

Abstract
The Korean Society for Electrolyte and Blood Pressure Research, in collaboration with the Korean Society of Nephrology, has published a clinical practice guideline (CPG) document for hyponatremia treatment. The document is based on an extensive evidence-based review of the diagnosis, evaluation, and treatment of hyponatremia with the multidisciplinary participation of representative experts in hyponatremia with methodologist support for guideline development. This CPG consists of 12 recommendations (two for diagnosis, eight for treatment, and two for special situations) based on eight detailed topics and nine key questions. Each recommendation begins with statements graded by the strength of the recommendations and the quality of the evidence. Each statement is followed by rationale supporting the recommendations. The committee issued conditional recommendations in favor of rapid intermittent bolus administration of hypertonic saline in severe hyponatremia, the use of vasopressin receptor antagonists in heart failure with hypervolemic hyponatremia, and syndrome of inappropriate antidiuresis with moderate to severe hyponatremia, the individualization of desmopressin use, and strong recommendation on the administration of isotonic fluids as maintenance fluid therapy in hospitalized pediatric patients. We hope that this CPG will provide useful recommendations in practice, with the aim of providing clinical support for shared decision-making to improve patient outcomes.
Keywords: Evidence-based practice, GRADE approach, Guideline, Hyponatremia, Recommendation
Introduction
Hyponatremia, defined as serum sodium (SNa) concentration of <135 mmol/L, is the most frequent body fluid and electrolyte balance disturbance encountered in clinical practice. Although several international guidelines for managing hyponatremia are available, the differential diagnosis of hyponatremia is frequently challenging in patients with complex clinical settings and varying treatment. To assist patients, clinicians, and other healthcare professionals with decisions about the diagnostic approach to and treatment of hyponatremia, a multidisciplinary guideline development committee representing specialists with a genuine interest in hyponatremia was convened by the Korean Society for Electrolyte and Blood Pressure Research in collaboration with the Korean Society of Nephrology clinical practice guideline (CPG) committee. The development committee has developed the CPG and applied strict management strategies to minimize potential bias. The committee prioritized clinical questions and outcomes according to their importance for clinicians and patients. The committee used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, including GRADE Evidence-to-Decision frameworks, to assess evidence and make recommendations. The level of evidence for each result is graded as high/moderate/low/very low. The recommendation grade was divided into four levels: strong recommendation (A), conditional recommendation (B), against recommendation (C), and inconclusive (I). Definitions of the evidence levels are shown in Table 1. The key questions that cannot be adapted or developed directly due to the limitations of existing research are expressed as expert consensus (E). In addition to a rigorous approach to methodology and evaluation, this document represents recommended approaches for multiple etiologies of hyponatremia based on both the consensus opinions of experts in hyponatremia and the most recent published data in this field. There is also a link to full-text documents and lists of the most important reports so that the readers can obtain further information (most of which is available online).
Table 1.
Strength of recommendations and quality of evidence
| Category/grade | Definition |
|---|---|
| Strength of recommendation | |
| Strong recommendation (A) | Considering the benefits and risks of the treatment, the level of evidence, values and preferences, and resources, it is strongly recommended in most clinical situations. |
| Conditional recommendation (B) | The use of the treatment may vary depending on the clinical situation or patient/social value, so it is recommended to use it selectively or conditionally. |
| Against recommendation (C) | The risk of the treatment may outweigh the benefit and, taking into account the clinical situation or patient/social value, implementation is not recommended. |
| Inconclusive (I) | Considering the benefits and risks of the treatment, values and preferences, and resources, the level of evidence is too low, the scale of benefit/risk is too uncertain, or the variability is large, so the decision to implement the intervention is not made. This means that we cannot recommend or object to the use of treatment, so the decision is at the clinician’s discretion. |
| Expert consensus (E) | Although clinical evidence is insufficient, use is recommended in accordance with clinical experience and expert consensus when considering the benefits and risks of the treatment, the level of evidence, values and preferences, and resources. |
| Quality of evidence | |
| High | We are confident that the estimate of the effect is close to the actual effect. |
| Moderate | The estimate of the effect appears to be close to the actual effect, but may vary considerably. |
| Low | The confidence in the estimate of the effect is limited. The actual effect may differ significantly from the estimated effect. |
| Very low | There is little confidence in the estimate of the effect. The actual effect will differ significantly from the estimated effect. |
Recommendations on diagnostic procedures
Classification of hyponatremia
Hyponatremia is defined by less than 135 mmol/L of SNa [1]. Hyponatremia can be classified based on different parameters, including SNa concentration, timing of development, symptom severity, serum osmolality, and volume status. The criteria are described in Table 2 [1–3]. Because consistency and clarity of classification of hyponatremia are critical for diagnosis and management, we sought to compare the terminology used in the existing two guidelines (European and American guidelines) when discussing the classification of hyponatremia (Table 2).
Table 2.
Classification of hyponatremia
| Classification in the Korean Society of Nephrology clinical practice guideline | European guideline [1] | American guideline [2] | |
|---|---|---|---|
| SNa concentration | |||
| Mild | 130–134 mmol/L | Mild | Mild |
| Moderate | 125–129 mmol/L | Moderate | Moderate |
| Severea | <125 mmol/L | Profound | Severe |
| Severity of clinical symptoms | |||
| Asymptomatic-mild | Less pronounced | Mild | Mild |
| Moderate | Nausea without vomiting, confusion, headache, drowsiness, general weakness, myalgia | Moderately severe | Moderate |
| Severea | Vomiting, stupor, seizures, coma (Glasgow Coma Scale ≤ 8) | Severe | Severe |
| Time of development | |||
| Acute | <48 hr | No difference | |
| Chronic | ≥48 hr | ||
| Serum osmolality | |||
| Hypotonic | <275 mOsm/kg | No difference | |
| Isotonic | 275–295 mOsm/kg | ||
| Hypertonic | >295 mOsm/kg | ||
| Clinical assessment of volume status | |||
| Hypovolemic, euvolemic, hypervolemic | No difference | ||
SNa, serum sodium.
The term ‘severe’ is used for both classifications according to concentration and symptoms. We considered replacing ‘severe’ with a new term to avoid confusion, but no other terms seemed appropriate. According to several studies, symptoms become more common when SNa concentration drops below 125 mmol/L [3]. Therefore, the expression ‘severe’ is used interchangeably, but the type of classification is added in parentheses.
Differential diagnosis of hyponatremia
A practical diagnostic approach can progress step by step as follows (Fig. 1) [1].
Figure 1. Algorithm for the diagnosis of hyponatremia.
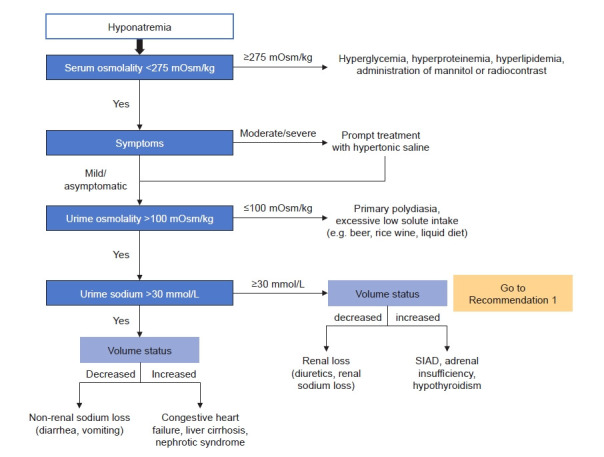
SIAD, syndrome of inappropriate antidiuresis.
1) Step 1
Check plasma osmolality for differentiating hypoosmolar hyponatremia from other causes of hyponatremia [1,3]. When plasma osmolality is reduced, you may require further steps of differential diagnosis. When plasma osmolality is above 275 mOsm/kg and hyponatremia is present, hyperglycemia should be checked. When serum glucose levels are increased, recheck the corrected sodium level according to the correction formula.
Corrected Na level (Hillier et al. [4]) = Na + 0.024 × (serum glucose [mg/dL] – 100)
Beyond hyperglycemia, hyperproteinemia, hyperlipidemia, and the use of mannitol or radiocontrast media can be a cause of hyper- or iso-osmolar hyponatremia [1–3].
2) Step 2
When hypoosmolar hyponatremia has been confirmed, the severity of clinical hyponatremic symptoms should be evaluated [1]. We have divided symptoms of hyponatremia into ‘asymptomatic-mild,’ ‘moderate,’ and ‘severe’ categories (Table 2). Symptomatic hyponatremia should be corrected immediately with acute management [1]. If acute management has been initiated or there are no symptoms of hyponatremia, go to the next step.
3) Step 3
Check urinary osmolality and discriminate excessive water intake.
When urinary osmolality is below 100 mOsm/kg, discriminate excessive water intake and excessive intake of hypotonic food or fluid (e.g., beer, rice wine, liquid diet) [1–3].
4) Step 4
Check urinary sodium to discriminate excessive renal excretion of sodium. When urinary sodium is above 30 mmol/L, discriminate the cause of hyponatremia according to volume status [1,3]. When volume status is decreased, check use of diuretics and cerebral salt wasting (CSW). When volume status is normal, check adrenal insufficiency, hypothyroidism, syndrome of inappropriate antidiuresis (SIAD), and other diseases or drugs that can cause SIAD.
When urinary sodium is below 30 mmol/L, recheck volume status and discriminate the causes. When volume status is decreased, check diarrhea or vomiting. When volume status is increased, discriminate congestive heart failure, liver cirrhosis, and nephrotic syndrome.
