

ABSTRACT
Objective:
Implant abutment screws can fracture due to various biomechanical factors. Improper fit of the prosthesis, inadequate seating of the abutment, occlusal interference, and manufacturing errors are some of the causes that can result in an abutment screw fracture. Retrieval of the retained fractured abutment screw is quite challenging to the clinician. The objective of this review is to provide information on various fractured abutment screw retrieval techniques reported in literature and to formulate a structured treatment protocol for the management of fractured abutment screws.
Materials and Methods:
An electronic search of Scopus and PubMed databases was performed for articles between January 1989 and December 2021 using the keywords “Implant screw fracture” and “screw retrieval.”
Results:
Most of the articles were of the opinion that abutment screw fractures occurred due to screw loosening. Both conservative approaches and the use of commercial retrieval kits have been advocated to retrieve the fractured abutment screws. Based on various review articles, an innovative novel technique to retrieve an abutment screw fractured due to excessive torque was devised in our unit.
Conclusion:
Although clinicians can use various techniques to remove fractured abutment screws, every effort should be made to eliminate the cause of screw fracture. Retrieval of the broken screw fragment should be done judiciously to prevent any internal damage to the implant structure.
KEYWORDS: Abutment screw retrieval, implant abutment screw fracture, implant abutment screw loosening
INTRODUCTION
Technical issues leading to failure of implant-supported restorations can occur due to problems related to the implant components and the prosthesis.[1,2] The implants are structurally strong to withstand the intense masticatory load.[3] Yet, implant abutment fractures have been reported due to screw loosening or as a result of abutment micro-movements.[4] The incidence of screw loosening was found in 25% of patients during routine follow-up.[5] Complications associated with the hardware, such as implant screw loosening, are common in single tooth implants.[6] Though screw loosening is the primary cause for abutment screw fractures, fractures due to excessive torque can also occur.
Though implant abutment screw fracture is uncommon (0.5–8%), the sheer difficulty in removing the fractured screw fragments makes its management challenging.[6,7,8,9] Fractured screw fragments, loosely engaged and not locked into the implant, can be easily retrieved with a sharp probe.[7,8] Difficulty in removal arises if the fractured abutment fragment is engaged tightly with the implant threads.[9,10] Retrieving a retained fractured abutment screw following excessive torque becomes challenging due to a lack of screw loosening. The retained fractured fragment is usually firmly embedded in the internal threading of the implant. Various methods for the retrieval of screw fragments from within the implant have been reported. Irreversible damage to the implants may occur when removal of the fractured screw fragment is attempted by low-speed rotary instruments.[10,11,12] When a fractured screw fragment removal becomes impossible or when a problematic retrieval results in damage to the internal threading of the implant, many clinicians choose removal and replacement of the implant or leave it behind unconnected to the superstructure.[10,11,12,13,14] However, once any fracture of an abutment screw has occurred, it is always desirable to remove it.[7]
Considering the various techniques described, the rationale for this review is to establish a current protocol in retrieval of fractured implant abutment screws without damaging the implant. Also, on the basis of various review articles, an innovative novel technique devised by the authors to retrieve an abutment screw fractured due to excessive torque is presented in this article. The objectives of the literature search were in accordance with the PICO statement: Participants (patients who underwent implant placement), Intervention (retrieval of fractured abutment screw), Comparisons (comparing various techniques employed for abutment screw retrieval), and Outcomes (ease or difficulty in retrieval of fractured abutment screws without damage to the dental implant).
MATERIALS AND METHODS
This review article reflects the current measures and tools employed in the retrieval of fractured implant abutment screws. A literature search was performed in PubMed/MEDLINE and Scopus databases for all published articles pertaining to implant abutment screw fractures from January 1989 to December 2021. The search terms used were “Implant screw fracture” and “screw retrieval.” The search generated 581 titles initially. Out of these, 462 articles were screened after removal of duplicates. About 430 articles were further excluded as they did not meet the eligibility criteria. This left us with 32 articles, out of which 15 articles were further excluded after full text screening. Finally, 17 articles were included in the final review [Figure 1]. Data extracted were of the study subject, intervention methods, different techniques used, and their outcomes.
