

Abstract
Objectives
To investigate the associations between physical activity pattern, sports participation, screen time and mental health in Swedish adolescents.
Design, setting and participants
A total of 1139 Swedish adolescents (mean age 13.4) from 34 schools participated in the cross-sectional study ‘Physical Activity for Healthy Brain Functions in School Youth’ in 2019.
Methods
Time spent sedentary and in moderate-to-vigorous physical activity (MVPA) was measured using accelerometers for seven consecutive days. Screen time and sports participation were self-reported. Anxiety and health-related quality of life (HRQoL) were assessed using a Short version of the Spence Children’s Anxiety Scale and Kidscreen-10.
Results
MVPA was positively associated (95% CI 0.01 to 0.05 in girls and 0.02 to 0.07 in boys) whereas screen time on weekdays was inversely associated with HRQoL (−4.79 to –2.22 in girls and −2.66 to –0.41 in boys). The largest effect sizes were observed between the high/low MVPA group in boys (Cohen’s d=0.51) and screen time groups in girls (Cohen’s d=0.59 on weekdays). With regards to anxiety, high compared with lower time spent in MVPA during leisure time on weekdays was associated with lower anxiety scores (95% CI −0.13 to –0.05 in girls and −0.07 to –0.01 in boys). Gender differences were observed, boys who participated in organised sports had low anxiety scores (95% CI −3.49 to –0.13) whereas girls who reported 5 hours or more of screen time had high scores (95% CI 1.94 to 6.18 on weekdays and 1.39 to 5.29 on weekend days).
Conclusions
This study showed that MVPA was associated with better mental health, whereas the opposite was seen for screen time. These associations were not consistently significant throughout all time domains, between the genders and mental health outcomes. Our results could create a paradigm for future studies to decide which types of PA patterns and time domains to target in intervention studies with the aim improve mental health among adolescents.
Keywords: Child & adolescent psychiatry, PUBLIC HEALTH, Community child health, Anxiety disorders, MENTAL HEALTH
Strengths and limitations of this study.
Physical activity and sedentary time were assessed using accelerometers.
The study included both positive and negative indicators of mental health.
Due to the cross-sectional design causation or the direction of these associations cannot be studied.
Introduction
The WHO describes health as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’.1 Thus, mental health is an important component of health and includes both positive indicators (eg, well-being) and negative indicators (eg, psychiatric symptoms). Poor mental health among youth is a global public health concern with major consequences for both individuals and society.2 Mental disorders at an early age have been associated with stigma, decreased academic achievements, increased risk of physical disorders in adulthood and premature death.3 The age of onset for approximately half of the mental disorders occurs before or during adolescence,4 with anxiety being the most common mental disorder with a prevalence of 6.5%.5 Therefore, it is important to investigate how modifiable lifestyle factors are associated with mental health in this population.
Physical activity (PA) has been found to be a protective factor for emotional problems6 and high levels of PA have cross-sectionally been associated with better mental health outcomes.7–10 Studies have also shown a lower prevalence of depressive symptoms in those engaging in organised sports compared with those being active on their own,11 12 suggesting that the context of activity could be important. However, the majority of adolescents do not meet the PA recommendations of 60 min of moderate-to-vigorous physical activity (MVPA) per day.13 A study on Swedish adolescents (11–18 years old) found that only 23% of girls and 43% of boys met the recommendations.14 In addition, sedentary behaviours, especially screen time have been associated with poor mental health.15 16
Although these associations have been studied before, most studies rely on self-reported PA,10 which has shown to have low validity in this population.17 A more robust measure is device-measured PA that provides a more detailed estimate of PA and sedentary time (SED). There is also a lack of studies that include both positive and negative indicators of mental health, with a tendency to focus on mental health disorders or symptoms. In this study, we chose health-related quality of life (HRQoL) as a positive indicator and anxiety as a negative indicator. Anxiety (rather than depression) was selected as it is the most common psychiatric problem in this age group (13–14 years), and because anxiety tends to have an earlier mean age of onset compared with for example depression, which typically has onset in late adolescence.
The objective of the study was therefore to examine cross-sectional associations between device-measured PA patterns (MVPA, SED), sports participation, screen time and mental health (anxiety and HRQoL) in Swedish adolescents.
Methods
Sample
This study is part of the larger cross-sectional study Physical Activity for Healthy Brain Functions in School Youth performed between September and December 2019. A sample size of 1000 students was estimated to provide a representative sample of students from schools with varying sizes, geographic locations and parental socioeconomic backgrounds. The Swedish school system is deregulated and has implemented the free choice reform which allows parents to choose which schools (independent and public) their children should attend. The schools follow a voucher system and the parents do not have to pay tuition fees.18 In the current study, 11 (32%) were independent schools and 23 (68%) were public schools. Figure 1 shows an overview of the participating schools and students. A total of 34 schools participated, the provided reasons for the schools that declined or dropped out were time constraints. From these schools, 1139 students participated (73% response rate), 49% boys and 51% girls, the recruitment process is described in more detail elsewhere.19 The characteristics of the students are shown in table 1.
Figure 1.
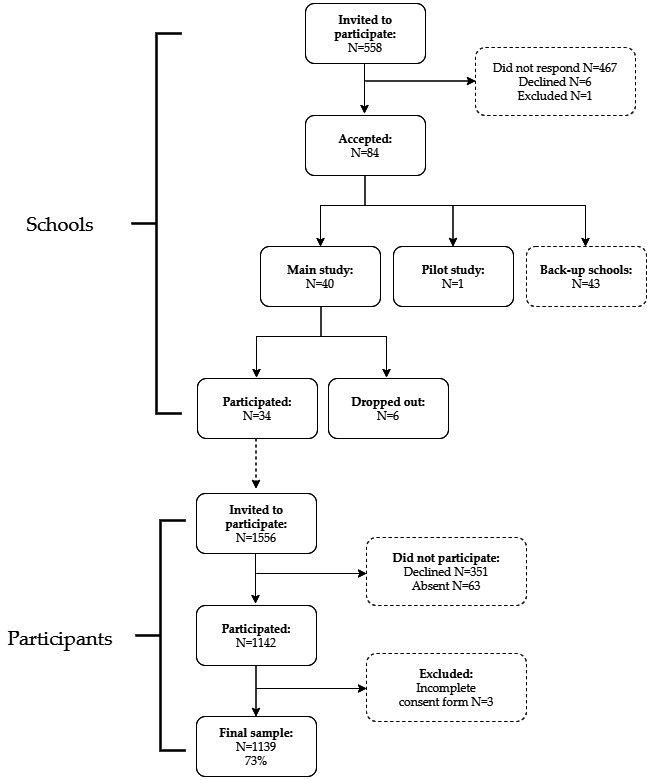
Participation of schools and students.