Volume status can be assessed through history-taking and physical examination. Symptoms of decreased volume status are usually nonspecific and may include thirst, fatigue, weakness, muscle cramps, and orthostatic dizziness. On physical examination, decreased skin turgor, low jugular vein pressure, orthostatic hypotension or postural tachycardia may appear. When more body fluid is lost, findings suggestive of decreased organ perfusion due to decreased intravascular fluid (low consciousness, oliguria, and peripheral cyanosis) or compensatory mechanisms (tachycardia, tachypnea, and sweating) may appear as symptoms of shock. On laboratory findings, increased urine osmolality, decreased urine sodium (UNa), alkalosis due to decreased volume status, relatively increased hemoglobin and albumin concentration may also be seen. Symptoms of increased volume status may include dyspnea on exercise, orthopnea, and peripheral edema. After underlying causes are evaluated, take further steps for managing them [1,3].
The diagnostic criteria of SIAD are summarized in Table 3 [1,2]. In addition, fractional excretion of uric acid (FEUA) can be used for discrimination of SIAD and use of diuretics (Recommendation 1) [3]. Serum copeptin/UNa ratio may also be used for discrimination of volume status. However, practical applications are still limited since copeptin measurement is not widely used (Recommendation 2).
Table 3.
| Essential criteria |
| Decreased effective osmolality (serum osmolality of <275 mOsm/kg) |
| Urine osmolality of >100 mOsm/kg at some level of serum hypoosmolality |
| Clinical euvolemia, as defined by the absence of signs of volume depletion |
| Elevated urine sodium concentration of >30 mmol/L with normal dietary salt and water intake |
| Absence of other potential causes of euvolemic hypoosmolality: severe hypothyroidism, adrenal insufficiency |
| Normal renal function and absence of diuretic intake (especially thiazide diuretics) |
| Supplemental criteria |
| Serum uric acid, <4 mg/dL |
| Serum urea, <21.6 mg/dL |
| Failure to correct hyponatremia after 0.9% saline infusion |
| Correction of hyponatremia through fluid restriction |
| Fractional sodium excretion, >0.5% |
| Fractional urea excretion, >55% |
| Fractional uric acid excretion, > 2% |
Diagnostic approaches should be performed step by step, including measuring plasma osmolality, urinary osmolality, and urinary sodium levels. Patient history and physical examination are also important to discriminate underlying causes of hyponatremia. Drug history should also be checked, as it can be associated with hyponatremia including SIAD [1].
For example, thiazide diuretics are a common cause in elderly women, and desmopressin in elderly men [5,6]. In patients with chronic pain, NSAID use should be checked. In patients with skin disorders or autoimmune diseases, adrenal insufficiency should be evaluated.
Recommendation 1
For patients with hyponatremia, we consider additional measurement of FEUA reasonable to differentiate likely causes of hyponatremia, such as SIAD or diuretic-induced hyponatremia (E).
Remarks:
1. FEUA was significantly higher in SIAD patients than in patients taking diuretics.
2. When patients taking diuretics were divided into thiazide and loop diuretics, SIAD- and thiazide-induced hyponatremia showed similar FEUA values.
FEUA is a supplemental diagnostic criterion for SIAD [7]; in patients using diuretics, FEUA performed best among UNa, fractional excretion of sodium (FENa), fractional urea excretion, and serum uric acid concentration (area under the curve, 0.96; 0.92–1.12) [8]. In the 2013 guideline published by the American Journal of Medicine, the measurement of FEUA in patients taking diuretics has been suggested to be helpful when trying to exclude hypovolemia [2]. According to the 2014 European guideline from the European Society of Endocrinology, European Society of Intensive Care Medicine, and European Renal Association European Dialysis and Transplant Association, FEUA using a threshold of >12% was most useful for distinguishing SIAD- from non-SIAD-related hyponatremia in patients on diuretics with a sensitivity of 0.86 and specificity of 1.00 [1]. However, the previous guidelines had no evidence derived from high-quality randomized controlled trials (RCTs). Our literature search identified two new observational studies from 2014 when the previous guideline was published.
In an observational study of 298 patients admitted with profound hypoosmolar hyponatremia (Na of <125 mmol/L), FEUA was higher in patients with SIAD compared with other hyponatremia etiologies (p < 0.001) [9]. We identified direct evidence from five observational studies (387 patients) that interpreted FEUA and FENa in hyponatremia patients due to SIAD and on diuretics [8-12]. Of these, one study was conducted with only patients taking thiazide diuretics, and in the other four studies, the group of patients taking thiazide or loop diuretics was not separated in our meta-analysis. A meta-analysis of studies showed that FEUA was significantly higher in SIAD patients than in patients taking diuretics. Two of five observational studies identified FEUA cutoff values of 10% and 12% (with specificity of 100% and 96%, respectively) [9,10]. Our meta-analysis found no differences in FENa. Since uric acid transporters are mostly located in the proximal tubules of the kidney, in which diuretics do not work primarily, we consider it reasonable that FEUA be used as a diagnostic test for the differential diagnosis of hyponatremia. However, caution is needed in interpreting FEUA. When patients taking diuretics were divided into thiazide and loop diuretics, SIAD- and thiazide-induced hyponatremia showed similar FEUA values in one study [10]. Furthermore, hypouricemia with increased FEUA is also observed in CSW. FEUA can be normalized after correction of hyponatremia in SIAD despite the continued increase in FEUA in CSW [13]. Lastly, concurrent use of drugs such as antihypertensives that alter uric acid excretion may affect FEUA levels [14]. Further evidence is needed to address the role of FEUA in diuretic-induced hyponatremia.
Recommendation 2
There are insufficient data to make a recommendation for using copeptin to UNa ratio to assess patient volume status (I, very low).
Remarks:
1. Copeptin levels overlap widely in hyponatremic patients and are affected by non-osmotic stimuli.
2. The ratio of copeptin to UNa was higher in disorders with secondary arginine vasopressin (AVP) release than those with primary AVP secretion such as SIAD.
Assessment of volume status in hyponatremic patients is important, but often challenging. Since the sensitivity and specificity of traditional clinical assessment of patient volume status are low, there have been efforts to identify novel biomarkers. Plasma AVP is a promising marker for the differentiation of volume disorders from a pathophysiological perspective. However, AVP is not routinely measured in clinical practice due to its instability. Copeptin has become a surrogate maker for AVP concentration and has advantages over AVP in aspects of stability and ease of measurement. Both American and European guidelines discussed copeptin briefly [1,2]. The American (2013) and European (2014) guidelines recommend that measurement of the copeptin to UNa ratio could distinguish hypovolemic hyponatremia from SIAD and that copeptin could discriminate euvolemia from hypovolemia and hypervolemia. Both guidelines were developed based on the same observational study [15]. There were no RCTs or meta-analyses exploring the value of copeptin in patients with hyponatremia. In the present guideline, one observational study published after 2015 was added and discussed [16].
Since copeptin levels overlap widely in hyponatremic patients and are affected by nonosmotic stimuli, copeptin to UNa ratio can be useful. In a previous report of 106 German hyponatremia patients, patients were classified into five categories: 1) normal volume with excessive water intake; 2) normal volume with SIAD; 3) decreased volume due to renal sodium loss; 4) decreased or normal volume due to non-renal sodium loss; and 5) increased volume [15]. A recent study of 100 Korean hyponatremic patients also classified patients into five categories: 1) normal volume with adrenal insufficiency; 2) normal volume with SIAD; 3) decreased volume due to renal sodium loss; 4) decreased volume due to non-renal sodium loss; and 5) increased volume [16]. Both observational studies revealed that copeptin to UNa ratio was superior to copeptin level for differentiating patient volume status. The ratio of copeptin to UNa was higher in disorders with secondary AVP release (decreased effective arterial volume) than conditions with primary AVP secretion such as SIAD.
Recommendations on treatment issues
The first step treatment evaluation of hyponatremia is identifying clinical symptoms and duration of hyponatremia, as mentioned above [1]. Treatment can be approached step by step as follows (Fig. 2).
Figure 2. Algorithm for the management of hyponatremia.
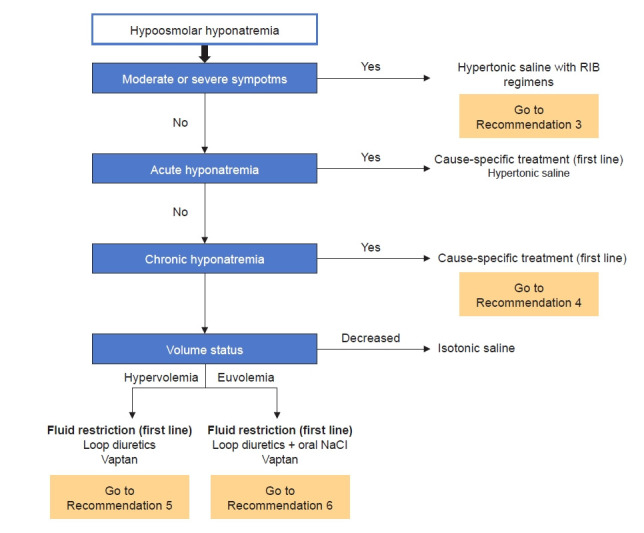
RIB, rapid intermittent bolus.
