

Introduction
A 38 -year-old woman presented with redness, pain, and blurred vision in her right eye for a duration of 10 days. Among her medical history was a recent diagnosis of Crohn's disease, treated with azathioprine for 2 months. Her best-corrected visual acuity was 20/30 in the right eye and 20/20 in the left eye. Findings under the slit-lamp and anterior segment optical coherence tomography (ASOCT) are presented in Figures 1 and 2.
Figure 1.
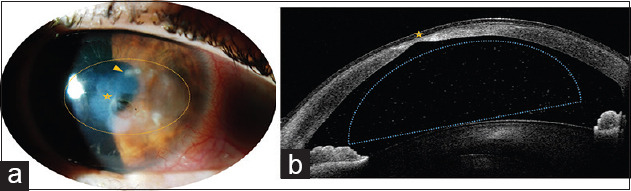
Slit lamp (a) and ASOCT (b) findings of the right eye at presentation
Figure 2.
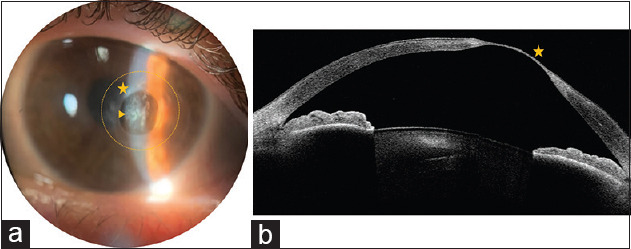
Same patient 1 month after the resolution of the initial presentation. The patient was afflicted with moderate eye discomfort, watering, and photophobia. (a) Slit-lamp photograph. (b) anterior segment tomography
Questions
Answers for Clinical Quiz
Answers
Figure 1: Herpetic necrotizing stromal keratitis. (a) slit-lamp exploration: Stromal disciform infiltrate (orange dashed circle), granulomatous keratic precipitates under the edematous lesion (some marked with an orange arrowhead), melting and corneal descemetocele (orange star) (b) ASOCT: Anterior chamber reaction (hyperreflective points inside the anterior chamber, blue dashed line) and descemetocele formation (orange star)
Figure 2: Herpetic dendritic epithelial lesion (orange arrowhead) over a preexisting corneal descemetocele (orange star) in the context of a likely necrotizing stromal keratitis incipient relapse (orange dashed circle). (a) slit-lamp exploration; (b) ASOCT
Topical corticosteroids and oral antiviral at therapeutic dosage. Bacterial keratitis should always be covered. If keratolysis is a prominent feature, bondage might be placed
A necrotizing stromal keratitis with a rapid development descemetocele should always be considered for a penetrating keratoplasty.
Discussion
Herpetic eye disease is the leading cause of infectious blindness in developed countries.[1]
It can involve any layer of the cornea, the harmful mechanism being a mixture between direct viral injury and autoimmune processes. In necrotizing stromal keratitis, direct viral activity is considered to be the main tissular aggressor.
Clinically, it is presented as stromal keratitis with epithelial ulceration. Keratolysis is of great concern. Melting can rapidly lead to descemetocele formation or corneal perforation. It can also involve granulomatous keratic precipitates and anterior chamber reaction. Limbal insufficiency, scarring, and lipid deposition can ensue.[2]
The diagnosis, as with the rest of stromal keratitis, is mainly clinical.
The recommended treatment regime is topical prednisolone acetate 1% one to four times daily and an oral antiviral at a therapeutic dosage. In this case, valacyclovir 1 g three times daily was used. Bacterial and fungal keratitis must be considered, and bacterial keratitis must be empirically covered until the microbiological results are given.[2,3] Herein, microbiological samples were taken, fulminant presentation by other microbial agents was ruled out, and herpetic etiology was confirmed.
In the case of severe sequelae or impending perforation, penetrating keratoplasty should be performed. This being so in the presented case.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initial s will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Farooq AV, Shah A, Shukla D. The role of herpesviruses in ocular infections. Virus Adapt Treat. 2010;2:115–23. [Google Scholar]
- 2.Valerio GS, Lin CC. Ocular manifestations of herpes simplex virus. Curr Opin Ophthalmol. 2019;30:525–31. doi: 10.1097/ICU.0000000000000618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kalezic T, Mazen M, Kuklinski E, Asbell P. Herpetic eye disease study: Lessons learned. Curr Opin Ophthalmol. 2018;29:340–6. doi: 10.1097/ICU.0000000000000482. [DOI] [PubMed] [Google Scholar]