

Abstract
Objective
To investigate the accuracy of ultrasonic diagnosis using the tele‐ultrasound robot in Leishen Shan Hospital.
Method
Twenty‐two patients with novel coronavirus pneumonia from Leishen Shan Hospital voluntarily participated in this study. Their thyroids, neck vessels, hepatobiliaries and kidneys were scanned by both tele‐ultrasound robot manufactured by Imabot Co., Ltd, Wuhan and conventional method. The ultrasound diagnosis of each patient was compared, and the ultrasound images obtained by the two methods were mixed together and double‐blindly diagnosed by an experienced ultrasound radiologist.
Results
There were 44 positive lesions in 110 sites of 22 patients. Of which the two methods, 40 positive lesions were detected by the robotic method with 4 lesions missed (2 small polyps of gallbladder, 1 small hemangioma of liver and 1 small cyst of kidney) and 1 lesion misdiagnosed (normal carotid artery was misdiagnosed as carotid atherosclerotic plaque); 44 positive lesions were detected by conventional method with 1 small cyst of the liver was missed. There was no statistically significant difference in the accuracy rate between the robotic method and the conventional method using the chi‐square test of the four‐grid data (P>.05).
Conclusion
The application of tele‐ultrasound robot meets the standard of patient care during the pandemic. The method is feasible to provide adequate ultrasound information to diagnose common abdominal, vascular, superficial organ pathologies in patients with COVID‐19 with acceptable accuracy compared with a conventional ultrasound scan.
Keywords: coronavirus disease 2019, novel coronavirus pneumonia, tele‐ultrasound, ultrasonic robot
Abbreviation
- AI
artificial intelligence
Objective
The novel coronavirus pneumonia (COVID‐19) is an acute infectious pneumonia which have a substantial heritability. Pneumonia patients with novel coronavirus infection are considered the main source of infection, of which the transmission ways are mainly dominated by respiratory droplets, but also through contact. 1 Although the source of the virus and human‐to‐human transmission are still unknown, an increasing number of cases appear to be caused by human‐to‐human transmission. 2 , 3 Since novel coronavirus can be isolated from feces and urine, attention should be paid to the aerosol or contact transmission caused by feces and urine to environmental pollution. In a relatively confined environment, there is a possibility of aerosol propagation in the case of prolonged exposure to high concentrations of aerosols. There may be an aerosol propagation risk in closed, unventilated areas, therefore, protection and isolation treatment are needed to prevent further disease spreading. 4 For ultrasound radiologist, there is a high risk of infection when close‐up scans of patients are needed, especially in isolation sites such as Leishen Shan Hospital. As a result, reducing unnecessary contact is of great importance. With the development and innovation of mobile information, 5G technology has redefined remote and mobile ultrasound, providing distance ultrasound services, extended medical services to outdoor, and even more complex field scenarios. 5 During an outbreak, ultrasound radiologists have to wear protective clothes when close‐up contact with patient and work for long hours in airtight places. That can be extremely uncomfortable. The emergence of tele‐ultrasound robot become a good remedy regarding this scenario. The tele‐ultrasound robot can minimize the contact between radiologists and patients, reduce the unnecessary consumption of medical workers in the shortage of medical resources, and plays an important role in the Leishen Shan Hospitals and general hospitals of novel coronavirus pneumonia combined with other diseases.
Information Materials and Methods
Subjects
Twenty‐two patients voluntarily participated in this study of the application of tele‐ultrasound robot. The robot consists of a doctor‐end and a patient‐end. The doctor‐end is composed by structure components, operation control system, audio and video system and doctor‐end software. The patient‐end consists of structure component, motion execution system, ultrasonic system, audio and video system and patient‐end software. The remote ultrasonic diagnosis system is based on the scanning protocols of conventional ultrasound, and makes use of the Internet information transmission principle, master–slave control principle and human–computer interaction principle to realize the sharing of medical resources across regions. The ultrasound radiologist performs an ultrasound on the patient by manipulating the profile probe in real time to control the ultrasonic probe mounted at the end of the patient‐end's robotic arm. During the examination, the ultrasound radiologist can communicate with the patient through the audio and video system with high‐quality, adjust the parameters of the ultrasonic equipment on the patient‐end in real time, and obtain the real‐time ultrasound images for medical diagnosis. After removing the probe on the robotic arm, conventional ultrasound scanning can be performed. The robot is suitable for ultrasound examination of abdomen, superficial, small organs and peripheral vessels. In this experiment, two types of C5‐1 and L15‐4 probes were selected to scan the thyroid, cervical vessels, hepatobiliary and kidneys of 22 patients with novel coronavirus pneumonia from Leishen Shan Hospital from February to April 2020. Of all the patients who participated in the robotic ultrasound study, 13 were male and 9 were female, aged 39–74. All participants gave their informed written consent and the study was approved by the medical ethics committee of Zhongnan hospital of Wuhan University (2020139).
