

Abstract
The COVID‐19 pandemic has radically changed daily life and the way we interact with others. It has also brought negative psychological consequences: several studies have reported increased levels of distress symptomatology at the onset of the pandemic. However, few longitudinal studies have been carried out, and even fewer in low‐ and middle‐income countries. Therefore, the aim of this study was to analyse longitudinally the anxiety and depressive symptomatology of the Argentine general population during the first 13 months of the pandemic. The total sample included 988 adults (ages 18–77) from different regions of Argentina. Open‐access surveys were distributed via social media at five time points (March, April, May, August 2020 and April 2021). Depression and anxiety symptoms were assessed through the Beck Depression Inventory‐II and the State‐Trait Anxiety Inventory. Mixed repeated‐measures ANOVA were applied, with time as a within‐subjects factor, and socioeconomic status, gender, and age group as between‐subjects factors. Results showed a progressive increases in anxiety (F (27.78, 3417.60) = 62.88, p < 0.01, ηp2 = 0.060) and depression (F (3.42, 3373.75) = 84.78, p < 0.01, ηp2 = 0.079) symptoms in the general population throughout the pandemic (except for a slight decrease in anxiety in Wave 2). All of the between‐subjects factors showed significant effects on both types of symptoms: female gender, younger age and lower income were associated with greater depression and anxiety in all waves. A time‐age interaction effect was found (F (10.26, 3364.05) = 2.99, p < 0.01, ηp 2 = 0.009): after the third wave, depressive symptoms tended to decrease or stabilise in the young adult group, whereas there was a positive linear increase in the older groups. This study provided evidence that anxiety and depression symptoms tend to increase during crisis contexts, and that this effect is even more pronounced for certain vulnerable population groups. Mental health monitoring and support interventions should be included in government strategies to deal with the long‐term impact of the pandemic.
Keywords: distress, emotional impact, infectious disease, mental health, psychopathology
Clinical Impact Statement: The present study found that participants experienced increases in anxiety (except for a slight decrease ain wave 2) and depressive symptoms during the pandemic. Women, youth and lower income were related to greater symptoms of depression and anxiety at all five time points. The findings reported here represent a contribution that can serve as a basis for the development of mental health prevention interventions and to address the psychological consequences of the current pandemic.
1. INTRODUCTION
Coronaviruses are a family of viruses that can cause a variety of illnesses, from the common cold to pneumonia or even death. In December 2019, authorities in Wuhan, China, informed the World Health Organisation (WHO) of cases of pneumonia, the cause of which was later identified as a coronavirus previously unknown in humans (World Health Organization ‐WHO‐, 2020). The virus was named SARS‐CoV‐2, colloquially known as COVID‐19. In March 2020, the WHO Director‐General declared COVID‐19 a pandemic.
On 20 March 2020, the Argentine government imposed a strict quarantine that was meant to last for 2 weeks. At that time, there were 93 confirmed cases of COVID‐19 and three deaths from the same disease. Measures to contain the spread of the virus included social isolation, school closing, border closure and social distancing. This initial strict isolation was extended by several weeks by the Argentine authorities. From May 2020, the progressive opening of activities was allowed depending on the sanitary situation in each district. That month, there were about 200 new confirmed cases and 10 deaths per day. In August 2020, the first wave of COVID‐19 began. There were about 5400 new cases and 190 deaths per day during that period. In April 2021, Argentina faced the beginning of a second wave of COVID‐19 infections. During this period, there were approximately 26,000 new cases and 320 deaths daily. Although vaccination began in December 2020 and seemed to have a favourable effect on controlling the disease, new strains are once again hampering the situation (locally and globally).
The pandemic and the containment measures had consequences on several levels. In addition to the loss of loved ones, many people lost their jobs, working conditions changed to home‐based work, education shifted to virtual environments, and social life and leisure activities were reduced. The uncertainty and constant fear of being infected remained present at all times (del‐Valle et al., 2021). Because of this, the pandemic has emotional consequences such as anxiety, depression, post‐traumatic stress disorder, and sleep disturbances (e.g., Canet‐Juric et al., 2020; Giorgi et al., 2020; Vindegaard & Eriksen Benros, 2020). These symptoms have been found in different populations such as the general population (Canet‐Juric et al., 2020), health care workers (Giorgi et al., 2020), pregnant women (López‐Morales, del Valle, Andrés, et al., 2021; López Morales, del Valle, Canet Juric et al., 2021), and psychiatric patients (Vindegaard & Eriksen Benros, 2020).
Several studies have reported increased levels of distress and symptomatology at the onset of the pandemic (e.g., Canet‐Juric et al., 2020). Social isolation, among other aspects of the pandemic, may be the catalyst for different mental health consequences (Kim & Bhullar, 2020). For example, Crestani Calegaro et al. (2021) reported that two‐thirds of their participants felt that their mental health worsened after the onset of social restraint measures. Hyland et al. (2020) also reported that generalised anxiety and depression were common in the population during the initial phase of the COVID‐19 pandemic.
Although the pandemic has been shown to have a negative impact on the general population, certain groups are at higher risk of developing mental health problems, which may be exacerbated in the current context of the pandemic (Holmes et al., 2020). Thus, the impact of the situation is expected to be unequal for different populations. The literature shows that various socio‐demographic factors are associated with worse psychological response to the pandemic. In general, women, young adults, and people with lower income and lower education levels have been found to be more prone to distress, negative affect, and anxious and depressive symptomatology during the COVID‐19 pandemic (e.g., Canet‐Juric et al., 2020; Pieh et al., 2020; Vloo et al., 2021; Xiong et al., 2020). This effect could be even more severe in low‐ and middle‐income countries characterised by inequality, where vulnerable populations lack guaranteed access to mental health services and do not have sufficient resources to cope with the social and economic side effects of restriction measures (Kola et al., 2021). These conditions increase the likelihood of experiencing the pandemic as a chronic and extreme stressor (Gassman‐Pines & Gennetian, 2020; Smith & Pollak, 2021), increasing the risk of suffering from distress and psychopathological symptoms.
However, not many longitudinal studies have been reported. For example, in the United Kingdom, O'Connor et al. (2021) conducted a longitudinal study of well‐being in the general population and reported that mental health appeared to be impaired during the initial phase of the COVID‐19 pandemic. Other studies of this type also tend to register and increase in the psychopathological symptoms in the population during the first weeks of the pandemic (González‐Sanguino et al., 2020; Robinson et al., 2022). Nevertheless, some authors in countries such as China, England or Germany indicated that the symptoms of anxiety and depression (which initially increased) decreased after a few months (Fancourt et al., 2021; O'Connor et al., 2021; Mata et al., 2021; Wang et al., 2020).
