

Abstract
Background
Nursing students are experiencing complex learning environments and will experience complex work environments in future clinical work, which lead to emotional problems easily. However, one’s beliefs about controlling their emotions portend a series of vital psychological outcomes. So, it is especially important to search for suitable tools to assess the emotion and regulation beliefs of nursing students and give timely intervention to improve their physical and mental health. This study aimed to translate the American version of the Emotion and Regulation Beliefs Scale (ERBS) into Chinese, revise the original scale and form a simplified version, and assess the reliability and validity of the brief Chinese version in nursing students.
Methods
The study adopted a cross-sectional design and the multistage sampling design. The ERBS was translated into Chinese, and the reliability and validity of the Chinese version were tested in 980 nursing students.
Results
The content validity index was 0.920. Exploratory factor analysis supported a three-factor model for the Chinese version of Brief-ERBS, and confirmatory factor analysis indicated that the model fit the Brief-ERBS well. Furthermore, the three-factors model was obtained by using exploratory factor analysis, explaining 51.023% variance, and the communalities of the items ranged from 0.359 to 0.680. With modified confirmatory factor analysis, the fit indices were chi-square/degree of freedom (CMIN/DF) = 4.092, goodness of fit index (GFI) = 0.949, adjusted goodness of fit index (AGFI) = 0.927, comparative fit index (CFI) = 0.913, incremental fit index (IFI) = 0.914, Tucker Lewis index (TLI) = 0.908, root-mean-square error of approximation (RMSEA) = 0.061. The two-tailed independent samples t-test showed the scores of the top (50%) and low (50%) groups reached the level of significance (P < 0.001). A highly positive correlation between the Brief-ERBS total score and the ERBS total score was found (r = 0.972, P < 0.01). The Cronbach’s α coefficient of the scale was 0.798, the split-half reliability coefficient was 0.784, and the retest coefficient was 0.879.
Conclusion
The Chinese version of Brief-ERBS has good reliability and validity, and may be used for the beliefs about emotional management in Chinese nursing students.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12912-022-00992-1.
Keywords: Emotions, Nursing, Students, Reliability, Validity
Background
Emotion regulation processes are goal-oriented behaviors functioning to modify dynamic features of emotion, such as the magnitude and duration of behavioral, experiential, and physiological responses [1, 2]. Emotion regulation refers to the processes by which we influence which emotions we have, when we have them, and how we experience and express them. It could be affected by intra- and extra-familial social factors [3], and also improved by interventions [4]. Emotion dysregulation has been linked to a variety of mental problems [5, 6], and teens with difficulty modulating emotions may be involved in more illegal activities, for poorly regulated emotions may interfere with cognitive function that reminds youth of rules during decision making [7]. Conversely, effective emotion regulation promotes mental health and is related to multiple positive mental outcomes, such as greater perceived well-being, better interpersonal relationships, and better physical health [5]. As a result, emotion regulation is crucial to successful social interactions and health and is used a lot in our daily life [8–10].
Nursing students are facing a range of pressure, such as academic pressure, interpersonal pressure, and professional pressure, which cause emotional issues easily. Nursing education involves situations where students engage in interaction with other people, learning to care for and help patients involves a variety of emotions [11]. For example, dissection and autopsies in the course of the preclinical study can provoke strong emotional reactions in some medical students [12]. The clinical placement experiences can elicit negative emotions in nursing students. However, nursing students may be unprepared for regulating their emotions [13–15]. Emotion is a key source of stress for the early career of nurses and nursing students. Developing emotional intelligence behaviors should be a very useful measure to improve academic and clinical performance [16–18], and effective emotion regulation to enhance nursing students’ professional identity and build the skills for effective patient care and their health and well-being [19, 20]. In clinical work, nurses do a lot of physical and mental work, but also pay more emotional work [21, 22]. In recent years, more and more scholars have realized the importance of nurses' physical and mental health to guarantee clinical nursing quality and stabilize nursing teams [21, 23, 24]. As future nurses, nursing students are experiencing complex learning environments and will experience complex work environments in future clinical work, which probably lead to emotional problems directly [25, 26]. However, one’s beliefs about controlling their emotions portend a series of vital psychological outcomes [27]. So, it is especially important to search for suitable tools to assess the emotion and regulation beliefs of nursing students, and give timely intervention to improve their physical and mental health [10, 27].
The Emotion and Regulation Beliefs Scale (ERBS), which was originally developed by Veilleux et al. in America, is a simple and effective tool to assess emotion and regulation belief. The ERBS assesses beliefs that emotions can hijack self-control, emotion regulation is a worthwhile pursuit, and emotions can constrain behavior. The ERBS has excellent internal consistency and powerfully predicts clinically relevant outcomes even after controlling for an existing short measure of beliefs in emotion controllability [28]. In Veilleux et al. 's study, participants were recruited from Amazon Mechanical Turk, has showed that negative beliefs about emotion are higher in individuals who would meet criteria for an eating disorder and depression, and Emotion Constraint predicts clinical groups uniquely [28].
Therefore, this study was to translate the American version of the ERBS into Chinese, revise the original scale and form a simplified version, and assess the reliability and validity of the brief Chinese version in nursing students.
Methods
Design and sample
A cross‐sectional survey was conducted from June to December 2015 in the Liaoning Province, China. The participants were nursing students in Dalian University and Jinzhou Medical University. All participants completed the tests voluntarily. Approval for the study was obtained from the College of Nursing’s Research Committee at Wannan Medical College (2,015,003). The inclusion criteria used for the participants were as follows: (i) full-time nursing student on campus; (ii) able to communicate and read; and (iii) consent to participate. Based on the criterion proposed by Kendall (10 to 20‐fold the number of items and expanded by at least 10% to ensure a sufficient sample size) [29], a sample size of at least 231 was calculated since the number of items in ERBS is 21. Finally, A total of 1087 nursing students took part in the survey, and 980 students completed the questionnaires effectively. 30 randomly selected students were invited to complete the questionnaires again two weeks later to test the reliability of the retest.
