

Abstract
Objectives
This study aimed to evaluate the effect of brace treatment on the stress level and quality of life (QoL) of adolescents with idiopathic scoliosis.
Patients and methods
A total of 194 adolescent individuals were evaluated in two groups: the adolescent idiopathic scoliosis (AIS) group with 97 patients (20 males, 77 females; mean age: 13.9±1.8 years; range 10 to 18 years) and the control group with 97 age-and sex-matched participants (20 males, 77 females; mean age: 14.3±1.7 years; range 10 to 18 years) with no spinal deformity. The AIS group wore the Milwaukee brace or a thoracolumbosacral orthosis based on the location of the apical vertebra. All participants of the AIS group filled the Persian versions of the revised Scoliosis Research Society 22-item questionnaire (SRS-22r), the eight-item Bad Sobernheim Stress Questionnaire (BSSQ)-Deformity, and BSSQ-Brace. The control group only answered the first 20 items (subtotal items) of the SRS-22r. The brace-related QoL and stress level were assessed based on sex, brace, and deformity types.
Results
The subtotal score of the SRS-22r in the AIS group was significantly lower than the control group (p<0.001). There was a significant difference between deformity-related stress and brace-related stress (p<0.001). Regarding the type of treatment, there were no significant differences in QoL and stress level between the Milwaukee brace and thoracolumbosacral orthosis groups (p>0.05). Moreover, there was a weak correlation between the BSSQ-Brace and the self-image, mental-health scores, and the total scores of the SRS-22r (r=0.39 to 0.42, p<0.001); the low level of perceived stress was associated with a high level of perceived QoL.
Conclusion
The stress due to brace treatment can decrease function/activity and self-image of adolescents with idiopathic scoliosis.
Keywords: Adolescent idiopathic scoliosis, brace, quality of life, self-image, stress
Introduction
Adolescent idiopathic scoliosis (AIS) affects 0.5 to 5.2% of people aged 10 to 16 years worldwide.[1] It is a progressive condition associated with psychosocial consequences.[2] An untreated curve greater than 30° is at risk of progression and needs surgical intervention.[3] Therefore, conservative approaches such as bracing and exercises, the most common nonsurgical treatments for immature patients with AIS, are needed to control the further curve progression.
In the assessment of the brace treatment’s effectiveness in AIS, several radiological and clinical parameters, including skeletal maturity,[4] curve flexibility,[5] curve magnitude,[6] and curve pattern,[7] must be considered. In addition, we should consider health-related quality of life (QoL) variables of AIS cases to evaluate the outcomes of treatment types as clinical and radiological parameters.[8]
Due to an individual’s concern about their body development and the significance of peer pressure in adolescence, scoliosis is a significant risk factor in creating psychosocial issues that may lead to alcohol consumption and suicidal thoughts.[9] The self-image of AIS patients can affect their cognition, thinking, and behavior. Therefore, QoL in AIS patients is mainly associated with psychological coping mechanisms rather than radiological parameters.[8]
The effect of brace treatment on body function, mental health, and psychosocial parameters in adolescents with AIS is still in debate. Some studies showed that brace treatment may increase the patients’ level of anxiety, stress, and depression and decrease self-esteem and QoL.[10-12] Increased stress level is related to decrease in brace compliance in different age groups, particularly adolescent girls.[13] In addition, some studies suggest that brace treatment has no significant effect on health-related QoL of AIS patients.[14,15] Cultural differences, brace type, and sex can be some of the reasons for these discrepancies in the previous studies.[16]
This study aimed to assess the effect of brace type and its treatment on stress levels and QoL of adolescents with idiopathic scoliosis compared to adolescents with no spinal deformity.