The COVID‐19 made it necessary to investigate how the pandemic affects people's mental health. Addressing these issues through accurate studies is essential to provide tools to the public health system. Knowing and understanding the emotional impact of this pandemic is an important tool to minimise the negative consequences for affected individuals, families, and communities. Furthermore, many of the studies on this topic have been conducted in developed countries, whereas there is less evidence in low‐ and middle‐income countries such as Argentina, which also has one of the highest COVID‐19 death rates in the world. Therefore, the aim of this study is to analyse longitudinally the anxiety and depressive symptomatology of the Argentine general population during the first 13 months of the pandemic.
2. METHOD
2.1. Participants
The total sample included 988 adults from different cities in Argentina (see “Procedure and ethical considerations” for more information on response rates and dropouts). Age ranged from 18 to 77 years (mean = 41.40; SD = 13.66). Of the 988 participants, 82% identified themselves as women (n = 810) and 18% as men (n = 178). At the end of the study, 158 participants (16%) reported having been infected with COVID at some point. Of all participants, 75.6% (n = 747) had no risk factors for COVID ‐19, whereas 7.8% (n = 77) were older than 60 years, 5.2% (n = 51) had respiratory disease, 3% (n = 30) had cardiovascular disease, 1. 1% (n = 11) were immunosuppressed, 0.4% (n = 4) had diabetes, 0.2% (n = 2) were obese, 0.2% (n = 2) reported being pregnant, and 6.5% (n = 64) reported a combination of some of these factors. Regarding educational level, 0.6% (n = 6) reported incomplete secondary education, 4.7% (n = 46) completed secondary education, 28.2% (n = 279) reported incomplete or ongoing university or tertiary studies, 35.1% (n = 347) completed university education, and 31.4% (n = 310) reported complete or incomplete postgraduate education. The socioeconomic status was distributed as follows: 8.2% (n = 81) low and lower middle, 51.4% (n = 508) middle and upper middle, and 40.4% (n = 399) high. The distribution of sociodemographic factors can be found in Table 1
TABLE 1.
Distribution of sociodemographic factors throughout the five study waves
| Variable | Categories | Total sample (n = 988) |
|---|---|---|
| Gender | Female | n = 810 (82%) |
| Male | n = 178 (18%) | |
| Other gender | n = 0 (0%) | |
| Age | M (DE) | 41.4 (13.66) |
| 18–25 | n = 111 (11.2%) | |
| 26–40 | n = 405 (41%) | |
| 41–60 | n = 358 (36.2%) | |
| +60 | n = 114 (11.5%) | |
| Educational level | Incomplete primary education | n = 0 (0%) |
| Complete primary education | n = 0 (0%) | |
| Incomplete secondary education | n = 6 (0.6%) | |
| Complete secondary education | n = 46 (4.7%) | |
| Incomplete or ongoing university or tertiary studies | n = 279 (28.2%) | |
| Completed university education | n = 347 (35.1%) | |
| Complete or incomplete postgraduate education | n = 310 (31.4%) | |
| Educational level of breadwinner | Incomplete primary education | n = 4 (0.4%) |
| Complete primary education | n = 10 (1.0%) | |
| Incomplete secondary education | n = 26 (2.6%) | |
| Complete secondary education | n = 72 (7.3%) | |
| Incomplete or ongoing university or tertiary studies | n = 204 (20.6%) | |
| Completed university education | n = 364 (36.8%) | |
| Complete or incomplete postgraduate education | n = 308 (31.2%) | |
| Socio‐economic status | Low and lower middle | n = 81 (8.2%) |
| Middle and upper middle | n = 308 (51.4%) | |
| High | n = 599 (40.4%) |
2.2. Measures
Beck Depression Inventory‐II: the Argentine adaptation (Brenlla & Rodríguez, 2006) of the Beck Depression Inventory‐II (BDI‐II, Beck et al., 1996) was used to assess depressive symptoms. The instrument is composed of 21 self‐administered items that assess the presence and intensity of depressive symptoms (e.g., sadness, crying, appetite changes) experienced by the individual in the past 15 days. Each item is answered on a scale of 0–3, describing the increasing severity of that symptom. The BDI‐II has demonstrated adequate reliability and validity in several studies (e.g., Beltrán et al., 2012; Sanz & Vázquez, 1998). The item that referred to suicidal ideation (item 9) was removed for this study due to ethical concerns about mentioning suicide in an uncontrolled setting such as an online survey. The minimum scale score is 0 and the maximum scale score (after removal of item 9) is 60. In this study, the Cronbach's α showed high internal consistency (Time 1: α = 0.93; Time 2: α = 0.94; Time 3: α = 0.95; Time 4: α = 0.95; Time 5: α = 0.95).
State‐Trait Anxiety Inventory: The Argentine adaptation (Leibovich de Figueroa, 1991) of the State‐Trait Anxiety Inventory (STAI; Spielberger et al., 1970) was used to assess anxiety symptoms. The State trait anxiety inventory is a 40‐item self‐report instrument that separately measures state anxiety (transient condition) and trait anxiety (stable condition). In the present study, only the state anxiety dimension was used. This subscale consists of 20 items that can be answered in a range from 0 to 3. Each participant's total score was weighted (divided) by the number of items, so that the minimum scale score was 0 and the maximum score was 3. Previous studies on this scale have consistently demonstrated its validity and reliability (e.g., del‐Valle et al., 2021; Guillén‐Riquelme & Buela‐Casal, 2011). In the present study, the state anxiety subscale exhibited high reliability (Time 1: α = 0.90; Time 2: α = 0.90; Time 3: α = 0.92; Time 4: α = 0.92; Time 5: α = 0.92).
Sociodemographic characteristics: Closed‐ended questions were asked about gender, age, COVID‐19 infection, risk factor for COVID‐19, educational level, and occupation and educational level of the main breadwinner. Socioeconomic level was estimated based on the educational level and occupation of the main breadwinner in the family. Educational level was classified according to the 7‐point scale of Pascual et al. (1993). Occupational level was classified according to the scale of occupational groups in Argentina established by Sautú's (1989) (higher scores correspond to more prestigious occupations). Hollingshead's (2011) index was used to classify these scores into general socioeconomic categories. In the present study, some categories were unified to reduce differences in the size of the groups.
