

Abstract
Introduction:
The quality of healthcare services can be determined by patient satisfaction as it affects the performance, sustainability, and durability of health services. This study aims to determine patients’ satisfaction with healthcare service providers and its determinants in the urban family physician program in Fars and Mazandaran provinces, Iran.
Methods:
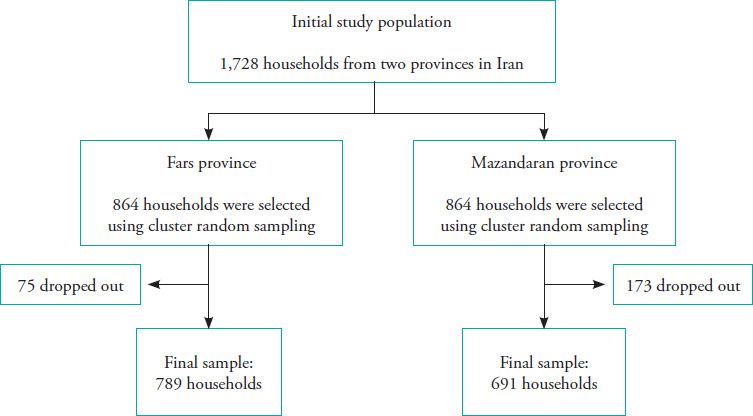
A cross-sectional study was conducted on the populations covered by the urban family physician program in Fars and Mazandaran provinces in 2016. In total, 864 households were selected in each province using random cluster sampling. Socio-demographic variables and underlying factors were gathered. Patient satisfaction levels were evaluated using a validated questionnaire.
Results:
Of the 1,480 participants with a mean age of 46.9 ± 14.2 years, 53.3% lived in Fars province and 74.2% were female. Furthermore, 67.9% of the patients were satisfied with their healthcare service providers. A higher satisfaction level was observed among the patients who resided in Fars province, lived in cities with <100,000 residents, walked <10 minutes to the family physician’s office, had a family physician they previously knew, accepted the family physician, had a positive attitude towards the importance of having a family physician and a referral system, and had adequate knowledge of the family physician program.
Conclusion:
The results indicated that two-thirds of the patients were satisfied with healthcare service providers. Several socio-demographic variables were associated with the patients’ satisfaction levels. Improving the family physician program by providing adequate medical equipment and monitoring physicians’ performance could increase patient satisfaction and improve the sustainability of the program.
Keywords: Satisfaction, Health Services, Family Physician, Iran
Introduction
Patient satisfaction plays an important role in the performance, sustainability, and durability of healthcare services, and determines the quality of healthcare services.1 Recent studies have emphasised that patient satisfaction is multifactorial. Lower patient satisfaction with healthcare providers leads to lower adherence to physician’s advice and treatment protocols and a lower rate of recovery from diseases. If they are dissatisfied, patients may change their physicians and healthcare centres.2
In Iran, health houses and health posts are the first levels of the healthcare system in rural and urban areas, respectively. Several health houses are under the supervision of a rural health centre, which is managed by a general practitioner. Urban health centres also supervise health posts. General practitioners refer patients to specialists at the second level of the healthcare system.3 The family physician program was implemented in rural and urban areas with populations under 20,000 to augment the referral system.4 In 2012, the family physician program was subsequently implemented in urban areas with populations over 20,000 only in Fars and Mazandaran provinces.5
Studies conducted in Iran have reported different levels of satisfaction among healthcare recipients. A study in Sabzevar indicated that 55.7% of patients were satisfied with their family physicians.6 Another study conducted on 11,200 patients covered by rural insurance in 32 provinces in Iran showed that the mean scores of satisfaction with family physicians and midwives were 70.1 (out of 85) and 33.5 (out of 40), respectively. They also reported that the overall score of satisfaction with healthcare services was 12.6 (out of 15).7 The higher level of satisfaction among the population covered by insurance was accompanied by an increased willingness to receive therapeutic and preventive services, lower motivation to access the second level of healthcare services without being referred by a family physician, and unwillingness to change one’s family physician.8 Therefore, assessment of patient satisfaction can reflect the quality of services and the success of the family physician program. The present study aimed to determine patients’ satisfaction with healthcare service providers and its determinants in the urban family physician program in Fars and Mazandaran provinces of Iran.