Method
Instrument Selection
The instrument is a tele‐ultrasound robot named MGIUS‐R3 from Imabot Co., Ltd, Wuhan (Figure 1). which consists of a patient‐end and a doctor‐end.
Figure 1.
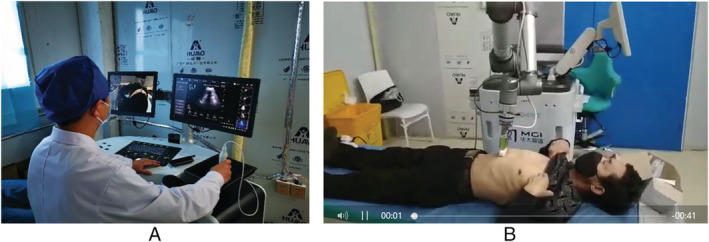
A. A doctor operates the tele‐ultrasound robot with the doctor‐end in the examination room. B. The patient‐end moves with correspondence to the operation in the isolation area of Leishen Shan Hospital to scan patients.
Image Acquisition
The 22 patients with novel coronavirus pneumonia were numbered, and their personal identity information was hidden for tele‐ultrasound robot examination. The patient‐end is located in the isolation area of Wuhan Leishen Shan Hospital (contaminated area). Experienced doctors performed remote ultrasound examinations on patients in the ultrasound examination room (clean area) of Leishen Shan Hospital with the doctor‐end, and the two are isolated from contact. All patients were fasted for more than 8 hours as required. Small organs (thyroid, Figure 2), peripheral blood vessels (neck vessels, Figure 3), digestive system (liver and gallbladder, Figure 4) and urinary system (kidneys, Figure 5) were scanned, respectively. The acquired images include: the first hepatic portal of the liver, the I‐shaped structure of the left portal vein, the second hepatic portal, the top of the diaphragm, the long axis of the gallbladder, the long axis of the kidneys, the transverse section and long axis of the thyroid, the transverse section and long axis of the common carotid artery and carotid sinus, internal carotid artery, and external carotid artery (see Table 1). Ultrasound diagnosis report will be issued immediately after an examination. Subsequently, a new round of numbering was performed on the 22 patients, the same ultrasound radiologist obtained the ultrasound probe from the robotic arm at the patient‐end to perform ultrasound examinations using conventional method. After the examination, an ultrasound diagnosis report shall be issued immediately. In traditional method, patient preparation and image acquisition are consistent with the tele‐ultrasound robot method.
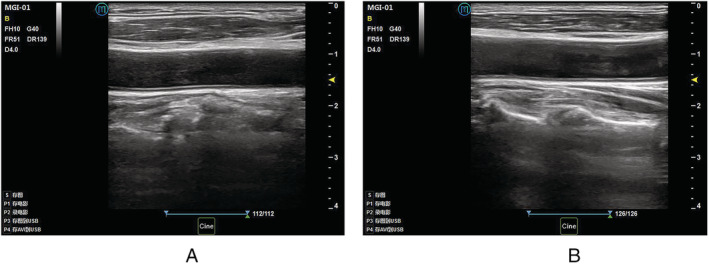
Figure 2.
A. Ultrasound image of thyroid generated by scanning with robotic method. B. Ultrasound image of thyroid generated by scanning with conventional method.
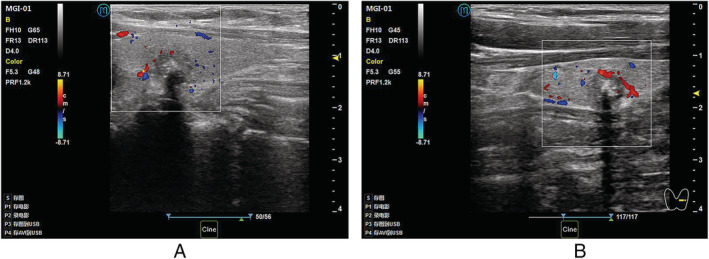
Figure 3.
A. Ultrasound image of neck vessels generated by scanning with robotic method. B. Ultrasound image of neck vessels generated by scanning with conventional method.
