their network (40)].
The remaining complexity characteristics demonstrated distinct patterns by model approach (e.g., lack of explicit space included in SD) (Table 2), confirming some of the obvious constraints of certain models. In contrast, ABM and hybrid models enabled extensive versatility as all complexity characteristics were commonly included in studies using these models. Even so, studies using ABM did not universally incorporate some key characteristics relevant to RFEs and population health that they can model, like feedbacks (e.g., between customers and stores) and interactions among heterogeneous actors (e.g., customer purchasing behavior that influences others). In addition, although spatial representations were more regularly incorporated in both ABM and hybrid models, we noted that most representations were limited to home-to-store distances (38–40, 44, 61–64, 69, 72, 73, 103), neglecting additional nonresidential food environments (e.g., work) individuals navigate.
We also noted a marked pattern in the complexity of model construction between microsimulations and other models, especially ABM, SD, and hybrid models. A key advantage of microsimulations is their ability to simulate intervention effects in a heterogeneous population while incorporating dynamic and probabilistic conditions. Yet, other models such as ABM and hybrids, possess these and additional capabilities which can facilitate a richer exploration of the conditions under which interventions may be effective. For example, Grummon et al. (82) and Lee et al. (37) both examined the effects of an SSB warning label policy on individuals’ weight status using microsimulation and ABM, respectively. Although both examined the simulated effects of different efficacy rates, Lee et al. (37) also explored these effects while incorporating customers’ daily travel patterns, probabilities of purchasing SSBs at different neighborhood retail sources (e.g., corner stores, supermarkets), and other conditions that precede SSB purchasing and intake (e.g., store compliance with the policy, warning label literacy rates). Alternatively, Grummon et al. (82) only looked at individual effects downstream of SSB intake (e.g., caloric intake and weight).
What was the model quality and transparency?
We assessed model quality by examining the rigor and inclusivity of methods across studies (Table 3). All studies used empirical information to develop and parameterize models, with most (n = 53) (37–47, 61–91, 94–104) using datasets and/or prior literature (e.g., published estimates) and a few (n = 5) (41, 92, 93, 97, 105) collecting primary data either to augment other data sources or model alone. Few studies (n = 10) (61, 81, 84–87, 95, 96, 100, 103) reported consulting with experts during model development, and Koh et al. (69) conducted the only study that explicitly engaged stakeholders in the modeling process via a group model building approach. Most studies specified additional methods of rigorous modeling, including sensitivity analyses to increase confidence in the robustness of their results (n = 40) (37, 39, 40, 42, 43, 46, 47, 61, 63, 66–72, 74, 75, 77–80, 82–86, 88–91, 94–100, 102, 104) and steps of model verification or external validation to ensure models ran as intended and/or accurately captured observed phenomenon (n = 37) (37–40, 42, 43, 47, 61–64, 67–70, 73, 75–78, 80–82, 84–86, 88, 90, 92, 96, 97, 99–104). We noted one-third of studies (n = 20) (38, 39, 42–44, 61, 65, 69, 73, 79, 81, 83, 89, 91, 95, 96, 101–104) used calibration to “tune” unknown parameters or create a synthetic population. Relatedly, this meant most studies (n = 40) (37, 38, 40, 45–47, 62–64, 67–69, 73–90, 92–94, 97–102, 105), especially those with microsimulation, network, and DES models, displayed a high degree of empirical anchoring (i.e., all model features are linked to empirical data), which facilitates precise insights but potentially limits generalizability to the data sources used. Only 3 studies (39, 65, 72) developed models that were simplistic and highly stylized.
TABLE 3.
Summary of computational modeling methods employed overall and by model type1 across included studies using complex systems models to study retail food environments for population health
| Overall (n = 56) | SD (n = 4) | DES (n = 2) | Networks (n = 4) | ABM (n = 13) | Hybrid (n = 10) | Microsimulation (n = 23) | |
|---|---|---|---|---|---|---|---|
| Characteristic | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N (%) |
| Model development methods2 | |||||||
| Literature review/data sources | 53 (95) | 4 (100) | 2 (100) | 1 (25) | 13 (100) | 10 (100) | 23 (100) |
| Primary data collection | 5 (9) | 1 (25) | 0 (0) | 3 (75) | 1 (8) | 0 (0) | 0 (0) |
| Consulted experts/advisory group | 10 (18) | 2 (50) | 0 (0) | 0 (0) | 0 (0) | 2 (20) | 6 (26) |
| Engaged stakeholders in modeling | 1 (2) | 0 (0) | 0 (0) | 0 (0) | 1 (8) | 0 (0) | 0 (0) |
| Additional methods2 | |||||||
| Calibration | 20 (36) | 3 (75) | 0 (0) | 0 (0) | 5 (39) | 5 (50) | 7 (30) |
| Verification/external validation | 37 (66) | 3 (75) | 0 (0) | 1 (25) | 9 (69) | 8 (80) | 16 (70) |
| Sensitivity analyses | 40 (71) | 4 (100) | 2 (100) | 0 (0) | 9 (69) | 6 (60) | 19 (83) |
| Empirical anchoring3 | |||||||
| High | 40 (71) | 1 (25) | 2 (100) | 4 (100) | 7 (54) | 4 (40) | 22 (96) |
| Medium | 13 (23) | 3 (75) | 0 (0) | 0 (0) | 4 (31) | 5 (50) | 1 (4) |
| Low | 3 (5) | 0 (0) | 0 (0) | (0) | 2 (15) | 1 (10) | 0 (0) |
| Transparency appraisal4 | |||||||
| High | 24 (43) | 2 (50) | 0 (0) | 0 (0) | 6 (46) | 1 (10) | 15 (65) |
| Adequate | 22 (39) | 1 (25) | 1 (50) | 3 (75) | 5 (39) | 5 (50) | 7 (30) |
| Low | 10 (18) | 1 (25) | 1 (50) | 1 (25) | 2 (15) | 4 (40) | 1 (4) |
Abbreviated model types include: ABM, agent-based model; DES, discrete event simulation; Hybrid, >2 model approaches used; SD, system dynamic model.
