

Abstract
Introduction:
With an increasing life expectancy and proportion of older adults, the number of people in need of care services is also increasing. This study aimed to determine and describe various available care services for older persons reported in literature.
Methods:
English-language articles published between the years of 1990 and 2018 in Scopus, ProQuest, PubMed, and Google Scholar databases or search engines were reviewed. The search resulted in 46,927 articles. All selected studies were systematically evaluated and screened based on title, abstract, and full text related to the study’s objective. Finally, 246 articles were included in the study. The care services in older persons care systems were identified from the selected articles and were presented in extraction tables. Final conclusions were made based on the types of services provided and their frequency of citation.
Results:
The research results showed that numerous systems exist to provide care services for older adults, including long-term care services, home care services, housing for the aged, day care centres, senior centres, nursing homes, and hospice care services. Regarding older adults’ care needs and the objectives and missions of each care system, different care services, such as personal care, social support services, medical care services, and nutrition services, have been identified in the service packages.
Conclusion:
This study describes the diverse care services available for older persons that have been reported in the literature. Further research in different healthcare systems is required regarding what is most essential and lacking in each setting.
Keywords: Older persons care, Service package, Health system
Introduction
The phenomenon of ageing is presently expanding, and the older populations of the world will increase to an expected two billion people by 2050.1 Currently, Iran is also experiencing a demographic transition, while the population aged 60 years and above has increased from 7.2% in 2006 to 8.2% in 20112; furthermore, it is anticipated that the older population of Iran will increase from 11 million in 2025 to 30 million in 2050.3 Whereas the growth of the global ageing population is greater in developing countries than in developed countries, these countries, including Iran, have fewer opportunities to confront old age and its consequences.4
The cumulative effects of physiological changes during ageing are accompanied by an increase in chronic disorders, diabetes, cardiovascular disease, cancer, osteoporosis, chronic obstructive pulmonary disease, depression, and dementia; with advancing age, the likelihood of developing comorbidities also increases.5 The prevalence of disability due to chronic disease is greater among older adults than other age groups, and with the growing older population, the number of dependent older persons who are in need of regular and continuous care services will increase. Furthermore, an increase in the oldest elderly population is accompanied by an increase in disabilities and a rising demand for long-term care services.6 Limitations in resources, reduced income, financial dependency, physical handicaps, social isolation, mental health disorders, including dementia and depression, result in greater vulnerability in these older individuals.7
Countries across the world are burdened with the high costs associated with increasing elderly populations and higher incidence of chronic disease.8 For example, the highest healthcare costs in low- and middle-income countries are related to heart disease, stroke, visual disorders, loss of hearing, and dementia.9 If individuals remain healthy and independent in their old age and without certain impairments, an increase in the older population will not become a social burden; however, if they do not receive the necessary services and support from community, social security systems, and healthcare systems, higher costs will be imposed on families, and providing care for older people will create limitations for family members to participate in social and educational activities and reduce access to job opportunities.10 Therefore, various care systems have been developed worldwide with the aim of reducing the negative consequences of ageing and enhancing the health and welfare status of older persons.10 Various studies indicated that, in less developed countries, the current healthcare systems that provide older adult care services have been inadequately and inefficiently designed.3
Regarding the growing burden of chronic disorders in later life and to ensure productive ageing, comprehensive healthcare and longterm care (LTC) services appropriate to the needs of the older persons should be provided; these services should be readily available and should result in a reduction in the detrimental effects of disease and enhancement of personal health and quality of life.10 Preventive policies, enhancing healthcare, and immediate treatment of older adults are of great significance.3 To achieve these goals, providing and developing comprehensive and targeted plans based on scientific findings is essential.11
According to a review of the literature, there have been no studies thus far that have evaluated the service packages of various care systems. In addition to identifying the highest priority services in each package, studies in which the relationships between the features of each care system and service recipients were specified were not carried out. This study was designed and implemented with the aim of identifying various older persons care services and their defined service packages and determining the highest priority services and the mission of each care service.
Methods
This study is a scoping review in which the keywords used were determined based on pilot studies and utilizing a MeSH system. In order to gain access to articles from a search of related studies in databases, keywords with different combinations of (elderly OR aging OR older OR aged OR senior) AND (care OR service) AND (long term care, nursing home, hospice care, extra care housing, sheltered housing, home care, respite care, assisted living, residential facilities, retirement housing, supportive service, senior centre, day care, health services, housing, administration, organization, characteristics, structure, standard) were used. English-language articles published between the years of 1990 and 2018 in Scopus, ProQuest, PubMed, and Google Scholar databases or search engines were reviewed. In addition, the grey literature—which refers to articles that were either unpublished or were published in non-commercial forms (including reports, policy statements, working papers, issues paper, government documents, etc.)— was reviewed. This literature was founded and reviewed from a 'grey literature database' and related governmental or non-governmental departments and agencies that focused on care for older persons.
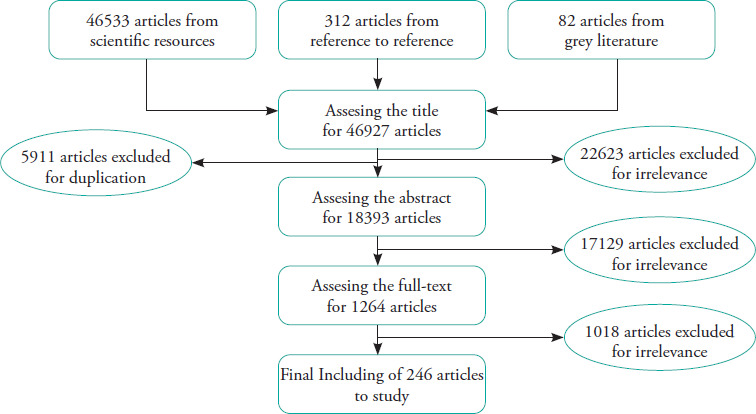
In this review, key studies cited in other articles that were related to the aim of the current research were also included. The result of this search was access to 46,927 articles. All studies were systematically analysed based on the relevance of the title, abstract, and full text to the research objectives. Finally, 246 articles were included in this study (Figure 1).
Figure 1. Systematic review approach for searched articles.
The services provided by each older persons care service were divided into main categories. These categories, which referred to the main care systems’ ability to provide delivery of services to older persons, were determined by primary (pilot) search or review. The main categories included personal care, nursing and medical services, social support services, rehabilitation services, and education. In cases where the required services were provided in the articles, they were ranked based on the star system, and the frequency of each service category was separately calculated and arranged in the final table based on the total frequency, in decreasing order. The final conclusions were made based on the types of services provided and their frequencies. The study received ethical permission from the Ethics Committee of Tabriz University of Medical Sciences (IR. TBZMED.REC.1393.250).
Results
Seven main systems of services provided were noted in this review: housing for the aged, home care (HC), LTC, day care centre (DCC), senior centre (SC), nursing home (NH), and hospice care services (HCS). Secondary systems were also referred to by other names, which could be situated in other systems depending on their features and could not be considered separate and independent systems, e.g., supportive services, assisted living, sheltered housing, extra care housing, and housing for the aged; all secondary systems focused on providing housing units for older persons and were categorised as ‘housing for the aged’. Of the 246 articles included in this review, 70 were related to LTC services, 43 to HC, 68 to housing for the aged, 17 to DCC, 15 to SC, 11 to NH, and 27 to HCS. Overall, there were three studies common to both LTC and HC and one study common to LTC and DCC, SC, and housing for the aged. Most of the articles included in the review were published between 2000 and 2015 (86%). Over 50% (136) of the articles were related to the USA, over 8% were related to the UK, 7.3% were related to Japan, 5.6% were related to China and Canada (2.8% each), 2.4% were related to Australia, and 10% were related to Germany, Israel, Taiwan, Turkey, and Korea. The remaining articles were related to countries such as Sweden, France, the Netherlands, Spain, Ukraine, South Korea, Finland, Norway, Malaysia, Slovakia, Lithuania, Singapore, and the World Health Organization (WHO). More than 94% of the included articles were original work, 3% were review articles, and 4% were related to reports or documents extracted from grey literature.
