

Abstract
Background
To date, the optimal treatment for potentially resectable metastatic colorectal cancer (mCRC) patients has yet to be determined. Encouraging results have been reported in studies exploring the efficacy of triplet chemotherapy plus anti-epidermal growth factor receptor (anti-EGFR) target agents. Thus, we conducted a meta-analysis to evaluate the efficacy and safety of triplet chemotherapy plus anti-EGFR target agents.
Methods
We systematically searched the PubMed, Embase, and Web of Science databases from December 2004 to October 2021 for studies examining the efficacy of triplet chemotherapy plus anti-EGFR target agents in mCRC patients. The primary outcomes were the objective response rate (ORR) and R0 resection rate (R0RR), and the secondary outcomes were median progression-free survival (mPFS), median overall survival (mOS), and toxicity. Data were analyzed with R software 4.1.2.
Results
Fourteen studies comprising 762 patients with mCRC were included in this meta-analysis. Analysis with a random effects model revealed that after treatment with triplet chemotherapy plus anti-EGFR target agents, the pooled ORR was 82% (95% CI= 76–88%, I2= 76%), and the pooled R0RR of colorectal liver metastasis (CLM) was 59% (95% CI= 49–68%, I2= 60%). The mPFS ranged from 9.5 to 17.8 months, and the mOS ranged from 24.7 to 62.5 months. A total of 648 grade 3 or 4 adverse events were reported; the most commonly reported events were diarrhea (174/648), neutropenia (157/648), and skin toxicity (95/648), which had pooled prevalence rates of 29% (95% CI= 20–39%, I2= 84%), 28% (95% CI= 20–37%, I2= 77%), and 17% (95% CI= 11–24%, I2= 66%), respectively.
Conclusions
Triplet chemotherapy plus anti-EGFR agents therapy seems to be capable of increasing the ORR of mCRC patients and the R0RR of CLM patients. The toxicity of this treatment is manageable. High-quality randomized controlled trial (RCT) studies are required for further validation.
Supplementary Information
The online version contains supplementary material available at 10.1186/s12957-022-02707-x.
Keywords: Metastatic colorectal cancer, Anti-EGFR, Triplet chemotherapy, Cetuximab, Panitumumab
Background
Colorectal cancer is the third most common malignancy and the second leading cause of cancer-related deaths worldwide. Approximately one-quarter of patients are unresectable or have metastatic colorectal cancer (mCRC) at the initial diagnosis [1]. The 5-year survival rate associated with mCRC is less than 20%, whereas the number is more than 80% in early-stage CRC patients [2].
With recent progress in cancer management, the median overall survival (mOS) of mCRC has widely improved from approximately 6 months (best supportive care) to nearly 30 months after standard systematic treatments in the past 20 years [3]. In addition to new drugs and novel technologies, these improvements are mainly attributed to biomarker-based patient selection and effective therapeutic combination strategies [4, 5]. The first-line therapy plays a critical role in the successful treatment of patients with mCRC, especially for patients with potentially resectable metastases. Triplet chemotherapy, the combination of 5-fluorouracil, irinotecan, and oxaliplatin [2, 6], has been proven to be effective and tolerable in pancreatic cancer with characteristics of rapid tumor shrinkage and improved secondary surgery rate since 2010 [7–9]. This regimen is also gaining importance in the treatment of mCRC. The randomized, controlled, phase 3 TRIBE study compared FOLFOXIRI plus bevacizumab to FOLFIRI plus bevacizumab and showed a better objective response rate (ORR; 65 vs. 54%, P<0.05) and mOS (29.8 vs. 25.8 months, hazard ratio [HR] 0.8, 95% confidence interval [CI] 0.65–0.98, P=0.03) in the triplet plus bevacizumab arm without increasing intolerant toxicity [10]. This finding led to major guideline recommendations for this therapy as a first-line treatment for mCRC patients. Anti-epidermal growth factor receptor (anti-EGFR) target agents (e.g., cetuximab or panitumumab) also proved to have a high response rate in mCRC treatment. The FIRE-3 trial established that in comparison with FOLFIRI plus bevacizumab, a combination of FOLFIRI and cetuximab improved the ORR (77 vs. 65%, P=0.014) and mOS (33 m vs. 26 m, HR=0.75, P=0.011) in rat sarcoma (RAS) gene wild-type patients with left-side disease [11]. Since multiple studies revealed the advanced efficacy of both FOLFOXIRI and anti-EGFR agents (in RAS and BRAF wild-type patients) [12–14], one question was raised: in RAS and BRAF wild-type mCRC patients, will the combination of triplet chemotherapy and anti-EGFR agents improve the ORR or secondary resection rate? Although this regimen is not recommended in major guidelines, there are an increasing number of clinical trials exploring its efficacy and safety [15]. The POTHER trial, the first phase II prospective trial aiming to assess the effectiveness of cetuximab plus triplet chemotherapy in colorectal liver metastasis (CLM), achieved an ORR and secondary R0 resection rate (R0RR) of 79.1% and 60%, respectively, with tolerable toxicity [14]. The VOLFI trial compared the efficacy of panitumumab plus mFOLFOXIRI with FOLFOXIRI alone in 96 patients with RAS wild-type unresectable mCRC randomized into two groups. The ORR in the panitumumab plus mFOLFOXIRI group was significantly higher than that in the FOLFOXIRI group (87.1 vs. 60.6%, odds ratio [OR]: 4.469, 95% CI 1.614–12.376, P=0.0041). However, despite the encouraging results, the majority of the studies were single-arm or retrospective studies, and thus, definitive conclusions about the efficacy and toxicity of anti-EGFR plus triplet chemotherapy could not be drawn.
It is generally acknowledged that meta-analysis is a powerful statistical tool to overcome the limitation of different sample sizes from individual studies and to generate the best estimation. Therefore, we conducted a meta-analysis of all eligible published studies to evaluate the efficacy and safety of triplet chemotherapy plus anti-EGFR agents in treating mCRC patients as a first-line regimen.
Methods
This systematic review and meta-analysis is registered in the PROSPERO database (CRD42021289370, https://www.crd.york.ac.uk/PROSPERO/). It was performed following the meta-analysis (PRISMA) guideline (details were presented in Additional file 1).
