

Abstract
Social media allows interventional cardiologists to disseminate and discuss research and clinical cases in real-time, to demonstrate and learn innovative techniques, to build professional networks, and to reach out to patients and the general public. Social media provides a democratic platform for all participants to influence the conversation and demonstrate their expertise. This review addresses the use of social media for these purposes in interventional cardiology, as well as respect for patient privacy, how to get started on social media, the creation of high-impact social media content, and the role of traditional journals in the age of social media. In the future, we hope that interventional cardiology fellowship programs will incorporate social media training into their curricula. Additionally, professional societies may adapt to the rapid dissemination of data on social media by developing processes to update guidelines more rapidly and more frequently.
Keywords: appropriate use, clinical trials, evidence-based medicine, health care policy, new devices, comparative effectiveness/patient centered outcomes research
Social Media Abstract
#SoMe allows ICs to discuss research, cases & techniques & to network.
This review discusses high-impact #SoMe & the role of traditional journals in the age of #SoMe.
Social media platforms have revolutionized how we obtain and process news. Twitter, Facebook, Instagram, LinkedIn, YouTube, and others allow anyone to disseminate information rapidly and interactively to a broad audience. In the last decade, social media has expanded from a venue for camaraderie to a vehicle for professional communication. Practicing in a rapidly-evolving field driven by the latest data, interventional cardiologists can harness the power of social media to disseminate and discuss research and clinical cases in real-time, demonstrate and learn innovative techniques, build professional networks, and reach out to patients and the general public. Social media provides a democratic platform for all participants to influence the conversation and demonstrate their expertise. This review addresses the use of social media for these purposes in interventional cardiology, as well as respect for patient privacy, how to get started on social media, the creation of high-impact social media content, and the role of traditional journals in the age of social media.
Benefits of Social Media for Interventional Cardiologists
Dissemination of Research
We conservatively estimate a minimum of 1000 cardiovascular medicine articles published weekly within the 362 cardiovascular medicine journals identified by Scopus (scopus.com). Faced with this information overload, physicians cannot hope to keep abreast of the latest research by reading every full-text article or even every abstract. Social media helps to manage the influx of information in two ways. First, posts are brief, typically consisting of a single image and accompanying caption, which are easily digestible. Twitter, for example, restricts posts to 280 characters. Second, social media algorithms actively promote more popular posts. As a result, users are more likely to see high-impact material that has been “liked” or shared by many of their colleagues: from this curated material, users may then select abstracts and full-texts to read.
While social media lacks a formal peer review process, it offers what Dr. Robert W. Yeh calls “peer review by the crowd”(1), democratically allowing all readers to comment, documenting how many readers concur with each opinion, and algorithmically giving preference to propagate the most popular opinions. Reviews are rapid, with social media users even critiquing research real-time during conference presentations(2). Altmetric (altmetric.com) calculates an Attention Score using an automated algorithm to generate a weighted count of the readership, social media attention, and citation for each published article (Figure 1).
Figure 1.