Table 1.
Descriptive characteristics of the study sample by gender (mean±SD unless otherwise specified)
| n | Missing | All | n | Girls | n | Boys | Sig. | |
| P value | ||||||||
| Total | 1139 (100) | 580 (51.0) | 558 (49.0) | |||||
| Age (year) | 1139 | 0 | 13.4±0.3 | 13.4±0.3 | 13.4±0.4 | 0.147 | ||
| Parental education, >12 years n (%) | 1102 | 37 | 730 (66.2) | 371 (65.9) | 358 (66.5) | 0.483 | ||
| Student country of birth, Sweden n (%) | 1129 | 10 | 967 (85.7) | 490 (84.9) | 476 (86.4) | 0.758 | ||
| BMI status* | 1135 | 4 | 580 | 554 | 0.203 | |||
| Underweight n (%) | 89 (7.8) | 38 (6.6) | 51 (9.2) | |||||
| Normal weight n (%) | 815 (71.8) | 430 (74.1) | 384 (69.3) | |||||
| Overweight n (%) | 179 (15.8) | 89 (15.3) | 90 (16.2) | |||||
| Obese n (%) | 52 (4.6) | 23 (4.0) | 29 (5.2) | |||||
| BMIsds† | 1134 | 5 | 0.36±1.23 | 580 | 0.45±1.11 | 554 | 0.26±1.35 | 0.012 |
| Sedentary time (min) | ||||||||
| SED (average week) | 903 | 236 | 602.0±66.6 | 490 | 608.9±62.65 | 413 | 593.7±70.2 | <0.001 |
| SED bouts over 10 min | 903 | 236 | 122.7±63.6 | 490 | 132.8±63.2 | 413 | 110.7±62.2 | <0.001 |
| SED leisure time (weekdays) | 1054 | 85 | 324.8±69.3 | 548 | 330.0±63.5 | 506 | 319.2±74.7 | 0.011 |
| SED leisure time (weekend) | 916 | 223 | 539.4±84.7 | 497 | 533.8±80.0 | 419 | 546.1±89.6 | 0.029 |
| SED school time | 1054 | 85 | 291.9±37.5 | 548 | 301.7±35.7 | 506 | 281.2±36.5 | <0.001 |
| MVPA time (min) | ||||||||
| MVPA (average week) | 903 | 236 | 52.0±19.0 | 490 | 49.5±17.7 | 413 | 54.9±20.1 | <0.001 |
| MVPA leisure time (weekdays) | 1054 | 85 | 31.6±15.0 | 548 | 30.9±13.8 | 506 | 32.3±16.1 | 0.145 |
| MVPA leisure time (weekend) | 916 | 223 | 37.9±25.3 | 497 | 36.8±23.3 | 419 | 39.1±27.4 | 0.156 |
| MVPA school time | 1054 | 85 | 26.5±11.2 | 548 | 23.2±9.6 | 506 | 30.1±11.7 | <0.001 |
| Reached the MVPA recommendations n (%) | 903 | 236 | 273 (30.2) | 490 | 121 (24.7) | 413 | 152 (36.8) | <0.001 |
| Accelerometer wear time | 903 | 236 | 490 | 413 | ||||
| Wear time (average week) | 792.6±60.8 | 796.0±58.1 | 788.5±63.8 | 0.067 | ||||
| Total included valid days (average week) | 6.0±1.1 | 6.2±1.0 | 5.8±1.1 | <0.001 | ||||
| Organised sports | ||||||||
| Participated in organised sports n (%) | 1094 | 45 | 788 (72.0) | 396 (71.4) | 391 (72.7) | 0.626 | ||
| Screen time (weekdays) | 1126 | 13 | 575 | 550 | 0.842 | |||
| ≤2 hours n (%) | 360 (32.0) | 179 (31.1) | 180 (32.7) | |||||
| 3–4 hours n (%) | 515 (46.0) | 267 (46.4) | 248 (45.1) | |||||
| ≥5 hours n (%) | 251 (22.3) | 129 (22.4) | 122 (22.2) | |||||
| Screen time (weekend) | 1123 | 16 | 576 | 546 | <0.001 | |||
| ≤2 hours n (%) | 178 (15.9) | 70 (12.2) | 108 (19.8) | |||||
| 3–4 hours n (%) | 412 (36.7) | 238 (41.3) | 173 (31.7) | |||||
| ≥5 hours n (%) | 533 (47.5) | 268 (46.6) | 265 (48.5) | |||||
| Mental health | ||||||||
| SCAS-S | 1073 | 66 | 13.7±7.9 | 547 | 16.6±8.0 | 525 | 10.6±6.6 | <0.001 |
| Kidscreen-10 | 1097 | 42 | 39.6±5.4 | 562 | 38.3±5.2 | 534 | 41.0±5.3 | <0.001 |
| Kidscreen-10‡ | 1097 | 42 | 49.6±9.0 | 562 | 47.3±7.5 | 534 | 51.9±9.8 | <0.001 |
*BMI status according to, IOTF 2012.
†BMIsds according to a Swedish reference standard.
‡International T-values based on Rasch person parameter.
