

Abstract
Fluid overload is a common complication of critical illness, associated with increased morbidity and mortality. Pulmonary fluid status is difficult to evaluate clinically and many clinicians utilize chest X-ray (CXR) to identify fluid overload. Adult data have shown lung ultrasound (LUS) to be a more sensitive modality. Our objective was to determine the performance of LUS for detecting fluid overload, with comparison to CXR, in critically ill children. We conducted a systematic review using multiple electronic databases and included studies from inception to November 15, 2020. The sensitivity and specificity of each test were evaluated. Out of 1,209 studies screened, 4 met eligibility criteria. Overall, CXR is reported to have low sensitivity (44–58%) and moderate specificity (52–94%) to detect fluid overload, while LUS is reported to have high sensitivity (90–100%) and specificity (94–100%). Overall, the quality of evidence was moderate, and the gold standard was different in each study. Our systematic review suggests LUS is more sensitive and specific than CXR to identify pulmonary fluid overload in critically ill children. Considering the clinical burden of fluid overload and the relative ease of obtaining LUS, further evaluation of LUS to diagnose volume overload is warranted.
Keywords: child, critical illness, X-rays, ultrasonography, lung, radiography, fluid overload
Introduction
Fluid overload is a common complication of critical care for conditions such as congenital heart surgery, bone marrow transplantation, chronic kidney disease, and severe sepsis. 1 2 3 4 Recent evidence has established a strong association between fluid overload and increased in-hospital mortality, as well as morbidity from a wide range of causes. 5 6 7 8 A significant body of literature suggests that the percentage of fluid overload is associated with increased morbidity and mortality in the pediatric intensive care unit (ICU), with some studies suggesting overload of >5 to 10% as a critical threshold and others demonstrating a linear relationship between increasing fluid overload and increasing incidence of adverse outcomes. 7 9 10 11 12 13 Early and accurate detection of fluid overload is therefore a crucial step to guide the successful treatment of critically ill patients. While detection of positive fluid balance can be achieved by serial weight measurement and/or by tracking intake and output, obtaining sufficiently accurate measurements to make this determination can be a challenge. For example, weighing a hemodynamically unstable patient with multiple lines and tubes is often imprecise. Additionally, conditions causing increased insensible losses can render the recorded fluid balance less accurate.
In the absence of reliable serial measurements, significant fluid overload may instead be detected by the observation of its clinical effects. One such effect is the presence of increased extravascular lung water (EVLW) which induces changes in lung compliance and gas exchange capability that are likely responsible for the increased oxygenation index 6 and prolonged mechanical ventilation 5 6 observed in patients with significant fluid overload. Typically, chest X-ray (CXR) is used to detect pleural effusion and/or pulmonary edema as indicators of EVLW. However, lung ultrasound (LUS) can also be used to detect EVLW 14 15 16 and offers several potential advantages such as point-of-care convenience, reduced cost, and lack of exposure to ionizing radiation. As a relatively unexplored modality to evaluate fluid overload in critically ill children, the evidence for its diagnostic performance has been limited.
Our primary objective was to perform a systematic review to characterize the diagnostic performance of LUS by comparison to CXR for detecting fluid overload in critically ill children.
Methods
Design
This is a systematic review to determine the performance of LUS for detecting fluid overload, by comparison to CXR, in critically ill children. The review followed recommendations contained within the PRISMA (preferred reporting items for systematic reviews and meta-analyses) statement. 17
Types of Studies
We included retrospective or prospective observational studies and randomized controlled trials, which enrolled patients admitted to a pediatric ICU for any indication, and which reported diagnostic performance metrics for LUS and CXR, or LUS alone, in the evaluation of fluid overload. We defined performance metrics as sensitivity and specificity, positive and negative predictive values, or area under the receiver operating characteristic curve (AUC ROC).
We excluded case reports, case series, studies enrolling less than 10 patients, studies not in English, and studies of patients admitted to adult or neonatal ICUs.
Types of Participants
We included studies that enrolled patients aged 0 to 21 years who were admitted to pediatric ICUs.
Types of Outcome Measures
Our primary outcomes were the sensitivity and specificity of LUS for detection of fluid overload with reference to either a gold standard or to CXR.