The instrument
The ERBS is a 21-item, three-factors scale, with factor one (emotion constraint, nine items), factor two (regulation worth, seven items), and factor three (Hijack, five items) [28]. Factor one represents the belief that emotions are forces that constrain or narrow an individual’s choices in an emotional situation, factor two represents the belief that emotion regulation is both possible and worthwhile, and factor three represents the belief that emotions hijack or usurp peoples’ self-control. The ERBS uses a 5-point Likert scale with response choices ranging from “very disagree” to “very agree”. The score of the scale ranges from 21 to 105. The higher the score of regulation worth represents the higher the emotion and regulation beliefs. Conversely, the higher the score of the emotion constraint and Hijack represents the weaker the emotion and regulation beliefs.
Translation procedure
Several steps were undertaken by translation guidelines [30, 31]. First, two bilingual professional translators translated the ERBS from English into Chinese. Another two bilingual professional translators translated the Chinese version back into English. Second, a bilingual expert panel consisting of four nursing experts and two psychology experts evaluated the cultural and linguistic equivalence of each item. Third, a preliminary field test was conducted on 30 nursing students with the Chinese version. According to their feedback, the ERBS was revised. The ERBS of English and Chinese versions are shown in Table 1.
Table 1.
The emotion and regulation beliefs scale (English version and Chinese version)
| Item | Item content (English/Chinese) | Score |
|---|---|---|
| Q1 | Emotions operate like a floodgate that is either open or closed. In other words, emotions are either “on” or “off.” | 1 2 3 4 5 |
| 情绪控制就像水闸门一样或开或关, 即情绪要么有, 要么没有 | ||
| Q2 | Emotions can either be expressed entirely or hidden from others-it isn’t possible to share only part of an emotional response | 1 2 3 4 5 |
| 情感只能完全表达或隐藏, 不可能同别人部分分享 | ||
| Q3 | People can learn to control/regulate their emotions | 1 2 3 4 5 |
| 人们能够学习控制或调节自己的情绪 | ||
| Q4 | People are ruled by their emotions | 1 2 3 4 5 |
| 人们被自己的情绪所左右 | ||
| Q5 | Putting forth effort to alter emotional experience is valuable | 1 2 3 4 5 |
| 努力改变情绪经历过程是值得追求的 | ||
| Q6 | When a person has a strong emotional reaction to another person, they will always feel that way about that other person | 1 2 3 4 5 |
| 当一个人对另一个人有很强的情感回应的时候, 他们通常会想法一致? | ||
| Q7 | When people are feeling down, they have to wait for a better mood to arrive before they can be productive | 1 2 3 4 5 |
| 当人们感觉情绪低落的时候, 他们必须等到情绪好的时候才能达到之前工作效率的水平 | ||
| Q8 | People would be better off if they took time to figure out where their emotions come from | 1 2 3 4 5 |
| 人们如果能知道自己情绪的出处就更好了 | ||
| Q9 | When strong emotions are present, they dictate what a person says or does | 1 2 3 4 5 |
| 当一个人强烈的情绪出现时, 这个人的语言或行为就被这种情绪所控制着 | ||
| Q10 | When an emotion comes along, it will continue unless there is a change in the environment | 1 2 3 4 5 |
| 当情绪产生时, 它会不断持续直到周围的环境发生了变化 | ||
| Q11 | When people acknowledge their emotions, the emotions will completely take them over | 1 2 3 4 5 |
| 当人们表露自己的情绪的时候, 他们完全被这种情绪所控制 | ||
| Q12 | Learning how to alter strong emotions is a worthwhile pursuit | 1 2 3 4 5 |
| 学习如何改变强烈的情绪是一个值得追求的事 | ||
| Q13 | It is possible, with effort, to alter strong feelings in any situation | 1 2 3 4 5 |
| 无论在何种情况下, 通过努力改变强烈的情绪都是可能的 | ||
| Q14 | When a person feels really angry, it’s virtually impossible to not take the anger out on people or objects nearby | 1 2 3 4 5 |
| 当一个人感到非常愤怒时, 几乎不可能不把愤怒发泄在周围的人或物上 | ||
| Q15 | People are slaves to their emotions | 1 2 3 4 5 |
| 人是情绪的奴隶 | ||
| Q16 | People would be better off if they spent more time learning how to control their emotions | 1 2 3 4 5 |
| 人们如果能花费更多的时间去学习如何控制自己的情绪就更好 | ||
| Q17 | Strong emotions will make people do things they wouldn’t normally do | 1 2 3 4 5 |
| 强烈的情绪会使人做平常不会做的事情 | ||
| Q18 | When feelings of sadness take over, a person can’t really do anything but wallow in the misery | 1 2 3 4 5 |
| 当悲伤占据一个人的情感时, 一个人除了沉溺在痛苦之中, 将无法做任何事 | ||
| Q19 | People benefit from learning how to regulate their feelings | 1 2 3 4 5 |
| 人们从如何控制自己的情绪中获益 | ||
| Q20 | It’s virtually impossible for people to act opposite to the way they feel | 1 2 3 4 5 |
| 人们实际上很难违背自己的感情行事 | ||
| Q21 | Emotions make people lose control | 1 2 3 4 5 |
| 情绪让人失控 |
Data collection
The questionnaire consisted of the Chinese version of the ERBS, as well as socio‐demographic information. The multistage sampling design was used to conduct this study. Firstly, Dalian University and Jinzhou Medical University were randomly selected from 6 nursing colleges in Liaoning Province. Secondly, 50% classes (ranging from one to three classes) in each grade were randomly selected from both universities [32], including the second batch of undergraduate, the third batch of undergraduate and higher vocational schools. As a result, a total of 39 classes were selected in the two universities. These included 24 classes in Dalian University and 15 classes in Jinzhou Medical University. Thirdly, the all of students ranged from 25 to 30 in each class were selected by cluster sampling. As a result, a total of 1125 nursing students were selected, including 694 nursing students in Dalian University and 431 nursing students in Jinzhou Medical University. The nursing students were interviewed face to face by the trained interviewers. Before data collection, 9 postgraduates in charge of the interview received unified training to learn how to use standardized language and instructions. Finally, of 1125 nursing students, a total of 1087 took part in the survey, and 980 completed the questionnaires effectively, including 640 and 340 in Dalian University and Jinzhou Medical University respectively. And the average time to finish the survey questionnaire was about 3.5 min.