Categories are not mutually exclusive. Multiple methods may be employed by authors in a single study; studies using >1 method are represented within each applicable category. Definitions for each method type are available in Supplemental Methods C.
Assessment based on Langellier et al. (34) definition of the degree of anchoring a model has to empirical data. Low consists of models that are primarily stylized or simplistic and do not directly link to empirical data; medium involves models that have some but not all features (e.g., parameters) linked to empirical data; and high consists of models that are entirely linked to empirical data sources. Categories are mutually exclusive.
10 items inspired by Jalali et al. (58, 59) (See Supplemental Table 1). The number of “Yes” answers was divided by the number of applicable criteria to derive a percentage score qualified as low (<70%), adequate (70–89%), or high transparency (≥90%). Categories are mutually exclusive.
Last, we assessed the transparency of studies which facilitates model clarity, reproducibility, and verifiability (Table 3). Twenty-four studies (47, 62, 68, 69, 71–74, 77–80, 82–86, 88, 89, 97, 98, 101, 102, 104) had a high degree of transparency; however, transparency criteria only examined presence and not extent, creating a potential ceiling effect for overall scores. Individually, the least common transparency criteria we identified across studies (n = 12 studies) (47, 68, 69, 74, 77, 78, 97, 98, 101–104) was providing a way for replication (e.g., public access to model code; see Supplemental Table 1).
Discussion
This systematic scoping review examined studies that used a complex systems computational modeling approach to address the RFE for population health. Across the literature, we examined the purpose for using the model, the RFE features studied, the extent to which complex systems approaches were maximized, and the quality and transparency of model methods employed. Below we summarize what has been accomplished across these applications of complex systems models by highlighting key strengths and areas for improvement.
Strengths
Several strengths were identified in our review. First, we identified more eligible studies than anticipated, with a total of 56 meeting inclusion criteria. Without imposing publication date restrictions, the earliest publication year was 2010 (95), which coincided with public health's growing interest in the use of complex systems approaches (24). Our review captures the early progress in applying complex systems approaches to study RFEs and demonstrates a clear acceleration in their utilization over the past decade (Figure 2). Such progress suggests research teams are finding effective ways to overcome the challenges inherent in transdisciplinary work to leverage the benefits of these models, including their use as policy and intervention laboratories (29), the primary use identified in this literature.
We also observed key strengths related to the outcomes studied using these models. Following health as the primary outcome of interest, the next most common outcomes were cost-effectiveness and business interests, like store revenue (Figure 3), which are important for making a compelling case for policy or intervention implementation. In addition, multiple outcomes were examined in 17 studies, reflecting the growing attention in the field to address multiple societal outcomes of RFEs (19, 106), and were most typically examined using microsimulation models that provided precise estimation of costs and health. At the same time, these microsimulation studies often only simulated a single RFE feature with few model dynamics, which limited novel or unexpected insights. In contrast, other approaches like ABM and hybrid models simulated both individuals and the systems that surround them. This facilitated a deeper exploration of the dynamic conditions that may affect policy and intervention effectiveness and provided a different but additionally useful strength in facilitating insights into the strategies that should be prioritized to best address health and other goals.
Other strengths were related to the extent models maximized complex systems approaches (Table 2) and the quality and transparency of methods used (Table 3). As the focus of this review was on RFEs and population health, it was unsurprising that nearly all models conceptually represented multiple levels (e.g., RFEs and individual customers). We also noted strong maximization among studies specifically using hybrid models (40, 42, 43, 61–66, 103), as all complexity characteristics were regularly incorporated, reflecting their strengths in realistically representing multiple levels, spatial and social features of RFEs, as well as individual heterogeneity among customers. Across all studies, there was also consistent use of empirically informed models and sensitivity analyses, which increased the rigor of both models and their results. Authors also displayed a consistent priority of transparency when reporting their investigations, as most had an overall adequate or high score (though, the criteria only measured presence not quality).
Areas for improvement
Across this review of literature, we also identified areas for improvement as these approaches are used in future research. One of the most concerning limitations we identified was the infrequency with which collaboration and community engagement were employed in developing models and informing investigators’ assumptions (Table 3). Proponents of systems science models have argued the advantages of using these tools to improve community health, inform structural changes, and reduce health disparities (20, 21, 29, 107–109). Yet, without a coproduction of models with decision-makers, food system players, customers, and other community members to help ensure sound assumptions and inform feasible change, it may be difficult to achieve these goals (107–109). Such limited stakeholder engagement has been identified in other reviews of systems science models for health behaviors (34, 35), like physical activity, indicating a gap that is not unique to the RFE literature. Intentionally addressing this gap is needed in future work, and although the tradition of community engagement is better established among some approaches, like SD, examples of cobuilding using other complex approaches, like ABM (110, 111), are increasingly demonstrating what is possible.
Another area for improvement identified was the dominant focus in models on individual customers and relatively limited focus on more upstream factors of the RFE and larger food system (Figure 4). Most models (n = 45) examined health and behavior outcomes, making the incorporation of customers key. Yet, in several studies using microsimulation models, RFE features (e.g., product label, taxes) were operationalized at the customer level using change in dietary intake. In addition, less than half of studies explicitly included RFE actors like managers and distributors, which may be a product both of author decisions and potential data gaps (112). Expanding models to consider RFE actors in addition to customers, such as performed by Basu and Lewis (67) which examined population health effects of the food industry's behavior within a cap-and-trade system on sugar, are important next steps. Similarly, models that focus only on RFE actors using a public health lens like Mui et al. (45), where distributor networks of corner stores were examined by product healthfulness, are critical to comprehensively understand how RFEs influence health.