2.3. Procedure and ethical considerations
This study was approved by the Bioethics Committee of the National University of Mar del Plata, Argentina. All procedures recommended by the Declaration of Helsinki and the American Psychological Association (2010) were followed. Participation in the study was voluntary and the signing of a digital informed consent form was required. The participants were offered opportunity to contact different sources of psychological help if needed.
To determine the minimum sample size required, a priori estimates were made using G*Power. At least 121 participants were needed to answer the hypotheses concerning within factors (ANOVA, 5 repeated measures, within factors). For answering the hypotheses on the between factors (ANOVA, max. Four groups, 5 repeated measures), at least 660 participants were required. Finally, for answering the interaction hypotheses (ANOVA within‐between interaction, 4 groups, 5 measures), at least 180 participants were needed.
Five open‐access surveys were launched via Google Forms and disseminated via social media at different time points during the pandemic. Email address provided by participants were used to match them across the surveys. The first survey was conducted between March 22 and 26 (shortly after isolation measures began in Argentina). The second survey was conducted approximately 2 weeks after the first one (i.e., between April 4 and April 9). The aim of this second survey was to assess the initial response to the pandemic. The strict initial quarantine imposed in Argentina on 20 March 2020 was relaxed in May (the progressive easing of the COVID‐19 containment measures depended on the sanitary situation in each district). For this reason, the third survey was conducted between May 7 and 13, 2020 (approximately 50 days after the start of social isolation measures in Argentina) to assess the population response to the gradual opening of activities. In August 2020, the first wave of COVID‐19 began, so the fourth survey was released and conducted between August 8 and 13, 2020 (approximately 3 months after the first survey). The fifth survey was conducted between April 17 and 23, 2021 (more than a year after the pandemic outbreak). At that time, the country was entering the second peak of the contagion curve and the implementation of new containment and isolation measures was imminent.
The first survey was answered by 16,503 people. The second survey was answered by 7323 people (44.4% of the original sample). The third survey was mailed to the original 16,503 participants. Of the 7323 participants who responded to the first and second surveys, 4114 also responded to the third survey (24.9% of the original sample). The fourth survey was also mailed to the original 16,503 participants. Of the 4114 who responded to the first, second, and third surveys, 1931 also responded to the fourth survey (11.7% of the original sample). Finally, the fifth survey was also mailed to the original 16,503 participants. Of the 1931 participants who answered the first, second, third, and fourth surveys, 988 also answered the fifth survey (6% of the original sample). Although the raw response rates were higher (first survey: 16,503; second survey: 7323; third survey: 5692; fourth survey: 3573; fifth survey: 3526), only the 988 participants who responded to the surveys at all five time points were retained in the final sample (i.e., those who did not respond to one or more of the surveys were excluded).
2.4. Data analysis
Mixed repeated measures ANOVA statistics were used to test the effect of the pandemic over time (intra‐subject factor). Age, gender and socioeconomic status were included as inter‐subject factors. Depressive and anxiety symptoms (in Wave 1, 2, 3, 4, and 5) were considered as the dependent variables. In cases where the W Mauchnik test resulted in a rejection of the sphericity test, the Greenhouse–Geisser correction was used. The Bonferroni statistic was used to adjust for multiple comparisons.
3. RESULTS
3.1. Anxiety in total sample
Results of the mixed repeated measures ANOVA demonstrated a significant effect of time (F (27.78, 3417.60) = 62.88, p < 0.01, η p 2 = 0.060). Initially, a significant decrease in anxiety was identified in Wave 2 compared to Wave 1 (p < 0.05). Then, a significant increase was found in Wave 3 (p < 0.01), homogeneous indicators in Wave 3 and 4 (p > 0.05) and again a significant increase in Wave 5 (p < 0.01) (Figure 1a).
FIGURE 1.
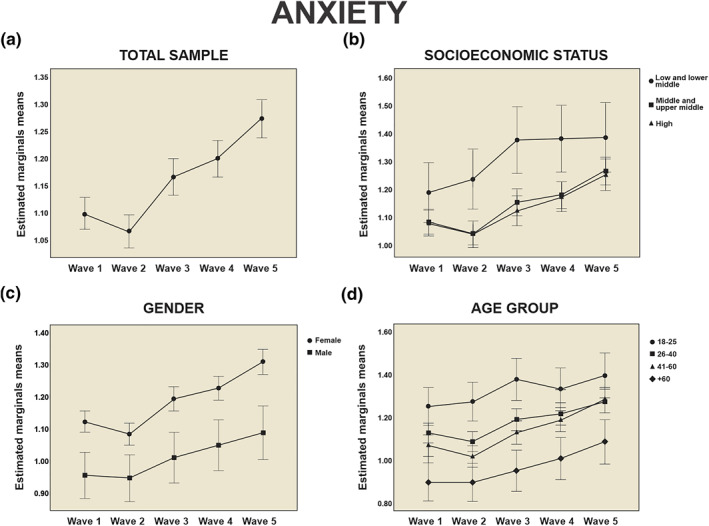
Comparison of the adjusted mean of the anxiety symptoms according to the different socioeconomic and demographic variables, during the five waves of the study. Figure 1 compares the adjusted means for anxiety (1A‐1D) in total sample and according to the different socioeconomic (socioeconomic status) and demographic (gender and age group) variables during the five phases of the study (Wave 1–5). Error bars +/− 2SD
3.2. Anxiety and socioeconomic status
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.46, 3408.07) = 33.81, p < 0.01, η p 2 = 0.033). No significant effect of time‐socioeconomic status interaction was found (F (6.92, 3408.07) = 1.13, p > 0.05, η p 2 = 0.002) (Figure 1b). A significant effect of the socioeconomic status (between‐subjects) was demonstrated (F (2, 985) = 5.88, p < 0.01, η p 2 = 0.012). According to the post‐hoc tests for paired comparisons with Bonferroni correction, there were statistically significant differences in anxiety between the groups at Wave 2, 3 and 4. In all cases, the low and lower middle group presented significantly higher mean scores compared to the middle and upper middle group and the high group (p < 0.01).
3.3. Anxiety and gender
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.46, 3415.54) = 29.50, p < 0.01, η p 2 = 0.029). No significant effect of time‐gender interaction was found (F (1.22, 3415.54) = 1.22, p > 0.05, η p 2 = 0.001) (Figure 1c). A significant effect of the gender factor (between‐subjects) was demonstrated (F (1, 986) = 24.57, p < 0.01, η p 2 = 0.024). According to the post‐hoc tests for paired comparisons with Bonferroni correction, there were statistically significant differences in anxiety between groups at Wave 1–5 (p < 0.01). For all comparisons, women showed higher indicators of anxiety compared to men.
