

Abstract
Background
Surveys of changes in drinking during the COVID‐19 pandemic have primarily relied on retrospective self‐report. Further, most such surveys have not included detailed measures of alcohol use patterns, such as beverage‐specific consumption, nor measures of alcohol use disorder (AUD) symptoms that would allow a comprehensive understanding of changes in alcohol use.
Methods
Data from 1819 completed interviews from the N14C follow‐up survey to the 2019 to 2020 National Alcohol Survey (N14) were conducted between January 30 and March 28, 2021. Questions on alcohol use from the Graduated Frequency series, beverage‐specific quantity and frequency, and DSM‐5 AUD items were asked in both surveys and used to estimate changes from pre‐pandemic drinking to drinking during the pandemic. Analyses focus on changes in these measures over time and comparisons between key subgroups defined by gender, race/ethnicity, and age.
Results
Key findings include particularly large increases in drinking and AUD for African Americans and women, reduced drinking and heavy drinking prevalence among men and White respondents, and a concentration of increased drinking and AUD among respondents aged 35 to 49. Increases in alcohol use were found to be driven particularly by increases in drinking frequency and the consumption of spirits.
Conclusions
Results confirm prior findings of overall increases and subgroup‐specific changes, and importantly, provide detailed information on the patterns of change across major socio‐demographic subgroups. Substantial increases in the prevalence of DSM‐5 moderate to severe AUDs are a novel finding that is of particular concern.
Keywords: beverage‐specific, COVID‐19, graduated frequency, high‐intensity drinking, national alcohol survey, panel survey
Longitudinal follow‐up in early 2021 of 2019 drinking measures found particularly large increases in drinking and alcohol use disorders for African Americans, women and those aged 35–49. In contrast, reduced drinking and heavy drinking prevalence was found among men and White respondents. Increases in alcohol consumption occurred through increased prevalence of drinking, particularly for spirits, rather than increases in average amounts per occasion. Substantial increases in DSM‐5 moderate to severe alcohol use disorders are a novel finding of particular concern.
INTRODUCTION
The COVID‐19 pandemic has affected the United States since March 2020 with about 380,000 COVID‐19 deaths and an estimated 522,000 excess deaths occurring in 2020 (Woolf et al., 2021). Significant economic and social impacts occurred in all states with an initial steep rise in the unemployment rate followed by a slower and incomplete recovery, as well as particularly large impacts on reduced labor force participation by women (Albanesi & Kim, 2021). Compared to 2019 rates, ED visits for disaster‐associated mental health conditions, suicide attempts, and drug overdoses increased (Holland et al., 2021). This mortality, economic, and health impacts have disproportionately affected African American, Hispanic, and Native American communities and other vulnerable groups (Karmakar et al., 2021; Okonkwo et al., 2021). Many Americans were also essential workers who were required to work in grocery, food service, shipping, and health care settings throughout the period.
In the early months of the pandemic, many states instituted stay‐at‐home orders, and office closures for nonessential businesses, school closures, and restaurant, bar, and other public, indoor gathering space closures continued into 2021 in many places (Chernozhukov et al., 2021). Alcohol policy changes included the closing of bars for long periods in some states and periodically in others, reduced or prohibited indoor dining at restaurants, and cancellation of most large events through 2020. However, most off‐premise retail alcohol outlets remained open throughout 2020 and many states allowed new or expanded alcohol delivery and to‐go drinks from bars and restaurants. Data from government‐controlled states on spirits sales show an increase of 6.6% in 9‐L cases for April 2020 through March 2021 from the prior 1‐year period (personal communication from National Alcohol Beverage Control Association). This included both on‐ and off‐premise sales. Yet, there was wide state variability, with declines in a few states (such as Pennsylvania, where retail stores closed temporarily in the early months of the pandemic) and large increases in others (such as Mississippi, where sales rose by 19%). Data on state alcohol sales for March through December 2020 provided by the National Institute on Alcohol Abuse and Alcoholism for 12 states also indicate an increase in spirits sales compared to the 2017 to 2019 average for the same months (National Institute on Alcohol Abuse & Alcoholism, 2021). Changes in wine sales were more variable, with declines in 3 of 10 months and increased sales overall; beer sales declined in 7 of the 10 months. Nielsen household data on alcohol sales expenditures also show increased retail sales after April 2020 for all beverage types, with a particularly large increase for spirits (Lee et al., 2021).
Survey studies of drinking during the pandemic have primarily relied on retrospective self‐report (Barbosa et al., 2021; Pollard et al., 2020), which has been validated against longitudinal data in one study (Minhas et al., 2021), and most have not included detailed measures of alcohol use patterns, including beverage‐specific consumption, needed to comprehensively understand shifts in drinking behaviors. Despite these methodological limitations, certain key findings have emerged. First, both general and subgroup‐specific increases in alcohol consumption and risky drinking have been established (Weerakoon et al., 2021). These findings appear robust, and replicated in studies with a variety of designs, including convenience samples (Capasso et al., 2021; French et al., 2020; Grossman, Benjamin‐Neelon, et al., 2020) and more rigorous web panel samples (Barbosa et al., 2021; Pollard et al., 2020).
Second, subgroups showing differential increases in drinking include women and people of color. For example, a commercial panel study comparing a retrospective assessment of prepandemic drinking in February to drinking in April 2020 found a 29% increase in alcohol volume, as well as increased prevalence of binge drinking and exceeding NIAAA recommended limits, with larger effect sizes among women and Black respondents (Barbosa et al., 2021). A study of adults aged 30 to 80 from the RAND American Life Panel found a 14% increase in drinking days for those aged 30 to 59 and an increase in 4+ drinking days and alcohol problems among women aged 30 to 59 from 2019 to early June 2020 (Pollard et al., 2020). However, most young adults’ reported decreased alcohol use in the early phase of the pandemic (e.g., through April 2020; Graupensperger et al., 2021).
The current study will be one of the first to utilize longitudinal data from a representative sample of US adults to evaluate multifaceted changes in drinking patterns and alcohol use disorders (AUDs) prior to the pandemic. Data are drawn from the 2019 to 2020 National Alcohol Survey (NAS; termed N14 as it is the 14th in the NAS series) and the associated follow‐up survey covering the period from April 2020 to January/February 2021, the 2021 NAS COVID‐19 Survey (N14C). Both used identical measures to assess alcohol consumption, including detailed drinking pattern assessments (the combined beverage Graduated Frequency measure and three beverage‐specific quantity and frequency measures) as well as a DSM‐5 AUD symptom scale. This permits quantification of changes in overall and beverage‐specific drinking patterns and uses disorders for the population and for subgroups defined by gender, age, and race/ethnicity. Based on alcohol sales data and prior studies using survey data, we hypothesized there would be an increase in drinking frequency and volume, including increases in spirits and wine, but not beer, consumption volume. We also expected to find larger increases in drinking volume for African Americans and women. The contribution of this study lies in the methodological rigor, attention to sub‐group changes, and the coverage of beverage‐specific consumption and alcohol problems, which have remained understudied to date.
METHODS
Data
Data for the current study are from the latest wave of the cross‐sectional adult National Alcohol Survey (N14 hereafter) and a COVID‐19 follow‐up survey (N14C hereafter) of N14 participants who consented to be re‐contacted. The N14 data collection was conducted from February 2019 to April 2020 (02 to 09/2019 pilot phase, 09/2019 to 04/2020 full‐scale data collection) by the Alcohol Research Group (Reif et al., 2022). We note that there were 158 interviews conducted after March 17, 2020, when a national alert on COVID‐19 was issued, and sensitivity analyses removing these cases were compared to the presented results.
The N14 was a population‐based survey of US noninstitutionalized adults 18 years of age or older, with a sampling frame representing 50 states and the District of Columbia. The N14 survey used two probability samples including (1) a random‐digit‐dialed (RDD) cell phone telephone sample and (2) an address‐based sample (ABS). These probability samples were supplemented with (3) a nonprobability sample was drawn from a prerecruited web panel (not included here, as respondents were not permitted by the panel provider to opt into the follow‐up study). Interviews were conducted via telephone for the RDD sample and via a web questionnaire for all others, both available in English and Spanish. Telephone respondents received a $15 or $25 Amazon.com gift code for completing the interview, depending on whether they were in an over‐sample area (see below).