Search strategy
We systematically searched the PubMed, Embase, and Web of Science databases for relevant studies published from December 2004 (date of cetuximab approval by the Food and Drug Administration [FDA]) to October 2021. Additionally, abstracts from the American Society of Clinical Oncology (ASCO) annual meeting (December 2004 to 2021), the European Society of Medical Oncology annual meeting (2004–2021), and the World Congress on Gastrointestinal Cancer (2004 to 2021) were screened. Reference lists of included studies were screened to identify other eligible studies. Abstracts from the meetings were searched through the meetings’ official websites to identify relevant citations.
Search strategies included the following:
The PubMed search terms were as follows:
((Colorectal Neoplasm) OR (Colorectal Tumor) OR (Colorectal Cancer) OR (Colorectal Carcinoma)) AND (Cetuximab OR Erbitux OR (IMC C225) OR (MAb C225) OR (C225) OR panitumumab OR (Human Panitumumab Antibody) OR (ABX-EGF MAb) OR (ABX EGF Monoclonal Antibody) OR Vectibix OR anti-EGFR) AND (FOLFOXIRI OR FOLFIRINOX OR (triplet chemotherapy))
The Embase search terms were as follows:
(‘colorectal neoplasm’ OR ‘colorectal tumor’ OR ‘colorectal cancer’ OR ‘colorectal carcinoma’) AND (‘c225’ OR ‘erbitux’ OR ‘imc 225’ OR ‘ly 2939777’ OR ‘Cetuximab’ OR ‘abx egf’ OR ‘panitunumab’ OR ‘vectibex’ OR ‘vectibix’ OR ‘anti-EGFR’) AND (‘FOLFOXIRI’ OR ‘FOLFIRINOX’ OR ‘triplet chemotherapy’)
Search terms for the Web of Science were as follows:
(Colorectal cancer) AND (cetuximab OR Erbitux OR (C225) OR panitumumab OR Vectibix OR anti-EGFR) AND (FOLFOXIRI OR FOLFIRINOX OR (triplet chemotherapy))
Inclusion criteria
Diagnosis: The studied patients were diagnosed with metastatic colorectal adenocarcinoma and pathologically confirmed.
No restriction existed for patient racial/publication status (full text or meeting abstract) as long as data were completed.
Patients were treated with triple chemotherapy (5-fluorouracil, irinotecan, and oxaliplatin/capecitabine) plus anti-EGFR (cetuximab or panitumumab) agent as a first-line chemotherapy.
At least three of the treatment outcomes mentioned below were reported.
The study design included RCTs, prospective nonrandomized trials, and observational studies (prospective or retrospective) published from December 2004 to October 2021 with a sample size of at least 10 patients.
Exclusion criteria
The studies were not written in English.
All patients in the study had a RAS or BRAF mutation.
The studies contained incomplete data on the outcome of interest.
Studies with duplicate data or report analysis.
Data extraction
All candidate articles were evaluated and extracted by two independent authors (H Wang and SQ Zhang). If disagreement occurred, a third author (Q Wu) was consulted. Data were extracted from the eligible studies using a standardized extraction form.
For each study, the following data were extracted: first author, year of publication, country, study period, median age, total number of cases, sex ratio, study design, treatment strategy, RAS status, BRAF status, ORR, number of liver-limited patients, R0 resection rate (R0RR), mPFS, mOS, follow-ups, and grade 3/4 adverse effects. The characteristics of the selected studies are shown in Table 1.
Table 1.
Summary of the study characteristic
| Author/year | Country/period of study | Trial name | Study design | Total patients | Gender(M/F) | Median age (years, range) | Primary location | RAS wt/mt/unknown | BRAF wt/mt/unknown |
Primary endpoint | ORR (%) | mPFS (month) | mOS (month) | CLM/R0RR in CLM | mfollow-up (month, range) | MINORS |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C Garufi [14]*/2010 | Italy/2006–2008 | POCHER | Pros-, case series | 43 | 27/16 | 61 (33–75) | 34/9a | 30/7/6d | NA | ORR | 79.1% | 14 | 37 | 43/60% | 22 (1–43) | 16 |
| Sougklakos I [16]/2011 | Greece/2007–2010 | - | Pros-, case series | 30 | 16/14 | 64 | NA | 30/0d | NA | ORR | 70% | 11e | NR | 16/57% | 15.1 (NA) | 14 |
| ERIC ASSENAT [17]/2011 | France/2006–2008 | ERBIRINOX | Pros-, case series | 42 | 22/20 | 60 (32–76) | 30/12a | 24/16/2d | NA | CRR | 80.90% | 9.5 | 24.7 | 15/NA | 18.1 (0.4–39.6) | 16 |
| Z Saridaki [18]/2012 | Greece/2007–2010 | - | Pros-, case series | 30 | 14/16 | 64 (36–70) | 22/8a | NA | NA | ORR | 70% | 10.2e | 30.3 | 16/62% | 31 (13–37) | 16 |
| Folprecht, G [19]/2013 | Germany/2014–2018 | CELIM2 | Pros-, cohort | 28 | NA | NA | NA | 28/0/0d | 28/0/0 | ORR | 86% | 15 | 55 | NA | NA | 22 |
| Fornaro, L [20]/2013 | Italy/2010–2011 | TRIP | Pros-, case series | 37 | 21/16 | 63 (33–72) | 26/11a | 37/0/0d | 37/0/0 | ORR | 89% | 11.3 | NR | 12/75% | 17.7 (NA) | 16 |
| Bendell, J. C [21]*/2016 | USA/NA | - | Pros-, case series | 15 | 13/2 | 55 (39–70) | NA | 8/0/7d | NA | ORR | 60% | 13.3 | NR | 15/67% | 15 (NA) | 16 |
| PietrantonioF [22]/2017 | Italy/NA | - | Pros-, case series | 31 | NA | NA | NA | NA | NA | ORR | 87% | 17.8 | 62.5 | 31/84% | 48 (NA) | 14 |
| Cremolini, C [23]/2018 | Italy/2011–2015 | MACBETH | Pros-, multi-center, cohort | 116 | 82/34 | 59.5 (53–67) | 95/21b | 116/0/0 | 116/0/0 | 10m PFR | 71.60% | 10.1 | 33.2 | 52/51.9% | 44 (30.5–52.1) | 24 |
| D Modest [24]/2019 | Germany/NA | VOLFI | RCT, multi-center | 63 | 41/22 | 58 (31–76) | 53/10b | 63/0/0 | 43/7/13 | ORR | 87.3% | 9.7 | 35.7 | NA | 44.2 (NA) | 14 |
| Ogata, T [25]./2019 | Japan/2014–2017 | - | Retro-, cohort | 17 | NA | 60 | 14/3b | 17/0/0 | NA | ORR | 100% | 13.1 | NR | NA | 18.4 (NA) | 21 |