Patients and Methods
This cross-sectional case-control study was conducted between November 2020 and January 2021. A total of 194 adolescents were evaluated in two groups: the AIS group with 97 patients (20 males, 77 females; mean age: 13.9±1.8 years; range 10 to 18 years) and the control group with 97 participants (20 males, 77 females; mean age: 14.3±1.7 years; range 10 to 18 years) without spinal deformities (Table 1). The mean age of male participants was 14.3±2.5 and 16.1±1.3 years in the AIS and control groups, respectively. The mean age of female participants was 13.9±1.7 and 13.8±1.4 years in the AIS and control groups, respectively. The inclusion criteria of the AIS group were having idiopathic scoliosis, a major Cobb angle of 20° to 45°, having worn a brace for at least three months, and having no history of spinal surgery. The control group included participants matched with the AIS group based on sex and age. Based on the location of the major curve, the patients were prescribed a Milwaukee brace or thoracolumbosacral orthosis (TLSO). The Milwaukee brace was prescribed to patients in whom the apex of the curve was at or above the T8 vertebra. The TLSO was prescribed to those in whom the apex of the curve was below the T8 vertebra.[17] All braces were fabricated for each patient by a qualified orthotist, and their appropriateness was confirmed by the prescribing surgeon. The patients were asked to wear the braces for 23 hours a day. Patients in the AIS group filled the Persian versions of the revised Scoliosis Research Society 22-item questionnaire (SRS-22r)[14] and the eight-item Bad Sobernheim Stress Questionnaire (BSSQ).[18] The participants in the control group were asked to respond to the first 20 items (subtotal items) of the Persian SRS-22r. All female participants wore a hijab as part of their faith. Hijab refers to a modest dressing, covering the head and body using a headscarf and a long coat or manteau.
Table 1. Demographic data of the participants.
| Adolescents with idiopathic scoliosis (n=97) | Adolescents without spinal deformity (n=97) | ||
| Variables | Mean±SD | Mean±SD | p |
| Age (year) | 13.9±1.8 | 14.3±1.7 | 0.18 |
| Weight (kg) | 48.7±12.0 | 54.4±12.9 | 0.002 |
| Height (cm) | 159.8±11.0 | 163.9±11.7 | 0.01 |
| BMI (kg/m2) | 19.0±3.1 | 20.3±4.0 | 0.01 |
| SD: Standard deviation; BMI: Body mass index. | |||
The SRS-22r is a disease-specific and patient- reported questionnaire[19] that has five subsections: (i) function/activity (five items); (ii) pain (five items); (iii) self-image/appearance (five items); (iv) mental health (five items); and (v) satisfaction with treatment (two items). It is scored on a 5-point Likert scale from 1 (worst) to 5 (best). For each subsection, the scores range from 5 to 25 (except for the satisfaction with treatment subsection that ranges from 2 to 10). The average scores of the function/activity, pain, self-image/ appearance, and mental health subsections can be a maximum subtotal score of 100. The total score ranges from 22 to 110. A higher score means a better QoL. The patients in the AIS group were asked to answer all of the questions in the SRS-22r, while the items in the satisfaction with treatment subsection (question 21 and 22) were removed from the questionnaire for the control group.
The deformity-and brace-related stress of AIS patients was evaluated using the Persian version of the BSSQ-Deformity and BSSQ-Brace, respectively.[18] The deformity version focuses on the impact of deformity on a patient’s mood, acceptance, and interactions with society.[20] The brace version focuses on the brace-related mood, social interactions, and subsequent stress levels.[21] The BSSQ has eight items with a 4-point Likert scale from 0 (highest level of stress) to 3 (lowest level of stress). The total score ranges from 0 to 24. The total score can be divided into three levels according to the level of stress: a score of 0 to 8 reveals a high level of stress, 9 to 16 indicates a moderate level of stress, and 17 to 24 demonstrates a low level of stress. All the participants of the AIS group answered the BSSQ-Deformity and BSSQ-Brace.
Statistical analysis
Statistical analyses were performed using the IBM SPSS version 20.0 software (IBM Corp., Armonk, NY, USA). The sample size was determined by analyzing the differences between the two independent means of the two groups. Therefore, a priori analysis revealed that for a power of 0.95, α error of 0.05 and effect size of 0.5, a minimum of 88 cases are needed in each group. Descriptive statistics were reported as means and standard deviations. Data normality was checked with the Kolmogorov-Smirnov test. The independent samples t-test was used to compare the brace-related QoL and stress level scores regarding participants’ sex, brace type, and presence of spinal deformity.
We used Pearson’s correlation coefficient to evaluate the relationship between the subsections of SRS-22r and BSSQ. The relationship strength was considered as strong (r>0.75), moderate (0.50<r<0.75), weak (0.25<r<0.50), and little to no correlation (r<0.25).[22] A threshold of 0.05 was considered the statistical significance level, with 95% confidence intervals (CIs) for all correlation coefficients. The graphs were created with the GraphPad Prism version 8.0 software (GraphPad Prism Software Inc., San Diego, CA, USA).
