

Abstract
Background
To systematically collate, appraise, and synthesize evidence of electroacupuncture (EA) as an adjunct therapy for poststroke aphasia (PSA) from randomized controlled trials (RCTs) through a systematic review and meta-analysis.
Methods
An electronic search was conducted in eight databases to identify RCTs evaluating EA adjuvant therapy versus speech and language therapy (SLT). Methodological quality of the included trails was assessed by the Cochrane risk of bias. The software Review Manager 5.4 was used for data analysis.
Results
Nineteen RCTs enrolling a total of 1263 subjects were identified. The use of EA combined with speech and language therapy (SLT) showed significant improvements in effective rate (RR 1.31, 95% CI [1.21, 1.41]), oral expression score (SMD 1.34, 95% CI [1.13, 1.56]), comprehension score (SMD 1.95, 95% CI [0.88, 3.03]), repetition score (SMD 1.84, 95% CI [0.75, 2.93]), naming score (SMD 1.97, 95% CI [0.81, 3.13]), and reading score (SMD 1.55, 95% CI [1.07, 2.04]) compared to the use of SLT alone.
Conclusions
The pooled data indicate that EA combined with SLT for the treatment of PSA may improve clinical effectiveness, compared with SLT alone. Future high quality RCTs with large samples are still needed to confirm and expand our findings.
1. Introduction
Stroke is the most common cause of mortality and morbidity worldwide. Globally, more than ten million new cases of stroke are reported each year and at least one third of the affected individuals live with aphasia [1, 2]. Economic and social consequences are highly relevant because poststroke aphasia (PSA) has a serious negative impact on patients' activities of daily living [3]. Furthermore, the impact of PSA on functional communication, everyday activities, and social abilities of patients is dramatic and is, therefore, essential for the effective management and rehabilitation of aphasia [4]. Clinically, speech and language therapy (SLT) remain the gold standard for the treatment of PSA [5]. However, the clinical efficacy of this therapy still cannot meet patients' expectations [5]. In this situation, some patients choose complementary and alternative therapies to treat PSA in an effort to improve their quality of life.
In China, acupuncture is a widely used clinical rehabilitation technique, which is also recommended as an alternative treatment option for poststroke rehabilitation by the Ottawa Panel clinical practice guidelines [6]. As sources of the highest level of evidence for evidence-based medicine, previous systematic reviews/meta-analyses [7–13] have almost all revealed the benefits of acupuncture on PSA. As an extended technique of acupuncture, electroacupuncture (EA) has both the effects of traditional acupuncture and the functions of modern electrotherapy [14]. A recently published network meta-analysis [15] concluded that the efficacy of EA combined with SLT for PSA was superior to that of SLT alone. In addition, a systematic review [16] conducted in Korea concluded that EA could be considered as an adjunctive therapy for PSA. Nevertheless, the relative effect of EA on PSA could not be assessed because quantitative synthesis was not performed. A preliminary literature search identified a growing number of randomized controlled trials (RCTs) on the effects of EA for PSA, whereas, controversial efficacy was reported. Thus, to systematically collate, evaluate, and synthesize current evidence, we conducted this study.
2. Methods
This meta-analysis was carried out following the guidelines of Cochrane handbook [17] and updated PRISMA checklists [18]. The protocol was registered in the PROSPERO database (no. CRD42021254369).
2.1. Literature Search and Selection
PubMed, the Cochrane Library, Web of Science, Embase, CNKI, Wanfang, VIP, and CBM were systematically searched from database establishment to June 2022. Stroke, aphasia, electroacupuncture, and randomized controlled trials were applied as search keywords. Detailed search strategy in PubMed was given in the supplementary material.
2.2. Inclusion and Exclusion Criteria
Trails met the following inclusion criteria: (I) type of studies: only randomized controlled trials were included; (II) types of participants: stroke was confirmed by neurological examination or by brain scanning, or both. Patients were not limited by gender and age; (III) types of interventions: the intervention was EA plus SLT; (IV) the comparison was SLT alone; (V) types of outcomes: language functions (oral expression, comprehension, repetition, naming, and reading) and effective rate. Language functions were assessed by scales including western aphasia battery (WAB) [19], China rehabilitation research center aphasia examination (CRRCAE) [20], and aphasia battery of Chinese (ABC) [21]. The definition of the effective rate: effective rate = (“total number of patients” - “number of patients with no response”) /total number of patients, and “no response” meant no significant change in any aspect of language function or regression of one aspect of language function after treatment [22]; and (VI) it was published in English or Chinese language.
The exclusion criteria were as follows: (I) duplicate studies, duplications; (II) full text cannot be obtained through various approaches or studies in which data cannot be extracted; and (III) aphasia caused by other diseases.
2.3. Data Extraction and Outcome Measures
For literature selection, two independent reviewers read the titles and abstracts in the first screening stage, read the full texts in the final screening stage, and assessed the articles based on the inclusion and exclusion criteria. Information including the first author, publication year, sample size, patient characteristics, interventions, and outcomes were extracted from the included trails.
2.4. Quality Assessment
The risk of bias was independently assessed by two independent reviewers with the Cochrane risk of bias tool from seven domains: (I) randomization process; (II) allocation concealment; (III) blind method; (IV) outcome assessors; (V) missing outcome data processing; (VI) selection of the reported result; and (VII) other bias.
2.5. Statistical Analysis
Data analyses were carried out using Review Manager 5.4 software. The pooled effects were the relative risk (RR) and 95% CI for dichotomous outcomes and the standard mean difference (SMD) with 95% CI for continuous outcomes. Heterogeneity between the trails was determined using I2 statistics. Fixed effects model was used if I2 < 50%; otherwise, a random effects model was used (I2 ≥ 50%). Subgroup analyses were performed on the basis of treatment duration. Sensitivity analyses were carried out by removing each study individually to estimate the quality and consistency of the results. Publication bias was carried out with funnel plot.
3. Results
3.1. Literature Search
A total of 814 records were obtained from the eight databases and 184 duplicates were excluded. 630 records were removed after the titles and abstracts were screened. Eventually, 38 records were identified for full-text analysis, and 19 trails [23–41] were deemed eligible finally (Figure 1).