In addition to a limited incorporation of upstream RFE factors, we observed a relatively limited incorporation of complexity into models themselves (Table 2) as well as the extent of RFE components examined among certain model types (Figure 5). For example, several studies using microsimulation only examined a single element of the RFE (e.g., nutrient reformulation), limiting understanding of the dynamics between other RFE components (e.g., price) that are relevant to purchasing as well as supply (e.g., industry response to reformulation policy). The limited complexity incorporated among microsimulations highlights some of their distinct limitations as a tool to study systems and explore unknown or emergent effects, which have been previously described (22). Other approaches like ABM and hybrid models are better equipped to handle this complexity and are quite versatile in addressing each study's unique RFE research question. Yet, which model to select and the degree of complexity to incorporate must be decisions guided by the research question and purpose (113). Adding additional complexity because a team can is not necessarily useful and might unintentionally obscure answers (113)—a scenario we did not observe in this literature. At the same time, drawing boundaries of the model too narrowly and not incorporating important complexity features can lead to setbacks in understanding (113) that may reflect similar challenges produced from relying only on traditional statistical models. Thus, each team is tasked with identifying the degree of complexity most relevant to their research problem and their intended purpose of the model (e.g., produce precise estimates, explore future policy scenarios).
Despite the greater versatility, ABMs and hybrid models used in this literature also displayed some limitations in capturing RFE complexity (Table 2). Some applications inconsistently incorporated feedbacks (e.g., between customer purchasing and store behavior) and assumed residential neighborhoods are the only relevant food environment for health (50) (i.e., neglecting other food environments at school and work). Future ABM and hybrid models that incorporate these key characteristics of RFE complexity will be able to be more fully utilized to answer RFE-related questions as well as enhance insight into unintended or unexpected effects.
Lastly, as noted by other authors (30, 34), issues remain around the methods employed when applying complex systems models, especially around validation and certain aspects of transparency (Table 3). External validation was common across studies, however, it was not universal; and when employed, was at times underdeveloped, as similarly identified in a review by Langellier et al. (34). Finally, although most studies demonstrated adequate transparency, only 12 studies (47, 68, 69, 74, 77, 78, 97, 98, 101–104) specified how to replicate their model (e.g., public access, pseudocode)—a gap that has been documented among ABMs at large (114). This, along with a need to make graphic representations of model relations a universal practice, is critical to help make complex systems modeling more reproducible, verifiable, and clearer to a wider audience. Setting author expectations to publish studies using existing model-specific reporting guidelines, such as the ODD (Overview, Design concepts, and Details) protocol (115, 116) and the PARTE (Properties, Actions, Rules, Time, and Environment) framework (117) for ABMs, and expanding these to include additional elements (e.g., graphical representations) that enhance transparency may be important future approaches.
Strengths and limitations of this review
This review has strengths and limitations. This review is the first of its kind to evaluate the utility, benefits, and limitations of using complex systems science approaches to examine RFEs for population health. Strengths included the extensive database search led by a public health librarian, and the implementation of PRISMA guidelines to select studies and extract data. We limited study inclusion to 6 specific complex systems computational approaches, which excluded other simulation and stochastic analytic methods, such as Markov models, and we omitted gray literature and studies that were not in English. Thus, results may have failed to provide a full synthesis of research to date that has used a complex systems computational modeling approach to study the RFE for population health. In addition, given the vast diversity of research questions and experiments simulated, we were limited in our ability to synthesize results across studies (e.g., which policies consistently demonstrated positive effects on nutrition-related health), and the lenient criteria of our transparency score may have overestimated the overall transparency among studies.
Conclusion
Tackling complexity within RFEs can be challenging if done unaided. Complex systems computational models are a useful tool to study this complexity and understand its potential solutions for health. The 6 approaches reviewed here all demonstrate potential in unraveling complexity, understanding RFEs as systems, and providing insights into future RFE policy and intervention effects. As these approaches become more common, it will be important for investigators to select the approach that best addresses their specific RFE research question, design models that adequately capture real-world complexity, better engage stakeholders, and provide greater transparency. Although room for improvement remains, this review helps demonstrate the utility of using these approaches to understand complex relations between RFEs and population health and inform future decision-making that improves RFEs.
Supplementary Material
ACKNOWLEDGEMENTS
We would like to thank Mohammad S Jalali of MGH Institute for Technology Assessment, Harvard Medical School, for sharing a preprint of the evaluation criteria used to assess reproducibility of simulation models.
The authors’ responsibilities were as follows—MRW: was responsible for leading the literature review including research inception, study design, study selection and data extraction, data analysis, and manuscript writing; YM: contributed to study design, performed study selection and data extraction, and contributed to data analysis; SH: performed and designed the database search; MNL: contributed to the research inception, study selection, and data analysis approach; JG: contributed to data analysis approach; MT: performed study selection and data extraction and contributed to the research inception, study selection, and data analysis; and all authors: critically revised the manuscript for intellectual content, and read and approved the final version.
Notes
Research reported in this publication was supported by the National Heart, Lung, and Blood Institute, of the National Institutes of Health under Award Number K99HL144824 (Principal Investigator: MRW). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author disclosures: The authors report no conflicts of interest.
Supplemental Methods A, B, and C, Supplemental Tables 1–2, and Supplemental References are available from the “Supplementary data” link in the online posting of the article and from the same link in the online table of contents at https://academic.oup.com/advances/.
Abbreviations used: ABM, agent-based model; DES, discrete event simulation; OECD, Organization for Economic Co-operation and Development; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RFE, retail food environment; SD, system dynamics; SSB, sugar-sweetened beverage.
