

Abstract
Caring for a patient with a hostile abdomen is one of the most challenging clinical situations one can encounter. It requires specialized technical skill coupled with bold but thoughtful decision-making to achieve good outcomes. An approach to the patient with a complex, hostile abdomen must be individualized to account for the patient's personal details. However, implementing an experienced-based algorithm to help make the difficult decisions required in this setting can be helpful, as evidence-based studies are few. The purpose of this review is to provide a structured, evidence, and experienced-based approach to the challenges that the surgeon encounters when faced with a patient with a hostile abdomen, and to discuss perioperative and intraoperative surgical strategies that can lead to most successful outcomes.
Keywords: hostile abdomen, revisional abdominal surgery, enteric fistula, dense adhesions
From time to time, the surgeon will be asked to care for a patient with a significant loss of normal abdominal anatomy, characterized by a friable, delicate intestine that is often scarred and congealed into one solid mass, and sometimes complicated with enteric fistulae. This surgical condition is termed a “hostile” abdomen, nomenclature that could certainly be considered an understated descriptor in many circumstances. The hostile abdomen may be a result of a multitude of organic and/or iatrogenic factors. Some of these factors are, but not limited to, inflammatory processes that result in sepsis such as perforating Crohn's disease, chronic fibrosis from external beam radiation therapy, sequela of anastomotic leak, traumatic injury, or adhesive disease after prior operation. 1 2 3 4 5 6
There are several reasons why the surgeon would be faced with the need to explore a hostile abdomen. A patient with such abdomen may be clinically unbothered by its “hostility” but may require surgery for primary or recurrent malignancy, or for other benign but symptomatic pathology without an effective nonsurgical treatment. The individual could be plagued with a complication associated with a hostile abdomen like a chronic bowel obstruction, anastomotic leak, or an entero-atmospheric fistula that requires repair. Additionally, exploration may be required for a traumatic or spontaneous perforated viscous. 1 4 7
There is no easy solution to managing the hostile abdomen. The approach to these challenging patients should be individualized to address patient-specific goals and to provide a tailored perioperative strategy for each patient. 7 8 9 However, an experience-driven, systematic approach to creating a surgical plan of care is essential for a successful outcome for patients in this setting. The following discussion will highlight perioperative strategies essential for these challenging patients. The preoperative approach to the patient will be discussed, with goal setting and preoperative maneuvers that are helpful. Intraoperative strategies will be highlighted and delineated, with surgery-specific techniques described. Finally, challenges of postoperative care that are unique to this patient population will be highlighted and examined, with discussion of common challenges and strategies for achieving success and reducing morbidity.
Preoperative Preparation
Initial Evaluation
One of the most difficult decisions to make regarding the hostile abdomen is whether or not to operate . The surgeon must decide whether the benefit is worth the often high risk of re-entering such a hostile cavity. Are there convincing reasons to do so, or is there an acceptable nonoperative option?
The process begins with a comprehensive review of the patient's health leading up to the present time. The current symptoms, medical history, and all prior abdominopelvic interventions should be reviewed in detail. Operative reports should be examined, with specifics of surgery and convalescence noted. Within the operative note, one should be aware of details related to length of remaining bowel, types of prior anastomoses, and descriptions of technical difficulty that may indicate mishap or unforeseen obstacles during surgery. Also of particular interest are complications that may have occurred after surgery requiring unplanned reoperation, an interventional procedure, and prolonged hospital stay or recovery.
The presence and severity of subacute and chronic medical problems should be determined. Cardiopulmonary, renal, or vascular disease, and associated medications such as anticoagulants or immunosuppressant therapy may portend a more difficult perioperative course. Nutritional and electrolyte status, as well as presence of existing sepsis, must be determined, as these elements may be improved or corrected preoperatively to make surgery less difficult and lessen morbidity of recovery. 10 11 12 For patients who have been treated with radiation therapy, the surgeon should investigate specifics, location, and timing of treatment. 4 5
Another important component of preoperative assessment of patients with a hostile abdomen is the establishment of surgical goals. This must be an honest, open, and humble discussion between surgeon and patient. It is imperative that there is a shared, common understanding of not only the goals of surgery, but also of the anticipated challenges and complications related to the surgery being considered. Patients are generally more accepting of complications or difficult recovery if they are informed of the possibility beforehand. They should be warned preoperatively about possible problems, like damage to pelvic nerves, urogynecologic organs, and damage to surrounding bowel. 13 14 15 16 They must know of the risk of needing to abandon the operation if the adhesions are too intense.
A tremendous amount of essential information can be gleaned from the physical exam that is necessary for surgical planning. Visual evaluation of the abdominal wall shows the location of prior entry points and indicates possible untouched or “virgin” areas that may have fewer adhesions and be more suitable for safe entry points on repeat laparotomy. Other key findings are areas that are actively draining sepsis, enteroatmospheric fistula tracts, locations of enterostomies or stomatized fistula tracts, and ventral/incisional hernias that may indicate loss of abdominal wall domain.
