

Abstract
Congenital deformities of the labyrinth of the inner ear may be associated with an increased risk of infection and varying degrees of otologic and vestibular dysfunction. Lateral semicircular canal abnormalities specifically can be associated with either normal hearing or hearing loss (conductive or sensorineural). In our patient, the acute symptoms of vertigo and tinnitus coincided with the diagnosis of COVID-19. It is unlikely that the symptomatology was related to the acute infection, even in the face of the underlying congenital abnormality. It has been shown that there is no correlation between the severity of the radiological abnormality and vestibular symptomatology in patients with isolated abnormalities of the semicircular canals. The abnormality can be asymptomatic.
Background
The Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) virus has been implicated in otologic and neurologic disorders.1,2 Malayala has described a case of COVID-19-induced vestibular neuritis.3 As it is a relatively new disease, there is still much work that needs to be done in this field.
Congenital deformities of the labyrinth of the inner ear may be associated with and increased risk of infection and varying degrees of otologic and vestibular dysfunction.4 Lateral semicircular canal abnormalities specifically can be associated with either normal hearing or hearing loss (conductive or sensorineural).5
We hereby present a case of a patient with a congenital confluence of the semicircular canal and vestibule that presented with sudden onset of vertigo and tinnitus associated with COVID-19 infection.
Case Presentation
Mr KP is a 44-year-old machine operator that was admitted to hospital after experiencing an acute onset of spontaneous vertigo with nausea/vomiting and associated right-sided nonpulsatile tinnitus.
He had recent contact with a patient with confirmed COVID-19 but was asymptomatic in terms of COVID-19 symptoms at the time of consultation.
His hearing was normal and there was no otalgia or otorrhea. There were no other otologic or neurological symptoms. He was alert and awake with no focal neurology. The middle ear was healthy and the tympanic membrane was intact bilaterally. Bedside vestibular testing revealed a falling tendency toward the right side. There was an associated horizontal torsional spontaneous nystagmus beating toward the unaffected side. Caloric testing revealed an impaired function of the semicircular canals. The pure tone and speech audiometry were within normal limits for his age (Figure 1).
Figure 1.

Pure tone audiogram demonstrating normal hearing.
He had no current or prior significant medical history, specifically there had been no previous episodic or chronic hearing disorder.
The COVID-19 throat swab was positive. His blood results (full blood count, urea and electrolytes, and C-reactive protein) were normal. The chest X-ray was showed no signs of chest infection.
His computed tomography scan showed a congenital lack of separation of the right lateral semicircular canal and vestibule, with no abnormal dilatation of the vestibular aqueduct, and normal appearing cochlea. The vestibule and the semicircular canal formed a common cavity. The right vestibular aqueduct was not enlarged (Figure 2). The cochlea had normal turns and was separate from the vestibule. The left inner ear labyrinth was normal. The left inner ear was normal in appearance.
Figure 2.