3.4. Anxiety and age group
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.47, 3410.83) = 38.91, p < 0.01, η p 2 = 0.038). No significant effect of time‐age interaction was found (F (10.40, 3158.43) = 1.36, p > 0.05, η p 2 = 0.004) (Figure 1d). A significant effect of the age group factor (between‐subjects) was demonstrated (F (3, 984) = 13.89, p < 0.01, η p 2 = 0.041). According to the post‐hoc tests for paired comparisons with Bonferroni correction, multiple significant differences were found between age groups. In Wave 1, the +60‐group showed significantly lower mean scores compared to all groups (p < 0.01). In turn, 18–25 group presented higher mean scores compared to the 41–60 group (p < 0.01). In Wave 2, the 18–25 group showed significantly higher mean scores compared to the other groups (p < 0.01). In turn, significant differences were found between the 26–40 group and the +60 group, in favour of the former (p < 0.01). In Wave 3, the 18–25 group presented significantly higher anxiety indicators compared to the other groups (p < 0.01), while the +60 group presented the lowest mean scores compared to the other groups (p < 0.01). Finally, in both Wave 4 and Wave 5, the +60 group showed the lowest mean scores among the study groups (p < 0.01), while the other groups presented homogeneous results (p > 0.05).
3.5. Depression in total sample
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.42, 3373.75) = 84.78, p < 0.01, η p 2 = 0.079) (Figure 2a). According to the post‐hoc tests for paired comparisons with Bonferroni correction, a significant increase in depressive symptoms was identified in Wave 2 and Wave 3 (p < 0.01). The registered means remained homogeneous through Wave 4 (p > 0.05), and return to a significant increase in Wave 5 (p < 0.01).
FIGURE 2.
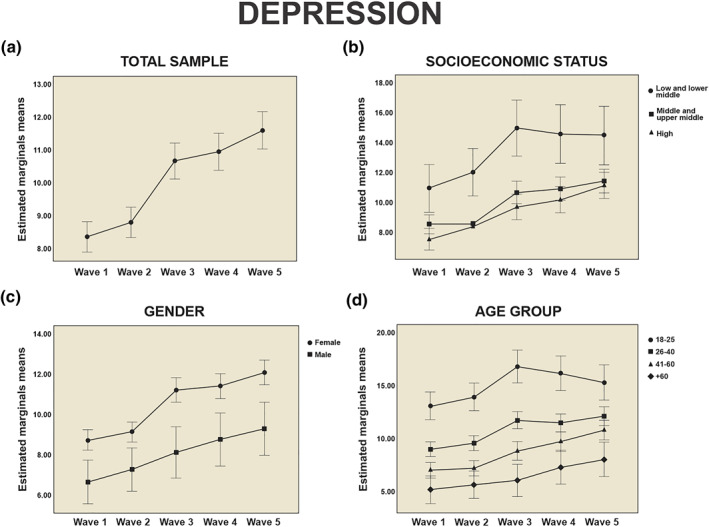
Comparison of the adjusted mean of the depressive symptoms according to the different socioeconomic and demographic variables, during the five waves of the study. Figure 2 compares the adjusted means for depression (2A‐2D) in total sample and according to the different socioeconomic (socioeconomic status) and demographic (gender and age group) variables during the five phases of the study (Wave 1–5). Error bars +/− 2SD
3.6. Depression and socioeconomic status
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.41, 3362.39) = 52.10, p < 0.01, η p 2 = 0.050). No significant effect of time‐socioeconomic status interaction was found (F (6.83, 3362.39) = 1.54, p > 0.05, η p 2 = 0.003) (Figure 2b). A significant effect of the socioeconomic status (between‐subjects) was demonstrated (F (2, 985) = 10.85, p < 0.01, η p 2 = 0.022). According to the post‐hoc tests for paired comparisons with Bonferroni correction, there were statistically significant differences in depression between groups in all waves. In all cases, the low and lower middle group presented significantly higher means than to the other groups (p < 0.01) at all temporal cuts. On the contrary, the middle and upper middle group and the high group presented homogeneous scores in all Waves (p > 0.05).
3.7. Depression and gender
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.42, 3369.56) = 41.01, p < 0.01, η p 2 = 0.040). No significant effect of time‐gender interaction was found (F (3.42, 3369.56) = 1.63, p > 0.05, η p 2 = 0.002) (Figure 2c). A significant effect of the gender factor (between‐subjects) was demonstrated (F (1, 986) = 18.19, p < 0.01, η p 2 = 0.018). According to the post‐hoc tests for paired comparisons with Bonferroni correction, there were statistically significant differences in depression between groups at Wave 1–5 (p < 0.01). For all comparisons, women showed higher indicators of depression compared to men.
3.8. Depression and age group
Results of mixed repeated measures ANOVA demonstrated a significant effect of time (F (3.42, 3364.05) = 53.55, p < 0.01, η p 2 = 0.052). A significant effect of time‐age interaction was also found (F (10.26, 3364.05) = 2.99, p < 0.01, η p 2 = 0.009) (Figure 2d). A significant effect of the age group factor (between‐subjects) was demonstrated (F (3, 984) = 36.89, p < 0.01, η p 2 = 0.101). According to the post‐hoc tests for paired comparisons with Bonferroni correction, several significant differences were found between age groups. In all cases, the 18–25‐year‐old group showed significantly higher mean scores than the rest of the groups in all Waves (p < 0.01). Subsequently, the 26–40 group showed significantly higher mean scores with respect to 41–60 group (except in Wave 5 where the means of both groups were homogeneous) and the +60 years group (p < 0.01). On the other hand, the 41–60 group and the +60 group showed homogeneous scores in Waves 1, 2 and 4, and only differed significantly in Wave 3 (p < 0.01) and Wave 5 (p < 0.05). The +60 group was the one that presented the significantly lower mean scores in depressive symptoms.
4. DISCUSSION
The COVID‐19 pandemic has brought with it a number of negative consequences for individuals that go beyond the medical problem of the disease itself. The pandemic context includes changes in work, family, social and daily life and has led to a general mental health impairment in various populations (Salari et al., 2020; Wang, et al., 2021). Considering the problematic nature of this situation and the importance of accurate studies in this area, the present study aimed to analyse longitudinally the anxiety and depressive symptomatology of the general Argentine population during the first 13 months of the pandemic.