The data collection protocol for the ABS‐push‐to‐web sample involved three successive contacts: (1) an invitation letter with details for taking the Web survey, (2) a reminder postcard, and (3) a final reminder letter; the ABS respondents received a $1 in the invitation letter and a $20 Amazon.com gift code for completing the survey. The RDD and ABS samples were stratified into minority and nonminority areas, with minority strata defined as census blocks with 40% or more of the population identified as Black/African American or Hispanic/Latinx. Minority strata were oversampled to increase representation among these demographic groups. The average interview duration was 40 min for the RDD interview and 36 min for the web survey. The N14 probability sample with completed data includes 1326 from the RDD telephone sample and 5184 from the ABS sample. The American Association for Public Opinion Research (AAPOR) COOP4 cooperation rate (The American Association for Public Opinion Research, 2011) for the combined RDD and ABS samples was 42.2%.
Of the 6510 N14 respondents recruited via ABS or RDD, 3146 (48.3%) agreed to be re‐contacted and were included in the N14C sample, with 2416 eligible from the ABS and 730 from the RDD sample. Starting on Januaury 28, 2021, all eligible respondents with a valid address were mailed an invitation letter with a $1 cash preincentive offering the opportunity to participate in the web survey, followed by reminder postcards as well as invitation/reminder emails or text messages. Respondents who completed the questionnaire were provided with a $10 Amazon.com gift code at the end of the web questionnaire. The N14C data collection began on January 30, 2021 and concluded on March 28, 2021, with 1819 completed interviews (57.8% response rate). The fieldwork of both N14 and N14C was implemented under contract by ICF, Inc., of Fairfax Virginia.
Measures
Drinking and alcohol problem measures in N14
All major drinking and alcohol problem measures at baseline follow the NAS tradition using the last 12‐month time frame. Current drinker status is defined by whether the respondent had any alcohol during the last 12 months before the interview (Midanik & Greenfield, 2003). All respondents were asked a usual frequency question “thinking of your overall drinking in the last 12 months, how often do you usually have any kind of beverage containing alcohol.” Those who answered “more than once a day,” “once a day” or “nearly every day” were included in Daily drinking.
All current drinkers were then asked the Graduated Frequency (GF) series (Greenfield, 2000; Greenfield et al., 2009) for all beverages combined, on which a number of volumes and heavy drinking measures are based. Following a 12‐month maximum item (Greenfield et al., 2006) determining entry level for the GF series, frequencies of consuming (if the level is relevant) 12 or more, 8 to 11, 5 to 7, 3 to 4 (3 and 4 drinks asked separately for women), and 1 to 2 drinks of any kind of alcohol beverage during the last 12 months were elicited and coded as 14, 9.5, 6.0, 3.5 (3 and 4 for women), and 1.5 drinks, respectively. These volume levels and their associated frequency of use, ranging from “every day or nearly every day” to “once in the last 12 months” were multiplied and summed to calculate the total number of drinks consumed in the last 12 months for the measure of GF volume. Additionally, based on the above GF series drinking levels, GF volume was further subdivided into volumes derived from 1 to 2 drinks, 3 to 4 drinks, and 5+ drinks. Further, Any 5+ drinking is defined as having five or more drinks at least once in a day during the last 12 months. The GF volume and the 12‐month maximum items were also used to define risky drinking as reporting more than 14 drinks weekly on average or 5 or more on any day during the last year for men, and more than 7 drinks weekly or 4 or more on any day for women.
A separate series of questions on beverage‐specific alcohol consumption also was included in the NAS survey. Using the same format as the usual frequency described above, the respondents were also asked how often they consumed (separately) wine, beer, and spirits during the last 12 months, and the corresponding typical quantity question “on those days when you drink wine/beer/spirits, how many drinks do you typically have.” The usual frequency response was coded to the number of days wine/beer/spirits were consumed, ranging from 0 to 365. The usual frequency days and the typical number of drinks consumed for each beverage were multiplied to derive wine, beer, and spirits volumes separately, which were then summed to yield the total alcohol volume.
Finally, N14 current AUD criteria were based on the DSM‐5 definition (American Psychiatric Association, 2013) for the last 12 months. The AUD scale includes symptoms in eleven domains: hazardous use, failure to fulfill major obligations, interpersonal problems, tolerance, withdrawal, drinking more than intended, unsuccessful efforts to control use, giving up pleasures or interests to drink, spending a great deal of time in drinking, continued use despite problems and craving. Mild AUD is defined as reporting symptoms in 2 or 3 domains, and moderate or severe AUD is defined as reporting symptoms in 4 or more domains.
Drinking and alcohol problem measures in N14C
All drinking and AUD measures in the N14C survey used the same format of questions as in N14, the only change being the reference timeframe. For all questions with a past 12‐month timeframe in N14, the respondents in the follow‐up survey were asked about the period “since April 1, 2020.” Thus, current drinking in N14C was defined as having any alcohol from April 1, 2020 to the interview date, ranging from 10 to 12 months for N14C respondents. This slightly shortened timeframe for the follow‐up survey (to indicate drinking and problems during the COVID‐19 pandemic period) could affect the AUD measures as this allows less time for criteria to be fulfilled. However, drinking measures should be minimally affected, given that the 12‐month timeframe coding was still applied.
Socio‐demographic and COVID‐19 impact measures
Socio‐demographic measures of gender, age, race/ethnicity, and highest education achieved were only collected at baseline. Family income and marital status information were collected at both baseline and follow‐up. A series of COVID‐19 impact measures were collected in the N14C survey, asking the respondents how the COVID‐19 pandemic has changed various aspects of their life since April 1, 2020. These questions include whether the respondent or an immediate family member (separately) had been diagnosed with COVID‐19, whether the respondent or someone in the household was an essential worker, whether the respondent or someone in the household had been laid off or unemployed or had hours or pay reduced at work. The respondent also was asked whether the household experienced difficulty paying rent or mortgage, whether the respondent had been occasionally or frequently without enough or good quality food, and whether access to extended family and trusted friends had experienced moderate or severe changes since April 1, 2020.
Data analysis
Analyses compare drinking and related problems for the pre‐Covid‐19 period as reported in the N14 survey with the pandemic period as reported in the N14C survey. Drinking outcomes are divided into two groups for both baseline and follow‐up: dichotomous measures (e.g., current drinkers, risky drinking, etc.) for which the percent prevalence is presented, and continuous measures (e.g., average volume from GF, average volume from wine, beer, spirits, etc.) for which both samples means and standard errors are presented. To test differences in drinking outcomes between the baseline and follow‐up surveys, generalized estimating equation (GEE) models are fit to predict drinking outcomes using a time indicator (0 = baseline, 1 = follow‐up), with its coefficient estimate indicating whether there are significant differences between pre‐ and during‐Covid‐19 drinking and AUD. The GEE model accounts for within‐person correlation and survey sampling weights (described below). For dichotomous outcomes, a logistic model is used; for continuous outcomes, a Poisson model is fit, along with robust random errors used in statistical inference to adjust for potential downward bias in (nonrobust) standard errors in the presence of over‐dispersion (Cameron & Trivedi, 2013). As a sensitivity analysis, a linear model also was fit for continuous measures, with results very similar to the Poisson models (results available upon request). All pre‐ and during‐Covid‐19 comparison analyses were conducted for the total N14C sample, then for groups defined by gender, age (18 to 34, 35 to 49, and 50+), and race/ethnicity (non‐Hispanic White, Non‐Hispanic Black, and Hispanic), separately. Power considerations allowed three age groups that were based on substantively meaningful cut‐points with relatively similar sample sizes across groups. Preliminary analyses considered a 35 to 54 group, but the 35 to 49 group highlights the largest increases in drinking and problem measures. To formally test whether pre‐ and during‐Covid‐19 drinking differences significantly varied by subgroup, the demographic group indicator and its interaction with time were entered in the GEE model. Significant interactions suggest differences in drinking are significant between two groups (men vs. women; age 34 to 49 or 50+ vs. age 18 to 34 as reference; Black or Hispanic vs. White as reference). While a large number of statistical tests were conducted across drinking outcomes and by demographic subgroups multiple comparison adjustments were not made. Adjusting p‐values to account for multiple comparisons, despite advantages in reducing type‐I error, has been criticized for reasons including sacrificing power and difficulty in defining a number of tests and selecting the best adjustment approach (Feise, 2002; Rothman, 1990). Particularly, an adjustment may not be desirable for exploratory studies (Althouse, 2016) like the current analysis. Readers should always be aware that significant results are subject to errors of chance and need to be considered together with the magnitude of the effect size.