Figure 1.

Flow chart of article selection
RESULT
There is no particular consensus on the technique to remove fractured abutment screws. Both conservative approaches and the use of commercial retrieval kits have been advocated to retrieve the fractured implant abutment screws. Most of the articles were of the opinion that abutment screw fractures occurred due to screw loosening. Abutment screw fractures occurring above the implant body were easier to retrieve when compared with those fracturing within the implant.
DISCUSSION
Clinicians have employed various methods to retrieve fractured implant abutment screws [Table 1]. A non-passive implant superstructure, manufacturing errors, and biomechanical overloading can lead to undetected screw loosening, which is the primary reason for screw fracture.[6,7,15] Improper fit of the prosthesis, inadequate seating of the abutment, and occlusal interference are some of the other causes that can result in an abutment screw fracture due to screw loosening.[6,10,15,16,17,18,19,20] The conservative approach in the management of abutment screw fractures is to retrieve the fractured screw to facilitate the reuse of the implant. When an abutment screw fractures above the implant body, the fractured screw is grasped with a hemostat, or a sharp explorer is used to remove it with a counterclockwise motion.[11,21] If the abutment screw fracture occurs within the body of the implant, retrieving the screw fragment will be more challenging. A modified spoon excavator can be used to engage the fractured screw after making a groove on it. The working end of the spoon excavator is cut perpendicularly to engage the groove on the fractured fragment.[22]
Table 1.
Articles on techniques in retrieving fractured implant abutment screws
| Number | Reference | Remedial measure employed |
|---|---|---|
| 1. | Nergiz et al.[7] | The implant repair system kit (IMZ TwinPlus Repair Set K 3.3; Dentsply Friadent) |
| 2. | Shah and Lee[8] (2016) | Replacement of two fractured, irretrievable, Locator abutment screws of a mandibular implant-retained overdenture with a cast dowel and laser welded Locator attachments. |
| 3. | Yilmaz and McGlumphy[9] | A specially designed forked-shaped end instrument from Astratech placed in a slow-speed handpiece with reverse torque to retrieve the fragment |
| 4. | Luterbacher et al.[10] | Used service set of ITI system when everything else failed |
| 5. | Harshakumar et al.[11] | Custom cast post and core |
| 6. | Canpolat et al.[12] | Fabricated a cast dowel to fit to the internal aspect of the implant for support of restoration |
| 7. | Williamson and Robinson[22] | The superior portion of the fracture screw was modified into a slot-like shape with a round bur. Another round bur was modified to engage the slot and a reverse torque was applied to remove the fractured screw |
| 8. | Satwalekar et al.[22] | Use of a modified spoon excavator to engage the fractured fragment after making a groove on the screw fragment |
| 9. | Gooty et al.[23] | Use of an ultrasonic scaler to engage a pit made on the occlusal surface of the fractured screw and loosen the fragment |
| 10. | Bhandari et al.[24] | Used the vibrating tip of a piezoelectric ultrasonic scaler on the top surface of the fractured screw with gentle reverse torque to spin it out of the screw hole |
| 11. | Chen and Cho[25] | An adhesive dental restoration holder was used to engage the top of the fragment and rotate it in the clockwise direction initially followed by counterclockwise direction |
| 12. | Chawali et al.[26] | Converted the healing abutment to a prosthetic abutment in irretrievable abutment screw fractures |
| 13. | Flanagan[17] | Modified a straight 557 bur from SS White by removing the lateral flukes and engaging it to the screw surface by moving in a counterclockwise direction to facilitate its removal |
| 14. | Sim et al.[27] | Introduced the concept of using a hollow abutment screw to facilitate its easy retrieval on fracturing |
| 15. | Imam et al.[28] | Suggested further driving in the fractured segment into the body of the implant by giving clockwise rotations and then backing it out after retapping threads above the fragment |
| 16. | Pipko et al.[29] | Fabricated a cast dowel to fit to the internal aspect of the implant for support of restoration |
| 17. | Yi et al.[30] | Use of a cut screw to reconnect the prostheses to the existing implants in case of a non-retrievable fractured screw |
