

Abstract
Introduction International studies on preterm birth rates during COVID-19 lockdowns report different results. This study examines preterm birth rates during lockdown periods and the impact of the mobility changes of the population in Bavaria, Germany.
Material and Methods This is a secondary analysis of centrally collected data on preterm births in Bavaria from 2010 to 2020. Preterm births (< 37 weeks) in singleton and twin pregnancies during two lockdowns were compared with corresponding periods in 2010 – 2019. Fisherʼs exact test was used to compare raw prevalence between groups. Potential effects of two fixed lockdown periods and of variable changes in population mobility on preterm birth rates in 2020 were examined using additive logistic regression models, adjusting for long-term and seasonal trends.
Results Unadjusted preterm birth rates in 2020 were significantly lower for singleton pregnancies during the two lockdown periods (Lockdown 1: 5.71% vs. 6.41%; OR 0.88; p < 0.001; Lockdown 2: 5.71% vs. 6.60%; OR = 0.86; p < 0.001). However, these effects could not be confirmed after adjusting for long-term trends (Lockdown 1: adj. OR = 0.99; p = 0.73; Lockdown 2: adj. OR = 0.96; p = 0.24). For twin pregnancies, differences during lockdown were less marked (Lockdown 1: 52.99% vs. 56.26%; OR = 0.88; p = 0.15; Lockdown 2: 58.06% vs. 58.91%; OR = 0.97; p = 0.70). Reduced population mobility had no significant impact on preterm birth rates in singleton pregnancies (p = 0.14) but did have an impact on twin pregnancies (p = 0.02).
Conclusions Reduced preterm birth rates during both lockdown periods in 2020 were observed for singleton and twin pregnancies. However, these effects are reduced when adjusting for long-term and seasonal trends. Reduced population mobility was associated with lower preterm birth rates in twin pregnancies.
Key words: COVID-19, SARS-CoV-2, preterm birth, lockdown measures, preterm delivery
Zusammenfassung
Einleitung Internationale Studien zu Frühgeburtenraten während den COVID-19-Lockdowns kommen zu unterschiedlichen Ergebnissen. Diese Studie untersucht die Frühgeburtenraten während den Lockdowns sowie die Auswirkungen von Änderungen der Bevölkerungsmobilität in Bayern auf die Frühgeburtenraten.
Material und Methoden Es handelt sich um eine Sekundäranalyse von zentral erhobenen Daten zu Frühgeburten in Bayern zwischen 2010 und 2020. Die Frühgeburten (< 37. Schwangerschaftswoche) bei Einlings- und Zwillingsschwangerschaften, die in der Zeit der beiden Lockdowns auftraten, wurden den Frühgeburten in den Vergleichszeiträume der Jahre 2010 – 2019 gegenübergestellt. Die Rohprävalenzen der Gruppen wurden mit dem exakten Test nach Fisher verglichen. Additive logistische Regressionsmodelle wurden eingesetzt, um die potenziellen Auswirkungen von 2 Lockdowns sowie von Änderungen der Bevölkerungsmobilität auf die Frühgeburtenraten im Jahre 2020 zu untersuchen. Die Effekte wurden dann zusätzlich auf langfristige und saisonbedingte Trends adjustiert.
Ergebnisse Die unbereinigten Frühgeburtenraten von Einlingsschwangerschaften während den 2 Lockdowns im Jahre 2020 waren signifikant niedriger (Lockdown 1: 5,71% vs. 6,41%; OR 0,88; p < 0,001; Lockdown 2: 5,71% vs. 6,60%; OR = 0,86; p < 0,001). Nachdem die Effekte auf langfristige und saisonbedingte Trends adjustiert worden waren, konnten die Auswirkungen aber nicht bestätigt werden (Lockdown 1: ber. OR = 0,99; p = 0,73; Lockdown 2: ber. OR = 0,96; p = 0,24). Die Unterschiede während der Lockdownzeiträume waren bei Zwillingsschwangerschaften weniger ausgeprägt (Lockdown 1: 52,99% vs. 56,26%; OR = 0,88; p = 0,15; Lockdown 2: 58,06% vs. 58,91%; OR = 0,97; p = 0,70). Eine geringere Bevölkerungsmobilität hatte keine signifikanten Auswirkungen auf die Frühgeburtenraten bei Einlingsschwangerschaften (p = 0,14), dafür aber auf die Frühgeburtenraten bei Zwillingsschwangerschaften (p = 0,02).
Schlussfolgerungen Es wurden niedrigere Frühgeburtenraten bei Einlings- und Zwillingsschwangerschaften während den beiden Lockdowns im Jahre 2020 beobachtet. Diese Effekte wurden teilweise gemindert, wenn sie auf langfristige und saisonale Trends adjustiert wurden. Die geringere Bevölkerungsmobilität war mit einer niedrigeren Frühgeburtenrate bei Zwillingsschwangerschaften assoziiert.
Schlüsselwörter: COVID-19, SARS-CoV-2, Frühgeburt, Lockdown-Maßnahmen
Introduction
In the context of the SARS-CoV-2 pandemic, countries around the world have implemented different measures to reduce the incidence of SARS-CoV-2 infection. Initially, obstetricians were concerned about the possible consequences of SARS-CoV-2 infection during pregnancy 1 , 2 . Furthermore, it was assumed that the quality of antenatal care would decline as a result of mandatory contact reductions. These worries were initially supported by studies showing an increase in preterm births and stillbirths 3 , 4 , 5 .