BMI, body mass index; BMIsds, body mass index SD score; MVPA, moderate-to-vigorous physical activity; SCAS-S, Short version of the Spence Children’s Anxiety Scale; SED, sedentary time.
The students participated in the measurements at the Swedish School of Sport and Health Sciences, GIH and during the visit, they were provided with an accelerometer, which they used for the following 7 days. The students received a 300 SEK (€30) gift card as compensation for their participation.
Patient and public involvement
The students were not involved in the design, conduct, reporting or dissemination plans of our research, however, the participating schools, students and their parents received a summary of the results from the study.
Measures
Mental health
HRQoL was assessed using Kidscreen-10. The scale includes 10 items of how often the students have felt during the last week, for example, ‘sad’, ‘lonely’ or ‘fit and well’. The answers range from never/not at all to always/extremely on a 5-point scale. The scores are summed up according to the handbook provided by the Kidscreen group, with higher values indicating greater well-being. To compare these values to a reference population, Rasch person-parameters were estimated by transforming the data into a T-score with a mean of 50 and SD of 10 using the provided syntax from the Kidscreen group.20
Anxiety was measured using a Short version of the Spence Children’s Anxiety Scale (SCAS-S), a tool used to assess self-reported anxiety symptoms in children and adolescents. The questionnaire includes 19 items, for example, ‘I worry about things’. Each item is rated on a 4-point scale ranging from ‘never’ to ‘always’. The scores are summed up with higher values reflecting more anxiety symptoms.21 The cut-off for elevated anxiety symptoms was set at 1 SD above the mean and the cut-off for high anxiety symptoms was set at 1.5 SD above the mean with separate cut-offs for girls and boys, respectively.
These two measures have been validated towards the longer versions and provide a global score for anxiety/HRQoL rather than a subscore for each domain of HRQoL or cluster of anxiety symptoms.21 22
Physical activity patterns and screen time
Physical activity patterns (time spent in MVPA and SED) were measured using a hip-worn accelerometer (Actigraph GT3X). The students were told to wear the monitor at all waken times for seven consecutive days (not counting the distribution day), except during water-based activities. Afterward, the monitors were sent back by the teachers in prepaid envelopes. Acceleration was measured at 30 Hz. The accelerometer data were processed in Actilife (V.6.13.3) as uniaxial data using epoch time intervals of 5 s. To define non-wear time, 60 min of zero counts and no spike tolerance was used. Further, an individual time filter was created based on the participant’s reported wake/sleep time (extracted from the questionnaire). A second time filter for school time was created by extracting the times from the school schedules. The criteria for a valid day were at least 500 min of wear time. The criteria for a valid measure were at least three valid days (including 1 weekend day) for analysis of the whole week, at least two valid weekdays for analysis of school-time or weekday leisure time, and at least one valid weekend day for analysis of weekends. The data were categorised into intensities using counts: SED (0–100 counts/min) and MVPA (≥2296 counts/min).23 The first day was excluded to minimise measurement bias.17
Participation in organised sports was self-reported by the students using the following question: ‘Are you active in any sports club/organization? (eg, football, swimming, dancing, scouts, gym)?’.
Screen time was self-reported by the students using the following question for weekdays and weekends. ‘During a normal weekday/weekend day, approximately how much time do you spend using a screen (not included schoolwork) including a cell phone, TV, computer, iPad? (For example, to play games, watch TV, chat, watch serials, YouTube, Snapchat, and Instagram)’. The answers were arranged from no time to 7 hours or more, and were later categorised into 2 hours and below, 3–4 hours, and 5 hours or above.
Background Characteristics
Parental education was collected using register data from Statistics Sweden. The parent with the highest level of education was used and the variable was dichotomised into ≤12 years and >12 years. Information about school type (independent or public) were collected from the National Agency for Education. Gender and country of birth were self-reported by the student. As the gender group, ‘other’ only included one student, this observation was excluded in the models stratified by gender. Country of birth were dicotomized into Sweden and outside Sweden. Bodyweight and height were measured using standardised procedures and rounded to the closest 0.1 kg or mL. BMI status was defined according to the International Obesity Task Force24 and BMIsds were calculated according to a Swedish reference standard.25
Statistical analysis
Data were analysed using STATA/SE V.17.0. Descriptive statistics are presented using mean, SD and proportions. To compare the difference between boys and girls independent t-tests were used for numerical variables and χ2 for categorical variables. To investigate the associations between PA patterns, sports participation screen time (as predictors) and mental health (as dependent variables) multi-level mixed linear regression models were used to account for the clustering of students within schools. Two levels were modelled, level 1 for school and level 2 for the individual student, and a random intercept for each school was applied. We explored both unstandardised and standardised beta-coefficients for the continuous predictors. The assumptions for mixed models were tested, and as data displayed heteroskedasticity (Breusch-Pagan test p>0.05) robust estimates were used.
Based on previous studies, parental education and body mass index SD score (BMIsd, ie, BMI adjusted for age and gender) were tested as confounders. As BMIsds were not significant in any of the models, this covariate was excluded from the final models. The final models were adjusted for parental education, and the models including accelerometer measured PA were adjusted for wear-time. The models with sports participation were also adjusted for time spent in MVPA. Only students with complete data on the mental health scales were included in the analyses. All models were stratified by gender as the PA and mental health outcomes were significantly different between boys and girls. However, we also explored if gender moderated the associations by running the same models with all subjects and adding an interaction term. Only significant interaction results are presented in the text. Crude models are included intable 1-2 in online supplemental material 1.
bmjopen-2022-061929supp001.pdf (79.5KB, pdf)
To analyse the effect size in SCAS-S and Kidscreen-10, standardised mean differences (Cohen’s d) were calculated between the low/high tertiles of MVPA, screen time and participants/non-participants in organised sports. The level of statistical significance was set at α<0.05, 95% CIs, p values and beta values are bold to indicate statistical significance.