Possibly the best physical exam maneuver that helps assess the status of abdominal adhesive disease in a patient with prior abdominal surgery is a maneuver to detect a “fluid wave.” To perform this maneuver, the surgeon places each hand on either side of the patient's abdomen and moves back and forth in tandem from side to side to detect a fluid wave of the viscera. If the viscera do not easily “shift,” the abdomen is fixed (adhesions are still significant), and more time should pass before exploration is performed. A fluid wave that is seen and felt is generally indicative of adhesions that have softened and are more amenable to exploration. 17
There are particular imaging studies that are helpful to determine anatomy and status of the abdominopelvis. Cross-sectional computed tomography (CT) can show evidence of prior surgery, locations of staple lines or surgical clips indicating prior dissection planes, ostomy or fistula tracts, loss of abdominal wall domain/hernias, and presence of persistent sepsis. It is also helpful to perform interventional procedures to better drain areas of sepsis if they are present prior to surgery.
Patients whose indication for surgery is malignancy will require oncological staging and may include preoperative diagnostic biopsies. 18
Magnetic resonance imaging is particularly useful to elucidate the presence of pelvic sepsis, specifically in the case of a distal colorectal/anal or ileoanal anastomosis. Personally reviewing such images with an experienced radiological colleague may be invaluable.
Ostomy or fistula injection studies utilize fluoroscopy to delineate anatomy of fistula tracts and adjacent bowel, and may show evidence of upstream bowel stricture or partial obstruction. A gastrografin enema is similarly employed to evaluate more distal anatomy. Endoscopy determines the health and length of accessible bowel, for example, to determine whether one can salvage an out-of-circuit rectal stump or mucous fistula.
Getting Ready for Surgery
When the decision is made to explore a hostile abdomen, it is helpful to have some practical guidelines to focus the surgical plan. The following areas should be considered.
Optimization of Nutrition, Electrolyte, Physical Fitness (Prehabilitation)
Patients with compromised nutrition should be offered preoperative nutrition supplementation. Those who are able to take enteral supplements should be given immune modulating nutritional shakes. Others unable to tolerate enteral feeds should be placed on parenteral nutrition (PN) for a period of time prior to surgery. Electrolyte abnormalities associated with high output fistulae or stomas should be corrected. Patients should also be engaged in physical activity appropriate for their particular level to improve cardiopulmonary function as much as possible, and smoking cessation should be strongly encouraged, or used as a requirement before proceeding with surgery when appropriate. 19 20 21
Control of Sepsis
If the hostile abdomen is a result of a catastrophic septic event, sepsis may persist for weeks to months after the event. CT imaging (and MRI when appropriate) can identify areas of ongoing sepsis that are amenable to surgical drainage or CT-guided catheter placement.
A useful strategy for control of chronic sepsis is the liberal use of preoperative fecal diversion, if possible, as a first step prior to full exploration of a hostile abdomen. Upstream diversion can cool off a diseased segment of bowel or an area of chronic sepsis, thereby improving the quality of the tissues and increase the patient's quality of health and life prior to full exploration. 22 Creation of a diverting ostomy in a hostile abdomen can be quite tough to achieve. One way to safely attempt this is to access the abdomen in the upper midline or in the left upper quadrant close to the location of the duodenal-jejunal flexure. The proximal jejunum is then identified and run caudally as far as possible, until the “disease” is encountered, and the distal-most bowel is brought out as an ostomy. This may create a high output ostomy requiring supplemental intravenous fluids or TPN, but is worthwhile in terms of its help in cooling off septic or obstructive pathology. Fecal diversion may also help to improve skin care in the case of an otherwise poorly controlled or pouched downstream fistula.
Organizing Consultants
Preoperative consultation with subspecialists whose expertise may be helpful should be arranged, even if their services are not always needed in the process. This allows the patient to meet the consulting surgeons, ask questions, and develop a relationship with them should their services be necessary. Common subspecialists are vascular, urologic, and gynecologic specialists. Equally as important is a consultation with an enterostomal therapist, who will assist with education and ostomy site marking, and help with preoperative wound care, i.e., in the case of an open abdomen or stomatized fistula bed. 23
If available, the surgeon should engage the help of specialty-trained surgical technologists or surgical assistants who have prior experience with operating in the hostile abdomen. Engaging the assistance of senior colleague may be invaluable and is a sign of confidence and maturity. Similarly, arranging an anesthesiology team experienced in managing major abdominal cases that span many hours and have the potential for significant blood loss is of great help.
Timing of Operation
The timing of exploration of the hostile abdomen, in relation to prior operations, is of paramount importance. This cannot be emphasized enough. Reoperative surgery is different than de novo surgery in two respects due to the presence of distorted anatomy and adhesions. From 7 days until 8 weeks from surgery, a period of “obliterative peritonitis” occurs, in which adhesion formation is greatest. 2 3 8 This period can be prolonged in times of severe sepsis. Therefore, it is prudent to wait anywhere from 6 to 12 months after surgery to re-enter a hostile abdomen to allow adhesions to settle down. Addressing ongoing sepsis and inflammation issues is also important. It is not always achievable to make things perfect for reoperation, but to create as favorable an environment as possible with which to re-enter. The timing of exploration should also be in keeping with the patient's mental and emotional fitness. If there is not an urgency to proceed with reoperation (as in the case of malignancy), do not rush. Give the patient time to regain physical, mental, and emotional health.