Statistical analysis
SPSS 20.0 and AMOS 22.0 were used to analyze the data. Pearson’s correlation analysis was used to advise the item to be removed or not. Content validity index (CVI) was used to evaluate the content validity of the Brief-ERBS, and 5 relevant experts were invited to assess the content validity. The exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used to measure the construct validity. Discriminant validity was analyzed by using a two-tailed independent samples t-test. Convergent validity was assessed by correlation between the Brief-ERBS and the ERBS. And the reliability of the Brief-ERBS was calculated by Cronbach’s alpha, split-half reliability, item-total score correlations, and retest reliability.
Ethical considerations
All individuals have provided informed consent before the data collection. Approval for the study was obtained from the College of Nursing’s Research Committee at Wannan Medical College (2,015,003).
Results
The sample
Of the participating 980 nursing students, their ages ranged from 17 to 26 years, most of them were female (871, 88.88%). Table 2 shows the other demographic characteristics of the participators.
Table 2.
Frequency distribution of demographic characteristics (n = 980)
| Variables | Groups | N | %/‾X ± S |
|---|---|---|---|
| City | Jinzhou | 340 | 34.69 |
| Dalian | 640 | 65.31 | |
| Sex | Male | 109 | 11.12 |
| Female | 871 | 88.88 | |
| Age (years) | 17–26 | 980 | 20.55 ± 1.45 |
| Grade | Freshman | 294 | 30.00 |
| Sophomore | 412 | 42.04 | |
| Junior | 274 | 27.96 | |
| Only child | Yes | 418 | 42.65 |
| No | 562 | 57.35 | |
| Education | Higher vocational schools | 301 | 30.71 |
| The third batch of undergraduate | 183 | 18.67 | |
| The second batch of undergraduate | 496 | 50.61 |
Items analysis
In the 21-item ERBS, there was statistically significant (P < 0.001) in item-total score correlations based on Pearson correlation analysis, and correlations ranged from 0.252 to 0.596 (Table 3). Three items (Q1, Q2, and Q6) were removed for item-total score correlations less than 0.4 [33]. However, the score of Q3 (people can learn to control/regulate their emotions) had significant positive correlation with total scores, and the correlation coefficient was 0.370, which was somewhat below 0.4. And Q3 was almost important and determined that this was a belief of emotion and regulation according to experts’ advice and the cultural background in China. Therefore, Q3 was retained for further testing. Consequently, 18-item ERBS were established. In the 18-item ERBS, item-total score correlations ranging from 0.420 to 0.613 except Q3 (r = 0.377), with higher correlation coefficients than the 21-item. Based on several EFA after that, both Q14 and Q9 had a lower load value (0.269 ~ 0.318 and 0.224 ~ 0.360) than 0.40 on all common factors and was removed [33], Q16 was deleted for in the fourth factor lonely which was too little item, Q20 was deleted for belonging to the Hijack which was not in according with original scale in the emotion constraint. Finally, the Chinese version of Brief-ERBS consisting of 14 items was formed.
Table 3.
Item-total score person correlation analysis results in ERBS of 21 Items (n = 980, α = 0.05)
| Item | Item content | r | P |
|---|---|---|---|
| Q1 | Emotions operate like a floodgate that is either open or closed. In other words, emotions are either “on” or “off.” | 0.350 | < 0.001 |
| Q2 | Emotions can either be expressed entirely or hidden from others-it isn’t possible to share only part of an emotional response | 0.252 | < 0.001 |
| Q3 | People can learn to control/regulate their emotions | 0.370 | < 0.001 |
| Q4 | People are ruled by their emotions | 0.490 | < 0.001 |
| Q5 | Putting forth effort to alter emotional experience is valuable | 0.512 | < 0.001 |
| Q6 | When a person has a strong emotional reaction to another person, they will always feel that way about that other person | 0.366 | < 0.001 |
| Q7 | When people are feeling down, they have to wait for a better mood to arrive before they can be productive | 0.539 | < 0.001 |
| Q8 | People would be better off if they took time to figure out where their emotions come from | 0.536 | < 0.001 |
| Q9 | When strong emotions are present, they dictate what a person says or does | 0.574 | < 0.001 |
| Q10 | When an emotion comes along, it will continue unless there is a change in the environment | 0.490 | < 0.001 |
| Q11 | When people acknowledge their emotions, the emotions will completely take them over | 0.540 | < 0.001 |
| Q12 | Learning how to alter strong emotions is a worthwhile pursuit | 0.586 | < 0.001 |
| Q13 | It is possible, with effort, to alter strong feelings in any situation | 0.476 | < 0.001 |
| Q14 | When a person feels really angry, it’s virtually impossible to not take the anger out on people or objects nearby | 0.541 | < 0.001 |
| Q15 | People are slaves to their emotions | 0.458 | < 0.001 |
| Q16 | People would be better off if they spent more time learning how to control their emotions | 0.532 | < 0.001 |
| Q17 | Strong emotions will make people do things they wouldn’t normally do | 0.579 | < 0.001 |
| Q18 | When feelings of sadness take over, a person can’t really do anything but wallow in the misery | 0.433 | < 0.001 |
| Q19 | People benefit from learning how to regulate their feelings | 0.504 | < 0.001 |
| Q20 | It’s virtually impossible for people to act opposite to the way they feel | 0.457 | < 0.001 |
| Q21 | Emotions make people lose control | 0.596 | < 0.001 |
Validity
Content validity
The CVI of the items ranged from 0.850 to 0.930, and the CVI of the Brief-ERBS was 0.920.