All analyses were performed in STATA, (StataCorp, 2019) applying sampling weights. Construction of N14C sampling weights started with the basic design weights for all N14 ABS and RDD respondents. These basic weights account for the initial disproportionate probability of selection caused by a number of telephone lines in a household (RDD) and the number of eligible adults in a household (RDD and ABS), and adjustment for oversampling of high‐density minority strata (for both RDD and ABS frames). Next, adjustments for nonresponse specific to N14C were made in two steps: (1) agreeing to be contacted for a follow‐up survey and (2) completing the follow‐up survey. A propensity score (PS) model was fit to adjust for the two stages of nonresponse/attrition sequentially. For the first stage, N14 respondents who lived in the South, were in the CATI sample, were infrequent spirits drinkers and had worse general health were more likely to agree to be contacted. At the second stage, participants who were successfully followed were statistically more likely to be female, have higher levels of education, report being married or cohabitating, report past‐year spirits drinking, were in the ABS sample and report a higher quality of life than those who were eligible and not included in N14C. Race/ethnicity, wine drinker, and beer drinker were not significant in either model. PS stratification was conducted by grouping PS into quintiles and ratio‐adjusting respondents to the total within each quintile. As the final weighting step, we poststratified the weighted N14C sample into demographic categories and ratio‐adjusted the weights, so that the final weighted sample matched the population with those demographic characteristics from the most recent American Community Survey. A raking algorithm iteratively calibrated with the weighted sample to match the population on the dimensions of gender by age, region, gender by race/ethnicity, age by race/ethnicity, education, and gender by marital status.
RESULTS
Table 1 shows the socio‐demographic representativeness of the weighted sample and highlights substantial COVID‐19 impacts. We present these selected COVID‐19 impacts here to illustrate the degree to which the sample experienced these relevant changes in drinking patterns and problems. More detailed results and statistical tests of comparisons between subgroups and the modeling of relationships between impacts and alcohol outcome measures are addressed in separate analyses. About 11% of the sample reported having COVID‐19 infection, with an additional 20% who reported having an immediate family member who was ill. More than half of the sample had an essential worker in their household, and more than half felt that their access to family and friends was moderately or severely changed. About a third of households had difficulty paying housing costs or had at least one member who lost a job and/or had reduced pay.
TABLE 1.
Demographics and COVID‐19 impacts for the NAS2019‐20 N14C follow‐up sample (weighted %)
| Total (n = 1819) | Men (n = 636) | Women (n = 1182) | |
|---|---|---|---|
| Gender male | 48.3% | – | – |
| Age group | |||
| 18 to 34 | 29.3 | 30.5% | 28.1% |
| 35 to 49 | 24.9 | 25.2 | 24.6 |
| 50+ | 45.9 | 44.3 | 47.3 |
| Race/ethnicity group | |||
| White | 64.4 | 65.0 | 63.9 |
| Black | 12.6 | 11.8 | 12.3 |
| Hispanic | 14.7 | 14.8 | 14.5 |
| Other | 8.4 | 8.4 | 8.4 |
| Education group | |||
| HS grad or less | 28.8 | 27.2 | 30.3 |
| Some college | 39.4 | 39.6 | 39.3 |
| College grad | 31.8 | 33.3 | 30.5 |
| Family income a | |||
| ≤$20 k | 17.8 | 16.5 | 19.4 |
| $20,001 to 40 k | 20.5 | 17.9 | 22.9 |
| $40,001 to 60 k | 23.0 | 23.6 | 22.4 |
| $60,001 to 80 k | 13.0 | 14.0 | 12.1 |
| >$80 k | 25.5 | 28.1 | 23.2 |
| Marital status a | |||
| Married/cohabit | 58.4 | 60.5 | 56.4 |
| Separated/divorced | 15.3 | 12.8 | 17.7 |
| Widowed | 5.0 | 2.8 | 7.2 |
| Never married | 21.3 | 24.0 | 18.8 |
| Respondent had COVID‐19 | 10.6 | 10.4 | 10.7 |
| Immediate family had COVID‐19 | 30.5 | 29.7 | 31.2 |
| Someone in household essential worker | 52.1 | 50.7 | 53.5 |
| Someone in household lost job | 31.8 | 31.5 | 32.2 |
| Someone in household had reduced pay | 35.0 | 35.1 | 34.9 |
| Had difficulty paying rent or mortgage | 36.1 | 35.3 | 36.9 |
| Occasionally/frequently without enough food | 8.2 | 6.3 | 10.1 |
| Access to extended family or friends was moderately/severely changed | 55.0 | 54.8 | 55.2 |
Baseline measures.
The results of analyses comparing alcohol measures from the pre‐COVID‐19 period assessment to the COVID‐19 period assessment are shown in Table 2 for the full sample and for men and women separately. Overall results indicate increased alcohol use, with significantly greater wine and spirits drinking days and volume, as well as total volume from the beverage‐specific measures. At the same time, there were also significant reductions in the prevalence of any drinking, risky drinking, and having any 5+ days. Importantly, however, large and significant increases were found for the prevalence of daily drinking and for moderate/severe AUD. This concentration of drinking, with fewer participating but increases among those who continue to drink, is particularly found among men, as women show small and nonsignificant changes in the prevalence of any and heavy drinking. Increases in drinking frequency and volume are generally similar for both genders, with the exceptions of wine volume and volume from days consuming 1 to 2 drinks, which are only significant for women. Further, the significant increase in moderate or severe AUD is only significant for women. Additional posthoc analyses were conducted to examine the eleven AUD symptom domains separately. Significant increases were found for seven of them: failure to fulfill major obligations (0.9% to 2.0%, p = 0.017), interpersonal problems (2.5% to 4.4%, p = 0.002), drinking more than intended (5.2% to 7.1%, p = 0.023), unsuccessful efforts to control use (1.6% to 3.2%, p < 0.001), giving up pleasures or interests to drink (1.7% to 2.6%, p = 0.027), spending a great deal time in drinking (1.1% to 2.0%, p = 0.011), and craving (2.1% to 3.5%, p = 0.040).
TABLE 2.