Results
In total, 1072 students (94%) completed all items on SCAS-S. Girls reported significantly higher anxiety scores compared with boys (16.6 vs 10.6, mean difference of 6.0, t(1070)=13.44, p<0.01). In girls, 82 (15%) had a score >1 SD above the mean (elevated anxiety) and 50 (9%) had a score >1.5 SD above the mean (high anxiety). In boys, the corresponding values were 75 (14%) students and 42 (8%) students. Boys to parents with low education had significantly higher anxiety symptoms (mean difference 1.6, t(505)= 2.7, p<0.01) compared with boys with high parental education. This difference was not observed in girls or for HRQoL.
A total of 1096 (96%) students completed all items on the Kidscreen-10 questionnaire where girls had significantly lower scores of HRQoL (mean difference of 2.63, t(1094)=−8.29, p<0.01) compared with boys. The Cronbach alpha for Kidsscreen-10 was 0.78 and 0.85 for SCAS-S, indicating acceptable to good internal consistency.
For the PA measurements, 903 students (79%) had valid accelerometer readings for the whole week, 1054 students (93%) for weekdays and 916 (80%) on weekends. There were no significant differences in mean values of SCAS-S or Kidscreen-10 between those who had a valid accelerometer reading and those who did not.
On an average day, boys spent significantly more time in MVPA. However, when breaking down the MVPA between domains, this difference was only significant during school time (mean difference of 6.9 min, t(1052)=−10.57, p<0.01). Students who participated in organised sports had 11.3 more minutes per day in MVPA compared to those who did not participate t(874)=−8.10, p<0.01. Similarly, the group who reported low screen time (≤2 hours) on weekends spent 15 more minutes in MVPA compared to those who reported 5 hours or more t(566)=6.32, p<0.01. Table 2 shows the associations between anxiety (SCAS-S) and HRQoL (Kidscreen-10) and predictors using multi-level mixed linear regression models.
Table 2.
Associations between predictors and anxiety (SCAS-S) and health-related quality of life (Kidsscreen-10) analysed with multi-level mixed linear regression models stratified by gender
| Model | Anxiety (SCAS-S) | Health-related quality of life (Kidsscreen-10) | ||||||||||
| Girls | Boys | Girls | Boys | |||||||||
| n | Unstandardised B (95% CI) |
Standardised beta | n | Unstandardised B (95% CI) |
Standardised beta | n | Unstandardised B (95% CI) |
Standardised beta | n | Unstandardised B (95% CI) |
Standardised beta | |
| 1. MVPA | ||||||||||||
| 1.1. MVPA whole week | 448 | −0.045 (−0.079 to –0.011) | −0.099 | 383 | −0.026 (−0.058 to 0.007) | −0.077 | 458 | 0.032 (0.009 to 0.054) | 0.110 | 390 | 0.040 (0.015 to 0.065) | 0.157 |
| 1.2. MVPA leisure time (weekdays) | 503 | −0.091 (−0.134 to –0.049) | −0.161 | 468 | −0.038 (−0.066 to –0.010) | −0.095 | 514 | 0.048 (0.023 to 0.073) | 0.130 | 477 | 0.036 (0.011 to 0.061) | 0.114 |
| 1.3. MVPA leisure time (weekend) | 455 | −0.023 (−0.049 to 0.002) | −0.067 | 388 | −0.001 (−0.024 to 0.021) | −0.005 | 465 | 0.023 (0.033 to 0.043) | 0.105 | 396 | 0.034 (0.020 to 0.048) | 0.183 |
| 1.4. MVPA school time | 503 | −0.027 (−0.100 to 0.047) | −0.032 | 468 | 0.015 (−0.039 to 0.069) | 0.027 | 514 | 0.013 (−0.033 to 0.059) | 0.025 | 477 | 0.020 (−0.024 to 0.064) | 0.046 |
| 2. SED | ||||||||||||
| 2.1. SED whole week | 448 | 0.011 (−0.007 to 0.029) | 0.084 | 383 | 0.011 (−0.005 to 0.028) | 0.120 | 458 | −0.021 (−0.032 to –0.009) | −0.251 | 390 | −0.021 (−0.033 to –0.008) | −0.285 |
| 2.2. SED bouts (10 min) whole week | 448 | −0.001 (−0.014 to 0.012) | −0.009 | 383 | 0.002 (−0.009 to 0.013) | 0.021 | 458 | −0.012 (−0.020 to –0.005) | −0.150 | 390 | −0.009 (−0.017 to –0.001) | −0.113 |
| 2.3. SED leisure time (weekdays) | 503 | 0.040 (0.017 to 0.062) | 0.315 | 468 | 0.017 (−0.002 to 0.036) | 0.195 | 514 | −0.034 (−0.051 to –0.017) | −0.421 | 477 | −0.020 (−0.036 to –0.005 | −0.299 |
| 2.4. SED leisure time (weekend) | 455 | 0.007 (−0.007 to 0.020) | 0.064 | 388 | 0.003 (−0.009 to 0.014) | 0.035 | 465 | −0.012 (−0.022 to –0.003) | −0.192 | 396 | −0.017 (−0.024 to –0.009) | −0.299 |
| 2.5. SED school | 503 | −0.009 (−0.039 to 0.021) | −0.041 | 468 | −0.011 (−0.034 to 0.012) | −0.062 | 514 | −0.009 (−0.026 to 0.009) | −0.060 | 477 | −0.012 (−0.033 to 0.010) | −0.083 |
| 3. Organised sports | ||||||||||||
| Did not participate | 112 | ref | 97 | ref | 114 | ref | 99 | ref | ||||
| Participated | 321 | −0.210 (−2.165 to 1.745) | 283 | −1.810 (−3.492 to –0.129) | 329 | −0.258 (−1.701 to 1.185) | 288 | 1.214 (−0.459 to 2.888) | ||||
| 4. Screen time weekday | ||||||||||||
| ≤2 hours | 162 | ref | 167 | ref | 166 | ref | 167 | ref | ||||
| 3–4 hours | 253 | 0.628 (−0.975 to 2.231) | 230 | 0.342 (−0.782 to 1.466) | 256 | −1.337 (−2.175 to –0.499) | 237 | −0.785 (-1.758 to 0.188) | ||||
| ≥5 hours | 116 | 4.056 (1.935 to 6.176) | 110 | 0.883 (−0.583 to 2.348) | 121 | −3.503 (−4.786 to –2.220) | 111 | −1.539 (-2.664 to –0.413) | ||||
| 5. Screen time weekend | ||||||||||||
| ≤2 hours | 61 | ref | 98 | ref | 65 | ref | 99 | ref | ||||
| 3–4 hours | 219 | 1.155 (−0.582 to 3.369) | 164 | −0.151 (−1.776 to 1.473) | 225 | −0.904 (−2.315 to 0.506) | 166 | 0.157 (-1.725 to 1.411) | ||||
| ≥5 hours | 252 | 3.340 (1.394 to 5.287) | 243 | 1.060 (−0.207 to 2.326) | 254 | −2.520 (−4.014 to –1.027) | 248 | −0.842 (-2.320 to 0.636) | ||||
B unstandardised coefficients, beta standardised coefficients. All models were adjusted for parental education. Model 3 was adjusted for time spent in MVPA. Models 1–3 were adjusted for accelerometer wear-time.