Mental Preparation
The surgeon, patient, and patient's support group must be mentally and emotionally ready for operation in the background of a hostile abdomen. These patients require more preoperative preparedness and have a higher risk for long, complicated convalescence than most any other surgical patient population. The patient must be committed to the process, as it is a marathon, not a sprint. They must be ready for good days and bad days, and be committed to keeping their eye on the proverbial prize.
Similarly, the surgeon requires mental and emotional toughness, as these operations require long hours of intense concentration, difficult technical maneuvers, and high-level decision-making. The surgeon must be ready to make the difficult decision of ending the case before the goals are met due to safety issues, a tremendously difficult move to make. It should be emphasized that deciding to terminate the case if goals are not achievable is a sign of maturity, not a sign of weakness. Of all the statements made in this review, this one is the most important to remember.
The recovery process can be slow and tedious, particularly when complications arise. Unfortunately, not every patient has a favorable outcome, and this can take an emotional toil on the surgeon as it does on patient and caregivers. The surgeon must keep the patient encouraged when hope wanes, and provide leadership and guidance when times are tough.
Operative Approach
Organizing the Day
On the day of surgery, the operation should start at the beginning of the day, and not follow one or more cases. This allows for the critical parts of the operation to be performed during daylight hours, when the hospital is fully staffed with helpers if needed. These operations commonly last many hours, and require more time to place invasive monitoring devices, ureteral stents, and more extensive patient positioning that add to the overall case length. Starting early also allows for the patient to be recovered (depending on the length of the case) in the post-anesthesia care unit or intensive care unit during the day shift, and not during a shift change or understaffed night shift. The patient can be checked on after surgery by the primary surgical team, and not a night team that did not participate in the case or who is limited by a verbal handoff of the details of the operation.
Ideally, the surgeon will not have any other cases or big responsibilities scheduled for the day and therefore focus their attention solely on the case at hand. Surgical consultants, who have already met the patient preoperatively, are ready for the chance of helping, and are not surprised by an intraoperative request that they have trouble or a delay in fulfilling.
Incision, Exploration, and Disease Identification
Be prepared for a long case: The patient should be positioned in a modified lithotomy (Lloyd-Davies) position with the arms tucked by the side. This allows for access to the perineum and anus if needed, even if there is no plan to explore the pelvis. One must have full access to anywhere in the abdominopelvis during hostile abdomen exploration. The case is begun early, when the teams are rested, fresh, and available. The surgeon should have an ongoing two-way dialogue with the anesthesia team to keep each other abreast of hemodynamics, bleeding issues, and both expected and unexpected events on each side. The blood bank should be ready to assist with blood products for transfusion.
Have necessary instruments in the room and ready: It is imperative to have the correct instruments ready and, in the room, to avoid delays should they be needed. Key pieces will be appropriate abdominal wall retractors, lighted pelvic retractors, extra-long instruments in the case of working in a deep cavity or quadrant, and endoscopic equipment to evaluate the bowel lumen. 24 A pair of curved, blunt tipped dissecting scissors that are preferred by the operating surgeon should be identified preoperatively.
Make a thoughtful incision: A midline incision is preferred even if paramedian incisions exist because they are easier to make and quicker to close. They can be extended laterally if needed. Take a look at the existing incisions, and see if there is an area that does not have a scar. This is usually a good place to start. For example, if the patient has a lower midline incision, or lower abdominal open wound, start above the midline for easier entry. Then, one can work from a “known” area to the “unknown” or more difficult area to delineate the anatomy.
Start away from pathology: Some key phrases that are helpful to remember are “circle the enemy” or “do the easy bits first.” Start at a location that is easier to deal with and restore normal anatomy, then perform the more difficult dissection or higher risk maneuvers, i.e., adhesions near a ureter or vessel. This also helps to develop and maintain an exit strategy throughout the operation (see below).
Have an exit strategy: As early as possible, and at each point in the operation, one should ask “what would I do if I had to stop the operation right now?” This “exit strategy” is effective when operating on a hostile abdomen. It allows the surgeon to successfully end the operation early in a controlled way if things go awry. This would be employed, for example, if adhesions are too great, if many enterotomies are made, or if the patient becomes unstable, and it is not appropriate to proceed. Therefore, never rush to divide the bowel or compromise the blood supply to the viscera.
One recommendation is to begin in the upper abdomen and restore normal anatomy, clearing the abdominal wall of adhesions and freeing upstream bowel in case an ostomy is needed. This way, if one continues dissection distally toward pathology and gets into trouble, one can quickly and efficiently make an upstream ostomy and close the abdomen.
Technical tips: A few technical pearls are helpful in dealing with difficult tissues and adhesions.