Participants were observed to have progressive increases in both anxiety (with the exception of a slight decrease in anxiety in wave 2) and depressive symptoms throughout the pandemic. The observed increase in psychopathological symptomatology in the population during the first four to 6 weeks of the pandemic is consistent with what has been reported in previous longitudinal studies in other countries (González‐Sanguino et al., 2020; Robinson et al., 2022). However, whereas in other countries (e.g., China, England, Germany) there was a decrease in anxiety and depression symptoms after a few months (Fancourt et al., 2021; O'Connor et al., 2021; Mata et al., 2021; Wang et al., 2020), in Argentina symptoms continued to increase even more than a year after the outbreak of the pandemic. This finding is alarming because it shows a marked difference from other higher‐income countries where most longitudinal studies have been conducted.
Women reported more symptoms of depression and anxiety at all five time points. Although women generally report more psychopathology than men (Lim et al., 2018), this deserves particular attention in a vulnerability context such as the current one, which highlights gender inequalities (Robinson et al., 2021). Several studies have already reported the greater tendency of women to develop psychopathology during the pandemic (Moghanibashi‐Mansourieh, 2020; Zhou et al., 2020). Similar attention should be paid to the results on socioeconomic status, as the highest levels of anxiety and depressive symptoms were found among those most at risk (lower income). Other empirical studies have already described associations between occupation, income, and economic conditions and vulnerability to mental health problems during the pandemic (e.g., Hossain et al., 2020; Li et al., 2020; Witteveen & Velthorst, 2020). This means that the most vulnerable populations in society will suffer disproportionately from this pandemic (Robinson et al., 2021).
Regarding participant age, higher baseline scores were observed in young adults (18–25 years) for both anxiety and depression. However, after the third wave, anxiety and depressive symptoms tended to decrease or stabilise in the young adult group. In contrast, older populations showed a positive linear trend for anxiety symptoms (from the second wave) and a more modest positive trend for depression. Even though age increases the risk of COVID‐19 infection and mortality, young adults showed higher vulnerability to mental health deterioration (Huang & Zhao, 2020; Liang et al., 2020; Moghanibashi‐Mansourieh, 2020; Wang et al., 2020). These findings are partially contradictory to what several authors suggest (e.g., Holmes et al., 2020; Kobayashi et al., 2021): that older adults are the most affected population during confinement. In contrast, the findings of this work are consistent with authors such as Horesh et al. (2020), who found higher levels of distress in young adults than in other populations. McKinlay et al. (2021) suggested that young adults experience the greatest stress due to uncertainty (in issues such as work, family, studies, etc.; Ochnik et al., 2021; Schubert et al., 2017), while older adults have lower social mobility and more stable living conditions, so they are less affected by changes in the environment. However, the sustained increase in anxiety and depressive symptomatology among older adults could indicate the depletion of coping strategies to deal with the pandemic (such as social isolation). In contrast, the tendency for symptomatology to stabilise or even decrease in younger adults could reflect adaptation to new living conditions after a year of the pandemic.
The findings reported here should be interpreted in light of some limitations. First, because the surveys are not evenly distributed over time, the results may be somewhat biased. Second, we worked with a non‐probabilistic sample, so we cannot generalise the results. There was also a high dropout rate, which is a third limitation. In addition, the sample presented a large proportion of individuals with high levels of education and socioeconomic status, which is not characteristic of the distribution of these variables in the Argentine population. Further studies are needed to reach other sectors and make more accurate estimates. The proportion of women was also high. Although it is common for women to participate to a greater extent in this type of study (e.g., Alomo et al., 2020; Torrente et al., 2021), this represents a bias and a limitation to be considered. Another limitation worth mentioning is that the present study only worked with symptoms (indicators) of anxiety and depression and not with clinical conditions. It would be interesting to conduct a study aimed at analysing the presence of anxiety and depression disorders based on cut‐off scores and minimal clinically important differences. Finally, we used only quantitative measures, which exclude many qualitative aspects of people's mental health. Future studies should use other methods to complement the results founded.
Nevertheless, this study is a contribution to mental health research in crisis contexts such as the current one and provides empirical evidence of a problem that remains present. A longitudinal study has the advantage of providing a more detailed understanding of the variability of anxiety and depressive symptomatology over time. Moreover, it is also one of the few longitudinal studies that have been conducted in low‐ and middle‐income countries. In summary, the study provides information on population mental health over time. There is a trend towards a moderate increase in anxiety and depression over time. These results suggest an emotional impact of the pandemic on the general population, and show that symptoms of anxiety and depression tend to increase in crisis contexts. Very slightly, the trend in indicators of psychopathology tends to stabilise and even slightly decrease in some subgroups. Moreover, the situation does not seem to have affected all people in the same way: women, young adults, and people of lower socioeconomic status were more vulnerable to the pandemic. This vulnerability is important because policymakers and service providers need reliable information to make appropriate knowledge‐based decisions (Pierce et al., 2020). Thus, it is hoped that the results will serve as a basis for considering that the COVID‐19 pandemic also has mental health implications that deserve attention.
FUNDING INFORMATION
The study was funded by the Ministry of Science, Technology and Innovation of the Argentine Nation. “Articulation Programme and Federal Strengthening of Capacities in Science and Technology COVID‐19”.
CONFLICT OF INTEREST
None.
del‐Valle, M. V. , López‐Morales, H. , Gelpi‐Trudo, R. , Poó, F. M. , García, M. J. , Yerro‐Avincetto, M. , Andrés, M. L. , Canet‐Juric, L. , & Urquijo, S. (2022). More than a year of pandemic: Longitudinal assessment of anxiety and depressive symptoms in the argentine general population during the COVID‐19 outbreak. Stress and Health, 1–10. 10.1002/smi.3163
L. Canet Juric and S. Urquijo are contributed equally.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available on request from the corresponding authors.