High-resolution axial cut computed tomography (CT) scan temporal bones orange arrow showing congenital lack of separation right semicircular canal.
These findings were confirmed on magnetic resonance imaging (MRI; Figure 3). There were no other abnormalities noted on the MRI scans.
Figure 3.
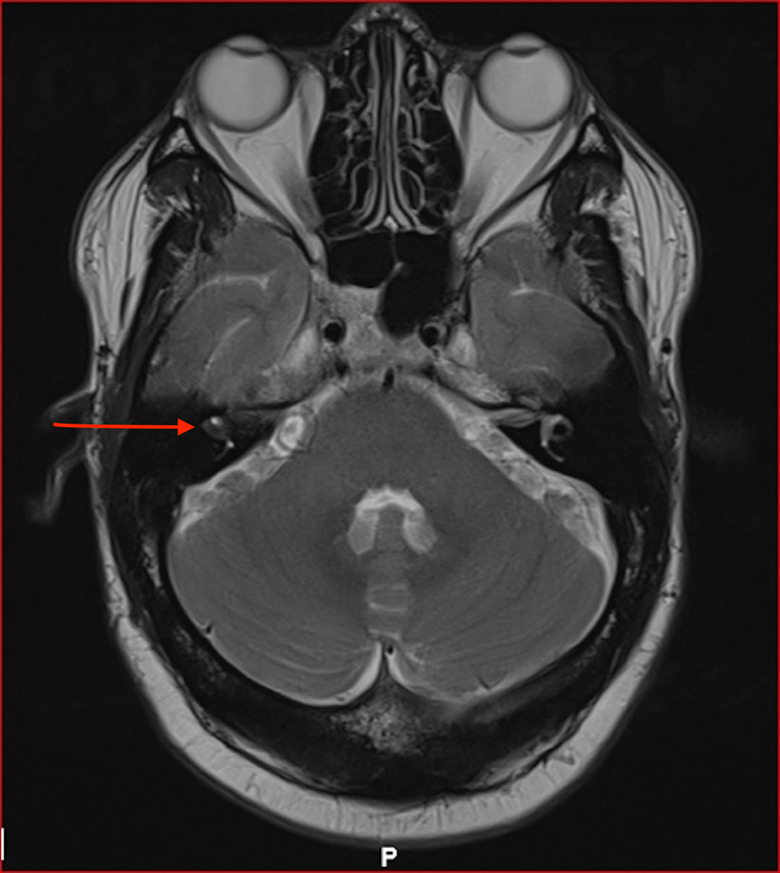
Magnetic resonance imaging (MRI) scan showing incomplete labyrinthine separation on the right (red arrow).
Discussion
In our patient, the acute symptoms of vertigo and tinnitus coincided with the diagnosis of COVID-19. It is unlikely that the symptomatology was related to the acute infection, even in the face of the underlying congenital abnormality. It has been shown that there is no correlation between the severity of the radiological abnormality and vestibular symptomatology in patients with isolated abnormalities of the semicircular canals. The abnormality can be asymptomatic.5
There has been a report of a patient in whom tinnitus accompanied by other features of otitis media (including hearing loss) heralded the onset of COVID-19, as was the case in our patient.6 Tinnitus has also been described in patients recovering from COVID-19. In a study from Manchester, United Kingdom,1 7% patients had self-reported tinnitus, with no accompanying hearing loss.7 Vertigo has been described as a neurological manifestation in patients with underlying COVID-19.1
Neurological disorders in the setting of COVID-19 usually occur in older patients with comorbidities and in critically ill patients.8 The vertigo in our patient is likely due to inner ear pathology, as there were no other features of neurological disease clinically and his MRI scans did not show any evidence of the features described previously in coronavirus infections, that is, encephalitis, leptomeningeal enhancement, and vascular complications such as microbleeds, subarachnoid hemorrhage, and infarcts.8
The patient symptoms coincided with the COVID-19 infection, though association is not necessarily causation. This case serves to highlight the increasing spectrum of otologic disorders associated with the novel SARS-CoV-2, notwithstanding the underlying congenital abnormality.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iD: Shivesh Maharaj  https://orcid.org/0000-0002-2118-2400
https://orcid.org/0000-0002-2118-2400
References
- 1.Mao L, Jin H, Wang M, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683–690. doi:10.1001/jamaneurol.2020.1127 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sriwijitalai W, Wiwanitkit V. Hearing loss and COVID-19: A note. Am J Otolaryngol. 2020;41(3):102473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Malayala SV, Raza A. A case of COVID-19-induced vestibular neuritis. Cureus. 2020;12(6):e8918. doi:10.7759/cureus.8918 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kimitsuki T, Inamitsu M, Komune S, Komiyama S. Congenital malformation of the inner ear associated with recurrent meningitis. Eur Arch Otorhinolaryngol. 1999;256(suppl 1):S11–S14. doi:10.1007/pl00014144 [DOI] [PubMed] [Google Scholar]
- 5.Johnson MD, Anil K, Lalwani MD. Sensorineural and conductive hearing loss associated with lateral semicircular canal malformation. Laryngoscope. 2000;110(10 Pt 1):1673–1679. doi:10.1097/00005537-200010000-00019 [DOI] [PubMed] [Google Scholar]
- 6.Fidan V. New type of corona virus induced acute otitis media in adult. Am J Otolaryngol. 2020;41(3):102487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Munro KJ, Uus K, Almufarrij I, Chaudhuri N, Yioe V. Persistent self-reported changes in hearing and tinnitus in post-hospitalisation COVID-19 cases. Int J Audiol. 2020;1–2. doi:10.1080/14992027.2020.1798519 [DOI] [PubMed] [Google Scholar]
- 8.Almqvist J, Granberg T, Tzortzakakis A, et al. Neurological manifestations of coronavirus infections - a systematic review. Ann Clin Transl Neurol. 2020;7(10):2057–2071. 1002/acn3.51166. doi:10.1002/acn3.51166 [DOI] [PMC free article] [PubMed] [Google Scholar]