Long-Term Care
LTC represents a wide range of community-based services and programmes provided in healthcare centres, homes, day care centres, or institutions; the services maintain and enhance physical performance, individual independence, and quality of life. LTC also includes informal assistance by family members and friends in caring for older persons.12
Based on the results obtained from the current study, LTC services included three categories: non-medical services, health-related services, and support services. Non-medical services in LTC included personal care (helping people with activities of daily living [ADL] and instrumental activities of Daily living [IADL]), housekeeping, nutrition services (delivering meals to the home, nutritional consultation, and providing nutritional diets), environment modification (creating a wheelchair ramp, installing auxiliary equipment, and home safety), transportation services, home maintenance, supervision services (full-time supervision by staff, night-time supervision, and relief bells).
Health-related services included medical care (advanced health treatment at home and during daily visits, referral, podiatry, and caring for people diagnosed with dementia), nursing care (periodic evaluation, skilled care services, medication administration, injections, wound dressing, referral, and case management), rehabilitation services (physiotherapy, speech therapy, occupational therapy, visual care services and audiology, and providing rehabilitation equipment), preventive services (screening programmes for illnesses such as depression, periodic assessment), education and consultation services, and other medical care services (hospital services, radiology, laboratory, and oral health services).
Social support services included recreational and entertainment activities, sports programmes, intergenerational programmes, respite care, financial support to caregivers and group homes for older persons (Table 1).
Table 1. Services covered by LTC, based on the literature review.
|
Included articles |
Personal Care |
Nursing care |
Medical care |
Social services |
Homemaker services |
Rehabilitation services |
Nutrition services |
Transportation |
Home modifications |
Education & counselling |
Hospice & palliative care |
Other medical services |
Supervision |
Psychological services |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
General Accounting Office, US |
† |
† |
† |
† |
† |
|
† |
† |
† |
|
|
|
† |
|
|
Pan, S-M |
† |
|
† |
† |
|
† |
|
|
|
|
|
† |
|
|
|
Ikegami, et al |
† |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
|
|
Doyle A, et al |
† |
|
† |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
|
Kane, et al |
† |
|
† |
|
† |
|
|
|
|
|
|
|
|
|
|
Ross MET, et al |
† |
† |
† |
† |
† |
|
† |
† |
|
|
|
† |
|
|
|
Hansen, et al |
|
† |
|
† |
|
† |
† |
† |
|
|
|
|
|
|
|
Rich ML |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
|
|
|
|
|
Pacolet, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
† |
|
|
|
|
Cuellar, et al |
† |
† |
† |
† |
† |
|
|
† |
|
|
|
|
|
|
|
Feder, et al |
† |
† |
† |
|
|
|
|
|
|
|
|
|
|
|
|
Kodner, et al |
† |
† |
† |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
Lutzky, et al |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
|
WHO |
† |
† |
† |
† |
† |
† |
|
|
† |
† |
|
|
|
|
|
Geraedts, et al |
† |
|
† |
† |
|
|
|
|
† |
† |
|
|
|
|
|
Brodsky, et al |
† |
† |
|
† |
† |
† |
† |
|
† |
|
† |
|
† |
|
|
LeBlanc, et al |
† |
|
† |
† |
† |
|
|
† |
|
|
|
|
|
|
|
Matsuda S, et al |
|
† |
† |
† |
|
† |
|
|
|
|
|
|
|
|
|
Miller, et al |
† |
† |
† |
|
† |
|
|
|
|
|
|
|
|
|
|
Borowski, et al |
† |
|
† |
|
† |
|
|
† |
|
|
|
|
|
|
|
Matsuda S |
|
† |
† |
† |
|
† |
|
|
|
|
|
|
|
|
|
Kwong EW-Y, et al |
† |
† |
† |
† |
|
† |
† |
|
|
|
† |
|
|
† |
|
Chan P, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
† |
|
|
|
|
United States General Accounting Office |
† |
|
† |
† |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
Chiu H-C |
† |
† |
† |
† |
† |
|
† |
† |
|
† |
|
† |
|
|
|
Mui AC |
† |
|
† |
† |
† |
|
† |
† |
|
|
|
† |
|
|
|
Wiener, et al |
† |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Webb P |
† |
† |
† |
† |
|
† |
|
|
|
† |
|
|
|
|
|
Murashima, et al |
† |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
|
|
Comas-Herrera, et al |
† |
† |
† |
|
† |
|
|
|
|
|
|
|
|
|
|
Brodsky, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
† |
|
Palley HA, et al |
† |
|
† |
† |
† |
|
† |
|
† |
|
|
|
|
|
|
Chen Y-M |
† |
† |
† |
|
† |
† |
† |
† |
† |
|
† |
|
|
|
|
Campbell, et al |
† |
† |
|
|
|
† |
|
|
† |
|
|
|
|
|
|
Mitchell, et al |
† |
† |
† |
|
|
† |
|
|
† |
|
|
|
|
|
|
Morris, et al |
† |
|
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
Hansen, et al |
|
† |
† |
|
|
|
|
† |
|
|
|
|
|
|
|
Costa-Font, et al |
† |
|
|
† |
† |
|
|
† |
|
|
|
|
|
|
|
Huber, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
|
|
Wu, et al |
† |
|
|
† |
† |
|
† |
† |
† |
|
|
|
|
† |
|
Gelfand DE |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
† |
|
|
Houde, et al |
† |
† |
† |
|
|
† |
|
|
† |
|
|
|
|
|
|
Tsutsui T, et al |
† |
† |
† |
|
† |
† |
|
|
† |
|
|
|
|
|
|
Hansen JC |
|
† |
† |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
|
Lezovic M |
† |
† |
† |
† |
|
† |
|
† |
† |
|
|
|
|
|
|
Heinicke, et al |
† |
|
|
† |
† |
|
† |
† |
|
|
|
|
|
|
|
Marcinkowska I |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
|
|
|
Schulz, et al |
† |
† |
|
|
† |
† |
|
|
|
|
|
|
|
|
|
Rothgang H |
† |
† |
|
† |
† |
|
|
|
|
|
|
|
|
|
|
Kassner, et al |
|
† |
|
|
† |
† |
† |
|
|
|
|
|
† |
|
|
Lehning AJ, et al |
|
† |
|
† |
|
|
† |
† |
|
|
|
|
|
|
|
Kendig, et al |
† |
† |
† |
† |
† |
|
|
† |
† |
|
|
|
|
|
|
Guo KL, et al |
† |
† |
† |
† |
† |
† |
† |
|
|
† |
† |
|
|
|
|
Franklin K |
† |
† |
† |
|
|
† |
|
|
|
|
† |
|
|
|
|
Yong V, et al |
† |
† |
† |
† |
|
† |
|
|
|
† |
|
|
|
|
|
Iecovich E |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
|
|
|
Olivares-Tirado P, et al |
† |
† |
† |
|
|
† |
|
|
|
† |
|
|
|
|
|
Harris-Kojetin, et al |
† |
† |
† |
† |
|
† |
|
|
|
|
† |
|
|
† |
|
Applebaum R, et al |
† |
† |
|
† |
† |
|
† |
|
† |
† |
|
|
|
|
|
Lee HS, et al |
† |
† |
† |
† |
|
† |
† |
|
|
|
|
|
|
|
|
Igarashi A, et al |
† |
† |
|
† |
|
† |
|
|
|
|
|
|
|
|
|
Olivares-Tirado, et al |
|
† |
† |
|
|
† |
|
|
† |
|
|
|
|
|
|
Wysocki A, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
Harris-Kojetin, et al |
† |
† |
† |
|
|
† |
|
|
|
|
† |
|
|
† |
|
Igarashi A, et al |
† |
† |
|
|
|
† |
|
|
|
|
|
|
|
|
|
Yang W, et al |
† |
† |
|
|
|
|
† |
|
|
|
|
|
|
|
|
Chin CW, et al |
|
† |
† |
† |
|
|
|
|
|
|
† |
|
|
|
|
Gonzalez L, et al |
† |
† |
† |
† |
† |
† |
|
† |
|
|
|
|
|
† |
|
Graham WC, et al |
† |
† |
|
|
|
|
|
|
|
|
|
|
|
|
|
Kwak C, et al |
† |
† |
|
|
† |
|
† |
|
|
|
|
|
|
|
|
Frequency of reference to the type of service |
61 |
55 |
51 |
48 |
42 |
42 |
31 |
28 |
20 |
14 |
14 |
6 |
6 |
6 |
A review of the literature in this field indicated that personal care, nursing and medical services, social support services, and housekeeping were the most frequent services provided by LTC. Palliative care, supervision, and psychology services were less frequent in this system. Nevertheless, relative heterogeneity was observed across various service packages.
