

A 46-year-old patient presented for the evaluation of a gonadotropin deficiency suspicion. The endocrinologic evaluation revealed – no pituitary deficiency. The pituitary MRI identified an incidental enlargement of the pituitary stalk with a diameter of 4.55mm, with hyperintense signal on T1W images with no contrast enhancement and without involvement of the optic chiasm (Fig. 1 A-D). The pituitary gland shows normal size, signal intensity and normal contrast enhancement, with a reduced pituitary bright spot located postero-inferiorly.
Figure 1.
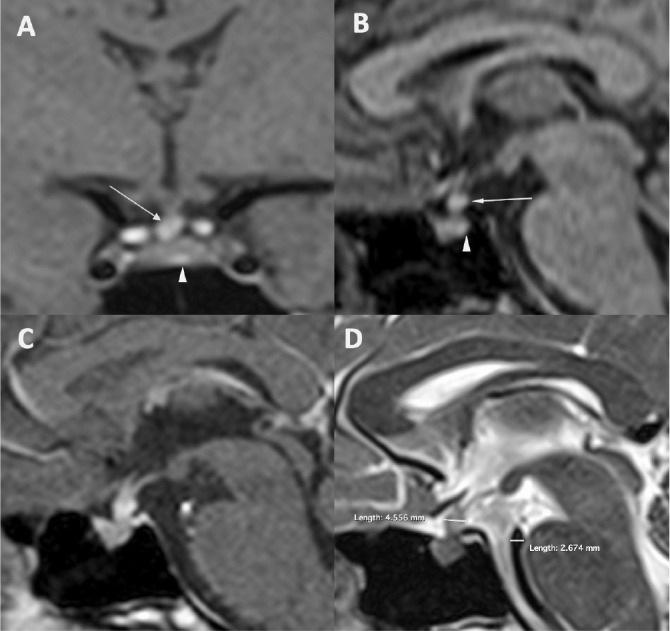
Pituitary bright stalk. Non enhanced Coronal T1W (A) and Sagittal T1W (B) showing the hyperintense and enlarged pituitary stalk (arrow) and the reduced pituitary bright spot (arrow head). C Sagittal T1W with contrast enhancement showing no pathological enhancement at the level of the pituitary region, D Sagittal T2W showing the diameters of the pituitary stalk and basilar artery.
The images are suggestive for accumulation of the vasopressin vesicles at the level of the pituitary stalk, phenomenon known as damming-up effect (1). Normally the pituitary stalk has a low to intermediate signal intensity on T1W images (hypointense relative to optic chiasm) and a diameter no greater than the basilary artery. This phenomenon is due to altered axonal transport of the ADH secretory vesicles and their accumulation at the level of the pituitary stalk. The damming-up effect appears mostly in the setting of a compressive pituitary pathology but idiopathic cases are being reported in the literature.
Differential diagnosis has to be made mainly with ectopic posterior lobe – in this case there is no pituitary bright spot at the level of the sella and most of the time is associated with isolated GH deficiency (2), and post-traumatic pituitary stalk transection – associate symptoms of pituitary insufficiency after severe traumatic brain injury or surgery (3).
Main features of this condition are – normal pituitary function with no DI and hyperintense pituitary stalk on T1 sequences with the presence of pituitary bright spot, although with reduced size.
There is no indication of treatment for this particular condition and there are no definitive recommendations for follow-up, although periodic imaging and endocrine evaluation would appear reasonable (Fig. 2).
Figure 2.
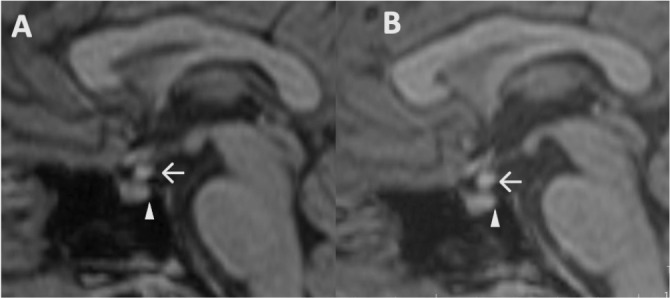
Comparative study. (A) Non enhanced MRI Sagittal T1W showing hyperintense bright stalk (arrow) and the posterior pituitary bright spot (arrowhead in 2018) and the same aspect in 2022 (B).
Conflict of interest
The authors declare that they have no conflict of interest.
References
- 1.Fujisawa I, Uokawa K, Horii N, Murakami N, Azuma N, Furuto-Kato S, Yamashita K, Nakao S, Kageyama N. Bright pituitary stalk on MR T1-weighted image: damming up phenomenon of the neurosecretory granules. Endocr J. 2002;49(2):165–173. doi: 10.1507/endocrj.49.165. [DOI] [PubMed] [Google Scholar]
- 2.Lahiri AK, Sundareyan R, Jenkins D, Nilak A. MRI of ectopic posterior pituitary gland with dysgenesis of pituitary stalk in a patient with hypogonadotropic hypogonadism. Radiol Case Rep. 2018;13(4):764–766. doi: 10.1016/j.radcr.2018.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zada G, Lopes MBS, Mukundan S, Laws E. Traumatic Injury of the Sellar Region, Pituitary Stalk Disruption, and Posttraumatic Anosmia. In: Zada G, Lopes M, Mukundan JrS, Laws JrE, editors. Atlas of Sellar and Parasellar Lesions. Springer, Cham; 2016. [Google Scholar]