Comparison of alcohol consumption and alcohol use disorders across pre‐ and post‐COVID‐19 period for total sample and by gender
| Total (n = 1819) | Men (n = 636) | Women (n = 1182) | ||||
|---|---|---|---|---|---|---|
| Pre‐COVID | Post‐COVID | Pre‐COVID | Post‐COVID | Pre‐COVID | Post‐COVID | |
| Drinking measures in % | ||||||
| Current drinker a | 72.7% | 70.1%* | 74.1% | 69.2%** | 71.3% | 70.9% |
| Risky drinking | 29.6 | 25.8* | 29.1 | 23.9* | 30.0 | 27.7 |
| Any 5+ | 21.9 | 19.2* | 27.2 | 22.1* | 17.1 | 16.4 |
| Daily drinking | 6.3 | 9.6** | 6.7 | 10.6** | 5.9 | 8.8** |
| AUD mild | 5.1 | 6.0 | 5.7 | 6.6 | 4.4 | 5.4 |
| AUD moderate/severe | 2.3 | 3.9** | 2.6 | 4.1 | 2.0 | 3.6** |
| Alcohol consumption in mean (SE) | ||||||
| Graduated frequency measures | ||||||
| GF volume | 176.8 (13.7) | 202.1 (14.2) | 191.0 (23.3) | 218.1 (23.9) | 163.6 (15.0) | 187.2 (15.9) |
| Volume from 1 to 2 drinks | 55.5 (3.4) | 63.0 (3.7)* | 63.4 (5.4) | 66.0 (5.8) | 48.1 (4.1) | 60.3 (4.7)** |
| Volume from 3 to 4 drinks | 49.0 (4.8) | 52.4 (5.3) | 38.0 (4.8) | 44.6 (6.6) | 59.4 (8.0) | 59.8 (8.3) |
| Volume from 5+ drinks | 72.3 (11.6) | 86.6 (11.9) | 89.6 (21.4) | 107.5 (21.2) | 56.1 (10.2) | 67.2 (11.8) |
| Beverage‐specific QF measures | ||||||
| Beer drinking days | 23.3 (1.7) | 24.3 (1.9) | 30.9 (2.9) | 30.3 (3.1) | 16.1 (1.8) | 18.8 (2.1) |
| Beer volume | 68.8 (6.4) | 75.3 (7.4) | 88.8 (10.6) | 93.5 (11.5) | 50.1 (7.6) | 58.4 (9.5) |
| Wine drinking days | 23.9 (1.6) | 27.2 (1.8)* | 21.5 (2.3) | 24.8 (2.8) | 26.2 (2.3) | 29.3 (2.3) |
| Wine volume | 48.7 (3.7) | 64.4 (6.7)** | 45.3 (5.4) | 60.9 (11.8) | 52.0 (5.1) | 67.7 (6.7)** |
| Spirits drinking days | 17.4 (1.6) | 23.5 (2.3)** | 20.1 (2.3) | 26.7 (3.4)** | 14.9 (2.3) | 20.4 (3.1)** |
| Sprits volume | 45.5 (5.1) | 67.7 (8.6)** | 53.2 (7.5) | 77.9 (13.2)** | 38.4 (7.0) | 58.2 (11.1)* |
| Total volume wine/beer/spirits | 162.9 (10.4) | 207.3 (14.8)** | 187.4 (16.4) | 232.2 (24.4)** | 140.1 (13.1) | 184.1 (17.3)** |
*p < 0.05, **p < 0.01, pre‐ and post‐COVID comparison.
Significant interaction (p < 0.05) between men and women on change in drinking.
Dividing the sample into three age groups illustrates differences in changes across age, as shown in Table 3. The youngest group aged 18 to 34 has the largest and only significant reductions in risky and 5+ drinking, but also large and significant increases in daily drinking prevalence and spirits drinking days, indicating a concentration of drinking in this population. Still, the largest increases are seen in the 35 to 49 age group, with significantly increased volume on both the GF‐ and beverage‐specific total volume measures, and on the wine and spirits frequency and volume measures. Of particular concern for this group of adults in middle adulthood are findings of an 82% increase in alcohol volume from 5+ drinking days and a 62% increase in the prevalence of moderate or severe AUD. A significant reduction in any drinking was found for the 50 and older age group, along with an increase in daily drinking. Spirits use frequency and volume of drinks were also found to increase significantly for those 50 and older. We have presented the patterns of change in drinking focusing on specific subgroups to facilitate interpretation. For comparison across groups, we acknowledge that one subgroup showing significant results while the other does not may suggest the interaction between the two groups is significant, while in many cases they are not as tests of interactions are generally less powerful and the nonsignificant changes are often in the same direction. Significant results between subgroups (e.g., 35 to 49 and 50+ vs. 18 to 34) are indicated in the tables and full interaction effects are shown in Tables S1–S3.
TABLE 3.
Comparison of alcohol consumption and Alcohol Use Disorders pre‐ and post‐COVID by age group
| 18 to 34 (n = 573) | 35 to 49 (n = 525) | 50+ (n = 721) | ||||
|---|---|---|---|---|---|---|
| Pre‐COVID | Post‐COVID | Pre‐COVID | Post‐COVID | Pre‐COVID | Post‐COVID | |
| Drinking measures in % | ||||||
| Current drinker | 75.9% | 76.0% | 74.5% | 71.1% | 69.5% | 65.8%* |
| Risky drinking | 40.6 | 34.1* | 33.5 | 32.1 | 20.4 | 17.2 |
| Any 5+ | 33.1 | 26.7** | 25.1 | 25.7 | 13.1 | 10.8 |
| Daily drinking | 4.1 | 8.2** | 6.7 | 9.8 | 7.4 | 10.5** |
| AUD mild | 8.1 | 8.4 | 5.9 | 5.7 | 2.7 | 4.6 |
| AUD moderate/severe | 4.4 | 6.3 | 1.8 | 4.7** | 1.2 | 1.8 |
| Alcohol consumption in mean (SE) | ||||||
| Graduated frequency measures | ||||||
| GF volume a | 222.5 (33.0) | 208.7 (27.1) | 168.5 (18.8) | 247.2 (26.3)** | 152.2 (18.3) | 173.5 (21.1) |
| Volume from 1 to 2 drinks | 49.5 (4.7) | 57.7 (5.9) | 58.8 (6.0) | 65.4 (6.7) | 57.5 (5.8) | 65.2 (6.2) |
| Volume from 3 to 4 drinks a | 55.4 (7.2) | 44.7 (6.3) | 51.6 (6.9) | 76.3 (10.9)* | 43.6 (8.6) | 44.4 (9.2) |
| Volume from 5+ drinks a | 117.6 (30.9) | 106.3 (25.7) | 58.1 (13.0) | 105.5 (19.4)** | 51.0 (14.0) | 63.8 (17.2) |
| Beverage‐specific QF measures | ||||||
| Beer drinking days | 26.3 (2.9) | 26.9 (3.8) | 27.5 (4.2) | 29.3 (4.0) | 19.0 (2.3) | 20.0 (2.4) |
| Beer volume | 86.4 (13.5) | 90.8 (16.0) | 76.6 (12.2) | 99.0 (16.0) | 53.4 (8.8) | 52.6 (8.9) |
| Wine drinking days | 19.5 (2.1) | 22.2 (2.3) | 20.5 (2.5) | 28.6 (3.7)* | 28.6 (3.0) | 29.5 (3.1) |
| Wine volume | 43.1 (5.4) | 50.9 (6.1) | 48.8 (8.5) | 75.9 (11.3)** | 52.3 (5.7) | 66.8 (12.6) |
| Spirits drinking days | 14.1 (1.7) | 20.6 (3.8)* | 19.5 (2.5) | 28.4 (4.7)* | 18.4 (3.1) | 22.6 (3.5)** |
| Sprits volume | 44.8 (7.0) | 62.6 (15.9) | 50.2 (8.0) | 98.9 (21.1)** | 43.5 (9.2) | 54.0 (10.6)* |
| Total volume wine/beer/spirits | 174.1 (19.1) | 204.2 (26.2) | 175.0 (19.4) | 273.8 (34.4)** | 149.2 (16.0) | 173.3 (20.2) |
*p < 0.05, **p < 0.01, pre‐ and post‐COVID comparison.
Significant interaction (p < 0.05) between 18 to 34 and 35 to 49 on change in drinking.
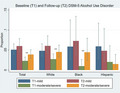
Analyses for the largest US racial/ethnic subgroups are presented in Table 4, illustrating different patterns of change in each group. Hispanic respondents had no significant changes in any of the drinking measures. The largest changes were seen for Black respondents, with significant increases in all of the alcohol volume and frequency measures with the exception of beer drinking days. Large increases also were found in the prevalence of daily drinking and moderate or severe AUD. White respondents displayed the same pattern of increased concentration as seen in the overall results, with more drinking among fewer drinkers. Tests of differences in changes between Black and White populations confirmed larger increases among Black respondents.
TABLE 4.
