

Abstract
Background
Solid organ transplant recipients (SOTRs) are at high‐risk for severe infection from severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2). Anti‐spike monoclonal antibodies are currently utilized under emergency use authorization to prevent hospitalization in high‐risk individuals with coronavirus disease 2019 (COVID‐19), including SOTRs. However, clinical data for bebtelovimab, the sole currently available anti‐spike monoclonal antibody for COVID‐19, is limited.
Methods
We conducted a retrospective cohort study of adult SOTRs diagnosed with mild‐to‐moderate COVID‐19 from January 2022 through May 2022 who received either bebtelovimab or sotrovimab. The primary outcome was COVID‐19‐related hospitalization within 30 days of COVID‐19 diagnosis. Data were analyzed with Fisher's exact test.
Results
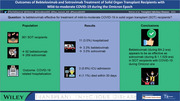
Among 361 SOTRs, 92 (25.5%) received bebtelovimab and 269 (74.5%) received sotrovimab. The most common organ transplant was a kidney (42.4%). SOTRs who received bebtelovimab had a higher proportion who had received a booster SARS‐CoV‐2 vaccine dose and had received their last vaccination dose more recently. Eleven (3.0%) SOTRs were hospitalized, and rates of hospitalization were similar between monoclonal antibody groups (3.3% versus 3.0%; p > .99). Three patients required admission to an intensive care unit, all of who received sotrovimab. Four (1.1%) patients died within 30 days of COVID‐19 diagnosis, two from each group.
Conclusions
SOTRs with mild‐to‐moderate COVID‐19 who received bebtelovimab had similar rates of COVID‐19‐related hospitalization as those who received sotrovimab. While differences in vaccination rates and viral subvariants could act as confounders, bebtelovimab appears to be of similar effectiveness as sotrovimab.
Keywords: COVID‐19, SARS‐CoV‐2, bebtelovimab, organ transplantation, anti‐spike monoclonal antibody
ABBREVIATIONS
- COVID‐19
coronavirus disease 2019
- EUA
emergency use authorization
- ICU
intensive care unit
- MASS
monoclonal antibody screening score
- SARS‐CoV‐2
severe acute respiratory syndrome coronavirus 2
- SOTR
solid organ transplant recipient
- US FDA
US Food and Drug Administration
1. BACKGROUND
Solid organ transplant recipients (SOTR) are at high‐risk for complications from severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2) including hospitalization, allograft loss, and mortality. 1 , 2 Several therapeutics have been developed for coronavirus disease 2019 (COVID‐19), including anti‐spike neutralizing monoclonal antibodies. These monoclonal antibodies were initially shown to be effective in preventing hospitalization and death in randomized clinical trials conducted in heterogeneous cohorts of high‐risk patients. 3 , 4 , 5 The effectiveness of anti‐spike monoclonal antibodies in SOTR has been demonstrated in retrospective studies of patients who were treated under emergency use authorization (EUA). 6 , 7 These studies have largely assessed bamlanivimab with or without etesevimab, casirivimab‐imdevimab, and sotrovimab. However, the clinical outcomes of treatment with newer therapies such as bebtelovimab are not known.
The emergence of SARS‐CoV‐2 Omicron variant B.1.1.529 led to revocation of the EUA of for bamlanivimab‐etesevimab and casirivimab‐imdevimab. In January 2022, sotrovimab was the sole anti‐spike neutralizing monoclonal antibody therapy authorized for use. Real‐world retrospective data have suggested that sotrovimab was effective in reducing hospitalization and mortality among SOTRs with COVID‐19 when compared to untreated patients. 8 , 9 However, SARS‐CoV‐2 Omicron further evolved into BA.2 subvariants with reduced susceptibility to sotrovimab. Subsequently, the EUA for sotrovimab was rescinded by the US Food and Drug Administration (US FDA), leaving bebtelovimab as the only anti‐spike monoclonal antibody available for outpatient treatment of mild to moderate COVID‐19.
Bebtelovimab received EUA from the US FDA in February 2022 based on in vitro data suggesting its activity against Omicron variants including BA.2 and very limited unpublished clinical data. 10 To date, there have been no reports on the outcomes of patients treated with bebtelovimab. In this study, we aimed to assess the outcomes of SOTRs with COVID‐19 treated with bebtelovimab and compared it to those treated with sotrovimab during the period dominated by SARS‐CoV‐2 Omicron variants.