MVPA, moderate-to-vigorous physical activity; SCAS-S, Short version of the Spence Children’s Anxiety Scale; SED, sedentary time.
Associations between PA patterns, screen time and anxiety (SCAS-S)
A significant inverse association between time spent in MVPA during leisure time on weekdays and anxiety was seen in girls and boys. There was a significant interaction of gender in this association (<0.01), such that the association was stronger in girls compared with boys. Time spent in MVPA over the whole week was only significantly associated with anxiety in girls, none of the other MVPA measures was significantly associated with anxiety among girls or boys. Boys who participated in organised sports also had a significantly lower prevalence of anxiety, compared with boys who did not participate. This association was not significant in girls.
In girls, time spent in SED during leisure time on weekdays was positively associated with anxiety. None of the other SED measures was significantly associated with anxiety in girls or boys.
With regards to screen time, significant associations were only found in the group of girls who reported ≥5 hours screen time on weekdays or weekends. These groups had significantly higher anxiety scores compared with those who reported up to 2 hours. When controlling for MVPA, this association remained significant (B=3.39, 95% CI 1.33 to 5.46) for weekdays and (B=2.53, 95% CI 0.27 to 4.80) for weekends. Further, there was a significant interaction of gender in the association between screen time on weekdays and anxiety with a stronger association among girls compared with boys (p=0.03) in the group who reported ≥5 hours screen time.
Associations between PA pattern, screen time and HRQoL (Kidsscreen-10)
There was a positive association between time spent in MVPA during the whole week, during leisure time on weekdays, on weekends, and HRQoL in girls and boys. There was a positive association between sports participation and HRQoL in boys, however, the significance disappeared after controlling for time spent in MVPA.
Inverse associations were seen between all SED time domains and HRQoL in both boys and girls, except SED during school time. There was a significant interaction of gender in the association between time spent in SED on weekends and HRQoL (p=0.04) with a stronger association in boys compared with girls.
Girls and boys who reported ≥5 hours screen time on weekdays had significantly lower HRQoL, compared with those who reported 2 hours or less. The results remained significant also after adjusting for time spent in MVPA (B=−3.32, 95% CI −4.50 to –2.14 in girls, and B=−1.65, 95% CI −2.70 to –0.61 in boys). A significant association between screen time on weekends and HRQoL was only found in girls who reported ≥5 hours of screen time.
Figure 2 shows the unadjusted mean anxiety (SCAS-S) scores and HRQoL (Kidscreen-10) scores between students reporting different levels of screen time on weekdays.
Figure 2.

Unadjusted mean anxiety (SCAS-S) scores and health related quality of life (Kidscreen-10) scores, between screen time groups, mean comparisons analysed using an analysis of variance and Bonferroni post hoc test. ***p<0.001; **p<0.01. SCAS-S, Short version of the Spence Children's Anxiety Scale
To assess the clinical significance, we calculated effect sizes (Cohen’s d) in mental health scores between participants/non-participants in organised sports, low/high screen time and low/high tertiles of MVPA. The average time (minutes) for MVPA in the lowest tertile was 32 and 34, and in the highest tertile 70 and 78 for girls and boys, respectively. Regarding anxiety, the effect sizes between low/high MVPA groups were 0.18 in girls (95% CI −0.05 to 0.40) and 0.31 in boys (0.07 to 0.56). The effect sizes between participants/non-participants in organised sports were 0.13 (95% CI −0.07 to 0.31) in girls and 0.31 (95% CI 0.12 to 0.51) in boys. The effect sizes between groups with low/high screen time on weekdays were −0.47 in girls (95% CI −0.70 to –0.23) and −0.18 in boys (95% CI −0.42 to 0.05) and on weekends −0.36 in girls (95% CI −0.64 to –0.09) and −0.17 (95% CI −0.40 to 0.06) in boys.
For HRQoL, the results showed that the effect sizes between low/high MVPA groups were −0.28 in girls (95% CI −0.50 to –0.06) and −0.51 in boys (95% CI −0.75 to –0.26) and between participants/non-participants in organised sports −0.01 (95% CI −0.20 to 0.18) in girls and −0.28 (95% CI −0.47 to –0.08) in boys. Between groups with high/low screen time on weekdays, the effect sizes were 0.59 in girls (95% CI 0.36 to 0.83) and 0.35 in boys (95% CI 0.12 to 0.59) and on weekends 0.50 (95% CI 0.23 to 0.77) and 0.14 (95% CI −0.09 to 0.36) for girls and boys, respectively (these results can be found in online supplemental material table 3).