Figure 1.
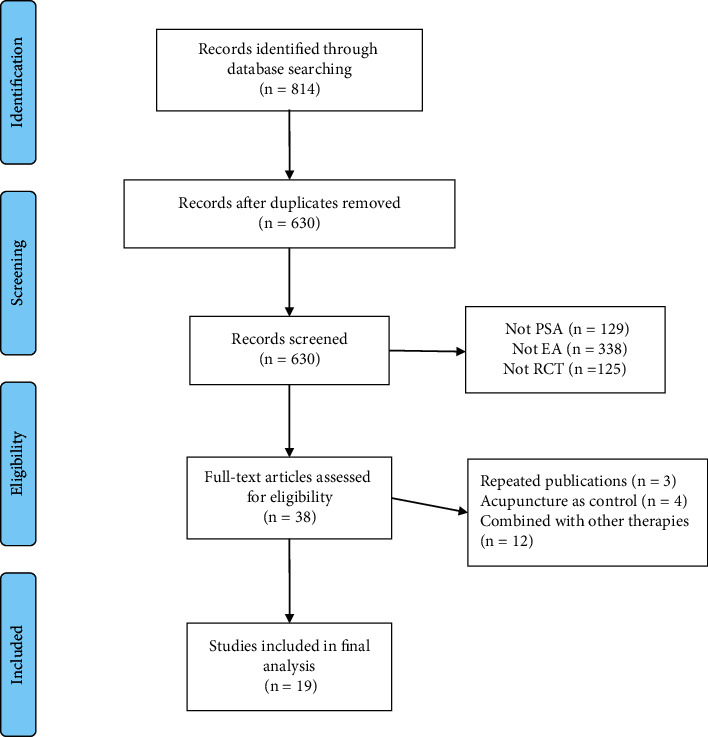
PRISMA flowchart for literature selection.
3.2. Characteristics of Included Studies
The included trails with sample sizes ranged from 20 to 120 published between 2000 and 2021. In total, 1263 subjects were included, with 638 in EA groups and 625 in control groups. The treatment cycle lasted 10 to 40 days, and each treatment lasted 15–60 min. More details are shown in Table 1.
Table 1.
Descriptive analysis of the characteristics.
| First author; year | Simple | Age | Time post onset | Acupoints | Duration & frequency of trial period | Main outcomes | |||
|---|---|---|---|---|---|---|---|---|---|
| I | C | I | C | I | C | ||||
| Wang et al. [23]. 2021 | 40 | 40 | 52.25 ± 4.71 | 52.30 ± 4.76 | 27.32 ± 3.83d | 29.21 ± 3.85 | DU16 (风府), DU15 (哑门) | 20 min each time, once daily, 4 w | Oral expression score, comprehension score, repetition score, naming score, and ER |
| Wang [24]. 2021 | 25 | 25 | Unclear | Unclear | Unclear | Unclear | DU20 (百会), Ex-HN13(金津), HT5 (通里), RN23(廉泉) | 30 min each time, once daily, 4 w | Oral expression score, comprehension score, repetition score, naming score, and ER |
| Nie et al. [25]. 2020 | 23 | 23 | 51.0 ± 2.31 | 52.0 ± 3.12 | Unclear | Unclear | Scalppoints | 15 min each time, once daily, 10 d | Oral expression score, reading score, comprehension score, and ER |
| Ma et al. [26]. 2020 | 20 | 20 | 52.15 ± 9.82 | 51.36 ± 10.11 | 60.87 ± 21.43d | 59.18 ± 24.21d | Scalppoints | 30 min each time, once daily, 3 w | Oral expression score, comprehension score, repetition score, and naming score |
| Lin et al. [27]. 2019 | 40 | 40 | 52.25 ± 4.71 | 52.30 ± 4.76 | Unclear | Unclear | MS6 (顶颞前斜线), MS10 (颞前线), EX-HN1(四神聪), DU16 (风府), DU20 (百会), EX-HN3(印堂), PC6(内关), DU26(水沟)、HT5(通里)、SP6(三阴, RN23(廉泉) | 30 min each time, once daily, 2 w | Oral expression score, comprehension score, repetition score, naming score, and ER |
| Zheng et al. [28]. 2018 | 60 | 60 | 53.58 ± 1.81 | 58.38 ± 1.31 | 69.23 ± 4.32d | 79.15 ± 3.53d | RN23(廉泉), GB8 (率谷) | 30 min each time, once daily, 4 w | Oral expression score, comprehension score, reading score, repetition score, and naming score |
| Sun [29]. 2018 | 50 | 50 | 53.7 ± 5.2 | 52.3 ± 4.9 | 42.1 ± 12.5d | 41.3 ± 11.2d | EX-HN13(玉液), Ex-HN13(金津) | 20 min each time, once daily, 4 w | ER |
| Yang et al. [30]. 2017 | 45 | 45 | 58.4 ± 10.38 | 60.6 ± 11.57 | 8.68 ± 3.24d | 6.78 ± 3.25d | Scalppoints, DU16 (风府), DU15 (哑门), DU20 (百会) | 20 min each time, 5 times weekly, 2 w | Oral expression score, comprehension score, repetition score, naming score, and ER |
| Li et al. [31]. 2017 | 30 | 30 | 57.10 ± 10.03 | 58.11 ± 9.96 | 21.33 ± 5.16 d | 22.10 ± 4.89 d | MS6 (顶颞前斜线), MS10 (颞前线), EX-HN1(四神聪), DU20 (百会), RN23(廉泉) | 30 min each time, twice daily, 14d | Oral expression score, comprehension score, repetition score, naming score, and ER |
| Jiang et al. [32]. 2017 | 10 | 10 | 63.7 ± 6.6 | 58.7 ± 10.4 | 90.1 ± 58.2d | 69.6 ± 43. 5d | MS6 (顶颞前斜线), MS7(顶颞后斜线), DU20 (百会) | 60 min each time, twice daily, 2w | Oral expression score and ER |
| Cui et al. [33]. 2016 | 33 | 33 | 56.1 ± 11.0 | 56.3 ± 10.7 | 42.2 ± 19.3d | 42.1 ± 19.5d | EX-HN13 (玉液), Ex-HN13 (金津) | 20 min each time, once daily, 4w | Repetition score, naming score, and ER |