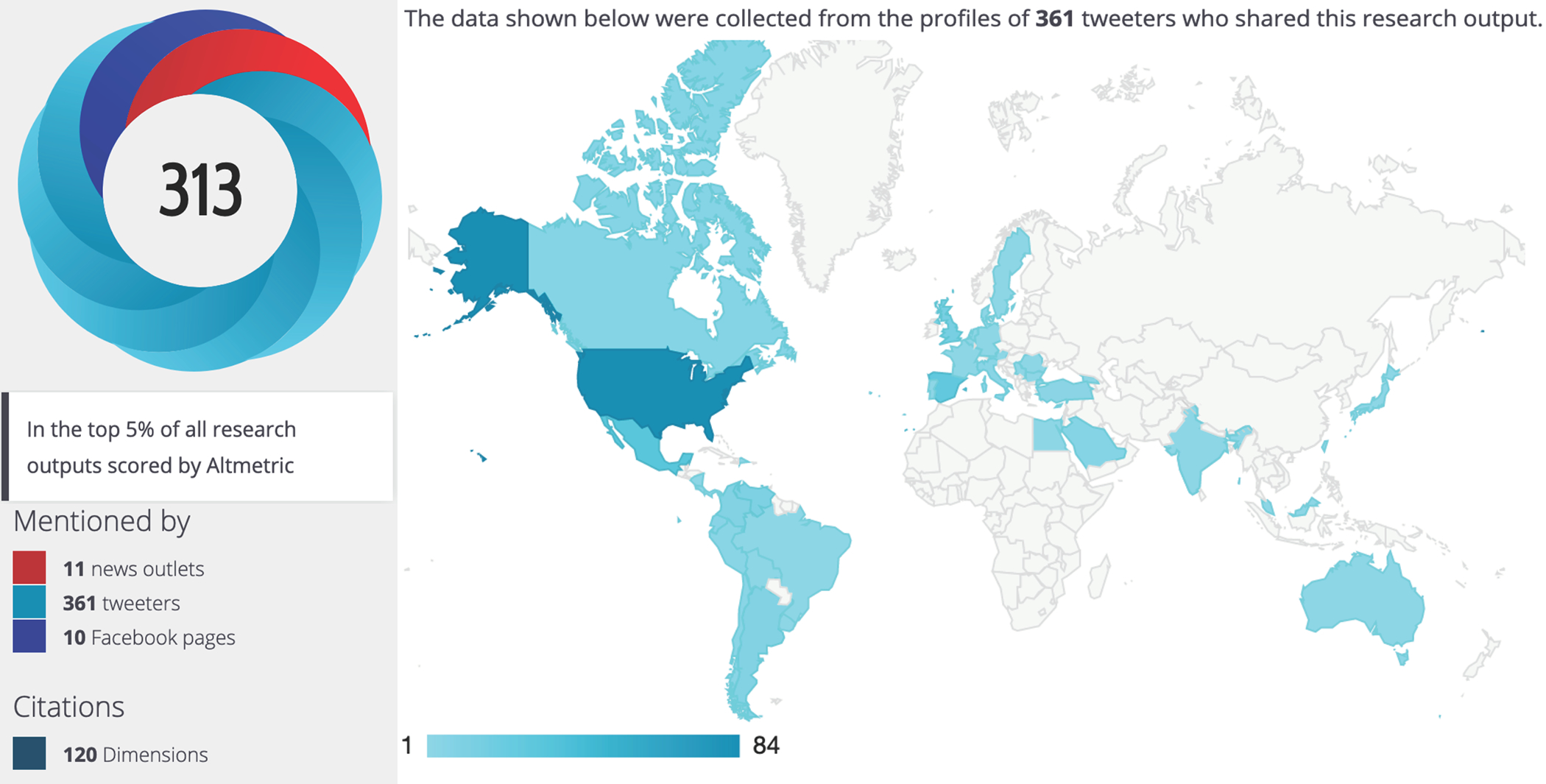
Altmetric Attention Score for publication of the SCAI Shock Classification(17) including news outlets, Tweeters, Facebook pages, citations, and map of Tweeters’ geographic locations.
Many authors routinely post their publications on social media both to share their research and clinical skills, and to promote themselves professionally. Accordingly, the effective use of social media has become a critical skill in academic cardiology. Many institutions use social media accounts to promote their affiliates’ research for professional- and patient-targeted marketing purposes(3). Additionally, many major journals post new articles on social media at the time of online publication, often months before print publication, which facilitates faster and wider dissemination(4). Many professional conferences designate official social media ambassadors, who share highlights of presentations in real-time. Even device manufacturers generate posts and advertisements, allowing them to participate in the online interventional cardiology community for marketing and educational purposes. Thus, social media has developed into a significant modality for interventional cardiologists to disseminate and obtain practice-changing scientific data, reviews, opinions, and guidelines while concurrently democratizing access to senior authors and opinion leaders.