| Removal of one fractured screw in the left mandibular posterior area, by rotating it counterclockwise by using a sharp explorer | ||
| Two fractured screw fragments in the maxillary premolar area were removed by counterclockwise rotation with an explorer and an ultrasonic scaler | ||
| Secured the existing prosthesis with a short screw cut to the length of the remaining internal threads in the maxillary right first molar implant |
Gooty et al.[23] proposed the use of an ultrasonic scaler to loosen a fractured screw successfully. A 1 mm pit is to be made on the occlusal surface of the fractured screw by using a round bur, and the scaler tip is placed in this slot to loosen the screw further. Also, the vibrating tip of a piezoelectric ultrasonic scaler can be run on the top surface of the fractured screw with gentle reverse torque to spin it out of the screw hole. The long non-cutting tip of the ultrasonic scaler provides good predictability to the procedure.[24] Chen and Cho[25] suggested the use of a TU17/23 double ended explorer from Hu-Friedy to rotate the fragment in a counterclockwise direction. If this technique failed, a stiffer hand scaler is used to engage the fractured surface. If the fragment is still not retrievable, an adhesive dental restoration holder (True Grip; Clinician’s Choice) is used to engage the top of the fragment and rotate it in the clockwise direction initially followed by counterclockwise direction.
A new innovative technique for management of irretrievable fractured abutment screws is to convert the healing abutment to a prosthetic abutment, particularly when the fracture occurs within the implant depth.[26] However, the height of the healing abutment should be sufficient enough to provide adequate retention for the prosthetic crown. Another innovative technique to retrieve a fractured abutment screw is by modifying a straight 557 bur from SS White, Longwood, NJ, USA.[17] The lateral flukes of the bur are removed with a stone and the end cutting blades are left intact. This bur is then placed against the fractured screw and rotated slowly in a counterclockwise direction. This facilitates movement of the broken screw out of the fixture.
The concept of using a hollow abutment screw to facilitate its easy retrieval on fracturing is one of the most versatile techniques in the retrieval of fractured abutment screws.[27] The hollow abutment screw consists of a 0.5 mm diameter hole extending from its lower tip up to the first thread. During fracture of the abutment screw, a H-file can be easily introduced into the existing hole and rotated in a counterclockwise direction to facilitate removal of the screw from the implant fixture.
When conservative approaches to retrieve the fractured screws failed, some authors advocated using commercial retrieval kits. The IMZ Twin Plus Repair Set K 3.3 (Dentsply Friadent, Mannheim, Germany) was used successfully to retrieve a fractured abutment screw.[7] The kit consists of three drill guides, four burs, one conical instrument to retrieve the fragment, and one tapping instrument. After roughening the fragment at its center, the 1.3 and 1.9 mm twist drills are used to perforate the fragment at its center, rotating in a clockwise direction. The drill guides are fixed on top of the implants to protect the internal aspect of the implants from the drills. Subsequently, the conical retriever instrument is inserted into the drilled hole, and the fragment is unscrewed.
Shah and Lee[8] fabricated custom-made laser-welded Locator abutments (Locator bar attachments; Zest Anchors) to replace fractured, irretrievable abutment screws of a mandibular implant-retained overdenture. A drawback of this technique is that after cementation, the attachment system cannot be replaced. A similar technique was advocated earlier by Canpolat et al.[12] After preparing the interior of the implant and the fractured screw, a custom-made cast dowel and ball attachment is prepared and cemented with glass ionomer cement. Imam et al.[28] suggested further driving of the fractured segment into the body of the implant by giving clockwise rotations and then backing it out after retapping threads above the fragment. A fork-shaped instrument from Astratech is used to drive the broken fragment deeper into the implant. The damaged implant threads are retapped using a Zimmer Dental retapping tool by rotating it initially in the clockwise direction and then subsequently in the counterclockwise direction. A forked screw retrieval tool is finally used to retrieve the fractured fragments.