| Sheng et al. [34]. 2015 | 20 | 20 | 55.05 ± 9.27 | 57.10 ± 8.30 | 24.20 ± 10.95d | 23.00 ± 10.40d | Unclear | 30 min each time, twice daily, 4w | Oral expression score |
| Jiang et al. [35]. 2015 | 30 | 30 | 57 ± 10 | 57 ± 9 | 42.3 ± 19.2d | 40.3 ± 19.4d | Unclear | 30 min each time, twice daily, 4w | Repetition score and ER |
| Zhang et al. [36]. 2014 | 42 | 30 | 62.4 ± 1.4 | 57.6 ± 1.6 | 78.0 ± 8.6d | 85.0 ± 9.2d | EX-HN13 (玉液), Ex-HN13 (金津) | 20 min each time, once daily, 1m | ER |
| Du [37]. 2012 | 30 | 30 | 42∼74 | 44∼74 | 7∼67d | 9∼66d | RN23 (廉泉) | 30 min each time, twice daily, 4w | Oral expression score and ER |
| Aili et al. [38]. 2012 | 35 | 34 | Unclear | Unclear | Unclear | Unclear | HT5 (通里), ST36 (足三里), KI6 (照海), PC6 (内关), LI4 (合谷), ST40 (丰隆), | 30 min each time, once daily, 1m | ER |
| LI et al. [39]. 2007 | 30 | 30 | 54 ± 7.8 | 53 ± 5.6 | 7 ± 3.2d | 7 ± 3.3d | RN23 (廉泉), EX-HN13 (玉液), Ex-HN13 (金津), EX-HN13 (翳明), GB20 (风池) | 30 min each time, once daily, 20 d | ER |
| Zhang et al. [40]. 2005 | 45 | 45 | 56.7 ± 15.6 | 58.4 ± 13.3 | 24.4 ± 20.1d | 23.4 ± 20.3d | RN23 (廉泉) | 30 min each time, once daily, 3w | Oral expression score and ER |
| Liu et al. [41]. 2000 | 30 | 30 | Unclear | Unclear | 3w-6m | 3w-6m | GB8 (率谷), GB13 (本神), DU20 (百会), GB20 (风池) | 30 min each time, once daily, 30 d | Oral expression score and ER |
3.3. Study Quality
A summary of the risk of biases is presented in Figures 2 and 3. With regards to random sequence generation, four studies [24, 33, 37, 39] had a high risk of bias. To reduce the impact of high risk of bias on the pooled results, these four trails [24, 33, 37, 39] were excluded from the performed meta-analysis. With regards to allocation concealment and blinding, all studies had an unclear risk of bias. All trails had a low risk of bias in incomplete outcome data. With regards to other sources of bias, eight studies had a low risk of bias.
Figure 2.
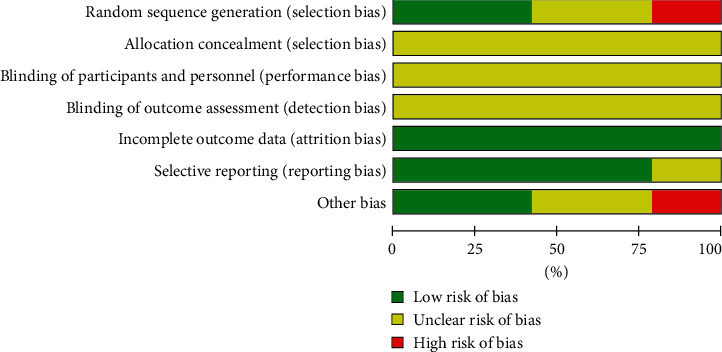
Risk of bias percentage chart.
Figure 3.
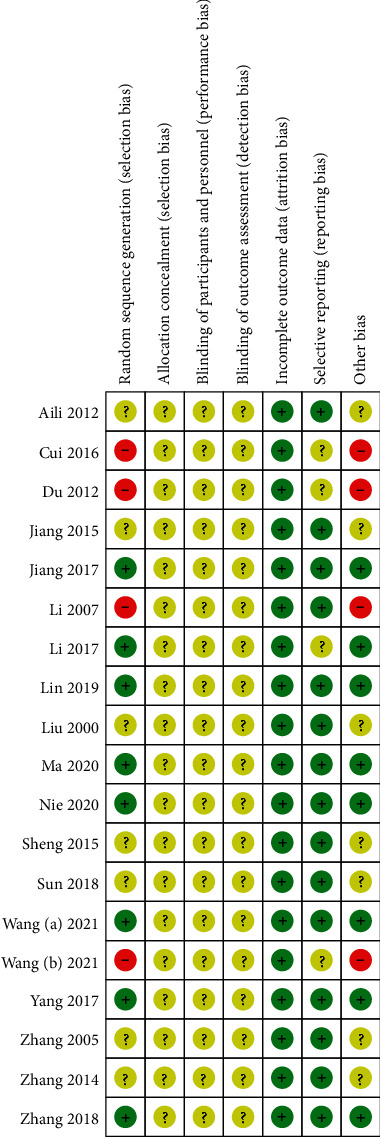
Risk of bias distribution diagram.
3.4. Meta-Analysis
3.4.1. Effective Rate
11 studies with a total of 747 subjects used the effective rate to evaluate the efficacy. A random-effect model was applied due to huge clinical heterogeneity in RCT, like acupoints and manipulation. The pooled analysis showed that EA combined with SLT had a higher effective rate (RR 1.31, 95% CI [1.21, 1.41]). In the subgroup analyses based on treatment duration, both subgroups showed statistically significant improvements in the effective rate with combined treatment compared to SLT alone (treatment for 2 weeks: RR 1.24, 95% CI [1.10, 1.40]; treatment for 3 weeks: RR 1.27, 95% CI [1.05, 1.54]; treatment for 4 weeks: RR 1.38, 95% CI [1.22, 1.57]). More details are shown in Figure 4,. The sensitivity analysis performed by the exclusion method showed that the study by Yang et al. [30] was the main cause of heterogeneity. In addition, the funnel plot was not symmetrical (Figure 5), which did not mean that there was a risk of publication bias because the sample size in this study was not small.