| E Samalin [26]*/2019 | NA | ESTER | Retro-, case series, multi-center | 70 | 43/27 | 58.7 (40.4–74) | 57/13b | 70/0/0 | NA | PFS | 85.70% | 13.3 | 48.5 | 68/79.5% | 49.2 (1.2–135) | 13 |
| Deng, Y [27].*/2020 | China/2014–2019 | FOCULM | Pros-, case series, multi-center | 67 | 58/9 | 52 (28–70) | 66/1b | 67/0/0 | 67/0/0 | Rate of NED | 95.50% | 15.5 | NR | 67/46.3% | 22.6 (NA) | 16 |
| Akihito Tsuji [28]/2021 | Japan/2015–2019 | DEEPER | RCT | 173 | NA | 65 | NA | 173/0/0 | NA | mDpR | 69.10% | 12.7 | 37.6 | NA | NA | 22 |
*All included patients were diagnosed as liver-limited colorectal cancer; acolon/rectum, bleft/right, c14 patients with cetuximab, 3 patients with panitumumab; donly KRAS; etime to progression, TTP; wt, wild-type, mt, mutant-type, ORR objective response rate, mPFS median progression-free survival, mOS median overall survival, CLM colorectal liver-limited metastases, R0RR R0 resection rate, mfollow-up median follow-up, MINORS methodological index for non-randomized studies, pros- prospective study, retro- retrospective study, NA not available, NR not reached, CRR complete response rate, mDpR median depth of response
The primary outcomes were ORR and R0RR in liver-limited mCRC patients. The secondary outcomes were mPFS, mOS, and grade 3/4 toxicity rate. ORR was defined as the ratio between the number of patients achieving an objective response (complete or partial response) and the total number of patients.
Quality assessment
Because both case series and cohort studies were included in this meta-analysis, the Methodological Index for Non-Randomized Studies (MINORS) was used by two independent authors (H Wang and SQ Zhang) to assess the quality of the studies. The MINORS comprises 12 methodological items with a maximum score of 24. The first eight items (i.e., a clearly stated aim, inclusion of consecutive patients, prospective collection of data, endpoints appropriate to the aim of study, unbiased assessment of the study endpoint, follow-up period appropriate to the aim of the study, loss to follow-up less than 5%, prospective calculation of the study size) apply to both comparative and noncomparative studies, whereas the remaining four items (i.e., an adequate control group, contemporary groups, baseline equivalence of groups, adequate statistical analyses) apply only to comparative studies. A score lower than 10 for a case-series study or lower than 16 for a cohort study indicates low quality, and studies with such scores were excluded. The MINORS scores of the included studies are shown in Table 1. None of the studies was excluded on the basis of their score. Details on the MINORS score of each study are presented in Table 2.
Table 2.
MINORS checklist for included studies
| Study | Garufi | Sougklakos | ASSENAT | Saridaki | Folprecht | Fornaro | Bendell | Pietrantonio | Cremolini | Modest | Ogata | Samalin | Deng | Tsuji |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Methodological items for non-randomized studies | ||||||||||||||
| A clearly stated aim | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Inclusion of consecutive patients | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Prospective collection of data | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 2 |
| Endpoints appropriate to the aim of study | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Unbiased assessment of the study endpoint | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Follow-up period appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Loss to follow up less than 5% | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Prospective calculation of the study size | 2 | 0 | 2 | 2 | 0 | 2 | 2 | 0 | 2 | 0 | 0 | 0 | 2 | 0 |
| Additional criteria for comparative studies | ||||||||||||||
| An adequate control group | - | - | - | - | 2 | - | - | - | 2 | - | 2 | - | - | 2 |
| Contemporary groups | - | - | - | - | 2 | - | - | - | 2 | - | 2 | - | - | 2 |
| Baseline equivalence of groups | - | - | - | - | 2 | - | - | - | 2 | - | 2 | - | - | 2 |
| Adequate statistical analyses | - | - | - | - | 2 | - | - | - | 2 | - | 2 | - | - | 2 |
| Total | 16 | 14 | 16 | 16 | 22 | 16 | 16 | 14 | 24 | 14 | 21 | 13 | 16 | 22 |
The items are scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate). The global ideal score being 16 for non-comparative studies and 24 for comparative studies
Statistical analysis
Statistical analyses were performed using the meta package of R 4.1.2 software. After data evaluation, we chose Freeman-Tukey double arcsine transformation to process the data presented as proportions with ORR, R0RR, and any grade 3/4 toxicity rate. We then aggregated using the inverse variance random-effect method (DerSimonian–Laird estimate). CIs for the individual studies were calculated based on the Clopper-Pearson interval method. Cochrane’s Q test and Higgins I-squared statistic were used to assess the heterogeneity of the included trials. P<0.1 in the Q test or I2>50% suggested significant heterogeneity. When significant heterogeneity was observed, the random effects model was used. Otherwise, the fixed effects model was adopted to evaluate the 95% CI. The sensitivity analysis was applied to explore the origin of heterogeneity. Publication bias was assessed by a visual inspection of the funnel plot, and the possibility of publication bias was assessed by Egger’s test.
Results
Search results and study characteristics
A flow chart of the search strategies and reasons for exclusion is shown in Fig. 1.
Fig. 1.