Methods
A cross-sectional study was conducted in Fars and Mazandaran provinces of Iran, where the urban family physician program was implemented. The study protocol was approved by the Ethics Committee of Babol University of Medical Sciences, Babol, Iran (IR.MUBABOL. REC.1397.032). The participants were provided with information about the study objectives and their verbal consent was obtained.
Using the sample size formula and considering p=0.9, a 95% confidence interval (CI), and an accuracy of 0.028, the sample size was estimated to be 864 households for each province. Sampling was conducted in the cities with populations >20,000 in Fars and Mazandaran provinces. Eligible households were recruited using the cluster random sampling method and through door-to-door visits. One person was selected from each household for interview. The inclusion criteria were age >15 years, being covered by the urban family physician program, and having received a visit by the family physician at least once during the past 3 months. Mentally disabled people and those who were unwilling to cooperate were excluded.
Data collection instruments
A door-to-door interview was conducted to gather the data using a data-gathering sheet and a questionnaire. Socio-demographic variables and underlying factors associated with the patients’ satisfaction with healthcare service providers were collected using the data-gathering sheet. This sheet included information about the residential area, sex, age, marital status, education level, occupation, supplemental health insurance, family size, distance to the family physician’s office on foot or by motor vehicle, number of visits, history of changing family physicians, choosing a previously known family physician, the family physician’s acceptance by the patient (regarding work experience, reputation, etc.), having the family physician’s phone number, patient’s attitude towards the importance of having a family physician, patient’s attitude towards the importance of a referral system (referral to level 2 of the referral system at the discretion of the family physician), and patient’s knowledge about the family physician program. Based on a Likert scale (‘strongly disagree’, ‘disagree’, ‘no opinion’, ‘agree’, and ‘strongly agree’), the patients’ attitudes were measured and categorised as ‘positive’ (‘very agree’ and ‘agree’) or ‘negative’ (‘very disagree’ and ‘disagree’). The patients’ knowledge about the family physician program was categorised into three levels: ‘low’ (<40%), ‘moderate’ (40-60%), and ‘high’ (≥60%). Accordingly, the ‘low’ and ‘moderate’ knowledge levels were considered inadequate, while the ‘high’ level was regarded as adequate.
Patients’ satisfaction with the healthcare service providers was assessed using a validated questionnaire completed through an interview. The questionnaire consisted of 11 questions scored from 0 to 5 based on a Likert scale (‘very low’, ‘low’, ‘moderate’, ‘high’, and ‘very high’) (Table 1). The patients were categorised as either ‘satisfied’ (score ≥3.5) or ‘dissatisfied’ (score <3.5). The total score of the patients’ satisfaction with the services provided by healthcare providers was estimated as the mean of the scores of the 11 questions. The validity of the questionnaire was verified by a panel of experts from Iranian health insurance organisations, urban family physicians, and health experts; its reliability was confirmed with a Cronbach’s alpha coefficient of 0.91.