Comparison of alcohol consumption and alcohol use disorders pre‐ and post‐COVID by race/ethnicity group a
| White (n = 1105) | Black (n = 307) | Hispanic (n = 228) | ||||
|---|---|---|---|---|---|---|
| Pre‐COVID | Post‐COVID | Pre‐COVID | Post‐COVID | Pre‐COVID | Post‐COVID | |
| Drinking measures in % | ||||||
| Current drinker b , c | 74.4 | 69.5** | 71.9 | 72.7 | 70.0 | 74.4 |
| Risky drinking | 29.1 | 25.3* | 28.9 | 24.9 | 33.6 | 32.0 |
| Any 5+ | 21.5 | 18.6* | 24.2 | 17.9 | 21.9 | 24.6 |
| Daily drinking | 6.9 | 10.8** | 3.1 | 8.1* | 8.1 | 7.6 |
| AUD mild | 4.8 | 6.0 | 5.9 | 7.3 | 5.9 | 4.8 |
| AUD moderate/severe | 2.7 | 4.5** | 1.0 | 4.4** | 2.0 | 1.5 |
| Alcohol consumption in mean (SE) | ||||||
| Graduated frequency measures | ||||||
| GF volume a | 186.1 (17.3) | 206.0 (18.6) | 133.2 (18.7) | 262.6 (42.4)** | 168.0 (31.7) | 172.9 (33.3) |
| Volume from 1 to 2 drinks a | 62.7 (4.5) | 67.4 (4.8) | 31.3 (3.9) | 58.8 (9.0)** | 48.6 (9.5) | 48.6 (8.8) |
| Volume from 3 to 4 drinks a | 45.6 (4.4) | 48.3 (5.2) | 38.5 (6.8) | 75.8 (18.2)* | 80.7 (24.3) | 62.7 (22.8) |
| Volume from 5+ drinks | 77.9 (15.1) | 90.2 (16.7) | 63.4 (13.8) | 128.0 (32.8)* | 38.7 (12.3) | 61.6 (20.0) |
| Beverage‐specific QF measures | ||||||
| Beer drinking days | 24.9 (2.0) | 26.2 (2.3) | 16.3 (3.7) | 25.4 (5.8) | 23.8 (6.3) | 15.7 (2.7) |
| Beer volume | 77.9 (9.0) | 83.0 (10.3) | 42.9 (9.0) | 71.9 (16.9)* | 67.1 (16.1) | 55.2 (12.5) |
| Wine drinking days a | 27.2 (2.2) | 28.7 (2.3) | 16.7 (2.9) | 33.6 (5.7)** | 20.1 (3.9) | 19.9 (4.2) |
| Wine volume a | 53.6 (5.0) | 68.9 (9.6)* | 34.3 (6.1) | 83.9 (15.1)** | 50.3 (10.8) | 45.2 (9.7) |
| Spirits drinking days | 17.9 (1.7) | 21.9 (2.4)** | 17.6 (3.4) | 30.2 (5.9)** | 17.4 (7.3) | 24.4 (9.0) |
| Sprits volume | 45.3 (5.5) | 59.6 (9.3)* | 47.8 (11.5) | 104.8 (24.3)** | 50.9 (21.9) | 86.8 (35.0) |
| Total volume wine/beer/spirits a | 176.6 (13.5) | 211.3 (18.5)* | 124.9 (18.5) | 260.6 (48.0)** | 168.0 (33.5) | 186.9 (39.1) |
*p < 0.05, **p < 0.01, pre‐ and post‐COVID comparison.
“Other” racial and ethnic groups who are neither White, Black or Hispanic were excluded from the analysis.
Significant interaction (p < 0.05) between White and Black groups on change in drinking.
Significant interaction (p < 0.05) between White and Hispanic groups on change in drinking.
Sensitivity analyses were performed excluding the 158 respondents whose N14 baseline interview was on March 17, 2020 or later, when the US public received the first COVID‐19 national alert. The results essentially remained the same. For the White respondents, differences in any 5+, wine and spirits volume, and total volume from all beverages that had been significant at the 0.05 level became marginally significant (p < 0.10), but the direction of change stayed the same. Note that this change in statistical significance may be due to the reduction in sample size rather than a change in the magnitude of difference. For example, the mean wine volume in Table 4 was 53.6 versus 68.9 drinks pre‐ and during the COVID‐19 period, respectively, and in the sensitivity analysis it was 53.3 versus 68.8 drinks, respectively. Separately, sensitivity analyses removing 251 respondents from the N14 RDD telephone sample were estimated with consistent results. Further, the issue of seasonal effects on alcohol consumption was considered in the comparison of N14 respondents across three periods: February to August 2019, September to December 2019, and January to April 2020. No significant seasonal differences were observed. For example, mean volume from the GF series was 182.4, 200.8, and 212.2 (p = 0.359) for the three groups respectively, and mean beverage‐specific volume was 193.5, 206.4, and 213.9 (p = 0.650).
DISCUSSION
The N14C follow‐up study is unique in assessing detailed alcohol use patterns and AUD symptom measures in the same individuals for comparable periods prior to and during the COVID‐19 pandemic. Our longitudinal survey highlights particularly large increases in drinking and AUD for African Americans and women, reduced drinking and heavy drinking prevalence among men and White respondents, and a concentration of increased drinking and AUD among those aged 35 to 49. Our results further show increases in alcohol use were driven by increases in drinking frequency overall, spirits consumption overall, and wine consumption among women. Significant increases in moderate/severe AUD involved increases in seven of the eleven AUD symptom domains, suggesting changes along with a variety of pathways including interpersonal, control, and physiological criteria. It will be essential to monitor whether interpersonal problems caused by alcohol are short‐term and resolve as the pandemic subsides, as well as whether cravings and uncontrolled use continue long‐term. These results confirm prior findings of overall increases and subgroup‐specific changes, and, importantly, provide more detail on the patterns of change across major socio‐demographic subgroups. Both alcohol sales studies and population surveys have consistently indicated that alcohol consumption in the United States rose during the 2020 COVID‐19 pandemic period. Key findings of prior studies include increased alcohol sales, and of spirits especially, (Castaldelli‐Maia et al., 2021; National Institute on Alcohol Abuse & Alcoholism, 2021), and survey data suggest an increased frequency of drinking occasions as the main source of increased consumption, with the largest increases among women and African Americans (Barbosa et al., 2021).
Increases in drinking during the pandemic in the United States appear to have built on observed trends in alcohol use, which should be considered in evaluating changes (Jager & Keyes, 2021). Prior to 2020, per capita apparent alcohol consumption in the United States had generally been increasing for over 20 years after earlier reductions from the 1970s and early 1980s epoch, with increases in wine and spirits along with declines in beer sales (Martinez et al., 2019; Slater & Alpert, 2021). This overall increase has occurred despite substantial declines in underage drinking and binge drinking (Jang et al., 2017; Ng Fat et al., 2018), and has been driven in part by increasing heavy drinking among middle‐aged and older adults (Breslow et al., 2017; Grucza et al., 2018; Han et al., 2017). Women, African Americans, and those in lower educational attainment groups have also been found to have had notable increases over the past several years and decades (Dawson et al., 2015; Grant et al., 2017; Grucza et al., 2018; Keyes et al., 2019). These increases in drinking have been accompanied by even larger increases in alcohol‐related morbidity (Moon et al., 2020; White et al., 2018) and mortality for middle and older age groups, (Spillane et al., 2020; White et al., 2020) indicating the salient health consequences of chronic heavy drinking at these ages. Changes in alcohol use during the COVID‐19 crisis appear to have accelerated existing trends with the largest pre–post increases occurring in the age, gender, and race/ethnicity, subgroups already experiencing increases in alcohol use, and spirits accounting for the largest share of increased use.
Increases in drinking during the 2020 pandemic period occurred mainly through increased frequency of drinking. This suggests that reductions in commuting, travel, and social and recreational activities allowed more time for drinking with reduced constraints, such as the need to drive between activities, and was aided by having more time at home. Changes in alcohol policy allowing increased delivery and to‐go options may also have facilitated increased drinking. While there is limited information from the United States on the impact of alcohol policy changes, a New Zealand survey from April to May 2020 found that 40% of respondents purchased alcohol online, about half of whom were new online purchasers and tended to be heavier drinkers (Huckle et al., 2021).