Home Care
As defined by the WHO, HC includes a set of healthcare and support services provided in homes that can represent a temporary replacement for LTC. These services prevent or delay the hospitalisation of individuals in nursing homes.13 The Services available in HC comprised nonmedical services, health-related services, and support services.
The non-medical services included personal care (helping older people with ADL and IADL), housekeeping, nutrition services (meal delivery at home, cooking and preparing meals), training classes, transportation, home modification, and home maintenance.
Health services included medical care (home health services, assessment of older adults, therapeutic care planning, providing medical equipment, acute care, and laboratory services), nursing care (setting doctor’s appointments, case management, medication administration, wound care, caring for patients with dementia, skilled nursing care, oxygen therapy, dialysis, tube feeding, and parenteral feeding), rehabilitation services (physiotherapy, occupational therapy, and providing rehabilitation equipment), psychology and consultation services, palliative care, and end of life care.
Social support services included family support services, friendly visits, recreational programmes, helping to establish social relationships, accommodations in group housing, providing a home for older adults, helping them find a job, and providing spiritual support (Table 2).
Table 2. Services covered by home care, based on the literature review.
|
Included articles |
Nursing care |
Personal Care |
Medical care |
Social services |
Homemaker services |
Rehabilitation services |
Nutrition services |
Education & counselling |
Transportation |
Palliative care |
Psychosocial services |
Home modifications |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Diwan S, et al |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
Buchanan RJ, et al |
† |
† |
† |
† |
† |
† |
† |
|
† |
|
† |
† |
|
Haupt BJ, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
Stuart M, et al |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
|
Stuart M, et al |
† |
† |
|
|
† |
† |
|
|
|
|
|
|
|
Bentur N |
|
† |
† |
|
|
|
|
† |
|
|
|
|
|
Wiener, et al |
† |
† |
† |
† |
|
|
|
|
|
|
|
|
|
Chan P, et al |
† |
† |
† |
† |
† |
† |
† |
|
† |
† |
|
|
|
Plumb AM |
|
† |
|
|
† |
|
† |
|
|
|
|
|
|
Kwong EW-Y, et al |
† |
† |
† |
† |
† |
|
|
|
|
|
|
† |
|
Wallace, et al |
|
† |
† |
† |
† |
|
|
|
|
|
|
|
|
Latif E |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
Perroca MG, et al |
† |
† |
† |
† |
|
† |
|
† |
|
† |
|
|
|
Albert SM, et al |
† |
† |
|
|
† |
|
† |
|
|
|
|
|
|
Mezey M, et al |
† |
|
† |
† |
|
|
|
|
† |
|
|
|
|
Venables D, et al |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
Stuart M, et al |
† |
† |
† |
† |
† |
† |
|
|
† |
|
|
|
|
Markle-Reid M, et al |
† |
† |
† |
|
† |
† |
|
|
|
|
|
|
|
Hansen JC |
† |
† |
† |
† |
† |
|
† |
|
† |
|
† |
|
|
Cruz M |
† |
† |
† |
† |
|
|
† |
|
|
|
† |
|
|
Darkins A, et al |
|
|
|
|
|
|
|
† |
|
|
|
|
|
Canadian Healthcare Association |
† |
† |
† |
† |
† |
† |
† |
|
† |
† |
|
† |
|
Forbes DA, et al |
† |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
|
Fuhrman MP |
† |
† |
† |
|
|
† |
|
† |
|
† |
|
|
|
Rabiee P, et al |
† |
† |
† |
† |
|
|
|
|
|
|
† |
|
|
Kmprnanpbcgnpbc D, et al |
|
|
† |
|
|
|
|
|
|
|
|
|
|
Crossen-Sills J, et al |
† |
|
|
|
|
|
|
† |
|
|
|
|
|
Chang H-T, et al |
† |
|
† |
|
|
|
|
|
|
|
|
|
|
Jones A, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
† |
|
O’Keeffe, et al |
|
† |
† |
† |
|
|
|
|
|
|
|
|
|
Bronowski P, et al |
† |
† |
† |
† |
|
|
|
† |
|
|
† |
|
|
Terrade O, et al |
|
|
† |
† |
|
† |
|
|
|
† |
† |
|
|
Sobis I |
|
† |
|
† |
|
|
† |
|
|
|
|
|
|
Otaga M |
† |
† |
|
|
|
|
|
|
|
|
|
|
|
Verulava T |
† |
|
† |
† |
|
|
|
|
|
|
|
|
|
Katahira N, et al |
† |
|
† |
|
|
|
|
† |
|
† |
|
|
|
Armstrong JJ, et al |
† |
† |
|
|
† |
† |
† |
|
|
|
|
|
|
Torun N, et al |
† |
|
† |
|
|
† |
|
† |
|
|
|
|
|
Fu YY, et al |
† |
† |
|
|
|
|
|
|
|
|
|
|
|
Gümüş R, et al |
† |
|
† |
† |
|
† |
† |
|
|
|
|
|
|
Kiersey RA, et al |
† |
† |
|
† |
|
|
† |
|
|
|
|
|
|
Holm SG, et al |
† |
† |
|
|
|
† |
|
|
|
|
|
|
|
Choi JK, et al |
† |
† |
† |
† |
|
|
|
|
|
|
|
|
|
Frequency of reference to the type of service |
35 |
33 |
32 |
27 |
19 |
1S |
15 |
11 |
9 |
7 |
6 |
4 |
A review of the previous studies indicated that nursing care, personal care, medical services, social support services, and housekeeping were all priority services provided in HC. The services of palliative care, mental healthcare, and home modification were of lesser significance. Nevertheless, relative heterogeneity was observed across various service packages.
