

Abstract
OBJECTIVES
This study sought to assess the association of baseline left atrial (LA) phasic function measured with cardia magnetic resonance (CMR) and incident ischemic cerebrovascular events (CVE).
BACKGROUND
LA remodeling is a known predictor of atrial fibrillation (AF), which is a risk factor for ischemic CVE. Despite studies showing an association between LA remodeling and ischemic CVE, the association of LA mechanical function with ischemic CVE in a population free of known cardiovascular disease is not fully studied.
METHODS
Phasic LA volumes; total, passive, and active LA emptying fractions (LAEF); and peak longitudinal LA strain were measured using feature-tracking CMR in 4,261 MESA (Multi-Ethnic Study of Atherosclerosis) participants (61 ± 10 years of age; 4 8 % male). All individuals were free of clinical cardiovascular disease at baseline. Participants were followed for 11.6 ± 3.5 years for the diagnosis of incident ischemic CVE, defined as ischemic stroke or transient ischemic attack adjudicated by vascular neurologists.
RESULTS
During the follow-up, 193 (1.26 per 1,000 person-years) ischemic CVE (134 ischemic strokes and 59 TIAs) occurred. Individuals with incident ischemic CVE had larger LA volumes and lower passive, active, and total LAEFs at baseline. In multivariate analysis adjusted for known CVE risk factors, left ventricular mass and interim AF, total LAEF was associated with incident ischemic CVE (hazard ratio [HR]: 0.85 per SD; 9 5 % confidence interval [Cl]: 0.74 to 0.98; p = 0.027). The unadjusted HR for the lowest tertile of total LAEF compared to the highest tertile was 2.0 (95% Cl: 1.43 to 2.79; p < 0.001), and the adjusted HR was 1.47 (95% Cl: 1.04 to 2.05; p = 0.031). Addition of total LAEF to known clinical risk factors of CVE and left ventricular mass resulted in an improved predictive accuracy (C statistic of 0.76 vs. 0.73, respectively; p = 0.039).
CONCLUSIONS
Reduced total LAEF was associated with incident ischemic CVE independent of known cerebrovascular risk factors and incident AF. Assessment of LA function may add further information in stratifying asymptomatic individuals at risk for ischemic stroke.
Keywords: atrial fibrillation, atrial function, cardiac magnetic resonance, ischemic stroke, left atrial remodeling
Graphical Abstract
Left atrial (LA) remodeling consists of mechanical, electrical, and structural changes. These changes are present before atrial fibrillation (AF) development and worsen with development of AF (1–3). In AF patients, the greater extent of LA remodeling is associated with worse outcomes, especially with a higher prevalence of cerebrovascular events (CVE) (4,5). Nonetheless, emerging data suggest an association between atrial structural changes such as increased LA size (6,7), electrical abnormalities of the P-wave on surface electrocardiography (ECG) (8–11), and elevated levels of N-terminal pro-B-type natriuretic peptide (NT-proBNP) (11) with risk of ischemic CVE independent of AF. The common hypothesis connecting LA remodeling and ischemic CVE is posited to be the potential role of LA mechanical dysfunction in blood stasis and therefore thromboembolism. Despite several prospective studies investigating the association of LA remodeling and ischemic stroke (Supplemental Table 1), no study has investigated the association of LA mechanical function with ischemic CVE in a population free of clinical cardiovascular disease. Accordingly, this study sought to examine the association of baseline LA mechanical function measured with CMR, the gold standard modality for assessing myocardial function, and incident ischemic CVE in a multiethnic population free of clinical cardiovascular disease at baseline. The hypothesis was that worse baseline LA function would be associated with a higher incidence of ischemic CVE independent of interim AF.
METHODS
STUDY POPULATION.
This study is embedded in the MESA (Multi-Ethnic Study of Atherosclerosis) study. Briefly, between July 2000 and August 2002, MESA recruited 6,814 individuals from 6 U.S. communities in North Carolina, New York, Maryland, Illinois, Minnesota, and California (12). Of the 6,814 participants, 5,098 underwent cardiac magnetic resonance (CMR) imaging (75%) and 5,004 (73%) had technically adequate data. The participants were between 45 and 84 years of age and were from 4 different self-reported racial/ethnic backgrounds (white, African-American, Hispanic, and Chinese). All participants were free of any clinically apparent cardiovascular disease at baseline. The Institutional Review Boards of the participating sites approved the study, and all participants gave written informed consent. The description and methods of collecting covariates have been explained in the Supplemental Appendix.
FOLLOW-UP.
In addition to 5 follow-up examinations, a telephone interviewer contacted each participant approximately every 9 months to inquire about hospital admissions, cardiovascular outpatient diagnoses, and deaths. Medical records were successfully obtained for 98% of reported hospitalized cardiovascular events and 95% of reported outpatient cardiovascular diagnostic encounters.
ADJUDICATION OF EVENTS.
A committee that included neurologists, cardiologists, and physician epidemiologists adjudicated strokes, transient ischemic attacks (TIA), and other cardiovascular events (12). Ischemic stroke consisted of rapid onset of a documented focal neurologic deficit lasting 24 h or until death or, if <24 h, there was a clinically relevant infarction shown on brain imaging. Patients with focal neurologic deficits secondary to hemorrhagic stroke, brain trauma, tumor, infection, or other nonvascular cause were excluded. TIA consisted of 1 or more documented episodes of focal neurologic deficit lasting 30 s to 24 h and without brain imaging suggesting stroke. For the purposes of this study, ischemic CVE was defined as fatal or nonfatal ischemic stroke or TIA.
Incident AF during follow-up was identified by using a combination of hospitalization surveillance, follow-up ECG in 2010 to 2012, and, for participants enrolled in fee-for-service Medicare, from inpatient, outpatient, and physician claims. The International Classification of Diseases-9th Revision, diagnostic code 427.31 (atrial fibrillation) or 427.31 (atrial flutter) in any position was considered evidence of AF. If the first AF claim occurred before the baseline MESA examination, the participant was considered to have prevalent AF and was excluded from the analysis.
IMAGE ANALYSIS.
Baseline MR images were acquired using 1.5-T CMR scanners, either Signa LX or CVi (GE Medical Systems, Waukesha, Wisconsin) or Symphony or Sonata (Siemens Medical Systems, Erlangen, Germany). Long-axis cine images were obtained from 2- and 4-chamber views, using ECG-gated fast gradient-echo pulse sequence. All cine images were acquired with a temporal resolution of approximately 50 ms. A stack of short-axis images recorded at end diastole was obtained for the LV mass assessment (13).
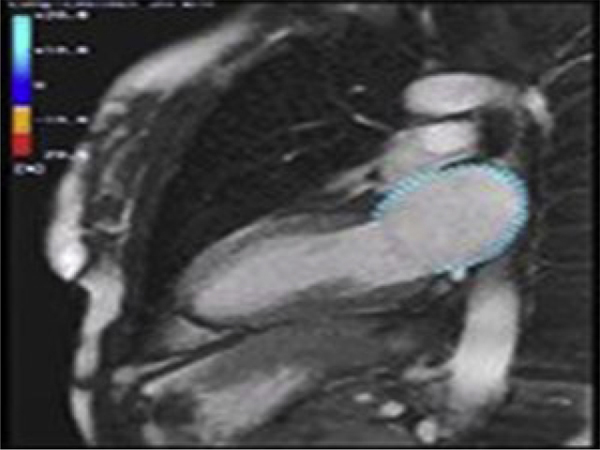
Five experienced operators analyzed all images in a core laboratory at Johns Hopkins University. Multimodal tissue tracking software (MTT, version 5.0, Toshiba, Japan) was used to quantify LA strain and phasic volumes from baseline 4- and 2-chamber cine CMR images. This method has been previously validated with excellent reproducibility (intraclass correlation coefficients between 0.90 to 0.97 for LA volumes and strain) (14). Endocardial and epicardial LA borders were defined at end-systole. In the 4-chamber view, the LA border started from the medial side of the mitral annulus and included interatrial septum, posterior, and lateral LA walls and ended at the lateral mitral annulus. In the 2-chamber view, the analyzed atrial border started from anterior mitral annulus and continued over the LA roof, the posterior wall, and the floor of the LA and ended at the inferior mitral annulus. Using the defined borders, the software then tracked the LA myocardium in subsequent frames (Video 1). The operator then followed the generated contours during the cardiac cycle for quality control. Images with poor tracking and/or foreshortened images were excluded. In each frame, the LA volume was calculated using this previously validated formula: [volume = (0.848 area4ch × area2ch)/([length2ch + length4ch]/2) (15). Maximum, minimum, and pre-atrial contraction LA volumes were extracted from volume curves which were calculated from apical 4- and 2-chamber views. The point on the LA volume curve during diastole just before the fast descent following a period of stability in LA volume was defined as pre-atrial (PreA) contraction volume. At that point, the atrial strain rate is equal to zero. If such a point could not be identified from the volume curve, only maximum and minimum volumes were reported. All measured volumes were indexed to body surface area. An example of an LA volume curve during a cardiac cycle is shown in Figure 1.