If all other methods fail, the internal threads of the implant are removed to prepare space for a post. A tungsten carbide bur in a high-speed air rotor with copious irrigation is used for this purpose. The coronal portion of the fractured screw is removed, and an acrylic resin pattern fabrication for the post is done. Finally, the custom-made post and core are cemented to the implant.[11] Similarly, a cast dowel core can be fabricated to support a single implant crown. Here the authors propose to retrofit the cast dowel core fabrication to achieve accurate fit and retention.[29]
A specially designed fork-shaped end instrument from Astratech was used by Yilmaz and McGlumphy[9] to engage the fractured screw fragment. The device is placed in a slow-speed handpiece with reverse torque to retrieve the fractured fragment. The authors claim that the stainless steel instrument helps in retrieving the fractured fragment from the apical portion of the implant screw hole easily. The instrument has two diameters of 1 and 1.4 mm and is compatible with different implant systems. One main drawback is that in the course of time, the fork-shaped tip may wear off and will require a replacement.
Some clinicians used less expensive and commonly available instruments readily available in a dental office. The superior portion of the fractured screw is modified into a slot-like shape with a round bur. Another round bur is modified to engage the slot, and a reverse torque is applied to remove the fractured screw.[21] Yi et al.[30] suggested a cost-effective and less time-consuming technique. Cut screws with at least 3.5 threads are used to reconnect the prosthesis to existing implants when the fractured screws are non-retrievable by conservative methods. The short screws are cut to the length of the remaining internal threads of the implant.
Management of fractured implant abutment screws is quite challenging. Though different techniques have been implemented in retrieving fractured abutment screws, there is a lack of proper guidelines regarding the treatment plan. In view of the various techniques discussed in this review article, the authors present a structured treatment protocol to retrieve fractured implant abutment screws [Figure 2].
Figure 2.

Flow chart of treatment protocol to retrieve fractured implant abutment screws
Almost all articles in this review paper were of the opinion that abutment screw fractures occurred due to screw loosening. Proper screw tightening and perfect alignment during tightening are essential in minimizing the risk of screw loosening and screw fractures. The limitation of this review is the lack of literature highlighting the ease or difficulty in retrieving fractured abutment screws induced by excessive torque or due to tightening of off-axis placed abutment screws. The absence of screw loosening in these conditions may make the retrieval of fractured screws more challenging. By using an ultrasonic scaler, the authors propose a novel technique for the retrieval of excessive torque-induced fracture of implant abutment screws [Figure 3]. The ultrasonic scaler tip is oscillated circumferentially around the fractured screw in a counterclockwise direction. An assistant simultaneously applies a sharp straight probe diagonally opposite to the scaler tip across the broken fragment to wedge it between the implant body and the fractured screw [Figures 4 and 5]. The wedging maneuver facilitates the loosening of the fractured screw and enables its removal [Figure 6]. Another limitation is that most of the review articles are case series or case reports due to limited research done in this aspect. Additional research in this regard is desirable.
Figure 3.
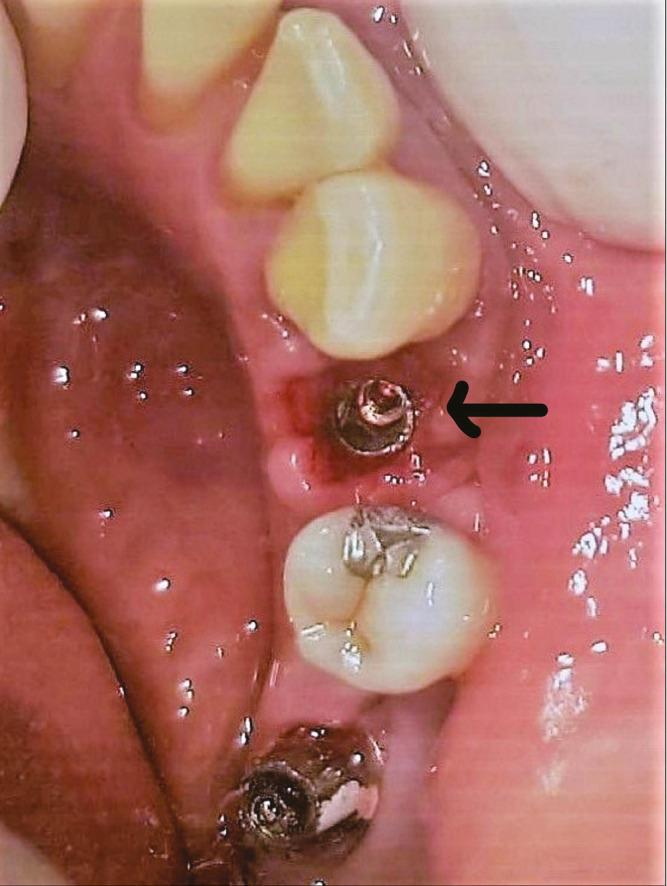
Lower right premolar implant with retained fractured abutment screw
Figure 4.
