

Abstract
Introduction
The COVID‐19 Anxiety Syndrome Scale (C‐19ASS) is a quick and reliable scale assessing dysfunctional coping strategies activated in response to COVID‐19 fear and threat. The present study aimed to provide a preliminary validation of the Italian version of the C‐19ASS and investigated whether the C‐19ASS would mediate the relationship between the Big Five personality traits and psychological outcomes.
Method
In Study 1, a community sample of 271 participants completed the Italian version of the C‐19ASS and results were subjected to a Principal Component Analysis. In study 2, a community sample of 484 participants completed the Italian version of the C‐19ASS and a series of measures assessing COVID‐19 anxiety, COVID‐19 fear, functional impairment, personality traits, depression, generalized anxiety and health anxiety. Internal consistency, concurrent and incremental validity were assessed. Path analyses were run.
Results
Factor analysis identified a two‐factor solution (i.e., C‐19ASS Perseveration and C‐19ASS Avoidance) and confirmatory factor analysis suggested a two‐factor model best fits the data. The Italian version of the C‐19ASS showed good internal consistency. There was also evidence of convergent validity and incremental validity. Path analyses showed that C‐19ASS Perseveration mediates the relationship between emotional stability and psychological symptoms (depression, generalized anxiety and health anxiety).
Conclusion
The Italian version of the C‐19ASS appears to be a reliable and valid measure of the COVID‐19 anxiety syndrome. The COVID‐19 anxiety syndrome could be a suitable therapeutic target to reduce psychological symptoms typically linked to pandemic events, such as depression generalized anxiety and health anxiety.
Keywords: COVID‐19 anxiety, COVID‐19 anxiety syndrome, depression, generalized anxiety, health anxiety, personality traits
Key Practitioner Message.
The Italian version of the C‐19ASS may allow clinicians and practitioners to identify COVID‐19 dysfunctional coping strategies (i.e., perseveration and avoidance) that may aggravate health outcomes.
C‐19ASS Perseveration may be more harmful than C‐19ASS Avoidance.
Females, those who perceived themselves to be vulnerable to the COVID‐19, and those with lower emotional stability may show more severe COVID‐19 anxiety syndrome.
The COVID‐19 anxiety syndrome could be a suitable therapeutic target to reduce psychological symptoms typically linked to pandemic events.
1. INTRODUCTION
The Coronavirus disease (COVID‐19) was first detected in Wuhan, China (Li et al., 2020), and quickly became a world health emergency of international concern. By 24 January 2022 there were over 340 million confirmed infections and over 5.5 million deaths worldwide (World Health Organization, 2022). The COVID‐19 pandemic and the consequent containment measures have quickly and abruptly changed people's customary life (Alzueta et al., 2021; Busch et al., 2021; Emmelkamp, 2021). A key change brought by the pandemic has been a worldwide increase of pandemic‐related psychological distress, including fear, worry, persistent avoidance, affective symptoms, posttraumatic stress symptoms, substance abuse, somatization, allostatic load, abnormal illness behaviour, fatigue, loneliness and violent behaviours, among the general population as well as the most vulnerable subgroups, including healthcare workers, older people and psychiatric patients (Amsalem et al., 2021; Akbari, Spada, et al., 2021; Brailovskaia et al., 2021, 2021; Busch et al., 2021; Cosci & Guidi, 2021; Davis et al., 2021; Emmelkamp, 2021; Fitzpatrick et al., 2020; Lebrasseur et al., 2021; Mansueto et al., 2021; Peng et al., 2021; Taylor et al., 2021; Zhang et al., 2020). Moreover, it has been suggested that the COVID‐19 pandemic may have also exacerbated dysfunctional coping strategies in response to fear or threat of the COVID‐19 pandemic itself, such as avoidant behaviours, checking, worrying and threat monitoring (Nikčević et al., 2021; Nikčević & Spada, 2020). Such dysfunctional coping strategies may ‘lock’ the person in a state of fear and threat of COVID‐19, hindering the return to ‘full/normal functioning’ (Lee, 2020a; Nikčević & Spada, 2020). This, in turn, may lead to the maintenance of the psychological distress well beyond the course of the COVID‐19 pandemic (Duffy & Allington, 2020; Lee, 2020a; Nikčević & Spada, 2020).
Given the role that COVID‐19 pandemic seems to be playing in shaping behaviour (Nikčević et al., 2021; Nikčević & Spada, 2020), from a clinical perspective, the development of clinical tools which can enable clinicians and researchers to understand the nature and degree of COVID‐19 psychological distress, as well as, to identify COVID‐19‐related dysfunctional coping strategies, have been recognized as a priority challenge (Busch et al., 2021; Lee, 2020a; Nikčević & Spada, 2020; Taylor, 2019). As result, in a short space of time, different measures have been developed for assessing fear, anxiety and stress related to COVID‐19, such as the Fear of COVID‐19 Scale (FCV‐19S; Ahorsu et al., 2020), the Coronavirus Anxiety Scale (CAS; Lee, 2020b), the COVID Stress Scales (CSS; Taylor et al., 2020), the Perceived Coronavirus Threat Questionnaire (PCTQ; Conway et al., 2020) and the Coronavirus Stress Scale (Arslan et al., 2021).
In early 2020, Nikčević and Spada developed a measure to specifically assess COVID‐19 dysfunctional cognitive–behavioural coping strategies, that is, avoidance, checking, worrying and threat monitoring in response to fear or threat of COVID‐19. Nikčević and Spada (2020) labelled this pattern of coping strategies as the ‘COVID‐19 anxiety syndrome’ and developed a self‐report measure to assess this construct, that is, the COVID‐19 Anxiety Syndrome Scale (C‐19ASS). The C‐19ASS comprises two factors, that is, perseveration (i.e., checking, worrying and monitoring because of the fear or threat of COVID‐19), and avoidance (i.e., avoidance of public spaces, transport and contact with objects because of the fear or threat of COVID‐19) (Nikčević & Spada, 2020). The C‐19ASS was firstly validated in a USA community sample (Nikčević & Spada, 2020) with futher validations in a UK community sample (Albery et al., 2021) and in an Iranian community sample (Akbari, Seydavi, et al., 2021), showing good internal consistency, construct, concurrent, divergent and incremental validity (Akbari, Seydavi, et al., 2021; Albery et al., 2021; Nikčević & Spada, 2020). The perseveration component of the COVID‐19 anxiety syndrome has been found to predict COVID‐19 anxiety, (Akbari, Seydavi, et al., 2021; Nikčević & Spada, 2020), generalized anxiety, depression (Albery et al., 2021) and functional impairments (Akbari, Seydavi, et al., 2021; Nikčević & Spada, 2020). In a representative sample of UK residents during the third national lockdown the total COVID‐19 anxiety syndrome score and its perseveration component were found to be positively correlated with general attentional bias indices, suggesting that increasing attentional bias could be a cognitive marker for increasing COVID‐19 anxiety syndrome (Albery et al., 2021). Moreover, in the USA and Iranian community samples, the total COVID‐19 anxiety syndrome score was found to mediate the association between Big Five personality traits and generalized anxiety, health anxiety, depressive symptoms and COVID‐19 anxiety (Akbari, Seydavi, et al., 2021; Nikčević et al., 2021).
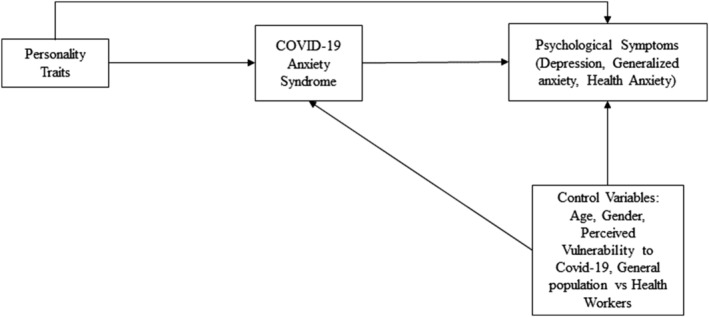
To sum up, the C‐19ASS appears to be a reliable tool to enable clinicians and practitioners to identify COVID‐19‐related dysfunctional coping strategies that may aggravate health outcomes (Akbari, Seydavi, et al., 2021; Albery et al., 2021; Nikčević et al., 2021; Nikčević & Spada, 2020). Within this framework, considering the current high prevalence of COVID‐19 in Italy (around 9%; Bassi et al., 2021) and lack of an instrument assessing the COVID‐19 anxiety syndrome, there is a clear need for an assessment tool in Italian to measure this construct. The present study aimed to: (1) provide a preliminary validation of the Italian version of the C‐19ASS by evaluating the factor structure, construct validity, internal reliabilit y, concurrent validity and incremental validity of the Italian version of the C‐19ASS; and (2) explore whether the C‐19ASS would mediate the relationship between Big Five personality traits and psychological outcomes (i.e., depression, generalized anxiety and health anxiety) in the Italian population (Figure 1), similarly to what has been found in USA and Iranian samples (Akbari, Seydavi, et al., 2021; Nikčević et al., 2021).
FIGURE 1.
Hypothesized model
Study 1: Translation and adaptation of an Italian Version of the C‐19ASS.
2. METHODS
2.1. Participants
A convenience sample was recruited from the general population between February and May 2021. Participants were eligible for inclusion in the study if they (1) were 18 years of age or above, (2) resided in Italy, (3) understood written Italian and (4) consented to participate. Eligibility criteria were minimal to attract a sample that represented a broad range of individuals.
A total of 271 individuals completed the C‐19ASS, 182 (67%) were females and 89 (33%) were males. The mean age was 31.71 ± 15.24 years. With regard to ethnic background, 261 (96.3%) participants were White, 2 (0.7%) were Black, 7 (2.6%) were Latin American and one (0.4%) was Asian. With regard to education level, 7 (3%) participants completed secondary school, 126 (46.5%) completed high school, 106 (39%) were graduates and 32 (12%) achieved post‐graduate degrees. With regard to civil status, 65 (24%) participants were married, 185 (68%) were unmarried, 20 (7%) were cohabitants and one (0.4%) was a widower. With regard to working status, 75 (28%) participants were unemployed, 115 (42%) were employed and 81 (30%) were retired and/or a housewife. With regard to COVID‐19‐related clinical features, 171 (63%) participants had been tested for COVID‐19, 22 (8%) had been diagnosed with COVID‐19, 253 (93%) knew people that had been diagnosed with COVID‐19, 30 (11%) had experienced loss as a consequence of COVID‐19 and 159 (59%) perceived themselves to be vulnerable to the disease.
2.2. Procedure and measures
Ethics approval for the study was obtained from Sigmund Freud University, Milan branch. All procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
The original C‐19ASS (Nikčević & Spada, 2020) was translated into Italian utilizing the forward and backward‐translation method (Sousa & Rojjanasrirat, 2011). First, the C‐19ASS was translated into Italian by two bilingual independent translators. Second, the Italian version was back translated into English by another two bilingual independent translators. A comparison was made between both the forward and backward translations of the measure to evaluate for any discrepancy of sentence structure and ensure the translation's accuracy. Discrepancies were examined with the collaboration of the authors of the C‐19ASS. Then, a pilot‐testing of the final version of the measure was tested in 10 healthy volunteers. Participants were asked about the clarity and understandability of the measure. There were no apparent issues regarding the clarity of the measure, and no changes were required. Thereafter, the final version of the Italian C‐19ASS (see Appendix A) was administered to the participants in our study.
Participants were recruited via email and social media. Those who agreed to participate provided a digital informed consent of privacy protection disclaimer and completed an online study pack. Participants were asked to provide a socio‐demographic details and information relating to COVID‐19, including whether they had been tested for COVID‐19, whether they had been diagnosed with COVID‐19, whether they knew people that had been diagnosed with COVID‐19, whether they had experienced a loss as a consequence of COVID‐19 and whether they perceived themselves to be vulnerable to COVID‐19.