Discussion of Clinical Cases
Following the SYNTAX and PARTNER trials, the “heart team” approach to interventional cardiology has become standard. Social media invites the “global heart team” to share their opinions on local cases. As many interventional cardiologists subspecialize further in specific aspects of coronary, structural, and peripheral techniques, local partners with expertise in their own subspecialties may be unavailable to provide a “second set of eyes.” Accordingly, interventional cardiologists have turned to social media for second opinions – sharing angiograms, echocardiograms, and computed tomographs and soliciting advice and consensus from far-flung colleagues.
Sharing Innovative Techniques
Historically, clinical innovation required operators to visit leading centers, work with pioneers, and promulgate their teachings. However, new techniques can also be promulgated very rapidly on social media. One of the most frequently referenced interventional cardiology social media posts was generated by Dr. Jason Wollmuth. On June 14, 2019, Dr. Wollmuth shared on Twitter a 1-minute 32-second video in which he placed an 8 French sheath through the rubber diaphragm of a 14 French mechanical circulatory support device sheath, permitting coronary intervention and circulatory support through a single 14 French access site (Figure 2)(5). Within days, social media documented rapid uptake of this technique, and single-access supported coronary intervention became mainstream within months, all without a single formal journal article. That video was viewed more than 9000 times before Dr. Wollmuth published the technique 4 months later in this Journal (6).
Figure 2.

Tweet from Dr. Jason Wollmuth that made single-access mechanical circulatory supported percutaneous coronary intervention a common practice 4 months before formal publication of the technique(5).
In another frequently referenced post, in December 2016, Dr. Ferdinand Kiemeneij first shared photographs on Twitter of distal left radial artery or anatomic snuffbox arterial access for coronary angiography. Through its introduction on social media, the distal left radial approach exploded(7), and over a 100 institutions on 5 different continents had adopted the approach in less than a year, based almost entirely upon learning about the approach on social media. Dr. Kiemeneij celebrated this accomplishment in December 2017 by compiling pictures of the first 100 distal left radial catheterizations posted on Twitter, sharing his compilation on Twitter (Figure 3)(8).
Figure 3.

Dr. Ferdinand Kiemeneij compiled the first 100 Twitter pictures of distal left radial cardiac catheterization to celebrate the spread of the technique via social media(8). Fittingly, he posted this compilation on Twitter.
In addition to single-access supported intervention and distal left radial access, several other techniques have been notably introduced and popularized on social media including intravascular lithotripsy to facilitate transfemoral transcatheter aortic valve replacement (TAVR), bioprosthetic valve fracture for valve-in-valve TAVR, and laceration of the anterior mitral leaflet to prevent left ventricular outflow tract obstruction (LAMPOON) for transcatheter mitral valve replacement. Through engagement in social media, interventional cardiologists can learn about cutting edge approaches to complex anatomy in real time without having to wait for case presentations at conferences or publications of case series.
At present, hundreds of clinical cases are discussed daily on social media, many labeled with the hashtag #CardioTwitter. Users frequently tag experts in the field to seek their input. This not only facilitates excellence in clinical care, but it provides a tremendous didactic opportunity for practicing interventional cardiologists and trainees alike, supporting life-long learning and practice development at low cost and in addition to traditional educational venues.
Building Professional Networks
Social media allows interventional cardiologists to build robust networks with colleagues to collaborate on research projects and clinical initiatives. Through interactions on social media, multiple research collaborations have been established between interventional cardiologists in different regions of the country who have actually never met. This includes the EXPLANT TAVR Registry, which evaluates the outcomes of patients undergoing surgical replacement of a previously-implanted TAVR valve.
Additionally, involvement in social media allows interventional cardiologists individually and across health systems to showcase their work and to develop relationships with other interventional cardiologists around the globe, regardless of background or practice location. For example, during the COVID-19 pandemic, physicians worldwide used social media to pool rapidly their experiences working with limited personal protective equipment, triaging semi-elective procedures, and using thrombolytics for ST-elevation myocardial infarction in infected patients.
Among medical subspecialties, interventional cardiology continues to lag in terms of physicians’ sex and racial disparities, especially among authors and speakers: the equal platform provided by social media may help to chip away at some of these disparities. In addition, involvement in social media among fellows-in-training has allowed for exposure to cardiac catheterization laboratory directors, providing possible job opportunities.