Search Methods for Identification of Studies
For this systematic review, we performed a search of Ovid MED-LINE, Ovid EMBASE, Cochrane, Proquest Dissertations and Theses, and Clinicaltrials.gov from January 1, 1990 through November 15, 2020. The search included keywords and controlled vocabulary for LUS, CXR, fluid overload, and EVLW (search strategy available as Supplementary Data [available in the online version]). We imported the results to Covidence (version 1784, Melbourne, Australia) which automatically detected and removed duplicates.
Selection of Studies
Six reviewers (E.S., J.G., G.G., K.G., M.M., and O.K.) independently examined all potential studies and decided on their inclusion in the review. We evaluated each study based on its methods and reported outcomes, without blinding of authors, institutions, journals of publication, or results. We resolved disagreements by reaching consensus among review authors.
Data Extraction and Management
For each study in the systematic review, two authors independently extracted data. We resolved disagreements by discussion. Where required, we contacted study authors to request relevant data (e.g., specifying the population or the performance of the LUS). The corresponding authors were e-mailed twice within a 2-week period. Ultimately, we were unable to obtain additional data beyond what was published which was incomplete for the purposes of our study.
Assessment of Risk of Bias in Included Studies
We evaluated the validity and design characteristics of each study using the QUIPS tool, which evaluates aspects of major potential biases (study participation, prognostic factor measurement, outcome measurement, study confounding, and statistical analysis). 18 Two authors (E.S. and O.K.) reviewed and ranked each study's quality factors separately and defined studies as having low risk of bias only if they adequately fulfilled all the criteria.
Assessment of Lung Ultrasound Performance
When possible, we reported the sensitivity, specificity, positive and/or negative predictive values, and/or AUC ROC, as well as their 95% confidence interval (CI) if available.
Results
Description of Studies
We identified a total of 1,232 references of which 23 were duplicates and therefore removed from review. Of the 1,209 studies screened, 1,176 were irrelevant, leaving 33 articles to review in full. Of these, four met eligibility criteria. Two were unavailable as full texts despite reaching out to the authors, 19 20 leaving two full-text articles ( Fig. 1 ). 21 22
Fig. 1.
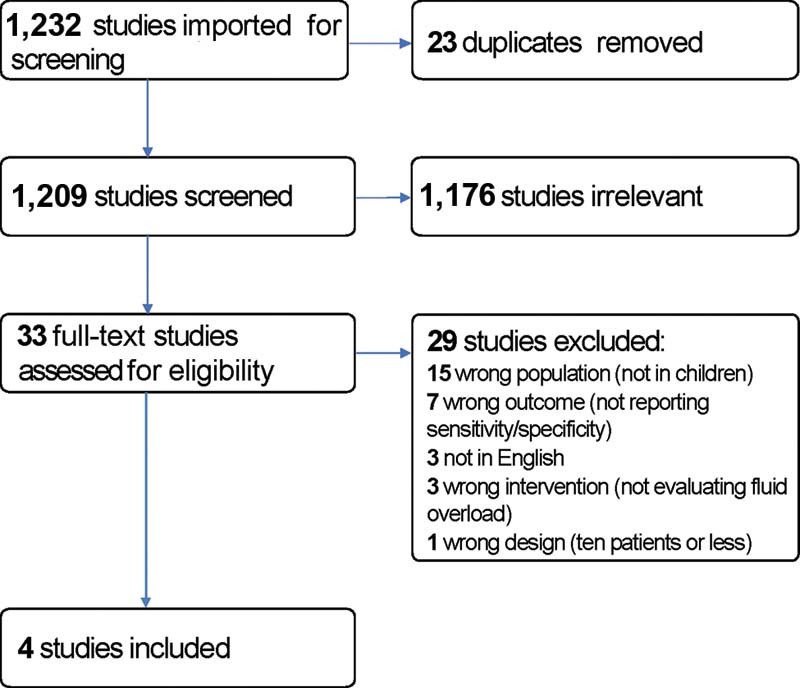
PRISMA diagram detailing the search and selection process applied during the systematic analysis. PRISMA, preferred reporting items for systematic reviews and meta-analyses.