The original C‐19ASS (C‐19ASS; Nikčević & Spada, 2020) is a self‐report measure comprising of nine items split into two factors: (1) Perseveration (six items), with items concerning checking (e.g., ‘I have checked myself for symptoms of coronavirus’), worrying (e.g., ‘I have imagined what could happen to my family members if they contracted coronavirus’) and threat monitoring (e.g., ‘I have been paying close attention to others displaying possible symptoms of coronavirus’); and (2) avoidance (three items) (e.g., ‘I have avoided touching things in public spaces because of the fear of contracting coronavirus’). Items are rated on a 5‐point Likert scale from 0 (‘Not at all’) to 4 (‘Nearly every day over the last two weeks’) with a total score ranging from 0 to 36. Higher scores indicate higher levels of COVID‐19 anxiety syndrome. The C‐19ASS has been shown to possess good psychometric proprieties (Nikčević & Spada, 2020).
2.3. Statistical analyses
Exploratory factor analysis (EFA), employing maximum likelihood method with Promax rotation adopting kappa = 4 was used to explore the factor structure of the Italian version of the C‐19ASS. Kaiser–Meyer–Olkin (KMO) test (Kaiser, 1970) and Bartlett's test of sphericity (Bartlett, 1937) were performed. The eigenvalue was set to 1.0 or above and lowest accepted loading was 0.30 or above (Barbaranelli & D'Olimpio, 2006; Costello & Osborne, 2005). The number of factors to be extracted was determined according to the consideration of the Kaiser's eigenvalue criterion (eigenvalues > 1) (Kaiser, 1970), Horn's parallel analysis (Horn, 1965) and the scree‐test criteria (Cattell, 1966). Data were analysed using version 27 of SPSS (IBM SPSS Statistics).
3. RESULTS
The KMO measure of sampling adequacy was 0.84, and the Barlett's test of sphericity was significant (<0.001), suggesting that data were suitable for factor analysis. Before factor analysis, the random eigenvalues were compared with the observed data using a parallel analysis (Horn, 1965). The first two random Eigenvalues (i.e., 0.42 and 0.32) were below the first two observed eigenvalues (i.e., 3.51 and 1.04), suggesting two factors. The scree‐plot also clearly indicated a two‐factor solution. Therefore, the EFA was conducted with two factors resulting in a solution comparable to the Nikčević and Spada (2020) study. A summary of the EFA is displayed in Table 1. All items loaded clearly on one of the two factors, with a minimum of 0.30. There were no significant cross‐loadings. The two factors together accounted for 50.54% of variance and the estimated correlation between the two factors was 0.54. Based on Nikčević and Spada's (2020) article, factor 1 was labelled ‘Perseveration’ (C‐19ASS‐P; six items) and factor 2 was labelled ‘Avoidance’ (C‐19ASS‐A; three items).
TABLE 1.
The Italian version of the COVID‐19 Anxiety Syndrome Scale (C‐19ASS ITA) factor loading
| Item | Factor 1 Perseveration | Factor 2 Avoidance | |
|---|---|---|---|
| 1 | I have avoided using public transport because of the fear of contracting coronavirus (COVID‐19). | 0.15 | 0.30 |
| 2 | I have checked myself for symptoms of coronavirus (COVID‐19) | 0.54 | 0.10 |
| 3 | I have avoided going out to public places (shops, parks) because of the fear of contracting coronavirus (COVID‐19) | −0.04 | 0.96 |
| 4 | I have been concerned about not having adhered strictly to social distancing guidelines for coronavirus (COVID‐19) | 0.36 | 0.12 |
| 5 | I have avoided touching things in public spaces because of the fear of contracting coronavirus (COVID‐19) | 0.24 | 0.35 |
| 6 | I have read about news relating to coronavirus (COVID‐19) at the cost of engaging in work (such as writing emails, working on word documents or spreadsheets) | 0.33 | 0.15 |
| 7 | I have checked my family members and loved one for the signs of coronavirus (COVID‐19) | 0.77 | −0.02 |
| 8 | I have been paying close attention to others displaying possible symptoms of coronavirus (COVID‐19) | 0.68 | 0.03 |
| 9 | I have imagined what could happen to my family members if they contracted coronavirus (COVID‐19) | 0.67 | −0.01 |
Note: n = 271. Bold values indicate which items are loading on each factor.
Study 2: Construct validity, internal reliability, concurrent validity and incremental validity of the Italian version of the C‐19ASS and investigation of association between the COVID‐19 anxiety syndrome and psychological symptoms in Italian population.
We conducted a second study aimed at (1) evaluating construct validity, internal reliability, concurrent validity and incremental validity of the Italian version of the C‐19ASS and (2) evaluating whether the C‐19ASS could mediate the relationship between Big Five personality traits and psychological outcomes (i.e., depression, generalized anxiety and health anxiety) in the Italian population (Figure 1).
4. METHODS
4.1. Participants
A convenience sample was recruited from the general population between June 2021 and September 2021. Participants were eligible for inclusion in the study if they (1) were 18 years of age, (2) resided in Italy, (3) understood spoken and written Italian and (4) consented to participate. Eligibility criteria were minimal to attract a sample that represented a broad range of individuals.
A total of 484 participated in the study, 364 (75%) of whom were females and 120 (25%) males with a mean age of 36.76 ± 12.53 years. The sample reported their ethnic background as follows: 476 (98.3%) were White, 2 (0.4%) were Black, 4 (0.8%) were Latin American and 2 (0.4%) were Asian. With regard to education level, 37 (8%) of the participants had completed secondary school, 155 (32%) had completed secondary school, 210 (43%) had graduated and 82 (17%) had achieved post‐undergraduate degrees. With regard to civil status, 137 (28%) were married, 226 (47%) were unmarried, 117 (24%) were cohabiting and 4 (0.83%) were widowers. With regard to working status, 37 (8%) were unemployed, 408 (84%) were employed and 39 (8%) were retired and/or housewives. With regard to working status, 113 (23%) were health workers. With regard to COVID‐19 clinical features, 344 participants (71%) had been tested for COVID‐19, 63 (13%) have been diagnosed with COVID‐19, 454 (94%) knew someone who had been diagnosed with COVID‐19, 85 (18%) had experienced a loss as a consequence of COVID‐19, 382 (79%) had been vaccinated for COVID‐19 and 235 (48%) perceived themselves to be vulnerable to COVID‐19.
4.2. Procedure and measures
The procedure used in Study 2 was the same as the one used in Study 1 (see Section 2.2). Participants provided the same information with regard to socio‐demographic details and information related to COVID‐19, that is, whether they had been tested for COVID‐19, whether they had been diagnosed with COVID‐19, whether they knew of people who had been diagnosed with COVID‐19, whether they had experienced loss as a consequence of COVID‐19, whether they had been vaccinated for COVID‐19 and whether they perceived themselves to be vulnerable to COVID‐19. They then completed the batch of self‐report measures.
4.2.1. COVID‐19 Anxiety Syndrome Scale (C‐19ASS; Nikčević & Spada, 2020)
The Italian translated version of the C‐19ASS administered in Study 1 was used also in Study 2.
4.2.2. Coronavirus Anxiety Scale (CAS; Lee, 2020b)
The CAS is a 5‐item self‐report measure assessing thoughts and physiological symptoms related to COVID‐19 during the last 2 weeks. The items are rated on a 5‐point Likert scale from 0 (‘Not at all’) to 4 (‘Nearly every day over the last two weeks’). The CAS total score ranges from 0 to 20, and higher scores indicate higher levels of COVID‐19‐related anxiety. The CAS has been shown to possess good psychometric proprieties (Lee, 2020a, 2020b; Mozzoni & Franzot, 2020). In the current study we used the Italian translation of the CAS (Mozzoni & Franzot, 2020). In the present study the CAS showed good internal consistency (Cronbach's alpha = 0.87).
4.2.3. Fear of COVID‐19 Scale (FCV‐19S; Ahorsu et al., 2020)
The FCV‐19S is a 7‐item self‐report measure assessing the fear of COVID‐19. The items (e.g., ‘I am most afraid of coronavirus‐19’) are rated on a 5‐point Likert scale from 1 (‘Strongly disagree’) to 5 (‘Strongly agree’) with scores ranging from 7 to 35. Higher scores indicate higher levels of fear of COVID‐19. The FCV‐19S has been shown to possess good psychometric properties (Ahorsu et al., 2020; Soraci et al., 2020). In the current study we used the Italian validated translation of the FCV‐19S (Soraci et al., 2020). In the present study the FCV‐19S showed good internal consistency (Cronbach's alpha = 0.91).
4.2.4. Work and Social Adjustment Scale (WSAS; Mundt et al., 2002)
The WSAS is a 5‐item self‐report measure assessing the functional impairment of a particular problem. The items are rated on a 9‐point Likert scale from 0 (‘Not at all’) to 8 (‘Very severely’). The WSAS scores range from 0 to 40, where higher scores indicate higher social and functional impairment levels. The WSAS has been shown to possess good psychometric properties (Mundt et al., 2002). In the present study the WSAS showed good internal consistency (Cronbach's alpha = 0.91).
4.2.5. Big Five Inventory‐10 (BFI‐10; Rammstedt & John, 2007)
The BFI‐10 is 10‐item self‐report measure assessing the Big Five personality traits, including agreeableness, conscientiousness, emotional stability, extraversion and openness. The items are rated on a 5‐point Likert scale from 1 (‘Disagree strongly’) to 5 (‘Agree strongly’). The BFI‐10 presents a score with a range of 2–10 for each dimension. Higher scores indicate higher levels of the given trait. The BFI‐10 has been shown to possess good psychometric proprieties (Guido et al., 2015; Rammstedt & John, 2007). In the current study we used the Italian validated translation of the BFI‐10 (Guido et al., 2015). In the present study the BFI‐10 showed acceptable internal consistency (Cronbach's alpha = 0.60).
4.2.6. Patient Health Questionnaire 9 (PHQ‐9; Kroenke et al., 2001)
The PHQ‐9 is a 9‐item self‐report measure assessing, screening, and monitoring depression severity during the past 2 weeks. The items are rated on a 4‐point Likert scale from 0 (‘Not at all’) to 3 (‘Nearly every day’). The PHQ‐9 scores range from 0 to 27. High scores indicate higher levels of depression. Scores ranging from 15 to 19 indicate depression of moderate severity, and scores ranging from 20 to 27 indicate severe depression. The PHQ‐9 has been shown to possess good psychometric proprieties (Kroenke et al., 2001; Manea et al., 2015; Mazzotti et al., 2003). In the current study we used the Italian validated translation of the PHQ‐9 (Mazzotti et al., 2003). In the present study the PHQ‐9 showed good internal consistency (Cronbach's alpha = 0.89).
4.2.7. Generalized Anxiety Disorder 7 (GAD‐7; Spitzer et al., 2006)
The GAD‐7 is a 7‐item self‐report measure assessing and screening generalized anxiety disorder and its severity during the past 2 weeks. The items are rated on a 4‐point Likert scale from 0 (‘Not at all’) to 3 (‘Nearly every day’), with a total score ranging from 0 to 21. Higher scores indicate higher levels of generalized anxiety. Scores ranging from 10 to 14 indicate generalized anxiety of moderate severity, and scores ranging from 15 to 21 indicate severe generalized anxiety. The GAD‐7 has been shown to possess good psychometric properties (Spitzer et al., 2006). In the current study, we used the Italian translation of the GAD‐7 (Spitzer et al., 2006). In the present study the GAD‐7 showed good internal consistency (Cronbach's alpha = 0.93).
4.2.8. Health Anxiety Questionnaire (HAQ;Lucock & Morley, 1996; Melli et al., 2007)
The HAQ is a 21‐item self‐report measure assessing the severity of health anxiety. The items are rated on a 4‐point Likert scale from 1 (‘Never or rarely’) to 4 (‘Almost always’). The HAQ includes four sub‐scales, which assess health worry and preoccupation, fear of illness and death, reassurance‐seeking behaviour and interference with life. Higher scores indicate higher levels of health anxiety. The HAQ had good psychometric properties (Lucock & Morley, 1996; Melli et al., 2007). In the present study we considered only the total score because we were interested in assessing the global severity of health anxiety. In the current study we used the Italian validated translation of the HAQ (Melli et al., 2007). In the present study the HAQ showed good internal consistency (Cronbach's alpha = 0.96).