REFERENCES
- Alomo, M. , Gagliardi, G. , Peloche, S. , Somers, E. , Alzina, P. , & Prokopez, C. R. (2020). Efectos psicológicos de la pandemia COVID‐19 en la población general de Argentina [Psychological effects of the COVID‐19 pandemic in the general population of Argentina]. Revista de la Facultad de Ciencias Médicas de Córdoba, 77(3), 176–181. 10.31053/1853.0605.v77.n3.28561 [DOI] [PubMed] [Google Scholar]
- American Psychological Association . (2010). Ethical principles of psychologists and code of conduct. Retrieved from www.apa.org/ethics/code/principles.pdf [Google Scholar]
- Beck, A. T. , Steer, R. A. , & Brown, G. K. (1996). Beck depression inventory‐II. The Psychological Corporation. [Google Scholar]
- Beltrán, M. C. , Freyre, M. Á. , & Hernández‐Guzmán, L. (2012). El Inventario de Depresión de Beck: Su validez en población adolescente [The Beck Depression Inventory: Its validity in adolescent population]. Terapia Psicologica, 30(1), 5–13. 10.4067/S0718-48082012000100001 [DOI] [Google Scholar]
- Brenlla, M. E. , & Rodríguez, C. M. (2006). Adaptación Argentina del Inventario de Depresión de Beck (BDI‐II) [Argentine adaptation of the Beck Depression Inventory (BDI‐II)]. In Beck A. T., Steer R. A., & Brown G. K. (Eds.), BDI‐II. Inventario de Depresión de Beck. Segunda edición. Manual [BDI‐II. Beck depression inventory (2nd ed.). Paidós. [Google Scholar]
- Canet‐Juric, L. , Andrés, M. L. , del Valle, M. , López‐Morales, H. , Poó, F. , Galli, J. I. , Yerro, M. , & Urquijo, S. (2020). A longitudinal study on the emotional impact cause by the COVID‐19 pandemic quarantine on general population. Frontiers in Psychology, 11, 565688. 10.3389/FPSYG.2020.565688 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crestani Calegaro, V. , Ramos‐Lima, L. F. , Scopel Hoffmann, M. , Zoratto, G. , Kerber, N. , Coloniese Dala Costa, F. , Picinin, V. D. , Köchler, J. , Rodrigues, L. , Maciel, L. , Braun, L. E. , Leite Girardi, F. , Olerich Cecatto, G. , Pompeo Weber, L. , Fragoso Rodrigues, B. , Naimaier Bertolazi, A. , Motta de Oliveira, J. , Lorenzi Negretto, B. , & Feijó de Mello, A. (2021). Closed doors: Predictors of stress, anxiety, depression, and PTSD during the onset of COVID‐19 pandemic in Brazil. medRxiv. 10.1101/2021.08.18.21262061 [DOI] [PMC free article] [PubMed] [Google Scholar]
- del‐Valle, M. V. , Andrés, M. L. , Urquijo, S. , Yerro Avincetto, M. , López Morales, H. , & Canet Juric, L. (2020). Intolerance of uncertainty over COVID‐19 pandemic and its effect on anxiety and depressive symptoms. Revista Interamericana de Psicología/Interamerican Journal of Psychology, 54(2), e1335. 10.30849/ripijp.v54i2.1335 [DOI] [Google Scholar]
- del‐Valle, M. V. , Andrés, M. L. , Urquijo, S. , Zamora, E. , Mehta, A. , & Gross, J. J. (2021). Argentinean adaptation and psychometric properties of the emotion regulation questionnaire –ERQ–. Psychological Reports, 10.1177/00332941211021343 [DOI] [PubMed] [Google Scholar]
- Fancourt, D. , Steptoe, A. , & Bu, F. (2021). Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID‐19 in England: A longitudinal observational study. The Lancet Psychiatry, 8(2), 141–149. 10.1016/S2215-0366(20)30482-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gassman‐Pines, A. , & Gennetian, L. A. (2020). COVID‐19 job and income loss jeopardize child well‐being: Income support policies can help. SCRD Child Evidence Brief, 9. https://www.srcd.org/research/covid‐19‐job‐and‐income‐loss‐jeopardize‐child‐well‐being‐income‐support‐policies‐can‐help [Google Scholar]
- Giorgi, G. , Lecca, L. I. , Alessio, F. , Finstad, G. L. , Bondanini, G. , Lulli, L. G. , Arcangeli, G. , & Mucci, N. (2020). COVID‐19‐related mental health effects in the workplace: A narrative review. International Journal of Environmental Research and Public Health, 17(21), 7857. 10.3390/ijerph17217857 [DOI] [PMC free article] [PubMed] [Google Scholar]
- González‐Sanguino, C. , Ausín, B. , Castellanos, M. Á. , Saiz, J. , López‐Gómez, A. , Ugidos, C. , & Muñoz, M. (2020). Mental health consequences of the coronavirus 2020 pandemic (COVID‐19) in Spain. A longitudinal study. Frontiers in Psychiatry, 11, 1256. 10.3389/fpsyt.2020.565474 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guillén‐Riquelme, A. , & Buela‐Casal, G. (2011). Actualización psicométrica y funcionamiento diferencial de los ítems en el State Trait Anxiety Inventory (STAI) [Psychometric update and differential item functioning in the State Trait Anxiety Inventory (STAI)]. Psicothema, 23(3), 510–515. http://www.psicothema.com/pdf/3916.pdf [PubMed] [Google Scholar]
- Hollingshead, A. B. (2011). Four factor index of social status. Yale Journal of Sociology, 8, 21–52. https://sociology.yale.edu/sites/default/files/files/yjs_fall_2011.pdf#page=21 [Google Scholar]
- Holmes, E. A. , O’Connor, R. C. , Perry, V. H. , Tracey, I. , Wessely, S. , Arseneault, L. , Ballard, C. , Christensen, H. , Cohen Silver, R. , Everall, I. , Ford, T. , John, A. , Kabir, T. , King, K. , Madan, I. , Michie, S. , Przybylski, A. K. , Shafran, R. , Sweeney, A. , & Bullmore, E. (2020). Multidisciplinary research priorities for the COVID‐19 pandemic: A call for action for mental health science. The Lancet Psychiatry, 7(6), 547–560. 10.1016/S2215-0366(20)30168-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horesh, D. , Kapel Lev‐Ari, R. , & Hasson‐Ohayon, I. (2020). Risk factors for psychological distress during the COVID‐19 pandemic in Israel: Loneliness, age, gender, and health status play an important role. British Journal of Health Psychology, 25(4), 925–933. 10.1111/bjhp.12455 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hossain, M. M. , Tasnim, S. , Sultana, A. , Faizah, F. , Mazumder, H. , Zou, L. , McKyer, E. L. J. , Ahmed, H. U. , & Ma, P. (2020). Epidemiology of mental health problems in COVID‐19: A review. F1000 Research, 9, 636. 10.12688/f1000research.24457.1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huang, Y. , & Zhao, N. (2020). Generalized anxiety disorder, depressive symptoms and sleep quality during COVID‐19 outbreak in China: A web‐based cross‐sectional survey. Psychiatry Research, 288. 112954. 10.1016/j.psychres.2020.112954 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hyland, P. , Shevlin, M. , McBride, O. , Murphy, J. , Karatzias, T. , Bentall, R. P. , Martinez, A. , & Vallières, F. (2020). Anxiety and depression in the Republic of Ireland during the COVID‐19 pandemic. Acta Psychiatrica Scandinavica, 142(3), 249–256. 10.1111/acps.13219 [DOI] [PubMed] [Google Scholar]