1) Symptomatic acute/chronic hyponatremia
Hypertonic saline should be administered for symptomatic hyponatremia as moderate or severe symptomatic hyponatremia reflects increased intracranial pressure. In terms of the infusion method of hypertonic saline, rapid intermittent bolus (RIB) regimens are suggested [1,2]. The treatment approach used for hypertonic saline in the American and European guidelines, and in a recent RCT performed in Korea is as follows (Table 4) [1–3,17]. A comparison of the efficacy and safety of hypertonic saline according to infusion methods (RIB vs. slow continuous infusion [SCI]) is discussed in Recommendation 3.
Table 4.
Approach to giving hypertonic saline and re-lowering excessive correction
| Variable | American guideline [2,3] | European guideline [1,3] | SALSA trial in Korea [17] |
|---|---|---|---|
| Initial infusion of hypertonic saline | |||
| Severe symptoms | Bolus: 100 mL over 10 min × 3 as needed | Bolus: 150 mL over 20 min × 2–3 as needed | Bolus: 2 mL/kg over 20 min × 2 as needed |
| Continuous infusion: 1 mL/kg/hr | |||
| Moderate symptoms | Continuous infusion: 0.5–2 mL/kg/hr | Bolus: 150 mL over 20 min once | Bolus: 2 mL/kg over 20 min once |
| Continuous infusion: 0.5 mL/kg/hr | |||
| Re-lowering treatment of SNa | |||
| 5% dextrose solution 3 mL/kg/hr ± desmopressin 2–4 µg IV | 5% dextrose solution 10 mL/kg over 1 hr ± desmopressin 2 µg IV | ||
IV, intravenous; SALSA, Efficacy and Safety of Rapid Intermittent Correction Compared With Slow Continuous Correction With Hypertonic Saline in Patients With Moderately Severe or Severe Symptomatic Severe Hyponatremia; SNa, serum sodium.
Recommendation 3
We suggest RIB administration of hypertonic saline in patients with symptomatic severe hypotonic hyponatremia (B, low).
Remarks:
In the treatment of symptomatic severe hypotonic hyponatremia,
1. RIB administration of hypertonic saline can effectively relieve symptoms within 12 hours compared to SCI.
2. RIB is more effective in increasing SNa within 1 hour and reaching the target correction rate than SCI.
3. RIB can result in a lower incidence of therapeutic re-lowering of SNa than SCI.
4. RIB has similar overcorrection, osmotic demyelination syndrome (ODS), and mortality rates to SCI.
Hypertonic saline has been used to treat symptomatic severe hypotonic hyponatremia. Overcorrection from indiscriminate prolonged use of hypertonic saline may result in irreversible neurologic sequelae from ODS, whereas under-correction of hyponatremia may insufficiently improve fatal complications of cerebral edema. Therefore, appropriate correction of SNa is needed. Although the American (2013) and European (2014) guidelines recommend administering hypertonic saline in small, fixed boluses (recommendation grade: expert opinion in the American guidelines, 1D in the European guidelines), they were not based on high-quality RCT evidence [1,2,17]. In order to examine whether RIB therapy of hypertonic saline has any benefit for symptom relief, correction of SNa, complications, and prognosis compared to SCI in patients with symptomatic severe hypotonic hyponatremia, we reviewed a prospective cohort study (24 hours of follow-up after treatment) and a RCT (48 hours of follow-up after treatment) published after the European guideline (2014).
A prospective cohort study reported that the RIB group had more rapid elevation of SNa and greater improvement in the Glasgow Coma Scale (GCS) at 6/12 hours than the SCI group. However, there was no difference between the two groups in GCS improvement at 24 hours [18].
A RCT demonstrated that the RIB group had the higher increment in SNa at 1 hour, a higher proportion meeting the target correction rate (achieving SNa of 5–9 mmol/L within 24 hours and SNa of 10–17 mmol/L or ≥130 mmol/L within 48 hours) at 1 hour, lower SNa at 12 hours, and a lower incidence of re-lowering treatment (5% dextrose infusion 10 mL/kg over 1 hour and/or intravenous desmopressin 2 µg if SNa level increase is ≥10 mmol/L within the first 24 hours or ≥18 mmol/L within 48 hours) than the SCI group [17].
In both studies, the target correction rate, the degree of SNa elevation at 24 hours, and overcorrection (increase in SNa by >12 mmol/L within the first 24 hours or increase in SNa by >18 mmol/L within 48 hours) did not differ between the two groups [17,18]. ODS did not occur in either study [17,18]. Death occurred in five patients in the RCT and four patients in the prospective cohort study, with no significant difference between the two groups [17,18]. Only one RCT for hypertonic saline infusion in symptomatic severe hypotonic hyponatremia has been reported in Korea; thus, additional large-scale RCTs are needed.
In cases of severe symptomatic hyponatremia, RIB regimens of hypertonic saline should be promptly administered to increase SNa by 4 to 6 mmol/L to relieve cerebral edema, and then cause-specific treatment can be planned [1]. In cases of moderate symptomatic hyponatremia, RIB or SCI methods of hypertonic saline can be used and cause-specific treatment can be prioritized without administration of hypertonic saline [1]. We suggest checking SNa concentration 1 hour after first hypertonic saline administration, then rechecking SNa concentration every 6 hours to adjust the administration interval or infusion rate of hypertonic saline [1]. We recommend that the rate of sodium correction be reevaluated when symptoms improve or SNa concentration increases by 5 to 9 mmol/L [1,2]. If symptoms do not improve or SNa concentrations do not reach target correction, infusion of hypertonic saline may be repeated [1,2]. In patients with hypervolemic hyponatremia, hypertonic saline and loop diuretics should be administered at the same time [3].
2) Asymptomatic acute hyponatremia
The absence of moderate or severe symptoms indicates that the clinically significant brain edema has not yet developed. Therefore, prompt diagnostic assessment of hyponatremia is suggested versus immediate infusion of hypertonic saline. Nonessential fluids and medications that can contribute to or provoke hyponatremia should be stopped. If the acute decrease in SNa concentration exceeds 10 mmol/L, we suggest administering the same amount of hypertonic saline as in patients with moderate symptoms to prevent a further drop in SNa concentration [1].
3) Asymptomatic chronic hyponatremia
Asymptomatic chronic hyponatremia does not require prompt correction but may lead to localized neurologic impairment and increased mortality compared to normonatremia. Even patients with mild hyponatremia have a higher mortality rate compared to patients with normonatremia.
Recommendation 4
We recommend rigorously evaluating the causes of mild hyponatremia and to managing causative diseases to improve clinical outcomes (E).
Remarks:
1. Mild hyponatremia increases the risk of mortality compared with those with normonatremia.
2. There is no clear evidence that correcting hyponatremia itself improves patient-important outcomes.
3. There are insufficient data to make a recommendation regarding treating mild hyponatremia with hypertonic saline or oral sodium chloride solely to increase SNa concentration.
In the case of mild hyponatremia, it is often unnoticed in clinical practice because it rarely presents with specific symptoms. Moreover, there is lack of evidence from RCTs that treatment of mild hyponatremia with fluid therapy or medication with the sole aim of correction to normal SNa concentration improves patient outcomes. The European guideline (2014) recommends against treatment simply to increase SNa concentration (grade of recommendation 2C). However, several observational studies have shown that mild hyponatremia increases the risk of mortality both in short-term and long-term follow-up. Waikar et al. [19] reported that hospitalized patients with mild hyponatremia defined as a SNa concentration of 130 to 134 mEq/L showed increased in-hospital mortality risk compared with those with normonatremia. Doshi et al. [20] found that hospitalized cancer patients with mild hyponatremia showed two-fold increased risk of morality compared to those with normonatremia. Furthermore, Kovesdy et al. [21] observed that mild hyponatremia defined as 130 to 135.9 mEq/L increased the risk of relatively long-term mortality (median follow-up duration, 5.5 years) in patients with chronic kidney disease with estimated glomerular filtration rate less than 60 mL/min/1.73 m2. From a meta-analysis including above studies that compared the short-term (less than 90 days or in-hospital mortality) and long-term (more than 5 years mortality) mortality risk, mild hyponatremia increased both short-term (odds ratio [OR], 2.09; 95% confidence interval [CI], 1.90–2.30; p < 0.001) and long-term (OR, 1.46; 95% CI, 1.44–1.48; p < 0.001) mortality risk compared with normonatremia.
In a domestic retrospective study [22], improved SNa concentration at discharge had the strongest association with long-term mortality in acute myocardial infarction patients with hyponatremia. However, because mild hyponatremia patients were not distinguished from other study patients, and interventions such as hypertonic saline were not addressed in this study, these findings were not included in the rationale under the consensus of the Development Committee. Although there is insufficient data that the correction of mild hyponatremia with the sole aim of correcting SNa concentration has clinical benefit, it is reasonable to rigorously evaluate the causes of mild hyponatremia and to manage the diseases because mild hyponatremia increases the risk of mortality.
(1) Hypervolemic hyponatremia is commonly seen in heart failure or liver cirrhosis. Restriction of sodium and free water intake (approximate <800–1,000 mL/day) is the first-line treatment. Additional pharmacologic therapies including loop diuretics and vasopressin receptor antagonists (‘vaptans’) can be used to increase renal free water excretion [1–3]. The possibility of using vaptans in patients with heart failure or liver cirrhosis is discussed greater detail in Recommendation 5. Fluid intake should not be restricted to prevent overcorrection when using vaptans [2].
Recommendation 5
1. We suggest vaptan use in heart failure with hypervolemic hyponatremia in terms of rapid sodium correction (B, moderate).