2. METHODS
2.1. Study design
We performed a multicenter cohort study of SOTRs with test‐confirmed mild‐to‐moderate COVID‐19 who received treatment with bebtelovimab or sotrovimab at our infusion therapy centers in Arizona, Florida, Minnesota, and Wisconsin. Sotrovimab (500‐mg single dose given by intravenous infusion) was used from January 1, 2022, to the week of March 21, 2022, when treatment was switched to Bebtelovimab (175‐mg single dose by an intravenous push over 1 min) because of the emergence of the BA.2 subvariants. Patients were identified from our COVID‐19 registry from January 1, 2022, through May 30, 2022. This study was reviewed by the Mayo Clinic institutional review board and granted an exempt status (#20‐012919).
Inclusion criteria were age ≥18 years, organ transplantation prior to COVID‐19 diagnosis, and receipt of bebtelovimab or sotrovimab for treatment of mild‐to‐moderate COVID‐19. Patients without research authorization were excluded. Data included baseline demographics, transplant‐specific characteristics, medical comorbidities, COVID‐19 vaccination and therapies, and outcomes. Charlson comorbidity index and monoclonal antibody screening score (MASS) were used as composite measures of medical comorbidities. MASS consists of the conditions set forth by the US FDA as criteria for treatment with neutralizing anti‐spike monoclonal antibodies, as previously described. 11
Full SARS‐CoV‐2 vaccination was defined as receipt of at least three doses of an mRNA vaccine or at least one dose each of an adenovirus vector vaccine and mRNA vaccine. A booster vaccine dose was defined as receipt of a vaccine after having met the criteria for full vaccination status. Partial vaccination included those who had received at least 1 dose of the SARS‐CoV‐2 vaccine but did not meet the criteria for full vaccination.
The primary outcome of interest was COVID‐19‐related hospitalization within 30 days of COVID‐19 diagnosis. Secondary outcomes included intensive care unit (ICU) admission and 30‐day mortality.
2.2. Statistical analysis
Continuous variables were summarized as either median with interquartile range or mean with standard deviation. Categorical variables were analyzed by Fisher's exact test. All analyses were performed using BlueSky Statistics version 7.40 (BlueSky Statistics LLC, Chicago, Illinois) and the Charlson comorbidity index was computed using the comorbidity package in RStudio version 1.4.1106 (PBC). 12
3. RESULTS
3.1. Patient population
Among 361 SOTRs who received anti‐spike neutralizing monoclonal antibody therapy during the Omicron period, 92 (25.5%) received bebtelovimab. The most common transplanted organ was the kidney (42.4%) and 44 (12.2%) had received multiple transplanted organs. Those who received bebtelovimab had more remote transplants (median 5.6 versus 4.0 years) but had MASS and Charlson comorbidity index that were compatible with those who received sotrovimab. The bebtelovimab group had a greater proportion who were fully vaccinated, and many more had received a SARS‐CoV‐2 vaccine booster dose (45.7% versus 4.1%). Sixty fully‐vaccinated patients without a booster dose (four bebtelovimab and 56 sotrovimab) had received their last vaccination less than 4 months prior and were not yet eligible for a booster dose. No patients had received tixagevimab‐cilgavimab as pre‐exposure prophylaxis. Further details of the two cohorts are included in Table 1.
TABLE 1.