Housing for the Aged
‘Housing for the aged’ is a broad term that includes all houses considered to be residences of older individuals. Extra-care housing (ECH), which is the common term in England, includes residential units in which special services are provided to support older persons with mental or physical disorders who require nursing services. Assisted living (AL), a term used in the United States, refers to complexes with a residential appearance designed as an environment far from regulations of institutions. Here, care and support services are provided to assist older people who need help in their daily activities, but do not require continuous care and nursing.14 The available services in housing for the aged included non-medical services, health-related services, and social support care.
Non-medical care in housing for the aged included personal care (assistance regarding ADL and IADL), nutrition services (general nutrition services and providing warm meals based on a menu), home maker services, ‘around-the-clock’ (i.e., 24-hour) supervision (including remote monitoring, on-site personnel, around-the-clock assistance), entertainment and group programmes (opportunities to take part in group activities such as playing games, having tea and lunch in groups, shopping inside or outside the complex, sports classes, swimming, or recreational activities), respite care, transportation services, and other services such as repair and maintenance (e.g., furniture, changing of light bulbs) and gardening.
Health-related services included preventive services (infection control, screening, vaccination, and environment modification), medical and nursing care services (visits by the physician, nurse, and other health personnel, intermediate care, medication administration, emergency services, ophthalmology services, supervision of health conditions, control of symptoms, pain management, emergency rescue, helping individuals with cognitive impairments and diabetes treatment, and management of chronic diseases), clinical nutrition services (nutrition education and prescribing a diet), psychological counselling, rehabilitation services (physiotherapy, occupational therapy, and speech therapy), palliative care (pain management and setting up advanced directives), and other healthcare (art therapy, music therapy, pet therapy, respiratory therapy, dance therapy, and chiropody).
Social support services included family support programmes, group and social activities, intergenerational programmes, transportation services, education classes, financial and legal counselling, and help with finding work (Table 3).
Table 3. Services covered by housing for the aged, based on the literature review.
|
Included articles |
Personal Care |
Nutrition services |
Social support |
Home maker services |
Medical care |
Nursing care |
Supervision |
Transportation |
Counselling |
Rehabilitation services |
Preventive care services |
Palliative care |
Other therapy |
Other services |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Just G, et al |
† |
|
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
Mollica, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
Hauser J, et al |
† |
† |
† |
† |
† |
|
|
† |
|
|
|
|
|
|
|
Hawes, et al |
† |
† |
|
† |
|
† |
† |
|
|
|
|
|
|
|
|
Mollica, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
|
|
|
|
Hawes, et al |
† |
† |
|
† |
|
† |
† |
† |
|
|
|
† |
|
|
|
Kraditor, et al |
† |
† |
† |
† |
|
† |
† |
† |
† |
† |
|
† |
|
|
|
Heumann, et al |
† |
† |
† |
† |
† |
|
|
† |
† |
|
|
|
|
|
|
Habell M |
† |
† |
† |
† |
† |
|
|
† |
† |
|
|
|
† |
† |
|
Mulvenna M, et al |
|
|
|
|
|
† |
|
|
† |
|
|
|
|
|
|
Kovner CT, et al |
† |
† |
† |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
Wilden R, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
Sloane PD, et al |
† |
† |
|
† |
† |
† |
|
|
|
|
|
† |
|
|
|
Kovner CT, et al |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
|
Mollica R |
|
|
† |
|
† |
|
|
† |
|
† |
|
|
|
|
|
Salmon JR, et al |
† |
† |
† |
† |
† |
|
|
|
|
† |
|
|
|
|
|
Hawes, et al |
† |
† |
|
† |
† |
† |
|
† |
|
|
|
|
|
|
|
Riseborough M, et al |
† |
|
† |
|
† |
|
|
|
|
† |
|
|
|
|
|
Wells, Lucy |
† |
|
|
† |
† |
|
|
|
|
† |
|
|
|
† |
|
Weisman GD, et al |
† |
|
† |
|
|
† |
|
|
|
|
|
|
|
|
|
Chao S, et al |
† |
† |
† |
|
† |
|
† |
|
|
|
|
|
|
|
|
Mitty EL |
† |
† |
† |
† |
|
† |
|
|
|
|
|
† |
|
|
|
Hawes C, et al |
† |
† |
|
† |
|
† |
† |
|
|
|
|
|
|
|
|
Reynold K |
† |
† |
|
† |
|
|
|
|
|
|
|
|
|
|
|
Wells L |
† |
† |
† |
|
† |
|
|
|
|
† |
|
|
† |
|
|
Care Services Improvement Partnership, UK |
† |
† |
|
|
† |
|
† |
|
|
† |
|
|
|
|
|
Wanless, et al |
|
† |
|
† |
† |
|
† |
|
|
|
|
|
|
|
|
Jones A |
† |
|
† |
† |
† |
|
|
|
|
† |
|
|
|
† |
|
Lee JH |
† |
† |
† |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
National Center for Assisted living |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
Wojgani H, et al |
† |
† |
|
† |
|
|
† |
|
† |
|
|
|
|
|
|
Mitty E, et al |
† |
† |
|
† |
|
† |
|
|
† |
|
|
|
|
|
|
Hyde J, et al |
|
† |
|
|
† |
† |
|
|
|
|
† |
|
† |
|
|
Evans S, et al |
† |
|
† |
|
† |
|
|
† |
† |
|
|
|
† |
|
|
MacLaren C, et al |
† |
† |
† |
† |
† |
|
|
† |
† |
† |
† |
|
|
|
|
Zimmerman S, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
Golant SM |
† |
† |
† |
† |
† |
† |
|
† |
† |
† |
† |
† |
|
† |
|
Gelfand, et al |
† |
† |
† |
† |
† |
† |
|
† |
|
† |
† |
|
|
|
|
Darton R, et al |
|
|
† |
|
† |
|
|
|
|
† |
|
|
|
|
|
Tinker A, et al |
† |
† |
|
|
|
|
† |
|
† |
|
|
|
|
|
|
Wright F, et al |
† |
† |
|
† |
|
|
† |
|
|
|
|
|
|
|
|
Dutton R |
† |
† |
|
|
|
|
† |
|
† |
|
|
|
|
|
|
Mitty E |
|
|
|
|
|
† |
|
|
|
|
|
|
|
|
|
Henning C, et al |
† |
|
† |
|
† |
|
|
† |
|
† |
|
|
|
|
|
Sprigg PE |
† |
|
|
|
|
† |
|
|
|
|
|
|
|
|
|
Park-Lee, et al |
† |
† |
† |
|
|
|
|
|
† |
† |
|
|
|
|
|
Egbu J, et al |
† |
† |
|
|
|
|
† |
|
|
|
|
|
|
|
|
Bow J, Et al. |
† |
|
|
|
|
|
|
|
† |
|
|
|
|
|
|
Jenkens R, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
Stachel AG, et al |
† |
|
† |
|
|
† |
|
|
|
|
† |
|
|
|
|
Allen J |
† |
† |
† |
|
|
† |
† |
|
|
† |
|
|
|
|
|
Heumann LF |
† |
† |
† |
† |
|
† |
† |
† |
† |
† |
|
|
|
|
|
Scharlach A, et al |
|
|
† |
† |
|
|
|
† |
|
|
|
|
|
|
|
Elkins JS |
† |
† |
† |
† |
† |
† |
† |
|
† |
|
|
|
|
|
|
Greco M |
† |
† |
† |
† |
† |
† |
|
† |
|
† |
|
|
† |
|
|
Wigfield A, et al |
|
|
|
|
|
|
|
|
† |
|
|
|
|
|
|
Greenfield EA, et al |
† |
† |
† |
|
† |
|
|
† |
|
|
|
|
|
|
|
Camarinha-Matos L, et al |
† |
|
† |
† |
† |
† |
|
|
|
† |
† |
† |
|
|
|
Pulkkinen T |
|
|
† |
|
† |
|
|
|
† |
† |
† |
|
|
|
|
Memon M, et al |
|
|
|
|
† |
|
† |
|
|
|
|
|
|
|
|
Camarinha-Matos LM, et al, |
† |
|
† |
|
|
† |
† |
|
† |
† |
† |
† |
|
|
|
Xia B, et al |
† |
† |
† |
|
† |
|
|
|
|
|
|
|
|
|
|
Wells L |
† |
|
|
† |
† |
|
|
|
† |
|
|
|
|
† |
|
Kisling A, et al |
† |
† |
† |
|
|
|
|
|
† |
|
|
|
|
|
|
Iecovich E |
† |
|
† |
† |
† |
† |
|
|
|
|
|
|
|
|
|
Kisling-Rundgren A et al |
† |
† |
|
|
|
† |
|
|
† |
|
|
|
|
|
|
Hu et al |
† |
† |
|
† |
† |
|
|
† |
|
† |
|
|
|
|
|
Writz J, et al |
† |
† |
|
† |
|
|
|
† |
|
|
|
|
|
|
|
Frequency of reference to the type of service |
58 |
46 |
42 |
40 |
39 |
34 |
27 |
27 |
24 |
22 |
10 |
7 |
5 |
5 |
A review of the literature indicated that personal care, nutrition services, social support, housekeeping services, medical and nursing care were among the priority services provided in housing for the aged. In some cases, services such as palliative care, rehabilitation services, and preventive services, including environmental modification, screening, and vaccination, were also observed.