Table 1. The levels of patients’ satisfaction with health service providers from the urban family physician program in Fars and Mazandaran provinces.
|
|
Total score |
Satisfaction level |
||
|---|---|---|---|---|
|
|
Very low and low |
Moderate |
High and very high |
|
|
Satisfaction with | ||||
|
Family physicians’ behaviours and communication skills |
4.02 ± 0.90 |
71 (4.9) |
294 (19.9) |
1114 (75.3) |
|
Healthcare workers’ behaviours and communication skills* |
3.95 ± 0.86 |
31 (3.7) |
198 (23.6) |
610 (72.7) |
|
Cleanliness and tidiness of the healthcare centre/office |
3.80 ± 0.79† |
62 (4.2)‡ |
401 (27.1) |
1015 (68.7) |
|
Timely attendance of the family physician at the healthcare centre/office |
3.80 ± 0.88 |
101 (6.8) |
336 (22.7) |
1042 (70.5) |
|
Health promotion education and recommendation by healthcare workers* |
3.79 ± 0.95 |
53 (6.4) |
238 (29.0) |
531 (64.6) |
|
Job discipline of healthcare workers and duration of their attendance at the healthcare centre/office* |
3.77 ± 0.81 |
43 (4.7) |
252 (27.3) |
627 (68.0) |
|
The knowledge and skill of the family physician in disease diagnosis and treatment |
3.73 ± 0.93 |
106 (7.2) |
436 (29.7) |
925 (63.1) |
|
Waiting time to receive healthcare services at the healthcare centre/office |
3.68 ± 0.87 |
123 (8.3) |
385 (26.0) |
970 (65.6) |
|
The effectiveness of the medications or treatment outcomes |
3.61 ± 0.92 |
134 (9.2) |
454 (31.1) |
872 (59.7) |
|
Health promotion education and recommendation by family physicians |
3.58 ± 1.06 |
198 (13.4) |
398 (27.0) |
878 (59.6) |
|
Medical equipment in the healthcare centre/office |
3.50 ± 0.84 |
131 (9.0) |
555 (38.0) |
774 (53.0) |
Data are presented as mean ± SD.
Data are presented as N (%). Satisfaction was scored based on a Likert scale ranging from 0 to 5.
Only households with pregnant women and/or children under 6 years old used these services and answered these questions. The satisfaction level was considered 3.5 (≥3.5 = satisfied; <3.5 = dissatisfied).
Statistical analysis
The data were analysed using SPSS 22.0 software for Windows (IBM Corp., Armonk, NY, USA). Numerical and categorical variables are expressed as mean ± SD and number (%), respectively. A chi-square test was used to determine the differences between the satisfied and dissatisfied groups regarding the demographic variables and the underlying factors associated with patient satisfaction. Backward stepwise logistic regression analysis was used to assess the relationship between the underlying factors and patient satisfaction. The significance level was set at p<0.05.
Results
This study was conducted on 1,480 patients with a mean age of 46.9 ± 14.2 years (Figure 1). Among the patients, 67.9% were satisfied and 32.1% were dissatisfied with the provided healthcare services. The mean score of satisfaction in the overall population was 3.74 ± 0.7. The patients’ levels of satisfaction with healthcare providers in the urban family physician program in Fars and Mazandaran provinces are presented in Table 1. The patients were more satisfied with their doctors’ behaviour and communication skills and less satisfied with the medical equipment in healthcare centres and offices.
Figure 1. Flowchart of the study participants.
The relationship between patient satisfaction and socio-demographic and underlying factors is shown in Table 2. The determinants of patient satisfaction identified via logistic regression analysis are listed in Table 3. According to the findings, satisfaction with healthcare service providers was higher among the patients who resided in cities with a population <100,000 compared with patients living in cities with a population >100,000 (OR=1.38, 95% CI: 0.95–2.00). Satisfaction was higher among patients who resided in Fars province compared with those living in Mazandaran province (OR=1.95, 95% CI: 1.39–2.74), and among the patients who walked less than 10 minutes to the family physician’s office (OR=1.50, 95% CI: 1.08–2.07). Patient satisfaction was also associated with choosing a previously known family physician (OR=1.73, 95% CI: 1.24–2.41), complete acceptance of the family physician (OR=2.93, 95% CI: 2.09–4.11), positive attitude towards the importance of having a family physician (OR=2.49, 95% CI: 1.65–3.77), positive attitude towards having a referral system (OR=1.60, 95% CI: 1.09–2.36), and having adequate knowledge about the family physician program (OR=1.51, 95% CI: 1.06–2.15).