2. We make no recommendation on the use of vaptans in liver cirrhosis with hypervolemic hyponatremia (E).
Remarks:
1. We evaluated the efficacy of adding vaptans to loop diuretics since few studies compared vaptans versus loop diuretics in heart failure with hypervolemic hyponatremia.
2. The addition of vaptans to loop diuretics is more effective to elevate SNa concentration compared with loop diuretics alone.
3. The addition of vaptans to loop diuretics does not worsen renal function compared with loop diuretics alone.
4. The addition of vaptans to loop diuretics does not show survival benefit compared with loop diuretics alone.
5. The addition of vaptans has the potential to lead to hepatotoxicity in patients with liver cirrhosis.
Although vaptans have shown effectiveness for correcting SNa in SIAD, heart failure, and liver cirrhosis, the U.S. Food and Drug Administration (FDA) limited the use of vaptans in liver cirrhosis in 2013 due to hepatic toxicity concerns. The European guideline recommended against treating vaptans in hypervolemic hyponatremia (grade of recommendation 1C). Therefore, we accepted the previous guideline in hyponatremia in liver cirrhosis and did not seek further evidence. We reviewed only patients with heart failure, excluding studies on liver cirrhosis patients.
Including 11 RCTs, one observational study, and two systematic reviews (SRs), the guideline found no clinical benefit to the use of vaptans in hypervolemic hyponatremia. However, the quality of the studies varied, the characteristics of enrolled patients were not similar, and most of the RCTs did not distinguish patients with hypervolemia from those with normal volume status. Also, two studies only included patients with liver cirrhosis, and three studies only enrolled patients with heart failure. Thus, it is difficult to conclude that vaptans are superior to loop diuretics. Although vaptans showed a clinical benefit compared with placebo in the two SRs, there was no comparison of vaptans with loop diuretics as a basic therapeutic agent in hypervolemic hyponatremia. Since 2015, various studies have investigated whether additional use of vaptans with loop diuretics could lead to clinical benefit in hyponatremia with heart failure. Only one study compared vaptans and loop diuretics [23], and nearly all studies sought to clarify the effectiveness of additional vaptan use on loop diuretics. Recent studies showed the efficacy of vaptans in patients with chronic kidney disease and heart failure [24,25].
Therefore, this guideline focused on the benefit of additional vaptan use with loop diuretics in hypervolemic hyponatremia with heart failure in terms of survival gain, sodium correction, and conservation of renal function. We reviewed nine RCTs [23–31], five SRs, and several observational studies. All RCTs were conducted in patients with hyponatremic heart failure prescribed tolvaptan 7.5 to 30 mg per day, and allowed furosemide intravenous or oral use. There was no survival benefit of adding tolvaptan on furosemide [23,25,26,29,31]. Renal function decline, which was defined as the increase of serum creatinine more than 0.3 mg/dL per week, was not different between the tolvaptan-added group and furosemide-alone group [23,26,27,30]. Sodium correction for 24 hours was higher when tolvaptan was added to furosemide [25–27].
(2) SIAD is a state of water retention due to a persistent increase in antidiuretic hormone, characterized by hypoosmolar hyponatremia, euvolemia, and high urine osmolarity. In patients with SIAD, the standard treatment is the restriction of free water because of water retention [32]. The following can be considered second-line treatment: a combination of oral sodium chloride (NaCl) and loop diuretics or vaptans (Recommendation 6) [2,3]. NaCl causes an electrolyte diuresis by increasing urine solute load. However, its primary role is the restoration of urinary sodium losses and preventing negative sodium balance in hyponatremia [33]. NaCl is available as 1 g (17 mEq sodium and chloride) tablets. Usual doses for NaCl tablets are 6 to 9 g daily in divided doses (e.g., 2–3 g two or three times per day). Loop diuretics decrease the medullary osmotic gradient necessary for water reabsorption in the collecting duct by inhibiting the Na-K+-2Cl– cotransporter and therefore, increase free water excretion. The dose of furosemide is 20 to 40 mg per oral one time per day. They are not approved by the U.S. FDA to treat hyponatremia. Daily intake of 0.25 to 0.50 g/kg urea or 600 to 1,200 mg demeclocycline can also be considered but has not been introduced in Korea.
Recommendation 6
We suggest treatment with vaptans in SIAD patients with moderate to severe hyponatremia (B, low).
Remarks:
1. There is no direct comparison of vasopressin receptor antagonists with loop diuretics in patients with SIAD. We compared the effects of vasopressin receptor antagonists with water restriction or placebo.
2. Vaptans have a beneficial effect on normalization of SNa in SIAD patients compared with water restriction or placebo.
3. Vaptans do not increase the risk of overcorrection of hyponatremia in SIAD patients compared with water restriction or placebo.
4. Vaptans do not improve survival in SIAD patients compared with water restriction or placebo.
Vaptans correct hyponatremia, effectively causing urinary excretion of free water without increased sodium excretion [34]. However, the European guideline recommends against vasopressin receptor antagonists in SIAD patients without severe or moderately severe symptoms. They emphasized that the safety of vaptans should be considered. First, vaptans can lead to overcorrection of SNa concentration, especially in patients with severe hyponatremia. Second, hepatotoxicity was reported in autosomal dominant polycystic kidney disease patients on high doses of tolvaptan [1].
Previous studies focused on short-term outcomes such as normalization of SNa or overcorrection. Few studies evaluated the effect of vaptans stratified by volume status: hypervolemia or euvolemia [35,36]. Aggravation of hyponatremia can cause severe symptoms such as poor oral intake, general weakness or altered consciousness, leading to hospitalization. Long-term outcomes were worse in patients who developed repeated symptoms of hyponatremia [19,37].
Placebo or water restriction was used as a control group for vaptans, as there were no studies comparing vaptans with loop diuretics in the previous guidelines or our literature search. Therefore, we reviewed 12 RCTs evaluating the effect of vaptans on sodium correction, survival or complications compared with water restriction or placebo [3,38–48]. All RCTs included euvolemic hyponatremia patients: three included only euvolemic hyponatremia, nine included euvolemic or hypervolemic patients. In our meta-analysis, vaptans effectively normalized SNa in euvolemic hyponatremia. Vaptans did not decrease mortality in euvolemic hyponatremia. Although data on complications of vaptans are insufficient, vaptans did not increase the risk of overcorrection of hyponatremia compared with water restriction or placebo. There were few data regarding hepatotoxicity in euvolemic hyponatremia. In conclusion, vaptans can effectively normalize SNa concentration without increased risk of overcorrection or death.
The evidence was low quality and grade (B) in this recommendation because the included participants were not clearly defined as having SIAD, but instead as hypoosmolar hyponatremia with euvolemia or hypervolemia in the included RCTs. However, most euvolemic hyponatremia is SIAD and the diagnostic criteria for SIAD are not clearly defined [49]. Experts agreed that most of included participants might have SIAD. Therefore, we suggest using vaptans in SIAD patients with moderate to severe hyponatremia.
(3) In patients with hypovolemic hyponatremia, restoring extracellular fluid volume with intravenous isotonic fluid (0.9% saline) or balanced crystalloid will suppress vasopressin secretion causing electrolyte-free water excretion to increase [1–3]. After a 0.5 to 1.0 L infusion of isotonic fluid or balanced crystalloid, hyponatremia will begin to be corrected without signs of volume overload in patients with hypovolemic hyponatremia [2].
4) Overcorrection and re-lowering treatment of serum sodium
Target correction is achieving a SNa increase of 5 to 9 mmol/L/10 to 17 mmol/L within the first 24/48 hours or reaching a SNa of 130 mmol/L [1]. SNa concentration should not be corrected by ≥10 mmol/L per day, with a more stringent limit of >8 mmol/L per day for patients at high risk of ODS (SNa concentration of ≤105 mmol/L, hypokalemia, alcoholism, malnutrition, and advanced liver disease) [2]. Overcorrection (defined as an increase in the SNa level by >12/18 mmol/L within 24/48 hours) may result in ODS [1–3]. ODS has no specific treatment and has a poor prognosis. Therefore, caution is required when correcting hyponatremia [1]. We recommend discontinuing ongoing treatment and prompt intervention to re-lower SNa concentration based on electrolyte-free water (5% dextrose solutions) and/or desmopressin if overcorrection occurs (Table 4) [1–3]. Desmopressin use as a re-lowering treatment for SNa is discussed in Recommendation 7. Diuresis as a result of antagonizing vasopressin-mediated free water retention by volume repletion or discontinuing hyponatremia inducing medications often occurs when correcting hyponatremia and is a common reason for overcorrection. Therefore, urine output should be monitored during treatment.
Recommendation 7
We suggest that desmopressin should be applied individually according to risk factors affecting overcorrection, hypertonic saline therapeutic regimen, and whether to administer dextrose solution during overcorrection in patients with hyponatremia (B, very low).
RRemarks:
1. There is no evidence that administration of desmopressin as a proactive or reactive strategy is effective for preventing overcorrection.
2. Administration of desmopressin in patients with hyponatremia has the potential to increase the incidence of ODS compared to no administration, but drawing a valid conclusion is difficult due to the low level of evidence.
3. Administration of desmopressin for the prevention of overcorrection in hyponatremic patients has the potential to improve survival compared to non-administration, but drawing a valid conclusion is difficult due to the low level of evidence.