In contrast, studies from Ireland and Denmark demonstrated a decrease in preterm birth rates as well as in the numbers of very low birth weight (VLBW) and extremely low birth weight (ELBW) neonates during defined lockdown periods 6 , 7 . These studies, both with small sample numbers, were complemented by a study from the Netherlands 8 based on data from approximately 1.6 million newborns. This study also demonstrated a reduction in preterm births during the lockdown period. Since the publication of these data, it has been discussed whether this is a coincidence or if a causal relationship could exist. A meta-analysis demonstrated that in high-income countries a moderate reduction in preterm birth rates was achieved by infection control measures.
However, the studies published so far have some limitations. It has not yet been investigated to what extent there might be a relationship between a reduction in population mobility and the risk of preterm birth. Population mobility might offer a better representation of the coherence of the population with regard to nonpharmacologic interventions rather than assuming homogeneous effects during complete lockdown periods 9 . Hence, the main hypothesis of our study was that the risk of preterm birth diminishes with decreasing population mobility. Furthermore, we hypothesized that some of the observed effects in 2020 might be confounded by an overall long-term trend towards a reduction in preterm births. Additionally, there is a lack of studies that have investigated these effects in twin pregnancies, which typically are associated with a higher overall risk of preterm birth.
Therefore, the aim of the present study was to investigate whether an association between lockdown measures or a lockdown-induced reduction in population mobility and preterm birth rates can be demonstrated based in a large full cohort (all births from 2010 to 2020) from Bavaria while also adjusting for long-term trends.
Material and Methods
Setting
Due to increasing numbers of infections, a number of measures were prescribed by law in 2020 to reduce the incidence of SARS-CoV-2. Starting from March 16th, the Bavarian government urged the population to reduce their social contacts to a minimum and to practice hygiene measures. After a decrease in infection rates, gradual opening up with a lessening of restrictions on social activities was permitted from April 20th while the general hygiene measures remained in force. The first lockdown ended on May 6th, 2020 with the end of the curfew for the Bavarian population.
After a new rise in the number of infections, contact restrictions were introduced again from November 2nd. These measures were tightened as infection rates remained high and were maintained until the end of 2020 ( Fig. 1 , 10 ). The most relevant Bavarian measures are shown in Fig. 2 .
Fig. 1.
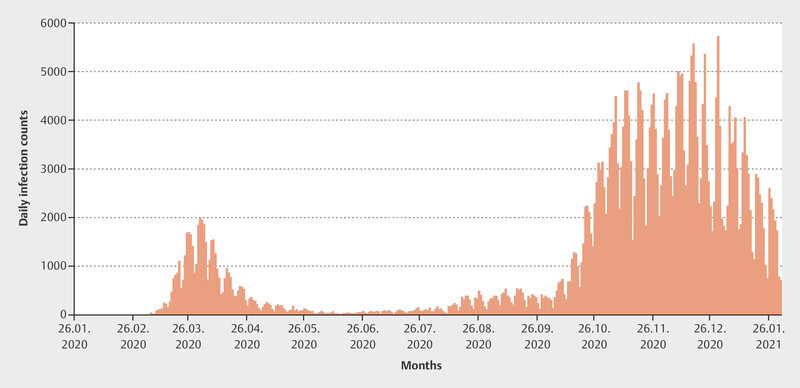
Daily reported counts of SARS-CoV-2 infections in Bavaria from January 2020 to January 2021 (data from: 10 ).
Fig. 2.
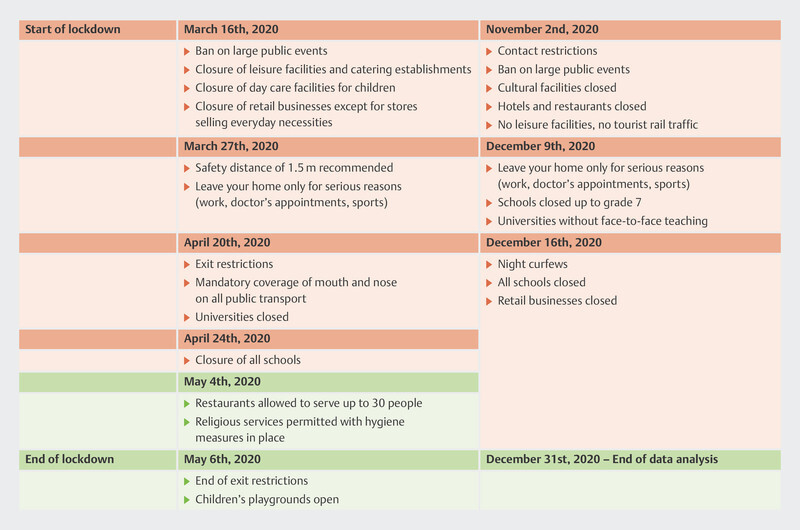
Infection control measures from March – May and November – December 2020 in Bavaria. Red: tightened measures; green: lightened measures.
Study population and examined lockdown periods
In Germany, it is mandatory to report specific fixed parameters for all births to the Institute for Quality Assurance and Transparency in Healthcare (IQTIG). In Bavaria, the Bavarian Institute for Quality Assurance (BAQ) accepts these obstetric quality data and forwards them to IQTIG. For this study, Bavariaʼs centrally collected obstetric data were made available by the BAQ in anonymized form for a secondary analysis of singleton and twin births.