Contributor Information
Megan R Winkler, Division of Epidemiology and Community Health, University of Minnesota School of Public Health, Minneapolis, MN, USA.
Yeeli Mui, Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Shanda L Hunt, Health Sciences Library, University of Minnesota, Minneapolis, MN, USA.
Melissa N Laska, Division of Epidemiology and Community Health, University of Minnesota School of Public Health, Minneapolis, MN, USA.
Joel Gittelsohn, Center for Human Nutrition, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA.
Melissa Tracy, Department of Epidemiology and Biostatistics, University at Albany School of Public Health, Rensselaer, NY, USA.
References
- 1. Murray CJL, Aravkin AY, Zheng P, Abbafati C, Abbas KM, Abbasi-Kangevari M, Abd-Allah F, Abdelalim A, Abdollahi M, Abdollahpour Iet al. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet North Am Ed. 2020;396(10258):1223–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Fleischhacker SE, Woteki CE, Coates PM, Hubbard VS, Flaherty GE, Glickman DR, Harkin TR, Kessler D, Li WW, Loscalzo Jet al. Strengthening national nutrition research: rationale and options for a new coordinated federal research effort and authority. Am J Clin Nutr. 2020;112(3):721–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zenk SN, Schulz AJ, Israel BA, James SA, Bao S, Wilson ML. Neighborhood racial composition, neighborhood poverty, and the spatial accessibility of supermarkets in metropolitan Detroit. Am J Public Health. 2005;95(4):660–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Richardson AS, Boone-Heinonen J, Popkin BM, Gordon-Larsen P. Are neighbourhood food resources distributed inequitably by income and race in the USA? Epidemiological findings across the urban spectrum. BMJ Open. 2012;2(2):e000698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Needham C, Orellana L, Allender S, Sacks G, Blake MR, Strugnell C. Food retail environments in Greater Melbourne 2008-2016: longitudinal analysis of intra-city variation in density and healthiness of food outlets. Int J Environ Res Public Health. 2020;17(4):1321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Díez J, Cebrecos A, Rapela A, Borrell LN, Bilal U, Franco M. Socioeconomic inequalities in the retail food environment around schools in a southern European context. Nutrients. 2019;11(7):1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Morland K, Wing S, Diez Roux A, Poole C. Neighborhood characteristics associated with the location of food stores and food service places. Am J Prev Med. 2002;22(1):23–9. [DOI] [PubMed] [Google Scholar]
- 8. Cooksey-Stowers K, Schwartz MB, Brownell KD. Food swamps predict obesity rates better than food deserts in the United States. Int J Environ Res Public Health. 2017;14(11):1366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Boone-Heinonen J, Gordon-Larsen P, Kiefe CI, Shikany JM, Lewis CE, Popkin BM. Fast food restaurants and food stores: longitudinal associations with diet in young to middle-aged adults: the cardia study. Arch Intern Med. 2011;171(13):1162–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Ohri-Vachaspati P, Acciai F, Lloyd K, Tulloch D, DeWeese RS, DeLia D, Todd M, Yedidia MJ. Evidence that changes in community food environments lead to changes in children's weight: results from a longitudinal prospective cohort study. J Acad Nutr Diet. 2021;121(3):419–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Brimblecombe J, McMahon E, Ferguson M, De Silva K, Peeters A, Miles E, Wycherley T, Minaker L, Greenacre L, Gunther Aet al. Effect of restricted retail merchandising of discretionary food and beverages on population diet: a pragmatic randomised controlled trial. Lancet Planet Health. 2020;4(10):e463–73. [DOI] [PubMed] [Google Scholar]
- 12. Mah CL, Luongo G, Hasdell R, Taylor NGA, Lo BK. A systematic review of the effect of retail food environment interventions on diet and health with a focus on the enabling role of public policies. Curr Nutr Rep. 2019;8(4):411–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Gittelsohn J, Rowan M, Gadhoke P. Interventions in small food stores to change the food environment, improve diet, and reduce risk of chronic disease. Prev Chronic Dis. 2012;9:E59. [PMC free article] [PubMed] [Google Scholar]
- 14. Hartmann-Boyce J, Bianchi F, Piernas C, Payne Riches S, Frie K, Nourse R, Jebb SA. Grocery store interventions to change food purchasing behaviors: a systematic review of randomized controlled trials. Am J Clin Nutr. 2018;107(6):1004–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Hecht AA, Perez CL, Polascek M, Thorndike AN, Franckle RL, Moran AJ. Influence of food and beverage companies on retailer marketing strategies and consumer behavior. Int J Environ Res Public Health. 2020;17(20):7381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Caspi CE, Sorensen G, Subramanian SV, Kawachi I. The local food environment and diet: a systematic review. Health Place. 2012;18(5):1172–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Cobb LK, Appel LJ, Franco M, Jones-Smith JC, Nur A, Anderson CA. The relationship of the local food environment with obesity: a systematic review of methods, study quality, and results. Obesity. 2015;23(7):1331–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Wilkins E, Radley D, Morris M, Hobbs M, Christensen A, Marwa WL, Morrin A, Griffiths C. A systematic review employing the GeoFERN framework to examine methods, reporting quality and associations between the retail food environment and obesity. Health Place. 2019;57:186–99. [DOI] [PubMed] [Google Scholar]
- 19. Winkler MR, Zenk SN, Baquero B, Steeves EA, Fleischhacker SE, Gittelsohn J, Leone LA, Racine EF. A model depicting the retail food environment and customer interactions: components, outcomes, and future directions. Int J Environ Res Public Health. 2020;17(20):7591. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hammond RA. Complex systems modeling for obesity research. Prev Chronic Dis. 2009;6(3):A97. [PMC free article] [PubMed] [Google Scholar]