Lysis of adhesions using a sharp blade instead of scissors or electrocautery allows for safe division of scar tissue when tissue planes are difficult or obliterated. A sharp blade is best and the blade should be changed often to keep it from getting dull. The authors find that using the belly of the blade pressed gently with controlled pressure toward the tissue plane allows for the scar to “pop” and the correct plane to be identified ( Fig. 1 ).
Fig. 1.
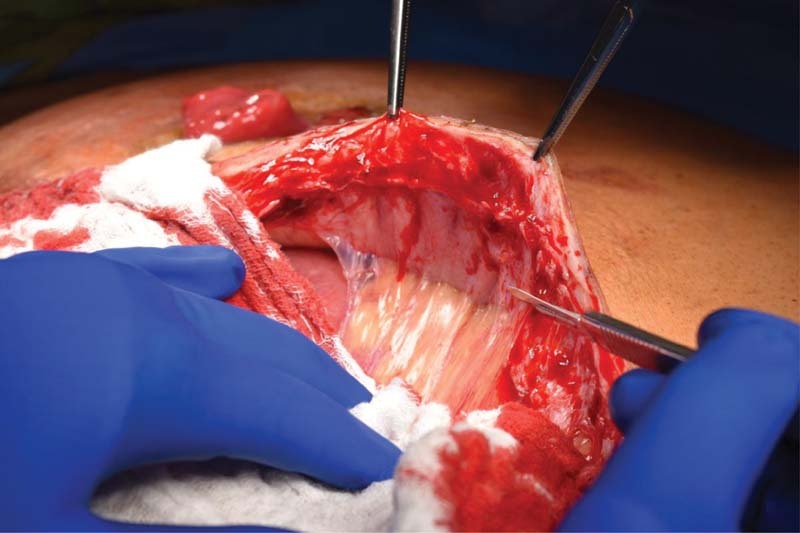
Sharp dissection using a blade to divide tough adhesive disease.
Hydro-dissection is a method of injecting saline into adhesive tissues between intestinal planes to create a pad of edema between two fused planes. This makes for easier identification and separation of the correct dissection planes, as it creates a “cushion” to reduce the likelihood of injuring a critical structure. To employ, a large syringe with a regular bore needle is filled with injectable saline, and the needle is inserted into the presumed tissue plane with slow injection of saline. A blunt tip bulb syringe is also effective. After the “cushion” is formed, the surgeon may continue with adhesiolysis within the plane using sharp dissection with the saline “pad” as a guide ( Fig. 2 ).
Fig. 2.
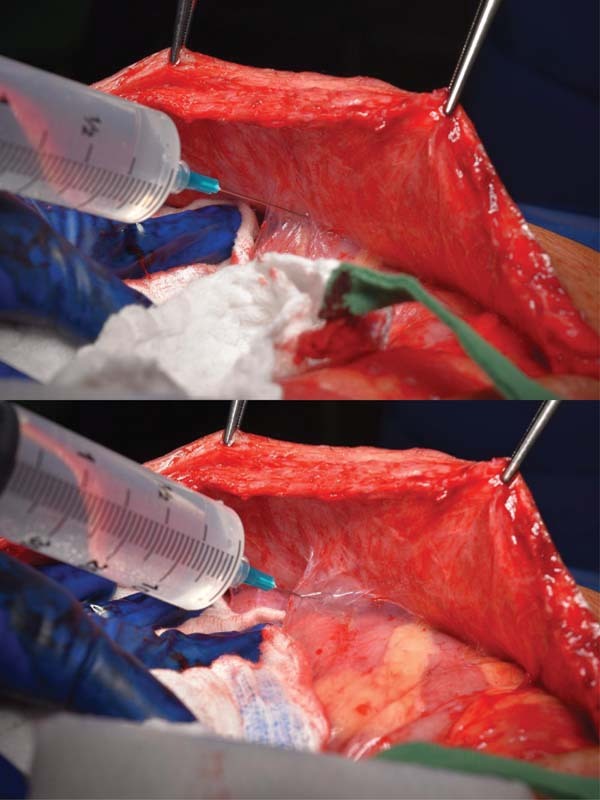
Hydrodissection using injectable saline to create a plane of edema between two fused tissue planes to safely perform lysis of adhesions.
Be prepared for challenging anastomoses : The hostile abdomen often requires the surgeon to make anastomoses using edematous or imperfect bowel with limited length or sew in a tight space. In these instances, hand sewing is best, and stapling devices should not to be relied on. When bowel is edematous or inflamed, hand-sewing in a modified one-or two-layer fashion is recommended. One technique for correcting size disparity between bowel segments is a Cheatle slit, in which the anti-mesenteric bowel of the narrower bowel is divided to increase its surface area, to more closely match the opposing bowel edge ( Fig. 3 ). Again, it is well-advised to have on hand a variety of long instruments for sewing in deep, tight quarters if necessary.
Fig. 3.