Study cohorts
Deliveries during the lockdown periods in 2020 constituted the study group, while births from 2010 to 2019 represent the historical cohort. The study specifically focused on births during the defined Bavarian lockdown periods (Lockdown 1 from March 16th, 2020 to May 6th, 2020; Lockdown 2 from November 2nd, 2020 to December 31st, 2020). According to gestational age at delivery (weeks + days), the analyzed population was divided into term deliveries and preterm births as follows:
term births (≥ 37 + 0 weeks of gestation)
preterm births (< 37 + 0 weeks of gestation)
Preterm births were additionally divided into subgroups as follows:
preterm births with delivery < 32 + 0 weeks of gestation
preterm births with delivery < 28 + 0 weeks of gestation
In addition, the frequency of the two different subgroups according to birth weight was included in the analysis:
very low birthweight (VLBW, < 1500 g)
extremely low birthweight (ELBW, < 1000 g)
Singleton and twin pregnancies were analyzed separately. Higher-order multiple pregnancies were excluded from the analysis.
Mobility patterns in Bavaria
In addition to the two lockdown periods, we investigated the general impact of population mobility in 2020 on preterm births compared to 2019.
For this purpose, anonymized phone data of two large mobile phone providers (Deutsche Telekom, Telefónica) were analyzed. The exact procedure is described in the COVID-19 Mobility Project 11 . Briefly summarized, mobility is defined as a change in the mobile cell to which the mobile phone is logged on. This technique allows structural changes in population mobility to be identified.
Statistical analysis
Descriptive statistics of preterm births are presented for both singleton and twin births as numbers and percentages. To explore the effects of lockdown measures on preterm birth rates in a first univariate analysis, Fisherʼs exact test was used to compare raw prevalence during lockdown periods compared to equivalent periods from 2010 to 2019.
In the multivariable analysis, the risk of preterm birth was modeled for the overall sample from 2010 to 2020 using generalized additive regression models 12 , adjusting for seasonal and long-term trends. More precisely, penalized splines were incorporated in logistic regression models to account for non-linear long-term trends (year), seasonal trends (cyclic spline for calendar week) and weekly patterns (cyclic spline for weekday) while estimating the potential effects of the lockdown periods (binary explanatory variables) or mobility change (continuous explanatory variable) in the year 2020. To explore these effects further, similar additive regression models were also fitted for gestational age and birthweight as continuous outcomes. All statistical analyses were performed using the statistical computing environment R (Version 4.1.2) with corresponding add-on packages for the additive regression models 13 .
Ethical approval
Since this was a secondary analysis of centrally collected anonymized data, no ethics vote was required for this study.
Results
Overall collective and examined study periods
In total, the overall study period included 1 263 959 births in Bavaria, Germany from 2010 to 2020. Of these, 1 217 442 (96.32%) were singleton births, 45 211 (3.58%) were twin births and 1302 (0.10%) were higher-order pregnancies. In 2020, a total of 125 089 births were reported, of which 120 669 (96.47%) were singleton pregnancies, 4296 (3.43%) were twin pregnancies and the remaining 124 (0.10%) pregnancies were higher-order pregnancies.
Preterm birth rates between 2010 and 2020
Annual birth counts and their corresponding preterm birth rates between 2010 and 2020 are shown in Table 1 . Over the years, the tendency to preterm births has decreased in Bavaria.
Table 1 Bavarian (preterm) birth rates from 2010 to 2020.
| 2020 | 2019 | 2018 | 2017 | 2016 | 2015 | 2014 | 2013 | 2012 | 2011 | 2010 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| n: case numbers, wks: weeks of gestation | |||||||||||
| Singleton births, n | 120 669 | 120 057 | 118 969 | 119 425 | 115 664 | 112 240 | 107 653 | 103 567 | 101 890 | 98 292 | 99 036 |
| Preterm births, < 37 + 0 wks | 6 787 | 7 203 | 7 101 | 7 316 | 7 246 | 7 185 | 7 002 | 6 796 | 6 718 | 6 572 | 6 609 |
| Preterm birth rate, % | 5.62 | 6.00 | 5.97 | 6.13 | 6.27 | 6.40 | 6.50 | 6.56 | 6.59 | 6.69 | 6.67 |
| Twin births, n | 4 296 | 4 426 | 4 318 | 4 451 | 4 371 | 4 260 | 4 252 | 3 966 | 3 638 | 3 571 | 3 662 |
| Preterm births, < 37 + 0 wks | 2 361 | 2 521 | 2 396 | 2 513 | 2 507 | 2 523 | 2 376 | 2 274 | 2 176 | 2 169 | 2 245 |
| Preterm birth rate, % | 54.96 | 56.96 | 55.49 | 56.46 | 57.36 | 59.23 | 55.88 | 57.34 | 59.81 | 60.74 | 61.31 |
Lockdown periods and preterm birth
In total, there were 361 737 preterm births during the studied periods (35 333 in the actual lockdown periods and 326 404 in the corresponding periods between 2010 and 2019), and they were included in our univariate analysis. Numbers of deliveries for each studied period are shown in Table 2 .
Table 2 Preterm birth rates during both lockdown periods in 2020 compared to 2010 – 2019.
| 2010 – 2019 | 2020 | Raw OR | p value | Adj. OR | Adj. p value | |
|---|---|---|---|---|---|---|
| n (%) | n (%) | |||||
|
n: case numbers, %: percentage, wks: weeks of gestation, VLBW: very low birth weight (< 1500 g), ELBW: extremely low birth weight (< 1000 g),
‡
p < 0.05.