Figure 4.
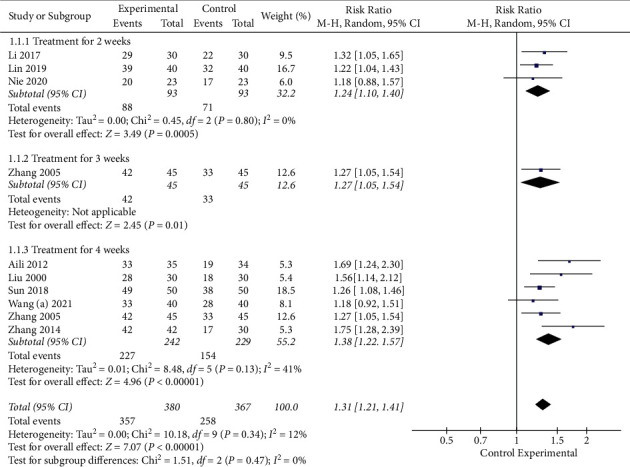
Meta-analysis in effective rate.
Figure 5.
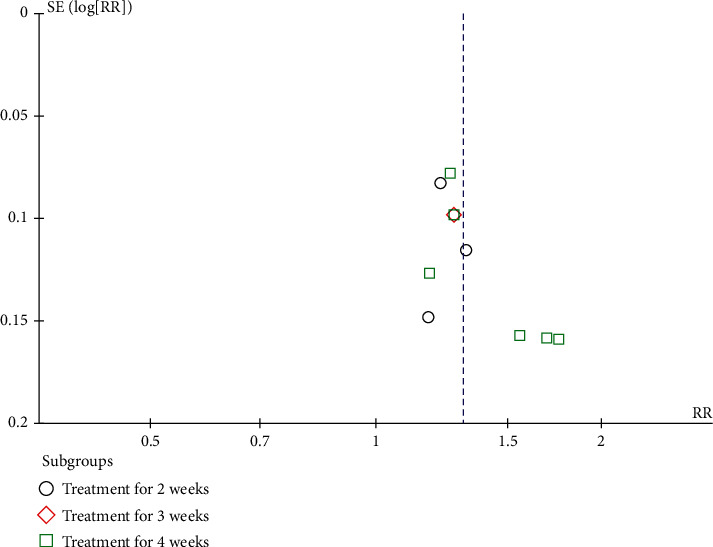
A funnel plot of effective rate.
3.4.2. Oral Expression Score
Nine studies with a total of 650 subjects used the oral expression score to evaluate the efficacy. A random-effect model was applied, the pooled analysis showed that EA combined with SLT had a higher oral expression score (SMD 1.34, 95% CI [1.13, 1.56]). In the subgroup analysis based on treatment duration, both subgroups showed statistically significant improvements in oral expression score with combined treatment compared to SLT alone (treatment for 2 weeks: SMD 1.30, 95% CI [0.97, 1.63]; treatment for 3 weeks: SMD 1.62, 95% CI [1.22, 2.02]; treatment for 4 weeks: SMD 1.37, 95% CI [1.02, 1.73]; and treatment for 6 weeks: SMD 0.72, 95% CI [0.08, 1.36]). More details are shown in Figure 6.
Figure 6.
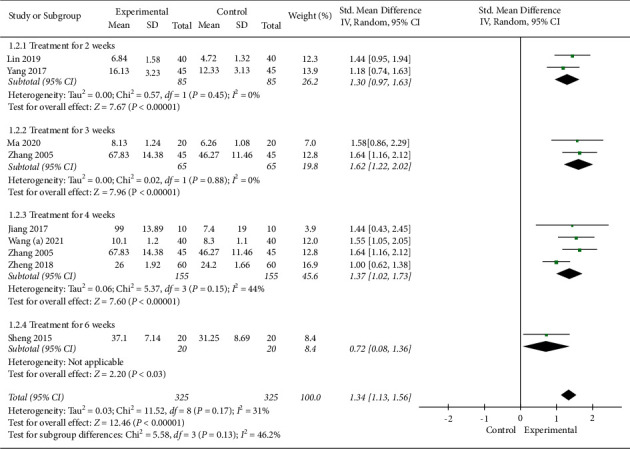
Meta-analysis in oral expression score.
The sensitivity analysis performed by the exclusion method showed that the study by Nie et al. [25] was the main cause of heterogeneity.
3.4.3. Comprehension Score
Six studies with a total of 456 subjects used the comprehension score to evaluate the efficacy. A random-effect model was applied, the pooled analysis showed that EA combined with SLT had a higher comprehension score (SMD 1.95, 95% CI [0.88, 3.03]). In the subgroup analysis based on treatment duration, both subgroups showed statistically significant improvements in comprehension score with combined treatment compared to SLT alone (treatment for 2 weeks: SMD 1.29, 95% CI [0.27, 2.30]; treatment for 3 weeks: SMD 1.58, 95% CI [0.86, 2.29]; and treatment for 4 weeks: SMD 3.10, 95% CI [0.74, 5.46]). More details are shown in Figure 7.
Figure 7.
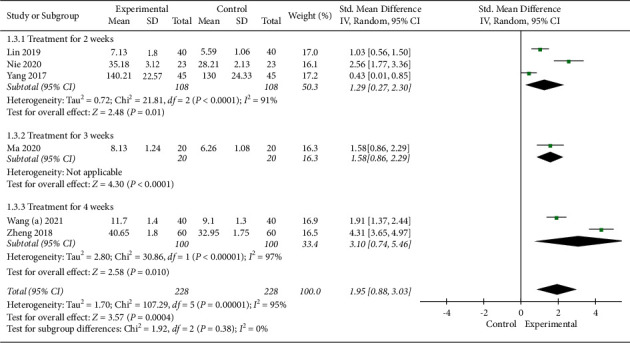
Meta-analysis in comprehension score.