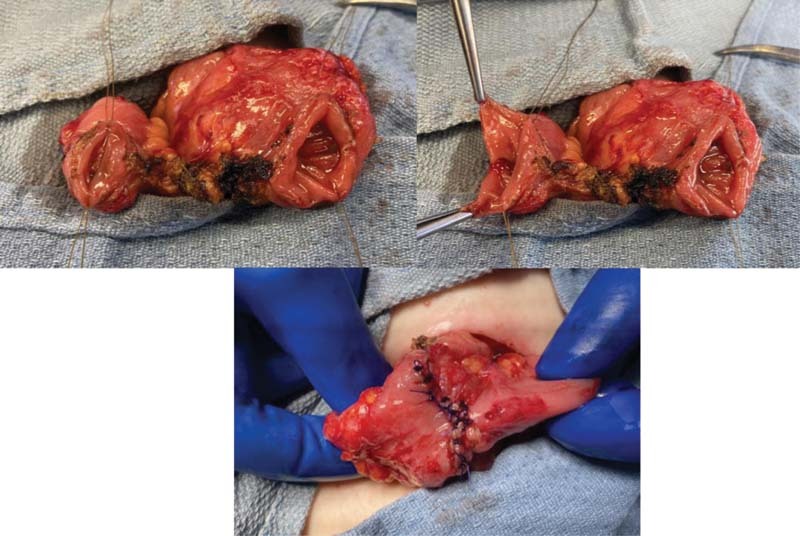
A Cheatle slit is an anti-mesenteric incision in a smaller diameter bowel edge that helps correct the disparity when an anastomosis is being attempted with differing sizes of bowel.
Control of pelvic bleeding : Reoperation in the pelvis can be complicated by bleeding from the presacral venous plexus. This is a potentially dangerous complication to manage, and the following algorithm may be helpful. After bleeding is identified, the surgeon should move to the patients left side if he/she is not already there. The site of bleeding should be temporarily controlled with a tightly wound dissector sponge to apply direct pressure to the particular bleeding area. The surgeon should alert the staff anesthesiologist of the critical nature of the situation and the need to prepare for large volume blood loss. Next, the surgeon can attempt to control the bleeding with high setting electrocautery directed at the source, or by removing a flap of abdominal wall muscle and placing this on the bleeding area, followed by direct coagulation on top of the muscle flap. The procoagulants in the muscle facilitate control of bleeding. If bleeding is ongoing after this maneuver, a sterile thumbtack may be inserted into the presacral area to tamponade the bleeding. Should these maneuvers be unsuccessful, the pelvis should be packed tightly, the abdomen temporarily closed, and the patient taken to the ICU for resuscitation, warming, and correction of coagulopathy. Re-exploration should ensue after 48 hours to allow for careful removal packs and expeditious completion of critical parts of the operation.
Drainage of the abdomen : When the operation is complete, the surgeon may desire to leave a drain in a particular area where there was bleeding or sepsis. An irrigating sump drain such as an Axiom drain is helpful to place in the pelvis when pelvic bleeding was encountered. This allows for postoperative saline sump irrigation of the pelvis to deal with ongoing oozing and clot removal. Typically, irrigation is continued for 24 to 48 hours after surgery until the effluent is light pink in color, then the irrigant is stopped and the drain is put to wall suction for 24 hours, then removed. When an area of sepsis is encountered or a great degree of enteric spillage is present, the authors suggest draining the area with a tuft of Penrose drains. Three or four long Penrose drains are gathered and inserted through a hole in the abdominal wall, with each end of the drains reaching into the target area. These can be pouched on the outside with an ostomy appliance to collect effluent. They are left for days to weeks and are backed out slowly during this time, forming a fistula tract to continue drainage of the dirty area. As the area heals, the tract dries up. This provides longer-term drainage for a particularly contaminated area, and is more reliable than closed-suction drains, as they commonly become clogged in this setting ( Fig. 4 ).
Fig. 4.

A tuft of 1-inch wide Penrose drain is placed to widely drain an area where there was enteric contamination and purulence. These are left in place and slowly backed out, so as to form a fistula tract for complete drainage of the area. When the quadrant is healed, the tract dries up.
Repairing serosal tears or enterotomies at the time they are noted will reduce the likelihood that they are forgotten about or lost, particularly if the operation is ended early and closure of the abdomen is performed hastily. It can never be emphasized enough that backing out of a hostile abdomen because things are not going well is a sign of maturity, not a sign of weakness. Treat enterotomies as diligently as a hand sewn anastomosis.
Strongly consider diverting high risk or multiple anastomoses : An enteric leak in these patients that could have been mitigated with a covering stoma can have devastating consequences like short bowel syndrome, sepsis, and even death. The authors strongly recommend diverting high risk or multiple anastomoses, particularly in chronically ill patients or those who would not tolerate additional complications. Many repeat surgical patients also have some degree of post-traumatic stress from complications they have experienced after prior unsuccessful operations, and it is our responsibility to reduce this risk if we can. We feel strongly that a high maintenance proximal diversion, i.e., high output/need for PN, that is closed in several months is much preferred to an anastomotic leak in a re-operative hostile abdomen.