Day Care Centres
DCCs represent comprehensive, organised, and community-based programmes designed with various health, social, and support services for responding to the disabled individual’s needs. Services are provided at any time of the day (within 24 hours). This type of service was designed for individuals who do not require full time care, to decrease admissions to NHs and LTC centres. The results of the current study indicated that the services available in older persons housing comprised non-medical services, health-related services, and social support care.
Non-medical services included personal care, transportation services, and environment modification. Health-related services included nursing care (healthcare services, case management, medication administration, wound care, injection, oxygen therapy, weight control, blood pressure control, diabetes control, infusion therapy, night-time care, and tube feeding), medical care (medical support, home palliative care at home, chemotherapy, access to a therapeutic team, and radiotherapy), rehabilitation services, psychology services, consultation and education, hospice care, and other therapies.
The social support services of DCCs included family support groups, respite care, consultation, recreational activities, intergenerational programmes, and sports programmes (Table 4).
Table 4. Services covered by day care centres, based on the literature review.
|
Included articles |
Social services |
Personal care services |
Nursing services |
Medical services |
Rehabilitation services |
Education & counselling |
Nutrition services |
Transportation |
Other therapy |
Psychological services |
Hospice care |
Home modification |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Copp G, et al |
† |
† |
† |
† |
|
|
|
|
|
† |
|
|
|
Jarrott SE, et al |
† |
† |
|
|
|
|
|
† |
† |
|
|
|
|
Williams SE |
|
|
|
|
|
|
† |
|
|
|
|
|
|
Higginson I, et al |
|
† |
† |
† |
† |
|
|
† |
† |
|
|
|
|
The National Council on the Aging |
† |
|
|
† |
|
† |
|
|
|
|
|
|
|
Cox N, et al |
† |
† |
† |
† |
† |
|
† |
† |
|
|
† |
|
|
Jennings-Sanders A |
† |
† |
† |
|
† |
† |
† |
† |
|
|
|
|
|
Gelfand DE |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
O’Keefe, et al |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
|
|
Alteras T |
† |
† |
† |
† |
† |
† |
† |
|
|
† |
|
|
|
Silverstein, et al |
† |
† |
† |
|
† |
† |
† |
† |
† |
|
|
† |
|
Silverstein NM, et al |
† |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
|
Dabelko-Schoeny, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
An Y |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
Wei DK, et al |
† |
† |
† |
† |
|
|
|
|
† |
|
|
|
|
Howard R |
† |
† |
|
|
|
† |
† |
† |
|
|
|
|
|
Lin W, et al |
† |
|
† |
|
† |
|
|
|
|
† |
|
|
|
Frequency of reference to the type of service |
15 |
14 |
13 |
11 |
11 |
10 |
9 |
9 |
6 |
5 |
2 |
1 |
Studies conducted in this area reported that social support services, personal care, medical and nursing care, and rehabilitation services were priority services delivered in the DCCs. In addition, home modification, hospice care, and psychological services were also observed in the service packages of some of these centres.
Senior Centres
SCs are centres in which various programmes and services are provided, such as nutrition programmes, healthcare programmes, art, recreational and volunteer programmes, transportation services, educational classes, helping staff members, intergenerational programmes, group and social programmes, support services for caregivers, social support, and daily care for older persons.
Non-medical services included personal care (helping older adults with ADL and IADL), nutrition services, transportation, recreational, art and sports programmes, educational classes (cooking and computer), consultation services (financial and legal counselling), and respite care.
Health and fitness services comprised screening programmes (e.g., depression, blood pressure, cancer, vision, hearing, and mammography), daily healthcare, personal training, nutrition services and weight control, special programmes for people with dementia, rehabilitation care, psychology services, personal counselling, and referrals.
The social support services of SCs include intergenerational programmes, cultural programmes, educational classes, support groups and volunteers, respite care, friendly visits, transportation, personal care at homes, and rehabilitation services (Table 5).
Table 5. Services covered by senior centres, based on the literature review.
|
Included articles |
Social services |
Educational & counselling |
Nutrition |
Health & fitness services |
Transportation |
In-home services |
Rehabilitation services |
|---|---|---|---|---|---|---|---|
|
Krout JA |
† |
† |
† |
† |
† |
† |
† |
|
Feinberg, et al, |
† |
† |
|
|
|
† |
|
|
Martin C, et al |
† |
† |
† |
† |
† |
|
|
|
Skarupski, et al |
† |
† |
† |
† |
† |
|
|
|
Staicovici S |
† |
† |
|
|
|
† |
|
|
Al Mahdy H |
|
|
|
|
|
† |
|
|
Turner, et al |
† |
† |
† |
† |
† |
|
|
|
Pardasani M |
† |
|
† |
† |
|
|
|
|
Gelfand DE |
† |
† |
† |
† |
† |
† |
|
|
Krout JA |
† |
† |
† |
† |
† |
|
|
|
Pardasani, et al |
† |
† |
† |
† |
† |
|
|
|
Dal Santo TS |
† |
† |
† |
† |
|
|
† |
|
Jellinek I, et al |
† |
† |
† |
† |
† |
† |
|
|
Pardasani M, et al |
† |
|
† |
† |
|
|
|
|
Pettigrew KA |
† |
† |
† |
|
|
|
|
|
Frequency of reference to the type of service |
14 |
12 |
12 |
11 |
8 |
6 |
2 |
Studies conducted in this area showed that social support, training and consultation, nutrition services, fitness, and healthcare were the priority services delivered in the SCs. In some cases, services such as home care and rehabilitation care were also provided.