Construct validity
Exploratory factor analysis
A Kaiser–Meyer–Olkin (KMO) value of 0.891 and a Bartlett spherical test value of 4740.447 (df = 210, P < 0.001) in an EFA of 21-items ERBS, showed that the factor analysis was suitable [33]. Five common factors were extracted after maximum variance rotation and explained 51.421% of the total variance (Table 4). A KMO value of 0.862 and a Bartlett spherical test value of 3147.164 (df = 91, P < 0·001) in an EFA of the Brief-ERBS, showed that the factor analysis was also suitable [33]. And three common factors were extracted by maximum variance rotation, which explained 51.023% of the total variance (Table 5).
Table 4.
Factor load and communalities of each item in ERBS of 21 Items (n = 980)
| Item | F1 | F2 | F3 | F4 | F5 | Communalities |
|---|---|---|---|---|---|---|
| Q13 | 0.748 | 0.131 | -0.058 | 0.071 | -0.020 | 0.585 |
| Q12 | 0.730 | 0.079 | 0.194 | 0.130 | 0.028 | 0.595 |
| Q16 | 0.702 | 0.231 | 0.088 | -0.101 | 0.070 | 0.569 |
| Q19 | 0.654 | -0.107 | 0.348 | 0.093 | -0.058 | 0.573 |
| Q5 | 0.592 | -0.128 | 0.224 | 0.321 | 0.102 | 0.530 |
| Q8 | 0.518 | 0.155 | 0.065 | 0.432 | -0.020 | 0.484 |
| Q18 | -0.034 | 0.678 | 0.079 | 0.042 | 0.166 | 0.496 |
| Q11 | 0.146 | 0.658 | 0.124 | 0.118 | 0.128 | 0.500 |
| Q10 | 0.006 | 0.608 | 0.089 | 0.305 | 0.139 | 0.490 |
| Q15 | 0.058 | 0.523 | 0.402 | -0.234 | 0.102 | 0.505 |
| Q20 | 0.130 | 0.498 | 0.207 | 0.136 | -0.150 | 0.349 |
| Q4 | 0.002 | 0.113 | 0.659 | 0.181 | 0.151 | 0.503 |
| Q14 | 0.300 | 0.159 | 0.574 | -0.016 | 0.055 | 0.448 |
| Q17 | 0.268 | 0.237 | 0.565 | 0.157 | -0.088 | 0.480 |
| Q21 | 0.180 | 0.497 | 0.534 | -0.054 | -0.000 | 0.567 |
| Q6 | 0.117 | 0.105 | -0.001 | 0.664 | -0.029 | 0.467 |
| Q9 | 0.085 | 0.277 | 0.438 | 0.495 | 0.018 | 0.520 |
| Q7 | 0.121 | 0.416 | 0.139 | 0.460 | 0.157 | 0.444 |
| Q3 | 0.376 | -0.357 | 0.319 | 0.414 | 0.072 | 0.548 |
| Q1 | 0.071 | 0.030 | 0.162 | 0.089 | 0.768 | 0.631 |
| Q2 | -0.014 | 0.246 | -0.052 | -0.047 | 0.739 | 0.612 |
F1 contained Q5, Q8, Q12, Q13, Q16, and Q 19, F2 contained Q10, Q11, Q15, Q18, and Q20, F3 contained Q4, Q14, Q17, and Q21, F4 contained Q3, Q7, Q6, and Q9, F5 contained Q1, and Q2
Table 5.
Factor load and communalities of each item in Brief-ERBS (n = 980)
| Item | F1 | F2 | F3 | Communalities |
|---|---|---|---|---|
| Q5 | 0.728 | 0.091 | 0.043 | 0.540 |
| Q12 | 0.722 | 0.189 | 0.104 | 0.567 |
| Q19 | 0.713 | 0.161 | -0.059 | 0.538 |
| Q3 | 0.666 | -0.036 | -0.083 | 0.452 |
| Q13 | 0.622 | 0.073 | 0.112 | 0.405 |
| Q8 | 0.579 | -0.008 | 0.356 | 0.462 |
| Q15 | -0.063 | 0.793 | 0.092 | 0.641 |
| Q21 | 0.198 | 0.672 | 0.224 | 0.540 |
| Q4 | 0.254 | 0.537 | 0.079 | 0.359 |
| Q17 | 0.402 | 0.418 | 0.169 | 0.366 |
| Q7 | 0.227 | 0.024 | 0.792 | 0.680 |
| Q10 | 0.006 | 0.281 | 0.665 | 0.521 |
| Q18 | -0.155 | 0.473 | 0.518 | 0.516 |
| Q11 | 0.055 | 0.467 | 0.502 | 0.473 |
F1 contained Q3, Q5, Q8, Q12, Q13, and Q19, F2 contained Q4, Q15, Q17, and Q21, F3 contained Q7, Q10, Q11, and Q18
Confirmatory factor analysis
With CFA, in an original three-factor model with the Brief-ERBS, the fit indices were not acceptable (Table 6 and Fig. 1). Then, modification indices were taken to improve the fit indices, and a new three-factors model was built and showed an acceptable goodness-of-fit, chi-square/degree of freedom (CMIN/DF) = 4.092, goodness of fit index (GFI) = 0.949, adjusted goodness of fit index (AGFI) = 0.927, comparative fit index (CFI) = 0.913, incremental fit index (IFI) = 0.914, Tucker Lewis index (TLI) = 0.908), root-mean-square error of approximation (RMSEA) = 0.061 (Table 6 and Fig. 2).
Table 6.
Evaluation fitness of SEM model
| Model | CMIN/DF | GFI | AGFI | NFI | RFI | IFI | TLI | CFI | PNFI | PCFI | RMSEA |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial model | 5.110 | 0.945 | 0.921 | 0.881 | 0.856 | 0.902 | 0.878 | 0.901 | 0.716 | 0.733 | 0.065 |
| Modified model | 4.092 | 0.949 | 0.927 | 0.907 | 0.900 | 0.914 | 0.908 | 0.913 | 0.716 | 0.733 | 0.061 |
| Standard value | < 5.000 | > 0.900 | > 0.900 | > 0.900 | > 0.900 | > 0.900 | > 0.900 | > 0.900 | > 0.500 | > 0.500 | < 0.08 |
Fig. 1.