FIGURE 1. Feature Tracking Derived Left Atrial Volume and Strain Curves.
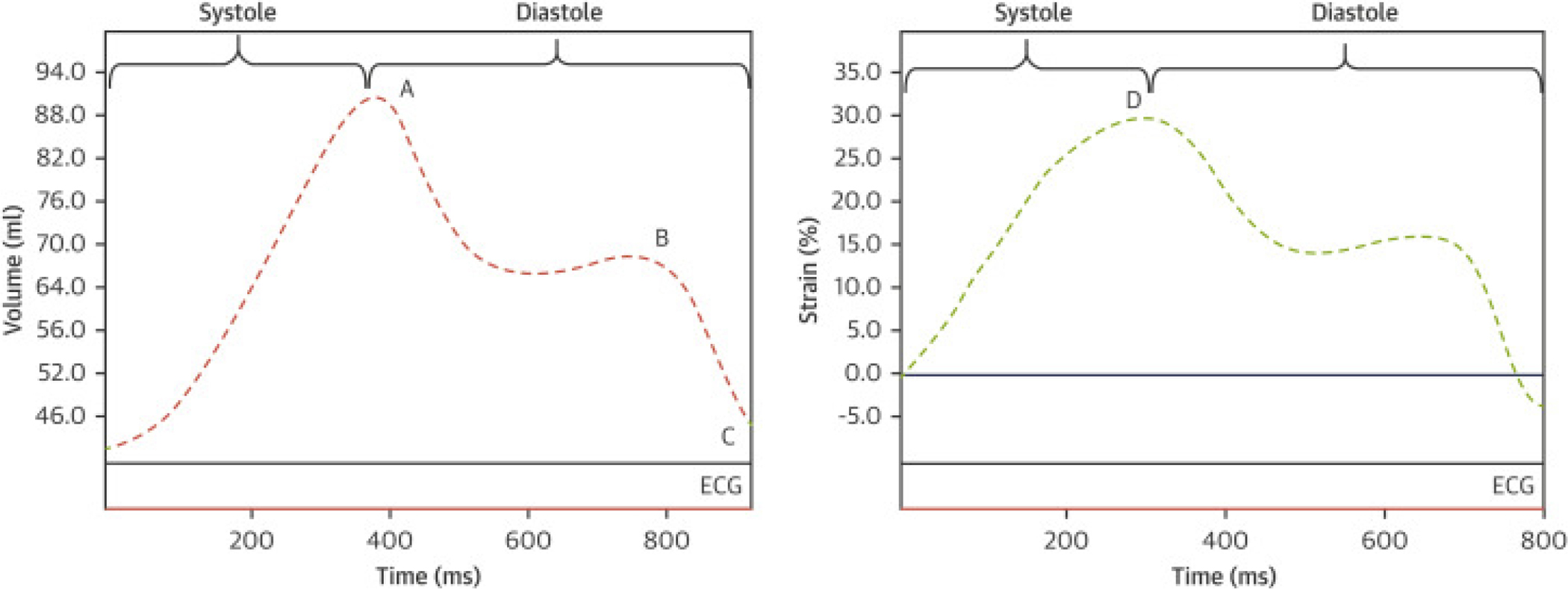
(Left) Changes in LA volume during cardiac cycle (ventricular systole and diastole). Maximum, pre-atrial contraction, and minimum LA volumes (points A, B, and C, respectively) were measured using LA volume curve. (Right) Changes in LA longitudinal strain during cardiac cycle. Point D indicates peak longitudinal strain. LA = left atrium.
We then calculated the volumetric LA function as follows:
STRAIN MEASUREMENT.
The software calculated the global longitudinal atrial strain by measuring fractional shortening or lengthening of each LA segment in 2- and 4-chamber views, using the defined LA borders during the cardiac cycle and averaging all segments. Global peak longitudinal LA strain (peak LA strain) was then extracted from the global longitudinal strain curve (Figure 1).
STATISTICAL ANALYSIS.
The baseline characteristics and LA parameters were compared between participants with and those without CVE, using the chi-square and t tests. Multivariate Cox proportional hazards models were used to determine the association of LA variables with incident ischemic CVE. Covariates were selected on the basis of the conceptual model and the association of these factors with incident ischemic CVE. The potential co-linearity was examined between continuous variables. Variables with Spearman correlation coefficient >0.50 were not included in the same multivariate model. The models included age, sex, race/ethnicity, body mass index, systolic and diastolic blood pressures, total cholesterol, high-density lipoprotein, cigarette smoking status, blood pressure medication use, statin use, diabetes mellitus, and left ventricular mass (model 1). To explore whether AF mediated associations between LA parameters and ischemic CVE, adjustments were also made for interim incident AF as a time-dependent covariate (model 2). Because in many cases the clinical diagnosis of AF follows a long period of subclinical AF (16), AF was adjusted for as a time-fixed covariate (i.e., with the assumption of AF presence since baseline as a subclinical form) (model 3). To explore the dose-response relationship of LA function with ischemic CVE, variables were modeled with restricted quadratic splines with knots at the 5th, 50th, and 95th percentiles of their distribution. To assess the additive value of LA parameters to the known ischemic CVE risk factors in predicting CVE, the area under the curve (AUC) was derived from receiver operating characteristic curve analysis (ROC). To assess the association of LA function and ischemic CVE in the absence of other known risk factors of stroke, the models were rerun in individuals with low stroke risk (CHA2DS2-VASc [Congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Prior stroke, transient ischemic attack [TIA], or thromboembolism, Vascular disease, Age 65–74 years, Sex category [female] score ≤1) and in those with no interim incident AF. In an additional step, adjustment was also made for the P-wave terminal force in lead V1 (PTFV1) and NT-proBNP as another known marker of LA remodeling to assess additive values of mechanical LA function variables. Statistical analyses were performed using STATA version 12.1 software (STATA Corp., College Station, Texas).
RESULTS
Of 5,004 participants with baseline CMR, 66 were excluded due to AF diagnosis prior to the enrollment. Other participants (n = 677) were excluded due to lack of either 2- or 4-chamber cine images through the LA, poor image quality, or low temporal resolution. It was feasible to measure LA volume in 4,261 participants (86.3%) and LA function in 4,214 participants (85.3%). After a mean follow-up of 11.6 ± 3.5 years, 193 individuals (4.5% of 4,261, 1.26 per 1,000 person-years) experienced incident ischemic CVE (134 cerebral infarctions and 59 TIAs).
Participant characteristics are summarized in Table 1. Individuals with ischemic CVE were older, had a less favorable cardiovascular risk profile, higher LV mass, higher levels of NT-proBNP, and higher prevalence of abnormal PTFVI. Participants with incident ischemic CVEs also developed more AF (30.7% vs. 12.4%, respectively) during the follow-up than those who did not have ischemic CVE. Of 193 participants with incident ischemic CVE, 34 (17.6%) were diagnosed with AF prior to or at the time of ischemic CVE, and 24 (12.4%) were diagnosed with AF after incident ischemic CVE, whereas 135 participants (70.0%) did not develop clinically recognized AF during the follow-up.
Table 1.
