Abstract
Objective The present paper aims to describe multiligament knee injuries and to associate their features with the profile of the patients and trauma mechanisms.
Methods This is a cross-sectional study evaluating 82 patients with multiligament knee injuries from September 2016 to September 2018. Evaluated parameters included age, gender, mechanical axis, affected side, range of motion, trauma mechanism, associated injuries, affected ligaments, and absence from work.
Results The sample included patients aged between 16 and 58 years old, with an average age of 29.7 years old; most subjects were males, with 92.7% of cases. The most common trauma mechanism was motorcycle accident (45.1%). The most injured ligament was the anterior cruciate ligament (80.5%), followed by the posterior cruciate ligament (77.1%), the posterolateral corner (61.0%), and the tibial collateral ligament (26.8%). The most frequent type of dislocation was KD IIIL (30.4%). Only 1 patient had a vascular injury, and 13 (15.9%) presented with neurological injuries. Most subjects took medical leave from work (52.4%).
Conclusion There is a big difference between patients with multiligament lesions in Brazil compared with international studies. Thus, it is advisable to carry out more specific studies on the topic with our population to improve the treatment of these patients.
Keywords: knee injuries, knee dislocation, joint instability
Introduction
Multiligament injuries of the knee are complex, rare, and difficult to treat conditions, usually resulting from a traumatic knee dislocation. The event is often followed by injuries in multiple structures, including knee stabilizers and neurovascular structures. Multiligament lesions are characterized by the involvement of two or more knee ligaments, such as the cruciate ligaments, the tibial collateral ligament, and the posterolateral corner, resulting in significant instability. 1 2 3
The complete dislocation of the tibiofemoral joint is highly associated with severe complications, including neurovascular injuries (popliteal artery, fibular nerve, and tibial nerve), compartmental syndrome, multidirectional instability, and chronic pain. 2
Knee dislocations were classified by Schenck 4 based on the number of affected ligaments and their nature, as shown in Box 1 .
Box 1. Classification of knee dislocations according to Schenck.
| Classification | Injury |
|---|---|
| KD I | Injury involves only one cruciate ligament and a collateral ligament |
| KD II | Injury involves both cruciate ligaments |
| KD III M | Injury involves both cruciate ligaments and the tibial collateral ligament |
| KD III L | Injury involves both cruciate ligaments and the fibular collateral ligament |
| KD IV | All four ligaments are injured |
| KD V | Knee dislocation associated with fracture |
Some studies, including those from Arom et al. 5 and Wilson et al., 3 reported that these injuries account for < 0.2% of orthopedic lesions, ranging from 7/10,000 to 1/100,000 patients per year. However, it is difficult to obtain data to correctly identify the incidence of knee dislocation, since it is a rare injury and half of the cases are reduced at the time of initial care. Thus, knee dislocation should be assessed in every patient with a lesion in two or more knee ligaments. 2 3 5 6 7 8 9 10
The most frequent injury mechanism is direct or indirect high-energy trauma to the knee, mostly caused by motor vehicle accidents. These lesions are also related to fall from height and sports traumas, usually football, skiing, soccer, and rugby. In addition, they can affect obese people in low-speed injuries after knee sprain. The most common trauma mechanism is knee hyperextension resulting in anterior dislocation. 5 6 7 11
The literature reports that the incidence of vascular injury ranges from 5 to 80%, whereas the incidence of neurological injury ranges from 16 to 50%. According to Medina et al., 12 the incidence of vascular injuries and neurological injuries was 18 and 25%, respectively.