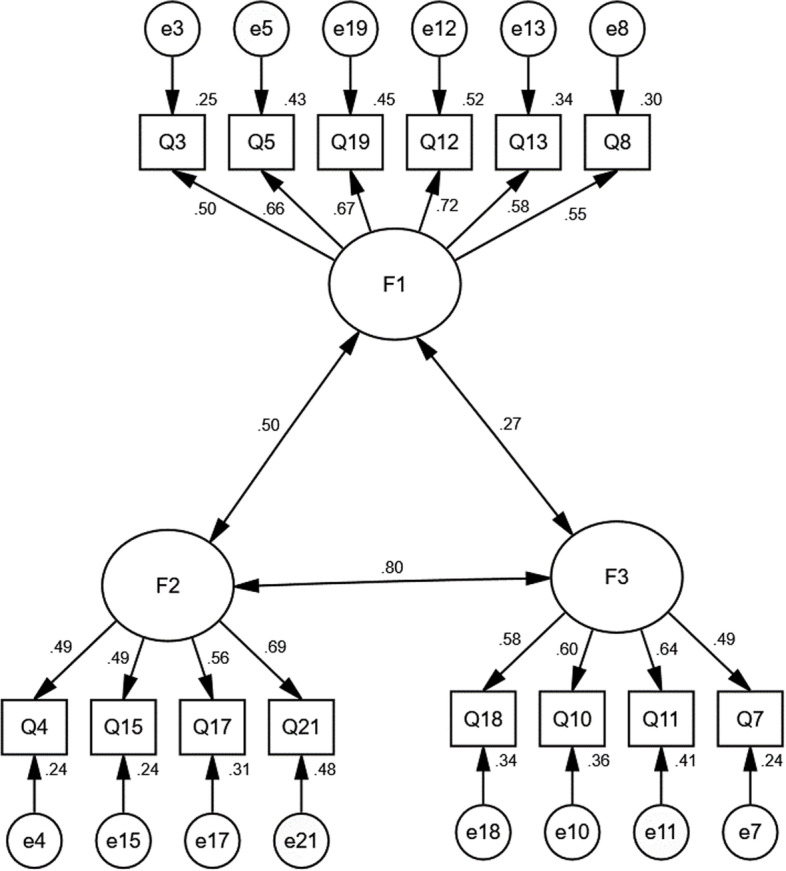
Standardized three-factors structural model of Brief-ERBS (n = 980); F1(Regulation Worth, six items), F2(Hijack, four items), and F3(Emotion Constraint, four items)
Fig. 2.

Standardized three-factors structural model of the modified Brief-ERBS (n = 980); F1(Regulation Worth, six items), F2(Hijack, four items), and F3(Emotion Constraint, four items)
Discriminant validity
In our study, the scores of each item in the top (50%) and low (50%) groups were analyzed by using a two-tailed independent samples t-test. Table 7 shows that the score difference of each item in the 2 groups reached the level of significance (P < 0.001).
Table 7.
Discriminant validity analysis in Brief-ERBS (n = 980)
| Item |
Low-score group mean ± SD |
High-score group mean ± SD |
t | P |
|---|---|---|---|---|
| Q3 | 2.99 ± 0.74 | 1.76 ± 0.43 | 32.235 | < 0.001 |
| Q4 | 3.46 ± 0.60 | 2.13 ± 0.54 | 36.550 | < 0.001 |
| Q5 | 2.96 ± 0.68 | 1.74 ± 0.44 | 33.512 | < 0.001 |
| Q7 | 3.54 ± 0.59 | 2.01 ± 0.52 | 42.921 | < 0.001 |
| Q8 | 2.93 ± 0.68 | 1.80 ± 0.40 | 32.087 | < 0.001 |
| Q10 | 3.64 ± 0.60 | 2.3 ± 0.56 | 36.161 | < 0.001 |
| Q11 | 3.66 ± 0.61 | 2.39 ± 0.58 | 33.347 | < 0.001 |
| Q12 | 2.87 ± 0.72 | 1.67 ± 0.47 | 31.029 | < 0.001 |
| Q13 | 3.07 ± 0.70 | 1.83 ± 0.37 | 34.582 | < 0.001 |
| Q15 | 4.01 ± 0.52 | 2.50 ± 0.62 | 41.172 | < 0.001 |
| Q17 | 3.04 ± 0.66 | 1.85 ± 0.36 | 35.286 | < 0.001 |
| Q18 | 4.08 ± 0.50 | 2.57 ± 0.57 | 44.154 | < 0.001 |
| Q19 | 2.83 ± 0.69 | 1.77 ± 0.42 | 28.988 | < 0.001 |
| Q21 | 3.40 ± 0.60 | 2.07 ± 0.51 | 37.260 | < 0.001 |
Convergent validity
To evaluate the convergent validity of the Brief-ERBS in the context of our study, we examined the relationship between the Brief-ERBS and the ERBS. A highly positive correlation between the Brief-ERBS total score and the ERBS total score was found (r = 0.972, P < 0.01).
Reliability
The Cronbach’s α of the Brief-ERBS was 0.798, the dimension of Regulation Worth was 0.782, the dimension of Hijack was 0.666, and the dimension of Emotion Constraint was 0.633. The split‐half reliability was 0.784. As seen in Table 8, there was a positive correlation and statistically significant (P < 0.001) in item-total score correlations, the correlations ranged from 0.400 to 0.634. The intragroup correlation coefficient was used to assess the retest reliability of the Brief-ERBS, and the retest coefficient was 0.879.
Table 8.