- 21. Galea S, Riddle M, Kaplan GA. Causal thinking and complex system approaches in epidemiology. Int J Epidemiol. 2010;39(1):97–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Arnold KF, Harrison WJ, Heppenstall AJ, Gilthorpe MS. DAG-informed regression modelling, agent-based modelling and microsimulation modelling: a critical comparison of methods for causal inference. Int J Epidemiol. 2019;48(1):243–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Speybroeck N, Van Malderen C, Harper S, Müller B, Devleesschauwer B. Simulation models for socioeconomic inequalities in health: a systematic review. Int J Environ Res Public Health. 2013;10(11):5750–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Luke DA, Stamatakis KA. Systems science methods in public health: dynamics, networks, and agents. Annu Rev Public Health. 2012;33(1):357–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Nianogo RA, Arah OA. Agent-based modeling of noncommunicable diseases: a systematic review. Am J Public Health. 2015;105(3):e20–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Hammond R, Osgood N, Wolfson M. Using complex systems simulation modeling to understand health inequality. In: Kaplan GA, Diez Roux A, Simon C, Galea S, editors. Growing Inequality: Bridging Complex Systems, Population Health, and Health Disparities. Washington, DC: Westphalia Press; 2017. p. 11–24. [Google Scholar]
- 27. The National Academies of Sciences, Engineering, Medicine . Integrating Systems and Sectors Toward Obesity Solutions: Proceedings of a Workshop – in Brief. Callahan EA, editor. Washington, DC: The National Academies Press; 2020. [Internet]. p. 10. Available from:https://www.nap.edu/catalog/25936/integrating-systems-and-sectors-toward-obesity-solutions-proceedings-of-a. [PubMed] [Google Scholar]
- 28. Mabry PL, Olster DH, Morgan GD, Abrams DB. Interdisciplinarity and systems science to improve population health: a view from the NIH Office of Behavioral and Social Sciences Research. Am J Prev Med. 2008;35(2):S211–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Institute of Medicine . Accelerating Progress in Obesity Prevention: Solving the Weight of the Nation. Washington, DC: Institute of Medicine; 2012. [Google Scholar]
- 30. Tracy M, Cerda M, Keyes KM. Agent-based modeling in public health: current applications and future directions. Annu Rev Public Health. 2018;39(1):77–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Gu Y, Kunc M. Using hybrid modelling to simulate and analyse strategies. J Model Manag. 2019;15(2):459–90. [Google Scholar]
- 32. Borshchev A, Filippov A. From system dynamics and discrete event to practical agent based modeling: reasons, techniques, tools. The 22nd International Conference of the System Dynamics Society; 25–29 July; Oxford, England: 2004. [Google Scholar]
- 33. Morshed AB, Kasman M, Heuberger B, Hammond RA, Hovmand PS. A systematic review of system dynamics and agent-based obesity models: evaluating obesity as part of the global syndemic. Obes Rev. 2019;20(S2):161–78. [DOI] [PubMed] [Google Scholar]
- 34. Langellier BA, Bilal U, Montes F, Meisel JD, Cardoso LO, Hammond RA. Complex systems approaches to diet: a systematic review. Am J Prev Med. 2019;57(2):273–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Frerichs L, Smith NR, Lich KH, BenDor TK, Evenson KR. A scoping review of simulation modeling in built environment and physical activity research: current status, gaps, and future directions for improving translation. Health Place. 2019;57:122–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, Moher D, Peters MD, Horsley T, Weeks Let al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–73. [DOI] [PubMed] [Google Scholar]
- 37. Lee BY, Ferguson MC, Hertenstein DL, Adam A, Zenkov E, Wang PI, Wong MS, Gittelsohn J, Mui Y, Brown ST. Simulating the impact of sugar-sweetened beverage warning labels in three cities. Am J Prev Med. 2018;54(2):197–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Blok DJ, de Vlas SJ, Bakker R, van Lenthe FJ. Reducing income inequalities in food consumption: explorations with an agent-based model. Am J Prev Med. 2015;49(4):605–13. [DOI] [PubMed] [Google Scholar]
- 39. Auchincloss AH, Riolo RL, Brown DG, Cook J, Diez Roux AV. An agent-based model of income inequalities in diet in the context of residential segregation. Am J Prev Med. 2011;40(3):303–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Zhang D, Giabbanelli PJ, Arah OA, Zimmerman FJ. Impact of different policies on unhealthy dietary behaviors in an urban adult population: an agent-based simulation model. Am J Public Health. 2014;104(7):1217–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Krejci CC, Stone RT, Dorneich MC, Gilbert SB. Analysis of food hub commerce and participation using agent-based modeling: integrating financial and social drivers. Hum Factors: J Hum Factors Ergonomics Soc. 2016;58(1):58–79. [DOI] [PubMed] [Google Scholar]
- 42. Orr MG, Galea S, Riddle M, Kaplan GA. Reducing racial disparities in obesity: simulating the effects of improved education and social network influence on diet behavior. Ann Epidemiol. 2014;24(8):563–9. [DOI] [PubMed] [Google Scholar]
- 43. Orr MG, Kaplan GA, Galea S. Neighbourhood food, physical activity, and educational environments and black/white disparities in obesity: a complex systems simulation analysis. J Epidemiol Community Health. 2016;70(9):862–7. [DOI] [PubMed] [Google Scholar]
- 44. Widener MJ, Metcalf SS, Bar-Yam Y. Agent-based modeling of policies to improve urban food access for low-income populations. Appl Geogr. 2013;40:1–10. [Google Scholar]