4.3. Statistical analyses
Statistical analyses followed five steps in order to (i) test the factor structure of the C‐19ASS, (ii) test the invariance between gender groups, (iii) evaluate concurrent and incremental validity, (iv) explore differences in C‐19ASS scores between several groups and (v) test the pattern of relationships specified by our hypothesized model (Figure 1).
First, a confirmatory actor analysis (CFA) using the Lavaan package (Rosseel, 2012) of software R (R Development Core Team, 2017) was implemented to evaluate the construct validity of the Italian version of the C‐19ASS. Weighted least estimation with robust standard errors and mean and variance estimator for ordinal items was adopted. The indices used to assess the fit of the model were: the Chi‐square (χ 2), the comparative fit index (CFI; acceptable fit ≥0.90), the goodness‐of‐fit index (GFI; acceptable fit ≥0.90), the root‐mean‐square error of approximation (RMSEA; acceptable fit ≤0.08) (Browne & Cudeck, 1993), the standardized root mean square residual (SRMR; good fit ≤0.08) (Hu & Bentler, 1999), the Tucker–Lewis Index (TLI), the normed fit index (NFI) and the incremental fit index (IFI). Cronbach's α (Cronbach, 1951) was used to assess internal reliability of the Italian version of the C‐19ASS.
Second, in order to test the measurement invariance across gender, multi‐group CFA was used (Van de Schoot et al., 2012). Configural, metric and scalar models were estimated. Measurement invariance was established when (a) the change in values for fit indices (e.g., ΔCFI and ΔRMSEA) was negligible (i.e., ΔCFI lower than 0.01 and a change lower than 0.015 in RMSEA as indicative of invariance; Cheung & Rensvold, 2002); and (b) the multi‐group model fit indexes indicated a good fit (Beaujean et al., 2012).
Third, descriptive analyses and univariate and multivariate normality tests were calculated. Skewness and kurtosis were assessed and were considered adequate for a linear model of analysis in a range of ±2 (Gravetter & Wallnau, 2016). Bivariate correlation analyses were run to evaluate concurrent validity of the Italian version of the C‐19ASS, by observing whether the two factors of the C‐19ASS would correlate significantly with established measures of COVID‐19 anxiety and perceived fear (i.e., CAS; Lee, 2020b; FCV‐19S; Ahorsu et al., 2020). Moreover, according to Nikčević and Spada's (2020) article, hierarchical linear regression analyses were run to evaluate incremental validity of Italian version of the C‐19ASS by observing (a) whether the C‐19ASS would explain additional variance in CAS (Lee, 2020b) when controlling for age, gender, Big‐Five personality traits, perception of vulnerability to COVID‐19 and COVID‐19 perceived fear and (b) whether the C‐19ASS would explain additional variance in WSAS (Mundt et al., 2002) when controlling for age, gender, Big‐Five personality traits, perception of vulnerability to COVID‐19 and COVID‐19 perceived fear. Statistical assumptions for using hierarchical linear regression analyses were evaluated (Barbaranelli & D'Olimpio, 2006; Field, 2013; Myers, 1990).
Fourth, a series of ANOVA and Welch's test were run to explore differences on C‐19ASS scores between: males versus females; participants who had tested for COVID‐19 versus those who had not tested for COVID‐19; participants who had been diagnosed with COVID‐19 versus those who had not been diagnosed with COVID‐19; participants who knew people who had been diagnosed with COVID‐19 versus those who did not know people who had been diagnosed with COVID‐19; participants who had experienced loss as a consequence of COVID‐19 versus those who had not experienced loss as a consequence of COVID‐19; participants who had been vaccinated for COVID‐19 versus those who had not been vaccinated for COVID‐19; participants who perceived themselves to be vulnerable to COVID‐19 versus those who did not perceive themselves to be vulnerable to COVID‐19; general population versus health workers.
Fifth, the pattern of relationships specified by our hypothesized model (Figure 1) was tested through path analysis, using the Lavaan package (Rosseel, 2012) of the software R (R Development Core Team, 2017). A single observed score for each variable and the maximum likelihood methods (Satorra & Bentler, 1994) were used. In our model, the Big Five personality traits were the independent variables; the two factors of the COVID‐19 anxiety syndrome (i.e., C‐19ASS Perseveration and C‐19ASS Avoidance) were the mediators; and depression, generalized anxiety and health anxiety were the dependent variables (Figure 1). Age, gender, employment status (general population versus health workers) and perceived vulnerability to COVID‐19 were included as covariates of the mediators and the dependent variables. The mediating role of the COVID‐19 anxiety syndrome was evaluated using bootstrap approach (1000 bootstrap samples). We first tested the full model and then we subsequently removed step‐by‐step path coefficients not significant at the 5% level in order to select the most plausible model. To evaluate the goodness of fit of the model we considered the explained variance of each endogenous variable (R 2) and the total coefficient of determination (TCD; Bollen, 1989; Jӧreskog & Sӧrbom, 1996), which is commonly considered a reliable fit index of models run as path analysis (that is SEM for observed variables). The TCD represents the joined effect of all predictor variables on all dependent variables, so that higher TCD scores indicate more variance explained.
5. RESULTS
5.1. Factor structure of the C‐19ASS and internal reliability
Table 2 presents the results of CFA, showing a comparison between the two‐factor model and one‐factor model. The two‐factor model (χ 2 = 33.746, df = 26, χ 2/df = 1.29, p = 0.142, SRMR = 0.040, RMSEA = 0.025 90%CI [0.000–0.046], GFI = 0.996, CFI = 0.997, NFI = 0.989, TLI = 0.996, IFI = 0.997) had the best model fit (Chi‐square difference test: χ 2 = 29.087, df = 1, p < 0.001). Therefore, the two dimensions of the C‐19ASS (i.e., C‐19ASS Perseveration and C‐19ASS Avoidance) were used in the subsequent analyses. Both the C‐19ASS Perseveration (six items; α = 0.810) and the C‐19ASS Avoidance (three items; α = 0.745) demonstrated acceptable internal consistency. The average variance extracted (AVE) was 0.45 for the C‐19ASS Perseveration, and 0.49 for the C‐19ASS, whereas the composite reliability was 0.81 for the C‐19ASS Perseveration, and 0.75 for the C‐19ASS Avoidance, which are overall considered acceptable (Fornell & Larcker, 1981; Hair et al., 2010).
TABLE 2.
Model fit indices of confirmatory factor analysis for the Italian version of the COVID‐19 Anxiety Syndrome Scale (C‐19ASS ITA)
| χ 2 | DF | χ 2/df | SRMR | RMSEA | GFI | CFI | NFI | TLI | IFI | |
|---|---|---|---|---|---|---|---|---|---|---|
| One‐factor solution | 59.235 | 27 | 2.19 | 0.051 | 0.050 | 0.993 | 0.989 | 0.981 | 0.986 | 0.989 |
| Two‐factor solution | 33.746 | 26 | 1.29 | 0.040 | 0.025 | 0.996 | 0.997 | 0.989 | 0.996 | 0.997 |
Note: n = 484. All the models were estimated with zero cross‐loadings and correlated errors.
Abbreviations: CFI, comparative fit index; GFI, goodness of fit; IFI, incremental fit index; NFI, normed fit index; RMSEA, root‐mean‐square error of approximation; SRMR, standardized root mean square residual; TLI, Tucker–Lewis Index; χ 2 = Chi‐square index.
5.2. Measurement invariance of the C‐19ASS across gender groups
Before testing for measurement invariance, the C‐19ASS model was estimated separately in males and females. Results demonstrated that the model fit was adequate to excellent for both gender groups (males: χ 2 = 13.312, df = 26, p = 0.981, RMSEA = 0.043 90%CI[0.000–0.088], CFI = 0.983; and females: χ2 = 29.152, df = 26, p = 0.304, RMSEA = 0.064 90%CI[0.045–0.084], CFI = 0.967, TLI = 0.954). Then, measurement invariance of the model was tested through multi‐group CFA. The fit indices of the unconstrained multi‐group model demonstrated the configural invariance of the model (χ 2 = 42.464, df = 52, p = 0.825, CFI = 1.000, RMSEA = 0.000 90%CI[0.000–0.026]), suggesting that the factor structure is similar across gender. Then, the metric model testing for invariance of all factor loadings was tested in which loadings were constrained to equality (χ 2 = 60.844, df = 59, p = 0.409, CFI = 0.999, RMSEA = 0.011 90%CI[0.000–0.042]). This did not lead to a significant reduction in model fit (ΔCFI = 0.001, ΔRMSEA = 0.011), suggesting that the C‐19ASS assesses similar underlying factors across males and females. Finally, all the item intercepts were constrained across groups to test for scalar invariance (χ 2 = 63.798, df = 66, p = 0.554, CFI = 1.000, RMSEA = 0.000 90%CI[0.000–0.036]). Results demonstrated that total scalar invariance across gender groups was confirmed (ΔCFI = 0.001, ΔRMSEA = 0.011).
5.3. Concurrent validity, and incremental validity of the Italian version of the C‐19ASS
Table 3 presents means, standard deviations, ranges, skewness and kurtosis, suggesting that the variables of interest were overall normally distributed.
TABLE 3.
Means, standard deviations, ranges and inter‐correlations of variables
| Mean ± SD | Range | Skewness | Kurtosis | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | BFI‐10‐Agr | 6.55 ± 3.11 | 2–10 | −0.22 | −0.29 | 1 | 0.169** | 0.246** | 0.213** | −0.018 | −0.026 | −0.171** | −0.214** | −0.248** | −0.186** | −0.104* | −0.043 | −0.007 |
| 2 | BFI‐10‐Con | 7.74 ± 1.64 | 2–10 | −0.30 | −0.55 | 1 | 0.297** | 0.203** | −0.014 | −0.088 | −0.210** | −0.415** | −0.330** | −0.296** | −0.139* | −0.113* | −0.040 | |
| 3 | BFI‐10‐Emo stab | 5.83 ± 5.49 | 2–10 | 0.02 | −0.88 | 1 | 0.167** | −0.045 | 0.358** | −0.512** | −0.483** | −0.559** | −0.414** | −0.419** | −0.278** | −0.201** | ||
| 4 | BFI‐10‐Ext | 6.30 ± 1.94 | 2–10 | −0.08 | −0.60 | 1 | 0.073 | −0.060 | −0.076 | −0.222** | −0.175** | −0.195** | −0.071 | −0.039 | −0.077 | |||
| 5 | BFI‐10‐Ope | 6.90 ± 3.45 | 2–10 | −0.13 | −0.47 | 1 | −0.033 | 0.047 | 0.049 | 0.045 | 0.031 | 0.036 | −0.060 | −0.069 | ||||
| 6 | FCV‐19 | 17.18 ± 39.46 | 7–35 | 0.44 | −0.42 | 1 | 0.610** | 0.390** | 0.419** | 0.367** | 0.685** | 0.611** | 0.503** | |||||
| 7 | HAQ | 39.82 ± 16.12 | 21–83 | 1.04 | 0.82 | 1 | 0.488** | 0.624** | 0.496** | 0.573** | 0.521** | 0.311** | ||||||
| 8 | PHQ‐9 | 7.86 ± 32.38 | 0–27 | 1.05 | 0.70 | 1 | 0.806** | 0.603** | 0.463** | 0.297** | 0.163** | |||||||
| 9 | GAD‐7 | 6.74 ± 29.04 | 0–21 | 0.99 | 0.05 | 1 | 0.573** | 0.518** | 0.334** | 0.184** | ||||||||
| 10 | WSAS | 7.12 ± 9.01 | 0–39 | 1.34 | 0.98 | 1 | 0.427** | 0.313** | 0.215** | |||||||||
| 11 | CAS | 3.94 ± 17.01 | 0–20 | 1.27 | 1.23 | 1 | 0.602** | 0.458** | ||||||||||
| 12 | C‐19ASS‐P | 9.78 ± 31.78 | 0–24 | 0.35 | −0.64 | 1 | 0.634** | |||||||||||
| 13 | C‐19ASS‐A | 6.10 ± 14.62 | 0–12 | −0.03 | −10.21 | 1 |
Note: n = 484.