Item-total score person correlation analysis results in Brief-ERBS (n = 980, α = 0.05)
| Item | Item content | r | P |
|---|---|---|---|
| Q3 | People can learn to control/regulate their emotions | 0.405 | < 0.001 |
| Q4 | People are ruled by their emotions | 0.487 | < 0.001 |
| Q5 | Putting forth effort to alter emotional experience is valuable | 0.549 | < 0.001 |
| Q7 | When people are feeling down, they have to wait for a better mood to arrive before they can be productive | 0.528 | < 0.001 |
| Q8 | People would be better off if they took time to figure out where their emotions come from | 0.569 | < 0.001 |
| Q10 | When an emotion comes along, it will continue unless there is a change in the environment | 0.469 | < 0.001 |
| Q11 | When people acknowledge their emotions, the emotions will completely take them over | 0.521 | < 0.001 |
| Q12 | Learning how to alter strong emotions is a worthwhile pursuit | 0.634 | < 0.001 |
| Q13 | It is possible, with effort, to alter strong feelings in any situation | 0.525 | < 0.001 |
| Q15 | People are slaves to their emotions | 0.400 | < 0.001 |
| Q17 | Strong emotions will make people do things they wouldn’t normally do | 0.595 | < 0.001 |
| Q18 | When feelings of sadness take over, a person can’t really do anything but wallow in the misery | 0.409 | < 0.001 |
| Q19 | People benefit from learning how to regulate their feelings | 0.559 | < 0.001 |
| Q21 | Emotions make people lose control | 0.598 | < 0.001 |
Discussion
The testing results provide evidence that the Chinese version of the Brief-ERBS has good psychometric properties, and is a reliable and valid instrument. Therefore, the scale can be used for the beliefs about emotional management in Chinese nursing students.
The CVI of the items ranged from 0.850 to 0.930, and the CVI of the scale was 0.920, which indicated excellent content validity.
Construct validity was tested by EFA and CFA. The three factors the Brief-ERBS can explain 51.023% of the variation, which was significantly higher than the American version (36%), and similar to the five factors of the 21-item Chinese version (51.421%). However, the three factors (14 items) were simpler and proper than the five factors (21 items), which were simplified from the five factors (21 items) based on Pearson correlation analysis and several EFA.
Construct validity is usually assessed by factor analysis. The ideal result is that each item has a higher load value than 0.40 on one of the common factors, having a low load value on other common factors, and the cumulative variance contribution ratio of the extracted common factors is not less than 40% [34]. In the EFA model, the Brief-ERBS had three common factors, which were in accordance with the American version. In the American version, the three extracted factors accounted for only 36.00% of the total variance, and the three-factors CFA model had acceptable model fit (CMIN/DF = 1.630, CFI = 0.930, RMSEA = 0.050) [28]. However, in the Brief-ERBS, all item loads in the common factors were above 0.40, the communality of each item ranged between 0.359 and 0.680, and the total accounted for variance was 51.023%, which were highly interpretable and demonstrated excellent construct validity [33]. In the CFA, the model fit indices were evaluated by CMIN/DF < 5, GFI > 0.900, AGFI > 0.900, CFI > 0.900, IFI > 0.900, TLI > 0.900, RMSEA < 0.08 [35]. The CFA showed all measurements of the model are well fitted in our research, CMIN/DF = 4.092, GFI = 0.949, AGFI = 0.927, CFI = 0.913, IFI = 0.914, TLI = 0.908, RMSEA = 0.061. The results indicated that there is strong factor loading and interpretation variance, accord with EFA results, and have an excellent model fitting index.
For the discriminant validity, the scores of the top and low groups reached the level of significance (P < 0.001). Therefore, the discriminant validity was excellent.
As for convergent validity, a highly positive correlation between the Brief-ERBS total score and the ERBS total score was found (r = 0.972, P < 0.01), which indicate that the Brief-ERBS has excellent convergent validity.
The recommended value of Cronbach’s α coefficient is not lower than 0.60 [33]. In the Brief-ERBS, the overall Cronbach’s α coefficient was 0.798, which indicate acceptable homogeneity. The Cronbach’s α coefficient was 0.782 in the dimension of Regulation Worth, which was slightly higher than the original version. In other two dimensions, the Cronbach’s α coefficient was all somewhat less than the American version. As the number of items decreased, internal consistency decreased. The split-half reliability was 0.784. Moreover, the item-total score correlations were statistically significant, and the correlations ranged from 0.400 and 0.634, within the recommended standard (not smaller 0.4) [33]. Therefore, the homogeneity of the Brief-ERBS was acceptable. The retest coefficient was 0.879, which indicated acceptable stability.
In general, the results showed that the Brief-ERBS had good content validity, construct validity, discriminant validity, convergent validity, as well as homogeneity and stability. Therefore, the Brief-ERBS is a suitable tool for assessing Emotion and Regulation for nursing students. Furthermore, measuring the emotions may be culturally sensitive in some culture. However, emotions and regulation belief are vital psychological constructs that need to be measured as well as possible, so that researchers can well understand the impact on psychological processes, and timely intervention can be provided based on the assessment [36]. In order to increase effective response rate, the emotions and regulation belief can be collected by interviewer administered such as anonymous way and web-based surveys [37, 38]. In our study, the anonymous measures were taken and most of the participants finished the questionnaires effectively.
Limitations
A cross-sectional study was conducted in our study, so further work is needed with longitudinal research to confirm these results. The participants were nursing students in two universities of Liaoning Province, and only two schools were selected in the survey. Hence, further work is needed to expand the sample coverage and take into consideration the adaptability of different groups. However, as a result of our study, a brief self-assessment tool is available for Chinese nursing undergraduate students to evaluate Emotion and Regulation belief.
Conclusion
The study examined the psychometric properties of the Brief-ERBS in Chinese nursing students and showed good validity and reliability of the scale. The content and structure are simple, the evaluation method is flexible, and may be used for the beliefs about emotional management in Chinese nursing students.
Supplementary Information
Acknowledgements
We express our great gratitude to the participants in the study.
