

Case Presentation
A 21-year–old female presented with progressive weight gain, amenorrhea, hyperpigmentation, and proximal muscle weakness for 4 years. She complained of bilateral hip joint pain for the preceding 1 year. On examination, she had discriminatory features of Cushing syndrome with proximal myopathy, easy bruising, rounded face, increased dorsocervical fat pad, thinning of skin, and hyperpigmented striae. She had severe antalgic gait, and examination of hips revealed bilateral anterior joint line tenderness with restriction of joint movement. There was no history of exogenous steroid use. Her evaluation showed an 8 am cortisol of 18.5 mcg/dL with an 11 pm cortisol of 22.1 mcg/dL. She also had unsuppressed cortisol after a post 1 mg overnight dexamethasone test (14.6 mcg/dL, normal range: <1.8 mcg/dL) and elevated adrenocorticotropin releasing hormone levels of 28.9 pg/mL (midnight 11 PM). Her 24-hour urine free cortisol was elevated (728 mcg) and high dose dexamethasone test showed more than 50% suppression (2.5 mcg/dL).The results were compatible with diagnosis of Cushing disease. Other hormonal axes were normal. Her bone biochemistry showed the following: corrected calcium, 8.9 mg/dL (normal range: 8.3-10.4 mg/dL); phosphate, 3.7 mg/dL (normal range: 2.5-4.6 mg/dL); alkaline phosphatase, 101 U/L (normal range: 40-125 U/L); and 25-hydroxy vitamin D, 23.1 ng/mL (normal range: 30-75 ng/mL). X-ray and Magnetic resonance imaging (MRI) of the hips are shown in Figure 1 A and B. MRI of the brain is shown in Figure 2.
Fig. 1.

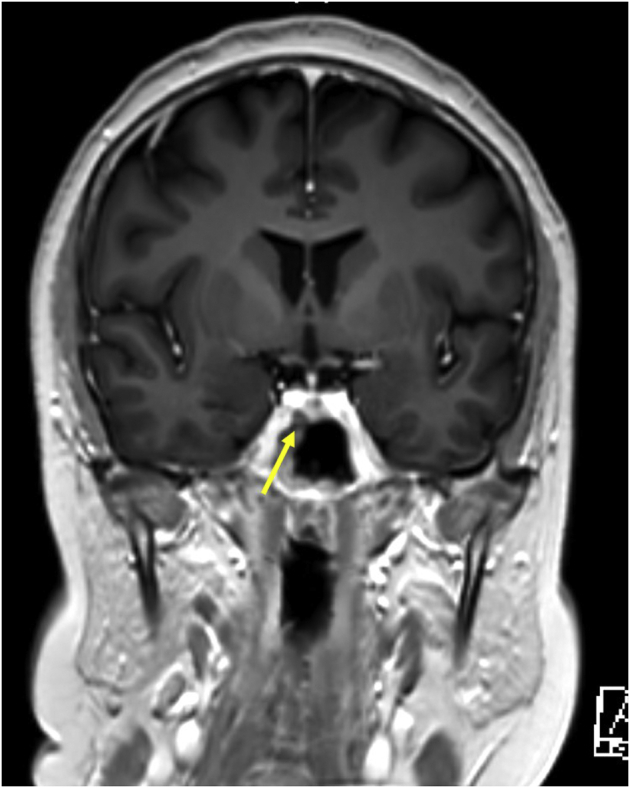
Fig. 2.
What is the diagnosis?
Answer
Bilateral avascular necrosis (AVN) of hips in Cushing disease. This patient’s hip x-ray showed ill-defined mixed sclerotic and lytic pattern of the femoral heads with cortical disruption of the round contour, typical of bilateral AVN of the hip. AVN is graded by radiologists using the Ficat classification in 4 stages, which in this patient was stage 2A on the right and stage 3 on the left. MRI of the hips showed low signal intensity in the subchondral region of the femoral necks on T1 weighted images, and MRI of the pituitary showed a hypoenhancing lesion measuring 2.5 mm × 2.5 mm, adjacent and inferior to the right cavernous internal carotid artery. She was started on medical management with ketoconazole, with which her hypercortisolemia was controlled, and was scheduled for stereotactic radiosurgery because of the proximity of the lesion to the right cavernous internal carotid artery. Expert opinion of the consultant orthopedic surgeon was sought and she was planned for total hip replacement at a later date in view of her young age. Decompression was not attempted as she had presented late with osteonecrosis and the benefit of surgery was uncertain. Bisphosphonates (parenteral zoledronate) were administered in view of low bone mass with a Z-score of −3.9 at the femoral neck and −3.5 at the lumbar spine. The prevalence of AVN of the hip following exogenous Cushing syndrome ranges between 3% and 38%.1 The Ficat classification (4 stages) is widely used for diagnosis and staging of AVN of the femoral head. Stage 1 is pain in the groin secondary to ischemia without radiographic changes. Stage 2 disease presents with radiological signs of increased density (2A) or mixed sclerotic and lytic pattern (2B). Stage 3 is characterized by disruption of the normal round contour of the femoral head, and stage 4 presents with complete collapse of the femoral head into a flattened contour, and decreased joint space.2 Bilateral AVN hip in endogenous Cushing syndrome is rare, and only few documented case reports are available to date.3 The exact mechanism of AVN in endogenous Cushing syndrome is not known. Fat-cell hypertrophy and vascular compromise, mini-fractures induced by glucocorticoids, osteocyte apoptosis, and intravascular thrombosis are the few proposed mechanisms for hip AVN.1,4 A multidisciplinary approach, with control of Cushing syndrome and orthopedic fixation is required for treatment.
Disclosure
The authors have no multiplicity of interest to disclose.
Footnotes
Editor’s Note: Submissions to “Visual Vignettes” are welcomed. Please submit online via the Journal’s Editorial Manager site.
References
- 1.Chan K.L., Mok C.C. Glucocorticoid-induced avascular bone necrosis: diagnosis and management. Open Orthop J. 2012;6:449–457. doi: 10.2174/1874325001206010449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Jawad M.U., Haleem A.A., Scully S.P. In brief: Ficat classification: avascular necrosis of the femoral head. Clin Orthop Relat Res. 2012;470(9):2636–2639. doi: 10.1007/s11999-012-2416-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ha J.S., Cho H.M., Lee H.J., Kim S.D. Bilateral avascular necrosis of the femoral head in a patient with asymptomatic adrenal incidentaloma. Hip Pelvis. 2019;31(2):120–123. doi: 10.5371/hp.2019.31.2.120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Koch C.A., Tsigos C., Patronas N.J., Papanicolaou D.A. Cushing’s disease presenting with avascular necrosis of the hip: an orthopedic emergency. J Clin Endocrinol Metab. 1999;84(9):3010–3012. doi: 10.1210/jcem.84.9.5992. [DOI] [PubMed] [Google Scholar]