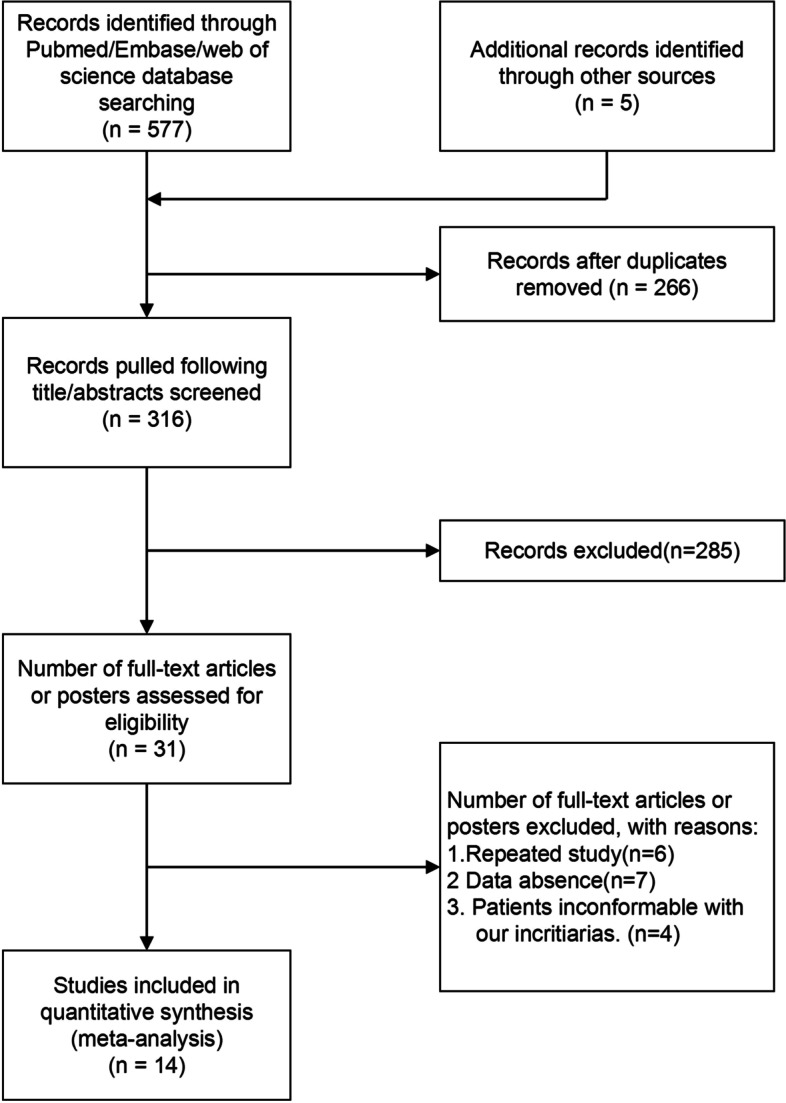
Flow diagram of literature search and study selection
In total, 577 potential articles were initially identified through the database, 266 articles were eliminated because of duplicate data, and 285 articles were removed after screening the title and abstract. The remaining 31 articles were retrieved for further assessment. Finally, 14 studies comprising 762 patients with mCRC were included in this meta-analysis. Among them, five studies were only described in conference abstracts.
The characteristics and study quality of all the included studies were evaluated by the MINORS and are presented in Table 2. Twelve studies were prospective, four were two-arm comparative cohort studies, ten were prospective/retrospective case series, four were multi-center investigations, and five were available only as conference abstracts or posters. A total of 762 patients were included across 14 studies. The median age range was 52–64 years (available in 11 studies), and the overall sex distribution was 338/175 (10 studies). All patients had an Eastern Cooperative Oncology Group (ECOG) performance status score of 0–1. RAS and BRAF mutations were detected in 701 and 311 patients, respectively. Among the 701 patients who accepted the RAS mutation test, 157 were KRAS wild-type, 390 were RAS wild-type (all tests were amended to the RAS test after the FDA changed its instructions for cetuximab), and 23 were KRAS mutants (all participated before the discovery of the negative role played in anti-EGFR agent treatment). Tumor primary locations were presented in 316 patients from 5 studies: 48 patients with tumors in the colon (side unspecified), 35 patients with tumors in the right colon, and 233 patients with tumors in the left colon or rectum. All patients were treated by a triplet chemotherapy (combination of 5-fluorouracil, irinotecan, and oxaliplatin/capecitabine) plus anti-EGFR agents (cetuximab or panitumumab). Details of the regimen in each study are shown in Table 3. Median cycles of chemotherapy were reported in eight studies with a range of 1–12. The metastasis location of 321 patients from 10 studies was limited to the liver; secondary R0RRs of these patients were reported in nine studies. In the four two-arm comparative studies, the treated arms included mFOLFOXIRI alone, mFOLFOXIRI plus anti-VEGF, and doublet chemotherapy (FOLFOX or FOLFIRI) plus anti-EGFR (one study).
Table 3.