Abbreviations
- ERBS
Emotion and Regulation Beliefs Scale
- Brief-ERBS
The Chinese version of Emotion and Regulation Beliefs Scale consisting of 14 items
- CVI
Content validity index
- EFA
Exploratory factor analysis
- CFA
Confirmatory factor analysis
- KMO
Kaiser–Meyer–Olkin
- CMIN/DF
Chi-square/degree of freedom
- GFI
Goodness of fit index
- AGFI
Adjusted goodness of fit index
- CFI
Comparative fit index
- IFI
Incremental fit index
- TLI
Tucker Lewis index
- RMSEA
Root-mean-square error of approximation
Authors’ contributions
Conceived and designed the research: LZ. Wrote the paper: D-m Z. Analyzed the data: LZ and D-m Z. Revised the paper: LZ, D-m Z, LY, C-z W, TY, H–h W, JL, Y-x L, LS, X-p L, YH, M-m L, and H-y L. The authors read and approved the final manuscript.
Funding
This study was funded by Anhui Education Department Foundation, PR China (SK2020A0367 and 2020jyxm2084); Wannan Medical College Foundation for Teaching Research Project, PR China (2019jyxm50).
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available to preserve anonymity of the respondents but are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
All individuals have provided informed consent before the data collection. Participating students were promised that the information provided would remain anonymous. Approval for the study was obtained from the College of Nursing’s Research Committee at Wannan Medical College (2015003), and all methods were performed in accordance with the relevant guidelines and regulations.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflicts of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Haiyang Liu and Lin Zhang contributed equally to this work.
Contributor Information
Dongmei Zhang, Email: dongmei.0715@163.com.
Liu Yang, Email: zqzqylyl5858@163.com.
Congzhi Wang, Email: 289957420@qq.com.
Ting Yuan, Email: yuanting@wnmc.edu.cn.
Huanhuan Wei, Email: whh0702@163.com.
Jing Li, Email: 475366616@qq.com.
Yunxiao Lei, Email: lyxheart@163.com.
Lu Sun, Email: 565196200@qq.com.
Xiaoping Li, Email: 349274808@qq.com.
Ying Hua, Email: 1542997737@qq.com.
Mingming Liu, Email: 672388457@qq.com.
Haiyang Liu, Email: liuhaiyang85@163.com.
Lin Zhang, Email: yaoran2008@163.com.
References
- 1.Thompson RA. Emotion regulation: a theme in search of definition. Monogr Soc Res Child Dev. 1994;59(2–3):25–52. doi: 10.1111/j.1540-5834.1994.tb01276.x. [DOI] [PubMed] [Google Scholar]
- 2.Christiansen H, Hirsch O, Albrecht B, Chavanon ML. Attention-Deficit/Hyperactivity Disorder (ADHD) and Emotion Regulation Over the Life Span. Curr Psychiatry Rep. 2019;21(3):17. doi: 10.1007/s11920-019-1003-6. [DOI] [PubMed] [Google Scholar]
- 3.Cole PM, AshanaRamsook K, Ram N. Emotion dysregulation as a dynamic process. Dev Psychopathol. 2019;31(3):1191–1201. doi: 10.1017/S0954579419000695. [DOI] [PubMed] [Google Scholar]
- 4.Andreescu C, Sheu LK, Tudorascu D, Gross JJ, Walker S, Banihashemi L, et al. Emotion reactivity and regulation in late-life generalized anxiety disorder: functional connectivity at baseline and post-treatment. Am J Geriatr Psychiatry. 2015;23(2):200–214. doi: 10.1016/j.jagp.2014.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kneeland ET, Dovidio JF, Joormann J, Clark MS. Emotion malleability beliefs, emotion regulation, and psychopathology: Integrating affective and clinical science. Clin Psychol Rev. 2016;45:81–88. doi: 10.1016/j.cpr.2016.03.008. [DOI] [PubMed] [Google Scholar]
- 6.Calkins SD, Dollar JM, Wideman L. Temperamental vulnerability to emotion dysregulation and risk for mental and physical health challenges. Dev Psychopathol. 2019;31(3):957–970. doi: 10.1017/S0954579419000415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kemp K, Thamotharan S, Poindexter B, Barker D, Tolou-Shams M, Houck CD. EMOTION REGULATION AS A PREDICTOR OF JUVENILE ARREST. Crim Justice Behav. 2017;44(7):912–926. doi: 10.1177/0093854817695842. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gyurak A, Goodkind MS, Kramer JH, Miller BL, Levenson RW. Executive functions and the down-regulation and up-regulation of emotion. Cogn Emot. 2012;26(1):103–118. doi: 10.1080/02699931.2011.557291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gross JJ. Emotion regulation: taking stock and moving forward. Emotion. 2013;13(3):359–365. doi: 10.1037/a0032135. [DOI] [PubMed] [Google Scholar]
- 10.DeSteno D, Gross JJ, Kubzansky L. Affective science and health: the importance of emotion and emotion regulation. Health Psychol. 2013;32(5):474–486. doi: 10.1037/a0030259. [DOI] [PubMed] [Google Scholar]
- 11.Weurlander M, Lonn A, Seeberger A, Broberger E, Hult H, Wernerson A. How do medical and nursing students experience emotional challenges during clinical placements? Int J Med Educ. 2018;9:74–82. doi: 10.5116/ijme.5a88.1f80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tseng WT, Lin YP. "Detached concern" of medical students in a cadaver dissection course: A phenomenological study. Anat Sci Educ. 2016;9(3):265–271. doi: 10.1002/ase.1579. [DOI] [PubMed] [Google Scholar]
- 13.McCloughen A, Levy D, Johnson A, Nguyen H, McKenzie H. Nursing students' socialisation to emotion management during early clinical placement experiences: A qualitative study. J Clin Nurs. 2020;29(13–14):2508–2520. doi: 10.1111/jocn.15270. [DOI] [PubMed] [Google Scholar]