Baseline Characteristics of Study Participants With and Without Cerebrovascular Events During the Follow-Up Period
| Empty Cell | No Ischemic CVE (n = 4,068) | Ischemic CVE (n = 193) | p Value |
|---|---|---|---|
|
| |||
| Age, yrs | 61.2 ± 10.0 | 66.5 ± 9.2 | <0.001 |
| Male | 1,922 (47.2) | 98 (50.8) | 0.337 |
| Race/ethnicity | 0.003 | ||
| Caucasian | 1,599 (39.3) | 78 (40.4) | |
| Chinese | 510 (12.5) | 9 (4.7) | |
| African American | 1,071 (26.3) | 50 (25.1) | |
| Hispanic | 888 (21.8) | 56 (29.0) | |
| Body mass index, kg/m2 | 27.8 ± 5.0 | 28.7 ± 4.7 | 0.008 |
| Cholesterol, mg/dl | |||
| Total | 194.4 ± 35.4 | 194.1 ± 36.7 | 0.927 |
| LDL | 117.3 ± 31.1 | 117.5 ± 31.0 | 0.936 |
| HDL | 51.3 ± 14.9 | 47.9 ± 13.8 | 0.002 |
| Triglyceride | 129.8 ± 81.1 | 149.1 ± 137.3 | 0.002 |
| Cigarette smoking | 0.171 | ||
| Never | 2,077 (51.2) | 94 (49.0) | |
| Former | 1,463 (36.1) | 65 (33.8) | |
| Current | 516 (12.7) | 33 (17.2) | |
| Diabetes mellitus | 504 (12.4) | 41 (21.4) | <0.001 |
| Resting heart rate | 63.0 ± 9.4 | 63.5 ± 9.5 | 0.446 |
| Blood pressure, mm Hg | |||
| Systolic | 125.2 ± 21.3 | 136.8 ± 21.9 | <0.001 |
| Diastolic | 71.8 ± 10.3 | 74.8 ± 11.0 | <0.001 |
| Antihypertensive use | 1,415 (34.8) | 95 (49.5) | <0.001 |
| Statin use | 589 (14.5) | 30 (15.6) | 0.192 |
| Developed atrial fibrillation | 505 (12.4) | 58 (30.7) | <0.001 |
| LV mass, g | 145.7 ± 39.4 | 157.9 ± 42.7 | <0.001 |
| LV ejection fraction, % | 68.9 ± 7.4 | 68.6 ± 7.7 | 0.522 |
| PTFV1 >4,000, ms*μV | 101 (2.5) | 11 (5.7) | 0.007 |
| Log (NT-proBNP) | 3.9 ± 1.2 | 4.3 ± 1.2 | <0.001 |
CVE = cerebrovascular events; HDL = high density lipoprotein; LDL = low density lipoprotein; LV = left ventricle; NT-proBNP = N-terminal pro–B-type natriuretic peptide; PTFV1 = P-wave terminal force in lead V1.
Table 2 presents variables of LA volume and function. Participants with incident ischemic CVE had larger LA volumes with lower passive, active, and total LAEFs at baseline than individuals who did not develop ischemic CVE. However, LA longitudinal strain was comparable between the 2 groups. LA variables were also compared by strata of incident AF and incident CVE. As illustrated in Figure 2, individuals with either incident ischemic CVE or AF had larger LA with lower function at baseline than those with neither incident AF nor incident CVE (p < 0.001 for all LA variables).
Table 2.
Baseline Left Atrial Volumes and Function in Participants With and Without Incident Cerebrovascular Events
| Empty Cell | No Ischemic CVE (n = 4,068) | Ischemic CVE (n = 193) | p Value |
|---|---|---|---|
|
| |||
| LAVImax, ml/m2 | 30.1 ± 9.7 | 32.4 ± 13.2 | 0.002 |
| LAVImin, ml/m2 | 15.9 ± 6.6 | 18.4 ± 10.0 | >0.001 |
| Passive LAEF, % | 20.4 ± 9.1 | 18.6 ± 8.2 | 0.009 |
| Active LAEF, % | 34.0 ± 10.0 | 31.3 ± 11.3 | <0.001 |
| Total LAEF, % | 47.6 ± 9.9 | 43.9 ± 11.0 | <0.001 |
| LA Strain, % | 30.6 ± 12.2 | 30.8 ± 14.8 | 0.805 |
Values are mean ± SD.
LA = left atrium; LAEF = left atrial emptying fraction; LAVImax = maximum left atrial volume index; LAVImin = minimum left atrial volume index; other abbreviations as in Table 1.
FIGURE 2. Atrial Variables by Strata of Atrial Fibrillation and Stroke/TIA.
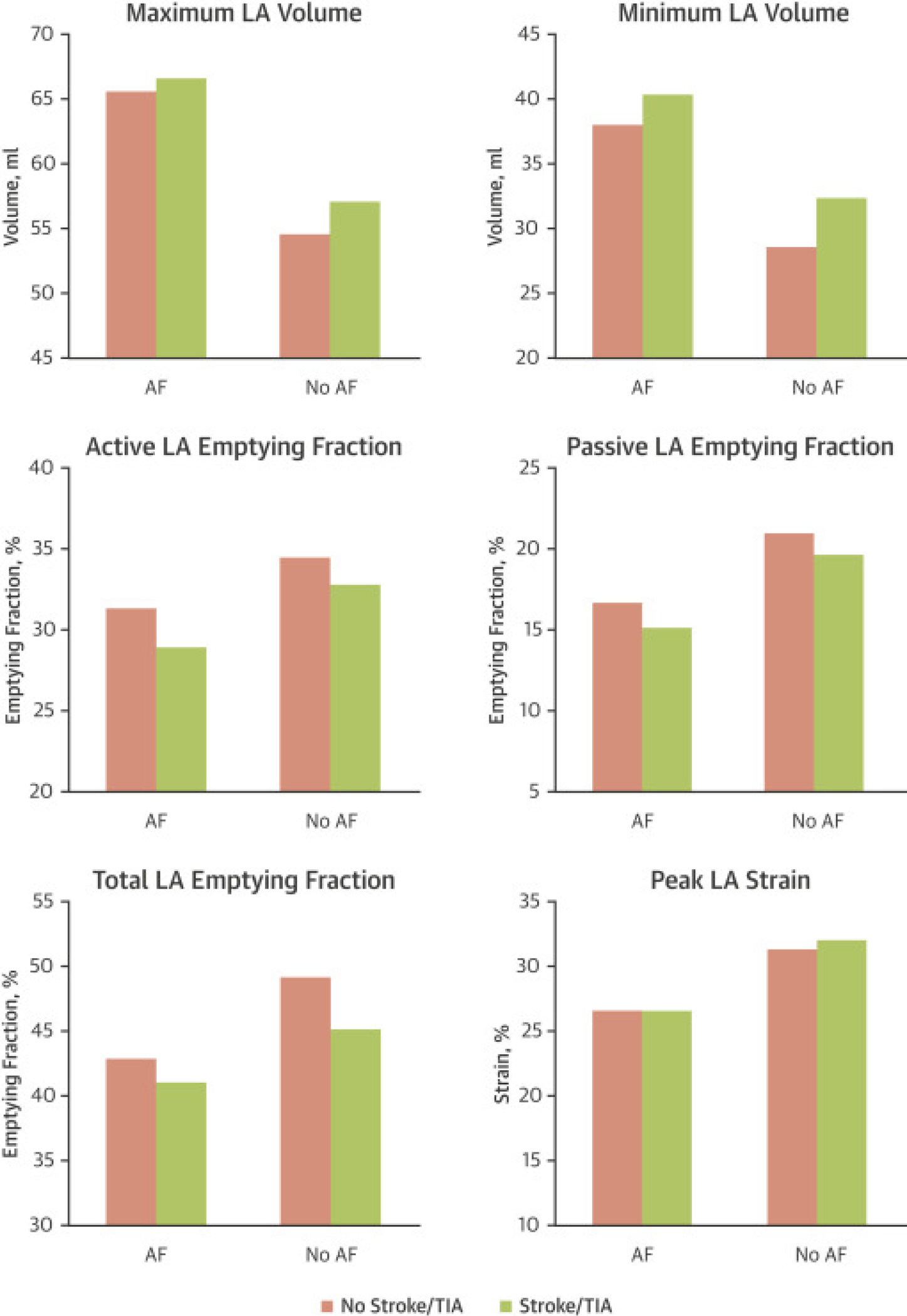
Bars demonstrate the means of each measured atrial variable by strata of atrial fibrillation and ischemic cerebrovascular events. AF = atrial fibrillation; LA = left atrial; TIA = transient ischemic attack.