Table 2. Distribution of the socio-demographic variables and underlying factors according to satisfaction status.
|
|
|
Satisfied patients |
Dissatisfied patients |
p-value |
|---|---|---|---|---|
|
Province of residence |
Fars |
571 (72.4) |
218 (26.6) |
<0.001 |
|
Mazandaran |
434 (62.8) |
257 (37.2) |
||
|
Residence in a city with a university of medical sciences |
Yes |
550 (67.9) |
260 (32.1) |
1.00 |
|
No |
455 (67.9) |
215 (32.1) |
||
|
Population of the city of residence |
≤100,000 |
313 (72.0) |
122 (28.0) |
0.03 |
|
>100,000 |
692 (66.2) |
353 (33.8) |
||
|
Sex |
Male |
244 (71.8) |
96 (28.2) |
0.45 |
|
Female |
678 (69.5) |
298 (30.5) |
||
|
Age (years) |
15-50 |
526 (68.9) |
237 (31.1) |
0.27 |
|
>50 |
385 (71.8) |
151 (28.2) |
||
|
Marital status |
Single |
124 (69.7) |
54 (30.3) |
0.86 |
|
Married |
791 (70.3) |
334 (29.7) |
||
|
Education level |
Illiterate to high school |
480 (72.1) |
186 (27.9) |
0.08 |
|
Diploma or higher |
424 (67.5) |
204 (32.5) |
||
|
Occupation |
Employed |
172 (68.0) |
81 (32.0) |
0.44 |
|
Homemaker, retired, or unemployed |
739 (70.4) |
310 (29.6) |
||
|
Having supplemental health insurance |
Yes |
397 (69.0) |
178 (31.0) |
0.46 |
|
No |
608 (67.2) |
297 (32.8) |
||
|
Family size |
1-3 |
587 (66.8) |
292 (33.2) |
0.26 |
|
4-7 |
418 (69.7) |
182 (30.3) |
||
|
Distance to family physician’s office on foot |
≤10 min |
513 (70.6) |
214 (29.4) |
0.04 |
|
>10 min |
422 (65.5) |
222 (34.5) |
||
|
Distance to family physician’s office by motor vehicle |
≤5 min |
574 (72.5) |
218 (27.5) |
0.01 |
|
>5 min |
206 (64.6) |
113 (35.4) |
||
|
Number of visits |
Less than twice a year |
261 (67.4) |
126 (32.6) |
0.16 |
|
More than twice a year |
635 (71.5) |
253 (28.5) |
||
|
Prior history of changing the family physician |
Yes |
290 (64.9) |
157 (35.1) |
0.10 |
|
No |
715 (69.3) |
317 (30.7) |
||
|
Choosing a previously known family physician |
Yes |
676 (75.4) |
220 (24.6) |
<0.001 |
|
No |
328 (56.4) |
254 (43.6) |
||
|
Family physician’s acceptance by the patients (regarding work experience, reputation, etc.) |
Completely acceptable |
753 (78.6) |
205 (21.4) |
<0.001 |
|
Relatively acceptable |
250 (48.2) |
269 (51.8) |
||
|
Having the family physicians phone number |
Yes |
338 (74.3) |
117 (25.7) |
<0.001 |
|
No |
660 (65.2) |
352 (34.8) |
||
|
Patient’s attitude towards the importance of having a family physician |
Positive |
771 (74.5) |
264 (25.5) |
<0.001 |
|
Negative |
162 (47.5) |
179 (52.5) |
||
|
Patient’s attitude towards the importance of a referral system (referring to level 2 of the referral system at the discretion of the family physician) |
Positive |
604 (75.1) |
200 (24.9) |
<0.001 |
|
Negative |
290 (54.8) |
239 (45.2) |
||
|
Patient’s knowledge of the family physician program |
Adequate (>60%) |
346 (73.5) |
125 (26.5) |
0.002 |
|
Inadequate (<60%) |
659 (65.3) |
350 (34.7) |
Table 3. Backward stepwise logistic regression analysis of the relationship between patient satisfaction and socio-demographic and underlying factors of the patients covered by the urban family physician program in Fars and Mazandaran provinces.