Desmopressin is an antidiuretic hormone that binds to the V2 receptor in the collecting duct and increases the expression of aquaporin channels to increase water reabsorption of urine passing through the collecting duct. A number of studies found that administration of desmopressin can prevent rapid correction of hyponatremia or stabilize SNa correction rate through water reabsorption if it has already been rapidly corrected. The European guideline recommended that 2 µg of intravenous desmopressin be given at intervals of 8 hours or more to prevent rapid correction (grade of recommendation 1D). In addition, they also recommend injecting 10 mL/kg of electrolyte-free water (dextrose solution) for 1 hour in consideration of urine volume and fluid balance (grade of recommendation 1D). However, there have been no prospective studies on this recommendation. In two retrospective observational studies cited in the guidelines, SNa concentration was corrected using desmopressin or electrolyte-free water to the target of 12 mmol/L within 24 hours and less than 18 mmol/L within 48 hours when overcorrection occurred [50]. In one of these retrospective studies, the proactive strategies in which hypertonic fluid and desmopressin were concurrently administered increased SNa concentration stably, and SNa concentration was maintained within the target range for 24 and 48 hours [51]. However, the quality of the studies included in the guidelines varied, the criteria for classification of hyponatremia among the study subjects varied, and there was no comparative study in which patients not using desmopressin were included as a control group. Eighty patients using desmopressin were classified into three strategies in one SR of desmopressin use for hyponatremia in 2015 [52]. The proactive strategy was based on initial SNa concentration, with desmopressin administered before concentration changes of SNa. In the reactive strategy, desmopressin was administered according to an increase in the concentration of SNa or urine output. In the rescue strategy, desmopressin was administrated to re-lower SNa concentration in case of overcorrection. However, final conclusions could not be drawn on the optimal strategy for administration of desmopressin for hyponatremia due to limitations of the study design and sample size.
In this guideline, we evaluated one SR study and three observational studies on whether the administration of desmopressin for hyponatremia has additional benefit in the prevention of overcorrection, complications (ODS), and prognosis (survival to discharge) compared to the non-administered group [50,52–54]. As a result of our analysis, overcorrection prevention did not differ significantly when comparing the group with and without use of desmopressin (proactive and reactive strategies). When the desmopressin use group and the non-desmopressin group were compared, including proactive, reactive, and rescue therapy, the incidence of ODS was higher in the group using desmopressin, but ODS occurred in only one or two cases, and there was a possibility of selection bias. When comparing the survival to discharge of the groups administered and not administered desmopressin (proactive, reactive and rescue strategies), survival rate was significantly higher in the desmopressin use group. However, a larger sample size and prospective studies are needed to determine the optimal strategy for desmopressin administration in hyponatremia.
5) Special situations 1. Treatment of hyponatremia in patients with brain lesions
Recommendation 8
We consider it reasonable that treatment with hypertonic or isotonic saline infusion, oral sodium chloride, or fludrocortisone for the correction of hypoosmolar hyponatremia should be individualized among patients with cerebral diseases (E).
Remarks:
1. The causes of hypoosmolar hyponatremia among patients with cerebral diseases are diverse, and include SIAD, CSW, and insufficient cortisol secretion.
2. There is insufficient evidence that hypoosmolar hyponatremia in patients with cerebral diseases can be effectively corrected with a crystalloid solution, including normal saline.
Hyponatremia occurs very frequently in patients with various cerebral diseases such as traumatic brain injury, intracranial or subarachnoid hemorrhage, brain tumor, brain surgery, cerebral infarction, and meningitis. The incidence of hyponatremia in traumatic brain injury patients has been reported to be 27% to 51% [55,56], 40% to 45% in cerebral infarction patients [57], 14% to 63% in subarachnoid hemorrhage [57,58], and 15% to 20% of brain tumor patients [59]. Various factors such as SIAD, CSW, and insufficient secretion of cortisol are major causes of hyponatremia in cerebral diseases. The most common cause of hyponatremia in patients with cerebral disease is SIAD, accounting for approximately 62%, and volume deficit or CSW accounted for about 30% [59].
Concomitant hyponatremia in patients with cerebral disease is closely related to the deterioration of patient condition. Therefore, appropriate treatment depending on the cause of hyponatremia is highly recommended [2]. However, in a clinical setting, it is not easy to accurately determine the cause based on patient volume status and it may require several hours or days to complete diagnostic tests and evaluations to determine the cause. Therefore, the CPG Committee sought to suggest appropriate treatment guidelines for hypoosmolar hyponatremia in patients with various cerebral diseases. We searched Ovid MEDLINE, Embase, Cochrane Library, and KMbase, and found a total of 72 research papers through additional manual searches. We selected 66 documents excluding duplicates and reviewed 13 original texts. We could not find any documents that suitably addressed this key question. Therefore, an expert consensus was made by organizing the results of related research with the existing CPGs.
The American guideline suggested that in the case of hyponatremia in patients with cerebral disease, treatment such as normal saline, oral salt supplementation, hypertonic saline, and fludrocortisone may be considered [2]. In general, treatment guidelines recommend water restriction or hypertonic saline depending on the severity of hyponatremia in SIAD. In addition, volume depletion is common in patients with various cerebral diseases [60]. In particular, volume deficit (body fluid deficiency) accompanying CSW can result in hyponatremia. The occurrence of cerebral infarction and other neurological complications increases when water restriction is implemented in patients with cerebral disease [61,62]. Therefore, in the case of hyponatremia accompanying these cerebral diseases, clinicians should avoid volume depletion through water restriction [63].
Hyponatremia accompanied by neurological symptoms related to hyponatremia can be corrected through hypertonic saline to prevent the progression of neurological complications. However, it should be treated cautiously by controlling the rate of correction to avoid overcorrection in accordance with the general principles of hyponatremia correction rate. Asymptomatic hypoosmolar hyponatremia occurring in patients with cerebral diseases can be initially corrected by preferentially using isotonic crystalloid solution including normal saline, unless volume depletion is clearly excluded by clinical judgment. In the case of asymptomatic hypoosmolar hyponatremia that does not improve despite administering isotonic crystalloid solution such as normal saline, evaluation and tests for differential diagnosis may be performed, and concomitant salt supplementation such as hypertonic saline or oral salt may be considered. In the case of CSW, hyponatremia can be corrected with a mineralocorticoid such as fludrocortisone. Hasan et al. [64] demonstrated the effectiveness of fludrocortisone treatment for the prevention of renal salt excretion and volume status decrease in 91 patients with subarachnoid hemorrhage, which is commonly accompanied by CSW, through a RCT. Misra et al. [65] conducted a RCT on 38 hyponatremic patients with tuberculous meningitis due to CSW and showed that fludrocortisone treatment can correct hyponatremia earlier than normal saline. Further evidence is needed for specific recommendations in hyponatremia patients with cerebral diseases.
6) Special situations 2. Selection of maintenance fluid to prevent hyponatremia in children aged ≤18 years
Recommendation 9
1. To prevent hyponatremia, we recommend the administration of isotonic fluids as maintenance fluid therapy in hospitalized pediatric patients over 1 month and under 18 years of age (A, high).
2. There are insufficient data to make a recommendation regarding administrating isotonic fluids as maintenance fluid therapy to prevent hyponatremia in neonates because of the risk of hypernatremia (I, moderate).
Remarks:
1. In maintenance fluid therapy for children and adolescents over 1 month and under 18 years of age, the administration of isotonic fluid is effective for preventing the development of hyponatremia and has similar risk of hypernatremia compared to the administration of hypotonic fluids.
2. In maintenance fluid therapy for neonates less than 1 month old, the administration of isotonic fluid is effective for preventing the development of hyponatremia and leads to a higher risk of developing hypernatremia compared to the administration of hypotonic fluids.
Traditionally, hypotonic solutions based on the Holliday-Segar formula have been used as maintenance fluids in hospitalized pediatric patients under the age of 18 years. However, the development of hyponatremia associated with hypotonic solution administration and related neurologic complications and death have been continuously reported. In addition, children are more likely to develop severe symptoms associated with hyponatremia because the brain is relatively large compared to the skull in children. Consequently, there has been controversy over the composition of optimal maintenance fluid. In 2018, the American Academy of Pediatrics recommended an isotonic solution as a maintenance fluid for pediatric patients over 1 month old by integrating evidence from 17 RCTs and seven SRs (grade of recommendation 1A) [66]. In the 2020 revised NICE (National Institute for Health and Care Excellence) guidelines, isotonic solutions were recommended as maintenance fluids in children, including term neonates 8 days of age or older [67]. However, RCT studies have shown inconsistent results.