- Kim, U. , Bhullar, N. , & Jackson, D. (2020). Life in the pandemic: Social isolation and mental health. Journal of Clinical Nursing, 29(15–16), 2756–2757. 10.1111/jocn.15290 [DOI] [PubMed] [Google Scholar]
- Kobayashi, L. C. , O’Shea, B. Q. , Kler, J. S. , Nishimura, R. , Palavicino‐Maggio, C. B. , Eastman, M. R. , Rikia Vinson, Y. , & Finlay, J. M. (2021). Cohort profile: The COVID‐19 Coping Study, a longitudinal mixed‐methods study of middle‐aged and older adults’ mental health and well‐being during the COVID‐19 pandemic in the USA. BMJ Open, 11(2), e044965. 10.1136/bmjopen-2020-044965 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kola, L. , Kohrt, B. A. , Hanlon, C. , Naslund, J. A. , Sikander, S. , Balaji, M. , Benjet, C. , Cheung, E. Y. L. , Eaton, J. , Gonsalves, P. , Hailemariam, M. , Luitel, N. P. , Machado, D. B. , Misganaw, E. , Omigbodun, O. , Roberts, T. , Salisbury, T. T. , Shidhaye, R. , Sunkel, C. , & Patel, V. (2021). COVID‐19 mental health impact and responses in low‐income and middle‐income countries: Reimagining global mental health. The Lancet Psychiatry, 8(6), 535–550. 10.1016/S2215-0366(21)00025-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leibovich de Figueroa, N. B. (1991). Ansiedad: Algunas concepciones teóricas y su evaluación [Anxiety: Some theoretical conceptions and its evaluation.]. In Casullo M. M., Leibovich de Figueroa N. B., & Aszkenazi M. (Eds.), Teoría y técnicas de evaluación psicológica [Theory and techniques of psychological assessment] (pp. 123–155). [Google Scholar]
- Li, G. , Miao, J. , Wang, H. , Xu, S. , Sun, W. , Fan, Y. , Zhang, C. , Zhu, S. , Zhu, Z. , & Wang, W. (2020). Psychological impact on women health workers involved in COVID‐19 outbreak in Wuhan: A cross‐sectional study. Journal of Neurology, Neurosurgery & Psychiatry, 91(8), 895–897. 10.1136/jnnp-2020-323134 [DOI] [PubMed] [Google Scholar]
- Liang, L. , Ren, H. , Cao, R. , Hu, Y. , Qin, Z. , Li, C. , & Mei, S. (2020). The effect of COVID‐19 on youth mental health. Psychiatric Quarterly, 91(3), 841–852. 10.1007/s11126-020-09744-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lim, G. Y. , Tam, W. W. , Lu, Y. , Ho, C. S. , Zhang, M. W. , & Ho, R. C. (2018). Prevalence of depression in the community from 30 countries between 1994 and 2014. Scientific Reports, 8(1), 2861. 10.1038/s41598-018-21243-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- López Morales, H. , del Valle, M. , Canet Juric, L. , Andrés, M. L. , Galli, J. I. , Poó, F. , & Urquijo, S. (2021). Mental health of pregnant women during the COVID‐19 pandemic: A longitudinal study. Psychiatry Research, 295, 113567. 10.1016/j.psychres.2020.113567 [DOI] [PMC free article] [PubMed] [Google Scholar]
- López‐Morales, H. , del Valle, M. V. , Andrés, M. L. , Gelpi Trudo, R. , Canet‐Juric, L. , & Urquijo, S. (2021). Longitudinal study on prenatal depression and anxiety during the COVID‐19 pandemic. Archives of Women's Mental Health, 24, 1027–1036. 10.1007/s00737-021-01152-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mata, J. , Wenz, A. , Rettig, T. , Reifenscheid, M. , Möhring, K. , Krieger, U. , Friedel, S. , Fikel, M. , Cornesse, C. , Blorn, A. , & Naumann, E. (2021). Health behaviors and mental health during the COVID‐19 pandemic: A longitudinal population‐based survey in Germany. Social Science & Medicine, 287, 114333. 10.1016/j.socscimed.2021.114333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKinlay, A. R. , Fancourt, D. , & Burton, A. (2021). A qualitative study about the mental health and wellbeing of older adults in the UK during the COVID‐19 pandemic. BMC Geriatrics, 21, 439. 10.1186/s12877-021-02367-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moghanibashi‐Mansourieh, A. (2020). Assessing the anxiety level of Iranian general population during COVID‐19 outbreak. Asian Journal of Psychiatry, 51, 102076. 10.1016/j.ajp.2020.102076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ochnik, D. , Rogowska, A. M. , Kuśnierz, C. , Jakubiak, M. , Schütz, A. , Held, M. J. , Arzenšek, A. , Benatov, J. , Berger, R. , Korchagina, E. V. , Pavlova, I. , Blažková, I. , Konečná, Z. , Aslan, I. , Çınar, O. , Cuero‐Acosta, Y. A. , & Wierzbik‐Strońska, M. (2021). A comparison of depression and anxiety among University students in nine countries during the COVID‐19 pandemic. Journal of Clinical Medicine, 10(13), 2882. 10.3390/jcm10132882 [DOI] [PMC free article] [PubMed] [Google Scholar]
- O'Connor, R. , Wetherall, K. , Cleare, S. , McClelland, H. , Melson, A. , Niedzwiedz, C. , Platt, S. , Scowcroft, E. , Watson, B. , Zortea, T. , Ferguson, E. , & Robb, K. (2021). Mental health and well‐being during the COVID‐19 pandemic: Longitudinal analyses of adults in the UK COVID‐19 Mental Health & Wellbeing study. The British Journal of Psychiatry, 218(6), 326–333. 10.1192/bjp.2020.212 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pascual, L. , Galperín, C. Z. , & Bornstein, M. H. (1993). La medición del nivel socioeconómico y la psicología evolutiva: El caso argentino [Measuring socioeconomic status and developmental psychology: The Argentinean case]. Revista Interamericana de Psicologia/Interamerican Journal of Psychology, 27(1), 59–74. https://journal.sipsych.org/index.php/IJP/article/view/786/680 [Google Scholar]