These variations are related to the type of trauma energy affecting each analyzed population. In addition, the rarity of this lesion makes it difficult to obtain a sufficient number of patients (N) to gather more accurate data, resulting in a considerable divergence between studies. 2 3 12
Secondary joint stiffness and ligament reconstruction failure are the most common early complications. Most of these patients will develop post-traumatic osteoarthritis, as demonstrated by Engebretsen et al., 13 who observed knee osteoarthritis in 34% of the patients 9 years after trauma. This results in major limitations to the patients, who are mostly young, economically active subjects. The treatment of this complex injury involves a large investment in public and/or supplementary health, in addition to a long period of absence from work. 10 12 13 14 15 16
During the acute phase, the goal is to reduce and stabilize the joint, and these procedures must be performed immediately. Neurovascular assessment is critical, and it must not be delayed. The vascular physical examination is performed by peripheral pulses palpation and limb temperature, capillary perfusion, and ankle-brachial index determination (an ankle-brachial index < 0.9 indicates a high suspicion of arterial injury). The severity of these vascular injuries is emphasized by the fact that, regardless of treatment, the incidence of amputations in these patients is of 12%. 3 6 8 9 12 14
Thus, demographics of patients with these knee injuries must be known to optimize their treatment and outline preventive strategies. As a result, the Brazilian literature was queried on multiligamental injuries and knee dislocation at databases (PubMed and SciELO) and journals (Revista Brasileira de Ortopedia [RBO]). This analysis revealed the scarce number of Brazilian studies addressing these subjects. Among the existing articles, the most relevant is from Kupczik et al., 10 which analyzed 23 patients.
As such, the present cross-sectional study aims at the epidemiological analysis of multiligament knee injuries and their associations with neurovascular and fracture pathologies. These data are correlated with trauma mechanism, gender, age, and time away from work.
Materials and Methods
Cross-sectional study evaluating 82 cases of knee instability in patients seen at the Multiligament Knee Injuries outpatient facility from September 2016 to September 2018. Data on age, trauma, gender, mechanical knee axis, affected side, range of motion (ROM), trauma mechanism, associated injuries (including neurological and vascular lesions, dislocations, and fractures), affected ligaments, gait, and time away from work under Brazilian Social Security Institute (INSS, in the Portuguese acronym) benefit were collected.
The present study included patients with multiligament knee instability affecting two or more ligaments. Patients with lesions on a single ligament and those who did not undergo a complete physical examination, either due to pain or to the presence of an external fixator, were excluded from the sample.
Collected data was inserted at database in an electronic spreadsheet and analyzed with IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA), and Microsoft Excel 2007 (Microsoft Corp., Redmond, WA, USA). Data were synthesized using descriptive statistics (mean, median, minimum, maximum, standard deviation [SD], coefficient of variation [CV], and proportions of interest for quantitative variables), in addition to simple frequency distributions and cross-tabulations for qualitative variables. 17 18
Results
Table 1 shows the following typical profile for this sample of 82 patients with multiligament knee injuries: males (92.7%), aged 20 to 40 years old (75.6%), either overweight or obese (71.4%). In addition, the left side was the most affected (52.4%), and the genu varum mechanical axis was more common when compared with the genu valgum (34.1 versus 18.3%, respectively). Slap gait was observed in 10 patients (12.2%), while 12 patients (14.6%) presented buckling gait.
Table 1. Characteristics of patients with injured knees.
| Variable | Frequency | |
|---|---|---|
| F | % | |
| Gender | ||
| Female | 6 | 7.3% |
| Male | 76 | 92.7% |
| Age at injury (years old) | ||
| 10 |— 20 | 8 | 9.8% |
| 20 | — 30 | 37 | 45.1% |
| 30 | — 40 | 25 | 30.5% |
| 40 |— 50 | 9 | 11.0% |
| 50 |— 60 | 3 | 3.7% |
| Body classification according to BMI * | ||
| Adequate | 14 | 28.6% |
| Overweight | 19 | 38.8% |
| Grade I obesity | 12 | 24.5% |
| Grade II obesity | 3 | 6.1% |
| Grade III obesity | 1 | 2.0% |
| Injured knee | ||
| Right | 39 | 47.6% |
| Left | 43 | 52.4% |
| Axis | ||
| Neutral | 39 | 47.5% |
| Valgus | 15 | 18.3% |
| Varus | 28 | 34.1% |
| Slap gait | 10 | 12.2% |
| Buckling | 12 | 14.6% |
| Fracture | 22 | 26.8% |
| Dislocation | 18 | 22.8% |
| Neurological Injury | 13 | 15.9% |
| Vascular Injury | 1 | 1.2% |
| Injury Type | ||
| KD I | 19 | 23.1% |
| KD II | 10 | 12.1% |
| KD III M | 12 | 14.6% |
| KD III L | 25 | 30.4% |
| KD IV | 6 | 7.3% |
| KD V | 10 | 12.1% |
| Range of Motion | ||
| - 5 to 110° | 1 | 1.2% |
| - 5 to 140° | 2 | 2.4% |
| - 5 to 128° | 1 | 1.2% |
| 0 to 70° | 1 | 1.2% |
| 0 to 90° | 3 | 3.7% |
| 0 to 100° | 7 | 8.5% |
| 0 to 105° | 1 | 1.2% |
| 0 to 110° | 28 | 34.1% |
| 0 to 120° | 11 | 13.4% |
| 0 to 130° | 18 | 22.0% |
| 0 to 135° | 1 | 1.2% |
| 0 to 136° | 1 | 1.2% |
| 0 to 140° | 4 | 4.9% |
| 5 to 100° | 1 | 1.2% |
| 10 to 110° | 1 | 1.2% |
| 20 to 100° | 1 | 1.2% |
| Time away from work under INSS benefit | 43 | 52.4% |
Abbreviations: BMI, body mass index; INSS, Brazilian Social Security Institute.