Have a plan for closing the abdomen : A hostile abdomen may result in loss of abdominal wall domain and require complex closure after re-exploration. Options for this include a tissue-based components separation or placement of a biologic or synthetic mesh derivative. The decision must be individualized and take into consideration the degree of spillage and risk for mesh contamination, the length of the corrective operation, and the quality of the tissues. 25 26 If the operation is already very lengthy with significant blood loss or enteric spillage, the surgeon may want to avoid prolonging the operation further with a complex, time-consuming abdominal wall closure. The authors would suggest a skin closure over bowel with dental rolls ( Fig. 5 ). This allows for an expeditious closure of the skin and subcutaneous tissue over the bowel, understanding that there will be an inherent “hernia” as the fascial layers are not dealt with during this operation. This closure is performed using a heavy Prolene or Ethibond suture (preferred) sewn in a vertical mattress fashion, with dental rolls folded as a buttress to support. 27 These are left for several weeks after surgery and removed after the skin is sealed. Later, after full recovery, the patient may opt to undergo a more definitive closure of the abdominal wall, when there is no bowel work to be done.
Fig. 5.

Dental roll closure of the skin and subcutaneous tissues to obtain coverage over bowel. These are left in place for weeks to allow complete healing.
Consider anti-adhesive barriers judiciously : It is greatly debated as to the utility of anti-adhesive barriers such as hyaluronic acid-carboxymethylcellulose membrane (Seprafilm) in re-operative surgery. Proponents argue that the risk of adhesive small bowel obstruction is lessened, and that reoperation, if necessary, would be easier with its use. There is no consensus in the literature, with many studies reporting only on its safety profile. 28 29 If a diverting stoma is formed, wrapping it in Seprafilm may limit local adhesions and therefore avoid a laparotomy at time of stoma closure. The authors do not routinely use antiadhesive barriers.
Post-surgical Strategies and Management
Although it is euphoric to finish a successful exploration of a hostile abdomen without major problems, the surgeon must remain vigilant during the postoperative period for early, aggressive management of complications is paramount.
Enhanced recovery protocols (ERAS), although perfectly acceptable to implement in the patients, may not be overly effective (authors experience). Extended length operations, edematous bowel, and excessive handling of bowel may lead to poor toleration of early feeding, and many patients are not narcotic naïve and require higher levels of pain medications to achieve adequate levels of pain control. Regardless, ERAS is certainly worth initiating after surgery, and may be most successful when there is some flexibility to tailor to the needs and response of each patient. 30
Preoperative PN should continue postoperatively until a full diet is tolerated, and then slowly weaned. Individuals who have a prolonged recovery and do not tolerate an adequate oral intake should be considered for home PN if they are otherwise appropriate for discharge, so that an enteral diet can be restored without pressure. 31
Electrolyte and fluid status should be closely monitored in those with proximal or high output ostomy. Immediate consultation with ET is of extreme importance, for pouching and wound care, and to avoid developing skin excoriation around the ostomy or new wounds. This also allows for multiple teaching sessions for new ostomate so that he/she is comfortable with ostomy care prior to discharge.
Early identification of postoperative complications is of great importance for a few reasons. First, early intervention may mitigate the negative health effects of the complications, such as early treatment of wound infections. Also, the patient with a hostile abdomen may have experienced similar complications after prior surgery, and may be worried that the present surgery too will fail. It is helpful for the surgeon to be patient , compassionate, and present when complications occur. Good communication and reassurance to the patient and family are essential. It is comforting to have frequent face-to-face contact with the surgeon, who should never send a proxy to deliver bad news or worrisome results if possible. We must not allow our patients to feel abandoned during times of complication, and to avoid this, we must be present, be compassionate, and be a good communicator.
Some patients doing poorly after surgery may be considered for early reoperation, for reasons such as abdominal sepsis, bleeding, or obstruction. The authors would strongly discourage reoperation after day 7 , unless the patient is unstable, as adhesion formation has begun and risk for additional complication is high. Radiologic-guided procedures can effectively treat intra-abdominal abscesses or unwanted hematoma/fluid collections, 32 and those suffering from early postoperative bowel obstruction or prolonged ileus are better suited on long-term PN, with gastrostomy tube to drain until bowel function is restored. Poor decision-making regarding re-exploration after an initial surgery can lead to bowel injury, fistula, or severe adhesive disease and cause a hostile abdomen, so these decisions are critically important.
Even without discrete complications, the recovery from re-operative surgery on the hostile abdomen can be toiling, and visits from experts in pet, music, and art therapy, reiki therapy, chaplain representatives or psychology team members offer support to the patient that is unique and effective in getting them through tough times. 33
The patient who is left with a diverting stoma after surgery is inevitably in a rush to have it closed to complete the process. Do NOT be in a rush to close this. The authors recommend waiting at least 3 to 6 months (or longer) after major reoperation to do this. The patient needs time to heal and regain health, and this process cannot be expedited. Do not allow social events, holidays, insurance restrictions or other outside influences to rush the process and compromise one making a prudent, safe decision. When the patient is ready, the authors recommend performing a Gastrografin enema to check the integrity of the distal, out-of-circuit anastomoses prior to restoration of intestinal continuity. An antegrade contrast study via a proximal loop jejunostomy may also be appropriate. Restoration of intestinal continuity for patients with a history of complex revisional surgery, in the setting of a distal obstruction is catastrophic.