Abbreviations: BFI‐10‐Agr, Big Five Inventory‐10‐Agreeableness; BFI‐10‐Con, Big Five Inventory‐10‐Conscientiousness; BFI‐10‐Emo stab, Big Five Inventory‐10‐Emotional stability; BFI‐10‐Ext, Big Five Inventory‐10‐Extraversion; BFI‐10‐Ope, Big Five Inventory‐10‐Openness; CAS, Coronavirus Anxiety Scale; C‐19ASS‐A, COVID‐19 Anxiety Syndrome Scale Avoidance; C‐19ASS‐P, COVID‐19 Anxiety Syndrome Scale Perseveration; FCV‐19, Fear of COVID‐19 Scale; GAD‐7, Generalized Anxiety Disorder 7; HAQ, Health Anxiety Questionnaire; PHQ‐9, Patient Health Questionnaire 9; WSAS, Work and Social Adjustment Scale.
p < 0.05.
p < 0.001.
Concurrent validity was evaluated by examining the correlation between C‐19ASS, CAS and FCV‐19S. Correlation analyses showed that both the C‐19ASS Perseveration and the C‐19ASS Avoidance were positively correlated with the CAS (C‐19ASS Perseveration r = 0.602, p < 0.001; C‐19ASS Avoidance r = 0.458, p < 0.001) and FCV‐19S (C‐19ASS Perseveration r = 0.611, p < 0.001; C‐19ASS Avoidance r = 0.503, p < 0.001) (Table 3).
The data also showed that the CAS was negatively correlated with BFI‐10‐Agreeableness (r = −0.104, p = 0.022), BFI‐10‐Conscientiousness (r = −0.139, p = 0.002) BFI‐10‐Emotional stability (r = −0.419, p < 0.001), and positively correlated with FCV‐19S (r = 0.685, p < 0.001) (Table 3). Both the C‐19ASS Perseveration (r = 0.313, p < 0.001) and the C‐19ASS Avoidance (r = 0.215, p < 0.001) were also positively correlated with the WSAS. Moreover, the WSAS was found to be negatively correlated with all dimensions of the BFI‐10 (r value range: −0.419 to −0.186, p < 0.005), with the exception of BFI‐10‐Openness (r = 0.045, p = 0.499), and positively correlated with FCV‐19S (r = 0.367, p < 0.001) and CAS (r = 0.427, p < 0.001) (Table 3).
Tables 4 and 5 report the hierarchical linear regression models examining the incremental validity of the Italian version of the C‐19ASS. Before analysing data, assumptions were tested. Multicollinearity statistics were within acceptable limits for both models (Model 1: Tolerance Index ranged from 0.47 to 1, Variance Inflation Factor [VIF] ranged from 1 to 2.11; Model 2: Tolerance Index ranged from 0.47 to 1, Variance Inflation Factor [VIF] ranged from 1 to 2.12) (Barbaranelli & D'Olimpio, 2006; Bowerman & O'Connell, 1990; Field, 2013; Hair et al., 1998). For both models histograms and normality plots suggested that regression‐standardized residuals were normally distributed (Barbaranelli & D'Olimpio, 2006; Field, 2013). Furthermore, the Durbin–Watson test (Model 1: 2.03; Model 2: 1.97) showed that there were no significant correlations between standardized residuals and independent variables (Barbaranelli & D'Olimpio, 2006; Field, 2013).
TABLE 4.
Hierarchical regression analyses predicting Coronavirus Anxiety Scale (CAS) scores
| Predictor | B | Std. Error | β | t | R | R 2 | Adjusted R 2 | ΔR 2 | 95% Confidence interval for B | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||||||
| Model | ||||||||||
| Step 1 | 0.22 | 0.05 | 0.05 | 0.05** | ||||||
| Age | −0.04 | 0.01 | −0.12** | −2.73 | −0.07 | −0.01 | ||||
| Gender | 1.18 | 0.42 | 0.19** | 4.26 | 0.98 | 2.65 | ||||
| Step 2 | 0.44 | 0.20 | 0.19 | 0.15** | ||||||
| Age | −0.004 | 0.01 | −0.01 | −0.27 | −0.03 | 0.02 | ||||
| Gender | 1.38 | 0.40 | 0.14** | 3.46 | 0.60 | 2.17 | ||||
| BFI‐10‐Agreeableness | −0.03 | 0.10 | −0.01 | −0.27 | −0.23 | 0.17 | ||||
| BFI‐10‐Conscientiousness | −0.07 | 0.11 | −0.03 | −0.66 | −0.29 | 0.15 | ||||
| BFI‐10‐Emotional stability | −0.68 | 0.08 | −0.39** | −8.59 | −0.84 | −0.53 | ||||
| Step 3 | 0.49 | 0.24 | 0.23 | 0.04** | ||||||
| Age | −0.01 | 0.01 | −0.04 | −0.97 | −0.04 | −0.12 | ||||
| Gender | 1.39 | 0.39 | 0.14** | 3.58 | 0.62 | 2.15 | ||||
| BFI‐10‐Agreeableness | −0.03 | 0.10 | −0.01 | −0.29 | −0.22 | −0.17 | ||||
| BFI‐10‐Conscientiousness | −0.06 | 0.11 | −0.03 | −0.60 | −0.28 | 0.15 | ||||
| BFI‐10‐Emotional stability | −0.64 | 0.08 | −0.36** | −8.20 | −0.79 | −0.48 | ||||
| Perception of vulnerability to COVID‐19 | −1.78 | 0.33 | −0.22** | −5.35 | −2.44 | −1.13 | ||||
| Step 4 | 0.72 | 0.52 | 0.52 | 0.28** | ||||||
| Age | −0.04 | 0.01 | −0.14** | −3.89 | −0.07 | −0.02 | ||||
| Gender | 0.33 | 0.31 | 0.03 | 1.04 | −0.29 | 0.94 | ||||
| BFI‐10‐Agreeableness | −0.04 | 0.08 | −0.02 | −0.47 | −0.19 | 0.12 | ||||
| BFI‐10‐Conscientiousness | −0.004 | 0.09 | −0.002 | −0.04 | −0.17 | 0.16 | ||||
| BFI‐10‐Emotional stability | −0.25 | 0.07 | −0.14** | −3.87 | −0.38 | −0.12 | ||||
| Perception of vulnerability to COVID‐19 | 0.36 | 0.29 | 0.04 | 1.24 | −0.21 | 0.94 | ||||
| FCV‐19‐Fear of COVID‐19 | 0.43 | 0.03 | 0.66** | 16.84 | 0.38 | 0.48 | ||||
| Step 5 | 0.76 | 0.57 | 0.56 | 0.05** | ||||||
| Age | −0.04 | −0.1 | −0.12** | −3.54 | −0.06 | −0.02 | ||||
| Gender | 0.38 | 0.30 | 0.04 | 1.28 | −0.20 | 0.97 | ||||
| BFI‐10‐Agreeableness | −0.04 | 0.07 | −0.02 | −0.59 | −0.19 | 0.10 | ||||
| BFI‐10‐Conscientiousness | 0.01 | 0.08 | 0.005 | 0.15 | −0.15 | 0.17 | ||||
| BFI‐10‐Emotional stability | −0.23 | 0.06 | −0.13** | −3.69 | −0.35 | −0.11 | ||||
| Perception of vulnerability to COVID‐19 | 0.55 | 0.28 | 0.07* | 1.97 | 0.001 | 1.10 | ||||
| FCV‐19‐Fear of COVID‐19 | 0.33 | 0.03 | 0.50** | 11.37 | 0.27 | 0.38 | ||||
| C‐19ASS Perseveration | 0.18 | 0.03 | 0.25** | 5.63 | 0.12 | 0.24 | ||||
| C‐19ASS Avoidance | 0.05 | 0.04 | 0.05 | 1.19 | −0.03 | 0.14 | ||||
Notes: N = 484. Gender (0 = male, 1 = female); perception of vulnerability to COVID‐19 (1 = yes, 2 = no).
Abbreviations: BFI‐10, Big Five Inventory; C‐19ASS, COVID‐19 Anxiety Syndrome Scale; FCV‐19, Fear of COVID‐19 Scale.
p < 0.001.
p < .05.
TABLE 5.
Hierarchical regression analyses predicting Work and Social Adjustment Scale (WSAS) scores
| Predictor | B | Std. Error | β | T | R | R 2 | Adjusted R 2 | ΔR 2 | 95% confidence interval for B | |
|---|---|---|---|---|---|---|---|---|---|---|
| Lower bound | Upper bound | |||||||||
| Model | ||||||||||
| Step 1 | 0.18 | 0.03 | 0.03 | 0.03** | ||||||
| Age | −0.11 | 0.03 | −0.15** | −3.46 | −0.17 | −0.05 | ||||
| Gender | 1.89 | 0.93 | 0.09* | 2.02 | 0.05 | 3.72 | ||||
| Step 2 | 0.47 | 0.22 | 0.21 | 0.19** | ||||||
| Age | 0.01 | 0.03 | 0.01 | 0.23 | −0.06 | 0.07 | ||||
| Gender | 1.38 | 0.86 | 0.07 | 1.61 | −0.30 | 3.07 | ||||
| BFI‐10‐Agreeableness | −0.33 | 0.22 | −0.06 | −1.47 | −0.77 | 0.11 | ||||
| BFI‐10‐Conscientiousness | −0.97 | 0.24 | −0.18** | −4.02 | −1.45 | −0.50 | ||||
| BFI‐10‐Emotional stability | −1.25 | 0.17 | −0.32** | −7.32 | −1.59 | −0.91 | ||||
| BFI‐10‐Extraversion | −0.43 | 0.19 | −0.09* | −2.17 | −0.81 | −0.04 | ||||
| Step 3 | 0.47 | 0.22 | 0.21 | 0.003 | ||||||
| Age | 0.001 | 0.03 | 0.002 | 0.035 | −0.06 | 0.06 | ||||
| Gender | 1.39 | 0.86 | 0.07 | 1.62 | −0.29 | 3.07 | ||||
| BFI‐10‐Agreeableness | −0.33 | 0.22 | −0.06 | −1.50 | −0.77 | 0.10 | ||||
| BFI‐10‐Conscientiousness | −0.97 | 0.24 | −0.18** | −4.02 | −1.44 | −0.50 | ||||
| BFI‐10‐Emotional stability | −1.22 | 0.17 | −0.32** | −7.14 | −1.56 | −0.89 | ||||
| BFI‐10‐Extraversion | −0.40 | 0.20 | −0.09* | −2.05 | −0.79 | −0.02 | ||||
| Perception of vulnerability to COVID‐19 | −1.05 | 0.74 | −0.06 | −1.42 | −2.50 | 0.40 | ||||
| Step 4 | 0.53 | 0.28 | 0.27 | 0.05** | ||||||
| Age | −0.03 | 0.03 | −0.04 | −0.92 | −0.09 | 0.03 | ||||
| Gender | 0.37 | 0.84 | 02 | 0.43 | 0.66 | 1.29 | ||||
| BFI‐10‐Agreeableness | 0.34 | 0.21 | −0.07 | −1.58 | −0.76 | 0.08 | ||||
| BFI‐10‐Conscientiousness | −0.91 | 0.23 | −0.16** | −3.90 | −1.37 | −0.45 | ||||
| BFI‐10‐Emotional stability | −0.85 | 0.18 | −0.22** | −4.85 | −1.20 | −0.51 | ||||
| BFI‐10‐Extraversion | −0.41 | 0.19 | −0.09* | −2.17 | −0.79 | −0.04 | ||||
| Perception of vulnerability to COVID‐19 | 1.02 | 0.79 | 0.06 | 1.29 | −0.53 | 2.58 | ||||
| FCV‐19‐Fear of COVID‐19 | 0.42 | 0.07 | 0.29** | 6.04 | 0.28 | 0.55 | ||||
| Step 5 | 0.53 | 0.29 | 0.27 | 0.007 | ||||||
| Age | −0.02 | 0.03 | −0.03 | −0.72 | −0.08 | 0.04 | ||||
| Gender | 0.41 | 0.84 | 0.02 | 0.48 | −1.24 | 2.06 | ||||
| BFI‐10‐Agreeableness | −0.34 | 0.21 | −0.07 | −1.59 | −0.76 | 0.08 | ||||
| BFI‐10‐Conscientiousness | −0.89 | 0.23 | −0.16** | −3.82 | −1.35 | −0.43 | ||||
| BFI‐10‐Emotional stability | −.84 | 0.18 | −.22** | −4.75 | −1.18 | −0.49 | ||||
| BFI‐10‐Extraversion | −0.43 | 0.19 | −0.09** | −2.26 | −0.80 | −0.06 | ||||
| Perception of vulnerability to COVID‐19 | 1.17 | 0.79 | 0.06 | 1.47 | −0.39 | 2.73 | ||||
| FCV‐19‐Fear of COVID‐19 | 0.33 | 0.08 | 0.22** | 4.14 | 0.18 | 0.49 | ||||
| C‐19ASS‐Persevaration | 0.18 | 0.09 | 0.11* | 1.97 | 0.001 | 0.36 | ||||
| C‐19ASS Avoidance | −0.03 | 0.12 | −0.01 | −0.24 | −0.27 | 0.21 | ||||
Notes: N = 484. Gender (0 = male, 1 = female); perception of vulnerability to COVID‐19 (1 = yes, 2 = no).