Based on n = 49, since body mass index (BMI) data was only available for 49 subjects.
Associated fractures and neurological injuries were observed in 26.8 and 15.9% of the cases, respectively; 18 patients (22.8%) presented knee dislocation requiring a reduction maneuver, and a single patient (1.2%) had an injury at the popliteal artery. The most frequent type of injury was KD IIIL (30.4%); in addition, 40 patients (48.8%) had a ROM < 110°, and 43 subjects (52.4%) were away from work and collecting INSS benefit due to multiligament knee injury.
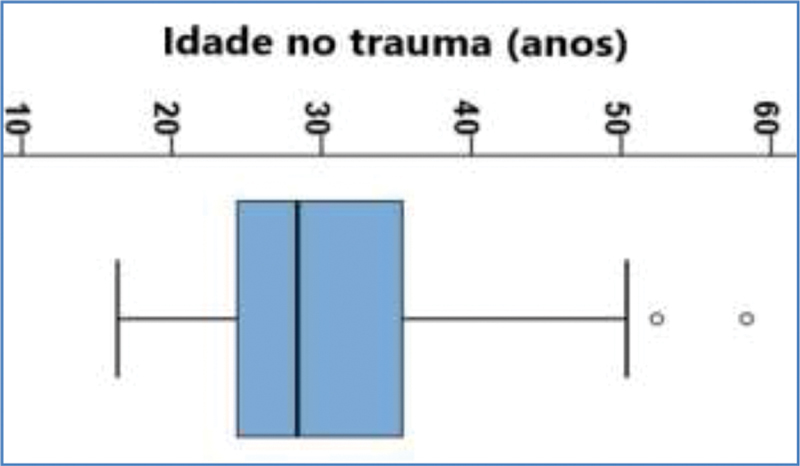
Patients with multiligament knee injury were aged between 16 and 58 years old, with a mean age of 29.7 years old, median age of 28 years old, and SD of 8.9 years; these values result in a CV of 0.30, showing moderate age variability in patients with multiligament knee injuries, according to the distribution shown in Figure 1 . The box diagram shows that the two highest ages, 52 and 58 years old, are atypical ages for patients with multiligament knee injuries, and are marked with the ° symbol on the graph.
Fig. 1.
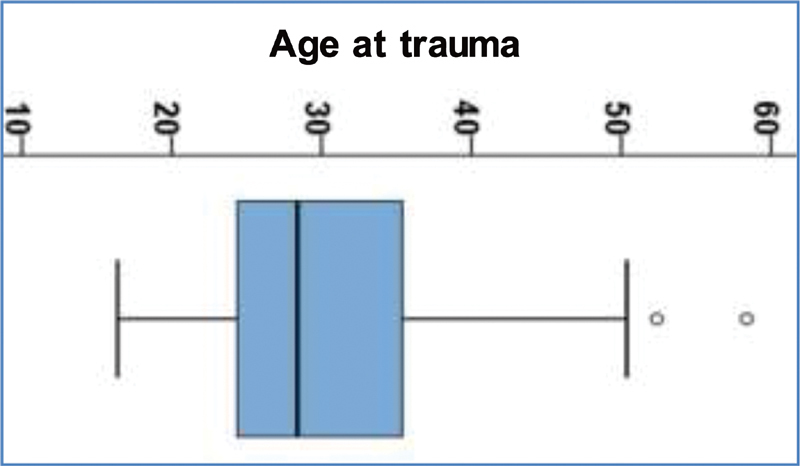
Box diagram showing the age distribution of patients with multiligament knee injuries.