The sensitivity analysis performed by the exclusion method showed that no significant changes in heterogeneity were observed.
3.4.4. Reading Score
Two studies with 86 subjects used the reading score to evaluate the efficacy. A random-effect model was applied, the pooled analysis showed that EA combined with SLT had a higher reading score (SMD 1.55, 95% CI [1.07, 2.04]). In the subgroup analysis based on treatment duration, both subgroups showed statistically significant improvements in reading score with combined treatment compared to SLT alone (treatment for 2 weeks: SMD 1.42, 95% CI [0.76, 2.07] and treatment for 4 weeks: SMD 1.73, 95% CI [0.99, 2.47]). More details are shown in Figure 8.
Figure 8.
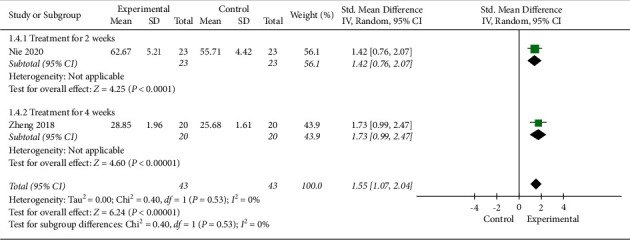
Meta-analysis in reading score.
The sensitivity analysis performed by the exclusion method showed that no significant changes in heterogeneity were observed.
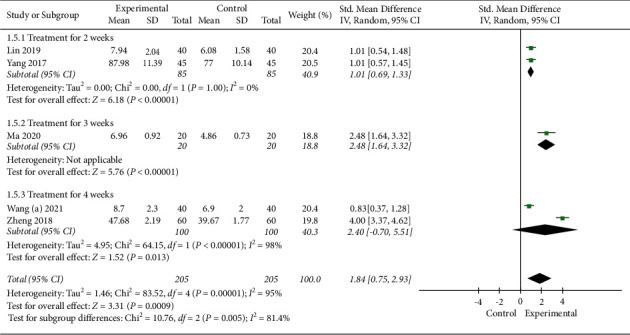
3.4.5. Repetition Score
Five studies with 410 subjects used the repetition score to evaluate the efficacy. A random-effect model was applied, the pooled analysis showed that EA combined with SLT had a higher repetition score (SMD 1.84, 95% CI [0.75, 2.93]). In the subgroup analysis based on treatment duration, subgroups showed statistically significant improvements in repetition score with combined treatment compared to SLT alone (treatment for 2 weeks: SMD 1.01, 95% CI [0.69, 1.33] and treatment for 3 weeks: SMD 2.48, 95% CI [1.64, 3.32]), however, with no evidence of benefit from treatment for 4 weeks (SMD 2.40, 95% CI [−0.70, 5.51]). More details are shown in Figure 9.
Figure 9.
Meta-analysis in repetition score.
The sensitivity analysis performed by the exclusion method showed that no significant changes in heterogeneity were observed.
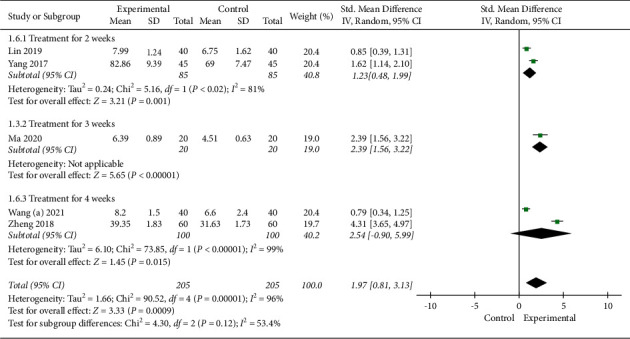
3.4.6. Naming Score
Five studies with 410 subjects used the naming score to evaluate the efficacy. A random-effect model was applied, the pooled analysis showed that EA combined with SLT had a higher naming score (SMD 1.97, 95% CI [0.81, 3.13]). In the subgroup analyses based on treatment duration, subgroups showed statistically significant improvements in naming score with combined treatment compared to SLT alone (treatment for 2 weeks: SMD 1.23, 95% CI [0.48, 1.99] and treatment for 3 weeks: SMD 2.39, 95% CI [1.56, 3.22]), however, with no evidence of benefit from treatment for 4 weeks (SMD 2.54, 95% CI [-0.90, 5.99]). More details are shown in Figure 10.
Figure 10.
Meta-analysis in naming score.
The sensitivity analysis performed by the exclusion method showed that no significant changes in heterogeneity were observed.
4. Discussion
Aphasia is a common complication following a stroke, often interfering with everyday activities, social abilities, and rehabilitation. In China, acupuncture has a long history of treating PSA, and its efficacy has been supported by evidence-based medical evidence [22]. As an extended technique of acupuncture, EA has both the effects of traditional acupuncture and the functions of modern electrotherapy and is widely used as a complementary therapy for poststroke rehabilitation. An increasing number of RCTs have begun to investigate the effects of EA in patients with PSA. However, there is no uniform conclusion on whether the combination of EA and SLT has positive clinical efficacy in PSA. To systematically collate, appraise, and synthesize the evidence, we conducted this meta-analysis of RCTs.
4.1. Summary of Main Findings
Comprehensive analysis of this meta-analysis revealed that subjects treated using combined EA and SLT showed significant improvements in effective rate, oral expression score, comprehension score, repetition score, naming score, and reading score compared to those treated by SLT alone. Therefore, we tentatively conclude that EA combined with SLT as an adjunctive for PSA can increase its clinical effectiveness. However, this conclusion must be considered with cautious, given there was too little information in most of these included trails. Firstly, the processes of randomization, allocation concealment, and binding of most trails are unclear, which may have led to a high risk of bias. Secondly, none of the included RCTs applied statistical methods to estimate the sample size, which resulted in the small sample size included in the study and therefore lowering the credibility of the evidence. In addition, all included studies assessed outcomes before and immediately after EA treatment, while the treatment duration was 10–40 days; therefore, this present study failed to further assess the long-term effects of EA on PSA. Moreover, the implementation program of EA was not uniform and showed large differences in acupoint selection, stimulation methods, needle retention time, and treatment period and frequency, which might have increased the source of heterogeneity [14]. Furthermore, all of the included trails were conducted in China, which may have led to publication bias.