Figure 4.
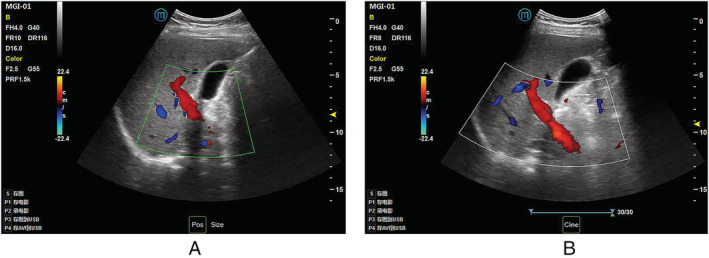
A. Ultrasound image of hepatobiliary generated by scanning with robotic method. B. Ultrasound image of hepatobiliary generated by scanning with conventional method.
Figure 5.
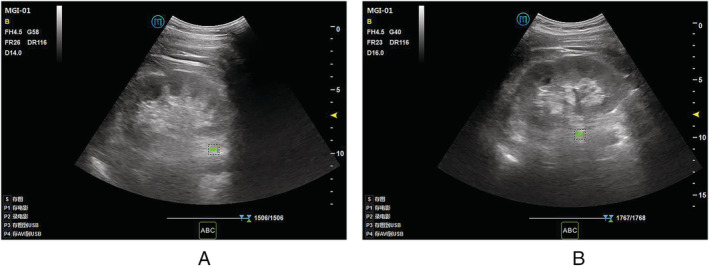
A. Ultrasound image of kidney generated by scanning with robotic method. B. Ultrasound image of kidney generated by scanning with conventional method.
Table 1.
The Acquired Images
| Types of Organ | Acquired Images |
|---|---|
|
Liver Gallbladder Kidney Thyroid Carotid Common carotid artery Carotid sinus Internal carotid artery External carotid artery |
The first hepatic portal The i‐shaped structure of the left portal vein The second hepatic portal The top of the diaphragm The long axis The long axis The transverse section and long axis The transverse section and long axis |
Comparison of Ultrasound Diagnostic Results
The doctor numbering the patients summarizes and compares the ultrasound images of the two batches of numbered patients while another senior doctor (associate chief physician) diagnoses the ultrasound images. If the two numbered examination results are different, the senior doctor will perform an ultrasound examination again on the patient to obtain the diagnosis result.
Statistical Analysis
All data were statistically analyzed using SPSS 26.0 software. The numeration data were statistically analyzed with χ 2 test and the difference was statistically significant with P < .05.
Results
Comparison of the Results of Robot Ultrasound and Conventional Ultrasound Scanning
In the 110 examination sites of 22 patients, 44 positive lesions were detected, including diffuse thyroid disease, thyroid nodules, carotid atherosclerosis, carotid atherosclerotic plaque formation, liver cyst, liver hemangioma, gallbladder stones, gallbladder polyps, kidney stones, renal cysts, renal atrophy, and diffuse renal parenchymal lesions. There are 16 positive lesions in the thyroid gland, 10 in the neck blood vessels, 6 in the liver, 4 in the gallbladder, and 8 in kidneys in total.
In the two ultrasound examination methods, a total of 41 positive lesions were detected by robotic method, 43 positive lesions were detected by traditional method. There were a total of 39 identical diagnosis between the two (see Table 2).
Table 2.
Comparison of Diagnosis Results between Robot Method and Traditional Method
| Types of Disease | Robot Method | Traditional Method |
|---|---|---|
| Diffuse thyroid disease | 3 | 3 |
| Thyroid nodules | 13 | 13 |
| Cervical atherosclerosis | 3 | 3 |
| Carotid atherosclerotic plaque formation | 8 | 7 |
| Liver cyst | 4 | 3 |
| Hepatic hemangioma | 1 | 2 |
| Gallbladder stones | 1 | 1 |
| Gallbladder polyps | 1 | 3 |
| Kidney stones | 3 | 3 |
| Renal cyst | 2 | 3 |
| Kidney atrophy | 1 | 1 |
| Diffuse renal parenchymal lesions | 1 | 1 |
Comparison the False Positive and False Negative between Robotic Method and Conventional Method
In the 44 cases of positive lesions, 41 positive lesions were detected 39 were diagnosed, 4 were missed, and 1 was misdiagnosed by tele‐ultrasound robotic method. The missed diagnosis included 2 small polyps of the gallbladder, 1 small hepatic hemangioma, and 1 small renal cyst. One carotid atherosclerotic plaque was misdiagnosed by normal neck vessels. Among the 43 positive lesions scanned by conventional method, 1 small liver cyst was missed (see Table 3). The χ 2 test of the four‐grid data was used to compare the diagnostic rate of ultrasonic scanning between the robot method and the traditional method (P > .05), and the difference between them was not statistically significant.