In the multivariate model (model 1), minimum but not maximum LA volume index was associated with incident ischemic CVE (hazard ratio [HR]: 1.18 per SD of left atrial volume index [LAVImin]; 95% confidence interval [CI]: 1.04 to 1.34). Among LA functional variables, active and total LAEF were inversely associated with incident ischemic CVE (HR for active LAEF: 0.84 per SD; 95% Cl: 0.73 to 0.97; HR for total LAEF: 0.80 per SD; 95% CI: 0.69 to 0.92). After AF was adjusted for, whether as a time-dependent or a time-fixed covariate, the association attenuated but remained significant for total LAEF (HR: 0.85 per SD; 95% CI: 0.71 to 0.97 in model 2, and HR: 0.83 per SD; 95% CI: 0.71 to 0.97 in model 3). However, the associations between LAVImin and active LAEF with ischemic CVE were not significant after adjusting for interim AF. These associations are shown in Table 3.
Table 3.
Association Between Left Atrial Volume and Function and Incident Ischemic Cerebrovascular Event
| Empty Cell | Model 1 | Model 2 | Model 3 | |||
|---|---|---|---|---|---|---|
|
| ||||||
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
|
| ||||||
| LAVImax, ml/m2 | 1.12 (0.98–1.28) | 0.100 | 1.02 (0.88–1.18) | 0.769 | 1.06 (0.92–1.21) | 0.412 |
| LAVImin, ml/m2 | 1.18 (1.04–1.34) | 0.009 | 1.09 (0.96–1.24) | 0.183 | 1.10 (0.97–1.27) | 0.134 |
| Passive LAEF, % | 0.93 (0.80–1.08) | 0.351 | 0.97 (0.83–1.13) | 0.688 | 0.96 (0.83–1.12) | 0.626 |
| Active LAEF, % | 0.84 (0.73–0.97) | 0.018 | 0.88 (0.76–1.01) | 0.074 | 0.87 (0.75–1.01) | 0.057 |
| Total LAEF, % | 0.80 (0.69–0.92) | 0.002 | 0.85 (0.74–0.98) | 0.027 | 0.83 (0.72–0.96) | 0.013 |
| LA Strain, % | 1.06 (0.94–1.21) | 0.308 | 1.11 (0.98–1.26) | 0.088 | 1.09 (0.97–1.24) | 0.150 |
Model 1 is adjusted for age, sex, ethnicity, body mass index, cigarette smoking, systolic and diastolic blood pressures, use of antihypertension medications, total cholesterol, high-density lipoprotein, statin use, diabetes mellitus, and left ventricular mass. Model 2 consists of variables in model 1 and interim incident atrial fibrillation as a time-dependent covariate. Model 3 consists of variables in model 1 and atrial fibrillation as a time-fixed covariate. Hazard ratios were calculated according to ±SD changes in LA variables.
CI = confidence interval; other abbreviations as in Table 2.
Figure 3 shows the association between total LAEF and ischemic CVE, using a restricted cubic spline model adjusted for baseline covariates. When assessed by tertiles, the relationship between total LAEF and incident ischemic CVE was significant and graded. When adjusted for covariates, the lowest tertile of total LAEF compared to the highest tertile was 2.0 (95% Cl: 1.43 to 2.79; p < 0.001), and adjusted for demographics, the clinical risk factors and interim AF was 1.47 (95% Cl: 1.04 to 2.05; p 0.031). Figure 4 shows the Kaplan-Meier analyses graphs for incident ischemic CVE based on tertiles of total LAEF.
FIGURE 3. Total Left Atrial Emptying Fraction and Incident Ischemic Cerebrovascular Events.
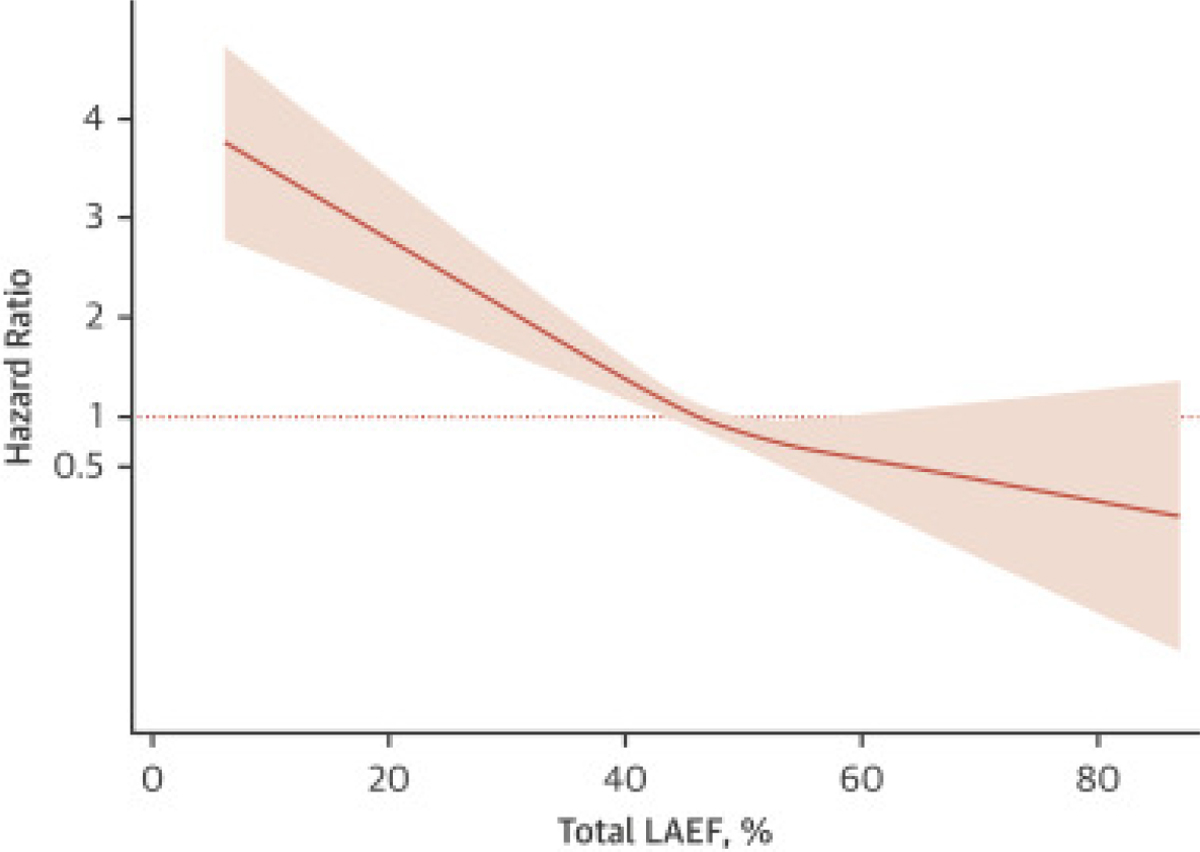
The plot demonstrates the results of a restricted cubic spline model. The pink area above and below the pink line indicates the 95% confidence interval.
FIGURE 4. Kaplan-Meier Event-Free Survival Curves.