Abbreviations: BFI‐10‐ = Big Five Inventory; C‐19ASS = COVID‐19 Anxiety Syndrome Scale; FCV‐19 = Fear of COVID‐19 Scale.
p < 0.001.
p < 0.05.
Table 4 shows the hierarchical linear regression examining the incremental validity of the Italian version of the C‐19ASS in the prediction of CAS. The criterion variable (i.e., dependent variable) in the hierarchical regression model was the CAS. The entry order of predictor variables (i.e., independent variables) was the following: age, gender on step 1; BFI‐10 factors found to be correlated with the dependent variable on step 2; perception of being vulnerable to COVID‐19 on step 3; FCV‐19S on step 4; and C‐19ASS Perseveration and C‐19ASS Avoidance on step 5. Results indicated that C‐19ASS Perseveration contributed an additional 4% variance to that explained by all other variables. The final equation indicated that age, BFI‐10‐Emotional stability, perception of being vulnerable to COVID‐19, FCV‐19S and C‐19ASS Perseveration were significant predictors of CAS accounting for a total of 56.3% of the variation in CAS (F = 70.11, df = 9, p < 0.001).
Table 5 shows the hierarchical linear regression examining the incremental validity of the C‐19ASS in the prediction of WSAS. The criterion variable (i.e., dependent variable) in the hierarchical regression model was the WSAS. The entry order of predictor variables (i.e., independent variables) was the following: age, gender on step 1; BFI‐10 factors found to be correlated with the dependent variable on step 2; perception of being vulnerable to COVID‐19 on step 3; FCV‐19S on step 4; and C‐19ASS Perseveration and C‐19ASS Avoidance on step 5. Results indicated that C‐19ASS‐Persevation and C‐19ASS Avoidance did not add a significant variance in the prediction of WSAS to that explained by all other variables. The final equation indicated that BFI‐10‐Conscientiousness, BFI‐10‐Emotional stability, BFI‐10‐Extraversion, FCV‐19 and C‐19ASS Perseveration were predictors of WSAS for a total of 27% of the variation in WSAS scores. (F = 19.02, df = 10, p < 0.001).
5.4. Differences on C‐19ASS on the basis sex, COVID‐19 related variables, and working status
Significant differences were found for gender on C‐19ASS Perseveration (males, mean ± SD = 8.75 ± 5.53 vs. females, mean ± SD = 10.12 ± 5.64; F (df) = 5.31(1), p = 0.022, Welch(df) = 5.43(206.733), p = 0.021), while no statistically significant differences were observed between males and females on C‐19ASS Avoidance (mean ± SD = 5.54 ± 3.88 vs. 6.29 ± 3.79; F (df) = 3.48(1), p = 0.062, Welch(df) = 3.40(198.96), p = 0.067).
When participants tested for COVID‐19 were compared with those not tested for COVID‐19, no statically significant differences were found on C‐19ASS Perseveration (mean ± SD = 9.96 ± 5.52 vs. 9.33 ± 5.90, F (df) = 1.24(1), p = 0.266, Welch(df) = 1.17(243.18), p = 0.28) and on C19‐ASS Avoidance (mean ± SD = 6.08 ± 3.61 vs. 6.16 ± 4.31, F (df) = 0.03(1), p = 0.849, Welch(df) = 0.03(222.57), p = 0.86).
No significant differences were observed between participants who had been diagnosed with COVID‐19 and those who had not been diagnosed with COVID‐19 on C‐19ASS Perseveration (mean ± SD = 11.03 ± 5.47 vs. 9.60 ± 5.64, F (df) = 3.57(1), p = 0.059, Welch(df) = 3.74(83.01), p = 0.056) and on C‐19ASS Avoidance (mean ± SD = 6.32 ± 3.55 vs. 6.07 ± 3.86, F (df) = .22(1), p = 0.637, Welch(df) = 0.25(85.54), p = 0.617).
When participants who know people that had been diagnosed with COVID‐19 were compared with those that did not know people who have been diagnosed with COVID‐19, no statistically significant differences were observed on C‐19ASS Perseveration (mean ± SD = 9.77 ± 5.66 vs. 9.93 ± 5.32, F (df) = 0.02(1), p = 0.880, Welch(df) = 0.02(33.50), p = 0.874) and on C‐19ASS Avoidance (mean ± SD = 6.06 ± 3.82 vs. 6.83 ± 3.79, F (df) = 1.16(1), p = 0.282, Welch(df) = 1.18(33.02), p = 0.285).
No statistically significant differences were observed between participants who had experienced loss as a consequence of COVID‐19 and those who had not on C‐19ASS Perseveration (mean ± SD = 10.19 ± 5.93 vs. 9.70 ± 5.57, F (df) = 0.53(1), p = 0.466, Welch(df) = 0.49(117.77), p = 0.485) and on C‐19ASS Avoidance (mean ± SD = 6.39 ± 3.93 vs. 6.04 ± 3.80, F (df) = 0.564(1), p = 0.453, Welch(df) = 0.53(119.73), p = 0.464).
No statistically significant differences were observed between participants who had been vaccinated from those had not been on C‐19ASS Perseveration (mean ± SD = 9.83 ± 5.48 vs. 9.62 ± 6.20, F (df) = 0.11(1), p = 0.739, Welch(df) = 0.09(145.92), p = 0.757) and on C‐19ASS Avoidance (mean ± SD = 6.15 ± 3.78 vs. 5.95 ± 3.98, F (df) = 0.21(1), p = 0.647, Welch(df) = 0.19(153.33), p = 0.656).
Participants who perceived themselves to be vulnerable to COVID‐19, compared with those who did not perceive themselves to be vulnerable to COVID‐19, reported higher scores on C‐19ASS Perseveration (mean ± SD = 11.67 ± 5.87 vs. 8.00 ± 4.78, F (df) = 57.27(1), p < 0.001, Welch(df) = 5.61(451.78), p < 0.001) and on C‐19ASS Avoidance (mean ± SD = 7.22 ± 3.81 vs. 5.06 ± 3.53, F (df) = 41.89(1), p < 0.001, Welch(df) = 41.70(473.31), p < 0.001).
When health care workers were compared to the general population, no statistically significant differences were found on C‐19ASS Perseveration (mean ± SD = 9.02 ± 5.22 vs. 10.02 ± 5.75, F (df) = 2.72(1), p = 0.099, Welch(df) = 3.02(201.74), p = 0.084), while statistically significant differences were observed on C‐19ASS Avoidance (mean ± SD = 4.95 ± 3.54 vs. 6.46 ± 3.89, F (df) = 13.90(1), p < 0.001, Welch(df) = 16.27(211.89), p < 0.001).
5.5. Mediating role of the Italian C‐19ASS between Big Five personality traits and psychological outcomes in the Italian population
The endogenous variables included in the path analysis (i.e., C‐19ASS Perseveration, C‐19ASS Avoidance, PHQ‐9 and GAD‐7, HAQ) did not follow a multivariate normal distribution (Mardia's skewness and Mardia's kurtosis both showed p < 0.001), sustaining the use of a bootstrap approach. Overall, bivariate correlations between the main variables of the study range from −0.007 to 0.806, indicating that the maximum common variance is 0.65, which is considered a medium coefficient and suggest that variables are distinct from each other. The strongest association (r = 0.806) is observed between PHQ‐9 and GAD‐7, but it is below r = 0.85.
Correlation analyses showed that (1) both the C‐19ASS Perseveration and the C‐19ASS Avoidance were positively correlated with HAQ (C‐19ASS Perseveration: r = 0.521, p < 0.01; C‐19ASS Avoidance r = 0.311, p < 0.01), PHQ‐9 (C‐19ASS Perseveration: r = 0.297, p < 0.01; C‐19ASS Avoidance r = 0.163, p < 0.01), GAD‐7 (C‐19ASS Perseveration: r = 0.334, p < 0.01; C‐19ASS Avoidance r = 0.184, p < 0.01); (2) C‐19ASS Perseveration was negatively correlated with BFI‐10‐Conscientiousness (r = −0.113, p < 0.05) and BFI‐10‐Emotional stability (r = −0.278, p < 0.001); (3) C‐19ASS Avoidance was negatively correlated with BFI‐10‐Emotional stability (r = −0.201, p < 0.001); and (4) all BFI‐10 factors were negatively correlated with HAQ, PHQ‐9, GAD‐7 (r value ranged from −0.559 to −0.171, p < 0.001), expected for BFI‐10 Openness (Table 3).
A first version of the model was tested including all the variables of interest. However, several path coefficients were not significant at the p < 0.05 level and were removed step by step. Therefore, the final model is depicted in Figure 2 and included all the significant paths. In this model, only one personality trait (i.e., BFI‐10‐Emotional Stability) was negatively associated with the two factors of the C‐19ASS (i.e., C‐19ASS Perseveration and C‐19ASS Avoidance). BFI‐10‐Emotional stability was also directly and negatively associated with the three outcomes, whereas BFI‐10‐Conscientiousness was directly and negatively associated with two outcomes (i.e., PHQ‐9 and GAD‐7), and BFI‐10‐Extraversion was negatively and directly associated with PHQ‐9, though very weakly.
FIGURE 2.

Tested model of the inter‐relationships between the study variables. Notes: N= 484; *p < .05; **p < .01, ***p < .001; Gender (0= Male, 1= Female); Health Worker (0=No, 1= Yes); Perceived vulnerability to COVID‐19 (0= No, 1= Yes). BFI‐10= Big Five Inventory‐10; C‐19ASS: COVID‐19 Anxiety Syndrome Scale; PHQ‐9= Patient Health Questionnaire 9;GAD‐7= Generalized Anxiety Disorder 7; HAQ= Health Anxiety Questionnaire
With regard to the COVID‐19 anxiety syndrome, only C‐19ASS Perseveration was associated with the three outcomes (i.e., PHQ‐9, GAD‐7, and HAQ). Regarding the control variables, perception of vulnerability to COVID‐19 was positively associated to both the two mediators, whereas health workers (no vs. yes) were negatively associated to C‐19ASS Avoidance, and to all the three outcomes. Gender (males vs. females) was weakly associated to the three outcomes, whereas age was only weakly and positively associated with GAD‐7.
Along with the direct paths, the mediating role of C‐19ASS Perseveration between BFI‐10‐Emotional stability and the three outcomes were found significant (that is their 95% confidence intervals did not include zero): PHQ‐9 (β = −0.048, b = −0.115 [−0.192 to −0.053], z = −3.195), GAD‐7 (β = −0.055, b = −0.125 [−0.194 to −0.066], z = −3.666), and HAQ (β = −0.109, b = −0.612 [−0.854 to −0.379], z = −5.185).