Table 3.
Comparison of Missing and Misdiagnosis Between Robot Method and Traditional Method
| Scanning method | Misdiagnosis and missed diagnosis | Correct diagnosis |
|---|---|---|
| Robot method | 5 | 39 |
| Traditional method | 1 | 43 |
| χ 2 | 2.86 | |
| P | 0.09 | |
Discussion
With the development of mobile communication and the improvement of network technology, the advent of 5G technology has become a popular trend in the new era. 6 Its characteristics, such as low power consumption, low delay, high speed and wide coverage, have broken technical barriers for the development of remote ultrasound robot.
Tele‐ultrasound is an integration of information technology, the Internet, artificial intelligence (AI), cloud computing, 5G technology, etc. The images on the ultrasound equipment are transmitted to the remote server or cloud through wired or wireless transmission, and the functions of data management and sharing, remote consultation, background analysis, reverse control and pre‐hospital emergency treatment are realized through remote data retrieval. 7 , 8 The robotic arm with a probe is remotely operated by doctors at the remote site through the simulation probe to obtain real‐time ultrasonic images. Compression strength and instrument parameters can be adjusted by the doctors with ease. Doctors are also able to communicate with patients, diagnose the patient and guide treatment directly through high‐quality audio and video system. 5G technology realizes the real‐time synchronous exchange for the images, voice, scene of the tele‐ultrasound robot system. 9 There is no need for an sonographer to be present in a remote area or in a isolation ward, especially during the COVID‐19 epidemic, where medical resources are in extreme short supply. It can save medical resources, and also avoid the risk of infection by direct contact.
COVID‐19 is an acute respiratory disease caused by novel Coronavirus infection. It is characterized as generally susceptible with rapid transmission, rapid progression, and high rates of critical illness. Cutting off the route of transmission, reducing unnecessary contact as well as contact isolation, are effective way to reduce infection. In the prevention and control of the epidemic, although CT plays an important role in the early detection of pulmonary lesions, COVID‐19 patients is not just simply characterized by respiratory disease, it can also involve disease in other systems such as liver, kidney, heart, vessels, reproductive systems. The incidence of complications in severe patients was significantly higher than that in non‐severe patients,the difference was statistically significant. 10 , 11 As a fast, non‐invasive and effective diagnostic and treatment tool, ultrasound obviously plays an important role in the prevention, control and treatment of the epidemic.
In this study, 22 patients with COVID‐19 at Leishen Shan Hospital were randomly selected, and all volunteered to participate in the tele‐ultrasound robot research. Multiple organs, such as thyroid, neck vessels, hepatobiliary and kidney, were scanned by both the robot method and the traditional method. It is concluded that there are some missed diagnosis and misdiagnosis by the robot method. However, there was no statistically significant difference between the two diagnosis rates achieved by the two methods (P > .05). Results shows that, to some extent, remote robotic ultrasonic scanning can replace conventional ultrasonic scanning. The two methods are consistent with the diagnosis of 39 cases, while 5 cases with different diagnoses are observed. Patients with different diagnoses were re‐examined by an associate chief ultrasound physician with 10 years of work experience, among which 2 cases of small gallbladder polyps, 1 case of small hepatic hemangioma, 1 case of small renal cyst were missed and 1 case of carotid atherosclerotic plaque was misdiagnosed by normal cervical vessels by robot method while 1 case of small liver cyst was missed by traditional methods. By comparing the ultrasound images acquired by the two ultrasound scanning methods, the senior physicians analyzed the possibility of misdiagnosis and missed diagnosis. The tele‐ultrasound robot used in this study is composed of a doctor‐end and patient‐end. The sonographer controlled a robotic arm in the patient‐end by the simulated controller in the doctor‐end to simulate a traditional ultrasound scan. Due to the mechanical arm activity limitations, the manipulator is less flexible than the traditional ultrasonic scanning in adjusting the probe position, tilting the angle and moving the target area slightly, 9 which easily causes misdiagnosis. In this study, the possible reasons for missed diagnosis in robotic scanning include not only the incomplete scope of robotic scanning, the unproficiency of the sonographer and the poor cooperation of the patients, but the small scope of the lesion, the hidden location of the lesion and the inconspicuous echo of the lesion. However, a small hepatic cyst was also missed by the conventional method. It can be seen that no matter which scanning method has its certain rate of missed diagnosis, but there is no statistical significance between the two; One case of carotid atherosclerotic plaque was misdiagnosed by the robot, which may be caused by false image due to improper gain and blood flow regulation.