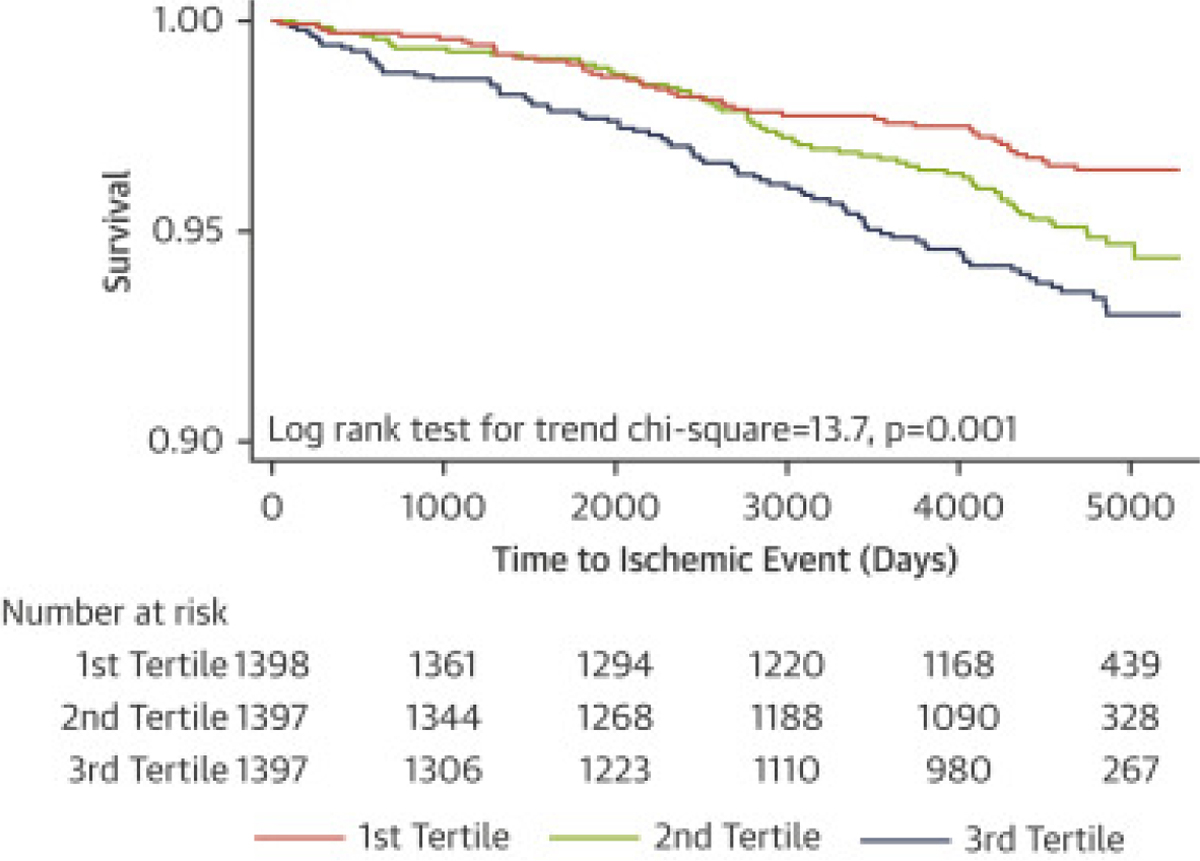
Kaplan-Meier survival curves showing the event-free survival of participants based on tertiles of total left atrial emptying fraction. The first tertile includes participants with the highest total LAEF, and the third tertile includes participants with the lowest total LAEF. LAEF = left atrial emptying fraction.
To examine the incremental value of total LAEF in risk stratification of participants for ischemic CVE, the AUC was calculated in a basic model including variables in model 1. The addition of total LAEF to the basic model improved the AUC from 0.73 to 0.76 (p = 0.039).
SUBGROUP ANALYSES.
In 3,525 participants with available measurements, additional adjustment for log-transformed NT-proBNP and PFTV1, the association between total LAEF and ischemic CVE remained essentially unchanged (Supplemental Table 2).
To minimize the possibility of residual bias and to assess the value of LA remodeling in participants with low baseline stroke risk, a subanalysis was performed in 2,187 individuals with a CHA2DS2-VASc score of ≤1. In model 1, after adjusting for remaining stroke risk factors not reflected in CHA2DS2-VASc score, total LAEF was still significantly associated with ischemic CVE (HR per SD: 0.58; 95% Cl: 0.44 to 0.77). The association remained significant after adjusting for interim incident AF in models 2 and 3 as a time-dependent or time-fixed covariate, respectively (HR: 0.60 per SD; 95% CI: 0.45 to 0.80 in model 2, and HR: 0.60 per SD; 95% CI: 0.45 to 0.80 in model 3). Figure 5 shows the Kaplan-Meier analyses graphs for incident ischemic CVE based on tertiles of total LAEF in participants with a CHA2DS2-VASc score ≤1. The association between total LAEF and ischemic CVE also remained significant after excluding individuals with interim incident AF (HR: 0.67 per SD; 95% Cl: 0.49 to 0.93).
FIGURE 5. Kaplan-Meier Event-Free Survival Curves in Individuals With CHA2DS2-VASc Score ≤1.
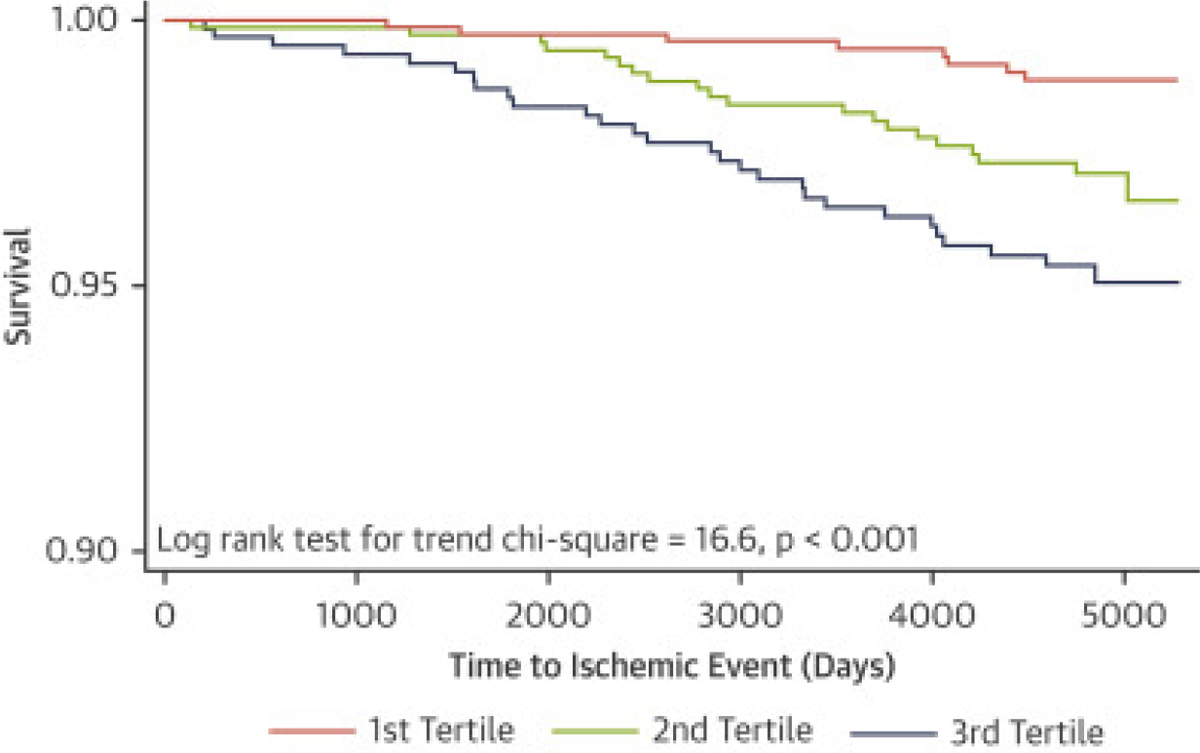
Kaplan-Meier survival curves show the event-free survival of participants based on tertiles of total left atrial emptying fraction. The first tertile includes participants with the highest total LAEF, and the third tertile includes participants with the lowest total LAEF. CHA2DS2-VASc = congestive heart failure, Hypertension, Age ≥75 years, Diabetes mellitus, Prior stroke, transient ischemic attack [TIA], or thromboembolism, Vascular disease, Age 65–74 years, Sex category [female]); other abbreviations as in Figure 4.
DISCUSSION
This prospective multiethnic population-based study of individuals free of clinical cardiovascular disease demonstrated an inverse association between total LAEF, as a marker of global/reservoir LA function, and incident ischemic CVE. This association was independent of known cerebrovascular disease risk factors and interim incident AF and persisted in participants with low stroke risk factors. Total LAEF improved risk stratification of individuals with no known cardiovascular disease for ischemic stroke development.