4.2. Agreements and Disagreements with Other Published Reviews
Previous systematic reviews/meta-analyses [7–13] have almost all revealed the benefits of acupuncture on PSA. Our review agrees with other studies in the aspect that EA as an adjunct therapy on PSA, though with uncertainty. As an extended technique of acupuncture, studies on systematic synthesis of the evidence on EA for PSA are relatively lacking. A network meta-analysis [15] concluded that the efficacy of EA combined with SLT for PSA was superior to SLT alone in effective rate. The results of this meta-analysis in effective rate are consistent with this network meta-analysis [15]. Furthermore, we also performed subgroup analyses based on treatment duration and assessed the effect of EA on oral expression score, comprehension score, repetition score, naming score, and reading score. In addition, a systematic review [16] of 10 RCTs involving 756 patients conducted in Korea concluded that EA could be considered as an adjunctive therapy for PSA. The difference with our meta-analysis was that it did not perform a quantitative synthesis to assess the relative effect of EA on PSA. Our pooled results are more conducive to the certainty of definitive evidence.
4.3. Implications for Research
Of the 19 included trials, only 8 was rated as low risk bias in randomization process, and none of which reported allocation concealment and blinding information. The sample sizes of the studies ranged from 20 to 120, studies with larger sample sizes, clear information about randomization and allocation concealment methods, and statements about whether participants, personnel, and outcome assessors were blinded are needed to assess the effectiveness of EA for PSA. Future studies should pay particular attention to the effects of EA on long-term functional outcomes. It is worth noting that the EA protocols in each study were diverse, including point selection and stimulation duration; therefore, a more standardized and uniform EA treatment protocol should be advocated, which would also facilitate the promotion of EA. In addition, the studies were all conducted in China, and further reliable studies in other ethnic populations are needed to determine population-specific response differences.
4.4. Potential Mechanism of Action
Although there is currently limited evidence of EA for PSA, the mechanism by which EA improve symptoms of PSA is being confirmed. An MRI study [42] revealed that the language-related brain areas can be activated through EA treatment. A wide range of brain functional areas such as frontal lobe, occipital lobe, parietal lobe, temporal lobe, precuneus, and insula showed active hyperintensity after EA treatment [42]. Similarly, another MRI study also confirmed this finding [43], that stimulation of acupoints associated with language deficits can selectively activate the brain on the lesional side of PSA patients. In addition, it has been found that EA helps to increase blood perfusion in higher speech centers, which in turn improves the ischemic and hypoxic state of brain tissue and awakens nerve cells [44]. The clinical findings were also demonstrated in rat experiments [45]. After receiving EA intervention, the researchers observed significant proliferation of endogenous neural stem cells in rats with cerebral ischemia-reperfusion injury, suggesting that EA can promote the repair of neurological function and reduce secondary nerve injury [45]. Hence, from the potential mechanism of action, EA seems to be a promising method for the treatment of PSA.
4.5. Limitations
There were several potential limitations in this meta-analysis. Firstly, because the included trials lacked follow-up information on EA for PSA, this study could not provide long-term effects of EA for PSA. Secondly, although different acupoint combinations have a significant effect on PSA, our meta-analysis only focused on the overall clinical effect of EA in the treatment of PSA, but did not evaluate the acupoint combination, there it could not provide a basis for specific acupoint selection strategies [46, 47]. Furthermore, the great differences in acupoints pose a challenge to the quantitative findings of this study, so future RCTs should be advocated to adopt standard EA treatment protocols and reduce the generation of heterogeneity to produce more persuasive results.
5. Conclusion
The modality of EA combined with SLT for PSA may improve clinical effectiveness compared to SLT alone, which provides a new option for clinical decision-making. However, limited data, poor methodological quality, and potentially exaggerated effect size evaluation limit the quality of the evidence. More high quality, multi-centers RCTs with large samples are still needed to provide higher evidence.
Acknowledgments
The study was supported by the 13th Chaoyang Talent Project of Guangdong Provincial Hospital of Traditional Chinese Medicine (No. ZY2022YL28), and the Scientific Research Project of Guangdong Provincial Bureau of Traditional Chinese Medicine (No. 20201165).
Abbreviations
- PSA:
Poststroke aphasia
- SLT:
Speech and language therapy
- RCTs:
Randomized clinical trials
- ER:
Effective rate.
Data Availability
The datasets used in the present review are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Authors' Contributions
Yao Shi conceived the study and drafted the manuscript. Caixia Hu, Shuhua Li, Tianhua Huang, Xingsheng Chen, Xiaohui Qin, and Guifu Li implemented the study. All authors read and approved the final manuscript.
Supplementary Materials
Supplementary material: detailed search strategy for PubMed.