Conclusion
The keys to safely approaching a hostile abdomen are patience with regards to timing of surgery, preparedness when planning for every possible challenge that one may encounter, and performance of thoughtful, meticulous maneuvers in the operating room. Evidence and experienced-based strategies are helpful to create a patient-centered surgical plan for best outcomes possible in these most challenging patients.
References
- 1.Becker H P, Willms A, Schwab R. Small bowel fistulas and the open abdomen. Scand J Surg. 2007;96(04):263–271. doi: 10.1177/145749690709600402. [DOI] [PubMed] [Google Scholar]
- 2.diZerega G S. Biochemical events in peritoneal tissue repair. Eur J Surg Suppl. 1997;(577):10–16. [PubMed] [Google Scholar]
- 3.Ahrendt G M, Tantry U S, Barbul A.Intra-abdominal sepsis impairs colonic reparative collagen synthesis Am J Surg 199617101102–107., discussion 107–108 [DOI] [PubMed] [Google Scholar]
- 4.Salmo E N, Haboubi N Y. Radiation bowel disease and its clinical implication. Acta Chir Iugosl. 2010;57(03):51–54. doi: 10.2298/aci1003051s. [DOI] [PubMed] [Google Scholar]
- 5.Haboubi N Y, El-Zammar O, O'Dwyer S T, James R J. Radiation bowel disease: pathogenesis and management. Colorectal Dis. 2000;2(06):322–329. doi: 10.1046/j.1463-1318.2000.00184.x. [DOI] [PubMed] [Google Scholar]
- 6.Ashburn J H, Kalady M F. Radiation-induced problems in colorectal surgery. Clin Colon Rectal Surg. 2016;29(02):85–91. doi: 10.1055/s-0036-1580632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Visschers R GJ, Olde Damink S WM, Winkens B, Soeters P B, van Gemert W G. Treatment strategies in 135 consecutive patients with enterocutaneous fistulas. World J Surg. 2008;32(03):445–453. doi: 10.1007/s00268-007-9371-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Leppäniemi A. The hostile abdomen—a systematic approach to a complex problem. Scand J Surg. 2008;97(03):218–219. doi: 10.1177/145749690809700301. [DOI] [PubMed] [Google Scholar]
- 9.Fazio V W, Coutsoftides T, Steiger E. Factors influencing the outcome of treatment of small bowel cutaneous fistula. World J Surg. 1983;7(04):481–488. doi: 10.1007/BF01655937. [DOI] [PubMed] [Google Scholar]
- 10.Hennessey D B, Burke J P, Ni-Dhonochu T, Shields C, Winter D C, Mealy K. Preoperative hypoalbuminemia is an independent risk factor for the development of surgical site infection following gastrointestinal surgery: a multi-institutional study. Ann Surg. 2010;252(02):325–329. doi: 10.1097/SLA.0b013e3181e9819a. [DOI] [PubMed] [Google Scholar]
- 11.Martinez J L, Bosco-Garate I, Souza-Gallardo L M. Effect of preoperative administration of oral arginine and glutamine in patients with enterocutaneous fistula submitted to definitive surgery: a prospective randomized trial. J Gastrointest Surg. 2020;24(02):426–434. doi: 10.1007/s11605-018-04099-4. [DOI] [PubMed] [Google Scholar]
- 12.Fiorindi C, Cuffaro F, Piemonte G. Effect of long-lasting nutritional prehabilitation on postoperative outcome in elective surgery for IBD. Clin Nutr. 2021;40(03):928–935. doi: 10.1016/j.clnu.2020.06.020. [DOI] [PubMed] [Google Scholar]
- 13.Huang W, Tang Y, Nong L, Sun Y. Risk factors for postoperative intra-abdominal septic complications after surgery in Crohn's disease: a meta-analysis of observational studies. J Crohn's Colitis. 2015;9(03):293–301. doi: 10.1093/ecco-jcc/jju028. [DOI] [PubMed] [Google Scholar]
- 14.Allocca M, Gilardi D, Fiorino G, Furfaro F, Peyrin-Biroulet L, Danese S. Sexual and reproductive issues and inflammatory bowel disease: a neglected topic in men. Eur J Gastroenterol Hepatol. 2018;30(03):316–322. doi: 10.1097/MEG.0000000000001074. [DOI] [PubMed] [Google Scholar]
- 15.Hor T, Lefevre J H, Shields C, Chafai N, Tiret E, Parc Y. Female sexual function and fertility after ileal pouch-anal anastomosis. Int J Colorectal Dis. 2016;31(03):593–601. doi: 10.1007/s00384-015-2497-y. [DOI] [PubMed] [Google Scholar]
- 16.Dutch Snapshot Research Group . Borstlap W AA, Westerduin E, Aukema T S, Bemelman W A, Tanis P J. Anastomotic leakage and chronic presacral sinus formation after low anterior resection: results from a large cross-sectional study. Ann Surg. 2017;266(05):870–877. doi: 10.1097/SLA.0000000000002429. [DOI] [PubMed] [Google Scholar]