Results
The mean Cobb angle at the time of brace treatment was 33.04±7.21° (24° to 45°). The mean brace wearing time for all AIS cases was 17.84±16.62 (range, 4 to 84) months. At the beginning of brace treatment, 21 (21.6%) participants had thoracic curve, 12 (12.4%) participants thoracolumbar curve, 14 (14.4%) participants lumbar curve, and 50 (51.6%) participants double major curve.
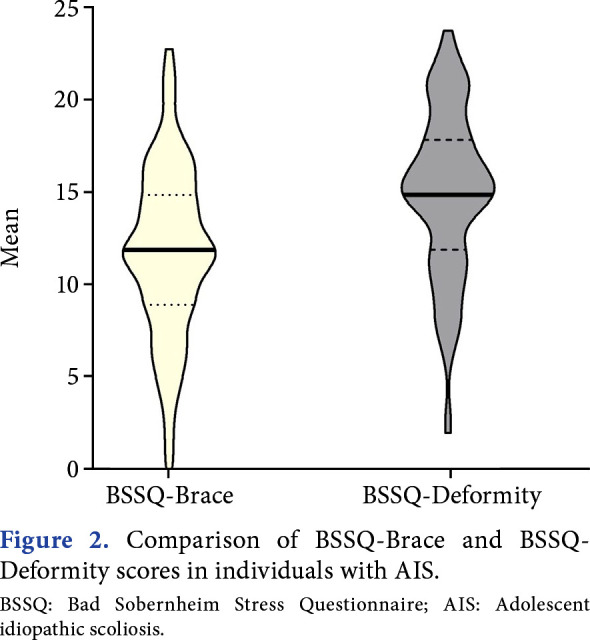
There was a significant difference in subtotal scores of SRS-22r (the average scores of the function/activity, pain, self-image/appearance, and mental health subsections) between AIS patients (3.27±0.51) and the control group (4.06±0.54) (p<0.001). In addition, compared to adolescents without spinal deformity, function/activity and self-image subsection scores were significantly lower than those of patients with AIS (p<0.001) (Figure 1). Additionally, there was a significant difference between deformity-related stress (15.11±4.53) and brace-related stress (11.89±4.65) (p<0.001) (Figure 2). The mean increase in stress level score was 3.22 with a 95% CI ranging from 2.30 to 4.15.
Figure 1. Comparison of the function/activity, pain, self- image, mental health, and subtotal scores of SRS-22r between adolescents with idiopathic scoliosis and those with no spinal deformity. SRS-22r: Scoliosis Research Society 22-item questionnaire;

Figure 2. Comparison of BSSQ-Brace and BSSQ- Deformity scores in individuals with AIS. BSSQ: Bad Sobernheim Stress Questionnaire; AIS: Adolescent idiopathic scoliosis.
The total and subsection scores of the SRS-22r and BSSQ in respect to Milwaukee brace and TLSO are shown in Table 2. There were no significant differences in QoL and stress level between those who wore Milwaukee brace and TLSO (p>0.05).
Table 2. Comparison of QoL and stress level between Milwaukee brace and TLSO groups.
| Parameters | Milwaukee brace (n=71) | TLSO (n=26) | p |
| Mean±SD | Mean±SD | ||
| SRS-22r Function/activity | 3.8±0.6 | 3.9±0.7 | 0.51 |
| SRS-22r Pain | 4.2±0.6 | 4.3±0.5 | 0.51 |
| SRS-22r Self-image/appearance | 3.2±0.8 | 3.1±0.6 | 0.36 |
| SRS-22r Mental-health | 3.7±0.8 | 3.9±0.8 | 0.77 |
| SRS-22r Satisfaction | 3.8±0.8 | 4.0±4.7 | 0.26 |
| SRS-22r Total | 3.7±0.5 | 3.8±0.5 | 0.38 |
| BSSQ-Deformity | 15.1±4.7 | 15.0±4.1 | 0.68 |
| BSSQ-Brace | 11.9±4.9 | 11.9±3.9 | 0.35 |
| QoL: Quality of life; TLSO: Thoracolumbosacral orthosis; SD: Standard deviation; SRS-22r: Scoliosis Research Society 22-item questionnaire; BSSQ: Bad Sobernheim Stress Questionnaire. | |||
The relationship between perceived brace-related stress (measured with BSSQ-Brace) and perceived QoL (measured with SRS-22r) was evaluated using Pearson’s correlation coefficient. There was a weak, positive correlation between BSSQ-Brace and the self-image, mental health, and the total scores of SRS-22r (r range of 0.39 to 0.42, p<0.001; with a low level of perceived stress associated with a higher level of perceived QoL) (Table 3).