The study by Tang and Hsieh enrolled 17 patients with congenital heart disease who were admitted with CXR findings suspicious for pulmonary edema, between October 2009 and December 2011, at Chang-Gung Memorial Hospital Kaoshiung, Kaoshiung, Taiwan. 19 The authors compared the LUS results of these patients with the LUS results of a control group of 30 patients without pulmonary edema. They reported that LUS revealed signs of fluid overload, defined as numerous comet-tail signs, in all 17 of the study group patients and stated a calculated sensitivity and specificity of 100%.
The study by Cantinotti et al enrolled 79 patients after cardiac surgery, from February to October 2016, at the Heart Hospital Gaetano Pasquinucci, Pisa, Italy. 21 They compared CXR with LUS, the latter being performed and interpreted by experienced pediatric cardiologists. A total of 138 examinations were performed. They reported that LUS was feasible in all cases, with the lateral view being accessible in 100% of patients, and the posterior view being most sensitive for the detection of pleural effusion and atelectasis. They noted that LUS agreed with CXR in 76.1% of examinations, with CXR tending to overestimate the degree of pulmonary congestion and underestimate the severity of pleural effusion and atelectasis. LUS ultimately generated 40 new diagnoses not detected by CXR, and 41 changes to a diagnosis initially established by CXR, either by confirming the CXR findings but contributing an additional diagnosis (14 cases) or by negating and replacing the diagnosis established by CXR (29 cases). Using LUS as the reference standard, they reported that CXR had a sensitivity of 58.0% (95% CI: 46.3–69.9) and a specificity of 82.1% (95% CI: 72.1–92.2).
The study by Gupta et al enrolled 413 patients admitted over the course of 10 months to the multidisciplinary pediatric ICU (PICU) at Sir Ganga Ram Hospital, New Delhi, India. 20 The authors compared CXR with LUS performed and interpreted by pediatric intensivists. A total of 1,002 examinations were performed. They reported that among examinations where CXR was reported as normal, LUS detected pulmonary edema in 39.5% and pleural effusion in 37% of cases. Using CXR as the reference standard, they reported that LUS had a sensitivity of >90% and specificity of >95% for detecting pulmonary edema, pleural effusion, and/or pneumothorax.
The study by Girona-Alarcon et al enrolled 17 patients with congenital heart disease who were admitted to the PICU following congenital cardiac surgery requiring cardiopulmonary bypass at Institut de Recerca Hospital San Joan de Deu, Barcelona, Spain. 22 LUS was performed preoperatively and at several time points postoperatively, and a numerical score was calculated and compared with the results of preoperative and 24-hour postoperative CXR, as read by a radiologist blinded to patient data. Using clinical assessment of pulmonary edema, based on respiratory distress, auscultation with rales, and need for diuretic treatment, the authors reported that, for preoperative evaluation of pulmonary edema, LUS outperformed CXR in sensitivity (91.7 vs. 44%), negative predictive value (88.2 vs. 53.3%), and positive predictive value (95.7 vs. 91.7%); LUS performed similarly to CXR in specificity (93.8 vs. 94.1%).
The various definitions of fluid overload used by the study authors are described in Table 1 . Overall, as summarized in Table 2 , CXR is reported to have low sensitivity (44–58%) and moderate specificity (52–94%) to detect fluid overload, while LUS is reported to have high sensitivity (90–100%) and specificity (94–100%).
Table 1. Description of diagnostic criteria used to define fluid overload.
| Study (year) | Chest X-ray | Lung ultrasound |
|---|---|---|
| Tang and Hsieh 19 (2017) | Pulmonary vascular congestion and pulmonary interstitial infiltration | B-lines arising from the pleural line, assessed qualitatively |
| Cantinotti et al 21 (2018) | Pulmonary vascular congestion and pulmonary interstitial infiltration | B-lines arising from the pleural line, assessed quantitatively |
| Gupta et al 20 (2018) | Unspecified | Unspecified |
| Girona-Alarcon et al 22 (2020) | Pulmonary interstitial infiltration | B-lines arising from the pleural line, assessed quantitatively; and presence of pleural effusion |
Table 2. Accuracy of CXR and LUS.