References
- 1.Correction to: heart disease and stroke statistics-2017 update: a report from the American heart association. Circulation . 2017;136:p. e196. doi: 10.1161/CIR.0000000000000530. [DOI] [PubMed] [Google Scholar]
- 2.Engelter S. T., Gostynski M., Papa S., et al. Epidemiology of aphasia attributable to first ischemic stroke: incidence, severity, fluency, etiology, and thrombolysis. Stroke . 2006;37(6):1379–1384. doi: 10.1161/01.str.0000221815.64093.8c. [DOI] [PubMed] [Google Scholar]
- 3.Hilari K., Cruice M., Sorin-Peters R., Worrall L. Quality of life in aphasia: state of the art. Folia Phoniatrica et Logopaedica . 2015;67(3):114–118. doi: 10.1159/000440997. [DOI] [PubMed] [Google Scholar]
- 4.Mattioli F. The clinical management and rehabilitation of post stroke aphasia in Italy: evidences from the literature and clinical experience. Neurological Sciences . 2019;40(7):1329–1334. doi: 10.1007/s10072-019-03844-0. [DOI] [PubMed] [Google Scholar]
- 5.Brady M. C., Kelly H., Godwin J., Enderby P. Speech and language therapy for aphasia following stroke. Cochrane Database of Systematic Reviews . 2012;5 doi: 10.1002/14651858.cd000425.pub3.CD000425 [DOI] [PubMed] [Google Scholar]
- 6.Panel O., Khadilkar A., Phillips K., et al. Ottawa panel evidence-based clinical practice guidelines for post-stroke rehabilitation. Topics in Stroke Rehabilitation . 2006;13(2):1–269. doi: 10.1310/3tkx-7xec-2dtg-xqkh. [DOI] [PubMed] [Google Scholar]
- 7.Zhang Y., Wang Z., Jiang X., Lv Z., Wang L., Lu L. Effectiveness of acupuncture for poststroke aphasia: a systematic review and meta-analysis of randomized controlled trials. Complement Med Res . 2021;28(6):545–556. doi: 10.1159/000512672. [DOI] [PubMed] [Google Scholar]
- 8.Tang He-Y., Tang W., Yang F., Wu W., Shen G. Efficacy of acupuncture in the management of post-apoplectic aphasia: a systematic review and meta-analysis of randomized controlled trials. BMC Complementary and Alternative Medicine . 2019;19(1):p. 282. doi: 10.1186/s12906-019-2687-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zhang B., Han Y., Huang X., et al. Acupuncture is effective in improving functional communication in post-stroke aphasia: a systematic review and metaanalysis of randomized controlled trials, Wien. Klin. Wiener Klinische Wochenschrift . 2019;131(9-10):221–232. doi: 10.1007/s00508-019-1478-5. [DOI] [PubMed] [Google Scholar]
- 10.Zhu W. M., Zhong W. J., Xu B., Chen X. H. Meta-analysis on the clinical efficacy of acupuncture combined with speech rehabilitation for aphasia after stroke. Lishizhen Med. Mater. Med. Res. . 2018;29(08):252–257. [Google Scholar]
- 11.Jiang Y. P., Zhou Y. F., Wang B. The efficacy of acupuncture on treating aphasia following stroke: a meta-analysis. Journal of Xinjiang Medical University . 2016;46(10):1237–1241. [Google Scholar]
- 12.Zhang Y., Fu L. X., Zhu Y., Xue P. J. Acupuncture treatment for aphasia after stroke: a systematic review. Journal of Clinical Acupuncture and Moxibustion . 2014;(11):66–69. [Google Scholar]
- 13.Pang Y., Wu L. B., Liu D. H. Acupuncture therapy for apoplectic aphasia: a systematic review. Chinese Acupuncture & Moxibustion . 2010;30(7):612–616. [PubMed] [Google Scholar]
- 14.Huang J., Shi Y., Qin X., Shen M., Wu M., Huang Y. Clinical effects and safety of electroacupuncture for the treatment of poststroke dysphagia: a comprehensive systematic review and meta-analysis. Evidence-based Complementary and Alternative Medicine . 2020;2020:9. doi: 10.1155/2020/1560978.1560978 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhong Y., Qin W. X., Wang Z. J., Yuan Q., Zhu W. T., Zhang Y. Efficacy of acupuncture and moxibustion for aphasia after stroke: a network meta—analysis. Liaoning Journal of Traditional Chinese Medicine . 2021;48(04):17–20+222. [Google Scholar]
- 16.Ha J.-b., Lee S.-J., Yang J.-S., Lew J. H. Electro-acupuncture on aphasia after stroke: a systemic review of randomized controlled trials. The Journal of Internal Korean Medicine . 2021;42(3):323–339. doi: 10.22246/jikm.2021.42.3.323. [DOI] [Google Scholar]
- 17.Julian P. H., Douglas G. A., Jonathan A. S. Assessingrisk of bias in included studies. In: Julian P. H., Sally G., editors. Cochrane Handbook of Systematic Reviewsof InterventionsVersion 5.1.0 . London, UK: Te Cochrane Collaboration; 2011. [Google Scholar]
- 18.Page M. J., McKenzie J. E., Bossuyt P. M., et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ . 2021;372:p. n71. doi: 10.1136/bmj.n71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dekhtyar M., Braun E. J., Billot A., Foo L., Kiran S. Videoconference administration of the western aphasia battery-revised: feasibility and validity. American Journal of Speech-Language Pathology . 2020;29(2):673–687. doi: 10.1044/2019_ajslp-19-00023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tao J., Fang Y., Wu Z., et al. Community-applied research of a traditional Chinese medicine rehabilitation scheme on Broca’s aphasia after stroke: study protocol for a randomized controlled trial. Trials . 2014;15(1):p. 290. doi: 10.1186/1745-6215-15-290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chen C., Liu X., Pan S., Wu X., Wu J. [Neurolinguistic features during recovery of a Chinese patient with pure alexia] Nan Fang Yi Ke Da Xue Xue Bao . 2013;33(5):713–718. [PubMed] [Google Scholar]
- 22.Huang J. K., Qin X. H., Shen M., Huang Y. An overview of systematic reviews and meta-analyses on acupuncture for post-stroke aphasia. European Journal of Integrative Medicine . 2020;37 doi: 10.1016/j.eujim.2020.101133.101133 [DOI] [Google Scholar]
- 23.Wang S. Q., Yuan X., Li M., Xu S. Y., Luo R. H. Clinical study of applying low prequency rTMS associated with electroacupuncture at fengfu and yamen acupoints in the treatment of broca aphasia after stroke. Journal of Sichuan of Traditional Chinese Medicine . 2021;39(01):194–197. [Google Scholar]