Table 3. Correlations between BSSQ-Brace and QoL.
| SRS-22r | |||||||
| Questionnaires | Function | Pain | Self-image | Mental-health | Satisfaction | Total | |
| r | 0.25 | 0.14 | 0.42 | 0.39 | 0.19 | 0.41 | |
| BSSQ-Brace | p-value | 0.01 | 0.16 | <0.001 | <0.001 | 0.06 | <0.001 |
| 95% CI | 0.08 to 0.41 | -0.002 to 0.33 | 0.23 to 0.61 | 0.24 to 0.57 | 0.01 to 0.29 | 0.26 to 0.58 | |
| BSSQ: Bad Sobernheim Stress Questionnaire; QoL: Quality of life; SRS-22r: Scoliosis Research Society 22-item questionnaire; CI: Configuration item. | |||||||
Considering the perceived stress level and QoL regarding the participants’ sex, results of the independent samples t-test demonstrated that there were no significant differences between males and females in BSSQ and SRS-22r scores (p>0.05) (Table 4).
Table 4. Quality of life and stress level between boys and girls with AIS.
| Parameters | Boys (n=20) | Girls (n=77) | p |
| Mean±SD | Mean±SD | ||
| SRS-22r Function/activity | 4.1±0.5 | 3.7±0.7 | 0.33 |
| SRS-22r Pain | 4.3±0.5 | 4.2±0.6 | 0.75 |
| SRS-22r Self-image | 3.4±0.6 | 3.1±0.7 | 0.45 |
| SRS-22r Mental-health | 4.0±0.6 | 3.7±0.8 | 0.08 |
| SRS-22r Satisfaction | 3.7±0.9 | 3.9±0.7 | 0.06 |
| SRS-22r Total | 3.9±0.4 | 3.7±0.5 | 0.08 |
| BSSQ-Deformity | 17.6±3.2 | 14.5±4.6 | 0.10 |
| BSSQ-Brace | 13.1±5.1 | 11.6±4.5 | 0.93 |
| AIS: Adolescent idiopathic scoliosis; SD: Standard deviation; SRS-22r: Scoliosis Research Society 22-item questionnaire; BSSQ: Bad Sobernheim Stress Questionnaire. | |||
Discussion
Our study aimed to assess the effect of wearing braces on stress levels and QoL of adolescents with idiopathic scoliosis, revealing that they have a lower QoL compared to their age-and sex-matched peers with no spinal deformity. Furthermore, the stress level associated with the brace was higher than the stress level associated with the deformity. However, there was a moderate perceived stress level between those who wore the Milwaukee brace and TLSO. There were no significant differences between males and females in BSSQ and SRS-22r scores.
The image of body deformity is a prime concern in AIS.[23] Adolescent idiopathic scoliosis patients may notice changes in their bodies and compare themselves with people without a spinal deformity.[9] Having a negative self-image may lead to various reactions, such as dissatisfaction with one's body, social isolation, and mental health disorders,[24,25] all of which may be aggravated by wearing a brace.[26,27] Reichel and Schanz[26] reported that a great concern among females with AIS is to receive negative comments and statements from others when they are wearing a brace.