| n | Type of publication | Test | Gold standard | Sensitivity (%) | Specificity (%) | Negative predictive value (%) | Positive predictive value (%) | |
|---|---|---|---|---|---|---|---|---|
| Tang and Hsieh 19 (2017) | 17 | Abstract | LUS | CXR | 100 | 100 | – | – |
| Cantinotti et al 21 (2018) | 79 | Full text | CXR | LUS | 58 | 52 | – | – |
| Gupta et al 20 (2018) | 1,002 a | Abstract | LUS | CXR | >90 | >95 | – | – |
| Girona-Alarcon et al 22 (2020) | 17 | Full text | CXR | Clinical b | 44 | 94 | 53 | 92 |
| LUS | Clinical b | 92 | 94 | 88 | 96 |
Abbreviations: CXR, chest X-ray; LUS, lung ultrasound.
1,002 LUS were performed in 413 patients.
Clinical assessment of pulmonary edema was based on respiratory distress, auscultation with rales, and need for diuretic treatment.
Quality of Evidence
Overall, the quality of evidence was moderate ( Table 3 ). Tang and Hsieh and Gupta et al, the two abstract-only publications, had a high and moderate risk of bias, respectively. The risk of bias was moderate in Cantinotti et al and Girona-Alarcon et al, the two full-text publications.
Table 3. Assessment of the risk of bias.
| Study participation | Prognostic factor measurement | Outcome measurement | Study confounding | Statistical analysis and reporting | Overall risk of bias | |
|---|---|---|---|---|---|---|
| Tang and Hsieh 19 (2017) | Low | High | Low | High | High | High |
| Cantinotti et al 21 (2018) | Low | Low | Low | High | Low | Moderate |
| Gupta et al 20 (2018) | Moderate | Moderate | Moderate | High | Low | Moderate |
| Girona-Alarcon et al 22 (2020) | Low | Low | Low | Moderate | High | Moderate |
Note: Low, moderate, and high refer to the risk of bias for each criterion.
Pooled Performance of Lung Ultrasound to Diagnose Fluid Overload
As this systematic review only included four studies which compared the accuracy of CXR and LUS in different ways (different gold standards), we were unable to combine them in a pooled random-effect model.
Discussion
In this systematic review, we evaluated the diagnostic performance, in terms of sensitivity and specificity, of LUS as compared with CXR in critically ill children. Only four studies met inclusion criteria, and the overall quality of evidence was moderate. Overall, CXR is reported to have low sensitivity and moderate specificity to detect fluid overload, while LUS is reported to have high sensitivity and specificity. Due to varied methods of reporting on the primary and secondary outcomes, data from the four included studies were not able to be pooled.
Despite the paucity of pediatric studies, the use of LUS as a diagnostic tool for detecting fluid overload has been more extensively studied in adults. In keeping with the most common causes of fluid overload in adult patients, the adult literature on LUS for evaluation of EVLW is focused on two main subpopulations: patients who have chronic kidney disease and patients with congestive heart failure or other causes of cardiogenic pulmonary edema. 23 24 25 A recent systematic review and meta-analysis compared LUS with CXR for the detection of pulmonary edema due to acute decompensated heart failure in adult patients. 26 The meta-analysis demonstrated a relative sensitivity ratio of 1.2 for LUS as compared with CXR, (95% CI: 1.08–1.34; p < 0.001) and a relative specificity ratio of 1.0 (95% CI: 0.90–1.11; p = 0.96), suggesting that LUS is more sensitive and equally specific compared with CXR for detecting increased EVLW in this population. These results are similar to our findings.
Methodologically, tests should ideally be compared with a gold standard. The lack of a practical gold standard for measuring EVLW additionally complicates the comparison between LUS and CXR. Transpulmonary thermodilution (TPTD) methods have been validated in both adults and children as methods for the direct measurement of EVLW 27 28 29 30 and have been shown to produce measurements that correlate with disease severity and prognosis 31 ; however, because this method is invasive and requires specialized equipment, it is infrequently employed in current practice and was not included as a gold-standard comparator in any of the studies we reviewed, nor in the adult literature referenced above. Given the latest European guidelines recommending “against targeting hemodynamic therapy based on lung water measurement to assess pulmonary edema in critically ill children,” 32 the prospect of a large-scale study using TPTD to evaluate the accuracy of LUS and CXR is unlikely.