|
|
Satisfaction status (satisfied/dissatisfied) |
|
|---|---|---|
|
|
OR |
95% Confidence Interval |
|
Province of residence Fars Mazandaran (Ref) |
1.95
|
1.39-2.74
|
|
Population of the city of residence <100,000 >100,000 (Ref) |
1.38
|
0.95-2.00
|
|
Distance to the family physician’s office on foot ≤10 min >10 min (Ref) |
1.50
|
1.08-2.07
|
|
Choosing a previously known family physician Yes No (Ref) |
1.73
|
1.24-2.41
|
|
Family physician’s acceptance by the patients (regarding work experience, reputation, etc.) Completely acceptable Relatively acceptable (Ref) |
2.93
|
2.09—4.11
|
|
Patient’s attitude towards the importance of having a family physician Positive Negative (Ref) |
2.49
|
1.65-3.77
|
|
Patient’s attitude towards the importance of a referral system (referring to level 2 of the referral system at the discretion of the family physician) Positive Negative (Ref) |
1.60
|
1.09-2.36
|
|
Patient’s knowledge of the family physician program Adequate Inadequate (Ref) |
1.51
|
1.06-2.15
|
Ref, Reference category
Discussion
The findings revealed that two-thirds of the patients were satisfied with their healthcare service providers. The patients were most satisfied with the doctors’ behaviour and communication skills, and least satisfied with the medical equipment in healthcare centres and offices. Patient satisfaction was affected by factors such as residence in Fars province, residence in less populated cities, and walking less than 10 minutes to the family physician’s office. In addition, the determinants of patient satisfaction included choosing a previously known family physician, acceptance of the family physician, positive attitude towards the importance of having a family physician and a referral system, and having adequate knowledge of the family physician program. Previous studies consistently revealed a high level of satisfaction in this area. For example, Ashrafian Amiri et al. conducted a study on 955 patients covered by rural insurance and reported that the mean scores of satisfaction with health houses and health centres were 4.5 ± 0.5 and 4.0 ± 0.7 (out of 5), respectively.9 Similarly, Ebrahimipour et al. reported that 80% of patients were satisfied with the services provided by the rural family physician program.10 In another study, the satisfaction with healthcare services provided by a family physician program was at a desirable or relatively desirable level.11 The higher level of satisfaction in rural areas might be attributed to the economic, social, and cultural factors of healthcare service recipients.12,13 High-quality services might also lead to higher satisfaction levels; the World Health Organization (WHO) reported that 85.7% of the patients in Canada were satisfied with their healthcare services.14
The results indicated that choosing previously known family physicians, accepting them, having a positive attitude towards the importance of having a family physician, referral to level two of the referral system at the discretion of the family physician, and having adequate knowledge about the family physician program affected patient satisfaction with healthcare services. It has also been hypothesised that satisfaction with healthcare providers could enhance the utilisation of healthcare services due to the fulfilment of patients’ expectations.15,16 These findings represent the necessity of culturalisation prior to the implementation of a family physician program.
The results revealed a marginally significant inverse association between the population of the residential area and patient satisfaction. The higher satisfaction levels observed in smaller populations, such as individuals living in rural areas, might be associated with economic, social, and cultural factors influencing the service recipients. In the present study, the patients were most satisfied with the behaviours and communication skills of the family physicians and healthcare workers. These results were in accordance with those of another study conducted in Iran.17 Generally, patient satisfaction is associated with healthcare workers’ behaviour, appropriate diagnosis of the disease by physicians, and being provided with information about health issues. Polite and proper behaviour not only satisfies patients at each stage of treatment and follow-up, but also encourages them to recommend other patients, relatives, and acquaintances to use such healthcare services.18,19 The patients in this study were least satisfied with the equipment at the healthcare centres and offices, which was similar to the results of another study carried out by Taheri et al.17 Regarding the importance of developing a referral system from the first level, Palmer et al. stated that satisfied patients would not bypass the system.20 Therefore, a healthcare centre should have sufficient personnel and should be well-equipped.