Table 2 shows the distribution of the injury-related mechanism. Both globally and for age groups (patients < 30 years old and ≥ 30 years old), the main injury-related mechanism was motorcycle accident, with 45.1% of the cases; 51.1% of these patients were < 30 years old. Car accident, football, and fight were also important causes of trauma. Traffic accidents, including motorcycle accidents, car accidents and running overs, accounted for 61.0% of multiligament knee injuries. Sports-related injuries occurred in 23.2% of the cases; the remaining traumas, representing only 15.8% of the sample, were caused by falls, job-related accidents, ox kicks, and torsional trauma.
Table 2. Distribution of the mechanism resulting in multiligament knee injuries.
| Injury-generating mechanism |
Global n = 82 |
Age < 30 years old n = 45 |
Age ≥ 30 years old | |||
|---|---|---|---|---|---|---|
| n = 37 | ||||||
| Motorcycle accident | 37 | 45.1% | 23 | 51.1% | 14 | 37.8% |
| Car accident | 9 | 11.0% | 4 | 8.9% | 5 | 13.5% |
| Soccer | 9 | 11.0% | 6 | 13.3% | 3 | 8.1% |
| Fight | 8 | 9.8% | 3 | 6.6% | 5 | 13.5% |
| Fall from height | 6 | 7.3% | 3 | 6.6% | 3 | 8.1% |
| Running over | 4 | 4.9% | 1 | 2.2% | 3 | 8.1% |
| Job-related accident | 2 | 2.4% | 2 | 4.4% | 0 | 0.0% |
| Ox kick | 2 | 2.4% | 1 | 2.2% | 1 | 2.7% |
| Fall from elevator | 1 | 1.2% | 0 | 0.0% | 1 | 2.7% |
| Fall in hole | 1 | 1.2% | 0 | 0.0% | 1 | 2.7% |
| Skate | 1 | 1.2% | 1 | 2.2% | 0 | 0.0% |
| Paintball match | 1 | 1.2% | 0 | 0.0% | 1 | 2.7% |
| Torsional trauma | 1 | 1.2% | 1 | 2.2% | 0 | 0.0% |
Table 3 shows that the most affected ligament, regardless of age, was the anterior cruciate ligament (80.5%), followed by the posterior cruciate ligament (77.1%). The posterolateral corner ligaments were injured more frequently than the medial collateral ligament, with rates of 61.0 and 26.8%, respectively. Medial menisci were injured more frequently than lateral menisci, with rates of 25.6 and 14.6%, respectively. The table shows the p-values , all > 5%, revealing that no injury was associated with any age group, and that there was no significant difference in injury rates between both age groups.
Table 3. Frequency of multiligament knee injuries identified by clinical examination and/or magnetic resonance imaging, both global and compared by age group.
| Injuries | Global n = 82 |
Age < 30 years old n = 45 |
Age ≥30 years old n = 37 |
p-value at the chi-squared test comparing frequencies from both age groups | |||
|---|---|---|---|---|---|---|---|
| Anterior cruciate ligament | 66 | 80.50% | 33 | 73.30% | 33 | 89.20% | 0.071 |
| Posterior cruciate ligament | 64 | 77.10% | 33 | 73.30% | 31 | 82.80% | 0.408 |
| CPL | 50 | 61.0% | 27 | 60.0% | 23 | 73.00% | 0.842 |
| Medial collateral ligament | 22 | 21.00% | 10 | 22.20% | 12 | 32.40% | 0.299 |
| Lateral collateral ligament | 7 | 8.5% | 5 | 11.1% | 2 | 5.40% | 0.449 * |
| Medial meniscus | 21 | 25.60% | 10 | 22.20% | 11 | 29.70% | 0.438 |
| Lateral meniscus | 12 | 14.60% | 4 | 8.90% | 8 | 21.60% | 0.105 |
| Fibular nerve | 2 | 2.40% | 0 | 0.00% | 2 | 5.40% | 0.201 * |
| Posterior plateau | 1 | 1.20% | 0 | 0.00% | 1 | 2.70% | 0.451 * |
| Biceps avulsion | 1 | 1.20% | 1 | 2.20% | 0 | 0.00% | 1.000 * |
The Fisher exact test was used in this case.