Limitations
Some limitations must be recognized. First, the main limitation of this systematic review is the paucity of data, as well as the heterogeneity in methods of evaluating the accuracy of LUS and CXR. Second, our review included only moderate-quality studies as assessed by the QUIPS tool. 18 This tool identified missing or underreported details in six domains that introduced a moderate or high risk of bias in the studies we analyzed. Importantly, information regarding interobserver variability and operator blinding to clinical data was incomplete. Given the significant dependence of LUS on operator training, these omissions had the potential to significantly alter the results of the studies. Additionally, only one study was performed in a general pediatric critical care setting, 20 while the others were specifically in children after cardiac surgery 21 22 or in children with known congenital heart disease. 19 22 There was significant overrepresentation of congenital heart disease patients and those under 6 years of age. Next, we were not able to address publication bias; it is possible that positive studies, in which LUS outperforms CXR, are likelier to be published. The inclusion of gray literature in our review is one method of addressing this effect and is promoted in the Cochrane Handbook, 33 34 but it did reduce the overall reliability of data as discussed above. Finally, due to the heterogeneous nature of the data reported in studies we reviewed, we were not able to perform a meta-analysis, although meta-analyses were published in the adult literature.
It is important to assess the accuracy and precision of a test. Other research avenues assessing the utility of LUS should be actively sought. For example, considering the increased morbidity and mortality associated with fluid overload, 5 6 7 8 one might consider evaluating the benefits of incorporating the use of LUS into fluid resuscitation strategies. So far, current literature has been limited to side-by-side comparison of LUS and CXR. Although echocardiography is believed to improve assessment of fluid responsiveness, 32 the addition of LUS into resuscitation algorithms might allow further improvement in outcomes.
Conclusion
In conclusion, despite a growing body of evidence in adults, there is scarce data comparing the accuracy of LUS versus CXR to identify fluid overload in critically ill children. LUS may have a significant advantage over CXR in high-resource settings with trained operators, where it can be performed with relative ease. Our systematic review suggests LUS may be more sensitive and specific than CXR to identify pulmonary fluid overload, although further study is needed to increase the quality of available evidence. Considering the clinical burden of fluid overload and the potential benefits of LUS over CXR, further study of the diagnostic performance of LUS is warranted. Additionally, use of LUS as a tool to guide fluid resuscitation deserves future study.
Footnotes
Conflict of Interest None declared.
Supplementary Material
References
- 1.Mah K E, Hao S, Sutherland S M. Fluid overload independent of acute kidney injury predicts poor outcomes in neonates following congenital heart surgery. Pediatr Nephrol. 2018;33(03):511–520. doi: 10.1007/s00467-017-3818-x. [DOI] [PubMed] [Google Scholar]
- 2.Bellos I, Iliopoulos D C, Perrea D N. Association of postoperative fluid overload with adverse outcomes after congenital heart surgery: a systematic review and dose-response meta-analysis. Pediatr Nephrol. 2020;35(06):1109–1119. doi: 10.1007/s00467-020-04489-4. [DOI] [PubMed] [Google Scholar]