Nursing Home
This term used in most countries to describe a centre in which support services and nursing are provided in addition to housing services for the older persons who are no longer able to live independently in their houses. Short-term services are also provided to individuals who require nursing care and help in completing daily activities due to chronic disorders. Skilled care services are also provided for the older persons in specialised centres.15 The results of the current research indicated that services provided in NHs included non-medical services, healthcare services, and social support services.
Non-medical services comprised personal care (assisting older adults with ADL and IADL), meal delivery, and transportation services.
Health services included nursing and medical services (daily curative care, emergency assistance, chiropody, dialysis, injection, fusion therapy, oral hygiene, and dental care services).
Social support services included family support, respite care, and counselling for older persons and their family members (Table 6).
Table 6. Services covered by nursing homes, based on the literature review.
|
Included articles |
Medical care |
Nursing care |
Rehabilitation services |
Social services |
Personal care |
Nutrition services |
Hospice care |
Transportation |
Home maker services |
|---|---|---|---|---|---|---|---|---|---|
|
Cates N |
† |
† |
† |
|
† |
† |
|
|
|
|
Ribbe MW, et al |
† |
|
† |
† |
|
|
† |
|
|
|
Ishizaki T, et al |
† |
† |
† |
|
|
|
|
|
|
|
Jones A |
|
† |
† |
† |
|
|
† |
† |
|
|
Rosewarne RC |
|
† |
|
† |
† |
|
|
|
|
|
Davis JA, et al |
† |
† |
† |
† |
† |
† |
|
|
† |
|
AARP Public Policy Institute |
† |
† |
|
|
† |
|
† |
|
|
|
Chu L-W, et al |
† |
† |
|
† |
† |
|
|
|
|
|
Molinari V, et al |
† |
|
|
† |
|
|
|
|
|
|
Kim S-H, et al |
† |
† |
† |
† |
† |
|
|
|
|
|
Day, T |
† |
† |
† |
|
† |
|
|
|
|
|
Frequency of reference to the type of service |
9 |
9 |
7 |
7 |
7 |
2 |
3 |
1 |
1 |
A review of the related literature showed that medical and nursing services, rehabilitation services, social support services, and personal care were among the highest priority services provided in NHs. In addition, hospice care, home modification, and transportation were also observed in some service packages.
Hospice Care
Palliative care includes care provided to the patient and their family with the aim of enhancing quality of life by predicting, preventing, and treating pain and suffering by responding to emotional, mental, social, spiritual, and physical needs while aiming to maintain the patients independence. Hospice care includes supportive care for patients in the final stages of a disease, to maintain the dignity and quality of life of patients who are in the final stages of their lives; this is achieved through relief and control of unpleasant symptoms. HC services comprised nonmedical services, medical services, and social support services.
Health-related services included nursing care (symptom and pain management, medication administration, case management, and providing the required medications), medical services (acute and outpatient care, overall patient assessment, radiology, advanced care planning, providing necessities, and other therapies such as respiratory therapy, music therapy, and message therapy), rehabilitation services (occupational therapy, providing assistive devices and equipment such as walkers and wheelchairs), palliative care services, and psychological services.
Social support included communicating with the patient, supportive counselling, spiritual and palliative consultation, emotional support, respite care, writing wills, support for family caregivers, volunteer services, having sympathy with family members, and bereavement care (Table 7).
Table 7. Services covered by hospice care, based on the literature review.
|
Included articles |
Nursing care |
Social support |
Spiritual counselling |
Rehabilitation services |
Bereavement services |
Home maker services |
Nutrition services |
Personal service |
Palliative care |
Psychosocial services |
Other therapy |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Taylor, et al |
† |
† |
|
† |
† |
† |
|
|
|
|
|
|
|
Wiener JM, et al |
† |
† |
† |
|
† |
† |
† |
† |
† |
† |
† |
|
|
Haupt, et al |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
|
|
Miller, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
Glass AP, et al |
† |
† |
† |
† |
† |
|
|
|
|
|
† |
|
|
Herbst L |
† |
† |
† |
|
† |
† |
|
|
† |
|
|
† |
|
Chung, et al |
|
† |
|
† |
† |
|
|
|
|
|
|
|
|
National Quality Forum |
|
|
† |
† |
|
† |
|
|
|
|
|
|
|
Fine PG, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
† |
|
|
Carlson MD, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
|
|
Harrison JP, et al |
† |
† |
|
|
† |
† |
† |
† |
† |
|
|
|
|
Stevenson DG, et al |
† |
† |
† |
† |
† |
|
† |
† |
† |
† |
† |
† |
|
Smith MA, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
† |
† |
|
Rich SE, et al |
† |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
† |
|
Stevenson, et al |
† |
† |
|
† |
|
† |
|
|
† |
|
|
|
|
Batchelor NH |
† |
|
† |
|
† |
† |
|
|
|
† |
|
|
|
Medicare Cf |
† |
† |
† |
† |
† |
|
† |
† |
|
|
|
|
|
Jeyaraman S, et al |
† |
|
|
|
|
|
|
|
|
|
|
|
|
Lee CY, et al |
† |
† |
† |
† |
† |
† |
† |
|
|
|
† |
|
|
Friebert S, et al |
† |
† |
† |
† |
† |
† |
† |
† |
|
|
|
|
|
Vogel SL |
† |
† |
† |
† |
† |
† |
|
† |
† |
† |
|
|
|
Litrivis E, et al |
† |
† |
† |
|
|
|
|
† |
|
† |
† |
|
|
Hutcheson A |
† |
† |
† |
† |
† |
† |
† |
|
|
† |
|
|
|
Sherman DW, et al |
† |
|
|
† |
|
|
† |
|
|
† |
|
† |
|
Lester PE, et al |
|
† |
|
† |
|
† |
|
|
|
|
|
|
|
Verderber S |
† |
† |
† |
|
|
|
|
† |
|
† |
|
|
|
Spiess JL, et al |
† |
|
† |
† |
|
† |
|
|
|
|
|
|
|
Frequency of reference to the type of service |
24 |
22 |
20 |
20 |
19 |
18 |
13 |
13 |
10 |
9 |
8 |
5 |
A review of the literature indicated that medical and nursing care, social support, spiritual counselling, rehabilitation services, and bereavement care were among highest priority services provided by HC Personal care and certain therapies, such as music therapy and pet therapy, were also reported in some studies.
Regarding the results of the current study and evaluating care services, the most common care provided to the older people included personal care, social support services, nursing and medical services, nutrition, rehabilitation, housekeeping, transportation, education, consultation, palliative and hospice care, supervision, psychological services, environment modification, home maintenance, and preventive services (Table 8).
Table 8. Most frequently reported services for older persons in the reviewed literature.
|
Included articles |
Personal care services |
Social support |
Nursing care |
Medical care |
Nutrition services |
Rehabilitative services |
Home maker services |
Education and counselling |
Transportation |
Hospice and palliative care |
Supervision |
Home modification |
Psychological services |
Bereavement services |
Fitness services |
Preventive care services |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Housing for the aged |
58 |
42 |
34 |
39 |
46 |
22 |
40 |
24 |
27 |
7 |
27 |
1 |
2 |
- |
- |
10 |
|
Day care |
14 |
15 |
13 |
11 |
9 |
11 |
- |
10 |
9 |
2 |
- |
1 |
5 |
- |
- |
- |
|
Home care |
34 |
28 |
36 |
33 |
15 |
18 |
20 |
11 |
9 |
7 |
- |
5 |
6 |
- |
- |
- |
|
Hospice care |
10 |
20 |
24 |
22 |
13 |
19 |
13 |
20 |
- |
9 |
- |
- |
8 |
18 |
- |
- |
|
Long-term care |
61 |
48 |
55 |
51 |
31 |
42 |
42 |
14 |
28 |
14 |
6 |
20 |
6 |
- |
- |
- |
|
Nursing homes |
7 |
7 |
9 |
9 |
2 |
7 |
1 |
- |
1 |
3 |
- |
- |
- |
- |
- |
- |
|
Senior centres |
6 |
14 |
- |
- |
12 |
2 |
3 |
12 |
8 |
- |
- |
- |
- |
- |
11 |
- |
|
Frequency of reference to the type of service |
190 |
174 |
171 |
165 |
128 |
121 |
119 |
91 |
82 |
42 |
33 |
27 |
27 |
18 |
11 |
10 |
Discussion
Nowadays, in developed countries, various care services have been designed and implemented to provide LTC services and to meet the needs of older persons. Regardless of the many similarities between some packages provided by these centres, relative heterogeneity was observed in the services provided by them. This can be due to differences in objectives, subsidiary structures, and the resources available to them. The current research results indicated that housing for the aged, LTC, and HC were among the more diverse and comprehensive services provided, compared with the models.