Summary of dose used in studies
| Study | Treatment/median cycles (range) | Dose | Dose reduction or dose intensity | |||
|---|---|---|---|---|---|---|
| Anti-EGFR | L-OHP (mg/m2) | CPT-11 (mg/m2) | 5-FU (mg/m2) | |||
| C Garufi/2010 [14] | Cet+Chrono-IFLO/6 (3–15) | Cet (400mg/m2 initial, 250 weekly mg/m2) | 80 | 130 | 2400 |
L-OHP:60mg/m2 CPT-11:110mg/m2 5-FU:2200mg/m2 |
| Sougklakos, I./2011 [16] | Cet+FOLFOXIRI/NR | Cet 500mg/m2 | 65 | 150 | 600+400 (bolus) | NA |
| ERIC ASSENAT./2011 [17] | Cet+FOLFIRINOX/9 (1–12) | Cet (400 initial/250 weekly) | 85 | 180 | 2400+400 (bolus) | 76%required dose reduction, overall dose intensity was >90% |
| Z Saridaki/2012 [18] | Cet+FOLFOXIRI/12 (1–16) | Cet 500mg/m2 | 65 | 150 | 1200+400 (bolus) | NA |
| Folprecht, G./2013 | Cet+FOLFOXIRI/NR | Cet 500mg/m2 | 85 | 125 | 3200 | NA |
| Fornaro, L./2013 [20] | Pan+FOLFOXIRI/11 (3–16) | Pan 6mg/kg | 85 | 150 | 3000 | Relative dose intensity: L-OHP 75%, CPT-11 74%, 5-FU 76% |
| Bendell, J. C./2016 [21] | Pan+FOLFOXIRI/NA | Pan 6mg/kg | 85 | 125 | 3200 | NA |
| Pietrantonio, F/2017 [2017] | Cet+COI-E/NA | 500mg/m2 | 85 | 180 | 1000 twice d2-5b | NA |
| Cremolini, C./2018 [23] | Cet+FOLFOXIRI/8 (6–8) | Cet 500mg/m2 | 85 | 130 | 2400 | NA |
| D Modest/2019 [24] | Pan+FOLFOXIRI/11 (2–12) | Pan 6mg/kg | 85 | 165 | 3200 | NA |
| Ogata, T./2019 [25] |
Cet+FOLFOXIRI/7 (1–14) Pan+FOLFOXIRI/12 (9–12) |
Cet (400mg/m2 initial, 250 weekly mg/m2) | 85 | 125/150/165a | 3200 | NA |
| E. Samalin/2019 [26] | Cet+FOLFIRINOX/10 (2–12) | NA | NA | NA | NA | NA |
| Deng, Y./2020 | Cet+mFOLFOXIRI/7 (4–12) | Cet 500mg/m2 | 85 | 165 | 2800 | Relative dose intensity: L-OHP 96%, CPT-11 96%, 5-FU 96% |
| Akihito Tsuji/2021 [28] | Cet+mFOLFOXIRI/10 (1–12) | Cet 500mg/m2 | 85 | 150 | 2400 | NA |
aModified on UGT1A1 status; bcapecitabine; Cet, cetuximab; Pan, panitumumab; CPT-11, irinotecan; L-OHP, oxaliplatin; 5-FU, 5-fluorouracil; mFOLFOXIRI, modified FOLFOXIRI; COI-E, irinotecan+oxaliplatin+capecitabine; NA, not available
Primary outcomes
Objective response rate and R0 resection rate
A total of 763 patients from 14 studies were analyzed. The ORR from individual studies ranged from 60 to 100%. The pooled ORR was 82% (95% CI=76–88%, I2=76%; Fig. 2), and a random effects model was used. The responses to all included studies were evaluated by Response Evaluation Criteria in Solid Tumors (RECIST) criteria. Among the 14 studies, 9 studies presented the secondary R0RR in patients diagnosed with unresectable colorectal liver metastases (CLM). After accepting triplet chemotherapy plus an anti-EGFR agent therapy, 179 out of 321 CLM patients achieved R0RR. The range of R0RR was 46.3 to 84%, and the pooled R0RR was 59% with a random effects model (95% CI=50–69%, I2=60%). The forest plots of ORR and R0RR are shown in Figs. 2 and 3, respectively.
Fig. 2.

Forest plot of ORR in mCRC patients treated with triplet chemotherapy plus an anti-EGFR. ORR, objective response rate; mCRC, metastasis colorectal cancer
Fig. 3.

Forest plot of R0RR in CLM patients treated with triplet chemotherapy plus an anti-EGFR. R0RR, R0 resection rate; CLM, colorectal liver metastasis
Secondary outcomes
Median progression-free survival and median overall survival
The mPFS and mOS were obtained in 14 and 9 studies, respectively. The median PFS ranged from 9.5 to 17.8 months, and the mOS ranged from 24.7 to 62.5 months (Table 1).
Grade 3/4 adverse events
Thirteen studies reported grade 3/4 adverse events. In these studies, 648 grade 3/4 adverse events were observed among 731 patients who accepted triplet chemotherapy plus anti-EGFR agent therapy. One study reported a treatment-related toxic death related to neutropenic septicemia. The grade 3/4 toxicities described the most were diarrhea (174/648), neutropenia (157/648), and skin toxicity (95/648). The pooled rates were 29% (95% CI=20–39%, I2=86%), 28% (95% CI=20–37%, I2=77%), and 17% (95% CI=11–24%, I2=66%), respectively. A forest plot of each is shown in Figs. 4, 5, and 6. Toxicity profiles were not completed in five studies that were only available as a conference abstract. Most of the side effects were treatable. There were three studies that reduced the dose for a high incidence of adverse events (two because of diarrhea; one because of febrile neutropenia). All of them observed a significant decrease in toxicity after reduction. The toxicity profile is presented in Table 4.
Fig. 4.

Forest plot of grade3/4 diarrhea in mCRC patients treated with triplet chemotherapy plus anti-EGFR. ORR, objective response rate; mCRC, metastatic colorectal cancer
Fig. 5.

Forest plot of grade3/4 neutropenia in mCRC patients treated with triplet chemotherapy plus anti-EGFR. ORR, objective response rate; mCRC, metastatic colorectal cancer
Fig. 6.

Forest plot of grade3/4 skin toxicity in mCRC patients treated with triplet chemotherapy plus anti-EGFR. ORR, objective response rate; mCRC, metastatic colorectal cancer
Table 4.