- Pieh, C. , Budimir, S. , & Probst, T. (2020). The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID‐19) lockdown in Austria. Journal of Psychosomatic Research, 136, 110186. 10.1016/j.jpsychores.2020.110186 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pierce, M. , Hope, H. , Ford, T. , Hatch, S. , Hotopf, M. , John, A. , Kontopantelis, E. , Webb, R. , Wessely, S. , McManus, S. , & Abel, K. M. (2020). Mental health before and during the COVID‐19 pandemic: A longitudinal probability sample survey of the UK population. The Lancet Psychiatry, 7(10), 883–892. 10.1016/S2215-0366(20)30308-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson, E. , Sutin, A. R. , Daly, M. , & Jones, A. (2022). A systematic review and meta‐analysis of longitudinal cohort studies comparing mental health before versus during the COVID‐19 pandemic in 2020. Journal of Affective Disorders, 296, 567–576. 10.1016/j.jad.2021.09.098 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson, L. , Schulz, J. , Ragnedda, M. , Pait, H. , Kwon, K. H. , & Khilnani, A. (2021). An unequal pandemic: Vulnerability and COVID‐19. American Behavioral Scientist, 65(12), 1603–1067. 10.1177/00027642211003141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salari, N. , Hosseinian‐Far, A. , Jalali, R. , Vaisi‐Raygani, A. , Rasoulpoor, S. , Mohammadi, M. , Rasoulpoor, S. , & Khaledi‐Paveh, B. (2020). Prevalence of stress, anxiety, depression among the general population during the COVID‐19 pandemic: A systematic review and meta‐analysis. Globalization and Health, 16(1), 1–11. 10.1186/s12992-020-00589-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sanz, J. , & Vázquez, C. (1998). Fiabilidad, validez y datos normativos del Inventario para la Depresión de Beck [Reliability, validity and normative data of the Beck Depression Inventory]. Psicothema, 10(2), 303–318. https://www.redalyc.org/pdf/727/72710207.pdf [Google Scholar]
- Sautú, R. (1989). Teoría y técnica en la medición del status ocupacional: Escalas objetivas de Prestigio [theory and technique in the measurement of occupational status: Objective prestige scales]. Universidad de Buenos Aires. [Google Scholar]
- Schubert, K. O. , Clark, S. R. , Van, L. K. , Collinson, J. L. , & Baune, B. T. (2017). Depressive symptom trajectories in late adolescence and early adulthood: A systematic review. Australian and New Zealand Journal of Psychiatry, 51(5), 477–499. 10.1177/0004867417700274 [DOI] [PubMed] [Google Scholar]
- Smith, K. E. , & Pollak, S. D. (2021). Early life stress and neural development: Implications for understanding the developmental effects of COVID‐19. Cognitive, Affective, & Behavioral Neuroscience. 10.3758/S13415-021-00901-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spielberger, C. D. , Gorsuch, R. L. , & Lushene, R. E. (1970). Manual for the state‐trait anxiety inventory. Consulting Psychologists Press. [Google Scholar]
- Torrente, F. , Yoris, A. , Low, D. M. , Lopez, P. , Bekinschtein, P. , Manes, F. , & Cetkovich, M. (2021). Sooner than you think: A very early affective reaction to the COVID‐19 pandemic and quarantine in Argentina. Journal of Affective Disorders, 282(March), 495–503. 10.1016/j.jad.2020.12.124 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vindegaard, N. , & Eriksen Benros, M. (2020). COVID‐19 pandemic and mental health consequences: Systematic review of the current evidence. Brain, Bahavior and Immunity, 89(October), 531–542. 10.1016/j.bbi.2020.05.048 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vloo, A. , Alessie, R. J. M. , Mierau, J. O. , Boezen, M. H. , Mierau, J. O. , Franke, L. , Dekens, J. , Deelen, P. , Lanting, P. , Vonk, J. M. , Nolte, I. , Ori, A. P. S. , Claringbould, A. , Boulogne, F. , Dijkema, M. X. L. , Wiersma, H. H. , Warmerdam, R. , & Jankipersadsing, S. A. (2021). Gender differences in the mental health impact of the COVID‐19 lockdown: Longitudinal evidence from The Netherlands. SSM ‐ Population Health, 15(September), 100878. 10.1016/J.SSMPH.2021.100878 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, C. , Pan, R. , Wan, X. , Tan, Y. , Xu, L. , McIntyre, R. S. , Choo, F. N. , Tran, B. , Ho, R. , Sharma, V. K. , & Ho, C. (2020). A longitudinal study on the mental health of general population during the COVID‐19 epidemic in China. Brain, Behavior, and Immunity, 87(July), 40–48. 10.1016/j.bbi.2020.04.028 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang, Y. , Di, Y. , Ye, J. , & Wei, W. (2021). Study on the public psychological states and its related factors during the outbreak of coronavirus disease 2019 (COVID‐19) in some regions of China. Psychology Health & Medicine, 26(1), 13–22. 10.1080/13548506.2020.1746817 [DOI] [PubMed] [Google Scholar]
- Witteveen, D. , & Velthorst, E. (2020). Economic hardship and mental health complaints during COVID‐19. Proceedings of the National Academy of Sciences, 117(44), 27277–27284. 10.1073/pnas.2009609117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization ‐WHO‐ (2020). Coronavirus disease (COVID‐19) pandemic. Retrieved from https://www.euro.who.int/en/health‐topics/health‐emergencies/coronavirus‐covid‐19/novel‐coronavirus‐2019‐ncov [Google Scholar]
- Xiong, J. , Lipsitz, O. , Nasri, F. , Lui, L. M. W. , Gill, H. , Phan, L. , Chen‐Li, D. , Iacobucci, M. , Ho, R. , Majeed, A. , & McIntyre, R. S. (2020). Impact of COVID‐19 pandemic on mental health in the general population: A systematic review. Journal of Affective Disorders, 277(December), 55–64. 10.1016/j.jad.2020.08.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou, S. J. , Zhang, L. G. , Wang, L. L. , Guo, Z. C. , Wang, J. Q. , Chen, J. C. , Liu, M. , Chen, X. , & Chen, J. X. (2020). Prevalence and socio‐demographic correlates of psychological health problems in Chinese adolescents during the outbreak of COVID‐19. European Child & Adolescent Psychiatry, 29(6), 749–758. 10.1007/s00787-020-01541-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding authors.