Patient Outreach
While social media platforms like Twitter may be well suited to sharing research, clinical cases, and new techniques, other platforms such as Facebook and Instagram are optimal avenues for interventional cardiologists to communicate directly with patients and the general public. Post targeting a more general audience may use terminology and explanations aimed at non-medical readers with separate links for further information for patients and professionals leading to more specifically targeted web pages. Tags in these posts may feature locations and events to facilitate reaching the local community. In the pre-social media era, the only ways for physicians to reach new patients was through established referral networks and direct outreach to patient groups. With social media, one post about offering the most safe and effective approach to care in the region can reach thousands of prospective patients and instantly grow the practice.
Patient Privacy and Consent
Social media posts must preserve patient privacy(9), with no patient-identifiable information ever shared on social media. Institutional policies may dictate what content employees are permitted to share in social media fora. Posting from personal or institutional accounts about a recent clinical experience inevitably reveals the geographic region and year of a procedure or patient encounter. In the United States, the Health Insurance Portability and Accountability Act (HIPAA) stipulates 18 types of Protected Health Information (PHI) that must be redacted entirely (Table 1)(10).
Table 1.
The 18 Protected Health Information (PHI) identifiers that must be de-identified per the Health Insurance Portability and Accountability Act (HIPAA)(10).
| The 18 PHI Identifiers Under HIPAA | |
|---|---|
| A. Names | J. Account numbers |
| B. Geographic locations smaller than a state (or initial 3 digits of a ZIP code if codes beginning with those digits include total population >20,000) | K. Certificate/license numbers |
| C. Dates more specific than year | L. Vehicle identifiers and serial numbers (e.g. license plate) |
| D. Telephone numbers | M. Device identifiers and serial numbers |
| E. Fax numbers | N. Web Universal Resource Locators (URLs) |
| F. E-mail addresses | O. Internet Protocol (IP) addresses |
| G. Social security numbers | P. Biometric identifiers (e.g. fingerprints, voice prints) |
| H. Medical record numbers | Q. Full-face photographs |
| I. Health plan beneficiary numbers | R. Any other unique identifying number, characteristic, or code |
In addition to protecting patient privacy, patient consent is recommended before sharing even deidentified descriptions and images. At minimum, verbal consent should be obtained. Many hospitals require written consent before sharing any deidentified patient information on social media. Hospitals’ traditional media consent forms may be used for this purpose: written consent should describe what information is to be shared and on what specific platform; the signed consent document should be maintained in the electronic medical record along with other patient consent forms.
Even if deidentified, cases of unique complexity or interest may be easily identifiable to the patient concerned. Furthermore, the patient may follow the social media discussion, and this may impact the physician-patient relationship. Care should be taken not to post rare cases immediately after they are performed, which makes identifying the patient relatively easy. As healthcare providers, we must be vigilant to protect our patients, not only on the catheterization table but also on the Internet.
Tips for Using Social Media Effectively
Getting Started on Social Media
Savvy interventional cardiologists can harness the power of social media to become research thought leaders and well-regarded clinicians. First, after creating an account, a user must develop a personal brand. Building a brand on social media requires identification of an area of expertise in which a user can generate impactful and influential content. Building a brand is the most important aspect of developing a social media persona. New users should also consider if their focus within interventional cardiology will be on research, approaches to complex cases, or development of innovative treatment strategies. The brand should be reflected the user’s profile on each platform.
After planning a brand, the next step is to start following others’ social media accounts. We recommend following thought leaders in areas in which the user hopes to have an impact. Identifying key leaders across the spectrum of opinions will help the user find a balanced approach. The user should dedicate time to reading posts and responses to understand the flow of information on social media.
Equipped with this information, the user is ready to begin posting. Initial posts may be questions or comments on others’ content. Soon, the user will be ready to post original content as well. To prevent issues of professional liability, users are advised to note in their profiles that posts constitute solely their personal opinions, not medical advice, and not the positions of their employers or professional societies.