It is less clear why there were larger increases in drinking and AUD for some groups than others. Drinking among African Americans increased the most dramatically in our sample. Potential explanations include increased trauma and stress associated with events such as the police killings of George Floyd and Breonna Taylor, and the resulting Black Lives Matter protests and counter‐protests, disproportionate COVID‐19 illness and mortality and economic impacts (Millett et al., 2020; Yancy, 2020) and responses to discrimination experiences (Desalu et al., 2019). Pandemic‐specific stress (Grossman, Benjamin‐Neelon, et al., 2020) and general stress appear to be associated with changes in drinking and alcohol problems during the pandemic period. For example, increases in risky drinking in a longitudinal cohort study were associated with racial tension, financial distress, psychological distress and virus‐related stress (Lechner et al., 2021) and web surveys of a Mechanical Turk sample found increasing mean AUDIT scores each month from April to September 2020 in areas with continued lockdown/stay at home orders, but not in those areas without such orders (Killgore et al., 2021). Anxiety and depression—including prior depression (Weerakoon et al., 2021)—also are consistent correlates of increased alcohol consumption during the pandemic (Capasso et al., 2021; Lechner et al., 2021). By contrast, monthly data on the frequency of drinking in the past week collected from March to June 2020 showed increasing drinking frequency in states with relatively lower COVID‐19 incidence, compared to the national median (McKetta et al., 2021).
Findings of no changes in Hispanic drinking were surprising in the context of disproportionate impacts on this group from COVID‐19 illness, mortality, and economic factors. Potentially being home with extended families, reductions in events and parties, higher proportions of essential workers, and reduced incomes were factors in minimal drinking changes. Our findings contribute to the mixed evidence on changes in drinking in the Latinx community during COVID‐19. A cross‐sectional panel survey in the early pandemic period of Spring 2020 reported that the increased or new initiation of substance use (including alcohol and other drugs) was highest among Latinx people compared to all other respondents (36.9% vs. 14.3% to 15.6%) (McKnight‐Eily et al., 2021; Nesoff et al., 2021). Similarly, a longitudinal study assessing substance use early in the pandemic found Latinx respondents reported a higher prevalence of increased substance use to cope with the stress or emotions related to the pandemic (Czeisler et al., 2020). Conversely, a longitudinal study of young adults reported no significant increase in alcohol use among young Latinx adults (Schepis et al., 2021). It is possible that given the extended length of our survey increases in drinking in the early stages of the pandemic were not captured, and that any changes in alcohol use in the Latinx community dissipated as the pandemic progressed (Romm et al., 2021).
Particularly large increases were found among those aged 35 to 49 while reductions in drinking and heavy drinking prevalence were seen for those 18 to 34. The 35 to 49 group may have been most impacted by increased working at home and reductions in other activities including children's activities along with increases in stressors. Those aged 35 to 49 were also found to have experienced the largest effects of economic loss on drinking and problems in a prior study of the Great Recession (Mulia et al., 2014). In the current study, reductions in the prevalence of drinking and 5+ drinking seen among those aged 18 to 34 and men may have been due to hours reductions, closures, and other limitations on bar and restaurant drinking, nightclubs, parties, and other events that are the main contexts for heavy drinking for some drinkers. These contexts are the most utilized by younger drinkers and some do not appear to have substituted home drinking for these.
Our findings also contribute to the international literature on changes in alcohol use during the 2020 COVID‐19 period. Changes in drinking have varied internationally, with some countries showing increased use and problems as has been seen in the United States, but others having reductions or no major changes. For example, a UK panel study of middle‐aged adults found increased drinking and high‐risk drinking (Daly & Robinson, 2021) while studies from Norway and Finland found no changes in alcohol consumption or heavy drinking (Mäkelä et al., 2021). A systematic review of changes in substance use during the pandemic at the population level reported that increases and decreases in alcohol consumption occurred and that certain groups, such as those who were drinking heavily prior to the pandemic and those struggling with mental health problems, were more likely to increase their alcohol and substance use (Schmidt et al., 2021). However, another systematic review of the international literature on alcohol and substance use during the pandemic noted a mixed picture of changes in alcohol use, and a clearer picture of increasing substance use (Roberts et al., 2021). Our findings similarly show that different segments of the population either increased or decreased their alcohol consumption and that these changes varied by demographic subgroup.
The results of this study are subject to limitations. The use of self‐reports might lead to recall and social desirability biases, although the use of most online surveys may have reduced bias normally associated with in‐person surveys. Although our sample was weighted to be representative of the US adult population, biases from selection into the survey sample and attrition may not be fully addressed by weighting. Recall periods also differed between the surveys with 10 or 11 months for N14C compared to 12 months in N14. The use of the same response categories for alcohol use measures adjusts for this difference but measures of accumulated harms, such as AUD, could be biased downward in the shorter period. US alcohol use patterns have a seasonal variation with more drinking in the fall holiday season and more heavy occasions in summer (Cho et al., 2001). Although the use of past year measures may not fully address this issue (Mojica‐Perez et al., 2019), sensitivity analyses of the N14 sample did not indicate seasonal bias in key measures. A strength of this study is the inclusion of two separate alcohol consumption measures with one focused on the frequencies of varying quantities per day, capturing high‐intensity occasions relevant to AUD and acute harms, and the other on beverage‐specific amounts, relevant to alcohol policies and some health outcomes. While both measures showed increases to N14C, only the beverage‐specific measure was significant, perhaps being more sensitive to the increases in spirits consumption.
In conclusion, this population‐level study of changes in alcohol use and problems during the COVID‐19 pandemic confirms previous findings that women and African Americans significantly increased alcohol consumption. Results also contribute important new information regarding increased AUD in middle adulthood, and increases in spirit frequency and volume of drinks in adults 50 years and older. The study additionally highlights concerning increases in alcohol use frequency, volume, and AUDs during 2020. Pattern changes are complex and include the reduced prevalence of drinking in some subgroups, increases in daily drinking, and a particularly large increase in spirits consumption. These drinking pattern details and subgroup‐specific results offer important perspectives relevant to understanding the risk and protective factors for drinking changes occurring during the 2020 and early 2021 phases of the COVID‐19 pandemic in the United States. Ongoing analyses of the N14 and N14C surveys will evaluate predictors of drinking and AUD changes during this period including individual and family COVID‐19 impacts, mental health measures, area characteristics, and alcohol and public health policies. The results of the current study highlight the strong likelihood of harm to health and society that are known to accompany heavy drinking and AUD, and the need to implement effective policy responses including increased taxation and reductions in alcohol availability (Grossman, Kerr, et al., 2020).
CONFLICT OF INTEREST
Content and opinions are those of the authors and do not reflect official positions of the U.S. National Institute on Alcohol Abuse and Alcoholism or the National Institutes of Health. The work of all authors was supported by the U.S. National Institute on Alcohol Abuse and Alcoholism (NIAAA) at the National Institutes of Health (NIH) (grant number P50 AA005595). Drs. Kerr and Greenfield and Ms. Patterson have received funding and travel support from the National Alcoholic Beverage Control Association. Dr. Kerr has been paid as an expert witness regarding cases on alcohol policy issues retained by the Attorney General's Offices of the US states of Indiana and Illinois under arrangements where half of the cost was paid by organizations representing wine and spirits distributors in those states.