Alterations in LA size and, more importantly, LA function are associated with cardiovascular disease in the general population and with poor outcomes in patients with cardiovascular disease (2). The contribution of LA remodeling is even more prominent in the pathogenesis of AF and stroke. Therefore, in the past few years significant efforts have been directed toward quantification and implementation of LA remodeling measurements in risk stratification of patients with cardiovascular disease, especially those with AF. Changes in P-wave morphology and elevated NT-proBNP concentration as indirect markers of LA structural and mechanical changes were associated with incident CVE independent of AF (8–11,17). These observations suggest that LA mechanical dysfunction may directly affect the stroke risk. Due to the anatomic profile of LA, direct assessment of LA mechanical function is challenging. In this study feature-tracking CMR was used to analyze phasic LA function by using a volumetric method to calculate LAEFs and deformation analysis to measure LA strain during the cardiac cycle.
LEFT ATRIAL SIZE AND FUNCTION IN RELATION TO ISCHEMIC STROKE.
LA enlargement is associated with incidence or prevalence of stroke in a general population and in patients with previous stroke independent of AF (6,7,18). Similar findings are observed in elderly patients (19) and in women (20). In contrast, in our study, minimum LA volume was a risk factor for incident CVE; however, this association was not independent of interim AF.
Most studies of LA mechanical function and stroke have been performed in patients with known cardiac disease, especially AF, or those with previous ischemic stroke (3,21). Those studies found lower LAEF, strain, and strain rates in patients with or without AF but with previous stroke (22–24). Lower LA strain is also associated with high-risk transesophageal echoradiography features of cardioembolism in patients who presented with acute stroke (25). In patients with AF, LA reservoir function has incremental value when added to the CHA2DS2-VASc score for risk of previous stroke events (4,5). In a study on 983 individuals with stable coronary heart disease, lower LA functional index was associated with ischemic stroke (26). Other supporting evidence of the role of LA contractile dysfunction in stroke comes from cardiac conditions such as amyloidosis and myosin light chain mutation, which involve predominantly LA and are associated with higher risk of stroke, even in the absence of AF (27,28).
To the best of the present authors’ knowledge, no other prospective study has investigated the association between mechanical LA function and ischemic CVE in a general population free of clinical cardiovascular disease. The present study showed an association between lower LA reservoir function and incident ischemic CVE independent of interim AF. Our findings complement previous retrospective and cross-sectional studies in patients with stroke and known AF. Importantly, in the present study this association persisted in low-risk population with a CHA2DS2-VASc score of ≤1 and was additive to other known markers of LA remodeling.
ATRIAL REMODELING AND ISCHEMIC STROKE: POSSIBLE MECHANISMS.
The exact contribution of LA to the pathogenesis of thromboembolic events is not fully understood. Results from population-based studies confirm the presence of LA remodeling before AF development (1,29). Therefore, LA dysfunction might be a marker of future AF episodes that leads to ischemic CVE. However, observations from patients with implanted rhythm monitoring devices do not confirm a temporal association between AF episodes and stroke events. In the ASSERT (Asymptomatic Atrial Fibrillation and Stroke Evaluation in Pacemaker Patients and the Atrial Fibrillation Reduction Atrial Pacing Trial), only 8% of the patients with stroke had AF episodes within 30 days prior to their CVE, whereas 16% of the stroke cases had their first AF episode after their strokes (30). Another study of patients with dual-chamber and biventricular defibrillators also found no temporal association between atrial tachyarrhythmia and thromboembolism (31). In this study, only 30.7% of participants with ischemic CVE had interim incident AF. Furthermore, the association between LA remodeling and ischemic CVE was present in those with no incident AF. Electrical markers of atrial myopathy and LA size have been specifically associated with cryptogenic or embolic stroke and not with cerebral small vessel occlusion (9,17,32). Therefore, in addition to be a marker of future AF episodes, LA dysfunction may be an independent risk factor for blood stasis and thromboembolism events. Although this hypothesis is intuitively appealing, several studies suggest a more complex stroke mechanism in patients with AF or atrial myopathy. Many of the underlying processes leading to atrial myopathy such as aging, hypertension, diabetes, smoking, inflammation, heart failure, and LV hypertrophy are also known risk factors for stroke unrelated to emboli from LA (Central Illustration) (2,3). A cross-sectional study shows an association between LA dysfunction and known stroke risk factors and also with silent infarcts found in brain MRI (33). Although there is a strong correlation between AF and ischemic stroke, 10% of patients with lacunar stroke also have AF. Large-artery atherosclerosis is also more common in AF patients compared to those with no AF (34).
Central Illustration. Factors leading to LA Remolding and Their Relationships to Ischemic Stroke.
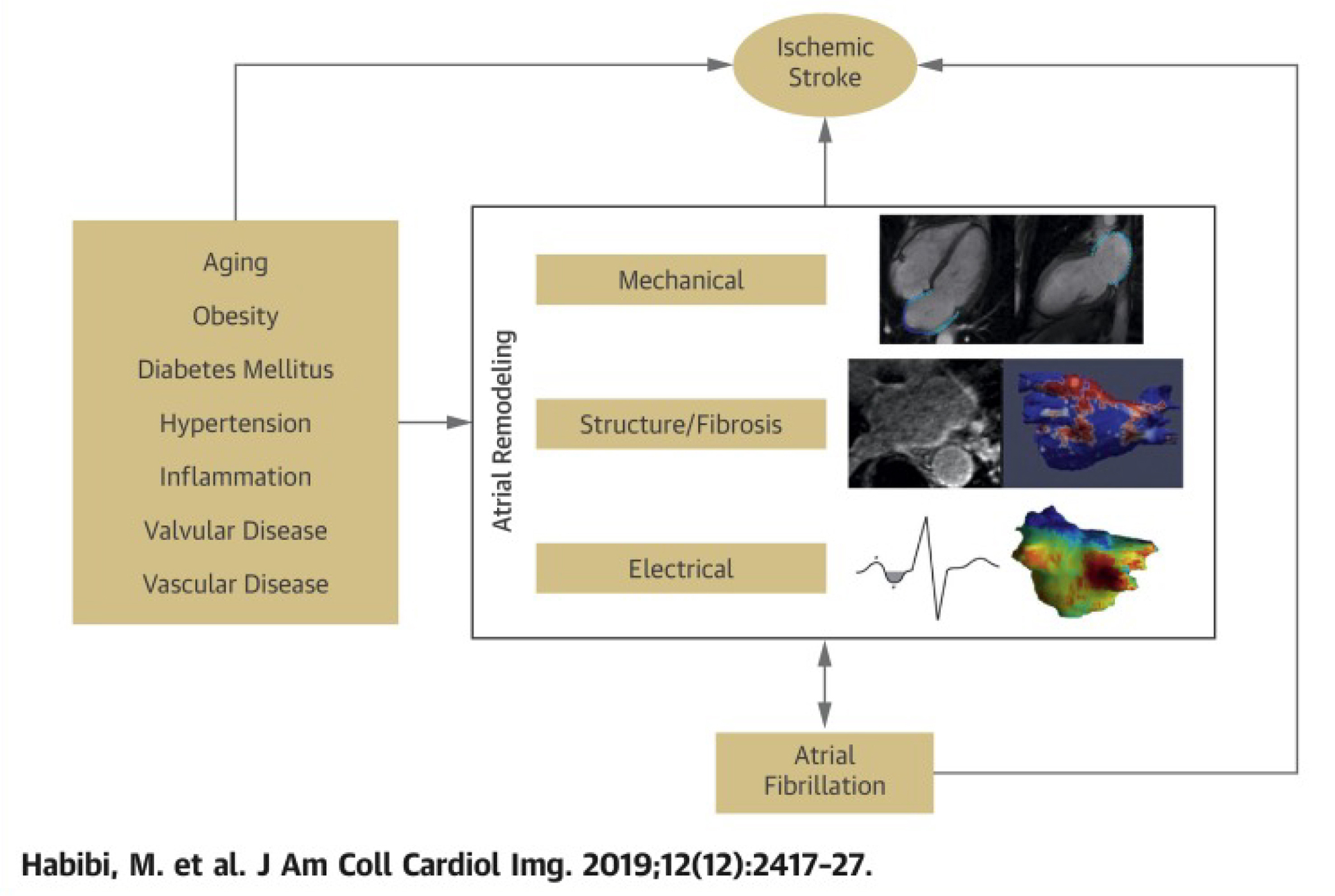
Shared risk factors results in mechanical, structural, and electrical LA remodeling. Electrical changes promote AF development which also worsens LA remodeling. Mechanical changes increase blood stasis and risk of thromboembolism.