Raw odds ratio (OR) refers to deliveries during the lockdown periods in 2020 compared to the corresponding periods in 2010 – 2019, the adjusted OR takes all births from 2010 to 2020 into account and was adjusted for non-linear long-term trends, seasonality and weekday effects. | ||||||
|
Lockdown period I
March 16th to May 5th | ||||||
| Total number of singleton births during Lockdown | 145 018 | 16 015 | ||||
| Number of singleton preterm births, n (%) | 9 295 (6.41) | 914 (5.71) | 0.88 | < 0.001 ‡ | 0.99 | 0.73 |
| < 32 + 0 wks | 1 312 (0.9) | 115 (0.72) | 0.79 | 0.02 ‡ | 0.82 | 0.04 ‡ |
| < 28 + 0 wks | 477 (0.33) | 50 (0.31) | 0.94 | 0.77 | 0.96 | 0.81 |
| VLWB | 1 190 (0.82) | 110 (0.69) | 0.84 | 0.08 | 0.84 | 0.09 |
| ELBW | 548 (0.38) | 47 (0.29) | 0.78 | 0.10 | 0.79 | 0.13 |
| Total number of twin births during Lockdown, n | 5 649 | 551 | ||||
| Twin preterm births, n (%) | 3 195 (56.26) | 292 (52.99) | 0.88 | 0.15 | 0.91 | 0.31 |
| < 32 + 0 wks | 593 (10.44) | 51 (9.26) | 0.87 | 0.42 | 0.95 | 0.77 |
| < 28 + 0 wks | 186 (3.28) | 18 (3.27) | 1.00 | 1.00 | 1.24 | 0.42 |
| VLWB | 545 (9.60) | 51 (9.26) | 0.96 | 0.88 | 1.06 | 0.71 |
| ELBW | 207 (3.65) | 17 (3.09) | 0.84 | 0.63 | 1.09 | 0.74 |
|
Lockdown period II
November 2nd to December 31st | ||||||
| Total number of singleton births during Lockdown | 168 989 | 18 159 | ||||
| Number of singleton preterm births, n (%) | 11 156 (6.60) | 1 037 (5.71) | 0.86 | < 0.001 ‡ | 0.96 | 0.24 |
| < 32 + 0 wks | 1 550 (0.92) | 172 (4.83) | 1.03 | 0.68 | 1.10 | 0.24 |
| < 28 + 0 wks | 587 (0.35) | 70 (0.39) | 1.11 | 0.39 | 1.20 | 0.17 |
| VLWB | 1 455 (0.86) | 173 (0.95) | 1.11 | 0.21 | 1.18 | 0.05 |
| ELBW | 688 (0.41) | 90 (0.50) | 1.21 | 0.09 | 1.30 | 0.02 ‡ |
| Total number of twin births during lockdown, n | 6 748 | 608 | ||||
| Twin preterm births, n (%) | 3 975 (58.91) | 353 (58.06) | 0.97 | 0.70 | 1.11 | 0.24 |
| < 32 + 0 wks | 605 (8.97) | 79 (12.99) | 1.51 | 0.002 ‡ | 1.70 | < 0.001 ‡ |
| < 28 + 0 wks | 164 (2.43) | 25 (4.11) | 1.72 | 0.02 ‡ | 1.69 | 0.02 ‡ |
| VLWB | 630 (9.34) | 73 (12.01) | 1.32 | 0.04 ‡ | 1.54 | 0.003 ‡ |
| ELBW | 202 (2.99) | 26 (4.28) | 1.44 | 0.09 | 1.52 | 0.06 |
In the more advanced regression analysis, we incorporated all births from 2010 to 2020. The additive generalized regression models demonstrated a seasonal increase in preterm births in the first winter months during the studied period as well as a considerable long-term trend towards a lower risk of preterm birth. In contrast, there is a lower incidence of preterm births in the summer months. Analysis of the individual weekdays showed only small impact on the risk of preterm birth ( Fig. 3 ).
Fig. 3.
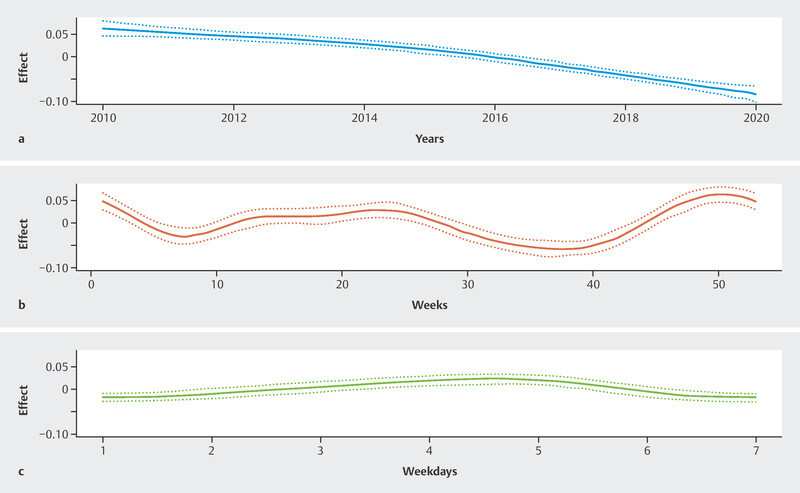
Preterm birth rates and possible impacts. a Trend of the Bavarian preterm birth rate between 2010 and 2020. b Impact of seasons on the risk of preterm birth. c Impact of weekdays on the risk of preterm birth.
Univariate analysis revealed a significant decrease in singleton preterm births with delivery occurring < 37 + 0 weeks of gestation (5.71% vs. 6.41%; OR 0.88; p < 0.001) during the first lockdown period ( Fig. 4 ). Similarly, we demonstrated a significant reduction in preterm births occurring < 32 + 0 weeks gestation (0.72% vs. 0.9%; OR 0.79; p = 0.02), while preterm births < 28 + 0 weeks gestation did not change significantly (0.31% vs. 0.22%; OR 0.04; p = 0.77). Table 1 illustrates the proportion of preterm births per 1000 live births in 2020 compared to 2010 – 2019. After adjusting for seasonality and long-term trends, no significant effect was found for preterm births (adj. OR 0.99; p = 0.73), while preterm birth rates < 32 weeks gestation continued to be significantly lower during the first lockdown period (adj. OR 0.82; p = 0.04).