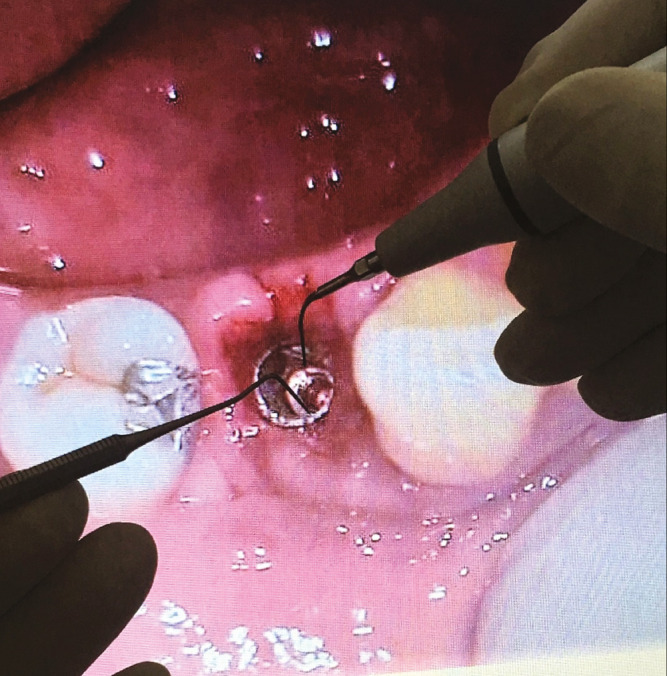
Ultrasonic scaler tip and probe application
Figure 5.
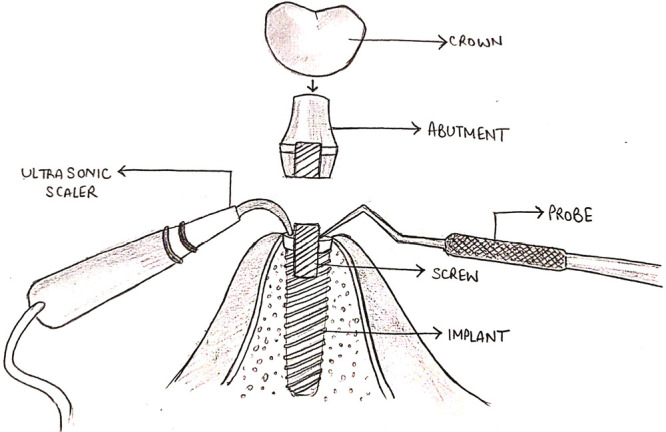
Diagrammatic representation of application of scaler tip and probe
Figure 6.

Retrieved fractured abutment screw fragments
CONCLUSION
Although clinicians can use various techniques to remove fractured abutment screws, every effort should be made to eliminate the cause of screw fracture. Conservative techniques are to be advocated initially before considering the use of commercial retrieval kits. Retrieval of the broken screw fragment should be done judiciously to prevent any internal damage to the implant structure. More clinical research should be conducted to determine the effectiveness of various techniques in the retrieval of fractured abutment screws.
ACKNOWLEDGEMENT
None.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
AUTHORS’ CONTRIBUTIONS
All the authors have contributed equally and have approved the final version of the manuscript for publication.
ETHICAL POLICY AND INSTITUTIONAL REVIEW BOARD STATEMENT
Not applicable.
PATIENT DECLARATION OF CONSENT
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
DATA AVAILABILITY STATEMENT
Not applicable.