Discussion
In this cross-sectional study, the associations between PA patterns, sports participation, screen time and mental health (anxiety and HRQoL) were investigated in Swedish adolescents. MVPA was positively associated with HRQoL whereas time spent in SED or using screens on weekdays was inversely associated. Although the effect sizes generally were small, the largest effect sizes were observed between the high/low MVPA group in boys and between the high/low screen time group in girls. With regards to anxiety, high MVPA during leisure time on weekdays was associated with low anxiety scores. Some gender differences were observed, boys participating in organised sports had low anxiety scores whereas girls who reported 5 hours or more of screen time had high anxiety scores.
The mean Kidscreen-10 score in our sample was 38.3 in girls and 41.0 in boys, which corresponds to a T-score of 47.3 in girls and 51.9 in boys. A suggested threshold to classify the values as ‘normal’ is ½ SD above or below the reference value.20 This indicates that our sample was within this range of the Swedish reference population (12–18 years old) with a T-score of 49.2 for girls and 52.4 for boys, as well as the overall European T-score based on 11 countries (48.6 for girls and 49.5 for boys).20 The current sample also had similar PA levels (on average 52 min in MVPA per day) and demographic characteristics (66% had parents with ≥12 years of education, 86% were born in Sweden and 21% had overweight or obesity) compared with a nationally representative study in Swedish adolescents which reported on average 53 min in MVPA per day, 61% with high parental education, 88% born in Sweden, 21% with overweight or obesity.14
The most common limitation in previous studies is the lack of detailed measures of PA. The current study used device-measured PA and could confirm many findings based on self-reported PA. One example is a review that found PA to be positively associated with HRQoL and a high proportion of SED to be associated with lower HRQoL.26 In general, the effect sizes in the current study were small, which is not uncommon in these types of studies. A previous study by Gopinath et al found similar mean differences in HRQoL between the high/low group of PA and screen time.27 However, this study did not stratify the analysis by gender. In our study, we found the largest effect sizes when comparing the lowest and highest tertiles of MVPA for boys (Cohen’s d=0.51), and screen time for girls (Cohen’s d=0.50 on weekends) and (Cohen’s d=0.59 on weekdays). Our findings suggest that the strengths of the associations to HRQoL could be different for boys and girls and these gender differences should be considered when designing future intervention studies to improve HRQoL.
Regarding screen time, this study found high screen time during weekdays to be associated with lower HRQoL which confirms the findings of a review that concluded moderate evidence for the association between screen time and HRQoL. In the current study, we found a significant difference in MVPA between the low/high screen time group. Interestingly, after controlling for time spent in MVPA screen time was still significantly associated with HRQoL independently of MVPA in both genders. As previously mentioned, we found the effect size of screen time to be larger in girls. These findings are similar to a study from the UK which concluded that the association between screen time and mental health was stronger in girls. The same study also found that the dose of screen time associated with problematic mental health was lower for girls (>2 hours) compared with boys (>5 hours).28 This was also evident in the current study, where screen time >3 hours were associated with lower HRQoL in girls, whereas for boys this association was significant only for the group reporting ≥5 hours.
A strength of this study is the inclusion of both a positive and a negative indicator of mental health, which shows that the type of PA pattern and screen time associated with each measure differs. Fewer measures of the PA pattern and screen time were significantly associated with anxiety compared with HRQoL. MVPA during leisure time on weekdays was inversely associated with anxiety in both genders. These results are consistent with those reported previously using self-reported PA.29 30 However, we only found sports participation to be associated with lower anxiety in boys. These findings were different from a study in 14-year-olds that found sports participation to be significantly associated with lower anxiety and higher well-being in both genders.31 Potential explanations for this could be that the study did not control for time spent in MVPA and that sports participation was lower (33%) compared with 72% in our study. Another study in older youth found that the significant association between sports participation and anxiety disappeared after controlling for time spent in MVPA.12 Previous studies have also suggested that the strength of the association could vary between genders. A review found a weak negative correlation between sports participation and anxiety, but in samples with a higher proportion of boys, the correlation was stronger.32 One potential explanation for the gender differences observed in the current study could be related to the context and sports environment. Where girls have reported a higher incidence of teasing during sports participation and participation in sports common to girls (aesthetic sports such as dance or gymnastics) have been associated with body image concerns and disordered eating.33 This indicates that depending on the sports culture the association between sports participation and mental health could differ between genders, this should be investigated further in future research.
About screen time, this study found that girls reporting ≥5 hours of screen time on weekdays and weekends had higher levels of anxiety compared with those who reported ≤2 hours. This association was not seen in boys. These findings were consistent with a study in Icelandic adolescents, that found screen time <5 hours to be associated with fewer symptoms of anxiety and depression.30 However, the results were not stratified by gender. Although not investigated in the current study, one suggested explanation for the gender differences is the type of screen time activity. A review found social media use to be associated with anxiety, with a stronger association in girls34 future studies should further investigate these associations. With regards to screen time, it is important to acknowledge the methodological challenges of measuring screen time, and that there is no consensus of how to best capture these behaviours. In this study, self-reported screen time was used with broad questions that included all types of screen devices and activities, except schoolwork. When comparing self-reported screen time to more objective measures (using an app for example) some under-reporting is evident, although total daily duration was more accurately reported compared with number of phone use.35 In the current study, self-report was used to decrease participant burden and privacy invasion, but it is worth noting that the screen time duration acquired in this study should not be considered an exact dose but rather interpreted as a proxy for high/low screen users.
There is a lack of studies that investigate the association between device-measured SED and mental health and many studies rely on screen time as a proxy for SED. In the current study, stronger associations were seen in the standardised beta coefficients for the SED measurements (especially during leisure time weekdays), compared with MVPA. This was seen in both genders for HRQoL and for anxiety in girls. A review concluded that sedentary behaviours were associated with an increased risk of anxiety, with the strongest associations found in sitting.36 However, it is important to note that causation or the direction of these associations cannot be studied in cross-sectional studies. Interestingly, a randomised controlled trial (RCT) showed significantly higher anxiety levels in the intervention group after a 1-week intervention of increased SED and eliminated PA compared with the control group, which continued their normal PA routine.37 These findings suggest that reducing SED could be a strategy to improve mental health among adolescents, although this should be investigated further in larger RCT studies.