Studies show that stress levels and QoL scores can be affected by brace type,[10] sex,[16] and curve magnitude[28] in adolescents with idiopathic scoliosis. In this study, we detected no significant difference in brace-related stress and QoL parameters between patients who use Milwaukee brace and TLSO. They equally affected the stress levels and QoL of our participants. Function/activity, self-image, and subtotal scores of SRS-22r were lower in braced patients compared to the healthy participants. These findings are consistent with the study of Babaee et al.[16] Regarding the effects of brace type on psychosocial parameters, Misterska et al.[10] conducted a study on 71 AIS patients. They found out that those who used the Chêneau brace had better emotional and social function and satisfaction with their body curve compared to those who were treated with a SpineCor brace. In this regard, Climent et al.[29] showed that patients treated with a Milwaukee brace have a lower QoL compared to those treated with a TLSO. A possible reason for the difference between our findings and these studies can be the cultural differences between the study populations. The level of QoL can be different between people with different cultural backgrounds.[30] A problem with the Milwaukee brace is its visible neck ring and superstructure, which can decrease the patient’s self-image[17] and brace compliance.[31] There is a direct relationship between psychosocial issues such as peer pressure at school, social relations, and brace compliance.[32] However, based on the findings of Korovessis et al.,[33] when AIS patients use their braces under special school uniforms, brace compliance increases and concerns about others seeing the brace decrease. In our study, since most of the participants preferred an Islamic clothing style (Hijab) in their social activities, their concerns about the visibility of the neck ring of the Milwaukee brace were minimized.
Another factor affecting QoL and stress levels in adolescents with AIS is the patient’s sex. Gratz et al.[34] showed that due to a negative body image, female AIS patients are more pronte to stop doing their favorite activities or having social interactions compared to male patients. Sapountzi-Krepia et al.[35] found that female AIS patients have more self-image disorders compared to males, and lower happiness and life satisfaction compared to normal healthy girls. Moreover, Aulisa et al.[36] determined that males are in better conditions compared to females from different aspects, such as social relevance and function, stress level, school activity, emotional functioning, self-image, vitality, and pain. Nonetheless, our findings are different from the previous studies regarding sex. We discovered that subsection scores of SRS-22r, BSSQ-Deformity, and BSSQ-Brace are not significantly different between the sexes. A possible cause could be the female clothing styles in our country. Another possible reason might be the number of males who participated in our study. Therefore, this findings should be interpreted with caution. Another study conducted on 928 females and 277 males with and without AIS also reported similar total SRS-22r scores in both sexes.[37]
Since wearing a brace can affect the stress level and QoL of patients with AIS, we assumed that there should be a significant relationship between the subsections of SRS-22r, BSSQ-Brace, and BBSQ-Deformity. There was a significant relationship between the subsections of SRS-22r and the brace and deformity-related stress except for the pain and satisfaction subsections. The strongest relationship was between BSSQ-Brace and self-image and the total scores of SRS-22r. These findings are in line with those of Misterska et al.[12] Appearance has an important role in social interactions and experiences. A brace can inf luence the self-perception of adolescents with idiopathic scoliosis. A negative self-perception can lead to increased levels of stress and anxiety, lower self-esteem, QoL, and depression. People who have different appearances than the norm might experience different social behaviors, including being stared at or pointed out in public. Studies show that stress, timidity, and anxiety resulting from visible dissimilarity can lead to social isolation.[38] This is a crucial issue for future research.
One of the limitations of the study is that there were more females included than males in both groups, which could be due to the higher prevalence of AIS in females.[39] In addition, AIS patients with a curve magnitude of more than 45° were not included in this study. Recently, some authors concluded that bracing is an effective strategy for controlling the AIS curves higher than 45°.[40] Future studies on the brace-related stress and QoL in patients with AIS curves higher than 45° are therefore recommended. In addition, an issue that was not addressed in this study was whether the difference of body mass index (BMI) values between AIS patients and adolescents with no spinal deformity could affect QoL scores. To our knowledge, there are no data on the effect of BMI on the QoL of braced adolescents with idiopathic scoliosis. In their study, Cheung et al.[27] showed that the SRS-22r scores of adolescents with AIS undergoing brace treatment are not significantly different from adolescents with no spinal deformity regarding BMI.
In conclusion, the stress due to brace treatment can decrease function/activity and self-image of adolescents with idiopathic scoliosis compared to age-and sex-matched adolescents without spinal deformity.
Footnotes
Ethics Committee Approval: The study protocol was approved by the University of Social Welfare and Rehabilitation Sciences Ethichs Committee (no: 1399.195). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Author Contributions: Methodology: H.P., T.B., B.B., M.A.; Investigation; T.B., B.B., Z.J., R.V.K.; Writing-original draft; T.B., H.P., B.B., M.A.; Resources: M.A.; Supervision: M.A.; Interpretation: All authors; Final approval: All authors.