- 45. Mui Y, Lee BY, Adam A, Kharmats AY, Budd N, Nau C, Gittelsohn J. Healthy versus unhealthy suppliers in food desert neighborhoods: a network analysis of corner stores' food supplier networks. Int J Environ Res Public Health. 2015;12(12):15058–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Wong MS, Nau C, Kharmats AY, Vedovato GM, Cheskin LJ, Gittelsohn J, Lee B. Using a computational model to quantify the potential impact of changing the placement of healthy beverages in stores as an intervention to “Nudge” adolescent behavior choice. BMC Public Health. 2015;15(1):1284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Beheshti R, Igusa T, Jones-Smith J. Simulated models suggest that price per calorie is the dominant price metric that low-income individuals use for food decision making. J Nutr. 2016;146(11):2304–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Utomo DS, Onggo BS, Eldridge S. Applications of agent-based modelling and simulation in the agri-food supply chains. Eur J Oper Res. 2018;269(3):794–805. [Google Scholar]
- 49. Powell K, Wilcox J, Clonan A, Bissell P, Preston L, Peacock M, Holdsworth M. The role of social networks in the development of overweight and obesity among adults: a scoping review. BMC Public Health. 2015;15(1):996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Giabbanelli PJ, Crutzen R. Using agent-based models to develop public policy about food behaviours: future directions and recommendations. Comput Math Methods Med. 2017;2017:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Eyles H, Ni Mhurchu C, Nghiem N, Blakely T. Food pricing strategies, population diets, and non-communicable disease: a systematic review of simulation studies. PLoS Med. 2012;9(12):e1001353–e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Brown DR, Brewster LG. The food environment is a complex social network. Soc Sci Med. 2015;133:202–4. [DOI] [PubMed] [Google Scholar]
- 53.Anderson Steeves E, Martins PA, Gittelsohn J. Changing the food environment for obesity prevention: key gaps and future directions. Curr Obes Rep. 2014;3(4):451–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. The World Bank Group . World Bank Country and Lending Groups: The World Bank Group. [Internet] [cited 1 June, 2020]. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
- 55. Organisation for Economic Co-operation and Development . Our Global Reach: Member Countries: OECD.org. [Internet] [cited 1 June, 2020]. Available from: https://www.oecd.org/about/members-and-partners/.
- 56. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan – a web and mobile app for systematic reviews. Systematic Reviews. 2016;5(1):210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Levy DT, Mabry PL, Wang YC, Gortmaker S, Huang TT, Marsh T, Moodie M, Swinburn B. Simulation models of obesity: a review of the literature and implications for research and policy. Obes Rev. 2011;12(5):378–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Jalali MS, DiGennaro C, Guitar A, Lew K, Rahmandad H. Evolution and reproducibility of simulation modeling in epidemiology and health policy over half a century. Epidemiol Rev. 2021, mxab006 [epub ahead of print]. doi.org/10.1093/epirev/mxab006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Jalali MS, DiGennaro C, Sridhar D. Transparency assessment of COVID-19 models. The Lancet Global Health. 2020;8(12):e1459–e60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Grieger JA, Johnson BJ, Wycherley TP, Golley RK. Evaluation of simulation models that estimate the effect of dietary strategies on nutritional intake: a systematic review. J Nutr. 2017;147(5):908–31. [DOI] [PubMed] [Google Scholar]
- 61. Abel KC, Faust KM. Modeling complex human systems: an adaptable framework of urban food deserts. Sustainable Cities and Society. 2020;52:101795. [Google Scholar]
- 62. Katapodis ND, Zhang D, Giabbanelli PJ, Li Y, Lyford CP, Rajbhandari-Thapa J. Evaluating the impact of improving access on consumption of fruits and vegetables in a rural community in Texas: a modeling study. Health Equity. 2019;3(1):382–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Li Y, Zhang D, Pagan JA. Social norms and the consumption of fruits and vegetables across New York City neighborhoods. J Urban Health. 2016;93(2):244–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Li Y, Zhang D, Thapa JR, Madondo K, Yi S, Fisher E, Griffin K, Liu B, Wang Y, Pagán J. Assessing the role of access and price on the consumption of fruits and vegetables across New York City using agent-based modeling. Prev Med. 2018;106:73–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Trogdon JG, Allaire BT. The effect of friend selection on social influences in obesity. Econ Hum Biol. 2014;15:153–64. [DOI] [PubMed] [Google Scholar]
- 66. Langellier BA. An agent-based simulation of persistent inequalities in health behavior: understanding the interdependent roles of segregation, clustering, and social influence. SSM - Population Health. 2016;2:757–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Basu S, Lewis K. Reducing added sugars in the food supply through a cap-and-trade approach. Am J Public Health. 2014;104(12):2432–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68. Beheshti R, Jones-Smith JC, Igusa T. Taking dietary habits into account: a computational method for modeling food choices that goes beyond price. PLoS One. 2017;12(5):e0178348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Koh K, Reno R, Hyder A. Examining disparities in food accessibility among households in Columbus, Ohio: an agent-based model. Food Secur. 2019;11(2):317–31. [Google Scholar]
- 70. Langellier BA, Lê-Scherban F, Purtle J. Funding quality pre-kindergarten slots with Philadelphia's new ‘sugary drink tax’: simulating effects of using an excise tax to address a social determinant of health. Public Health Nutr. 2017;20(13):2450–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71. Chen HJ, Xue H, Kumanyika S, Wang Y. School beverage environment and children's energy expenditure associated with physical education class: an agent-based model simulation. Pediatric Obesity. 2017;12(3):203–12. [DOI] [PubMed] [Google Scholar]