In the present study, the association between atrial mechanical dysfunction and incident ischemic CVE was attenuated after adjustments were made for known stroke risk factors. This indicates that LA dysfunction may be a marker for coexisting risk factors leading to stroke through mechanisms outside the LA. Although a higher incidence of ischemic CVE is still found in individuals with lower total LAEF but otherwise low-stroke risk factors (e.g., CHA2DS2-VASc score ≤1), data for ischemic stroke subtypes were not available for this study.
POTENTIAL CLINICAL IMPLICATIONS.
Several studies have shown the usefulness of including mechanical LA functional measures in risk stratification of individuals for ischemic CVE in the absence of clinical AF. However, except for the maximum LA volume, other parameters of LA function are not routinely measured in clinical settings. CMR was used for analyzing LA function, but those measurements were also obtainable using 2D or 3D echocardiography in clinical settings. Diagnosis of atrial cardiomyopathy may also have therapeutic and preventive implications. Emerging evidence supports upstream effects of angiotensin-converting enzyme inhibitors, aldosterone blockers, and statins in prevention of AF in high-risk populations (35–37). Although data for the role of these medications in LA reverse remodeling in humans are limited, future studies of the effects of risk-factor modifications and also medical therapy on LA reverse remodeling and subsequent incident ischemic stroke in susceptible populations are of great value. In addition, presence of atrial myopathy may be useful for decision making in initiation of anticoagulation in a high-risk population. Results of the ongoing ARCADIA (Atrial Cardiopathy and Antithrombotic Drugs In Prevention After Cryptogenic Stroke) trial will help us to understand whether diagnosis of atrial cardiomyopathy in ischemic stroke patients with no known AF warrants anticoagulation (38). However, use of a combination of low-dose anticoagulation and aspirin such as that shown to be beneficial in the COMPASS (Rivaroxaban for the Prevention of Major Cardiovascular Events in Coronary or Peripheral Artery Disease) trial needs further investigations (39).
STUDY LIMITATIONS.
A few limitations in this study should be addressed. CMR images were acquired in the time period between 2000 and 2002; since that time, cine CMR sequences have improved, with higher temporal and spatial resolution. Therefore, CMR images were not interpretable for the assessment of LA function in 14% of the study population. However, this percentage is about the same or lower than those in other studies using speckle-tracking echocardiography in measurements of LA function (40). The lower temporal resolution might have resulted in lower accuracy of strain measurements. The area-length method was used to measure LA volumes. Therefore, the calculated volumes may be an underestimation of the true volumes by 11.5% to 20%, depending on the alignment of the acquired slice with true orientation of LA (15,41). However, this method is widely used in clinical and research studies (42). Incident AF was identified based on hospital discharge codes and MESA follow-up visits, which may underestimate AF diagnosis as many of AF cases are asymptomatic and do not require hospitalization. A validation substudy of 45 MESA participants with the diagnosis of AF based on hospital discharge codes confirmed the diagnosis of AF in 93% of the hospitalizations (43). Additionally, based on a systematic review using information from 16 unique studies, a large proportion of prevalent AF cases identified by International Classification of Diseases, Ninth Revision codes were valid (positive predictive value 70% to 96%; median, 89%) (44). Individuals with the new diagnosis of AF may have had undiagnosed subclinical AF at baseline. AF was adjusted as both a time-dependent variable and time-fixed covariate with the assumption of AF presence since baseline.
CONCLUSIONS
An inverse association was found between LA reservoir function, measured as total LAEF, and the risk of CVE. This association was independent of known cerebrovascular risk factors and AF. These findings complement other studies in questioning whether AF itself is always required in the pathogenesis of cardiac thromboembolism. These findings suggest possible value of LA functional parameters in stratification of individuals at risk for ischemic CVE especially those with no clear evidence of AF.
Supplementary Material
PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE:
In individuals with no clinical cardiovascular disease, CMR measured LA mechanical dysfunction is associated with incident ischemic CVE independent of known cardiovascular risk factors and interim AF. This association persisted in individuals with low CVE risk factors. Addition of LA mechanical function to known clinical risk factors of ischemic CVE improves risk prediction accuracy.
TRANSLATIONAL OUTLOOK:
Future studies are required to explore possible benefits of anticoagulation in patients with atrial myopathy in the absence of known AF. In addition, potential role of interventions leading to atrial reverse remodeling in reducing the risk of stroke needs to be investigated.
ACKNOWLEDGMENTS
The authors thank the investigators, staff, and participants of the MESA study for their valuable contributions. A full list of participating MESA investigators and institutions can be found at the MESA (Multi-Ethnic Study of Atherosclerosis) website.
Supported by National Heart, Lung, and Blood Institute contracts Noi-HC-95159 through No1-HC-95166, N01-HC-95168, and R01HL127659; and National Center for Research Resources, National Institutes of Health contracts UL1-RR-024156 and UL1-RR-025005. The views expressed in this paper are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute, the National Institutes of Health, or the U.S. Department of Health and Human Services. Dr. Shea has received funding from National Heart, Lung, and Blood Institute. Dr. Gottesman is an Associate Editor for the Journal of Neurology. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
ABBREVIATIONS AND ACRONYMS
- AF
atrial fibrillation
- CMR
cardiac magnetic resonance
- CVE
cerebrovascular events
- LA
left atrium
- LAEF
left atrial emptying fraction
- LAV
left atrial volume
- LAVI
left atrial volume index
- TIA
transient ischemic attack
Footnotes
APPENDIX For an expanded Methods section as well as supplemental tables, a video, and references, please see the online version of this paper.