REFERENCES
- 1.Brägger U, Aeschlimann S, Bürgin W, Hammele CH, Lang NP. Biological and technical complications and failures with fixed partial dentures (FDP) on implants and teeth after four to five years of function. Clin Oral Implants Res. 2001;12:26–34. doi: 10.1034/j.1600-0501.2001.012001026.x. [DOI] [PubMed] [Google Scholar]
- 2.Tagger Green N, Machtei EE, Horwitz J, Peled M. Fracture of dental implants: Literature review and report of a case. Implant Dent. 2002;11:137–43. doi: 10.1097/00008505-200204000-00014. [DOI] [PubMed] [Google Scholar]
- 3.Wiskott HW, Belser UC. Mechanical resistance of cemented post and core buildups for ITI-Bonefit implants. Clin Oral Implants Res. 1992;3:128–35. doi: 10.1034/j.1600-0501.1992.030305.x. [DOI] [PubMed] [Google Scholar]
- 4.Bakaeen LG, Winkler S, Neff PA. The effect of implant diameter, restoration design, and occlusal table variations on screw loosening of posterior single-tooth implant restorations. J Oral Implantol. 2001;27:63–72. doi: 10.1563/1548-1336(2001)027<0063:TEOIDR>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Wie H. Registration of localization, occlusion and occluding materials for failing screw joints in the Brånemark Implant System. Clin Oral Implants Res. 1995;6:47–53. doi: 10.1034/j.1600-0501.1995.060106.x. [DOI] [PubMed] [Google Scholar]
- 6.Goodacre CJ, Kan JY, Rungcharassaeng K. Clinical complications of osseointegrated implants. J Prosthet Dent. 1999;81:537–52. doi: 10.1016/s0022-3913(99)70208-8. [DOI] [PubMed] [Google Scholar]
- 7.Nergiz I, Schmage P, Shahin R. Removal of a fractured implant abutment screw: A clinical report. J Prosthet Dent. 2004;91:513–7. doi: 10.1016/j.prosdent.2004.03.010. [DOI] [PubMed] [Google Scholar]
- 8.Shah K, Lee DJ. An alternative approach for the management of fractured implant abutment screws on a mandibular implant-retained overdenture: A clinical report. J Prosthet Dent. 2016;115:402–5. doi: 10.1016/j.prosdent.2015.09.027. [DOI] [PubMed] [Google Scholar]
- 9.Yilmaz B, McGlumphy E. A technique to retrieve fractured implant screws. J Prosthet Dent. 2011;105:137–8. doi: 10.1016/S0022-3913(11)60015-2. [DOI] [PubMed] [Google Scholar]
- 10.Luterbacher S, Fourmousis I, Lang NP, Brägger U. Fractured prosthetic abutments in osseointegrated implants: A technical complication to cope with. Clin Oral Implants Res. 2000;11:163–70. [PubMed] [Google Scholar]
- 11.Harshakumar K, Bhatia S, Ravichandran R, Joy PT. Salvaging an implant with abutment screw fracture by a custom titanium post and core supported prosthesis—A novel technique. Int J Sci Study. 2014;2:36–9. [Google Scholar]
- 12.Canpolat C, Ozkurt-Kayahan Z, Kazazoğlu E. Management of a fractured implant abutment screw: A clinical report. J Prosthodont. 2014;23:402–5. doi: 10.1111/jopr.12111. [DOI] [PubMed] [Google Scholar]
- 13.Aglietta M, Siciliano VI, Zwahlen M, Brägger U, Pjetursson BE, Lang NP, et al. A systematic review of the survival and complication rates of implant supported fixed dental prostheses with cantilever extensions after an observation period of at least 5 years. Clin Oral Implants Res. 2009;20:441–51. doi: 10.1111/j.1600-0501.2009.01706.x. [DOI] [PubMed] [Google Scholar]
- 14.Yi Y, Koak JY, Kim SK, Lee SJ, Heo SJ. Comparison of implant component fractures in external and internal type: A 12-year retrospective study. J Adv Prosthodont. 2018;10:155–62. doi: 10.4047/jap.2018.10.2.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.McGlumphy EA, Mendel DA, Holloway JA. Implant screw mechanics. Dent Clin North Am. 1998;42:71–89. [PubMed] [Google Scholar]