In this guideline, we performed a meta-analysis by synthesizing 18 RCTs (16 RCTs for children over 1 month and two RCTs for newborns) [68–85] and seven SRs [86–88]. We sought to examine whether the administration of isotonic fluid compared to hypotonic fluids reduced the incidence of hyponatremia without increasing the risk of hypernatremia during maintenance fluid therapy in pediatric patients including newborns. In 18 RCTs, normal saline or Ringer’s lactate solution as an isotonic solution and 0.20% to 0.45% saline as a hypotonic solution were administered to hospitalized pediatric patients. In most studies, 5% dextrose solution was added to the maintenance fluid. A total of 3,231 patients were included in 16 RCT studies of children 1 month and older, including patients who were hospitalized for surgery or were admitted to the intensive care unit, and those who were hospitalized for pneumonia or central nervous system infection. Of these, isotonic solutions were used in 1,608 patients and hypotonic solutions were used in 1,623 patients as maintenance fluid. The incidence of hyponatremia in patients using isotonic solution as maintenance treatment was significantly lower than in the group using hypotonic solution as maintenance treatment (OR, 0.32; 95% CI, 0.24–0.43; p < 0.001). Although hypernatremia was increased in patients administered isotonic solutions in some studies [68–71,74,78], there was no significant difference in a meta-analysis between isotonic fluid and hypotonic fluid (OR, 1.67; 95% CI, 0.92–3.04; p = 0.09). In two non-RCTs, the incidence of hyponatremia had a tendency to be low in patients administered isotonic fluids; however, this was not statistically significant (OR, 0.54; 95% CI, 0.28–1.02; p = 0.05), and the incidence of hypernatremia in patients receiving isotonic fluids was not significantly different from that in patients receiving hypotonic fluids (OR, 1.25; 95% CI, 0.73–2.13; p = 0.58). Two RCTs enrolled a total of 144 neonates, including premature babies aged 34 weeks or older and full-term neonates. Of these, 73 patients received isotonic fluid and 71 received 0.15% to 0.20% hypotonic fluid. These studies reported a significantly lower incidence of hyponatremia in patients receiving isotonic fluids (OR, 0.11; 95% CI, 0.03–0.35; p < 0.001) than in patients receiving hypotonic fluids. However, the incidence of hypernatremia was significantly higher in patients receiving isotonic fluids than in patients receiving hypotonic fluids (OR, 8.24; 95% CI, 1.84–36.91; p < 0.001) [73,77].
Footnotes
Access to the full-text version
The full-text version of this clinical practice guideline is available on the Korean Society of Nephrology website (https://doi.org/10.23876/j.krcp.33.666).
Conflict of interest
All authors have no conflicts of interest to declare.
References
- 1.Spasovski G, Vanholder R, Allolio B, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Nephrol Dial Transplant. 2014;29 Suppl 2:i1–i39. doi: 10.1093/ndt/gfu040. [DOI] [PubMed] [Google Scholar]
- 2.Verbalis JG, Goldsmith SR, Greenberg A, et al. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. 2013;126:S1–S42. doi: 10.1016/j.amjmed.2013.07.006. [DOI] [PubMed] [Google Scholar]
- 3.Hoorn EJ, Zietse R. Diagnosis and treatment of hyponatremia: compilation of the guidelines. J Am Soc Nephrol. 2017;28:1340–1349. doi: 10.1681/ASN.2016101139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hillier TA, Abbott RD, Barrett EJ. Hyponatremia: evaluating the correction factor for hyperglycemia. Am J Med. 1999;106:399–403. doi: 10.1016/s0002-9343(99)00055-8. [DOI] [PubMed] [Google Scholar]
- 5.Filippatos TD, Makri A, Elisaf MS, Liamis G. Hyponatremia in the elderly: challenges and solutions. Clin Interv Aging. 2017;12:1957–1965. doi: 10.2147/CIA.S138535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ebell MH, Radke T, Gardner J. A systematic review of the efficacy and safety of desmopressin for nocturia in adults. J Urol. 2014;192:829–835. doi: 10.1016/j.juro.2014.03.095. [DOI] [PubMed] [Google Scholar]
- 7.Decaux G, Musch W. Clinical laboratory evaluation of the syndrome of inappropriate secretion of antidiuretic hormone. Clin J Am Soc Nephrol. 2008;3:1175–1184. doi: 10.2215/CJN.04431007. [DOI] [PubMed] [Google Scholar]
- 8.Fenske W, Störk S, Koschker AC, et al. Value of fractional uric acid excretion in differential diagnosis of hyponatremic patients on diuretics. J Clin Endocrinol Metab. 2008;93:2991–2997. doi: 10.1210/jc.2008-0330. [DOI] [PubMed] [Google Scholar]
- 9.Nigro N, Winzeler B, Suter-Widmer I, et al. Copeptin levels and commonly used laboratory parameters in hospitalised patients with severe hypernatraemia - the “Co-MED study”. Crit Care. 2018;22:33. doi: 10.1186/s13054-018-1955-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bassi V, Fattoruso O. The role of fractional excretion of uric acid in the differential diagnosis of hypotonic hyponatraemia in patients with diuretic therapy. Cureus. 2020;12:e7762. doi: 10.7759/cureus.7762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Musch W, Decaux G. Utility and limitations of biochemical parameters in the evaluation of hyponatremia in the elderly. Int Urol Nephrol. 2001;32:475–493. doi: 10.1023/a:1017586004688. [DOI] [PubMed] [Google Scholar]
- 12.Musch W, Thimpont J, Vandervelde D, Verhaeverbeke I, Berghmans T, Decaux G. Combined fractional excretion of sodium and urea better predicts response to saline in hyponatremia than do usual clinical and biochemical parameters. Am J Med. 1995;99:348–355. doi: 10.1016/s0002-9343(99)80180-6. [DOI] [PubMed] [Google Scholar]
- 13.Maesaka JK, Imbriano LJ, Miyawaki N. Determining fractional urate excretion rates in hyponatremic conditions and improved methods to distinguish cerebral/renal salt wasting from the syndrome of inappropriate secretion of antidiuretic hormone. Front Med (Lausanne) 2018;5:319. doi: 10.3389/fmed.2018.00319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Choi HK, Soriano LC, Zhang Y, Rodríguez LA. Antihypertensive drugs and risk of incident gout among patients with hypertension: population based case-control study. BMJ. 2012;344:d8190. doi: 10.1136/bmj.d8190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Fenske W, Störk S, Blechschmidt A, Maier SG, Morgenthaler NG, Allolio B. Copeptin in the differential diagnosis of hyponatremia. J Clin Endocrinol Metab. 2009;94:123–129. doi: 10.1210/jc.2008-1426. [DOI] [PubMed] [Google Scholar]
- 16.Go S, Kim S, Son HE, et al. Association between copeptin levels and treatment responses to hypertonic saline infusion in patients with symptomatic hyponatremia: a prospective cohort study. Kidney Res Clin Pract. 2021;40:371–382. doi: 10.23876/j.krcp.20.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Baek SH, Jo YH, Ahn S, et al. Risk of overcorrection in rapid intermittent bolus vs slow continuous infusion therapies of hypertonic saline for patients with symptomatic hyponatremia: the SALSA randomized clinical trial. JAMA Intern Med. 2021;181:81–92. doi: 10.1001/jamainternmed.2020.5519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Garrahy A, Dineen R, Hannon AM, et al. Continuous versus bolus infusion of hypertonic saline in the treatment of symptomatic hyponatremia caused by SIAD. J Clin Endocrinol Metab. 2019;104:3595–3602. doi: 10.1210/jc.2019-00044. [DOI] [PubMed] [Google Scholar]
- 19.Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009;122:857–865. doi: 10.1016/j.amjmed.2009.01.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Doshi SM, Shah P, Lei X, Lahoti A, Salahudeen AK. Hyponatremia in hospitalized cancer patients and its impact on clinical outcomes. Am J Kidney Dis. 2012;59:222–228. doi: 10.1053/j.ajkd.2011.08.029. [DOI] [PubMed] [Google Scholar]
- 21.Kovesdy CP, Lott EH, Lu JL, et al. Hyponatremia, hypernatremia, and mortality in patients with chronic kidney disease with and without congestive heart failure. Circulation. 2012;125:677–684. doi: 10.1161/CIRCULATIONAHA.111.065391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Choi JS, Kim CS, Bae EH, et al. Prognostic impact of hyponatremia occurring at various time points during hospitalization on mortality in patients with acute myocardial infarction. Medicine (Baltimore) 2017;96:e7023. doi: 10.1097/MD.0000000000007023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jujo K, Saito K, Ishida I, et al. Randomized pilot trial comparing tolvaptan with furosemide on renal and neurohumoral effects in acute heart failure. ESC Heart Fail. 2016;3:177–188. doi: 10.1002/ehf2.12088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Tanaka T, Minatoguchi S, Yamada Y, et al. Addition of tolvaptan compared with increased dose of furosemide in heart failure patients with chronic kidney disease under furosemide treatment. Circ Rep. 2018;1:35–41. doi: 10.1253/circrep.CR-18-0002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tominaga N, Kida K, Inomata T, et al. Effects of tolvaptan addition to furosemide in normo- and hyponatremia patients with heart failure and chronic kidney disease stages G3b-5: a subanalysis of the K-STAR study. Am J Nephrol. 2017;46:417–426. doi: 10.1159/000481995. [DOI] [PubMed] [Google Scholar]