Fig. 4.
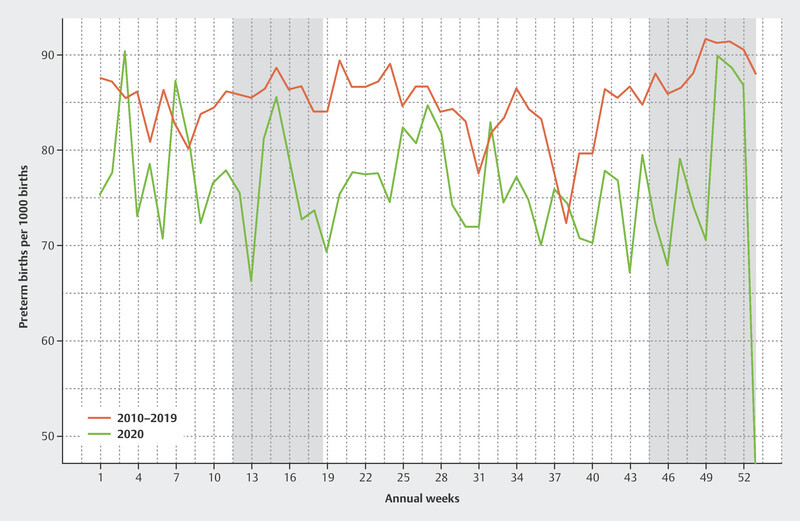
Preterm birth rates in singleton pregnancies per 1000 births from 2010 to 2019 vs. 2020.
During the second lockdown period, there was also a significant reduction in all studied preterm births (5.71% vs. 6.60%; OR 0.86; p < 0.001), although this effect did not remain significant after adjustment (adj. OR 0.96; p = 0.24).
There was no significant impact on the rates of neonates born < 32 weeks of gestation (0.95% vs. 0.92%; OR 1.03; p = 0.68; adj. OR 1.10; p = 0.24) and < 28 weeks of gestation (0.39% vs. 0.35%; OR 1.11; p = 0.39; adj. OR 1.20; p = 0.17), respectively.
For twin pregnancies, no significant difference in preterm birth rates was observed during the first lockdown period (52.99% vs. 56.26%; OR 0.88; p = 0.14; adj. OR 0.91; p = 0.31). There was also no difference in the subgroups showing delivery < 32 weeks of gestation (9.26% vs. 10.44%; OR 0.87; p = 0.42; adj. OR 0.95; p = 0.77) and < 28 weeks gestation (3.27% vs. 3.28%; OR 1.00; p = 1.00; adj. OR 1.24; p = 0.42).
During the second lockdown, there was no difference in the preterm birth rate for all twin pregnancies (58.06% vs. 58.91%; OR 0.97; p = 0.70; adj. OR 1.11; p = 0.24). However, there were more children born < 32 weeks of gestation (12.99% vs. 8.97%; OR 1.51; p = 0.002; adj. OR 1.70; p < 0.001) and < 28 weeks gestation (4.11% vs. 2.43%; OR 1.72; p = 0.02; adj. OR 1.69; p = 0.02) in 2020 ( Table 2 ).
Lockdown periods and birth weight
Analyses of VLBW and ELBW fetuses do not provide evidence for significant differences during the first lockdown period in 2020 compared to 2010 – 2019, neither for singleton (VLBW: 0.69% vs. 0.82%; OR: 0.84; p = 0.08; adj. OR: 0.84; p = 0.09; ELBW: 0.29% vs. 0.38%; OR: 0.78; p = 0.10; adj. OR 0.79; p = 0.13) nor for twin pregnancies (VLBW: 9.26% vs. 9.60%; OR: 0.96; p = 0.88; adj. OR: 1.06; p = 0.71; ELBW: 3.09% vs. 3.65; OR: 0.84; p = 0.63; adj. OR: 1.09; p = 0.74).
Regarding the second lockdown, the rate of VLBW neonates was higher for twin pregnancies (12.01% vs. 9.34%; OR 1.32; p = 0.04; adj. OR 1.54; p = 0.003) but not for singleton pregnancies (0.95% vs. 0.86%; OR 1.11; p = 0.21; adj. OR: 1.18; p = 0.05). With regard to ELBW, rates were significantly higher in singleton pregnancies (0.50% vs. 0.41%; OR 1.21; p = 0.09; adj. OR 1.30; p = 0.02), but not in twin pregnancies (4.28% vs. 2.99%; OR: 1.44; p = 0.09; adj. OR: 1.52; p = 0.06) ( Table 2 ).
Mobility change and preterm birth
During the first lockdown period, a maximum mobility reduction of 63.9% was observed in the Bavarian population on April 13th, 2020 due to contact restrictions. Compared to 2019, the first lockdown period showed a mean mobility reduction of 34.8%.
In the second lockdown, the mean mobility was only 10% lower than in the previous year. Fig. 5 shows the changes in mobility of the Bavarian population based on the data provided by the Covid-19 Mobility Project 14 .
Fig. 5.