A limitation of the current study was the lack of questions concerning functioning to further understand if the group with low mental health experienced impairment in their daily lives. However, including a positive and negative measure still provides a better understanding of the students’ overall mental health compared with studies that only focus on symptoms of mental illness. Moreover, other measures not included in this article such as academic attainment and cognition could be important in this association. Another limitation was the cross-sectional design, which makes it impossible to study the direction or cause of these relationships. A strength was the detailed PA measure (accelerometer) with individual time filters, which enabled comparisons between different time domains. Furthermore, the relatively large sample size and a high participation rate (73%), which resulted in a non-homogenous study population of adolescents with different PA levels and mental health scores. As our population were within the range of the European norm values for HRQoL it is plausible that our findings could be generalised to other European adolescent populations. However, as our questionnaires were in Swedish, immigrant adolescents with a low proficiency in Swedish could not participate, neither did we have a representation of adolescents with physical impairments. Therefore, future studies should ensure that these groups are represented as well to enhance the generalisability of the findings.
Conclusions
This cross-sectional study showed that MVPA was associated with better mental health, whereas SED or screen time was associated with lower mental health. However, these associations were not significant throughout all time domains and some gender differences were observed. Although this cross-sectional study cannot conclude causation or direction the relationship, our results suggest that adolescents with worse mental health scores also spend less time being physically active and more time being sedentary or using screens. Therefore, it is important in future research and school efforts to consider how to reach this group, as they might be the ones most in need of an intervention. Our results could create a paradigm for future studies to decide which types of PA patterns and time domains to target in intervention studies with the aim improve mental health among adolescents.
Supplementary Material
Acknowledgments
We want to thank all the students, their parents and the teachers involved in the study. We would also like to thank the hardworking research personnel involved in the data collection making this study possible.
Footnotes
Contributors: KK recruited the schools. GN, OE, BH, KK designed the study and participated in the data collection. BH and KK cleaned and processed the data. JA contributed to the design of the statistical model and the interpretation of the results. KK drafted the manuscript and acted as a guarantor. All authors read and approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding: This study is part of the 'Physical activity for healthy brain functions in school youth', which was funded by the Knowledge Foundation (grant 20180040) and conducted in collaboration with Coop, IKEA, Skanska, Skandia, Stockholm Consumer Cooperative Society and the Swedish Crown Princess Couple’s Foundation/Generation Pep.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
No data are available. The datasets are not available for download to protect the confidentiality of the participants. The data are held at The Swedish School of Sport and Health Sciences.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
This study involves human participants and was approved by the Regional Ethical Review Board in Stockholm ID No. 2019-03579 and was conducted by the Declaration of Helsinki. Participants gave informed consent to participate in the study before taking part.
References
- 1.World Health Organization . Basic documents: World Health organization; 2020.
- 2.Gore FM, Bloem PJN, Patton GC, et al. Global burden of disease in young people aged 10–24 years: a systematic analysis. The Lancet 2011;377:2093–102. 10.1016/S0140-6736(11)60512-6 [DOI] [PubMed] [Google Scholar]
- 3.Patel V, Flisher AJ, Hetrick S, et al. Mental health of young people: a global public-health challenge. Lancet 2007;369:1302–13. 10.1016/S0140-6736(07)60368-7 [DOI] [PubMed] [Google Scholar]
- 4.Solmi M, Radua J, Olivola M, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry 2022;27:1–15. 10.1038/s41380-021-01161-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Polanczyk GV, Salum GA, Sugaya LS, et al. Annual research review: a meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry 2015;56:345–65. 10.1111/jcpp.12381 [DOI] [PubMed] [Google Scholar]
- 6.Bell SL, Audrey S, Gunnell D, et al. The relationship between physical activity, mental wellbeing and symptoms of mental health disorder in adolescents: a cohort study. Int J Behav Nutr Phys Act 2019;16:138. 10.1186/s12966-019-0901-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McMahon EM, Corcoran P, O’Regan G, et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur Child Adolesc Psychiatry 2017;26:111–22. 10.1007/s00787-016-0875-9 [DOI] [PubMed] [Google Scholar]
- 8.Kremer P, Elshaug C, Leslie E, et al. Physical activity, leisure-time screen use and depression among children and young adolescents. J Sci Med Sport 2014;17:183–7. 10.1016/j.jsams.2013.03.012 [DOI] [PubMed] [Google Scholar]
- 9.Sigvartsen J, Gabrielsen LE, Abildsnes E, et al. Exploring the relationship between physical activity, life goals and health-related quality of life among high school students: a cross-sectional study. BMC Public Health 2016;15:709. 10.1186/s12889-016-3407-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Biddle SJ, Ciaccioni S, Thomas G. Physical activity and mental health in children and adolescents: an updated review of reviews and an analysis of causality. Psychology of Sport and Exercise 2018. 10.1136/bjsports-2011-090185 [DOI] [Google Scholar]
- 11.Kleppang AL, Hartz I, Thurston M, et al. The association between physical activity and symptoms of depression in different contexts - a cross-sectional study of Norwegian adolescents. BMC Public Health 2018;18:1368. 10.1186/s12889-018-6257-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Doré I, O'Loughlin JL, Beauchamp G, et al. Volume and social context of physical activity in association with mental health, anxiety and depression among youth. Prev Med 2016;91:344–50. 10.1016/j.ypmed.2016.09.006 [DOI] [PubMed] [Google Scholar]