Supporting information
Table S1‐S3
Kerr, W.C. , Ye, Y. , Martinez, P. , Karriker‐Jaffe, K.J. , Patterson, D. , Greenfield, T.K. & et al (2022) Longitudinal assessment of drinking changes during the pandemic: The 2021 COVID‐19 follow‐up study to the 2019 to 2020 National Alcohol Survey. Alcoholism: Clinical and Experimental Research, 46, 1050–1061. Available from: 10.1111/acer.14839
REFERENCES
- Albanesi, S. & Kim, J. (2021) The gendered impact of the COVID‐19 recession on the US labor market [Working Paper 28505]. NBER Working Paper Series, National Buerau of Economic Research. [Google Scholar]
- Althouse, A.D. (2016) Adjust for multiple comparisons? It's not that simple. The Annals of Thoracic Surgery, 101, 1644–1645. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders, 5th edition (DSM‐5). American Psychiatric Publishing, Incorporated. [Google Scholar]
- Barbosa, C. , Cowell, A.J. & Dowd, W.N. (2021) Alcohol consumption in response to the COVID‐19 pandemic in the United States. Journal of Addiction Medicine, 15, 341–344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Breslow, R.A. , Castle, I.‐J.‐P. , Chen, C.M. & Graubard, B.I. (2017). Trends in alcohol consumption among older Americans: National Health Interviews Surveys, 1997–2014. Alcoholism: Clinical and Experimental Research, 41, 976–986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cameron, A.C. & Trivedi, P.K. (2013) Regression analysis of count data, 2nd edition. Cambridge University Press. [Google Scholar]
- Capasso, A. , Jones, A.M. , Ali, S.H. , Foreman, J. , Tozan, Y. & Diclemente, R.J. (2021) Increased alcohol use during the COVID‐19 pandemic: the effect of mental health and age in a cross‐sectional sample of social media users in the U.S. Preventive Medicine, 145, 106422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castaldelli‐Maia, J.M. , Segura, L.E. & Martins, S.S. (2021) The concerning increasing trend of alcohol beverage sales in the U.S. during the COVID‐19 pandemic. Alcohol, 96, 37–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chernozhukov, V. , Kasahara, H. & Schrimpf, P. (2021) Causal impact of masks, policies, behavior on early covid‐19 pandemic in the U.S. Journal of Econometrics, 220, 23–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cho, Y.I. , Johnson, T.P. & Fendrich, M. (2001) Monthly variations in self‐reports of alcohol consumption. Journal of Studies on Alcohol, 62, 268–272. [DOI] [PubMed] [Google Scholar]
- Czeisler, M.É. , Lane, R.I. , Petrosky, E. , Wiley, J.F. , Christensen, A. , Njai, R. et al. (2020) Mental health, substance use, and suicidal ideation during the COVID‐19 pandemic – United States, June 24–30, 2020. MMWR, Morbidity and Moxrtality Weekly Report, 69, 1049–1057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daly, M. & Robinson, E. (2021) High‐risk drinking in midlife before versus during the COVID‐19 crisis: longitudinal evidence from the United Kingdom. American Journal of Preventive Medicine, 60, 294–297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dawson, D.A. , Goldstein, R.B. , Saha, T.D. & Grant, B.F. (2015) Changes in alcohol consumption: United States, 2001–2002 to 2012–2013. Drug and Alcohol Dependence, 148, 56–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Desalu, J.M. , Goodhines, P.A. & Park, A. (2019) Racial discrimination and alcohol use and negative drinking consequences among Black Americans: a meta‐analytical review. Addiction, 114, 957–967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feise, R.J. (2002) Do multiple outcome measures require p‐value adjustment? BMC Medical Research Methodology, 2, 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- French, M.T. , Mortensen, K. & Timming, A.R. (2020) Changes in self‐reported health, alcohol consumption, and sleep quality during the COVID‐19 pandemic in the United States. Applied Economics Letters, 29(3), 219–225. 10.1080/13504851.2020.1861197 [DOI] [Google Scholar]
- Grant, B.F. , Chou, P. , Saha, T.D. , Pickering, R.P. , Kerridge, B.T. , Ruan, J. et al. (2017) Prevalence of 12‐month alcohol use, high‐risk drinking, and DSM‐IV alcohol use disorder in the United States, 2001–2002 to 2012–2013: Results from the national epidemiolgic survey on alcohol and related conditions. JAMA Psychiatry, 74, 911–923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graupensperger, S. , Fleming, C.B. , Jaffe, A.E. , Rhew, I.C. , Patrick, M.E. & Lee, C.M. (2021) Changes in young adults’ alcohol and marijuana use, norms, and motives from before to during the COVID‐19 pandemic. The Journal of Adolescent Health, 68, 658–665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenfield, T.K. (2000) Ways of measuring drinking patterns and the difference they make: experience with graduated frequencies. Journal of Substance Abuse, 12, 33–49. [DOI] [PubMed] [Google Scholar]
- Greenfield, T.K. , Kerr, W.C. , Bond, J. , Ye, Y. & Stockwell, T. (2009) Improving graduated frequencies alcohol measures for monitoring consumption patterns: results from an Australian national survey and a US diary validity study. Contemporary Drug Problems, 36, 705–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenfield, T.K. , Nayak, M.B. , Bond, J. , Ye, Y. & Midanik, L.T. (2006) Maximum quantity consumed and alcohol‐related problems: assessing the most alcohol drunk with two measures. Alcoholism: Clinical and Experimental Research, 30, 1576–1582. [DOI] [PubMed] [Google Scholar]
- Grossman, E.R. , Benjamin‐Neelon, S.E. & Sonnenschein, S. (2020) Alcohol consumption during the COVID‐19 pandemic: a cross‐sectional survey of US adults. International Journal of Environmental Research and Public Health, 17, 9189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grossman, E.R. , Kerr, W.C. & Toomey, T.L. (2020) The role of law and policy in reducing deaths attributable to alcohol to reach healthy people's substance abuse goals in the United States. Department of Health and Human Services, Office of Disease Prevention and Health Promotion (ODPHP). [Google Scholar]
- Grucza, R.A. , Sher, K.J. , Kerr, W.C. , Krauss, M.J. , Lui, C.K. , McDowell, Y.E. et al. (2018) Trends in adult alcohol use and binge drinking in the early 21st century United States: A meta‐analysis of six national survey series. Alcoholism: Clinical and Experimental Research, 42, 1939–1950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han, B. , Compton, W.M. , Blanco, C. , Crane, E. , Lee, J. & Jones, C.M. (2017) Prescription opioid use, misuse, and use disorders in U.S. adults: 2015 National Survey on Drug Use and Health. Annals of Internal Medicine, 167, 293–301. [DOI] [PubMed] [Google Scholar]
- Holland, K.M. , Jones, C. , Vivolo‐Kantor, A.M. , Idaikkadar, N. , Zwald, M. , Hoots, B. et al. (2021) Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID‐19 pandemic. JAMA Psychiatry, 78, 372–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huckle, T. , Parker, K. , Romeo, J.S. & Casswell, S. (2021) Online alcohol delivery is associated with heavier drinking during the first New Zealand COVID‐19 pandemic restrictions. Drug and Alcohol Review, 40, 826–834. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jager, J. & Keyes, K.M. (2021) Is substance use changing because of the COVID‐19 pandemic? Conceptual and methodological considerations to delineating the impact of the COVID‐19 pandemic on substance use and disorder. Addiction, 116, 1301–1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jang, J.B. , Patrick, M.E. , Keyes, K.M. , Hamilton, A.D. & Schulenberg, J.E. (2017) Frequent binge drinking among US adolescents, 1991 to 2015. Pediatrics, 139, e20164023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karmakar, M. , Lantz, P.M. & Tipirneni, R. (2021) Association of social and demographic factors with COVID‐19 incidence and death rates in the US. JAMA Network Open, 4, e2036462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keyes, K.M. , Jager, J. , Mal‐Sarkar, T. , Patrick, M.E. , Rutherford, C. & Hasin, D. (2019) Is there a recent epidemic of women's drinking? A critical review of national studies. Alcoholism: Clinical and Experimental Research, 43, 1344–1359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Killgore, W.D.S. , Cloonan, S.A. , Taylor, E.C. , Lucas, D.A. & Dailey, N.S. (2021) Alcohol dependence during COVID‐19 lockdowns. Psychiatry Research, 296, 113676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lechner, W.V. , Sidhu, N.K. , Jin, J.T. , Kittaneh, A.A. , Laurene, K.R. & Kenne, D.R. (2021) Increases in risky drinking during the COVID‐19 pandemic assessed via longitudinal cohort design: associations with racial tensions, financial distress, psychological distress and virus‐related fears. Alcohol and Alcoholism, 56(6), 702–707. 