- 3.Rondón G, Saliba R M, Chen J. Impact of fluid overload as new toxicity category on hematopoietic stem cell transplantation outcomes. Biol Blood Marrow Transplant. 2017;23(12):2166–2171. doi: 10.1016/j.bbmt.2017.08.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Chen J, Li X, Bai Z. Association of fluid accumulation with clinical outcomes in critically ill children with severe sepsis. PLoS One. 2016;11(07):e0160093. doi: 10.1371/journal.pone.0160093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Alobaidi R, Morgan C, Basu R K. Association between fluid balance and outcomes in critically ill children: a systematic review and meta-analysis. JAMA Pediatr. 2018;172(03):257–268. doi: 10.1001/jamapediatrics.2017.4540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Arikan A A, Zappitelli M, Goldstein S L, Naipaul A, Jefferson L S, Loftis L L. Fluid overload is associated with impaired oxygenation and morbidity in critically ill children. Pediatr Crit Care Med. 2012;13(03):253–258. doi: 10.1097/PCC.0b013e31822882a3. [DOI] [PubMed] [Google Scholar]
- 7.Selewski D T, Goldstein S L. The role of fluid overload in the prediction of outcome in acute kidney injury. Pediatr Nephrol. 2018;33(01):13–24. doi: 10.1007/s00467-016-3539-6. [DOI] [PubMed] [Google Scholar]
- 8.Goldstein S L, Somers M JG, Baum M A. Pediatric patients with multi-organ dysfunction syndrome receiving continuous renal replacement therapy. Kidney Int. 2005;67(02):653–658. doi: 10.1111/j.1523-1755.2005.67121.x. [DOI] [PubMed] [Google Scholar]
- 9.Selewski D T, Cornell T T, Lombel R M. Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med. 2011;37(07):1166–1173. doi: 10.1007/s00134-011-2231-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hazle M A, Gajarski R J, Yu S, Donohue J, Blatt N B. Fluid overload in infants following congenital heart surgery. Pediatr Crit Care Med. 2013;14(01):44–49. doi: 10.1097/PCC.0b013e3182712799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lane P H, Mauer S M, Blazar B R, Ramsay N K, Kashtan C E. Outcome of dialysis for acute renal failure in pediatric bone marrow transplant patients. Bone Marrow Transplant. 1994;13(05):613–617. [PubMed] [Google Scholar]
- 12.Hassinger A B, Wald E L, Goodman D M. Early postoperative fluid overload precedes acute kidney injury and is associated with higher morbidity in pediatric cardiac surgery patients. Pediatr Crit Care Med. 2014;15(02):131–138. doi: 10.1097/PCC.0000000000000043. [DOI] [PubMed] [Google Scholar]
- 13.Sinitsky L, Walls D, Nadel S, Inwald D P. Fluid overload at 48 hours is associated with respiratory morbidity but not mortality in a general PICU: retrospective cohort study. Pediatr Crit Care Med. 2015;16(03):205–209. doi: 10.1097/PCC.0000000000000318. [DOI] [PubMed] [Google Scholar]
- 14.Allinovi M, Saleem M, Romagnani P, Nazerian P, Hayes W. Lung ultrasound: a novel technique for detecting fluid overload in children on dialysis. Nephrol Dial Transplant. 2017;32(03):541–547. doi: 10.1093/ndt/gfw037. [DOI] [PubMed] [Google Scholar]
- 15.Pediatric Research in Emergency Departments International Collaborative . Long E, O'Brien A, Duke T, Oakley E, Babl F E. Effect of fluid bolus therapy on extravascular lung water measured by lung ultrasound in children with a presumptive clinical diagnosis of sepsis. J Ultrasound Med. 2019;38(06):1537–1544. doi: 10.1002/jum.14842. [DOI] [PubMed] [Google Scholar]
- 16.Kaskinen A K, Martelius L, Kirjavainen T, Rautiainen P, Andersson S, Pitkänen O M. Assessment of extravascular lung water by ultrasound after congenital cardiac surgery. Pediatr Pulmonol. 2017;52(03):345–352. doi: 10.1002/ppul.23531. [DOI] [PubMed] [Google Scholar]
- 17.PRISMA Group . Moher D, Liberati A, Tetzlaff J, Altman D G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi: 10.1136/bmj.b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hayden J A, van der Windt D A, Cartwright J L, Côté P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158(04):280–286. doi: 10.7326/0003-4819-158-4-201302190-00009. [DOI] [PubMed] [Google Scholar]
- 19.Tang C, Hsieh K. Sonographic evidence of pulmonary edema in pediatric patients with congenital heart disease. Pediatr Pulmonol. 2017;52 46:S155–S156. [Google Scholar]