Become an Influencer: Creating High-Impact Posts
We propose an approach to optimize the impact of social media posts (Figure 4). Influential social media users must develop a base of followers who look to them for information. To establish a social media following, users should post useful and reliable information in a concise, digestible format. Daily posts, particularly at times when followers are online, keep the poster’s name and content perpetually in front of their target audience. Users can further cultivate their online audience through engagement with followers by liking, reposting, and commenting on their posts.
Figure 4.

Top ten tips for high-impact social media.
Additionally, users should maximize the draw and accessibility of each post. Graphics are critical for visual appeal: every post should contain pictures, charts, or videos, to attract attention. Content should also be congruent with the user’s brand so that readers appreciate the source of their information and will become reliable followers. The use of 1 to 3 hashtags (#) facilitates topic-focused discussions and makes posts keyword-searchable within each platform (Twitter, Facebook, Instagram, and LinkedIn). Tagging (@) authors, colleagues, and subject matter experts by their usernames encourages discussion, liking, and reposting. Links to webpages such as journal articles, news blogs, or personal profiles, drive traffic toward further content and allow followers to obtain in-depth information. Of note, to be counted by Altmetric, a posted or re-posted link must include the complete digital object identifier (DOI, https://doi.org/...); “likes” do not affect the Attention Score.
The amplification power of social media can be harnessed not only by bright and innovative cardiologists, but also by brash, brazen, entrepreneurial, and outrageous individuals. A pseudo-metric comically named the Kardashian Index has been proposed as the ratio of a researcher’s number of Twitter followers to the number of citations of published work(11). The very existence of this metric suggests that some individuals may attain undue social media popularity discordant with their academic accomplishments or authoritative expertise, essentially becoming “famous for being famous.” Social media should be used ethically and responsibly to democratize and disseminate valuable information, not abused for purposes of self-promotion and grandstanding.
Each social media platform has a slightly different niche within interventional cardiology as well as different geographic penetration(12). Twitter benefits from its enforced brevity, allowing for a high volume of rapid, short posts and replies. According to the company, approximately 21% of Twitter’s 330 million users are in the United States. Facebook, the oldest and most widely used of the platforms, has almost three billion unique users, 9% in the United States, with a greater focus on personal rather than professional material. LinkedIn is designed for job applications and presentation of credentials, serving 760 million users of whom 23% are in the United States. Users may post different material to reach different audiences via different platforms or may simply post the same material on multiple platforms to expand its reach.
Role of Traditional Journals in the Age of Social Media
In the age of social media, many traditional journals have become well-respected social media content providers (13). Unlike individual or institutional users, journals bring to social media the imprimatur of peer review and frequently the gravitas of endorsement by a professional organization. Many journals (including this one) state the authors’ Twitter usernames as part of the author listing and corresponding address. Also, journals often request that authors provide a social media abstract and visual abstract at the time of manuscript submission. These materials allow journals to promote new articles and stimulate discussion on social media simultaneous with online publication. In addition, journals’ social media divisions have begun to experiment with brief author or expert interviews to coincide with online publication and major professional meetings.
Journals have embraced social media to varying degrees. Within cardiology, Circulation and the Journal of the American College of Cardiology have developed robust, professionally-curated social media divisions with more than 100,000 followers. By contrast, the European Heart Journal is still planning its first foray into social media. Social media has also upended traditional measures of journal penetration. Many journals’ popularity on social media platforms (Table 2) and articles’ Altmetric Attention Scores differ markedly from established print journal metrics such as citation score, impact factors, and h-indices. The ease of contacting researchers through social media and e-mail has fueled the rise of innumerable journals of questionable validity, ranging from open access and quick review formats to frankly predatory publishers and scams, which account for up to 25% of open access journals(14). Competition from these journals for authors and readers is beyond the scope of this review but will doubtless grow and need to be addressed as the uptake of social media expands.
Table 2.