One of the limitations of the present study was the unequal cooperation on the part of males and females. Moreover, because this study was conducted in Fars and Mazandaran provinces, the results cannot be generalised to the whole country. Furthermore, a cause-and-effect relationships could not be determined due to the cross-sectional nature of the research.
In conclusion, two-thirds of the patients were satisfied with healthcare service providers. The lowest satisfaction was with the equipment in healthcare centres, while the patients were most satisfied with the family physicians’ behaviour and communication skills. Culturalisation within the community towards the importance of a referral system in the family physician program, providing adequate medical equipment in all healthcare centres, providing the patients with the opportunity to choose their family physician, and monitoring and evaluating the provided healthcare services periodically in larger cities can enhance the quality of the services and patient satisfaction. Furthermore, conducting training courses or workshops may augment the scientific skills of family physicians. Finally, utilisation of the appropriate guidelines by family physicians to diagnose and treat diseases can be effective in increasing the quality and effectiveness of healthcare services.
Acknowledgments
This study was financially supported by the Health Insurance Organization of Iran, Tehran, I.R. Iran. The authors are grateful to the health vice-chancellors of Babol, Fasa, Jahrom, Larestan, Mazandaran, and Shiraz Universities of Medical Sciences for their cooperation. They also appreciate all the households who participated in the study. Thanks are also extended to Ms. A. Keivanshekouh at the Research Consultation Center (RCC) of Shiraz University of Medical Sciences for improving the use of English in the manuscript.
Conflicts of Interest
The authors have no conflict of interests to declare.
How does this paper make a diffrence in general practice?
Two-thirds of the patients were satisfied with healthcare service providers.
The lowest satisfaction was with the equipment in healthcare centres.
The patients were most satisfied with the family physicians’ behaviour and communication skills.
References
- 1.Karavida A, Stamouli M-A, Balis C, editors. Patients' satisfaction evaluation with the health center of Elis province. ICIMTH. 2014 doi: 10.3233/978-1-61499-423-7-283. [DOI] [PubMed] [Google Scholar]
- 2.Rao JK, Weinberger M, Kroenke K. Visit-specific expectations and patient-centered outcomes: a literature review. Arch Fam Med. 2000;9(10):1148. doi: 10.1001/archfami.9.10.1148. [DOI] [PubMed] [Google Scholar]
- 3.Iran Ministry of Health and Medical Education. Reform Structure of Ministry of Health and Medical Education. 1st ed. Tehran: Ministry of Health and Medical Education; 1999. pp. 4–17. [in Persian] [Google Scholar]
- 4.Iran Ministry of Health and Medical Education. Family Physician Instruction Version 9. Iran: Ministry of Health and Medical Education; 2009. pp. 4–102. [in Persian] [Google Scholar]
- 5.Iran Ministry of Health and Medical Education. Family Physician and Referral System Instruction in Urban Version 2. Iran: Ministry of Health and Medical Education; 2012. p. 22. [in Persian] [Google Scholar]