Summary of grade 3/4 toxicity in patients treated by triplet chemotherapy plus anti-EGFR agents
| Author | Total | Neutropenia | FN | Thrombopnia | Diarrhea | Nausea/vomiting | Anorexia | Stomatitis | Asthenia | Skin toxicity | Neurotoxicity | HFS | Hypomagnesemia | Others |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| C Garufi | 43 | 2 | - | - | 15 | 4 | - | - | 5 | 6 | - | - | - | 3 |
| Sougklakos, Ia | 30 | 7 | NA | NA | 16 | NA | NA | NA | NA | 13 | 5 | NA | NA | NA |
| ERIC ASSENAT | 42 | 16 | 2 | 5 | 22 | 4 | 10 | - | 13 | 14 | 8 | 4 | - | 4 |
| Z Saridaki | 30 | 7 | 1 | 2 | 16 | 5 | - | 3 | - | 1 | - | 1 | - | 1 |
| Folprecht, Ga | 28 | 13 | NA | NA | NA | NA | NA | NA | NA | 5 | NA | NA | NA | NA |
| Fornaro, L | 37 | 18 | 2 | - | 13 | 5 | - | 5 | 10 | 5 | 3 | 1 | 5 | - |
| Bendell, J. C | 15 | 2 | - | 1 | 5 | 1 | 2 | - | 3 | 3 | - | 1 | 1 | 2 |
| Cremolini, C | 116 | 36 | 4 | - | 21 | 3 | 4 | 7 | 11 | 18 | - | - | - | - |
| D Modest | 63 | 10 | - | - | 16 | 6 | - | 6 | 5 | 9 | 2 | 4 | 3 | 17 |
| Ogata, T | 17 | 10 | - | - | 2 | 1 | - | - | - | - | - | - | 2 | - |
| E. Samalina | 70 | 15 | 2 | NA | 22 | NA | NA | NA | NA | NA | NA | NA | NA | NA |
| Deng, Y | 67 | 21 | 2 | 1 | 5 | 1 | - | 1 | 1 | - | 3 | - | - | 6 |
| Akihito Tsujia | 173 | NA | NA | NA | 21 | NA | NA | NA | NA | 21 | NA | NA | 7 | NA |
| Total | 731 | 157 | 13 | 9 | 174 | 30 | 16 | 22 | 48 | 95 | 21 | 11 | 18 | 33 |
aToxicity profile uncompleted; FN febrile neutropenia, HFS hand/foot syndrome, NA not available
Publication bias
As shown in Figs. 7 and 8, the possible publication bias of the included studies was assessed by the funnel plot test and Egger’s linear regression test. No significant publication bias was detected from statistical tests based on ORR (t=1.33, P=0.2083).
Fig. 7.

Funnel plot of ORR in mCRC patients treated with triplet chemotherapy plus anti-EGFR. ORR, objective response rate; mCRC, metastatic colorectal cancer
Fig. 8.

Egger’s test of ORR in mCRC patients treated with triplet chemotherapy plus anti-EGFR. ORR, objective response rate; mCRC, metastatic colorectal cancer
Discussion
To the best of our knowledge, our study is the first meta-analysis evaluating the efficacy of triplet chemotherapy plus anti-EGFR agent therapy. Nevertheless, there are multiple reviews and studies of this topic, which implies that researchers have devoted considerable attention to this important issue. Our meta-analysis combined the outcomes of 762 mCRC patients treated with triple chemotherapy plus anti-EGFR therapy from 14 studies, indicating that the treatment can improve the ORR to 82% and improve the secondary R0 rate without increasing the G3/4 adverse effect.
Despite the large number of studies comparing the efficacy of different regimens in mCRC first-line treatment, the optimal therapy is still controversial [29, 30], especially in CLM patients or potentially resectable mCRC patients who may need more intensive treatment to achieve distinct tumor shrinkage to purchase the chance of secondary surgery [31]. Since both FOLFOXIRI and anti-EGFR target therapy were considered to be related to more rapid tumor responses, we conducted this meta-analysis to assess the efficacy and safety of their combination.
In our meta-analysis, the pooled ORR of patients who accepted triplet chemotherapy plus anti-EGFR therapy was 82% (95% CI=76–88%, I2=76%), ranging from 60 to 100%. For comparison, we summarized several meta-analyses of important studies in mCRC treatment. Details are presented in Table 5. This result clearly dominates the efficacy of all the other treatments. This indicates that triplet chemotherapy plus anti-EGFR therapy conspicuously increases the chance of secondary resection in mCRC patients. The same advantages can be observed in other outcomes, such as the R0RR of CLM, mPFS, and mOS. A possible explanation of such a remarkable improvement is discussed below.
Table 5.
Summary of related meta-analysis for a first-line treatment of mCRC
| Meta-analysis | Included studies | Treatment | ORR | mPFS (month) | mOS (month) | SRR | Grade3/4 toxicity |
|---|---|---|---|---|---|---|---|
| Cremolini C [32] |
CHARTA OLIVIA STEAM TRIBE TRIBE2 |
bev+3-CT vs bev+2CTa |
64.5 vs 53.6% OR 1.57, P<0.001 |
12.2 vs 9,9 HR:0.74, P<0.001 |
28.9 vs 24.5 HR:0.81, P<0.001 |
16.4 vs 11.8% OR 1.48, P=0.007 |
Neutropenia 45.8 vs 21.5%; P<0.001 FN 6.3 vs 3.7%; P=0.019 Diarrhea 17.8 vs 8.4%; P<0.001 |
| C Bokemeyer [33] |
CRYSTAL OPUS |
Cet+2CT vs 2CT |
60.7 vs 40.9% OR 2.27, P <0.0001 |
10.9 vs 7.7 HR 0.64, P<0.0001 |
24.8 vs 21.1 HR 0.84, P =0.0048 |
NA | NA |
| F Pietrantonio [34] |
Valentino TRIBE TRIBE2 STEAM CHARTA. |
pan+3CT vs bev+3CT |
73 vs 77% OR 0.79, P =0.4 |
11.4 vs 13.3 HR 0.83, P =0.11 |
30.3 vs 33.1 HR 0.8, P =0.14 |
22 vs 18% P =0.51 |
Neutropenia 26 vs 48%; P =0.001 Diarrhea 14 vs 6%; P =0.82 Febrile stomatitis 8 vs 6%; P =0.67 |
| G Tomasello [35] | 11 studies | Bev+3CT |
69% (95%CI, 65–72%) |
12.4 (95%CI,10-14.3) |
30.2 (95%CI,26.5-33.7) |
36.6% (95%CI,24.6%-50.5%) |
NA |
aAll KRAS and BRAF wild type; ORR Objective response rate, SRR Secondary resection rate, mPFS Median progression-free survival, mOS Median overall survival, 2CT Doublet chemotherapy, 3CT Triplet chemotherapy, FN Febrile neutropenia
RAS and BRAF mutation status
KRAS codons 12 and 13, 61, HRAS, NRAS, and BRAF V600E mutations are the most important and widely studied biomarkers for anti-EGFR agents. Both RAS and BRAF mutations have been proven to be prognostic factors associated with worse survival [36]. Because anti-EGFR target therapy is not recommended for patients with RAS or BRAF mutations, there were notable differences in patient baseline gene status selection in the included studies. In our meta-analysis, among the 701 patients who accepted the RAS mutation test, 157 were KRAS wild-type, 390 were RAS wild, and three were KRAS mutants. Among the 311 patients who accepted the BRAF mutation test, 291 were wild-type, and seven were mutant. It is assumed that the impressive efficacy was associated with the large number of RAS and BRAF wild-type patients.