Housing for the aged, such as AL in the United States and ECH in England, were developed with the aim of helping the older persons to achieve independence, authority, dignity, enhancing social cooperation, and improving quality of life, with emphasis on privacy, having living conditions similar to their home, and ageing in place.16,17 These residential care settings are intended mainly for older persons, individuals who are dependent on others, or have medical and nursing needs, and provide tailored personcentred services to respond to the care needs of the individuals.18 For this reason, a range of services, including personal care, nutrition services, preventive care, and palliative care, are provided in AL and ECH. Whereas the main objective of housing for the aged is to help maintain individuals’ independence and quality of life, services such as personal care and housekeeping services are included in most service packages; services such as medical and nursing care are of second priority.
HC is rapidly expanding in developed countries, with the aim of reducing the healthcare costs of the older persons in hospitals and decreasing their reliance on NHs. HC services are frequently provided to older persons based on medical and nursing needs and the individuals’ functional limitations in ADL and IADL.13,19 For this reason, a number of services are provided in this structure, including personal care, nursing and medical care, and home modification. One of the special objectives of HC is the prevention of unnecessary hospitalisation and admission to NHs, and services such as medical and nursing care are of higher priority than educational and palliative services.
LTC services are social-based and aim to maintain and enhance physical performance, personal independence, and quality of life.20 Therefore, a range of services are provided in LTC systems, such as rehabilitation services, nutrition services and meals delivery, home modification, and mental health services. The current research findings indicated that LTC services were mainly based on criteria such as age, extent of disability and vulnerability, medical or nursing needs, and individual income.21,22 On this basis, services such as personal care and medical and nursing care were included in most service packages.
In developed countries, only older people with severe problems who cannot live at home are transferred to institutional settings. In Sweden, individuals being treated for chronic disorders, dementia, and severely frail patients are admitted to NHs. In the Netherlands, many NH residents suffer from physical disabilities, dementia, and mental disorders, and they are thus provided with full-time medical and nursing care. Individuals are admitted to a NH after surgery or a severe illness and high-level rehabilitation services are provided.23 Special units exist in NHs in the United States, such as acute care and a special section for Alzheimer’s patients.24
SCs are centres created for enhancing the health and welfare of older persons and encouraging them to participate in recreational activities, group programmes, and health and nutrition programmes.25 Various services such as health and wellbeing, transportation, and rehabilitation are provided for older persons in SCs. Volunteer groups provide most services in these centres. Among the social support programmes is the family member support programme. As the main goal of SCs is to increase welfare and social participation of older persons, social support services are emphasized.
DCCs are centres in which a series of parttime social support services and personal care is provided. Different models of DCC, such as the social model, health model, and specialised model, were created for different groups of older persons. In the social model, programmes are considered for older persons suffering from physical or cognitive disabilities, and include games, art and handicrafts, and discussion groups. In the health model, which is combined with the social group, nursing services are included in addition to the social model activities. In the specialised model, special services are provided for certain groups, such as older persons diagnosed with dementia, Alzheimer’s or mental health disorders.26 Considering that providing services in various DCC units is social-based, and each group focuses on a specific group of older persons, social support services and personal care have higher priority in most service-providing centres.
HSCs represent support care for maintaining quality of life and dignity of patients and their family members.27 Hospice services are provided in various centres, such as NHs, patients’ homes, hospitals, special hospice care centres, health service agencies, and social clinics.28,29 The target group of these care services is mainly end-stage patients and individuals with life expectancies of less than 6 months; these individuals and their family members are provided with a series of services, such as spiritual counselling and bereavement care.30,31 Considering that hospice services aim to relieve pain and control the unpleasant symptoms of endstage patients, and also provide mental support for their families, special attention to spiritual counselling and special services for the remaining family members are emphasised. Therefore, medical care, nursing care, and rehabilitation services are of higher priority than other services in these settings. The aforementioned results can be used for prioritising services in case of limitations in resources. LTC and HC services have received more attention in terms of scientific resources, which can be used efficiently to design a proposed model for the care of older persons. Services related to each care system are separately evaluated and reported, and centres providing services for older adults can be proactive in meeting the needs of their recipients based on their priorities and available resources.10 We believe that the results of this study can represent a guiding point for managers and policy makers in older persons care for the development and implementation of an adequate and evidence-based care structures.
Among the strengths of the current research is the evaluation of a large number of databases and search engines, evaluating the services provided with a division of systems, prioritising the services provided based on their frequency, linking the type and nature of the care system with service recipients, and prioritising identified services. A limitation of this study is that we were unable to determine which care services were most essential but lacking in different healthcare settings; however, we were able to describe the availability of services for older persons as they were reported in the literature. Another limitation is that this study only reported on healthcare services for older persons that were published in the literature and would have excluded many services that were not published.
The results of the current study can represent a beneficial guideline for planners and policy makers in the field of designing older persons care services, based on the identified priorities, the nature and mission of each older persons care system, and needs of the service recipients. In line with localisation and adaptation of the older persons care model, we suggest that the implementation and significance rate of each of the identified factors be studied and assessed by considering specialist opinions. In addition, it is important to obtain the opinions of the service recipients and beneficiaries and to consider them when defining and implementing the final model. Finally, it is necessary to conduct a pilot test to study the satisfaction rate of service recipients and the implementation rate of the defined package, especially considering cost effectiveness prior to its expansion.
Conclusion
This study described the diverse care services available to older persons that have been reported in the literature. The results can assist in selecting care service systems based on older persons’ needs, defining service packages in care systems based on the availability of resources, and providing the required resources, including manpower, physical space, medical or non-medical devices, and materials based on the defined service package. Further research is required in different healthcare systems regarding which service is most required and lacking in the relative settings.
Acknowledgments
The researchers are grateful for the financial support of the Tabriz University of Medical Sciences.
Conflicts of Interest
The authors declare that there are no conflicts of interests.
Appendix file
The complete reference list can be found at: https://e-mfp.org/wp-content/uploads/RV1221-Care-Services-for-Older_Appendix.docx
How does this paper make a difference to general practice?
The service package defined in different systems for providing services to the elderly varies according to the nature of the system and the clinical and social needs of elderly.
This review identified and prioritized different cares provided in various service systems for the elderly.
Due to the limited resources available to the health system, and considering the importance of improving efficiency and effectiveness in them, the results of this study can be used in selecting the service providing system for the elderly, defining the service providing package, and optimal use of the available resources.