Financial Disclosure: This study was supported by the Research Committee of University of Social Welfare and Rehabilitation Sciences (Letter No. IR.USWR.REC.1399.195).
Patient Consent for Publication: Written informed consent was obtained from the participants’ parents.
References
- 1.Dunn J, Henrikson NB, Morrison CC, Blasi PR, Nguyen M, Lin JS. Screening for adolescent idiopathic scoliosis: Evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2018;319:173–187. doi: 10.1001/jama.2017.11669. [DOI] [PubMed] [Google Scholar]
- 2.Savvides P, Gerdhem P, Grauers A, Danielsson A, Diarbakerli E. Self-experienced trunk appearance in individuals with and without idiopathic scoliosis. Spine (Phila Pa 1976) 2020;45:522–527. doi: 10.1097/BRS.0000000000003308. [DOI] [PubMed] [Google Scholar]
- 3.Grothaus O, Molina D, Jacobs C, Talwalkar V, Iwinski H, Muchow R. Is it growth or natural history. Increasing spinal deformity after Sanders stage 7 in females with AIS. e176-e181J Pediatr Orthop. 2020;40 doi: 10.1097/BPO.0000000000001415. [DOI] [PubMed] [Google Scholar]
- 4.Karol LA, Virostek D, Felton K, Jo C, Butler L. The effect of the Risser stage on bracing outcome in adolescent idiopathic scoliosis. J Bone Joint Surg [Am] 2016;98:1253–1259. doi: 10.2106/JBJS.15.01313. [DOI] [PubMed] [Google Scholar]
- 5.He C, Wong MS. Spinal flexibility assessment on the patients with adolescent idiopathic scoliosis: A literature review. E250-E258Spine (Phila Pa 1976) 2018;43 doi: 10.1097/BRS.0000000000002276. [DOI] [PubMed] [Google Scholar]
- 6.Hawary RE, Zaaroor-Regev D, Floman Y, Lonner BS, Alkhalife YI, Betz RR. Brace treatment in adolescent idiopathic scoliosis: Risk factors for failure-a literature review. Spine J. 2019;19:1917–1925. doi: 10.1016/j.spinee.2019.07.008. [DOI] [PubMed] [Google Scholar]
- 7.Thompson RM, Hubbard EW, Jo CH, Virostek D, Karol LA. Brace success is related to curve type in patients with adolescent idiopathic scoliosis. J Bone Joint Surg [Am] 2017;99:923–928. doi: 10.2106/JBJS.16.01050. [DOI] [PubMed] [Google Scholar]
- 8.Rivett L, Rothberg A, Stewart A, Berkowitz R. The relationship between quality of life and compliance to a brace protocol in adolescents with idiopathic scoliosis: A comparative study. BMC Musculoskelet Disord. 2009;10:5–5. doi: 10.1186/1471-2474-10-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Payne WK 3rd, Ogilvie JW, Resnick MD, Kane RL, Transfeldt EE, Blum RW. Does scoliosis have a psychological impact and does gender make a difference. Spine (Phila Pa 1976) 1997;22:1380–1384. doi: 10.1097/00007632-199706150-00017. [DOI] [PubMed] [Google Scholar]
- 10.Misterska E, Glowacki J, Kołban M. Does rigid spinal orthosis carry more psychosocial implications than the flexible brace in AIS patients. A cross-sectional study. J Back Musculoskelet Rehabil. 2019;32:101–109. doi: 10.3233/BMR-181121. [DOI] [PubMed] [Google Scholar]
- 11.Lin T, Meng Y, Ji Z, Jiang H, Shao W, Gao R, et al. Extent of depression in juvenile and adolescent patients with idiopathic scoliosis during treatment with braces. e27-e32World Neurosurg. 2019;126 doi: 10.1016/j.wneu.2019.01.095. [DOI] [PubMed] [Google Scholar]
- 12.Misterska E, Glowacki M, Latuszewska J, Adamczyk K. Perception of stress level, trunk appearance, body function and mental health in females with adolescent idiopathic scoliosis treated conservatively: A longitudinal analysis. Qual Life Res. 2013;22:1633–1645. doi: 10.1007/s11136-012-0316-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kotwicki T, Kinel E, Stryła W, Szulc A. Estimation of the stress related to conservative scoliosis therapy: An analysis based on BSSQ questionnaires. Scoliosis. 2007;2:1–1. doi: 10.1186/1748-7161-2-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mousavi SJ, Mobini B, Mehdian H, Akbarnia B, Bouzari B, Askary-Ashtiani A, et al. Reliability and validity of the Persian version of the Scoliosis Research Society-22r questionnaire. Spine (Phila Pa 1976) 2010;35:784–789. doi: 10.1097/BRS.0b013e3181bad0e8. [DOI] [PubMed] [Google Scholar]