With regard to the model fit, the model accounted for 17% of the variance of C‐19ASS Perseveration and 14% of C‐19ASS Avoidance, 36% for PHQ‐9, 40% for GAD‐7, and 44% for HAQ. Finally, the total amount variance explained by the model (TCD = 0.59) indicated a very good fit to the observed data. In terms of effect size, TCD = 0.59 corresponds to a correlation of r = 0.77 (which is large effect size according to the Cohen's [Cohen, 1988] traditional criteria).
6. DISCUSSION
The current study aimed to provide a preliminary validation of the Italian version of the C‐19ASS and investigated the association between the COVID‐19 anxiety syndrome and psychological outcomes in an Italian population.
6.1. Validation of the Italian version of C‐19ASS
The EFA revealed that the Italian version of the C‐19ASS is composed by nine items divided in two factors corresponding to the two sub‐scales of perseveration (six items) and avoidance (three items). The CFA confirmed the two factors solution where the two‐factor solution model outperformed the one‐factor solution model. Moreover, the factor structure of the scale was invariant across males and females, allowing to use the C‐19ASS in both gender groups. The final version of the Italian C‐19ASS showed a good fit for the data and satisfactory levels of reliability. These results are consistent with the original version of the C‐19ASS (Nikčević & Spada, 2020) and with a previous C‐19ASS validation study in a general community sample of Iranians (Akbari, Seydavi, et al., 2021).
Concerning convergent validity, correlation analyses revealed that both factors of the C‐19ASS are positively correlated with measures of the COVID‐19 fear (i.e., FVC‐19, Ahorsu et al., 2020) and COVID‐19 anxiety (i.e., CAS; Lee, 2020b), as been found elsewhere (Akbari, Seydavi, et al., 2021; Nikčević & Spada, 2020). However, it should be noted that a high correlation does not indicate similar clinical validity: rating scales may have a common content that ensures a positive association, but they may display differential validity (Carrozzino et al., 2021). In addition, correlation coefficients are often of statistical but not of clinical significance (Carrozzino et al., 2021). Therefore, caution should be paid when interpreting these results.
Concerning the incremental validity, hierarchical linear regression analyses showed that C‐19ASS Perseveration added significant additional variance in the prediction of COVID‐19 anxiety (i.e., CAS, Lee, 2020b) over and above age, the Big Five personality traits, perception of being vulnerable to COVID‐19 and COVID‐19 fear, as been found elsewhere (Akbari, Seydavi, et al., 2021; Nikčević & Spada, 2020). With regard to the incremental validity of the C‐19ASS in the prediction of functional impairment (i.e., WSAS; Mundt et al., 2002) although C‐19ASS Perseveration was found to predict the WSAS, consistently with previous studies (Akbari, Seydavi, et al., 2021; Nikčević & Spada, 2020), it did not add a significant variance in the prediction of WSAS to that explained by all other variables. The Italian version of the C‐19ASS showed good fit for the data and satisfactory levels of reliability and concurrent validity, although further studies are required to explore in depth the incremental validity.
6.2. COVID‐19 anxiety syndrome: differences on the basis of sex, COVID‐19 related variables, and working status
Exploring gender differences related to C‐19ASS our findings suggested that females had higher levels of C‐19ASS Perseveration than males, consistently to what has been found in an Iranian general community sample (Akbari, Seydavi, et al., 2021). A possible explanation for this result may lie with previous findings, which have suggested that females, compared to males, are more likely to engage in specific forms of perseverative thinking such as worry (Dugas et al., 1997; Dugas et al., 2001; McCann et al., 1991; Robichaud et al., 2003; Stavosky & Borkovec, 1988).
Consistently with a previous study (Akbari, Seydavi, et al., 2021), we found that participants who perceived themselves to be vulnerable to the COVID‐19, compared with those who did not, had higher levels of C‐19ASS Perseveration and C‐19ASS Avoidance. Being the construct of the COVID‐19 anxiety syndrome conceptually aligned with the Self‐Regulatory Executive Function model (S‐REF) (Wells & Matthews, 1994, 1996), within this theoretical frame, it may be purported that those who perceive themselves to be vulnerable to the COVID‐19 may also hold beliefs about the need to control thinking (metacognitive beliefs) in response to COVID‐19 fear (Akbari, Spada, et al., 2021; Aydın et al., 2021), that in turn, might increase the likelihood of using dysfunctional coping strategies (Akbari, Spada, et al., 2021; Wells & Matthews, 1996) such as C‐19ASS Perseveration and C‐19ASS Avoidance. However, the lack of studies exploring this hypothesis prevents us to draw firm conclusions about the relationship between the perception of vulnerability to COVID‐19 and the COVID‐19 anxiety syndrome.
Moreover, our findings suggested that those diagnosed with COVID‐19 and those who had not been diagnosed with COVID‐19 did not differ in terms of the COVID‐19 anxiety syndrome. This finding is in contrast to that of Håkansson and Claesdotter (2021) who found higher levels of fear of COVID‐19 in those not diagnosed with COVID‐19 than in those who had had a COVID‐19 diagnosis. However, this discrepancy between our results and what was observed by Håkansson and Claesdotter (2021) might be based on a conceptual difference between the COVID‐19 anxiety syndrome and COVID‐19 fear (Nikčević & Spada, 2020).
Furthermore, we did not find any significant differences on the C‐19ASS between participants who had experienced a loss as a consequence of COVID‐19 and those who had not experienced a loss as a consequence of COVID‐19, as well as between participants who had been vaccinated for COVID‐19 and those who had not been vaccinated for COVID‐19. This could be explained by the fact that neither the close death due to COVID‐19 nor the vaccination status may make COVID‐19 related stimuli remarkably salient (Albery et al., 2021). Albery et al. (2021) observed that both close death due to COVID‐19 and vaccination status were not associated with an increased attentional bias to COVID‐19‐related stimuli, suggesting that these variables may be not important in describing the way of elaboration of relevant COVID‐19‐related stimuli by the attentional system.
Finally, exploring differences on C‐19ASS on the basis of work status, we found that health care workers had lower levels of C‐19ASS Avoidance than the general population. This could be explained by the fact that during COVID‐19 pandemic health care workers, due to their role in tackling the COVID‐19 pandemic (Busch et al., 2021; Theorell, 2020), have preserved their full/normal functioning (e.g., spending more time outside home, going to work, using public transport, social relationship and being exposed to subjects infected by COVID‐19) (Bielicki et al., 2020; Mansueto et al., 2021; Peng et al., 2021; Zhang et al., 2020). By contrast, in the general population the restrictions released to limit the spread of COVID‐19 (e.g., the closure of school, shifting to on‐line learning and working from home) (Mansueto et al., 2021; Viner et al., 2020) may have increased the use of dysfunctional coping strategies as C‐19ASS Avoidance. With regard to C‐19ASS Perseveration, no significant differences were observed between health care workers and the general population. This finding is consistent to previous studies showing an increased level of worry during the COVID‐19 pandemic in both healthcare workers and the general population (Busch et al., 2021; Cosci & Guidi, 2021; Mansueto et al., 2021; Wahlund et al., 2021).
6.3. The mediating role of COVID‐19 anxiety syndrome in the association between Big Five personality traits and psychological symptoms
We tested a model where we hypothesized that the COVID‐19 anxiety syndrome would mediate the relationship between Big Five personality traits and psychological outcomes (i.e., depression, generalized anxiety and health anxiety) (see Figure 1). The path analyses of our hypothesized model and the amount of variance explained revealed that it fits the data well, suggesting that the proposed model may be of value. Specifically, in the model we observed that (1) the Big Five personality traits (i.e., conscientiousness, emotional stability and extraversion) appear to be negatively associated with psychological symptoms; (2) emotional stability is negatively associated with C‐19ASS Perseveration and C‐19ASS Avoidance; and (3) C‐19ASS Perseveration may play a mediating role in the relationship between emotional stability and psychological symptoms, while, C‐19ASS Avoidance does not.
The association between Big Five personality traits (i.e., conscientiousness and extraversion emotional stability) and psychological symptoms is well established. Our findings confirm previous observations of conscientiousness being a protective factor for both depression and generalized anxiety (Koorevaar et al., 2017), and extraversion being a protective factor for depression (Akbari, Seydavi, et al., 2021; Lyon et al., 2021; Koorevaar et al., 2017), and emotional stability being a protective factor for depression, generalized anxiety and health anxiety (Akbari, Seydavi, et al., 2021; Jylhä & Isometsä, 2006; Nikčević et al., 2021). With regard the association between Big Five personality traits and C‐19ASS, as been observed elsewhere (Akbari, Seydavi, et al., 2021; Nikčević et al., 2021), lower emotional stability may be a vulnerability factor for C‐19ASS Perseveration and C‐19ASS Avoidance.
With regard to the association between C‐19ASS and psychological outcomes our findings confirm the vulnerability role of C‐19ASS Perseveration for depression, generalized anxiety and health anxiety (Albery et al., 2021; Akbari, Seydavi, et al., 2021; Nikčević et al., 2021; Nikčević & Spada, 2020), on the other hand, no significant associations were found between C‐19ASS Avoidance and psychological outcomes. It possible to suppose that C‐19ASS Perseveration may be more harmful than C‐19ASS Avoidance or that the latter was not being ‘tested’ as lockdowns and measures to contain the virus allowed for generally avoidant behaviour (i.e., recommendations not to travel, to clean one's hands and to wear masks). However, the present study is the first to explore the mediating role of the two components of C‐19ASS in the association between Big Five personality traits and psychological outcomes. Thus, the lack of studies investigating this issue prevents us to draw firm conclusions about the potential differences between C‐19ASS Perseveration and C‐19ASS Avoidance.
6.4. Clinical implications
The Italian version of the C‐19ASS may be a useful tool for clinicians to identify COVID‐19 dysfunctional coping strategies (i.e., perseveration and avoidance) that may aggravate health outcomes. Rehabilitative efforts could focus on reducing such dysfunctional coping strategies and in promoting alternative styles of thinking and behaviours that would attenuate the COVID‐19 anxiety syndrome and enhance psychological re‐adjustment (Nikčević & Spada, 2020). Treatments aimed at interrupting perseverative thinking (e.g., metacognitive therapy; Wells, 2000), reducing checking, safety behaviours, and avoidance (e.g., graded exposure and response prevention; Barlow et al., 2014) and training and recalibrating attention (e.g., attention training technique; Wells, 2000) may all help to weaken the COVID‐19 anxiety syndrome, as well as, to reduce the longer term occurrence of psychological symptoms typically linked to pandemic events, such as depression, generalized anxiety and health anxiety.
6.5. Limitations
Results of this study must be considered with regard to its limitations. Firstly, the participants in this study may not have been representative of the general population as the sample was self‐selected. Secondly, a cross‐sectional design was adopted, and this precludes drawing conclusions as to whether or not Big Five personality traits and the COVID‐19 anxiety syndrome play a causal role in predicting psychological symptoms. Thirdly, social desirability, self‐report biases, context effects and poor recall may have contributed to errors in self‐report measurements.
Fourthly, a high proportion of females. The employment of a longitudinal study designs and ensuring a more diverse sample of participants are warranted.
7. CONCLUSION
The Italian version of the C‐19ASS is a measure that could prove useful in better understanding the developing COVID‐19 anxiety syndrome and its impact on psychological symptoms. The COVID‐19 anxiety syndrome could be a suitable therapeutic target to reduce psychological symptoms related to the COVID‐19 pandemic.
CONFLICT OF INTEREST
Two of the authors were involved in developing the original version of the C19‐ASS for English‐speaking populations. The authors have no known competing financial interests or personal relationships that could have influenced this work.
Appendix A. ITALIAN VERSION OF THE COVID‐19 ANXIETY SYNDROME SCALE (C‐19ASS ITA)
Di seguito sono elencate una serie di affermazioni riguardanti il modo in cui le persone affrontano la minaccia del coronavirus (COVID‐19). Per favore valuta la misura in cui ciascuna affermazione si applica a lei nelle ultime due settimane.