- 72. Gouri Suresh SS, Schauder SA. Income segregation and access to healthy food. Am J Prev Med. 2020;59(2):e31–38. [DOI] [PubMed] [Google Scholar]
- 73. Li Y, Du T, Peng J. Understanding out-of-home food environment, family restaurant choices, and childhood obesity with an agent-based Huff model. Sustainability. 2018;10(5):1575. [Google Scholar]
- 74. Basu S, O'Neill J, Sayer E, Petrie M, Bellin R, Berkowitz SA. Population health impact and cost-effectiveness of community-supported agriculture among low-income US adults: a microsimulation analysis. Am J Public Health. 2020;110(1):119–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Basu S, Seligman H, Bhattacharya J. Nutritional policy changes in the supplemental nutrition assistance program: a microsimulation and cost-effectiveness analysis. Med Decis Making. 2013;33(7):937–48. [DOI] [PubMed] [Google Scholar]
- 76. Basu S, Seligman HK, Gardner C, Bhattacharya J. Ending SNAP subsidies for sugar-sweetened beverages could reduce obesity and type 2 diabetes. Health Aff. 2014;33(6):1032–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Choi SE, Brandeau ML, Basu S. Expansion of the national salt reduction initiative: a mathematical model of benefits and risks of population-level sodium reduction. Med Decis Making. 2016;36(1):72–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78. Choi SE, Seligman H, Basu S. Cost effectiveness of subsidizing fruit and vegetable purchases through the supplemental nutrition assistance program. Am J Prev Med. 2017;52(5):e147–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79. Collins B, Kypridemos C, Pearson-Stuttard J, Huang Y, Bandosz P, Wilde P, Kersh R, Capewell S, Mozaffarian D, Whitsel LPet al. FDA sodium reduction targets and the food industry: are there incentives to reformulate?. Microsimulation cost-effectiveness analysis. Milbank Q. 2019;97(3):858–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80. Dehmer SP, Cogswell ME, Ritchey MD, Hong Y, Maciosek MV, LaFrance AB, Roy K. Health and budgetary impact of achieving 10-year U.S. sodium reduction targets. Am J Prev Med. 2020;59(2):211–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Gortmaker SL, Wang YC, Long MW, Giles CM, Ward ZJ, Barrett JL, Kenney EL, Sonneville KR, Afzal AS, Resch SCet al. Three interventions that reduce childhood obesity are projected to save more than they cost to implement. Health Aff. 2015;34(11):1932–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Grummon AH, Smith NR, Golden SD, Frerichs L, Taillie LS, Brewer NT. Health warnings on sugar-sweetened beverages: simulation of impacts on diet and obesity among U.S. adults. Am J Prev Med. 2019;57(6):765–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83. Huang Y, Kypridemos C, Liu J, Lee Y, Pearson-Stuttard J, Collins B, Bandosz P, Capewell S, Whitsel L, Wilde Pet al. Cost-effectiveness of the US Food and Drug Administration added sugar labeling policy for improving diet and health. Circulation. 2019;139(23):2613–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Kristensen AH, Flottemesch TJ, Maciosek MV, Jenson J, Barclay G, Ashe M, Sanchez EJ, Story M, Teutsch SM, Brownson RC. Reducing childhood obesity through U.S. federal policy: a microsimulation analysis. Am J Prev Med. 2014;47(5):604–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85. Lee Y, Mozaffarian D, Sy S, Liu J, Wilde PE, Marklund M, Abrahams-Gessel S, Gaziano TA, Micha R. Health impact and cost-effectiveness of volume, tiered, and absolute sugar content sugar-sweetened beverage tax policies in the United States: a microsimulation study. Circulation. 2020;142(6):523–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Liu J, Mozaffarian D, Sy S, Lee Y, Wilde Parke E, Abrahams-Gessel S, Gaziano T, Micha R. Health and economic impacts of the National Menu Calorie Labeling Law in the United States. Circ Cardiovasc Qual Outcomes. 2020;13(6):e006313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Long MW, Polacsek M, Bruno P, Giles CM, Ward ZJ, Cradock AL, Gortmaker SL. Cost-effectiveness analysis and stakeholder evaluation of 2 obesity prevention policies in Maine, US. J Nutr Educ Behav. 2019;51(10):1177–87. [DOI] [PubMed] [Google Scholar]
- 88. Mozaffarian D, Liu J, Sy S, Huang Y, Rehm C, Lee Y, Wilde P, Abrahams-Gessel S, de Souza Veiga Jardim T, Gaziano Tet al. Cost-effectiveness of financial incentives and disincentives for improving food purchases and health through the US Supplemental Nutrition Assistance Program (SNAP): a microsimulation study. PLoS Med. 2018;15(10):e1002661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Pearson-Stuttard J, Kypridemos C, Collins B, Mozaffarian D, Huang Y, Bandosz P, Capewell S, Whitsel L, Wilde P, O'Flaherty Met al. Estimating the health and economic effects of the proposed US Food and Drug Administration voluntary sodium reformulation: microsimulation cost-effectiveness analysis. PLoS Med. 2018;15(4):e1002551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90. Wilde P, Huang Y, Sy S, Abrahams-Gessel S, Jardim TV, Paarlberg R, Mozaffarian D, Micha R, Gaziano T. Cost-effectiveness of a US national sugar-sweetened beverage tax with a multistakeholder approach: who pays and who benefits. Am J Public Health. 2019;109(2):276–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91. Pitt A, Bendavid E. Effect of meat price on race and gender disparities in obesity, mortality and quality of life in the US: a model-based analysis. PLoS One. 2017;12(1):e0168710–e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92. Brinkley C. The small world of the alternative food network. Sustainability. 2018;10(8):2921. [Google Scholar]
- 93. Monteban MF, Bess KD, Walsh CC, Baily H, Flocke SA, Borawski EA, Freedman DA. People and places shaping food procurement among recipients of Supplemental Nutrition Assistance Program (SNAP). Health Place. 2018;53:155–63. [DOI] [PubMed] [Google Scholar]