Primary tumor side
There is now a consensus that the primary tumor side of mCRC is biologically distinct [37]. The CALGB/SWOG 80405 study presented a significantly longer mPFS and mOS of the left side than the right side (mOS 33.3 months vs. 19.4 months, P<0,001) [38]. Subgroup analysis showed that in left-side-originated mCRC patients, compared with doublet chemotherapy plus bevacizumab, the combination of doublet chemotherapy and cetuximab was associated with a significantly longer mOS (36 vs. 31.4 months, P=0.018). This advantage was not reflected in the right-side originated mCRC patients; the mOS of cetuximab-arm and bevacizumab-arm were 16.7 vs. 24.2 months, P=0.065 [39]. The same tendency was found in the sub-analysis of trials FIRE-3 and PEAK [9, 40]. Based on this evidence, guidelines recommended treatment separately according to the primary tumor side. Anti-EGFR-targeted therapy is only recommended in left-side colon cancer combined with doublet chemotherapy, including FOLFOX, FOLFIRI, and XELOX [41]. In our meta-analysis, among the 762 patients included, tumor primary location was reported for 316 patients from five studies, including 48 patients with tumors in the colon, 35 patients with tumors in the right colon, and 233 patients with tumors in the left colon or rectum. Thus, a large proportion of left colon or rectal cancer patients may be one reason for our high ORR.
R0 resection rate and conversion therapy
Conversion therapy is a standard therapy for mCRC patients, especially for patients with CLM. Recent studies verified that CLM is a particular type of mCRC that is heterogeneous to other mCRC patients [37]. Convincing evidence has proven that the R0RR of CLM can significantly increase the 5-year survival rate and mOS [42]. This inspiring discovery reflects the importance of seeking optimal treatment for the appropriate patients. The new treatment goal of CLM is currently to maximize the possibility of eradicating all LM lesions, which require rapid and distinct tumor shrinkage [43]. In our meta-analysis, the pooled R0RR in CLM patients was 60% with a random effects model (95% CI=49–70%, I2=69%). Among the 14 included studies, five studies were designed specifically to evaluate the R0RR of CLM after treatment with triplet chemotherapy plus anti-EGFRs agent, and the R0RR ranged from 60 to 84%. Despite these encouraging results, there were an additional 14 patients from two studies who accepted R1 resection (two patients) or R2 resection (12 patients). Other important indices for conversion therapy include early tumor shrinkage and depth of response (DpR), which were verified as capable of predicting treatment outcomes and cetuximab efficacy [44, 45]. Two studies used these indices as end points. The FOCULM study demonstrated that compared with mFOLFOXIRI alone, the addition of cetuximab improved the DpR from 44 to 56.1% (P=0.012), and the overall resection rates were 55.2% and 29.4%, respectively [27]. Consistent results of R0RR were presented in the POCHER trial (60%, 95% CI=45.8–75.1%), and another study conducted by E Samalin (57.4%) [14, 26]. All the results mentioned above demonstrated that the use of triplet chemotherapy plus the anti-EGFR agents significantly increased the possibility of the R0 resection of CLM patients, indicating that this treatment is preferable for CLM patients. It is important to identify the possible molecular and genetic markers of the patients who may benefit most from the treatment. As evidence has shown that anti-EGFR treatment is more effective in left-side colorectal cancer [46], it is safe to hypothesize that RAS and BRAF wild-type patients with liver metastatic left-sided cancer may possibly be the selected group to benefit most from triplet chemotherapy plus anti-EGFR agent therapy. We should acknowledge the small sample size and low quality of the included studies. This hypothesis needs to be tested in large-scale RCTs.
Toxicity and dose adjustment
The most commonly observed adverse event in our study was diarrhea (174/648), followed by neutropenia (157/648) and skin toxicity (95/648). The toxicity profile was slightly different from that of triplet chemotherapy plus anti-VEGF therapy, in which neutropenia was the most frequently observed grade 3/4 adverse event, with an incidence of 45.8%, and the incidence of diarrhea was only 17.8% [30]. In our meta-analysis, the pooled rates were 29% (95% CI=20–39%, I2=86%), 28% (95% CI=20–37%, I2=77%), and 17% (95% CI=11–24%, I2=66%) for diarrhea, neutropenia, and skin toxicity, respectively. Three studies reported a dose reduction after a high incidence of toxicity, mainly because of diarrhea and neutropenia. After a dose adjustment, all studies considered the side effects manageable through symptomatic measures. The detailed dosage of each drug is presented in Table 2. Two studies pointed out that dose reduction did not influence efficacy. The results should be interpreted discreetly due to the retrospective design and small sample size. It should also be noted that nearly all included patients had an ECOG performance score of 0–1.
Future prospects
With the development of surgery and toxicity management, the role of conversion therapy has become increasingly important in colorectal cancer treatment, especially in CLM patients. Thus, anti-EGFR plus triplet chemotherapy, which is considered to be able to increase the secondary surgery rate, has attracted researchers’ attention. However, despite the inspiring results mentioned above, several questions still should be answered. First, we discuss the dose and the treatment schedule of this therapy. It should be noted that the drug dose and treatment cycles in each clinical trial were not completely in accordance. Patients in several trials experienced dose reduction. In addition, there were also apprehensions about the adjuvant or second-line treatment selection. The second question relates to treatment endpoints. Since one of the important objectives of anti-EGFR plus triplet chemotherapy treatment was to enhance the R0RR, some clinical trials chose ETS and DpR as primary endpoints instead of the ORR, which is the most frequently used endpoint. These indices might be easier for readers to interpret. However, we should not neglect our ultimate purpose, which is to prolong overall survival. Thus, complete follow-up is necessary for the final evaluation of this treatment. Third, the optimal criteria for patient selection remain unclear. It remains unclear how we can identify suitable treatment for patients according to their gene status, original side, metastatic condition, and so on. Fortunately, there are several ongoing RCTs, including DEEPER (mFOLFOXIRI+cetuximab vs. mFOLFOXIRI+bevacizumab, NCT02515734), TRIPLETE (mFOLFOXIRI+panitumumab vs. mFOLFOX6+panitumumab, NCT03231722), and PANIRINOX (mFOLFIRINOX+panitumumab vs. mFOLFOX6+panitumumab, NCT02980510), which aim to compare the efficacy of different combinations of doublet or triplet chemotherapy plus different target agents, and their results may be helpful in this regard.