- 13.Guthold R, Stevens GA, Riley LM, et al. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health 2020;4:23-35. 10.1016/S2352-4642(19)30323-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nyberg G, Kjellenberg K, Fröberg A, et al. A national survey showed low levels of physical activity in a representative sample of Swedish adolescents. Acta Paediatr 2020;109:2342–53. 10.1111/apa.15251 [DOI] [PubMed] [Google Scholar]
- 15.Hoare E, Milton K, Foster C, et al. The associations between sedentary behaviour and mental health among adolescents: a systematic review. Int J Behav Nutr Phys Act 2016;13:108. 10.1186/s12966-016-0432-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Liu M, Wu L, Yao S. Dose-response association of screen time-based sedentary behaviour in children and adolescents and depression: a meta-analysis of observational studies. Br J Sports Med 2016;50:1252–8. 10.1136/bjsports-2015-095084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Corder K, Ekelund U, Steele RM, et al. Assessment of physical activity in youth. J Appl Physiol 2008;105:977–87. 10.1152/japplphysiol.00094.2008 [DOI] [PubMed] [Google Scholar]
- 18.Trumberg A, Urban S. School choice and its long-term impact on social mobility in Sweden. Scandinavian Journal of Educational Research 2021;65:569–83. 10.1080/00313831.2020.1739129 [DOI] [Google Scholar]
- 19.Nyberg G, Ekblom Örjan, Kjellenberg K, et al. Associations between the school environment and physical activity pattern during school time in Swedish adolescents. Int J Environ Res Public Health 2021;18:10239. 10.3390/ijerph181910239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.KIDSCREEN Group. Europe.(2006) . The KIDSCREEN questionnaires: quality of life questionnaires for children and adolescents. Germany: Handbook Lengerich Pabst Science Publishers, 2011. [Google Scholar]
- 21.Ahlen J, Vigerland S, Ghaderi A. Development of the spence children's anxiety scale - short version (SCAS-S). J Psychopathol Behav Assess 2018;40:288–304. 10.1007/s10862-017-9637-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ravens-Sieberer U, Erhart M, Rajmil L, et al. Reliability, construct and criterion validity of the KIDSCREEN-10 score: a short measure for children and adolescents' well-being and health-related quality of life. Qual Life Res 2010;19:1487–500. 10.1007/s11136-010-9706-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Evenson KR, Catellier DJ, Gill K, et al. Calibration of two objective measures of physical activity for children. J Sports Sci 2008;26:1557–65. 10.1080/02640410802334196 [DOI] [PubMed] [Google Scholar]
- 24.Cole TJ, Lobstein T. Extended International (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes 2012;7:284–94. 10.1111/j.2047-6310.2012.00064.x [DOI] [PubMed] [Google Scholar]
- 25.Karlberg J, Luo ZC, Albertsson-Wikland K. Body mass index reference values (mean and SD) for Swedish children. Acta Paediatr 2001;90:1427–34. 10.1111/j.1651-2227.2001.tb01609.x [DOI] [PubMed] [Google Scholar]
- 26.Wu XY, Han LH, Zhang JH, et al. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: a systematic review. PLoS One 2017;12:e0187668. 10.1371/journal.pone.0187668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gopinath B, Hardy LL, Baur LA, et al. Physical activity and sedentary behaviors and health-related quality of life in adolescents. Pediatrics 2012;130:e167–74. 10.1542/peds.2011-3637 [DOI] [PubMed] [Google Scholar]
- 28.Twenge JM, Farley E. Not all screen time is created equal: associations with mental health vary by activity and gender. Soc Psychiatry Psychiatr Epidemiol 2021;56:207–17. 10.1007/s00127-020-01906-9 [DOI] [PubMed] [Google Scholar]
- 29.Bélair M-A, Kohen DE, Kingsbury M, et al. Relationship between leisure time physical activity, sedentary behaviour and symptoms of depression and anxiety: evidence from a population-based sample of Canadian adolescents. BMJ Open 2018;8:e021119. 10.1136/bmjopen-2017-021119 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hrafnkelsdottir SM, Brychta RJ, Rognvaldsdottir V, et al. Less screen time and more frequent vigorous physical activity is associated with lower risk of reporting negative mental health symptoms among Icelandic adolescents. PLoS One 2018;13:e0196286. 10.1371/journal.pone.0196286 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.McMahon EM, Corcoran P, O'Regan G, et al. Physical activity in European adolescents and associations with anxiety, depression and well-being. Eur Child Adolesc Psychiatry 2017;26:111–22. 10.1007/s00787-016-0875-9 [DOI] [PubMed] [Google Scholar]
- 32.Panza MJ, Graupensperger S, Agans JP, et al. Adolescent sport participation and symptoms of anxiety and depression: a systematic review and meta-analysis. J Sport Exerc Psychol 2020;42:201–18. 10.1123/jsep.2019-0235 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Slater A, Tiggemann M. Gender differences in adolescent sport participation, teasing, self-objectification and body image concerns. J Adolesc 2011;34:455–63. 10.1016/j.adolescence.2010.06.007 [DOI] [PubMed] [Google Scholar]
- 34.Keles B, McCrae N, Grealish A. A systematic review: the influence of social media on depression, anxiety and psychological distress in adolescents. Int J Adolesc Youth 2020;25:79–93. 10.1080/02673843.2019.1590851 [DOI] [Google Scholar]
- 35.Andrews S, Ellis DA, Shaw H, et al. Beyond self-report: tools to compare estimated and real-world smartphone use. PLoS One 2015;10:e0139004. 10.1371/journal.pone.0139004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Allen MS, Walter EE, Swann C. Sedentary behaviour and risk of anxiety: a systematic review and meta-analysis. J Affect Disord 2019;242:5–13. 10.1016/j.jad.2018.08.081 [DOI] [PubMed] [Google Scholar]
- 37.Edwards MK, Loprinzi PD. Experimentally increasing sedentary behavior results in increased anxiety in an active young adult population. J Affect Disord 2016;204:166–73. 10.1016/j.jad.2016.06.045 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2022-061929supp001.pdf (79.5KB, pdf)
Data Availability Statement
No data are available. The datasets are not available for download to protect the confidentiality of the participants. The data are held at The Swedish School of Sport and Health Sciences.