Twitter and Facebook followings of selected major cardiology journals in December 2020. Note that numbers of followers may not correlate with perceived journal prestige or impact factor.
| Journal | Twitter Followers | Facebook Likes |
|---|---|---|
| Circulation (@CircAHA) | 44,700 | 184,654 |
| JACC (@JACCJournals) | 45,900 | 117,580 |
| Heart (@Heart_BMJ) | 36,000 | 5078 |
| EuroIntervention (@EuroInterventio) | 10,400 | 14,212 |
| CCI (@CCIJournal) | 4250 | 185 |
| Vascular Medicine (@VMJ_SVM) | 4216 | n/a |
| Circulation: Cardiovascular Interventions (@CircIntv) | 4157 | n/a |
| Structural Heart (@crfshj) | 3818 | n/a |
| American Heart Journal (@AmericanHeartJ) | 3637 | n/a |
| CRM (@CardiovascRevascMed) | n/a | 3730 |
JACC = Journal of the American College of Cardiology
CCI = Catheterization and Cardiovascular Interventions
CRM = Cardiovascular Revascularization Medicine
Also, the rapidity of social media challenges the traditional journal model of a months-long submission-to-publication process. Journals (including this one) increasingly offer rapid review processes leading to faster initial online publication. Thanks to the Internet, articles may be published and disseminated online many months prior to print publication. By the time of formal print publication, most articles’ findings are “old news.” In fact, less prominent articles maybe published online only, which saves on printing costs and allows journals to accept and publish more manuscripts. Open access to journal articles further augments the ability to share on social media: by clicking on a shared DOI link to an open access article, users can instantly access the full text of an article, unlike the cumbersome and expensive process to access traditional subscription articles.
Interventional cardiology journals often focus on outcomes data in the papers that they publish. Therefore, the analytic tools built into social media platforms are particularly appealing to such journals in that they provide the “outcomes data” about publication and posting. Users can readily determine temporal trends in their posts’ viewership and engagement (Figure 5). Granular data elements regarding the distribution and reception of each individual post are available with a few simple mouse clicks. Equipped with such data, journals can tailor their posting behavior to optimize delivery and uptake by the target audience. In particular, randomized trial data in thoracic surgery have shown that sharing articles on Twitter may increase subsequent academic journal citations at 1 year(15).
Figure 5.

Social media platforms provide automatic analytic tools to assess broad trends in users’ reach and engagement as well as granular data about the performance of each individual post.
Indeed, traditional journals continue to play a very important role in the age of social media. However, that role has evolved, and journals must continue to adapt and innovate to provide up-to-date content to their readers in the most convenient and impactful forms.
Limitations of Social Media
In addition to its unique strengths, social media presents significant limitations when applied to research and clinical medicine. As described above, structured peer review is impossible, which may compromise data quality. Without formal peer review, there is a real risk of propagating misinformation: users must be appropriately skeptical and may seek confirmation of information gleaned from social media by surveying other social media posts and alternative information sources before arriving at their own conclusions. Even journals’ peer review processes may be affected: with the shortened time from manuscript submission to social media sharing, pre-print versions may be shared prior to the completion of peer review.
An important form of publication bias or survivor bias, sometimes termed “Twitter bias” results from the fact that interventional cardiologists principally post only regarding successful procedures. Social media feeds may be filled with images of complex and heroic procedures, critically ill patients, and off-label device usage. Conversely, cases resulting in adverse outcomes are rarely shared. The result is a highly skewed view of procedural appropriateness and feasibility.
Biases may also result from the social media platform and its users. Facebook and YouTube allow users to “like” or “dislike” content, but Twitter and LinkedIn only allow “liking,” relegating divergent opinions to text comments. Comments from individuals with larger followings may be viewed, “liked,” and reposted disproportionately. Specific content may be promoted aggressively by users or media outlets with conflicts of interest, skewing which articles are most visible. Advertising dollars can boost industry-related posts and distort the otherwise even-handed judgement of a platform’s algorithm, although boosted posts are universally labeled as such. Additionally, with platforms only restricting direct incitement to violence, social media critiques may degenerate into insults, inappropriate language, or even harassment. Social media content is archived, so even when “deleted,” posts may be permanently retrievable.