- 14.Edo-Gual M, Tomás-Sábado J, Bardallo-Porras D, Monforte-Royo C. The impact of death and dying on nursing students: an explanatory model. J Clin Nurs. 2014;23(23–24):3501–3512. doi: 10.1111/jocn.12602. [DOI] [PubMed] [Google Scholar]
- 15.Jack K, Wibberley C. The meaning of emotion work to student nurses: a Heideggerian analysis. Int J Nurs Stud. 2014;51(6):900–907. doi: 10.1016/j.ijnurstu.2013.10.009. [DOI] [PubMed] [Google Scholar]
- 16.Birks Y, McKendree J, Watt I. Emotional intelligence and perceived stress in healthcare students: a multi-institutional, multi-professional survey. BMC Med Educ. 2009;9:61. doi: 10.1186/1472-6920-9-61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Cherry MG, Fletcher I, O'Sullivan H, Dornan T. Emotional intelligence in medical education: a critical review. Med Educ. 2014;48(5):468–478. doi: 10.1111/medu.12406. [DOI] [PubMed] [Google Scholar]
- 18.McCloughen A, Foster K. Nursing and pharmacy students' use of emotionally intelligent behaviours to manage challenging interpersonal situations with staff during clinical placement: A qualitative study. J Clin Nurs. 2018;27(13–14):2699–2709. doi: 10.1111/jocn.13865. [DOI] [PubMed] [Google Scholar]
- 19.Lewis GM, Neville C, Ashkanasy NM. Emotional intelligence and affective events in nurse education: A narrative review. Nurse Educ Today. 2017;53:34–40. doi: 10.1016/j.nedt.2017.04.001. [DOI] [PubMed] [Google Scholar]
- 20.Saedpanah D, Salehi S, Moghaddam LF. The Effect of Emotion Regulation Training on Occupational Stress of Critical Care Nurses. J Clin Diagn Res. 2016;10(12):Vc01–vc4. doi: 10.7860/JCDR/2016/23693.9042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Foster K, Roche M, Giandinoto JA. Workplace stressors, psychological well-being, resilience, and caring behaviours of mental health nurses: A descriptive correlational study. Int J Ment Health Nurs. 2020;29(1):56–68. doi: 10.1111/inm.12610. [DOI] [PubMed] [Google Scholar]
- 22.Rouxel G, Michinov E, Dodeler V. The influence of work characteristics, emotional display rules and affectivity on burnout and job satisfaction: A survey among geriatric care workers. Int J Nurs Stud. 2016;62:81–89. doi: 10.1016/j.ijnurstu.2016.07.010. [DOI] [PubMed] [Google Scholar]
- 23.Peng YN, Liu CY, Zhang H, Zhang N, Cao Y, Wu YY. Psychological health of nurses in operating room participating in organ donation and intervention effect. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. 2020;38(4):271–274. doi: 10.3760/cma.j.cn121094-20190521-00207. [DOI] [PubMed] [Google Scholar]
- 24.Glasofer A, Townsend AB. Supporting nurses' mental health during the pandemic. Nursing. 2020;50(10):60–63. doi: 10.1097/01.NURSE.0000697156.46992.b2. [DOI] [PubMed] [Google Scholar]
- 25.Sun N, Wei L, Shi S, Jiao D, Song R, Ma L, et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am J Infect Control. 2020;48(6):592–598. doi: 10.1016/j.ajic.2020.03.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Khalaf IA, Al-Dweik G, Abu-Snieneh H, Al-Daken L, Musallam RM, BaniYounis M, et al. Nurses' Experiences of Grief Following Patient Death: A Qualitative Approach. J Holist Nurs. 2018;36(3):228–240. doi: 10.1177/0898010117720341. [DOI] [PubMed] [Google Scholar]
- 27.De Castella K, Platow MJ, Tamir M, Gross JJ. Beliefs about emotion: implications for avoidance-based emotion regulation and psychological health. Cogn Emot. 2018;32(4):773–795. doi: 10.1080/02699931.2017.1353485. [DOI] [PubMed] [Google Scholar]
- 28.Veilleux JC, Salomaa AC, Shaver JA, Zielinski MJ, Pollert GA. Multidimensional assessment of beliefs about emotion: development and validation of the emotion and regulation beliefs scale. Assessment. 2015;22(1):86–100. doi: 10.1177/1073191114534883. [DOI] [PubMed] [Google Scholar]
- 29.Fang JQ, Lu Y. Advanced Medical Statistics. Beijing, China: People's Medical Publishing House; 2002. [Google Scholar]
- 30.Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191. doi: 10.1097/00007632-200012150-00014. [DOI] [PubMed] [Google Scholar]
- 31.Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):S80–S89. doi: 10.4103/sja.SJA_203_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Fang DM, Gao Y, Dai B, Zhou M, Li J. Application of different statistical sampling methods in prescription evaluation. China Pharmacy. 2011;22(13):1240-1.
- 33.Wu ML. Questionnaire statistical analysis practice. Chongqing, China: Chongqing University Press; 2010. [Google Scholar]
- 34.Liu K. The Application of SPSS in Medical Scientific Research. Beijing, China: People’s Medical Publishing House; 2012. [Google Scholar]
- 35.Wu ML. Structural Equation Modeling. Chongqing, China: Chongqing University Press; 2010. [Google Scholar]
- 36.Harmon-Jones C, Bastian B, Harmon-Jones E. The Discrete Emotions Questionnaire: A New Tool for Measuring State Self-Reported Emotions. PLoS ONE. 2016;11(8):e0159915. doi: 10.1371/journal.pone.0159915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zannette AU, Chantay MD. Sensitive topics: Are there model differences. Comput Hum Behav. 2009;25:76–87. doi: 10.1016/j.chb.2008.06.007. [DOI] [Google Scholar]
- 38.Thompson LF, Surface EA, Martin DL, Sanders MG. From paper to pixels: Moving personnel surveys to web. Pers Psychol. 2003;56(1):197–227. doi: 10.1111/j.1744-6570.2003.tb00149.x. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available to preserve anonymity of the respondents but are available from the corresponding author on reasonable request.