References
- 1.Mulumba M, Nantaba J, Brolan CE, et al. Perceptions and experiences of access to public healthcare by people with disabilities and older people in Uganda. Int J Equity Health. 2014;13(76):1–9. doi: 10.1186/s12939-014-0076-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Noroozian M. The elderly population in Iran: an ever-growing concern in the health system. Iran J Psychiatry Behav Sci. 2012;6(2):1–6. [PMC free article] [PubMed] [Google Scholar]
- 3.Gavarskhar F, Matlabi H, Gharibi F. A systematic review to compare residential care facilities for older people in developed countries: practical implementation for Iran. Cogent Soc Sci. 2018;4(1):1478493. doi: 10.1080/23311886.2018.1478493. [DOI] [Google Scholar]
- 4.Shrestha LB. Population aging in developing countries: the elderly populations of developing countries are now growing more rapidly than those in industrialized nations, thanks to health advances and declining fertility rates. Health Aff. 2000;19(3):204–212. doi: 10.1377/hlthaff.19.3.204. [DOI] [PubMed] [Google Scholar]
- 5.Bindels J, Cox K, Abma TA, et al. Implementing care programmes for frail older people: a project management perspective. Health Policy. 2015;119(1):9–16. doi: 10.10l6/j.healthpol.20l4.09.008. [DOI] [PubMed] [Google Scholar]
- 6.Bindels J, Cox K, Widdershoven G, et al. Care for community-dwelling frail older people: a practice nurse perspective. J Clin Nurs. 2014;23(15-16):2313–2322. doi: 10.1111/jocn.12513. [DOI] [PubMed] [Google Scholar]
- 7.Luanaigh CÓ, Lawlor BA. Loneliness and the health of older people. Int J Geriatr Psychiatry. 2008;23(12):1213–1221. doi: 10.1002/gps.2054. [DOI] [PubMed] [Google Scholar]
- 8.Threapleton DE, Chung RY, Wong SY. Integrated care for older populations and its implementation facilitators and barriers: a rapid scoping review. Int J Qual Health Care. 2017;29(3):327–334. doi: 10.1093/intqhc/mzx041. [DOI] [PubMed] [Google Scholar]
- 9.Prince MJ, Wu F, Guo Y. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–562. doi: 10.1016/S0140-6736(14)61347-7. [DOI] [PubMed] [Google Scholar]
- 10.Gavarskhar F, Matlabi H, Gharibi F. An Iranian model for the elderly care in residential long-term care institutions: a Delphibased study. Middle East J Rehab Health Stud. 2021;8(3):e112944. doi: 10.5812/mejrh.112944. [DOI] [Google Scholar]
- 11.Peyrovi H, Mortazavi H, Joolaee S. Challenges of Iranian family members in decision making to put elderly people with chronic diseases in nursing homes: a qualitative study. Arch Sci. 2012;65(10):1–8. doi: 10.1186/s12877-022-02881-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lehning AJ, Austin MJ. Long-term care in the United States: policy themes and promising practices. J Gerontol Soc Work. 2010;53(1):43–63. doi: 10.1080/01634370903361979. [DOI] [PubMed] [Google Scholar]
- 13.Venables D, Reilly S, Challis D, et al. Standards of care in home care services: a comparison of generic and specialist services for older people with dementia. Aging Ment Health. 2006;10(2):187–194. doi: 10.1080/13607860500310518. [DOI] [PubMed] [Google Scholar]
- 14.Jones A, Howe A, Tilse C, et al. Service integrated housing for Australians in later life: Australian Housing & Urban Research Institute. 2010 [Google Scholar]
- 15.Hallberg IR, Leino-Kilpi H, Meyer G. Dementia care in eight European countries: developing a mapping system to explore systems. J Nurs Scholarsh. 2013;45(4):412–424. doi: 10.1111/jnu.12046. [DOI] [PubMed] [Google Scholar]
- 16.Wilson KB. Historical evolution of assisted living in the United States, 1979 to the present. Gerontologist. 2007;47(1):8–22. doi: 10.1093/geront/47.Supplement_1.8. [DOI] [PubMed] [Google Scholar]
- 17.Hawes C, Phillips CD, Holan S, et al. Assisted living in rural America: results from a national survey. J Rural Health. 2005;21(2):131–139. doi: 10.1111/j.1748-0361.2005.tb00073.x. [DOI] [PubMed] [Google Scholar]
- 18.Mollica R. Coordinating services across the continuum of health, housing, and supportive services. J Aging Health. 2003;15(1):165–188. doi: 10.1177/0898264302239022. [DOI] [PubMed] [Google Scholar]
- 19.Schmid H. The Israeli long-term care insurance law: selected issues in providing home care services to the frail elderly. Health Soc Care Community. 2005;13(3):191–200. doi: 10.1111/j.1365-2524.2005.00548.x. [DOI] [PubMed] [Google Scholar]
- 20.Mui AC. The program of all-inclusive care for the elderly (PACE) an innovative long-term care model in the United States. J Aging Soc Policy. 2002;13(2-3):53–67. doi: 10.1300/J031v13n02_05. [DOI] [PubMed] [Google Scholar]
- 21.Tsutsui T, Muramatsu N. Japan's universal long-term care system reform of 2005: containing costs and realizing a vision. J Am Geriatr Soc. 2007;55(9):1458–1463. doi: 10.1111/j.15325415.2007.01281.x. [DOI] [PubMed] [Google Scholar]
- 22.Applebaum R, Bardo A, Robbins E. International approaches to long-term services and supports. Generations. 2013;37(1):59–65. https://www.jstor.org/stable/26555977 [Google Scholar]
- 23.Ribbe MW, Ljunggren G, Steel K. Nursing homes in 10 nations: a comparison between countries and settings. Age Ageing. 1997;26(2):3–12. doi: 10.1093/ageing/26.suppl_2.3. [DOI] [PubMed] [Google Scholar]
- 24.Chan JP. From elderly care institutions to longterm care policy: evolution of nursing homes in the United States and China: The American University; 2002. [Google Scholar]
- 25.Pardasani M, Thompson P. Senior centers: innovative and emerging models. J Applied Gerontol. 2012;31(1):52–77. doi: 10.1177/0733464810380545. [DOI] [Google Scholar]
- 26.Silverstein NM, Wong CM, Brueck KE. Adult day health care for participants with Alzheimer's disease. Am J Alzheimer's Dis Other Demen. 2010;25(3):276–283. doi: 10.1177/1533317510361237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Verderber S. Residential hospice environments: evidence-based architectural and landscape design considerations. J Palliat Care. 2014;30(2):69–82. doi: 10.1177/082585971403000202. [DOI] [PubMed] [Google Scholar]
- 28.Lee CY, Komatsu H, Zhang W. Comparison of the hospice systems in the United States, Japan and Taiwan. Asian Nurs Res. 2010;4(4):163–173. doi: 10.1016/S1976-1317(11)60001-7. [DOI] [PubMed] [Google Scholar]
- 29.Sherman DW, Cheon J. Palliative care: a paradigm of care responsive to the demands for health care reform in America. Nurs Econ. 2012;30(3):153–162. [PubMed] [Google Scholar]
- 30.Wiener JM, Tilly J. End-of-life care in the United States: policy issues and model programs of integrated care. Int J Integ Care. 2003;3(1):e24. doi: 10.5334/ijic.81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Harrison JP, Ford D. A comprehensive community-based model for hospice care. Am J Hosp Palliat Med. 2007;24(2):119–125. doi: 10.1177/1049909106297070. [DOI] [PubMed] [Google Scholar]