- 26.Felker GM, Mentz RJ, Cole RT, et al. Efficacy and safety of tolvaptan in patients hospitalized with acute heart failure. J Am Coll Cardiol. 2017;69:1399–1406. doi: 10.1016/j.jacc.2016.09.004. [DOI] [PubMed] [Google Scholar]
- 27.Kimura K, Momose T, Hasegawa T, et al. Early administration of tolvaptan preserves renal function in elderly patients with acute decompensated heart failure. J Cardiol. 2016;67:399–405. doi: 10.1016/j.jjcc.2015.09.020. [DOI] [PubMed] [Google Scholar]
- 28.Kin H, Matsumura K, Yamamoto Y, et al. Renoprotective effect of tolvaptan in patients with new-onset acute heart failure. ESC Heart Fail. 2020;7:1764–1770. doi: 10.1002/ehf2.12738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Konstam MA, Kiernan M, Chandler A, et al. Short-term effects of tolvaptan in patients with acute heart failure and volume overload. J Am Coll Cardiol. 2017;69:1409–1419. doi: 10.1016/j.jacc.2016.12.035. [DOI] [PubMed] [Google Scholar]
- 30.Matsue Y, Suzuki M, Torii S, et al. Clinical effectiveness of tolvaptan in patients with acute heart failure and renal dysfunction. J Card Fail. 2016;22:423–432. doi: 10.1016/j.cardfail.2016.02.007. [DOI] [PubMed] [Google Scholar]
- 31.Shanmugam E, Doss CR, George M, et al. Effect of tolvaptan on acute heart failure with hyponatremia: a randomized, double blind, controlled clinical trial. Indian Heart J. 2016;68 Suppl 1:S15–S21. doi: 10.1016/j.ihj.2015.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ellison DH, Berl T. Clinical practice. The syndrome of inappropriate antidiuresis. N Engl J Med. 2007;356:2064–2072. doi: 10.1056/NEJMcp066837. [DOI] [PubMed] [Google Scholar]
- 33.Rondon-Berrios H, Berl T. Mild chronic hyponatremia in the ambulatory setting: significance and management. Clin J Am Soc Nephrol. 2015;10:2268–2278. doi: 10.2215/CJN.00170115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Berl T, Quittnat-Pelletier F, Verbalis JG, et al. Oral tolvaptan is safe and effective in chronic hyponatremia. J Am Soc Nephrol. 2010;21:705–712. doi: 10.1681/ASN.2009080857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bhandari S, Peri A, Cranston I, et al. A systematic review of known interventions for the treatment of chronic nonhypovolaemic hypotonic hyponatraemia and a meta-analysis of the vaptans. Clin Endocrinol (Oxf) 2017;86:761–771. doi: 10.1111/cen.13315. [DOI] [PubMed] [Google Scholar]
- 36.Nagler EV, Haller MC, Van Biesen W, Vanholder R, Craig JC, Webster AC. Interventions for chronic non-hypovolaemic hypotonic hyponatraemia. Cochrane Database Syst Rev. 2018;6:CD010965. doi: 10.1002/14651858.CD010965.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Goldberg A, Hammerman H, Petcherski S, et al. Hyponatremia and long-term mortality in survivors of acute ST-elevation myocardial infarction. Arch Intern Med. 2006;166:781–786. doi: 10.1001/archinte.166.7.781. [DOI] [PubMed] [Google Scholar]
- 38.Torres VE, Chapman AB, Devuyst O, et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med. 2012;367:2407–2418. doi: 10.1056/NEJMoa1205511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Abraham WT, Decaux G, Josiassen RC, et al. Oral lixivaptan effectively increases serum sodium concentrations in outpatients with euvolemic hyponatremia. Kidney Int. 2012;82:1215–1222. doi: 10.1038/ki.2012.274. [DOI] [PubMed] [Google Scholar]
- 40.Annane D, Decaux G, Smith N, Conivaptan Study Group Efficacy and safety of oral conivaptan, a vasopressin-receptor antagonist, evaluated in a randomized, controlled trial in patients with euvolemic or hypervolemic hyponatremia. Am J Med Sci. 2009;337:28–36. doi: 10.1097/MAJ.0b013e31817b8148. [DOI] [PubMed] [Google Scholar]
- 41.Ghali JK, Koren MJ, Taylor JR, et al. Efficacy and safety of oral conivaptan: a V1A/V2 vasopressin receptor antagonist, assessed in a randomized, placebo-controlled trial in patients with euvolemic or hypervolemic hyponatremia. J Clin Endocrinol Metab. 2006;91:2145–2152. doi: 10.1210/jc.2005-2287. [DOI] [PubMed] [Google Scholar]
- 42.Gheorghiade M, Gottlieb SS, Udelson JE, et al. Vasopressin v(2) receptor blockade with tolvaptan versus fluid restriction in the treatment of hyponatremia. Am J Cardiol. 2006;97:1064–1067. doi: 10.1016/j.amjcard.2005.10.050. [DOI] [PubMed] [Google Scholar]
- 43.Abraham WT, Hensen J, Gross PA, et al. Lixivaptan safely and effectively corrects serum sodium concentrations in hospitalized patients with euvolemic hyponatremia. Kidney Int. 2012;82:1223–1230. doi: 10.1038/ki.2012.275. [DOI] [PubMed] [Google Scholar]
- 44.Chen S, Zhao JJ, Tong NW, et al. Randomized, double blinded, placebo-controlled trial to evaluate the efficacy and safety of tolvaptan in Chinese patients with hyponatremia caused by SIADH. J Clin Pharmacol. 2014;54:1362–1367. doi: 10.1002/jcph.342. [DOI] [PubMed] [Google Scholar]
- 45.Koren MJ, Hamad A, Klasen S, Abeyratne A, McNutt BE, Kalra S. Efficacy and safety of 30-minute infusions of conivaptan in euvolemic and hypervolemic hyponatremia. Am J Health Syst Pharm. 2011;68:818–827. doi: 10.2146/ajhp100260. [DOI] [PubMed] [Google Scholar]
- 46.Salahudeen AK, Ali N, George M, Lahoti A, Palla S. Tolvaptan in hospitalized cancer patients with hyponatremia: a double-blind, randomized, placebo-controlled clinical trial on efficacy and safety. Cancer. 2014;120:744–751. doi: 10.1002/cncr.28468. [DOI] [PubMed] [Google Scholar]
- 47.Schrier RW, Gross P, Gheorghiade M, et al. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N Engl J Med. 2006;355:2099–2112. doi: 10.1056/NEJMoa065181. [DOI] [PubMed] [Google Scholar]
- 48.Soupart A, Gross P, Legros JJ, et al. Successful long-term treatment of hyponatremia in syndrome of inappropriate antidiuretic hormone secretion with satavaptan (SR121463B), an orally active nonpeptide vasopressin V2-receptor antagonist. Clin J Am Soc Nephrol. 2006;1:1154–1160. doi: 10.2215/CJN.00160106. [DOI] [PubMed] [Google Scholar]
- 49.Wong F, Blei AT, Blendis LM, Thuluvath PJ. A vasopressin receptor antagonist (VPA-985) improves serum sodium concentration in patients with hyponatremia: a multicenter, randomized, placebo-controlled trial. Hepatology. 2003;37:182–191. doi: 10.1053/jhep.2003.50021. [DOI] [PubMed] [Google Scholar]
- 50.Perianayagam A, Sterns RH, Silver SM, et al. DDAVP is effective in preventing and reversing inadvertent overcorrection of hyponatremia. Clin J Am Soc Nephrol. 2008;3:331–336. doi: 10.2215/CJN.03190807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Sood L, Sterns RH, Hix JK, Silver SM, Chen L. Hypertonic saline and desmopressin: a simple strategy for safe correction of severe hyponatremia. Am J Kidney Dis. 2013;61:571–578. doi: 10.1053/j.ajkd.2012.11.032. [DOI] [PubMed] [Google Scholar]
- 52.MacMillan TE, Tang T, Cavalcanti RB. Desmopressin to prevent rapid sodium correction in severe hyponatremia: a systematic review. Am J Med. 2015;128:1362.e15–1362.e24. doi: 10.1016/j.amjmed.2015.04.040. [DOI] [PubMed] [Google Scholar]
- 53.MacMillan TE, Cavalcanti RB. Outcomes in severe hyponatremia treated with and without desmopressin. Am J Med. 2018;131:317.e1–317.e10. doi: 10.1016/j.amjmed.2017.09.048. [DOI] [PubMed] [Google Scholar]
- 54.Ward FL, Tobe SW, Naimark DMJ. The role of desmopressin in the management of severe, hypovolemic hyponatremia: a single-center, comparative analysis. Can J Kidney Health Dis. 2018;5:2054358118761051. doi: 10.1177/2054358118761051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lohani S, Devkota UP. Hyponatremia in patients with traumatic brain injury: etiology, incidence, and severity correlation. World Neurosurg. 2011;76:355–360. doi: 10.1016/j.wneu.2011.03.042. [DOI] [PubMed] [Google Scholar]
- 56.Yumoto T, Sato K, Ugawa T, Ichiba S, Ujike Y. Prevalence, risk factors, and short-term consequences of traumatic brain injury-associated hyponatremia. Acta Med Okayama. 2015;69:213–218. doi: 10.18926/AMO/53557. [DOI] [PubMed] [Google Scholar]