- 24.Wang X. P. Effective value of electroacupuncture combined with low frequency repetitive transcranial magnetic stimulation in the treatment of motor aphasia after stroke. Healthmust-Readmagazine. . 2021;11:211–212. [Google Scholar]
- 25.Nie T., Huang Y., Mo C. X. An analysis of treating aphasia after stroke by language rehabilitation training plus scalp electroacupuncture. Clinical Journal of Chinese Medicine . 2020;12(29):80–82. [Google Scholar]
- 26.Ma Y. P., Yang K. Therapeutic effect of scalp electro acupuncture combined with language training on stroke motor aphasia. Chinese Manipulation & Qi Gong Therapy . 2020;11(11):62–64. [Google Scholar]
- 27.Lin M., Lin M. J. Effect of scalp electroacupuncture combined with speech training in the treatment of aphasia after stroke. China Modern Medicine . 2019;26(19):62–65. [Google Scholar]
- 28.Zheng Y. B., Lin S. F. A clinical study of electroacupuncture at lian quan (CV23) and shuai gu (G8) in the treatment of motor aphasia patients after stroke. Chinese Medicine Modern Distance Education of China . 2018;16(9):122–124. [Google Scholar]
- 29.Sun Y. L. Clinical study of speech rehabilitation training combined with electroacupuncture stimulation of nerve trunk therapy in the treatment of stroke speech disorder. Journal of Practical Traditional Chinese Medicine . 2018;34(10):1248–1249. [Google Scholar]
- 30.Yang L., Guo Y. G. Clinical study of scalp electroacupuncture combined with language training on post- stroke aphasia patients. Chinese Journal of Rehabilitation Medicine . 2017;32(3):305–308+312. [Google Scholar]
- 31.Li T., Wang Y., Zhang L. Evaluation of scalp electro—acupuncture combined with speech training on broca language dysfunction after stroke. Journal of Clinical Acupuncture and Moxibustion . 2017;33(9):13–16. [Google Scholar]
- 32.Jiang Y. P., Zhou Y. F., Niu W. Q. Effect of electroacupuncture combined with aphasia training system on Uygur patients with aphasia. Chinese Journal of Gerontology . 2017;37(02):444–446. [Google Scholar]
- 33.Cui N., Yu B., Jiang J. Observation on therapeutic effect of electroacupuncture stimulation of nerve trunk on apoplectic speech disorder. Shaanxi Journal of Traditional Chinese Medicine . 2016;37(07):915–916. [Google Scholar]
- 34.Sheng G. B., Yin X. N., Tang Y. Clinical observation on treatment of non-fluent aphasia after stroke with electroacupuncture in temporal area. Chinese Journal of Traditional Medical Science and Technology . 2015;22(2):p. 235. [Google Scholar]
- 35.Jiang Y., Yang Y., Xiang R., et al. Clinical study of post-stroke speech apraxia treated with scalp electric acupuncture under anatomic orientation and rehabilitation training. Chinese Acupuncture & Moxibustion . 2015;33 [PubMed] [Google Scholar]
- 36.Zhang S. Y., Liu S. B. Observation on therapeutic effect of electroacupuncture stimulation of nerve trunk on apoplectic speech disorder. Chinese Journal of Rehabilitation . 2014;29(5):p. 336. [Google Scholar]
- 37.Du J. Y. Clinical Observation of Electroacupuncture on Speech and Swallowing Disorders Caused by Pseudobulbar Palsy . Harbin, China: Heilongjiang University of Chinese Medicine; 2012. [Google Scholar]
- 38.Aili B. Clinical effect of electroacupuncture combined with rehabilitation training on dysphagia and speech disorder after stroke. Chinese Manipulation & Qi Gong Therapy . 2012;003(009):p. 46. [Google Scholar]
- 39.Li H. X., Liu L. R., Yang Z. C. Clinical study of electroacupuncture on dysphagia and dysphonia after Wallenberg syndrome. Acta Chinese Medicine and Pharmacology . 2007;35(5):24–26. [Google Scholar]
- 40.Zhang X. L., Wang A. P., Zhang J. R. Clinical study of electroacupuncture stimulation combined with language training on aphasia after stroke. Chinese Journal of Practical Nervous Diseases . 2005;8(001):16–17. [Google Scholar]
- 41.Liu L. A., Mou N., He X. Clinical observation on the treatment of apoplectic aphasia by electroacupuncture combined with language training. Chinese Acupuncture & Moxibustion . 2000;20(3):145–148. [Google Scholar]
- 42.Chang J., Zhang H., Tan Z., Xiao J., Li S., Gao Y. Effect of electroacupuncture in patients with post-stroke motor aphasia: neurolinguistic and neuroimaging characteristics. Wiener Klinische Wochenschrift . 2017;129(3-4):102–109. doi: 10.1007/s00508-016-1070-1. [DOI] [PubMed] [Google Scholar]
- 43.Li G., Yang E. S. An fMRI study of acupuncture-inducedbrain activation of aphasia stroke patients. Complementary Therapies in Medicine . 2011;19(1):S49–S59. doi: 10.1016/j.ctim.2010.11.004. [DOI] [PubMed] [Google Scholar]
- 44.Huang J., Wu M., Liang S., et al. A critical overview of systematic reviews and meta-analyses on acupuncture for poststroke insomnia. Evid Based Complement Alternat Med . 2020;2020:7. doi: 10.1155/2020/2032575.2032575 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Zhang Y. G., Gong X., Li H. B. Effects of electroacupuncture on the expressions of nestin and glial fibrilliary Acidic protein in dentate gyrus of focal cerebral ischemia-reperfusion rats. Chinese Journal of Histochemistry and Cytochemistry . 2014;23(2):148–153. [Google Scholar]
- 46.Huang J., Liu J., Liu Z., et al. Reliability of the evidence to guide decision-making in acupuncture for functional dyspepsia. Frontiers in Public Health . 2022;10 doi: 10.3389/fpubh.2022.842096.842096 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Huang J., Lu M., Zheng Y., et al. Quality of evidence supporting the role of acupuncture for the treatment of irritable bowel syndrome. Pain Research and Management . 2021;2021:10. doi: 10.1155/2021/2752246.2752246 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary material: detailed search strategy for PubMed.
Data Availability Statement
The datasets used in the present review are available from the corresponding author on reasonable request.