Through this study, it can be seen that robotic ultrasound can replace conventional ultrasound in the diagnosis of common diseases to a certain extent, meet daily needs. Especially in areas where medical resources are scarce, in rural areas, in remote mountainous areas, and in isolated areas like Leishen Shan Hospital, 5G tele‐ultrasonic robots can be better utilized. The improvement of robot performance and the accumulation of operator experience may reduce the rate of missed diagnosis.
At present, 5G ultrasound robot technology is still in its infancy and is rarely used in clinical practice. First, the equipment is large、heavy and expensive, the mobility is poor and the operation flexibility needs to be improved. Second, the inspection time‐consuming and accuracy are related to the operator's proficiency. The proficiency of sonographers in tele‐ultrasound robot operation cannot be more exercised. Compared with traditional ultrasound scanning, it takes a long time which is positively correlated with the proficiency of the operator. Moreover, the current sample size is small and the positive disease is relatively single. The sample size, multi‐organ and multi‐disease research can be expanded in the future, then the feasibility of tele‐ultrasound robots in clinical applications and the advantages of scanning different organs can be discussed more accurately, so as to better and more widely used in clinical practice, especially in areas of shortage of medical resources and epidemic situation. Ultrasound techniques differ from CT and MRI, which are not affected by air and bony structures to produce adequate images. There is still a long way for robotic ultrasound to replace conventional ultrasound scans in clinical patient care.
In conclusion, the application of tele‐ultrasound robot is feasible to provide adequate ultrasound information to diagnose common abdominal, vascular, superficial organ pathologies in patients with COVID 19 with acceptable accuracy compared with a conventional ultrasound scan.
Wenli Jiang, Xia Zhao, Tian Gan, Ying Liu contributed equally to this work.
The authors would like to express our gratitude to all participating clinicians. Thanks to Imabot Co. Ltd. for the tele‐operated ultrasound robot. No funding was received for conducting this study.
References
- 1.General Office of National Health Committee Office of National Administration of Traditional Chinese Medicine. Notice on the issuance of a programme for the diagnosis and treatment of novel coronavirus (2019‐nCoV) infected pneumonia (Trial Version 7). 2020. http://bgs.satcm.gov.cn/zhengcewenjian/2020-03-04/13594.html. Accessed 4 Mar 2020.
- 2. Chan JFW, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person‐to‐person transmission: a study of a family cluster. Lancet 2020; 395:514–523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China. N Engl J Med 2020; 382:727–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Bureau of Disease Prevention and Control, National Health Committee, Disease Prevention and Control Center of China . Public protection guideline to the novel coronavirus infectious pneumonia. Beijing: People's Medical Publishing House; 2020:26. [Google Scholar]
- 5. Ability Building and Continuing Education Center of National Health Committee , Ultrasonic Committee of Trauma, Emergency and Critical Care , Committee of Remote and Mobile Ultrasound , Ultrasonic Equipment Technology Branch , China Associate of Medical Equipment . Expert Consensus on The 5G's Remote and Ultrasonic Application. Chin J Med Ultrasound (Electron Ed) 2020; 17:115–123. [Google Scholar]
- 6. Soni NJ, Boyd JS, Mints G, et al. Comparison of in‐person versus tele‐ultrasound point‐of‐care ultrasound training during the COVID‐19 pandemic. Ultrasound J 2021; 13:39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Liu YH, Lyu FQ, Li TS. The advent of 5G era: current situation and development of remote ultrasound. Chin J Med Ultrasound (Electron Ed). 2019; 16:241–243. [Google Scholar]
- 8. Rabie NZ, Sandlin AT, Barber KA, et al. Teleultrasound: how accurate are we? J Ultrasound Med 2017; 36:2329–2335. [DOI] [PubMed] [Google Scholar]
- 9. Lv FQ. Remote ultrasound and its application Prospect of 5G. Chin. J. Med. Ultrasound (Electron. Ed.) 2019; 16:320. [Google Scholar]
- 10. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of 2019 novel coronavirus infection in China. medRxiv 2020; 382:1708–1720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 2020; 395:507–513. [DOI] [PMC free article] [PubMed] [Google Scholar]