- 17.Fazio V W. London: Blackwell Science Ltd; 1999. Colon and Rectal Surgery. [Google Scholar]
- 18.Benson A B, Venook A P, Al-Hawary M M. NCCN Guidelines Insights: Rectal Cancer, Version 6.2020. J Natl Compr Canc Netw. 2020;18(07):806–815. doi: 10.6004/jnccn.2020.0032. [DOI] [PubMed] [Google Scholar]
- 19.Marimuthu K, Varadhan K K, Ljungqvist O, Lobo D N. A meta-analysis of the effect of combinations of immune modulating nutrients on outcome in patients undergoing major open gastrointestinal surgery. Ann Surg. 2012;255(06):1060–1068. doi: 10.1097/SLA.0b013e318252edf8. [DOI] [PubMed] [Google Scholar]
- 20.Daniels S L, Lee M J, George J. Prehabilitation in Elective Abdominal Cancer Surgery in Older Patients: Systematic Review and Meta-Analysis. BJS Open. 2020;4(06):1022–1041. doi: 10.1002/bjs5.50347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Christensen M A, Gaitanidis A, Parks J. Thirty-day outcomes in the operative management of intestinal-cutaneous fistulas: a NSQIP analysis. Am J Surg. 2021;221(05):1050–1055. doi: 10.1016/j.amjsurg.2020.08.038. [DOI] [PubMed] [Google Scholar]
- 22.Schwartzberg D M, Esen E, Remzi F H. Thoughtful ileostomy creation in patients undergoing redo IPAA. Dis Colon Rectum. 2020;63(01):117–120. doi: 10.1097/DCR.0000000000001535. [DOI] [PubMed] [Google Scholar]
- 23.Brooke J, El-Ghaname A, Napier K, Sommerey L. Executive summary: Nurses Specialized in Wound, Ostomy and Continence Canada (NSWOCC) nursing best practice recommendations: enterocutaneous fistula and enteroatmospheric fistula. J Wound Ostomy Continence Nurs. 2019;46(04):306–308. doi: 10.1097/WON.0000000000000555. [DOI] [PubMed] [Google Scholar]
- 24.Fazio V W. London: Blackwell Science Ltd; 1999. Retractors and exposure in the pelvis. [Google Scholar]
- 25.Latifi R, Gustafson M. Abdominal wall reconstruction in patients with enterocutaneous fistulas. Eur J Trauma Emerg Surg. 2011;37(03):241–250. doi: 10.1007/s00068-011-0108-3. [DOI] [PubMed] [Google Scholar]
- 26.Leppäniemi A.Open abdomen for the management of catastrophic abdomen: evidence and controversies Cir Esp (Engl Ed) 2020(e-pub ahead of print) 10.1016/j.ciresp.2020.06.011 [DOI] [PubMed] [Google Scholar]
- 27.Aydinli H H, Peirce C, Aytac E, Remzi F H. A novel closure technique for complex abdominal wounds. Dis Colon Rectum. 2018;61(04):521–526. doi: 10.1097/DCR.0000000000001032. [DOI] [PubMed] [Google Scholar]
- 28.van der Wal J B, Iordens G I, Vrijland W W, van Veen R N, Lange J, Jeekel J. Adhesion prevention during laparotomy: long-term follow-up of a randomized clinical trial. Ann Surg. 2011;253(06):1118–1121. doi: 10.1097/SLA.0b013e318217e99c. [DOI] [PubMed] [Google Scholar]
- 29.Fazio V W, Cohen Z, Fleshman J W. Reduction in adhesive small-bowel obstruction by Seprafilm adhesion barrier after intestinal resection. Dis Colon Rectum. 2006;49(01):1–11. doi: 10.1007/s10350-005-0268-5. [DOI] [PubMed] [Google Scholar]
- 30.Delaney C P, Fazio V W, Senagore A J, Robinson B, Halverson A L, Remzi F H. ‘Fast track’ postoperative management protocol for patients with high co-morbidity undergoing complex abdominal and pelvic colorectal surgery. Br J Surg. 2001;88(11):1533–1538. doi: 10.1046/j.0007-1323.2001.01905.x. [DOI] [PubMed] [Google Scholar]
- 31.Fragkos K C, Sebepos-Rogers G, Rahman F. When is parenteral nutrition indicated in the hospitalized, acutely ill patient? Curr Opin Gastroenterol. 2020;36(02):129–135. doi: 10.1097/MOG.0000000000000615. [DOI] [PubMed] [Google Scholar]
- 32.Sahai A, Bélair M, Gianfelice D, Coté S, Gratton J, Lahaie R. Percutaneous drainage of intra-abdominal abscesses in Crohn's disease: short and long-term outcome. Am J Gastroenterol. 1997;92(02):275–278. [PubMed] [Google Scholar]
- 33.Dale V H.The impact of perioperative music on abdominal surgery patients' experience of postoperative pain: a systematic review and meta-analysis J Perioper Pract 202131(1-2):31–43. [DOI] [PubMed] [Google Scholar]