Characteristics of 361 solid organ transplant recipients treated with bebtelovimab or sotrovimab for mild‐to‐moderate coronavirus disease 2019 (COVID‐19)
| Bebtelovimab (N = 92) | Sotrovimab (N = 269) | Total (N = 361) | |
|---|---|---|---|
| Age, mean (SD), years | 59.7 (14.0) | 56.9 (14.8) | 57.7 (14.6) |
| Female sex | 37 (40.2) | 102 (37.9) | 139 (38.5) |
| Race (N = 360) | |||
| ‐ American Indian or Alaska Native | 0 (0) | 3 (1.1) | 3 (0.8) |
| ‐ Asian | 3 (3.3) | 10 (3.7) | 13 (3.6) |
| ‐ Black or African American | 4 (4.3) | 26 (9.7) | 30 (8.3) |
| ‐ Native Hawaiian or Other Pacific Islander | 0 (0) | 4 (1.5) | 4 (1.1) |
| ‐ White | 85 (92.4) | 222 (82.8) | 307 (85.3) |
| ‐ Other | 0 (0) | 3 (1.1) | 3 (0.8) |
| Hispanic or Latino ethnicity (N = 357) | 5 (5.4) | 25 (9.4) | 30 (8.4) |
| Transplant Type | |||
| ‐ Heart | 23 (25.0) | 39 (14.5) | 62 (17.2) |
| ‐ Kidney | 34 (37.0) | 119 (44.2) | 153 (42.4) |
| ‐ Liver | 22 (23.9) | 57 (21.2) | 79 (21.9) |
| ‐ Lung | 4 (4.3) | 17 (6.3) | 21 (5.8) |
| ‐ Pancreas | 0 (0) | 2 (0.7) | 2 (0.6) |
| ‐ Multiorgan a | 9 (9.8) | 35 (13.0) | 44 (12.2) |
| Subsequent transplant | 8 (8.7) | 36 (13.4) | 44 (12.2) |
| Time from transplant, median (IQR), years | 5.6 (2.0, 10.8) | 4.0 (1.6, 9.4) | 4.4 (1.7, 9.8) |
| Body mass index, median (IQR), kg/m2 | 28.3 (25.8, 32.1) | 27.9 (24.0, 32.0) | 28.0 (24.1, 32.0) |
| Diabetes mellitus | 36 (39.1) | 105 (39.0) | 141 (39.1) |
| Chronic pulmonary disease | 12 (13.0) | 29 (10.8) | 41 (11.4) |
| MASS, median (IQR) | 9.0 (6.0, 10) | 8.0 (6.0, 10) | 8.0 (6.0, 10) |
| Charlson comorbidity index, median (IQR) | 4.0 (2.0, 5.0) | 4.0 (2.0, 5.0) | 4.0 (2.0, 5.0) |
| Vaccination status | |||
| ‐ Booster vaccine dose | 42 (45.7) | 11 (4.1) | 53 (14.7) |
| ‐ Fully vaccinated, unboosted | 26 (28.3) | 167 (62.1) | 193 (53.5) |
| ‐ Partially vaccinated | 11 (12.0) | 56 (20.8) | 67 (18.6) |
| ‐ Unvaccinated | 13 (14.1) | 35 (13.0) | 48 (13.3) |
| Vaccine manufacturer (N = 313) | |||
| ‐ Johnson & Johnson | 3 (3.8) | 12 (5.1) | 15 (4.8) |
| ‐ Moderna | 34 (43.0) | 93 (39.7) | 127 (40.6) |
| ‐ Pfizer‐BioNTech | 42 (53.2) | 129 (55.1) | 171 (54.6) |
| Time from last vaccine dose to diagnosis, median (IQR), days | 104.0 (68.0, 220.5) | 140 (98.2, 158.0) | 137.0 (89.0, 162.0) |
| Time from diagnosis to monoclonal antibody infusion, median (IQR), days | 1.0 (1.0, 2.0) | 2.0 (1.0, 3.0) | 2.0 (1.0, 3.0) |
Data are N (%)unless otherwise specified.
Abbreviations: IQR, interquartile range; MASS, monoclonal antibody screening score; SD, standard deviation.
Multiorgan transplants include kidney‐pancreas (17), heart‐kidney (12), liver‐kidney (11), heart‐liver (2), and heart‐lung (2).
3.2. Outcomes
Eleven (3.0%) SOTRs required hospitalization for COVID‐19, including three (0.8%) who were admitted to the ICU. Nine admitted patients received additional COVID‐19‐directed therapy, including remdesivir (N = 7), corticosteroids (N = 7), and tocilizumab (N = 1). No patients received baricitinib or convalescent plasma.
Among eleven hospitalized patients, three (3.3%) had received bebtelovimab and eight (3.0%) had received sotrovimab. No patients who received bebtelovimab required ICU admission. Treatment with bebtelovimab was not associated with hospitalization (p > 0.99). In contrast, lack of full vaccination status was significantly associated with hospitalization (p = 0.007).
Four patients died within 30 days of COVID‐19 diagnosis; one was unvaccinated, one was fully vaccinated without a booster dose, and two were fully vaccinated with a booster. Two had received bebtelovimab and the other two had received sotrovimab. The causes of death were an acute respiratory failure from progressive COVID‐19, subarachnoid hemorrhage, and two were from unknown causes. The patient who died from progressive COVID‐19 was fully vaccinated, boosted, and received bebtelovimab. Next‐generation sequencing of the SARS‐CoV‐2 in bronchoalveolar fluid identified Omicron BA.2 variant with multiple spike mutations of interest (Supplementary Table).