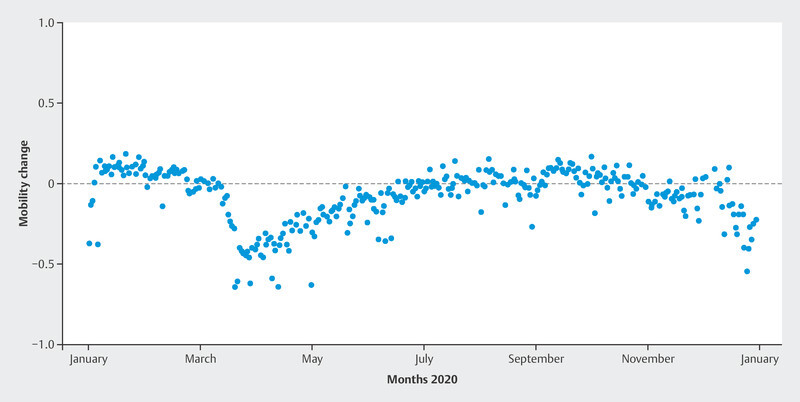
Mobility changes in 2020 compared to 2019 in Bavaria.
When all births are considered, the decreased population mobility in 2020 had a significant impact on the odds of a preterm birth (adj. OR [25% reduction] = 0.95, p = 0.002) while adjusting for long-term trends and potential seasonality.
However, subgroup analysis only showed a significant effect for twin births (adj. OR [25% reduction] = 0.89, p = 0.02) and the effect did not reach significance for singleton pregnancies (adj. OR [25% reduction] = 0.97, p = 0.14).
Further modeling suggests that decreased population mobility might also have a potential impact on gestational length in a combined cohort of singleton and twin births (0.19 days per 25% reduction, p = 0.002). However, in a subgroup analysis, this effect did not reach significance in singleton (p = 0.05) and twin pregnancies (p = 0.10).
Additional analysis showed that decreased population mobility has a small positive effect on birth weight. Thus, for a 25% decrease in population mobility, an increase in birth weight of 5.3 g was estimated across all births (p = 0.04). When analyzing the effect of population mobility on preterm VLBW and ELBW infants, the odds of neonates having a birth weight < 1500 g decreased with reduced population mobility (VLBW, adj. OR [25% reduction] = 0.91, p = 0.03), but the effect failed to reach significance for neonates with a birth weight < 1000 g (ELBW, adj. OR [25% reduction] = 0.90, p = 0.14).
Discussion
In the context of the infection control measures during the SARS-CoV-2 pandemic, studies showed a significant reduction in preterm births 8 and VLBW and ELBW neonates 7 . The discussion on whether and how these measures could be responsible for the reduced risk of preterm birth is still ongoing. While analyses from China 15 , Sweden 16 and Spain 17 failed to demonstrate an effect of country-specific lockdown measures on preterm birth risk, other studies indicate an association with these measures 18 , 19 , 20 . However, a meta-analysis of 15 studies revealed a moderate effect of lockdown measures on preterm births in high-income countries, whereas this effect was not detectable in three low-income countries 21 .
In our initial univariate analysis, we also found significantly lower preterm birth rates in singleton pregnancies in both lockdown periods. In contrast to previously published studies, we performed these analyses in a high number of cases. Thus, initially, we were able to confirm the results of the studies from Ireland and the Netherlands.
After adjusting for long-term trends and seasonality, however, multivariable semiparametric regression analysis failed to provide evidence for a significant effect of both lockdown periods. Hence, it should be questioned whether the preterm birth rate really is linked to the establishment of infection control measures during these periods. So far, only one study has investigated potential long-term trends. That study summarized centrally reported data from Norway, Sweden and Denmark 22 . The results of that study and our work are congruent.
An analysis based on fixed temporal lockdown periods must be assessed critically. At the beginning of the SARS-CoV-2 pandemic, it was demonstrated that the population in Germany was already aware of SARS-CoV-2 through media reports prior to the implementation of specific legislative measures on infection prophylaxis (e.g., the use of face masks and social distancing) and this may have led to an early reduction in the time-dependent reproductive rate R 23 . Furthermore, it is difficult to assess how strictly these restrictions and recommended behavioral measures were applied by the population over the course of the pandemic.
To further objectify population coherence with respect to legislative contact restrictions, we performed semiparametric regression modeling based on population mobility but were not able to demonstrate that decreased mobility had an impact on the risk of preterm birth in singleton pregnancies. To our knowledge, no other study has yet examined the effect of population mobility on a potential reduction in preterm birth rates. The data show that the coherence of the Bavarian population was significantly stronger during the first lockdown than during the second one. Assuming a causal relationship, this could theoretically explain the significant increase in ELBW neonates during the second lockdown.
Multiple pregnancies are generally at higher risk of preterm birth and this cohort of pregnancies is of considerable interest with respect to the prevention of preterm birth.
However, due to the increased a-priori risk of preterm birth, multiple pregnancies have been excluded from comparable studies, with the exception of a study by Klumper et al. 24 . Hence, our study is one of the first to also investigate the risk of preterm birth for twin pregnancies in the context of lockdown measures. We did not show a significant difference in twin preterm births during both lockdown periods while the risk of preterm birth at < 32 and < 28 weeks of gestation was significantly higher in the second lockdown period. This rather unexpected result is in line with a study from the Netherlands which also showed an increase in the risk of preterm birth < 28 weeks of gestation 24 . The interpretation of these findings is challenging and we can only guess whether the deterioration in population adherence and the increased incidence of SARS-CoV-2 during the second lockdown had significant impacts on the increased risk of preterm birth before 32 and 28 weeks of gestation in twin pregnancies.