- 57.Barkas F, Liamis G, Milionis H. Hyponatremia in acute stroke: to treat or not to treat? J Stroke Cerebrovasc Dis. 2019;28:104421. doi: 10.1016/j.jstrokecerebrovasdis.2019.104421. [DOI] [PubMed] [Google Scholar]
- 58.Mapa B, Taylor BE, Appelboom G, Bruce EM, Claassen J, Connolly ES., Jr Impact of hyponatremia on morbidity, mortality, and complications after aneurysmal subarachnoid hemorrhage: a systematic review. World Neurosurg. 2016;85:305–314. doi: 10.1016/j.wneu.2015.08.054. [DOI] [PubMed] [Google Scholar]
- 59.Sherlock M, O’Sullivan E, Agha A, et al. Incidence and pathophysiology of severe hyponatraemia in neurosurgical patients. Postgrad Med J. 2009;85:171–175. doi: 10.1136/pgmj.2008.072819. [DOI] [PubMed] [Google Scholar]
- 60.Sivakumar V, Rajshekhar V, Chandy MJ. Management of neurosurgical patients with hyponatremia and natriuresis. Neurosurgery. 1994;34:269–274. doi: 10.1227/00006123-199402000-00010. [DOI] [PubMed] [Google Scholar]
- 61.Hasan D, Vermeulen M, Wijdicks EF, Hijdra A, van Gijn J. Effect of fluid intake and antihypertensive treatment on cerebral ischemia after subarachnoid hemorrhage. Stroke. 1989;20:1511–1515. doi: 10.1161/01.str.20.11.1511. [DOI] [PubMed] [Google Scholar]
- 62.Wijdicks EF, Vermeulen M, Hijdra A, van Gijn J. Hyponatremia and cerebral infarction in patients with ruptured intracranial aneurysms: is fluid restriction harmful? Ann Neurol. 1985;17:137–140. doi: 10.1002/ana.410170206. [DOI] [PubMed] [Google Scholar]
- 63.Rahman M, Friedman WA. Hyponatremia in neurosurgical patients: clinical guidelines development. Neurosurgery. 2009;65:925–935. doi: 10.1227/01.NEU.0000358954.62182.B3. [DOI] [PubMed] [Google Scholar]
- 64.Hasan D, Lindsay KW, Wijdicks EF, et al. Effect of fludrocortisone acetate in patients with subarachnoid hemorrhage. Stroke. 1989;20:1156–1161. doi: 10.1161/01.str.20.9.1156. [DOI] [PubMed] [Google Scholar]
- 65.Misra UK, Kalita J, Kumar M. Safety and efficacy of fludrocortisone in the treatment of cerebral salt wasting in patients with tuberculous meningitis: a randomized clinical trial. JAMA Neurol. 2018;75:1383–1391. doi: 10.1001/jamaneurol.2018.2178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Feld LG, Neuspiel DR, Foster BA, et al. Clinical practice guideline: maintenance intravenous fluids in children. Pediatrics. 2018;142:e20183083. doi: 10.1542/peds.2018-3083. [DOI] [PubMed] [Google Scholar]
- 67.Neilson J, O’Neill F, Dawoud D, Crean P, Guideline Development Group Intravenous fluids in children and young people: summary of NICE guidance. BMJ. 2015;351:h6388. doi: 10.1136/bmj.h6388. [DOI] [PubMed] [Google Scholar]
- 68.Almeida HI, Mascarenhas MI, Loureiro HC, et al. The effect of NaCl 0.9% and NaCl 0.45% on sodium, chloride, and acid-base balance in a PICU population. J Pediatr (Rio J) 2015;91:499–505. doi: 10.1016/j.jped.2014.12.003. [DOI] [PubMed] [Google Scholar]
- 69.Bagri NK, Saurabh VK, Basu S, Kumar A. Isotonic versus hypotonic intravenous maintenance fluids in children: a randomized controlled trial. Indian J Pediatr. 2019;86:1011–1016. doi: 10.1007/s12098-019-03011-5. [DOI] [PubMed] [Google Scholar]
- 70.Balasubramanian K, Kumar P, Saini SS, Attri SV, Dutta S. Isotonic versus hypotonic fluid supplementation in term neonates with severe hyperbilirubinemia - a double-blind, randomized, controlled trial. Acta Paediatr. 2012;101:236–241. doi: 10.1111/j.1651-2227.2011.02508.x. [DOI] [PubMed] [Google Scholar]
- 71.Choong K, Arora S, Cheng J, et al. Hypotonic versus isotonic maintenance fluids after surgery for children: a randomized controlled trial. Pediatrics. 2011;128:857–866. doi: 10.1542/peds.2011-0415. [DOI] [PubMed] [Google Scholar]
- 72.Coulthard MG, Long DA, Ullman AJ, Ware RS. A randomised controlled trial of Hartmann’s solution versus half normal saline in postoperative paediatric spinal instrumentation and craniotomy patients. Arch Dis Child. 2012;97:491–496. doi: 10.1136/archdischild-2011-300221. [DOI] [PubMed] [Google Scholar]
- 73.Dathan K, Sundaram M. Comparison of isotonic versus hypotonic intravenous fluid for maintenance fluid therapy in neonates more than or equal to 34 weeks of gestational age - a randomized clinical trial. J Matern Fetal Neonatal Med. 2021 Apr 20; doi: 10.1080/14767058.2021.1911998. [Epub]. DOI: [DOI] [PubMed] [Google Scholar]
- 74.Friedman JN, Beck CE, DeGroot J, Geary DF, Sklansky DJ, Freedman SB. Comparison of isotonic and hypotonic intravenous maintenance fluids: a randomized clinical trial. JAMA Pediatr. 2015;169:445–451. doi: 10.1001/jamapediatrics.2014.3809. [DOI] [PubMed] [Google Scholar]
- 75.Kannan L, Lodha R, Vivekanandhan S, Bagga A, Kabra SK, Kabra M. Intravenous fluid regimen and hyponatraemia among children: a randomized controlled trial. Pediatr Nephrol. 2010;25:2303–2309. doi: 10.1007/s00467-010-1600-4. [DOI] [PubMed] [Google Scholar]
- 76.Kumar M, Mitra K, Jain R. Isotonic versus hypotonic saline as maintenance intravenous fluid therapy in children under 5 years of age admitted to general paediatric wards: a randomised controlled trial. Paediatr Int Child Health. 2020;40:44–49. doi: 10.1080/20469047.2019.1619059. [DOI] [PubMed] [Google Scholar]
- 77.Lehtiranta S, Honkila M, Kallio M, et al. Risk of electrolyte disorders in acutely ill children receiving commercially available plasmalike isotonic fluids: a randomized clinical trial. JAMA Pediatr. 2021;175:28–35. doi: 10.1001/jamapediatrics.2020.3383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.McNab S, Duke T, South M, et al. 140 mmol/L of sodium versus 77 mmol/L of sodium in maintenance intravenous fluid therapy for children in hospital (PIMS): a randomised controlled double-blind trial. Lancet. 2015;385:1190–1197. doi: 10.1016/S0140-6736(14)61459-8. [DOI] [PubMed] [Google Scholar]
- 79.Montañana PA, Modesto i Alapont V, Ocón AP, López PO, López Prats JL, Toledo Parreño JD. The use of isotonic fluid as maintenance therapy prevents iatrogenic hyponatremia in pediatrics: a randomized, controlled open study. Pediatr Crit Care Med. 2008;9:589–597. doi: 10.1097/PCC.0b013e31818d3192. [DOI] [PubMed] [Google Scholar]
- 80.Neville KA, Sandeman DJ, Rubinstein A, Henry GM, McGlynn M, Walker JL. Prevention of hyponatremia during maintenance intravenous fluid administration: a prospective randomized study of fluid type versus fluid rate. J Pediatr. 2010;156:313–319.e1-e2. doi: 10.1016/j.jpeds.2009.07.059. [DOI] [PubMed] [Google Scholar]
- 81.Pemde HK, Dutta AK, Sodani R, Mishra K. Isotonic intravenous maintenance fluid reduces hospital acquired hyponatremia in young children with central nervous system infections. Indian J Pediatr. 2015;82:13–18. doi: 10.1007/s12098-014-1436-1. [DOI] [PubMed] [Google Scholar]
- 82.Ramanathan S, Kumar P, Mishra K, Dutta AK. Isotonic versus hypotonic parenteral maintenance fluids in very severe pneumonia. Indian J Pediatr. 2016;83:27–32. doi: 10.1007/s12098-015-1791-6. [DOI] [PubMed] [Google Scholar]
- 83.Rey C, Los-Arcos M, Hernández A, Sánchez A, Díaz JJ, López-Herce J. Hypotonic versus isotonic maintenance fluids in critically ill children: a multicenter prospective randomized study. Acta Paediatr. 2011;100:1138–1143. doi: 10.1111/j.1651-2227.2011.02209.x. [DOI] [PubMed] [Google Scholar]
- 84.Shamim A, Afzal K, Ali SM. Safety and efficacy of isotonic (0.9%) vs. hypotonic (0.18%) saline as maintenance intravenous fluids in children: a randomized controlled trial. Indian Pediatr. 2014;51:969–974. doi: 10.1007/s13312-014-0542-5. [DOI] [PubMed] [Google Scholar]
- 85.Torres SF, Iolster T, Schnitzler EJ, Siaba Serrate AJ, Sticco NA, Rocca Rivarola M. Hypotonic and isotonic intravenous maintenance fluids in hospitalised paediatric patients: a randomised controlled trial. BMJ Paediatr Open. 2019;3:e000385. doi: 10.1136/bmjpo-2018-000385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Chromek M, Jungner Å, Rudolfson N, Ley D, Bockenhauer D, Hagander L. Hyponatraemia despite isotonic maintenance fluid therapy: a time series intervention study. Arch Dis Child. 2020;106:491–495. doi: 10.1136/archdischild-2019-318555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Velasco P, Alcaraz AJ, Oikonomopoulou N, Benito M, Moya R, Sánchez Á. Hospital-acquired hyponatremia: does the type of fluid therapy affect children admitted to intensive care? Rev Chil Pediatr. 2018;89:42–49. doi: 10.4067/S0370-41062018000100042. [DOI] [PubMed] [Google Scholar]
- 88.Tuzun F, Akcura Y, Duman N, Ozkan H. Comparison of isotonic and hypotonic intravenous fluids in term newborns: is it time to quit hypotonic fluids. J Matern Fetal Neonatal Med. 2022;35:356–361. doi: 10.1080/14767058.2020.1718094. [DOI] [PubMed] [Google Scholar]