REFERENCES
- 1.Habibi M, Samiei S, Ambale Venkatesh B, et al. Cardiac magnetic resonance-measured left atrial volume and function and incident atrial fibrillation: results from MESA (Multi-Ethnic Study of Atherosclerosis). Circ Cardiovasc Imaging 2016;9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hoit BD. Left atrial size and function: role in prognosis. J Am coli Cardiol 2014;63:493–505. [DOI] [PubMed] [Google Scholar]
- 3.Goldberger JJ, Arora R, Green D, et al. Evaluating the atrial myopathy underlying atrial fibrillation: identifying the arrhythmogenic and thrombogenic substrate. Circulation 2015;132:278–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Inoue YY, Alissa A, Khurram IM, et al. Quantitative tissue-tracking cardiac magnetic resonance (CMR) of left atrial deformation and the risk of stroke in patients with atrial fibrillation. J Am Heart Assoc 2015;4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Obokata M, Negishi K, Kurosawa K, et al. Left atrial strain provides incremental value for embolism risk stratification over CHA (2)DS (2)-VASc score and indicates prognostic impact in patients with atrial fibrillation. J Am Soc Echocardiogr 2014;27:709–16. [DOI] [PubMed] [Google Scholar]
- 6.Benjamin EJ, D’Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham heart study. Circulation 1995;92:835–41. [DOI] [PubMed] [Google Scholar]
- 7.Nagarajarao HS, Penman AD, Taylor HA, et al. The predictive value of left atrial size for incident ischemic stroke and all-cause mortality in African Americans: the Atherosclerosis Risk in Communities (ARIC) study. Stroke 2008;39:2701–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kamel H, Bartz TM, Longstreth WT Jr., et al. Association between left atrial abnormality on ECG and vascular brain injury on MRI in the Cardiovascular Health Study. Stroke 2015;46:711–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kamel H, O’Neal WT, Okin PM, Loehr LR, Alonso A, Soliman EZ. Electrocardiographic left atrial abnormality and stroke subtype in the atherosclerosis risk in communities study. Ann Neurol 2015;78:670–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kamel H, Soliman EZ, Heckbert SR, et al. P-wave morphology and the risk of incident ischemic stroke in the Multi-Ethnic Study of Atherosclerosis. Stroke 2014;45:2786–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kamel H, Bartz TM, Elkind MSV, et al. Atrial cardiopathy and the risk of ischemic stroke in the CHS (Cardiovascular Health Study). Stroke 2018;49:980–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study of atherosclerosis: objectives and design. Am J Epidemiol 2002;156:871–81. [DOI] [PubMed] [Google Scholar]
- 13.Natori S, Lai S, Finn JP, et al. Cardiovascular function in multi-ethnic study of atherosclerosis: normal values by age, sex, and ethnicity. AJR Am J Roentgenol 2006;186:S357–65. [DOI] [PubMed] [Google Scholar]
- 14.Zareian M, Ciuffo L, Habibi M, et al. Left atrial structure and functional quantitation using cardiovascular magnetic resonance and multimodality tissue tracking: validation and reproducibility assessment. J Cardiovasc Magn Reson 2015;17:52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rodevan O, Bjornerheim R, Ljosland M, Maehle J, Smith HJ, lhlen H. Left atrial volumes assessed by three- and two-dimensional echocardiography compared to MRI estimates. Int J Cardiac Imaging 1999;15:397–410. [DOI] [PubMed] [Google Scholar]
- 16.Healey JS, Connolly SJ, Gold MR, et al. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med 2012;366:120–9. [DOI] [PubMed] [Google Scholar]
- 17.Kamel H, Hunter M, Moon YP, et al. Electrocardiographic left atrial abnormality and risk of stroke: northern Manhattan study. Stroke 2015;46:3208–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Di Tullio MR, Sacco RL, Sciacca RR, Homma S. Left atrial size and the risk of ischemic stroke in an ethnically mixed population. Stroke 1999;30:2019–24. [DOI] [PubMed] [Google Scholar]
- 19.Pierdomenico SD, Pierdomenico AM, Di Carlo S, Di Tommaso R, Cuccurullo F. Left atrial enlargement and risk of ischemic stroke in elderly treated hypertensive patients. Am J Hypertens 2014;27:1179–84. [DOI] [PubMed] [Google Scholar]
- 20.Bouzas-Mosquera A, Broullon FJ, AlvarezGarcia N, et al. Left atrial size and risk for all-cause mortality and ischemic stroke. CMAJ 2011;183:E657–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Delgado V, Di Biase L, Leung M, et al. Structure and function of the left atrium and left atrial appendage: AF and stroke implications. J Am Coll Cardiol 2017;70:3157–72. [DOI] [PubMed] [Google Scholar]
- 22.Leong DP, Joyce E, Debonnaire P, et al. Left atrial dysfunction in the pathogenesis of cryptogenic stroke: novel insights from speckle-tracking echocardiography. J Am Soc Echocardiogr 2017;30:71–9. [DOI] [PubMed] [Google Scholar]
- 23.Shih JY, Tsai WC, Huang YY, et al. Association of decreased left atrial strain and strain rate with stroke in chronic atrial fibrillation. J Am Soc Echocardiogr 2011;24:513–9. [DOI] [PubMed] [Google Scholar]
- 24.Sanchis L, Montserrat S, Obach V, et al. Left atrial function is impaired in some patients with stroke of undetermined etiology: potential implications for evaluation and therapy. Rev Esp Cardiol (Engl Ed) 2016;69:650–6. [DOI] [PubMed] [Google Scholar]
- 25.Kim D, Shim CY, Hong GR, et al. Clinical implications and determinants of left atrial mechanical dysfunction in patients with stroke. Stroke 2016;47:1444–51. [DOI] [PubMed] [Google Scholar]
- 26.Wong JM, Welles CC, Azarbal F, Whooley MA, Schiller NB, Turakhia MP. Relation of left atrial dysfunction to ischemic stroke in patients with coronary heart disease (from the heart and soul study). Am J Cardiol 2014;113:1679–84. [DOI] [PubMed] [Google Scholar]
- 27.Hausfater P, Costedoat-Chalumeau N, Amoura Z, et al. AL cardiac amyloidosis and arterial thromboembolic events. Scand J Rheumatol 2005;34:315–9. [DOI] [PubMed] [Google Scholar]
- 28.Peng W, Li M, Li H, et al. Dysfunction of myosin light-chain 4 (MYL4) leads to heritable atrial cardiomyopathy with electrical, contractile, and structural components: evidence from genetically-engineered rats. J Am Heart Assoc 2017;6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham heart study. Circulation 1994;89:724–30. [DOI] [PubMed] [Google Scholar]
- 30.Brambatti M, Connolly SJ, Gold MR, et al. Temporal relationship between subclinical atrial fibrillation and embolic events. Circulation 2014;129:2094–9. [DOI] [PubMed] [Google Scholar]
- 31.Martin DT, Bersohn MM, Waldo AL, et al. Randomized trial of atrial arrhythmia monitoring to guide anticoagulation in patients with implanted defibrillator and cardiac resynchronization devices. Eur Heart J 2015;36:1660–8. [DOI] [PubMed] [Google Scholar]
- 32.Yaghi S, Moon YP, Mora-McLaughlin C, et al. Left atrial enlargement and stroke recurrence: the Northern Manhattan Stroke Study. Stroke 2015;46:1488–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Russo C, Jin Z, Liu R, et al. LA volumes and reservoir function are associated with subclinical cerebrovascular disease: the CABL (Cardiovascular Abnormalities and Brain Lesions) study. J Am Coll Cardiol Img 2013;6:313–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kamel H, Okin PM, Elkind MS, ladecola C. Atrial fibrillation and mechanisms of stroke: time for a new model. Stroke 2016;47:895–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Zhang Y, Zhang P, Mu Y, et al. The role of renin-angiotensin system blockade therapy in the prevention of atrial fibrillation: a meta-analysis of randomized controlled trials. Clin Pharmacol Ther 2010;88:521–31. [DOI] [PubMed] [Google Scholar]
- 36.Swedberg K, Zannad F, McMurray JJ, et al. Eplerenone and atrial fibrillation in mild systolic heart failure: results from the EMPHASIS-HF (Eplerenone in Mild Patients Hospitalization And Survival Study in Heart Failure) study. J Am Coll Cardiol 2012;59:1598–603. [DOI] [PubMed] [Google Scholar]
- 37.Wang Z, Zhang Y, Gao M, et al. Statin therapy for the prevention of atrial fibrillation: a meta-analysis of randomized controlled trials. Pharmacotherapy 2011;31:1051–62. [DOI] [PubMed] [Google Scholar]
- 38.Kamel H, Longstreth WT Jr., Tirschwell DL, et al. The AtRial cardiopathy and antithrombotic drugs in prevention after cryptogenic stroke randomized trial: rationale and methods. Int J Stroke 2018. 1747493018799981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Eikelboom JW, Connolly SJ, Bosch J, et al. Rivaroxaban with or without aspirin in stable cardiovascular disease. N Engl J Med 2017;377:1319–30. [DOI] [PubMed] [Google Scholar]
- 40.Kumagai K, Nakashima H, Urata H, Gondo N, Arakawa K, Saku K. Effects of angiotensin II type 1 receptor antagonist on electrical and structural remodeling in atrial fibrillation. J Am Coll Cardiol 2003;41:2197–204. [DOI] [PubMed] [Google Scholar]
- 41.Vardoulis O, Monney P, Bermano A, et al. Single breath-hold 3D measurement of left atrial volume using compressed sensing cardiovascular magnetic resonance and a non-model-based reconstruction approach. J Cardiovasc Magn Reson 2015;17:47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am soc Echocardiogr 2015;28:1–39 e14.. [DOI] [PubMed] [Google Scholar]
- 43.Patton KK, Heckbert SR, Alonso A, et al. N-terminal pro-B-type natriuretic peptide as a predictor of incident atrial fibrillation in the Multi-Ethnic Study of Atherosclerosis: the effects of age, sex and ethnicity. Heart 2013;99:1832–6. [DOI] [PubMed] [Google Scholar]
- 44.Jensen PN, Johnson K, Floyd J, Heckbert SR, Carnahan R, Dublin S. A systematic review of validated methods for identifying atrial fibrillation using administrative data. Pharmacoepidemiol Drug Saf 2012;21 suppl 1:141–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.