Since we were able to demonstrate that reduced population mobility could have a favorable effect on the preterm birth rate in twin pregnancies, one could conclude that mothers of twins should stay at home to increase the length of their pregnancy. In this context, however, it is important to note that other risk factors for preterm birth were also influenced by nonpharmacological interventions during the SARS-CoV-2 pandemic; for instance, contact restrictions, social distancing, increased awareness of hygiene measures, and the use of mouth-nose protection are also thought to be responsible for significantly reduced rates of respiratory infections such as influenza 25 , 26 , 27 . The Robert Koch Institute reported a significant decrease in respiratory infections in the German population following the introduction of contact restrictions and hygiene recommendations during the studied periods 28 . Furthermore, lower levels of air pollution could also be related to the reduced rates of preterm births 29 . Significantly lower levels of pollutants were measured in Germany during the analyzed period. Compared to the corresponding period in the previous year, a reduction of NO 2 by 37% was detected in Munich between March 15th, 2020, and April 30th, 2020, for example 30 .
In addition, a possible negative effect of the measures during the SARS-CoV-2 pandemic has to be discussed. For instance, pregnant women reported anxiety and depressive symptoms more often 31 , which have been identified as possible risk factors for preterm birth 32 .
A limitation of the study is that the considered second lockdown period ends at the end of 2020, while the second wave of infections and corresponding mitigation measures continued in 2021.
Another limitation of our analysis is that the considered adjustment for the effects of seasonal, weekday and long-term trends could theoretically also somewhat reduce the true effects of lockdown or mobility changes. As the pandemic influenced the behavior of the population for nearly the whole of 2020, parts of the spline effect at the border of the study period (2020, Fig. 3 ) might not just be part of an overall long-term trend but could also reflect the impact of the lockdown periods or reduced mobility. It is difficult to disentangle such partly overlapping effects.
In summary, it is of course very hard to design a study that can prove a causal relationship between lockdown periods, reduced population mobility and a lower preterm birth rate. Our observational study can therefore only provide additional evidence for a multifactorial phenomenon leading to a lower preterm birth rate during these periods.
Nevertheless, the strength of our study is that we investigated a possible impact of population mobility on the risk of preterm birth in singleton and twin pregnancies. Another strength is the large number of cases: in total, our study includes 1.2 million births, which allowed us to investigate various outcome parameters for preterm birth in singleton and twin pregnancies in detail.
Conclusion
Reduced preterm birth rates during the two lockdown periods in 2020 were also observed for singleton and twin pregnancies in Bavaria, Germany. These effects were no longer detectable after adjusting for seasonal and long-term trends, indicating that they might not be large enough to have a real clinical impact. Reduced population mobility was associated with lower preterm birth rates for twin pregnancies even after adjusting for seasonal and long-term trends. Further studies are needed and should be conducted to estimate these effects, including in smaller subgroups such as twin pregnancies.
Acknowledgements
The authors would like to thank the BAQ for providing the data analyzed in this paper. Furthermore, we would like to thank the research group led by Prof. Brockmann, who provided us with mobility data for this work.
Conflict of Interest The authors declare that they have no conflict of interest.
Joint senior authors.
References
- 1.Stumpfe F M, Titzmann A, Schneider M O. SARS-CoV-2 Infection in Pregnancy – a Review of the Current Literature and Possible Impact on Maternal and Neonatal Outcome. Geburtshilfe Frauenheilkd. 2020;80:380–390. doi: 10.1055/a-1134-5951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hein A, Kehl S, Haberle L. Prevalence of SARS-CoV-2 in Pregnant Women Assessed by RT-PCR in Franconia, Germany: First Results of the SCENARIO Study (SARS-CoV-2 prEvalence in pregNAncy and at biRth In FrancOnia) Geburtshilfe Frauenheilkd. 2022;82:226–234. doi: 10.1055/a-1727-9672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.De Curtis M, Villani L, Polo A. Increase of stillbirth and decrease of late preterm infants during the COVID-19 pandemic lockdown. Arch Dis Child Fetal Neonatal Ed. 2020 doi: 10.1136/archdischild-2020-320682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kc A, Gurung R, Kinney M V. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: a prospective observational study. Lancet Glob Health. 2020;8:e1273–e1281. doi: 10.1016/S2214-109X(20)30345-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Khalil A, von Dadelszen P, Draycott T. Change in the Incidence of Stillbirth and Preterm Delivery During the COVID-19 Pandemic. JAMA. 2020 doi: 10.1001/jama.2020.12746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hedermann G, Hedley P L, Baekvad-Hansen M. Danish premature birth rates during the COVID-19 lockdown. Arch Dis Child Fetal Neonatal Ed. 2021;106:93–95. doi: 10.1136/archdischild-2020-319990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Philip R K, Purtill H, Reidy E. Unprecedented reduction in births of very low birthweight (VLBW) and extremely low birthweight (ELBW) infants during the COVID-19 lockdown in Ireland: a ‘natural experiment’ allowing analysis of data from the prior two decades. BMJ Glob Health. 