Table 4 shows that 18 patients (22%) presented knee dislocation requiring a reduction maneuver, and that 22 patients (26.8%) had associated fractures. The occurrence of trauma-related dislocations and fractures was not associated with age, since the p-values were all > 5%, revealing that there was no significant difference between dislocation and fracture rates between both groups.
Table 4. Frequencies of dislocation and fractures associated with multiligament knee injuries.
| Dislocation and Fractures | Global n = 82 | Age < 30 years old n = 45 |
Age ≥ 30 years old n = 37 |
chi-squared test comparing frequencies from both age groups |
|---|---|---|---|---|
| Knee dislocation | 18 (22.0%) | 7 (15.6%) | 11 (29.7%) | 0.180 |
| At least one fracture | 22 (26.8%) | 12 (26.7%) | 10 (27.0%) | 0.908 |
| Acetabular fracture | 4 (4.9%) | 2 (4.4%) | 2 (5.4%) | 1.000 * |
| Tibial fracture | 4 (4.9%) | 4 (8.9%) | 0 (0.0%) | 0.123 * |
| Ankle fracture | 4 (4.9%) | 1 (2.2%) | 3 (8.1%) | 0.323 * |
| Femoral fracture | 3 (3.7%) | 2 (4.4%) | 1 (2.7%) | 1.000 * |
| Knee fracture | 3 (3.7%) | 1 (2.2%) | 2 (5.4%) | 0.586 * |
| Tibial plateau fracture | 2 (2.4%) | 1 (2.2%) | 1 (2.7%) | 0.201 * |
| Compartmental syndrome | 1 (1.2%) | 1 (2.2%) | 0 (0.0%) | 1.000 * |
| Fibular fracture | 1 (1.2%) | 0 (0.0%) | 1 (2.7%) | 0.451 * |
| Medial malleolus fracture | 1 (1.2%) | 1 (2.2%) | 0 (0.0%) | 1.000 * |
| Tibial diaphyseal fracture | 1 (1.2%) | 1 (2.2%) | 0 (0.0%) | 1.000 * |
The Fisher exact test was used in this case for comparison.
The prevalence of neurological injuries was of 15.9% (13 patients), with 12 cases of fibular nerve damage, 2 cases of fibular and tibial nerve damage, and 1 patient with a radial nerve injury that was not related to the specific knee trauma. Table 5 shows the p-values , all > 5%, revealing that neurological injuries, either globally or by lesion type, are not associated with age since there was no significant difference in their incidence between both age groups.
Table 5. Frequency of neurological injuries associated with multiligament knee injuries, both global and compared by age group.
| Neurological Injury | Global n = 82 |
Age < 30 years old n = 45 |
Age ≥ 30 years old n = 37 |
p-value from the chi-squared test comparing frequencies from both age groups |
|---|---|---|---|---|
| Neurological injury | 13 (15.9%) | 8 (17.7%) | 5 (13.5%) | 0.599 |
| Fibular nerve | 12 (14.6%) | 8 (17.7%) | 4 (10.8%) | 0.674 * |
| Tibial nerve | 2 (1.2%) | 2 (4.4%) | 0 (0.0%) | 0.451 * |
The Fisher exact test was used in this case for comparison.
Knee dislocation is significantly associated with neurological injury. Knee dislocation was observed in 15.9% of the cases with no neurological injury and in 53.8% of the cases with neurological injury. Neurological injury occurred in 9.4% of cases with no knee dislocation and in 38.9% of cases with knee dislocation. The difference between these proportions is statistically significant ( p = 0.006; Fisher exact test). The odds ratio is 6.2, with a confidence interval (CI) ranging from 1.7 to 21.8. It is estimated that the chance of a patient with knee dislocation to have a neurological injury is 6.2 times higher compared with a subject with no knee dislocation who presents a neurological injury.
It was investigated whether obesity was associated with any study parameter, but no association with statistical significance was found.
Discussion
Multiligament lesion was more frequent in men (92.7%). This gender-related difference was expected, since men are more exposed to high-energy injuries, such as motorcycle accidents and higher intensity sports. These findings were consistent with those from Wilson et al. 3 and Medina et al., 12 who identified percentages of 72 and 78%, respectively, of male patients in their populations. In contrast, for Kupczik et al., 10 only 65% of the subjects were males, perhaps due to local cultural characteristics and sample size.