Furthermore, the portability of social media blurs the boundary between users’ work and home lives. Every platform is accessible via smartphone, and the greatest volume of user activity occurs during the evening hours. As such, the advent of social media in interventional cardiology may contribute to burnout. Users must exercise self-restraint and be aware of the potential for adverse, addiction-like behavior. Similar to recommendations for the prevention of other compulsive behaviors, limiting social social media activities to a prescribed time schedule, daily duration, or number of posts may help users avoid unhealthy social media behaviors.
The on-going rapid uptake of social media within the interventional cardiology community has not been symmetric. Social media use rates are highest among younger cardiologists, excluding opinions from many experienced physicians and scientists. As with print journals, most social media posts are authored in English, potentially limiting participation by non-English speakers.
With its virtually infinite storage capacity, social media may result in an information overload. Keyword searches and search filters may help locate specific information, but they cannot compete with the organization of a cataloged electronic library. Particularly, social media lacks the capacity for long-term data storage and access.
Conclusion and Future Directions
Beyond wires, balloons, and stents, social media provides interventional cardiologists with a revolutionary new tool. Social media grants all users the opportunity to disseminate research, share clinical knowledge, build professional relationships, and reach a global audience. We must harness this opportunity to benefit our profession, our trainees, and our patients. Indeed, the best practices for social media described in this review are widely applicable beyond interventional cardiology to the entire medical community and to many other fields.
The interventional cardiology literature is a living corpus, and social media enhances the quantity, rapidity, and availability of information. Just as researchers, clinicians, and journals are adapting, so too, professional societies must embrace social media. Instead of updating guidelines every few years based upon accumulating evidence, subcommittees could rapidly process new evidence and incorporate it into professional recommendations. This type of guideline development would require a wholesale restructuring of the guideline writing process, replacing the glacially paced sequence of evidence review, writing, and professional society approval with a more streamlined, continuous review and update process. However, by way of analogy, Microsoft previously distributed compact discs with major revisions to Windows operating systems (95, 98, 2000, XP, etc.) every few years; today, minor Windows updates to repair bugs are automatically and seamlessly pushed to users on the second Tuesday of every month.
Eventually, we expect that most interventional cardiologists will incorporate social media into their work. The ascendency of social media has accelerated during the COVID-19 pandemic, when major professional conferences have been cancelled or held in virtual formats. Navigating social media and creating high-impact posts have become a fundamental skills in interventional cardiology, whether for scientific, marketing, or continuing education purposes. Interventional cardiology trainees should be welcomed to the social media community. Moreover, they should receive training and mentorship regarding how to use social media optimally to stay up to date and to promote their work(16). Vehicles for such training may include review articles such this one, topical seminars at in-person and online meetings, and specific feedback from mentors regarding trainees’ individual posts. Current fellowship guidelines include a requirement for research participation with an eye toward publication; future educational guidelines may even incorporate a recommendation for social media within the training framework.
Social media is, by definition, a public forum. Accordingly, in addition to addressing colleagues and trainees, interventional cardiologists should use social media to address the most important audience, patients. Patients can learn about the gamut of cardiology, from prevention to procedures, and share their perspectives in a fashion available both to physicians and other patients. Software applications to harness the vast universe of social media and render it more accessible are in their infancy but developing rapidly. Such applications may ultimately define an online cardiovascular community including physicians, patients, industry, and regulators.
Although predictions are difficult, especially about the future (h/t [hat tip] Yogi Berra), we believe that social media is here to stay as a permanent part of interventional cardiology practice. Sharing knowledge and experience will enable our professional community to move forward together toward a bright, collaborative future.
Footnotes
Disclosures:
Dr. Cohen reports research grant support from Abbott, Edwards Life Sciences, Boston Scientific, Medtronic, Svelte, and Corvia; consulting income from Abbott, Edwards Life Sciences, Boston Scientific, Medtronic, Svelte, Corvia, Philips, Impulse Dynamics, and MyoKardia. Dr. Goldsweig reports grant support from the National Institute of General Medical Sciences, 1U54GM115458, and the UNMC Center for Heart and Vascular Research. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. None of the other authors have any conflicts of interest to disclose.