4. DISCUSSION
This study provides the first real‐world data on the outcomes of bebtelovimab therapy for SOTRs. Outcomes were favorable, with low rates of hospitalization, ICU admission, and death within 30 days of diagnosis. This study showed comparable outcomes between SOTRs treated with bebtelovimab and sotrovimab, which implies the potential effectiveness of bebtelovimab in treating SOTRs with mild‐to‐moderate COVID‐19.
The existing data regarding outcomes of bebtelovimab were from phase 1/2 clinical trials performed primarily during the SARS‐CoV‐2 Delta era. 10 While bebtelovimab displayed significant reductions in SARS‐CoV‐2 viral loads compared to placebo in low‐risk individuals, these trials were underpowered to detect differences in clinical outcomes. The high‐risk arm of this study found a hospitalization rate of 3.0% among bebtelovimab‐treated patients during the Delta era, and this is comparable to our current study that was performed during the Omicron era.
Several studies have examined the outcomes of anti‐spike monoclonal antibody therapy in high‐risk patients, including specific transplant populations. 6 , 7 , 8 , 9 While much of these data predate the Omicron era, these studies have largely demonstrated overall good outcomes, including low rates of progression to severe infection, hospitalization, and death. Previous anti‐spike monoclonal antibody therapies have largely been considered equivalent in effectiveness, assuming the current circulating variant has adequate susceptibility. 11 The present study does not show any significant differences in the rates of hospitalization between bebtelovimab or sotrovimab, the rate of hospitalization in this study was lower when compared to prior studies that reported as high as 12% after treatment with bamlanivimab and casirivimab‐etesevimab during a period prior to Delta. 6 , 7 , 13 This is reassuring and may reflect the higher rates of vaccination in our cohort and the lower virulence of the Omicron variant. There was one patient who died of progressive COVID‐19, whose SARS‐CoV‐2 was sequenced as the BA.2 subvariant. It is unclear if any of the multiple spike mutations of interest may have impacted bebtelovimab's efficacy, and this requires further study.
Limitations of this study include its retrospective nature which is subject to intrinsic sources of bias or confounding. The two anti‐spike monoclonal antibody products were used sequentially during two different time points of the Omicron epoch. Patients who received bebtelovimab were treated later in the study period and had more opportunities for SARS‐CoV‐2 vaccination, as reflected in the larger proportions of patients with full vaccination or who received a vaccine booster dose. COVID‐19 vaccination has been associated with improved outcomes and this could have biased the results in favor of bebtelovimab. 8 Given the small number of hospitalizations, we were unable to perform multivariable analysis to adjust for vaccination status or other potential confounders. Furthermore, transplant providers have been successful in connecting SOTRs to care when they are diagnosed with COVID‐19. This has led to high rates of uptake and rapid time to infusion of these antibody treatments. Accordingly, we did not have a contemporary group of untreated SOTRs with mild‐to‐moderate COVID‐19 who can serve as a control to confirm the effectiveness of bebtelovimab. Without an untreated control group, we decided to compare bebtelovimab with sotrovimab, another anti‐spike monoclonal antibody used during the Omicron epoch that has been shown to improve outcomes of SOTRs. Our analysis suggests that the outcomes of bebtelovimab to sotrovimab are comparable in the Omicron era. Finally, while most SOTRs in this study are presumably infected with the Omicron SARS‐CoV‐2 variant, based on CDC tracking, there are differences in Omicron subvariant predominance during the study period. This includes the emergence of the Omicron BA.2 variant during the later period, which rendered sotrovimab as an ineffective therapy. It is possible that there may be biological differences among the Omicron subvariants which could have influenced our outcomes.
In conclusion, this study shows similar outcomes between bebtelovimab and sotrovimab in SOTRs with mild‐to‐moderate COVID‐19 during the Omicron epoch. These data support the continued use of bebtelovimab as a treatment for mild‐to‐moderate COVID‐19 in this high‐risk SOT population. Larger prospective and controlled studies are required to confirm our findings.