The most common trauma mechanism was traffic accident, affecting 61.0% of the patients. Among them, motorcycle accidents were the most prevalent (45.1%), followed by car accidents (11.0%) and running overs (4.9%). Sports-related injuries accounted for 23.2% of the cases, involving mostly football (11.0%), and fights (9.8%). These data were consistent with a Brazilian study by Kupczik et al., 10 who reported that 60% of the cases were associated with motorcycle accidents. However, these data differed from the international literature.
The anterior cruciate ligament was the most affected (80.5%), followed by the posterior cruciate ligament (77.1%); posterolateral corner ligament injuries were more frequent when compared with medial collateral ligament lesions, with rates of 61.0 and 26.8%, respectively. The most common injury pattern was KD III-L (30.4%) according to the Schenck classification, representing an injury both to the cruciate and posterolateral corner ligaments. We believe that the low prevalence of medial collateral ligament injury is due to its healing, which may occur after adequate, early conservative treatment. Most of the patients from this study were seen at the chronic phase at the multiligament injury outpatient clinic, explaining this finding; this is also a limitation of our study.
A single patient had a popliteal artery lesion (1.2%), in a rate which is lower than that reported in the literature. Medina et al. 12 observed a 15% prevalence of popliteal artery injury, and 17% of these patients progressed to limb amputation. This difference may be due to the characteristic of the multiligament lesions outpatient clinic, which is a referral center, not an emergency department. As a result, many cases with poor clinical outcomes, such as amputations, were not surgically treated at the reference facility, but submitted to initial care at an emergency hospital, thus decreasing the prevalence of popliteal artery injuries in our population.
An association between multiligament knee instability and neurological injury was identified, at a 14.6% rate. All these patients had fibular nerve damage, and only two of them also presented an associated tibial nerve damage. In contrast, Medina et al. 12 found a 25% association between neurological injury and knee dislocation. There are two potential explanations for this finding; first, in some patients, the neuropraxia symptoms may have improved before the visit to the referral clinic; alternatively, they evolved with complications that contraindicate surgery and, therefore, were not referred to our facility.
In total, 52.4% of the patients were away from work and collecting INSS benefits. This data is higher than the international values, as reported by Levy et al., 14 which showed a 50% return to work after conservative treatment and 72% after surgical treatment. This can be explained due to the Brazilian socioeconomic features, with a high unemployment rate, which may result in patients who simulate the clinical exacerbation of the injury to maintain the financial benefit. In addition, work accessibility for people with limited mobility remains scarce. As such, multiligament knee injuries have an important financial impact because the most affected group consists of young, economically active people.
The present study had limitations, including a selection bias, since it evaluated patients referred to an outpatient clinic for multiple knee injuries, which is a tertiary center for this type of lesion. Cases with surgical indication were referred to this clinic, which may have excluded patients with contraindications for ligament reconstruction, such as those with serious complications, including amputations and other neurovascular injuries. In addition, another limitation of the study is that many patients had a chronic disease, with partial healing of the tibial collateral and posterior cruciate ligaments.
Conclusion
There was a significant gender-related difference, with males being more affected than females in a 13:1 ratio. Regarding trauma dynamics, traffic accidents accounted for 61.0% of the cases, mostly motorcycle accidents, with a 45.1% rate.
As a result, there is a great difference between Brazilian patients with multiligament knee injuries in comparison with international studies. Thus, further Brazilian, specific studies are required to improve the treatment of our patients.
Conflito de Interesses Os autores declaram não haver conflito de interesses.
Suporte Financeiro
Não houve suporte financeiro de fontes públicas, comerciais, ou sem fins lucrativos.
Financial Support
The present study received no financial support from public, commercial, or not-for-profit sources.