Data Availability Statement:
Data sharing not applicable to this article as no datasets were generated or analyzed during the writing of this review article.
References
- 1.Yeh R Academic Cardiology and Social Media: Navigating the Wisdom and Madness of the Crowd. Circulation. Cardiovascular quality and outcomes 2018;11(4). [DOI] [PubMed] [Google Scholar]
- 2.Tanoue M, Chatterjee D, Nguyen H, Sekimura T, West B, Elashoff D, Suh W, Han J. Tweeting the Meeting. Circulation. Cardiovascular quality and outcomes 2018;11(11). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alraies MC, Raza S, Ryan J. Twitter as a New Core Competency for Cardiologists. Circulation 2018;138(13):1287–1289. [DOI] [PubMed] [Google Scholar]
- 4.Alraies MC, Sahni S. Why cardiologists should be on social media - the value of online engagement. Expert Rev Cardiovasc Ther 2017;15(12):889–890. [DOI] [PubMed] [Google Scholar]
- 5.Wollmuth J 2019.https://twitter.com/jason_wollmuth/status/1139550156032897026?s=20. Twitter.
- 6.Wollmuth J, Korngold E, Croce K, Pinto D. The Single-access for Hi-risk PCI (SHiP) technique. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions 2020;96(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.D C. Twitterature. EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology 2018;14(9). [DOI] [PubMed] [Google Scholar]
- 8.Kiemeneij F Left distal transradial access in the anatomical snuffbox for coronary angiography (ldTRA) and interventions (ldTRI). EuroIntervention : journal of EuroPCR in collaboration with the Working Group on Interventional Cardiology of the European Society of Cardiology 2017;13(7). [DOI] [PubMed] [Google Scholar]
- 9.Parwani P, Choi A, Lopez-Mattei J, Raza S, Chen T, Narang A, Michos E, Erwin J, Mamas M, Gulati M. Understanding Social Media: Opportunities for Cardiovascular Medicine. Journal of the American College of Cardiology 2019;73(9). [DOI] [PubMed] [Google Scholar]
- 10.Guidance Regarding Methods for Deidentification of Protected Health Information in Accordance with the Health Insurance Portability and Accountability Act (HIPAA) Privacy Rule. https://www.hhs.gov/sites/default/files/ocr/privacy/hipaa/understanding/coveredentities/De-identification/hhs_deid_guidance.pdf. Washington, DC: Office for Civil Rights, Department of Health and Human Services. [Google Scholar]
- 11.N H. The Kardashian index: a measure of discrepant social media profile for scientists. Genome biology 2014;15(7). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Alasnag M, Mamas M, Fischman D, Brugaletta S, Safirstein J, Meier P, Kunadian V, Koltowski L, Sahni S, AlRaies C and others. View point on social media use in interventional cardiology. Open heart 2019;6(1). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Vidal-Perez R, Gómez de Diego J, Grapsa J, Fontes-Carvalho R, Gonzalez-Juanatey J. Social media in cardiology: Reasons to learn how to use it. World journal of cardiology 2019;11(10). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moss AJ, Marcus FI. Changing Times in Cardiovascular Publications: A Commentary. Am J Med 2017;130(1):11–13. [DOI] [PubMed] [Google Scholar]
- 15.Luc J, Archer M, Arora R, Bender E, Blitz A, Cooke D, Hlci T, Kidane B, Ouzounian M, Varghese T and others. Does Tweeting Improve Citations? One-Year Results from the TSSMN Prospective Randomized Trial. The Annals of thoracic surgery 2020. [DOI] [PubMed] [Google Scholar]
- 16.Widmer R, Larsen C. Call for FITs/ECs to Become Engaged With Social Media. Journal of the American College of Cardiology 2016;68(4). [DOI] [PubMed] [Google Scholar]
- 17.Baran D, Grines C, Bailey S, Burkhoff D, Hall S, Henry T, Hollenberg S, Kapur N, O’Neill W, Ornato J and others. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions 2019;94(1). [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the writing of this review article.