- 16.Yilmaz B, McGlumphy E. A technique to salvage a single implant-supported fixed dental prosthesis having a nonretrievable implant screw fragment. J Oral Implantol. 2013;39:81–3. doi: 10.1563/AAID-JOI-D-11-00051. [DOI] [PubMed] [Google Scholar]
- 17.Flanagan D. Management of a fractured implant abutment screw. J Oral Implantol. 2016;42:508–11. doi: 10.1563/aaid-joi-D-16-00105. [DOI] [PubMed] [Google Scholar]
- 18.Oh SL, Barnes D. Managing a fractured implant: A clinical report. J Prosthet Dent. 2016;115:397–401. doi: 10.1016/j.prosdent.2015.08.027. [DOI] [PubMed] [Google Scholar]
- 19.Quek HC, Tan KB, Nicholls JI. Load fatigue performance of four implant-abutment interface designs: Effect of torque level and implant system. Int J Oral Maxillofac Implants. 2008;23:253–62. [PubMed] [Google Scholar]
- 20.Eckert SE, Meraw SJ, Cal E, Ow RK. Analysis of incidence and associated factors with fractured implants: A retrospective study. Int J Oral Maxillofac Implants. 2000;15:662–7. [PubMed] [Google Scholar]
- 21.Williamson RT, Robinson FG. Retrieval technique for fractured implant screws. J Prosthet Dent. 2001;86:549–50. doi: 10.1067/mpr.2001.118922. [DOI] [PubMed] [Google Scholar]
- 22.Satwalekar P, Chander KS, Reddy BA, Sandeep N, Sandeep N, Satwalekar T. A simple and cost effective method used for removal of a fractured implant abutment screw: A case report. J Int Oral Health. 2013;5:120–3. [PMC free article] [PubMed] [Google Scholar]
- 23.Gooty JR, Palakuru SK, Guntakalla VR, Nera M. Noninvasive method for retrieval of broken dental implant abutment screw. Contemp Clin Dent. 2014;5:264–7. doi: 10.4103/0976-237X.132382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bhandari S, Aggarwal N, Bakshi S. Ultrasonic oscillations for conservative retrieval of a rare fracture of implant healing abutment. J Oral Implantol. 2013;39:475–8. doi: 10.1563/AAID-JOI-D-11-00126. [DOI] [PubMed] [Google Scholar]
- 25.Chen JH, Cho SH. An accessory technique for the intraoral removal of a fractured implant abutment screw. J Prosthet Dent. 2018;120:812–5. doi: 10.1016/j.prosdent.2018.01.026. [DOI] [PubMed] [Google Scholar]
- 26.Chawali F, Daouahi N, Khelifa MB, Harzallah B, Cherif M, Hadyaoui D. Management of implant abutment screw fracture using a non-invasive technique: 9 months follow up case report. J Dent Report. 2020;1:1–7. [Google Scholar]
- 27.Sim BK, Kim B, Kim MJ, Jeong GH, Ju KW, Shin YJ, et al. Hollow abutment screw design for easy retrieval in case of screw fracture in dental implant system. J Healthc Eng. 2017;2017:4842072. doi: 10.1155/2017/4842072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Imam AY, Moshaverinia A, Chee WW, McGlumphy EA. A technique for retrieving fractured implant screws. J Prosthet Dent. 2014;111:81–3. doi: 10.1016/j.prosdent.2013.04.007. [DOI] [PubMed] [Google Scholar]
- 29.Pipko DJ, Kukunas S, Ismail YH. Retrofitting a cast dowel-core on salvaged dental implants. J Prosthodont. 2004;13:52–4. doi: 10.1111/j.1532-849X.2004.04006.x. [DOI] [PubMed] [Google Scholar]
- 30.Yi Y, Heo SJ, Koak JY, Kim SK. Alternative approach to salvaging an implant with a fractured screw fragment: A clinical report. J Prosthet Dent. 2021;125:18–21. doi: 10.1016/j.prosdent.2019.12.015. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.