10.1093/alcalc/agab019 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, B.P. , Dodge, J.L. , Leventhal, A. & Terrault, N.A. (2021) Retail alcohol and tobacco sales during COVID‐19. Annals of Internal Medicine, 174(7), 1027–1029. 10.7326/M20-7271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mäkelä, P. , Rossow, I. , Moan, I.S. , Bye, E.K. , Kilian, C. , Raitasalo, K. et al. (2021) Measuring changes in alcohol use in Finland and Norway during the COVID‐19 pandemic: Comparison between data sources. International Journal of Methods in Psychiatric Research, 30, e1892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Martinez, P. , Kerr, W.C. , Subbaraman, M. & Roberts, S.C.M. (2019) New estimates of the mean ethanol content of beer, wine, and spirits sold in the United States show a greater increase in per capita alcohol consumption than previous estimates. Alcoholism: Clinical and Experimental Research, 43, 509–521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKetta, S. , Morrison, C.N. & Keyes, K.M. (2021) Trends in US alcohol consumption frequencey during the first wave of the SARS‐CoV‐2 pandemic. Alcoholism: Clinical and Experimental Research, 45, 773–783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McKnight‐Eily, L.R. , Okoro, C.A. , Strine, T.W. , Verlenden, J. , Hollis, N.D. , Njai, R. et al. (2021) Racial and ethnic disparities in the prevalence of stress and worry, mental health conditions, and increased substance use among adults during the COVID‐19 pandemic – United States, April and May 2020. MMWR, Morbidity and Mortality Weekly Report, 70, 162–166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Midanik, L.T. & Greenfield, T.K. (2003) Defining ‘current drinkers’ in national surveys: Results of the 2000 National Alcohol Survey. Addiction, 98, 517–522. [DOI] [PubMed] [Google Scholar]
- Millett, G.A. , Jones, A.T. , Benkeser, D. , Baral, S.D. , Mercer, L. , Beyrer, C. et al. (2020) Assessing differential impacts of COVID‐19 on black communities. Annals of Epidemiology, 47, 37–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minhas, M. , Belisario, K. , Gonzalez‐Roz, A. , Halladay, J. , Morris, V. , Keough, M. et al. (2021) Is talk cheap? Correspondence between self‐attributions about changes in drinking and longitudinal changes in drinking during the coronavirus disease 2019 pandemic. Alcoholism: Clinical and Experimental Research, 45(12), 2560–2568. 10.1111/acer.14724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mojica‐Perez, Y. , Callinan, S. & Livingston, M. (2019) Time of year effects on self‐reported estimates of past‐year alcohol consumption. Alcohol and Alcoholism, 54, 540–544. [DOI] [PubMed] [Google Scholar]
- Moon, A.M. , Yang, J.Y. , Barritt, A.S. IV , Bataller, R. & Peery, A.F. (2020) Rising mortality from alcohol‐associated liver disease in the United States in the 21st Century. American Journal of Gastroenterology, 115, 79–87. [DOI] [PubMed] [Google Scholar]
- Mulia, N. , Zemore, S.E. , Murphy, R. , Liu, H. & Catalano, R. (2014) Economic loss and alcohol consumption and problems during the 2008 to 2009 U.S. recession. Alcoholism: Clinical and Experimental Research, 38, 1026–1034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism (2021) Surveillance Report COVID‐19: Alcohol Sales During the COVID‐19 Pandemic [Online]. National Institute on Alcohol Abuse and Alcoholism. https://pubs.niaaa.nih.gov/publications/surveillance‐covid‐19/COVSALES.htm [Google Scholar]
- Nesoff, E.D. , Gutkind, S. , Sirota, S. , McKowen, A.L. & Veldhuis, C.B. (2021) Mental health and economic stressors associated with high‐risk drinking and increased alcohol consumption early in the COVID‐19 pandemic in the United States. Preventive Medicine, 153, 106854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ng Fat, L. , Shelton, N. & Cable, N. (2018) Investigating the growing trend of non‐drinking among young people: Analysis of repeated cross‐sectional surveys in England 2005–2015. BMC Public Health, 18, 1090. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okonkwo, N.E. , Aguwa, U.T. , Jang, M. , Barré, I.A. , Page, K.R. , Sullivan, P.S. et al. (2021) COVID‐19 and the US response: accelerating health inequities. BMJ Evidence‐Based Medicine, 26, 176–179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollard, M.S. , Tucker, J.S. & Green, H.D. (2020) Changes in adult alcohol use and consequences during the COVID‐19 pandemic in the US. JAMA Network Open, 3, e2022942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reif, S. , Karriker‐Jaffe, K.J. , Valentine, A. , Patterson, D. , Mericle, A.A. , Adams, R.S. et al. (2022) Substance use and misuse patterns and disability status in the 2020 US National Alcohol Survey: a contributing role for chronic pain. Disability and Health Journal, 101290. 10.1016/j.dhjo.2022.101290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts, A. , Rogers, J. , Mason, R. , Siriwardena, A.N. , Hogue, T. , Whitley, G.A. et al. (2021) Alcohol and other substance use during the COVID‐19 pandemic: a systematic review. Drug and Alcohol Dependence, 229, 109150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Romm, K. , Patterson, B. , Wysota, C.N. , Wang, Y. & Berg, C.J. (2021) Predictors of negative psychosocial and health behavior impact of COVID‐19 among young adults. Health Education Research, 36(4), 385–397. 10.1093/her/cyab026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothman, K.J. (1990) No adjustments are needed for multiple comparisons. Epidemiology, 1, 43–46. [PubMed] [Google Scholar]
- Schepis, T.S. , de Nadai, A.S. , Bravo, A.J. , Looby, A. , Villarosa‐Hurlocker, M.C. , Earleywine, M. et al. (2021) Alcohol use, cannabis use, and psychopathology symptoms among college students before and after COVID‐19. Journal of Psychiatric Research, 142, 73–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schmidt, R.A. , Genois, R. , Jin, J. , Vigo, D. , Rehm, J. & Rush, B. (2021) The early impact of COVID‐19 on the incidence, prevalence, and severity of alcohol use and other drugs: A systematic review. Drug and Alcohol Dependence, 228, 109065– 10.1016/j.drugalcdep.2021.109065 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Slater, M.E. & Alpert, H.R. (2021) Surveillance report #117: Apparent per capita alcohol consumption: National, State, and Regional Trends, 1977–2019. National Institute on Alcohol Abuse and Alcoholism. [Google Scholar]
- Spillane, S. , Shiels, M.S. , Best, A.F. , Haozous, E.A. , Withrow, D.R. , Chen, Y. et al. (2020) Trends in alcohol‐induced deaths in the United States, 2000–2016. JAMA Network Open, 3, e1921451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- StataCorp (2019) Stata statistical software: Release 16. StataCorp LLC. [Google Scholar]
- The American Association for Public Opinion Research (2011) Standard Definitions: Final dispositions of case codes and outcome rates for surveys, Revised 2011, 7 th Edition [Accessed: 2011‐05‐18. Archived by WebCite® at: http://www.webcitation.org/5ymByeilL] The American Association for Public Opinion Research. [Google Scholar]
- Weerakoon, S.M. , Jetelina, K.K. & Knell, G. (2021) Longer time spent at home during COVID‐19 pandemic is associated with binge drinking among US adults. The American Journal of Drug and Alcohol Abuse, 47, 98–106. [DOI] [PubMed] [Google Scholar]
- White, A.M. , Castle, I.‐J.‐P. , Hingson, R.W. & Powell, P.A. (2020) Using death certificates to explore changes in alcohol‐related mortality in the United States. Alcoholism: Clinical and Experimental Research, 44, 178–187. [DOI] [PubMed] [Google Scholar]
- White, A.M. , Slater, M.E. , Ng, G. , Hingson, R. & Brewlow, R. (2018) Trends in alcohol‐related emergency department visits in the United States: results from the Nationwide Emergency Department Sample, 2006–2014. Alcoholism: Clinical and Experimental Research, 42, 352–359. [DOI] [PubMed] [Google Scholar]
- Woolf, S.H. , Chapman, D.A. , Sabo, R.T. & Zimmerman, E.B. (2021) Excess deaths from COVID‐19 and other causes in the US, March 1, 2020 to January 2, 2021. JAMA, 325, 1786–1789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yancy, C.W. (2020) COVID‐19 and African Americans. JAMA, 323, 1891–1892. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1‐S3