2020 doi: 10.1136/bmjgh-2020-003075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Been J V, Burgos Ochoa L, Bertens L CM. Impact of COVID-19 mitigation measures on the incidence of preterm birth: a national quasi-experimental study. Lancet Public Health. 2020;5:e604–e611. doi: 10.1016/S2468-2667(20)30223-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Askitas N, Tatsiramos K, Verheyden B. Estimating worldwide effects of non-pharmaceutical interventions on COVID-19 incidence and population mobility patterns using a multiple-event study. Sci Rep. 2021;11:1972. doi: 10.1038/s41598-021-81442-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Robert Koch-Institut . COVID-19 Datenhub. 2021. https://npgeo-corona-npgeo-de.hub.arcgis.com/datasets/ef4b445a53c1406892257fe63129a8ea_0/explore?location=51.164254%2C8.127781%2C6.73&showTable=true https://npgeo-corona-npgeo-de.hub.arcgis.com/datasets/ef4b445a53c1406892257fe63129a8ea_0/explore?location=51.164254%2C8.127781%2C6.73&showTable=true
- 11.Schlosser F, Maier B F, Jack O. COVID-19 lockdown induces disease-mitigating structural changes in mobility networks. Proc Natl Acad Sci U S A. 2020;117:32883–32890. doi: 10.1073/pnas.2012326117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wood S N.Generalized Additive Models – An Introduction with R 1st ed.ed.Chapman and Hall/CRC; 2006 [Google Scholar]
- 13.Wood S N, Goude Y, Shaw S. Generalized additive models for large data sets. Journal of the Royal Statistical Society: Series C (Applied Statistics) 2015;64:139–155. doi: 10.1111/rssc.12068. [DOI] [Google Scholar]
- 14.Brockmann D. Covid-19 Mobility Project. 2021. https://www.covid-19-mobility.org/ https://www.covid-19-mobility.org/
- 15.Dong M, Qian R, Wang J. Associations of COVID-19 lockdown with gestational length and preterm birth in China. BMC Pregnancy Childbirth. 2021;21:795. doi: 10.1186/s12884-021-04268-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Pasternak B, Neovius M, Soderling J. Preterm Birth and Stillbirth During the COVID-19 Pandemic in Sweden: A Nationwide Cohort Study. Ann Intern Med. 2021;174:873–875. doi: 10.7326/M20-6367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Arnaez J, Ochoa-Sangrador C, Caserio S. Lack of changes in preterm delivery and stillbirths during COVID-19 lockdown in a European region. Eur J Pediatr. 2021;180:1997–2002. doi: 10.1007/s00431-021-03984-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Matheson A, McGannon C J, Malhotra A. Prematurity Rates During the Coronavirus Disease 2019 (COVID-19) Pandemic Lockdown in Melbourne, Australia. Obstet Gynecol. 2021;137:405–407. doi: 10.1097/AOG.0000000000004236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Berghella V, Boelig R, Roman A. Decreased incidence of preterm birth during coronavirus disease 2019 pandemic. Am J Obstet Gynecol MFM. 2020;2:100258. doi: 10.1016/j.ajogmf.2020.100258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Meyer R, Bart Y, Tsur A. A marked decrease in preterm deliveries during the coronavirus disease 2019 pandemic. Am J Obstet Gynecol. 2021;224:234–237. doi: 10.1016/j.ajog.2020.10.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chmielewska B, Barratt I, Townsend R. Effects of the COVID-19 pandemic on maternal and perinatal outcomes: a systematic review and meta-analysis. Lancet Glob Health. 2021 doi: 10.1016/S2214-109X(21)00079-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Oakley L L, Ortqvist A K, Kinge J. Preterm birth after the introduction of COVID-19 mitigation measures in Norway, Sweden, and Denmark: a registry-based difference-in-differences study. Am J Obstet Gynecol. 2021 doi: 10.1016/j.ajog.2021.11.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.an der Heiden M, Hamouda O. Schätzung der aktuellen Entwicklung der SARS-CoV-2-Epidemie in Deutschland – Nowcasting. Epidemiologisches Bulletin. 2020;2020:10–15. doi: 10.25646/6692.4. [DOI] [Google Scholar]
- 24.Klumper J, Kazemier B M, Been J V. Association between COVID-19 lockdown measures and the incidence of iatrogenic versus spontaneous very preterm births in the Netherlands: a retrospective study. BMC Pregnancy Childbirth. 2021;21:767. doi: 10.1186/s12884-021-04249-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gomez G B, Mahé C, Chaves S S. Uncertain effects of the pandemic on respiratory viruses. Science. 2021;372:1043–1044. doi: 10.1126/science.abh3986. [DOI] [PubMed] [Google Scholar]
- 26.Huang Q S, Wood T, Jelley L. Impact of the COVID-19 nonpharmaceutical interventions on influenza and other respiratory viral infections in New Zealand. Nat Commun. 2021;12:1001. doi: 10.1038/s41467-021-21157-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.WHO . Review of global influenza circulation, late 2019 to 2020, and the impact of the COVID-19 pandemic on influenza circulation. 2021. https://www.who.int/publications/i/item/who-wer-9625-241-264 https://www.who.int/publications/i/item/who-wer-9625-241-264
- 28.Buchholz U, Buda S, Prahm K. Abrupter Rückgang der Raten an Atemwegserkrankungen in der deutschen Bevölkerung. Epidemiologisches Bulletin. 2020;2020:7–9. doi: 10.25646/6636.2. [DOI] [Google Scholar]
- 29.Ortiz A, Guerreiro C. Air Quality in Europe – 2020 report. 2020. https://www.actu-environnement.com/media/pdf/36559.pdf https://www.actu-environnement.com/media/pdf/36559.pdf [DOI]
- 30.Bekkar B, Pacheco S, Basu R. Association of Air Pollution and Heat Exposure With Preterm Birth, Low Birth Weight, and Stillbirth in the US: A Systematic Review. JAMA Netw Open. 2020;3:e208243. doi: 10.1001/jamanetworkopen.2020.8243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lebel C, MacKinnon A, Bagshawe M. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J Affect Disord. 2020;277:5–13. doi: 10.1016/j.jad.2020.07.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bussières E-L, Tarabulsy G M, Pearson J. Maternal prenatal stress and infant birth weight and gestational age: A meta-analysis of prospective studies. Developmental Review. 2015;36:179–199. doi: 10.1016/j.dr.2015.04.001. [DOI] [Google Scholar]