CONFLICT OF INTEREST
Raymund R. Razonable receives research support (funds provided to the institution) from Gilead, Regeneron, Roche, the MITRE corporation, and Nference, Inc. Raymund R. Razonable serves on the advisory board for Glaxo Smith Kline and the Data Safety Monitoring Board for Novartis. None of these entities have provided support for this current study. John C. O'Horo received grants from Nference, Inc., and the MITRE Corporation, as well as consulting fees from Bates College. All other authors have no conflicts of interest to report.
AUTHOR CONTRIBUTIONS
All authors participated in the research design. Zachary A. Yetmar and John C. O'Horo participated in the acquisition of the data. Zachary A. Yetmar and John C. O'Horo participated in the data analysis. All authors participated in the interpretation of the data. Zachary A. Yetmar wrote the first draft and all other authors provided critical revisions to the manuscript.
Supporting information
Supporting Information
Graphical Abstract
ACKNOWLEDGMENTS
This work was supported by the National Institutes of Health [UL1TR002377]. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. The work is supported by an intramural research grant from the Mayo Clinic to RRR.
Yetmar ZA, Beam E, O'Horo JC, et al. Outcomes of bebtelovimab and sotrovimab treatment of solid organ transplant recipients with mild‐to‐moderate coronavirus disease 2019 during the Omicron epoch. Transpl Infect Dis. 2022;eid13901. 10.1111/tid.13901
REFERENCES
- 1. Kates OS, Haydel BM, Florman SS, et al. Coronavirus disease 2019 in solid organ transplant: a multicenter cohort study. Clin Infect Dis. 2021;73(11):e4090‐e4099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Vinson AJ, Agarwal G, Dai R, et al. COVID‐19 in solid organ transplantation: results of the national COVID cohort collaborative. Transplant Direct. 2021;7(11):e775. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Dougan M, Nirula A, Azizad M, et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID‐19. N Engl J Med. 2021;385(15):1382‐1392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Gupta A, Gonzalez‐Rojas Y, Juarez E, et al. Early Treatment for Covid‐19 with SARS‐CoV‐2 neutralizing antibody sotrovimab. N Engl J Med. 2021;385(21):1941‐1950. [DOI] [PubMed] [Google Scholar]
- 5. Weinreich DM, Sivapalasingam S, Norton T, et al. REGEN‐COV antibody combination and outcomes in outpatients with COVID‐19. N Engl J Med. 2021;385(23):e81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Sarrell BA, Bloch K, El Chediak A, et al. Monoclonal antibody treatment for COVID‐19 in solid organ transplant recipients. Transpl Infect Dis. 2022;24(1):e13759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Yetmar ZA, Beam E, O'Horo JC, et al. Monoclonal antibody therapy for COVID‐19 in solid organ transplant recipients. Open Forum Infect Dis. 2021;8(6):ofab255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Solera JT, Arbol BG, Alshahrani A, et al. Impact of vaccination and early monoclonal antibody therapy on COVID‐19 outcomes in organ transplant recipients during the omicron wave. Clin Infect Dis. 2022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Wong G, Rowlandson M, Sabanayagam D, et al. COVID‐19 infection with the omicron SARS‐CoV‐2 variant in a cohort of kidney and kidney pancreas transplant recipients: clinical features, risk factors, and outcomes. Transplantation. 2022. [DOI] [PubMed] [Google Scholar]
- 10. Food and Drug Administration . Fact sheet for healthcare providers: emergency use authorization for bebtelovimab. 2022. https://www.fda.gov/media/156152/download. Accessed June 27, 2022.
- 11. Ganesh R, Philpot LM, Bierle DM, et al. Real‐world clinical outcomes of bamlanivimab and casirivimab‐imdevimab among high‐risk patients with mild to moderate coronavirus disease 2019. J Infect Dis. 2021;224(8):1278‐1286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Gasparini A, Salmasian H, Williman J, Chia S, Teo E. Comorbidity: computing comorbidity scores. 2022. https://cran.r‐project.org/web/packages/comorbidity/index.html. Accessed June 27, 2022.
- 13. Yetmar ZA, Bhaimia E, Bierle DM, Ganesh R, Razonable RR. Breakthrough COVID‐19 after SARS‐CoV‐2 vaccination in solid organ transplant recipients: An analysis of symptomatic cases and monoclonal antibody therapy. Transpl Infect Dis. 2022;24(2):e13779. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information
Graphical Abstract