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorn
-
Ho evitato di usare i mezzi di trasporto pubblici a causa della paura di contrarre il coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Mi sono controllato per i sintomi del coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Ho evitato di uscire in luoghi pubblici (negozi, parchi) a causa della paura di contrarre il coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Sono stato preoccupato per non aver aderito rigorosamente alle linee guida sul distanziamento sociale per il coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Ho evitato di toccare oggetti nei luoghi pubblici a causa della paura di contrarre il coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Ho letto di notizie legate al coronavirus (COVID‐19) compromettendo l'impegno nel lavoro (ad esempio scrivere email, lavorare su documenti di testo o fogli di calcolo).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Ho controllato i segni del coronavirus (COVID‐19) nei membri della mia famiglia e nella persona amata.
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Ho prestato molta attenzione alle persone che mostravano possibili sintomi del coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
-
Ho immaginato cosa potrebbe succedere ai membri della mia famiglia se avessero contratto il coronavirus (COVID‐19).
0 = Per niente
1 = Raramente, meno di un giorno o due
2 = Diversi giorni
3 = Più di 7 giorni
4 = Quasi ogni giorno
Mansueto, G. , Palmieri, S. , Marino, C. , Caselli, G. , Sassaroli, S. , Ruggiero, G. M. , Nikčević, A. V. , & Spada, M. M. (2022). The Italian COVID‐19 Anxiety Syndrome Scale: Investigation of the COVID‐19 anxiety syndrome and its association with psychological symptoms in an Italian population. Clinical Psychology & Psychotherapy, 1–19. 10.1002/cpp.2767
Funding information
This research received no specific grant from any funding agency, commercial or not‐for‐profit sectors.
DATA AVAILABILITY STATEMENT
The data of this study are available from the corresponding author, upon request.
REFERENCES
- Ahorsu, D. K. , Lin, C. Y. , Imani, V. , Saffari, M. , Griffiths, M. D. , & Pakpour, A. H. (2020). The Fear of COVID‐19 Scale: Development and Initial Validation. Intenational Journal of Mental Health and Addiction, 27, 1–9. 10.1007/s11469-020-00270-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akbari, M. , Seydavi, M. , Zamani, E. , Nikčević, A. V. , & Spada, M. M. (2021). The Persian COVID‐19 Anxiety Syndrome Scale (C‐19ASS): Psychometric properties in a general community sample of Iranians. Clinical Psycholy & Psychothery. 10.1002/cpp.2686 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Akbari, M. , Spada, M. M. , Nikčević, A. V. , & Zamani, E. (2021). The relationship between fear of COVID‐19 and health anxiety among families with COVID‐19 infected: The mediating role of metacognitions, intolerance of uncertainty, and emotion regulation. Clinical Psychology & Psychotherapy, 28(6), 1354–1366. 10.1002/cpp.2628 [DOI] [PubMed] [Google Scholar]
- Albery, I. P. , Spada, M. M. , & Nikčević, A. V. (2021). The COVID‐19 anxiety syndrome and selective attentional bias towards COVID‐19‐related stimuli in UK residents during the 2020–2021 pandemic. Clinical Psycholy & Psychothery, 28(6), 1367–1378. 10.1002/cpp.2639 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alzueta, E. , Perrin, P. , Baker, F. C. , Caffarra, S. , Ramos‐Usuga, D. , Yuksel, D. , Arango‐Lasprilla, J. C. , & Lasprilla, J. C. (2021). How the COVID‐19 pandemic has changed our lives: A study of psychological correlates across 59 countries. Journal of clinical psychology, 77(3), 556–570. 10.1002/jclp.23082 [DOI] [PubMed] [Google Scholar]
- Amsalem, D. , Lazarov, A. , Markowitz, J. C. , Dixon, L. B. , & Neria, Y. (2021). Psychiatric symptoms and moral injury among US healthcare workers in the COVID‐19 era. BMC Psychiatry, 21(1), 546. 10.1186/s12888-021-03565-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arslan, G. , Yıldırım, M. , Tanhan, A. , Buluş, M. , & Allen, K. A. (2021). Coronavirus stress, optimism‐pessimism, psychological inflexibility, and psychological health: Psychometric properties of the Coronavirus Stress Measure. International Journal of Mental Health and Addiction, 19(6), 2423–2439. 10.1007/s11469-020-00337-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aydın, O. , Balıkçı, K. , Arslan, Y. , Ünal‐Aydın, P. , Müezzin, E. , & Spada, M. M. (2021). The Combined Contribution of Fear and Perceived Danger of COVID‐19 and Metacognitions to Anxiety Levels during the COVID‐19 Pandemic. Journal of Rational‐Emotive & Cognitive‐Behavior Therapy, 6, 1–15. 10.1007/s10942-021-00429-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barbaranelli, C. , & D'Olimpio, F. (2006). Analisi dei dati con SPSS (1st ed., Vol. 2). [Google Scholar]
- Barlow, D. H. , Sauer‐Zavala, S. , Carl, J. R. , Bullis, J. R. , & Ellard, K. K. (2014). The nature, diagnosis, and treatment of neuroticism: Back to the future. Clinical Psychology Science, 2, 344–365. 10.1177/2167702613505532 [DOI] [Google Scholar]
- Bartlett, M. S. (1937). Properties of sufficiency and statistical tests. Proceedings of the Royal Statistical Society, Series A, 160, 268–282. 10.1098/rspa.1937.0109 [DOI] [Google Scholar]
- Bassi, F. , Arbia, G. , & Falorsi, P. D. (2021). Observed and estimated prevalence of Covid‐19 in Italy: How to estimate the total cases from medical swabs data. Science of the Total Environment, 764, 142799. 10.1016/j.scitotenv.2020.142799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beaujean, A. A. , Freeman, M. J. , Youngstrom, E. , & Carlson, G. (2012). The structure of cognitive abilities in youths with manic symptoms: A factorial invariance study. Assessment, 19, 462–471. 10.1177/1073191111399037 [DOI] [PubMed] [Google Scholar]
- Bielicki, J. A. , Duval, X. , Gobat, N. , Goossens, H. , Koopmans, M. , Tacconelli, E. , & van der Werf, S. (2020). Monitoring approaches for health‐care workers during the COVID‐19 pandemic. The Lancet Infectious Diseases, 20(10), e261–e267. 10.1016/S1473-3099(20)30458-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bollen, K. A. (1989). Structural equations with latent variables. Wiley. [Google Scholar]
- Bowerman, B. L. , & O'Connell, R. T. (1990). Linear statistical models: An applied approach (2nd ed.). Duxbury. [Google Scholar]
- Brailovskaia, J. , Cosci, F. , Mansueto, G. , & Margraf, J. (2021). The relationship between social media use, stress symptoms and burden caused by Coronavirus (Covid‐19) in Germany and Italy: A cross‐sectional and longitudinal investigation. Journal of Affective Disorders Reports, 3, 100067. 10.1016/j.jadr.2020.100067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brailovskaia, J. , Cosci, F. , Mansueto, G. , Miragall, M. , Herrero, R. , Baños, R. M. , Krasavtseva, Y. , Kochetkov, Y. , & Margraf, J. (2021). The association between depression symptoms, psychological burden caused by Covid‐19 and physical activity: An investigation in Germany, Italy, Russia, and Spain. Psychiatry Research, 295, 113596. 10.1016/j.psychres.2020.113596 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Browne, M. W. , & Cudeck, R. (1993). Alternative ways of assessing model fit. In Bollen K. A. & Long J. S. (Eds.), Testing structural equation models (pp. 136–162). Sage. [Google Scholar]
- Busch, I. M. , Moretti, F. , Mazzi, M. , Wu, A. W. , & Rimondini, M. (2021). What we have learned from two decades of epidemics and pandemics: a systematic review and meta‐analysis of the psychological burden of frontline healthcare workers. Psychotherapy and Psychosomatics, 90(3), 178–190. 10.1159/000513733 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carrozzino, D. , Patierno, C. , Guidi, J. , Montiel, C. B. , Cao, J. , Charlson, M. E. , & Fava, G. A. (2021). Clinimetric criteria for patient‐reported outcome measures. Psychotherapy and Psychosomatics, 90(4), 222–232. 10.1159/000516599 [DOI] [PubMed] [Google Scholar]
- Cattell, R. B. (1966). The scree test for the number of factors. Multivariate Behavioral Research, 1(2), 245–276. 10.1207/s15327906mbr0102_10 [DOI] [PubMed] [Google Scholar]
- Cheung, G. W. , & Rensvold, R. B. (2002). Evaluating goodness of‐fit indexes for testing measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal, 9, 233–255. 10.1207/S15328007SEM0902_5 [DOI] [Google Scholar]
- Cohen, J. (1988). Statistical power analysis for behavioral science (2nd ed.). Erlbaum. [Google Scholar]
- Conway, L. G. III , Woodard, S. R. , & Zubrod, A. (2020). Social psychological measurements of COVID‐19: Coronavirus perceived threat, government response, impacts, and experiences questionnaires. PsyArXiv. 10.31234/osf.io/z2x9aDe [DOI] [Google Scholar]
- Cosci, F. , & Guidi, J. (2021). The role of illness behavior in the COVID‐19 pandemic. Psychotherapy and Psychosomatics, 90(3), 156–159. 10.1159/000513968 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costello, A. B. , & Osborne, J. (2005). Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Practical Assessment, Research and Evaluation, 10(1), 1–9. 10.7275/jyj1-4868 [DOI] [Google Scholar]
- Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika, 16, 297–334. [Google Scholar]
- Davis, M. , Gilbar, O. , & Padilla‐Medina, D. M. (2021). Intimate partner violence victimization and perpetration among U.S. adults during the earliest stage of the COVID‐19 Pandemic. Violence and Victims, 36(5), 583–603. 10.1891/VV-D-21-00005 [DOI] [PubMed] [Google Scholar]
- Duffy, B. , & Allington, D. (2020). The Trusting, the Dissenting and the Frustrated: how the UK is dividing as lockdown is eased. Kings' College London Policy Institute. https://www.kcl.ac.uk/policy-institute/assets/how-the-uk-is-dividing-as-the-lockdown-is-eased.pdf [Google Scholar]
- Dugas, M. J. , Freeston, M. H. , & Ladouceur, R. (1997). Intolerance of uncertainty and problem orientation in worry. Cognitive Therapy and Research, 21(6), 593–606. 10.1023/A:1021890322153 [DOI] [Google Scholar]
- Dugas, M. J. , Gosselin, P. , & Ladouceur, R. (2001). Intolerance of uncertainty and worry: Investigating specificity in a nonclinical sample. Cognitive Therapy and Research, 25(5), 551–558. 10.1023/A:1005553414688 [DOI] [Google Scholar]
- Emmelkamp, P. M. (2021). Psychological consequences of COVID‐19. Clinical Psychology & Psychotherapy, 28(6), 1315–1316. 10.1002/cpp.2701 [DOI] [PubMed] [Google Scholar]
- Field, A. (2013). Discovering statistics using IBM SPSS statistics (4th ed.). London. [Google Scholar]
- Fitzpatrick, K. M. , Drawve, G. , & Harris, C. (2020). Facing new fears during the COVID‐19 pandemic: The State of America's mental health. Journal of Anxiety Disorders, 75, 102291. 10.1016/j.janxdis.2020.102291 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fornell, C. , & Larcker, D. F. (1981). Evaluating structural equation models with unobservable variables and measurement error. Journal of Marketing Research, 18, 39–50. 10.2307/3151312 [DOI] [Google Scholar]
- Gravetter, F. J. , & Wallnau, L. B. (2016). Statistics for the behavioral sciences. Cengage Learning. [Google Scholar]
- Guido, G. , Peluso, A. M. , Capestro, M. , & Miglietta, M. (2015). An Italian version of the 10‐item Big Five Inventory: An application to hedonic and utilitarian shopping values. Personality and Individual Differences, 76, 135–140. 10.1016/j.paid.2014.11.053 [DOI] [Google Scholar]