- 15.Danielsson AJ, Hasserius R, Ohlin A, Nachemson AL. Health-related quality of life in untreated versus brace- treated patients with adolescent idiopathic scoliosis: A long- term follow-up. Spine (Phila Pa 1976) 2010;35:199–205. doi: 10.1097/BRS.0b013e3181c89f4a. [DOI] [PubMed] [Google Scholar]
- 16.Babaee T, Kamyab M, Ganjavian MS, Kamali M. Milwaukee brace or thoracolumbosacral orthosis? Which one affects the quality of life of adolescents with idiopathic scoliosis more? A cross-sectional study using the SRS-22 questionnaire. Current Orthopaedic Practice. 2014;25:478–483. [Google Scholar]
- 17.Hsu JD, Michael JW, Fisk JR. In: AAOS Atlas of Orthoses and Assistive Devices. Katz DE, editor. Philadelphia: Elsevier; 2008. Orthoses for spinal deformities; pp. 125–139. [Google Scholar]
- 18.Rezaei Motlagh F, Pezham H, Babaee T, Saeedi H, Hedayati Z, Kamali M. Persian adaptation of the Bad Sobernheim stress questionnaire for adolescent with idiopathic scoliosis. Disabil Rehabil. 2020;42:562–566. doi: 10.1080/09638288.2018.1503728. [DOI] [PubMed] [Google Scholar]
- 19.Asher M, Min Lai S, Burton D, Manna B. The reliability and concurrent validity of the Scoliosis Research Society-22 patient questionnaire for idiopathic scoliosis. Spine (Phila Pa 1976) 2003;28:63–69. doi: 10.1097/00007632-200301010-00015. [DOI] [PubMed] [Google Scholar]
- 20.Weiss HR, Reichel D, Schanz J, Zimmermann-Gudd S. Deformity related stress in adolescents with AIS. Stud Health Technol Inform. 2006;123:347–351. [PubMed] [Google Scholar]
- 21.Weiss HR, Werkmann M, Stephan C. Brace related stress in scoliosis patients - Comparison of different concepts of bracing. Scoliosis. 2007;2:10–10. doi: 10.1186/1748-7161-2-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Portney L, Watkins MP, editors . Upper Saddle River: Prentice Hall Health; Philadelphia: F. 2015 Foundations of clinical research: application to practice. [Google Scholar]
- 23.Bago J, Matamalas A, Sánchez-Raya J, Pellise F, Pérez-Grueso FJS. Responsiveness of image perception outcome scales after surgical treatment of idiopathic scoliosis: A comparison between the Trunk Appearance Perception Scale (TAPS) and Scoliosis Research Society-22 (SRS-22) questionnaire. Spine Deform. 2018;6:417–423. doi: 10.1016/j.jspd.2017.12.010. [DOI] [PubMed] [Google Scholar]
- 24.Thompson A, Kent G. Adjusting to disfigurement: Processes involved in dealing with being visibly different. Clin Psychol Rev. 2001;21:663–682. doi: 10.1016/s0272-7358(00)00056-8. [DOI] [PubMed] [Google Scholar]
- 25.Matsunaga S, Hayashi K, Naruo T, Nozoe S, Komiya S. Psychologic management of brace therapy for patients with idiopathic scoliosis. Spine (Phila Pa 1976) 2005;30:547–550. doi: 10.1097/01.brs.0000154648.53535.52. [DOI] [PubMed] [Google Scholar]
- 26.Reichel D, Schanz J. Developmental psychological aspects of scoliosis treatment. Pediatr Rehabil. 2003;6:221–225. doi: 10.1080/13638490310001644593. [DOI] [PubMed] [Google Scholar]
- 27.Cheung PWH, Wong CKH, Cheung JPY. An insight into the health-related quality of life of adolescent idiopathic scoliosis patients who are braced, observed, and previously braced. E596-E605Spine (Phila Pa 1976) 2019;44 doi: 10.1097/BRS.0000000000002918. [DOI] [PubMed] [Google Scholar]