Trabalho desenvolvido no Centro de Atenção Especializada ao Joelho, Instituto Nacional de Traumatologia Jammil Haddad -INTO/ MS, Rio de Janeiro, RJ, Brasil
Study developed at the Knee Specialized Care Center, Instituto Nacional de Traumatologia Jammil Haddad -INTO/MS, Rio de Janeiro, RJ, Brazil
Referências
- 1.Ferrari M B, Chahla J, Mitchell J J. Multiligament Reconstruction of the Knee in the Setting of Knee Dislocation With a Medial-Sided Injury. Arthrosc Tech. 2017;6(02):e341–e350. doi: 10.1016/j.eats.2016.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Levy B A, Dajani K A, Whelan D B. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy. 2009;25(04):430–438. doi: 10.1016/j.arthro.2009.01.008. [DOI] [PubMed] [Google Scholar]
- 3.Wilson S M, Mehta N, Do H T, Ghomrawi H, Lyman S, Marx R G. Epidemiology of multiligament knee reconstruction. Clin Orthop Relat Res. 2014;472(09):2603–2608. doi: 10.1007/s11999-014-3653-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schenck R C., Jr The dislocated knee. Instr Course Lect. 1994;43:127–136. [PubMed] [Google Scholar]
- 5.Arom G A, Yeranosian M G, Petrigliano F A, Terrell R D, McAllister D R. The changing demographics of knee dislocation: a retrospective database review. Clin Orthop Relat Res. 2014;472(09):2609–2614. doi: 10.1007/s11999-013-3373-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hegyes M S, Richardson M W, Miller M D. Knee dislocation. Complications of nonoperative and operative management. Clin Sports Med. 2000;19(03):519–543. doi: 10.1016/s0278-5919(05)70222-2. [DOI] [PubMed] [Google Scholar]
- 7.Henrichs A. A review of knee dislocations. J Athl Train. 2004;39(04):365–369. [PMC free article] [PubMed] [Google Scholar]
- 8.Goyal A, Tanwar M, Joshi D, Chaudhary D. Practice Guidelines for the Management of Multiligamentous Injuries of the Knee. Indian J Orthop. 2017;51(05):537–544. doi: 10.4103/ortho.IJOrtho_228_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fanelli G C, Stannard J P, Stuart M J. Management of complex knee ligament injuries. J Bone Joint Surg Am. 2010;92(12):2235–2246. [PubMed] [Google Scholar]
- 10.Kupczik F, Shiavon M E, Vieira L, Genius D, Fávaro R. Luxação do joelho: Estudo descritivo das lesões. Rev Bras Ortop. 2013;48(02):145–151. doi: 10.1016/j.rboe.2012.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Vaidya R, Roth M, Nanavati D, Prince M, Sethi A. Low-Velocity Knee Dislocations in Obese and Morbidly Obese Patients. Orthop J Sports Med. 2015;3(04):2.325967115575719E15. doi: 10.1177/2325967115575719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Medina O, Arom G A, Yeranosian M G, Petrigliano F A, McAllister D R. Vascular and nerve injury after knee dislocation: a systematic review. Clin Orthop Relat Res. 2014;472(09):2621–2629. doi: 10.1007/s11999-014-3511-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Engebretsen L, Risberg M A, Robertson B, Ludvigsen T C, Johansen S. Outcome after knee dislocations: a 2-9 years follow-up of 85 consecutive patients. Knee Surg Sports Traumatol Arthrosc. 2009;17(09):1013–1026. doi: 10.1007/s00167-009-0869-y. [DOI] [PubMed] [Google Scholar]
- 14.Knee Dislocation Study Group . Levy B A, Fanelli G C, Whelan D B. Controversies in the treatment of knee dislocations and multiligament reconstruction. J Am Acad Orthop Surg. 2009;17(04):197–206. doi: 10.5435/00124635-200904000-00001. [DOI] [PubMed] [Google Scholar]
- 15.Howells N R, Brunton L R, Robinson J, Porteus A J, Eldridge J D, Murray J R. Acute knee dislocation: an evidence based approach to the management of the multiligament injured knee. Injury. 2011;42(11):1198–1204. doi: 10.1016/j.injury.2010.11.018. [DOI] [PubMed] [Google Scholar]
- 16.LaPrade R F, Muench C, Wentorf F, Lewis J L. The effect of injury to the posterolateral structures of the knee on force in a posterior cruciate ligament graft: a biomechanical study. Am J Sports Med. 2002;30(02):233–238. doi: 10.1177/03635465020300021501. [DOI] [PubMed] [Google Scholar]
- 17.Medronho R, Bloch K V, Luiz R R, Werneck G L. 2 a . ed. . São Paulo: Atheneu; 2009. [Google Scholar]
- 18.Pagano M, Gauvreau K. São Paulo: Pioneira Thomson Learning; 2004. Princípios de Bioestatísitca. [Google Scholar]