- Hair, J. , Black, W. , Babin, B. , & Anderson, R. (2010). Multivariate data analysis (7th ed.). Prentice‐Hall, Inc. Upper Saddle River NJ. [Google Scholar]
- Hair, J. F. , Anderson, R. E. , Tatham, R. L. , & Black, W. C. (1998). Multivariate Data Analysis (5th ed.). USA. [Google Scholar]
- Håkansson, A. , & Claesdotter, E. (2021). Fear of COVID‐19, compliance with recommendations against virus transmission, and attitudes towards vaccination in Sweden. Heliyon, e08699. 10.1016/j.heliyon.2021.e08699 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika, 30, 179–185. 10.1007/BF02289447 [DOI] [PubMed] [Google Scholar]
- Hu, L. T. , & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- Jylhä, P. , & Isometsä, E. (2006). The relationship of neuroticism and extraversion to symptoms of anxiety and depression in the general population. Depression and Anxiety, 23(5), 281–289. 10.1002/da.20167 [DOI] [PubMed] [Google Scholar]
- Jӧreskog, K. G. , & Sӧrbom, D. (1996). LISREL 8: User's reference guide. Scientific Software International. [Google Scholar]
- Kaiser, H. F. (1970). A second generation little jiffy. Psychometrika, 35(4), 401–415. 10.1007/BF02291817 [DOI] [Google Scholar]
- Koorevaar, A. M. L. , Hegeman, J. M. , Lamers, F. , Dhondt, A. D. F. , Van der Mast, R. C. , Stek, M. L. , & Comijs, H. C. (2017). Big Five personality characteristics are associated with depression subtypes and symptom dimensions of depression in older adults. International Journal of Geriatric Psychiatry, 32(12), e132–e140. 10.1002/gps.4670 [DOI] [PubMed] [Google Scholar]
- Kroenke, K. , Spitzer, R. L. , & Williams, J. B. (2001). The PHQ‐9: validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. 10.1046/j.1525-1497.2001.016009606.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lebrasseur, A. , Fortin‐Bédard, N. , Lettre, J. , Raymond, E. , Bussières, E. L. , Lapierre, N. , Faieta, J. , Vincent, C. , Duchesne, L. , Ouellet, M.‐C. , Gagnon, E. , Tourigny, A. , & Routhier, F. (2021). Impact of the COVID‐19 pandemic on older adults: rapid review. JMIR aging, 4(2), e26474. 10.2196/26474 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, S. A. (2020a). How much “Thinking” about COVID‐19 is clinically dysfunctional? Brain, Behavior, and Immunity, 87, 97–98. 10.1016/j.bbi.2020.04.067 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, S. A. (2020b). Coronavirus Anxiety Scale: A brief mental health screener for COVID‐19 related anxiety. Death Studies, 44(7), 393401. 10.1080/07481187.2020.1748481 [DOI] [PubMed] [Google Scholar]
- Li, Q. , Guan, X. , Wu, P. , Wang, X. , Zhou, L. , & Tong, Y. (2020). Early transmission dynamics in Wuhan, China, of novel coronavirus‐infected pneumonia. The New England Journal of Medicine, 382(13), 1199–1207. 10.1056/NEJMoa2001316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucock, M. P. , & Morley, S. (1996). The health anxiety questionnaire. British Journal of Health Psychology, 1(2), 137–150. 10.1111/j.2044-8287.1996.tb00498.x [DOI] [Google Scholar]
- Lyon, K. A. , Elliott, R. , Ware, K. , Juhasz, G. , & Brown, L. J. E. (2021). Associations between facets and aspects of big five personality and affective disorders: a systematic review and best evidence synthesis. Journal of Affective Disorders, 288, 175–188. 10.1016/j.jad.2021.03.061 [DOI] [PubMed] [Google Scholar]
- Manea, L. , Gilbody, S. , & McMillan, D. (2015). A diagnostic meta‐analysis of the Patient Health Questionnaire‐9 (PHQ‐9) algorithm scoring method as a screen for depression. General Hospital Psychiatry, 37(1), 67–75. 10.1016/j.genhosppsych.2014.09.009 [DOI] [PubMed] [Google Scholar]
- Mansueto, G. , Lopes, F. L. , Grassi, L. , & Cosci, F. (2021). Impact of COVID‐19 outbreak on Italian healthcare workers versus general population: Results from an online survey. Clinical Psychology & Psychotherapy, 28(6), 1334–1345. 10.1002/cpp.2644 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mazzotti, E. , Fassone, G. , Picardi, A. , Sagoni, E. , Ramieri, L. , Lega, I. , Camaioni, D. , Abeni, D. , & Pasquini, P. (2003). II Patient Health Questionnaire (PHQ) per lo screening dei disturbi psichiatrici: Uno studio di validazione nei confronti della Intervista Clinica Strutturata per il DSM‐IV asse I (SCID‐I). Italian Journal of Psychopathology, 9(3), 235–242. [Google Scholar]
- McCann, S. J. W. , Stewin, L. L. , & Short, R. H. (1991). Sex differences, social desirability, masculinity, and the tendency to worry. The Journal of Genetic Psychology, 152, 295–301. 10.1080/00221325.1991.9914687 [DOI] [PubMed] [Google Scholar]
- Melli, G. , Coradeschi, D. , & Smurra, R. (2007). The Italian version of Health Anxiety Questionnaire: reliability and factorial analysis. Psicoterapia Cognitivo e Comportamentale, 13, 37–48. [Google Scholar]
- Mozzoni, M. , & Franzot, E. (2020). Coronavirus Anxiety Scale (CAS). Department of Psychology Christopher Newport University. [Google Scholar]
- Mundt, J. C. , Marks, I. M. , Shear, M. K. , & Greist, J. H. (2002). The work and social adjustment scale: a simple accurate measure of impairment in functioning. British Journal of Psychiatry, 180, 461–464. 10.1192/bjp.180.5.461 [DOI] [PubMed] [Google Scholar]
- Myers, R. (1990). Classical and modern regression with applications (2nd ed.). Duxbury. [Google Scholar]
- Nikčević, A. V. , Marino, C. , Kolubinski, D. C. , Leach, D. , & Spada, M. M. (2021). Modelling the contribution of the Big Five personality traits, health anxiety, and COVID‐19 psychological distress to generalised anxiety and depressive symptoms during the COVID‐19 pandemic. Journal of Affective Disorders, 279, 578–584. 10.1016/j.jad.2020.10.053 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nikčević, A. V. , & Spada, M. M. (2020). The COVID‐19 anxiety syndrome scale: Development and psychometric properties. Psychiatry Research, 292, 113322. 10.1016/j.psychres.2020.113322 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peng, M. , Wang, L. , Xue, Q. , Yin, L. , Zhu, B. H. , Wang, K. , … Wang, H. X. (2021). Post‐COVID‐19 epidemic: allostatic load among medical and nonmedical workers in China. Psychotherapy and Psychosomatics, 90(2), 127–136. 10.1159/000511823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- R Development Core Team . (2017). R: A language and environment for statistical computing. R Foundation for Statistical Computing. ISBN 3–900051–07‐0. http://www.R-project.org/ [Google Scholar]
- Rammstedt, B. , & John, O. P. (2007). Measuring personality in one minute or less: A 10‐item short version of the Big Five inventory in English and German. Journal of Research in Personality, 41, 203–212. 10.1016/j.jrp.2006.02.001 [DOI] [Google Scholar]
- Robichaud, M. , Dugas, M. J. , & Conway, M. (2003). Gender differences in worry and associated cognitive‐behavioral variables. Anxiety Disorders, 17, 501–516. 10.1016/S0887-6185(02)00237-2 [DOI] [PubMed] [Google Scholar]
- Rosseel, Y. (2012). Lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48, 1–36. 10.18637/jss.v048.i02 [DOI] [Google Scholar]
- Satorra, A. , & Bentler, P. M. (1994). Corrections to test statistics and standard errors in covariance structure analysis. In Von Eye A. & Clogg C. C. (Eds.), Latent variable analysis. Applications for developmental research (pp. 399–419). Sage. [Google Scholar]
- Soraci, P. , Ferrari, A. , Abbiati, F. A. , Del Fante, E. , De Pace, R. , Urso, A. , & Griffiths, M. D. (2020). Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID‐19 Scale. International Journal of Mental Health and Addiction, 4, 1–10. 10.1007/s11469-020-00277-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sousa, V. D. , & Rojjanasrirat, W. (2011). Translation, adaptation and validation of instruments or scales for use in cross‐cultural health care research: A clear and user‐friendly guideline. Journal of Evaluation in Clinical Practice, 17(2), 268–274. 10.1111/j.13652753.2010.01434.x [DOI] [PubMed] [Google Scholar]
- Spitzer, R. L. , Kroenke, K. , Williams, J. B. , & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: the GAD‐7. Archives of Internal Medicine, 166(10), 1092–1097. 10.1001/archinte.166.10.1092 [DOI] [PubMed] [Google Scholar]
- Stavosky, J. M. , & Borkovec, T. D. (1988). The phenomenon of worry: theory, research, treatment and its implications for women. Women & Therapy, 6, 77–95. 10.1300/J015V06N03_07 [DOI] [Google Scholar]
- Taylor, S. (2019). The psychology of pandemics: Preparing for the next global outbreak of infectious disease. Cambridge Scholars Publishing. [Google Scholar]
- Taylor, S. , Landry, C. A. , Paluszek, M. M. , Fergus, T. A. , McKay, D. , & Asmundson, G. J. (2020). Development and initial validation of the COVID Stress Scales. Journal of Anxiety Disorders, 72, 102232. 10.1016/j.janxdis.2020.102232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taylor, S. , Paluszek, M. M. , Rachor, G. S. , McKay, D. , & Asmundson, G. J. (2021). Substance use and abuse, COVID‐19‐related distress, and disregard for social distancing: A network analysis. Addictive Behaviors, 114, 106754. 10.1016/j.addbeh.2020.106754 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Theorell, T. (2020). COVID‐19 and working conditions in health care. Psychotherapy and Psychosomatics, 89(4), 193–194. 10.1159/000507765 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van de Schoot, R. , Lugtig, P. , & Hox, J. (2012). A checklist for testing measurement invariance. European Journal of Developmental Psychology, 9, 486–492. 10.1080/17405629.2012.686740 [DOI] [Google Scholar]
- Viner, R. M. , Russell, S. J. , Croker, H. , Packer, J. , Ward, J. , Stansfield, C. , Mytton, O. , Bonell, C. , & Booy, R. (2020). School closure and management practices during coronavirus outbreaks including COVID‐19: A rapid systematic review. The Lancet Child & Adolescent Health, 4(5), 397–404. 10.1016/S2352-4642(20)30095-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wahlund, T. , Mataix‐Cols, D. , Lauri, K. O. , de Schipper, E. , Ljótsson, B. , Aspvall, K. , & Andersson, E. (2021). Brief online cognitive behavioural intervention for dysfunctional worry related to the COVID‐19 pandemic: a randomised controlled trial. Psychotherapy and Psychosomatics, 90(3), 191–199. 10.1159/000512843 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wells, A. (2000). Emotional disorders and metacognition: Innovative cognitive therapy. Wiley. [Google Scholar]
- Wells, A. , & Matthews, G. (1994). Attention and emotion: A clinical perspective. Erlbaum. [Google Scholar]
- Wells, A. , & Matthews, G. (1996). Modelling cognition in emotional disorder: The S‐REF model. Behaviour Research and Therapy, 34(11–12), 881–888. 10.1016/S0005-7967(96)00050-2 [DOI] [PubMed] [Google Scholar]
- World Health Organization . (2022). Retrieved, January 24, 2022 Available from https://covid19.who.int/
- Zhang, W. R. , Wang, K. , Yin, L. , Zhao, W. F. , Xue, Q. , Peng, M. , Min, B.‐Q. , Tian, Q. , Leng, H.‐X. , Du, J.‐L. , Chang, H. , Yang, Y. , Li, W. , Shangguan, F.‐F. , Yan, T.‐Y. , Dong, H.‐Q. , Han, Y. , Wang, Y.‐P. , Cosci, F. , & Wang, H. X. (2020). Mental health and psychosocial problems of medical health workers during the COVID‐19 epidemic in China. Psychotherapy and Psychosomatics, 89(4), 242–250. 10.1159/000507639 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data of this study are available from the corresponding author, upon request.