- 28.Khoshhal Y, Jalali M, Babaee T, Ghandhari H, Gum JL. The effect of bracing on spinopelvic rotation and psychosocial parameters in adolescents with idiopathic scoliosis. Asian Spine J. 2019;13:1028–1035. doi: 10.31616/asj.2018.0307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Climent JM, Sánchez J. Impact of the type of brace on the quality of life of adolescents with spine deformities. Spine (Phila Pa 1976) 1999;24:1903–1908. doi: 10.1097/00007632-199909150-00007. [DOI] [PubMed] [Google Scholar]
- 30.Watanabe K, Lenke LG, Bridwell KH, Hasegawa K, Hirano T, Endo N, et al. Cross-cultural comparison of the Scoliosis Research Society outcomes instrument between American and Japanese idiopathic scoliosis patients: Are there differences. Spine (Phila Pa 1976) 2007;32:2711–2714. doi: 10.1097/BRS.0b013e31815a7ef0. [DOI] [PubMed] [Google Scholar]
- 31.Sharifi P, Kamyab M, Babaee T, Ganjavian MS. Objective monitoring of brace wearing time in adolescents with Scheuermann's kyphosis. Asian Spine J. 2019;13:942–948. doi: 10.31616/asj.2019.0008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hasler CC, Wietlisbach S, Büchler P. Objective compliance of adolescent girls with idiopathic scoliosis in a dynamic SpineCor brace. J Child Orthop. 2010;4:211–218. doi: 10.1007/s11832-010-0249-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Korovessis P, Zacharatos S, Koureas G, Megas P. Comparative multifactorial analysis of the effects of idiopathic adolescent scoliosis and Scheuermann kyphosis on the self-perceived health status of adolescents treated with brace. Eur Spine J. 2007;16:537–546. doi: 10.1007/s00586-006-0214-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Gratz RR, Papalia-Finlay D. Psychosocial adaptation to wearing the Milwaukee brace for scoliosis. A pilot study of adolescent females and their mothers. J Adolesc Health Care. 1984;5:237–242. doi: 10.1016/s0197-0070(84)80124-2. [DOI] [PubMed] [Google Scholar]
- 35.Sapountzi-Krepia DS, Valavanis J, Panteleakis GP, Zangana DT, Vlachojiannis PC, Sapkas GS. Perceptions of body image, happiness and satisfaction in adolescents wearing a Boston brace for scoliosis treatment. J Adv Nurs. 2001;35:683–690. doi: 10.1046/j.1365-2648.2001.01900.x. [DOI] [PubMed] [Google Scholar]
- 36.Aulisa AG, Guzzanti V, Perisano C, Marzetti E, Specchia A, Galli M, et al. Determination of quality of life in adolescents with idiopathic scoliosis subjected to conservative treatment. Scoliosis. 2010;5:21–21. doi: 10.1186/1748-7161-5-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rainoldi L, Zaina F, Villafañe JH, Donzelli S, Negrini S. Quality of life in normal and idiopathic scoliosis adolescents before diagnosis: Reference values and discriminative validity of the SRS-22. A cross-sectional study of 1,205 pupils. Spine J. 2015;15:662–667. doi: 10.1016/j.spinee.2014.12.004. [DOI] [PubMed] [Google Scholar]
- 38.Moss TP. The relationships between objective and subjective ratings of disfigurement severity, and psychological adjustment. Body Image. 2005;2:151–159. doi: 10.1016/j.bodyim.2005.03.004. [DOI] [PubMed] [Google Scholar]
- 39.Hsu JD, Michael JW, Fisk JR. In: AAOS Atlas of Orthoses and Assistive Devices. Condie DN, editor. Philadelphia: Elsevier; 2008. International Organization for Standardization (ISO) terminology; pp. 3–7. [Google Scholar]
- 40.Verhofste BP, Whitaker AT, Glotzbecker MP, Miller PE, Karlin LI, Hedequist DJ, et al. Efficacy of bracing in skeletally immature patients with moderate-severe idiopathic scoliosis curves between 40° and 60°. Spine Deform. 2020;8:911–920. doi: 10.1007/s43390-020-00131-3. [DOI] [PubMed] [Google Scholar]