- 94. Nau C, Kumanyika S, Gittelsohn J, Adam A, Wong MS, Mui Y, Lee B. Identifying financially sustainable pricing interventions to promote healthier beverage purchases in small neighborhood stores. Prev Chron Dis. 2018;15:E12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95. Homer J, Milstein B, Wile K, Trogdon J, Huang P, Labarthe D, Orenstein D. Simulating and evaluating local interventions to improve cardiovascular health. Prev Chronic Dis. 2010;7(1):A18. [PMC free article] [PubMed] [Google Scholar]
- 96. Liu S, Osgood N, Gao Q, Xue H, Wang Y. Systems simulation model for assessing the sustainability and synergistic impacts of sugar-sweetened beverages tax and revenue recycling on childhood obesity prevention. J Oper Res Soc. 2016;67(5):708–21. [Google Scholar]
- 97. Jalali MS, Rahmandad H, Bullock SL, Lee-Kwan SH, Gittelsohn J, Ammerman A. Dynamics of intervention adoption, implementation, and maintenance inside organizations: the case of an obesity prevention initiative. Soc Sci Med. 2019;224:67–76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98. Barrientos-Gutierrez T, Zepeda-Tello R, Rodrigues ER, Colchero-Aragonés A, Rojas-Martínez R, Lazcano-Ponce E, Hernández-Ávila M, Rivera-Dommarco J, Meza R. Expected population weight and diabetes impact of the 1-peso-per-litre tax to sugar sweetened beverages in Mexico. PLoS One. 2017;12(5):e0176336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99. Grieger JA, Johnson BJ, Wycherley TP, Golley RK. Comparing the nutritional impact of dietary strategies to reduce discretionary choice intake in the Australian adult population: a simulation modelling study. Nutrients. 2017;9(5):442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100. Johnson BJ, Grieger JA, Wycherley TP, Golley RK. Theoretical reductions in discretionary choices intake via moderation, substitution, and reformulation dietary strategies show improvements in nutritional profile: a simulation study in Australian 2- to 18-year-olds. J Acad Nutr Diet. 2019;119(5):782–798.e6. [DOI] [PubMed] [Google Scholar]
- 101. Kypridemos C, Guzman-Castillo M, Hyseni L, Hickey GL, Bandosz P, Buchan I, Capewell S, Flaherty M. Estimated reductions in cardiovascular and gastric cancer disease burden through salt policies in England: an IMPACTNCD microsimulation study. BMJ Open. 2017;7(1):e013791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Laverty AA, Kypridemos C, Seferidi P, Vamos EP, Pearson-Stuttard J, Collins B, Capewell S, Mwatsama M, Cairney P, Fleming Ket al. Quantifying the impact of the public health responsibility deal on salt intake, cardiovascular disease and gastric cancer burdens: interrupted time series and microsimulation study. J Epidemiol Community Health. 2019;73(9):881. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103. Calisti R, Proietti P, Marchini A. Promoting sustainable food consumption: an agent-based model about outcomes of small shop openings. J Artif Soc Soc Simul. 2019;22(1):2. [Google Scholar]
- 104. Struben J, Chan D, Dubé L. Policy insights from the nutritional food market transformation model: the case of obesity prevention. Ann N Y Acad Sci. 2014;1331(1):57–75. [DOI] [PubMed] [Google Scholar]
- 105. Fehér O, Boros P. Network analysis of nutrition marketing communication on food packaging. IJMC. 2011;13(3):584–90. [Google Scholar]
- 106. Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S, Garnett T, Tilman D, DeClerck F, Wood Aet al. Food in the anthropocene: the EAT-Lancet commission on healthy diets from sustainable food systems. Lancet North Am Ed. 2019;393(10170):447–92. [DOI] [PubMed] [Google Scholar]
- 107. Király G, Miskolczi P. Dynamics of participation: system dynamics and participation – an empirical review. Syst Res Behav Sci. 2019;36(2):199–210. [Google Scholar]
- 108. Frerichs L, Lich KH, Dave G, Corbie-Smith G. Integrating systems science and community-based participatory research to achieve health equity. Am J Public Health. 2016;106(2):215–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109. Gittelsohn J, Mui Y, Adam A, Lin S, Kharmats A, Igusa T, Lee B. Incorporating systems science principles into the development of obesity prevention interventions: principles, benefits, and challenges. Current Obesity Reports. 2015;4(2):174–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Frerichs L, Smith N, Kuhlberg JA, Mason G, Jackson-Diop D, Stith D, Corbie-Smith G, Lich KH. Novel participatory methods for co-building an agent-based model of physical activity with youth. PLoS One. 2020;15(11):e0241108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Homa L, Rose J, Hovmand PS, Cherng ST, Riolo RL, Kraus A, Biswas A, Burgess K, Aungst H, Stange KCet al. A participatory model of the paradox of primary care. Ann Fam Med. 2015;13(5):456–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112. Lin X, Ruess PJ, Marston L, Konar M. Food flows between counties in the United States. Environ Res Lett. 2019;14(8):084011. [Google Scholar]
- 113. Meadows DH. Thinking in Systems: A Primer. White River Junction, VT: Chelsea Green Publishing; 2008. [Google Scholar]
- 114. Janssen MA, Pritchard C, Lee A. On code sharing and model documentation of published individual and agent-based models. Environ Modell Softw. 2020;134:104873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Grimm V, Berger U, Bastiansen F, Eliassen S, Ginot V, Giske J, Goss-Custard J, Grand T, Heinz SK, Huse Get al. A standard protocol for describing individual-based and agent-based models. Ecol Modell. 2006;198(1–2):115–26. [Google Scholar]
- 116. Grimm V, Berger U, DeAngelis DL, Polhill JG, Giske J, Railsback SF. The ODD protocol: a review and first update. Ecol Modell. 2010;221(23):2760–8. [Google Scholar]
- 117. Hammond R. Considerations and best practices in agent-based modeling to inform policy. In: Wallace R, Geller A, Ogawa VA, editors. Assessing the Use of Agent-Based Models for Tobacco Regulation. Washington, DC: National Academies Press; 2015. [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.