- 20.Gupta D, Sachdev A, Khatri A.To study the correlation between chest radiograph and lung sonography in children admitted to pediatric intensive care unit Pediatr Crit Care Med J Soc Crit Care Med World Fed Pediatr Intensive Crit Care Soc 201819(6S)231 [Google Scholar]
- 21.Cantinotti M, Ait Ali L, Scalese M. Lung ultrasound reclassification of chest X-ray data after pediatric cardiac surgery. Paediatr Anaesth. 2018;28(05):421–427. doi: 10.1111/pan.13360. [DOI] [PubMed] [Google Scholar]
- 22.Girona-Alarcón M, Cuaresma-González A, Rodríguez-Fanjul J. LUCAS (lung ultrasonography in cardiac surgery) score to monitor pulmonary edema after congenital cardiac surgery in children. J Matern Fetal Neonatal Med. 2022;35(06):1213–1218. doi: 10.1080/14767058.2020.1743660. [DOI] [PubMed] [Google Scholar]
- 23.Covic A, Siriopol D, Voroneanu L. Use of lung ultrasound for the assessment of volume status in CKD. Am J Kidney Dis. 2018;71(03):412–422. doi: 10.1053/j.ajkd.2017.10.009. [DOI] [PubMed] [Google Scholar]
- 24.Miglioranza M H, Gargani L, Sant'Anna R T. Lung ultrasound for the evaluation of pulmonary congestion in outpatients: a comparison with clinical assessment, natriuretic peptides, and echocardiography. JACC Cardiovasc Imaging. 2013;6(11):1141–1151. doi: 10.1016/j.jcmg.2013.08.004. [DOI] [PubMed] [Google Scholar]
- 25.Picano E, Pellikka P A. Ultrasound of extravascular lung water: a new standard for pulmonary congestion. Eur Heart J. 2016;37(27):2097–2104. doi: 10.1093/eurheartj/ehw164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Maw A M, Hassanin A, Ho P M. Diagnostic accuracy of point-of-care lung ultrasonography and chest radiography in adults with symptoms suggestive of acute decompensated heart failure: a systematic review and meta-analysis. JAMA Netw Open. 2019;2(03):e190703. doi: 10.1001/jamanetworkopen.2019.0703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sakka S G, Reuter D A, Perel A. The transpulmonary thermodilution technique. J Clin Monit Comput. 2012;26(05):347–353. doi: 10.1007/s10877-012-9378-5. [DOI] [PubMed] [Google Scholar]
- 28.Monnet X, Teboul J-L. Transpulmonary thermodilution: advantages and limits. Crit Care. 2017;21(01):147. doi: 10.1186/s13054-017-1739-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lemson J, Backx A P, van Oort A M, Bouw T PWJM, van der Hoeven J G. Extravascular lung water measurement using transpulmonary thermodilution in children. Pediatr Crit Care Med. 2009;10(02):227–233. doi: 10.1097/PCC.0b013e3181937227. [DOI] [PubMed] [Google Scholar]
- 30.Proulx F, Lemson J, Choker G, Tibby S M. Hemodynamic monitoring by transpulmonary thermodilution and pulse contour analysis in critically ill children. Pediatr Crit Care Med. 2011;12(04):459–466. doi: 10.1097/PCC.0b013e3182070959. [DOI] [PubMed] [Google Scholar]
- 31.Khan S, Trof R J, Groeneveld A BJ. Transpulmonary dilution-derived extravascular lung water as a measure of lung edema. Curr Opin Crit Care. 2007;13(03):303–307. doi: 10.1097/MCC.0b013e32811d6ccd. [DOI] [PubMed] [Google Scholar]
- 32.Singh Y, Villaescusa J U, da Cruz E M. Recommendations for hemodynamic monitoring for critically ill children-expert consensus statement issued by the cardiovascular dynamics section of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC) Crit Care. 2020;24(01):620. doi: 10.1186/s13054-020-03326-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hopewell S, McDonald S, Clarke M, Egger M. Grey literature in meta-analyses of randomized trials of health care interventions. Cochrane Database Syst Rev. 2007;(02):MR000010. doi: 10.1002/14651858.MR000010.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Cumpston M, Li T, Page M J. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019;10:ED000142. doi: 10.1002/14651858.ED000142. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.