- 6.Ghorbani A, Raeissi P, Saffari E, Reissi N. Patient satisfaction with the family physician program in Sabzevar, Iran. Global J Health Sci. 2016;8(2):219. doi: 10.5539/gjhs.v8n2p219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Maftoon F, Aeenparast A, Montazeri A, et al. Midwives' satisfaction in family physician and referral system: a national study. Payesh. 2015;14(3):343–9. http://payeshjournal.ir/article-l-237-en.html URL: [Google Scholar]
- 8.Nasrollahpour Shirvani KM, Ashrafian Amiri H, Rabiee SM, Keshavarzi A, Kourosh F. Experience of Implementation of Urban Family Physician Program in Iran. Tehran: Health Insurance Organization of Iran; 2017. [Google Scholar]
- 9.Ashrafian Amiri H, Mikaniki E, Nasrollahpour Shirvani S, et al. Satisfaction of patients with rural insurance in terms of the first and second levels of health services presentation in Northern Provinces of Iran. J Guilan Univ Med Sci. 2014;23(90):14–23. http://journal.gums.ac.ir/article-1-630-en.html URL. [Google Scholar]
- 10.Ebrahimipour H, Vejdani M, Vafaee-Najar A, Nejatzadegan Z, Amini A, Vejdani M. Patients satisfaction from family physicians in health centers affiliated with Sabzevar University of Medical Sciences with EUROPEP-2012. Tolooe Behdasht. 2015;13(6):25–34. http://tbj.ssu.ac.ir/article-1-1371-en.html URL: [Google Scholar]
- 11.Nasrollahpour Shirvani S, Kabir M, Touran S, Shabestani Mounfared A. Satisfaction in service recipients of health centers with family physician program in Northern Provinces of Iran: 2008. JRafsanjan Nurs Midwifery Fac. 2009;3(4):1–10. [Google Scholar]
- 12.Ghasemi M, Hadian M, Sotoudeh Gagasari H, Malaki Moghadam H. Evaluating satisfaction among recipients of family physician services in Birjand and Khusf, Iran. Mod Care J. 2018;15(1) https://www.sid.ir/en/journal/ViewPaper.aspx?id=658454 URL: [Google Scholar]
- 13.Omorogbe CE. Socio-economic factors influencing in-patient satisfaction with health care at the university of Benin Teaching Hospital (UBTH), Benin City, Nigeria. IJNMH. 2017;3(4):1–17. [Google Scholar]
- 14.Statistics Canada. Patient Satisfaction with Any Health Care Services Received in Past 12 Months, by Age Group and Sex, Household Population Aged 15 and Over, Canadian Community Health Survey Cycle 1.1, Canada, Provinces and Territories. Canada: Statistics Canada; 2008. [Google Scholar]
- 15.Gilbert GR. Measuring internal customer satisfaction. Manag Serv Qual. 2000;10(3):178–86. [Google Scholar]
- 16.Kravitz RL, Cope DW, Bhrany V, Leake B. Internal medicine patients’ expectations for care during office visits. J Gen Intern Med. 1994;9(2):75–81. doi: 10.1007/BF02600205. [DOI] [PubMed] [Google Scholar]
- 17.Taheri M, Mohammadi M, Amani A, Zahiri R, Mohammadbeigi A. Family physician program in Iran, patients’ satisfaction in a multicenter study. PJBS. 2014;17(2):227–33. doi: 10.3923/pjbs.2014.227.233. [DOI] [PubMed] [Google Scholar]
- 18.Liang W, Burnett CB, Rowland JH, et al. Communication between physicians and older women with localized breast cancer: implications for treatment and patient satisfaction. J Clin Oncol. 2002;20(4):1008–16. doi: 10.1200/JC0.2002.20.4.1008. [DOI] [PubMed] [Google Scholar]
- 19.Butow P Dowsett S, Hagerty R, Tattersall M. Communicating prognosis to patients with metastatic disease: what do they really want to know? Support Care Cancer. 2002;10(2):161–8. doi: 10.1007/s005200100290. [DOI] [PubMed] [Google Scholar]
- 20.Palmer, Philip ES. Feeling unwell: must you go straight to hospital? / P. E. S. Palmer. 1. Vol. 12. World health forum; 1991. pp. 38–42.https://apps.who.int/iris/handle/10665/49178 [PubMed] [Google Scholar]