Limitations
This study has several limitations that should be recognized. First, the eligible studies and the sample sizes of the included studies were relatively small. Heterogeneity between studies was relatively high, which may bias the results. Despite the utility of sensitivity analysis, the origin of heterogeneity could not be fully traced. Second, most of the studies were case series or retrospective studies, which may influence the accuracy of the results (especially in the assessment of adverse events). Third, a portion of the studies were only obtainable as conference abstracts. Despite efforts made to get in touch with authors for complete results, there remained crucial data uncollected. Fourth, the dosage of each study was not consistent; one of the included studies used capecitabine instead of 5-fluorouracil, affecting the outcome of the study and toxicity evaluation. Finally, this study was constrained to studies published in the English language only. Thus, the potential for publication bias cannot be ignored.
Conclusion
Triplet chemotherapy plus anti-EGFR therapy seems to be capable of increasing the ORR of mCRC patients and R0RR of CLM patients. The toxicity of this treatment is manageable. High-quality RCT studies are required for further validation.
Supplementary Information
Acknowledgements
Not applicable.
Abbreviations
- mCRC
Metastatic colorectal cancer
- anti-EGFR
Anti-epidermal growth factor receptor
- ORR
Objective response rate
- R0RR
R0 resection rate
- mPFS
Median progression-free survival
- mOS
Median overall survival
- RCT
Randomized controlled trial
- CLM
Colorectal liver metastasis
- HR
Hazard ratio
- CI
Confidence interval
- RAS
Rat sarcoma
- FDA
Food and Drug Administration
- ASCO
American Society of Clinical Oncology
- MINORS
Methodological Index for Non-Randomized Studies
- ECOG
Eastern Cooperative Oncology Group
- RECIST
Response Evaluation Criteria in Solid Tumors
- DpR
Depth of response
- TTP
Time to progression
- wt
Wild-type
- mt
Mutant-type
- pros-
Prospective study
- retro-
Retrospective study
- NA
Not available
- NR
Not reached
- CRR
Complete response rate
- Cet
Cetuximab
- Pan
Panitumumab
- CPT-11
Irinotecan
- L-OHP
Oxaliplatin
- 5-FU
5-Fluorouracil
- mFOLFOXIRI
Modified FOLFOXIRI
- FN
Febrile neutropenia
- HFS
Hand/foot syndrome
- SRR
Secondary resection rate
- 2CT
Doublet chemotherapy
- 3CT
Triplet chemotherapy
Authors’ contributions
Conceptualization: QW. Data curation: HW, SQZ. Formal analysis: WY, HW. Methodology: QW, GDH. Software: WJP, QW. Supervision: WBG. Writing: QW, YFZ. The author(s) read and approved the final manuscript.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Torre LA, Siegel RL, Ward EM, Jemal A. Global cancer incidence and mortality rates and trends--an update. Cancer Epidemiol Biomarkers Prev. 2016;25(1):16–27. doi: 10.1158/1055-9965.EPI-15-0578. [DOI] [PubMed] [Google Scholar]
- 2.Engstrand J, Nilsson H, Stromberg C, Jonas E, Freedman J. Colorectal cancer liver metastases - a population-based study on incidence, management and survival. BMC Cancer. 2018;18(1):78. doi: 10.1186/s12885-017-3925-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.De Falco V, Napolitano S, Roselló S, Huerta M, Cervantes A, Ciardiello F, Troiani T. How we treat metastatic colorectal cancer. ESMO Open. 2020;4(Suppl 2):e000813. doi: 10.1136/esmoopen-2020-000813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Maher B, Ryan E, Little M, Boardman P, Stedman B. The management of colorectal liver metastases. Clin Radiol. 2017;72(8):617–625. doi: 10.1016/j.crad.2017.05.016. [DOI] [PubMed] [Google Scholar]
- 5.López RI, Castro JL, Cedeño H, Cisneros D, Corrales L, González-Herrera I, Lima-Pérez M, Prestol R, Salinas R, Soriano-García JL, T Zavala A, Zetina LM, Zúñiga-Orlich CE. Consensus on management of metastatic colorectal cancer in Central America and the Caribbean: San José, Costa Rica, August 2016. ESMO Open. 2018;3(3):e000315. doi: 10.1136/esmoopen-2017-000315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Modest DP, Pant S, Sartore-Bianchi A. Treatment sequencing in metastatic colorectal cancer. Eur J Cancer. 2019;109:70–83. doi: 10.1016/j.ejca.2018.12.019. [DOI] [PubMed] [Google Scholar]
- 7.Conroy T, Gavoille C, Samalin E, Ychou M, Ducreux M. The role of the FOLFIRINOX regimen for advanced pancreatic cancer. Curr Oncol Rep. 2013;15(2):182–189. doi: 10.1007/s11912-012-0290-4. [DOI] [PubMed] [Google Scholar]
- 8.Saif MW. Advancements in the management of pancreatic cancer: 2013. JOP. 2013;14(2):112–118. doi: 10.6092/1590-8577/1481. [DOI] [PubMed] [Google Scholar]
- 9.Vivaldi C, Fornaro L, Cappelli C, Pecora I, Catanese S, Salani F, Cacciato Insilla A, Kauffmann E, Donati F, Pasquini G, Massa V, Napoli N, Lencioni M, Boraschi P, Campani D, Boggi U, Caramella D, Falcone A, Vasile E. Early tumor shrinkage and depth of response evaluation in metastatic pancreatic cancer treated with first line chemotherapy: an observational retrospective cohort study. Cancers (Basel). 2019;11(7):939. doi: 10.3390/cancers11070939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Cremolini C, Loupakis F, Antoniotti C, Lupi C, Sensi E, Lonardi S, Mezi S, Tomasello G, Ronzoni M, Zaniboni A, Tonini G, Carlomagno C, Allegrini G, Chiara S, D'Amico M, Granetto C, Cazzaniga M, Boni L, Fontanini G, Falcone A. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015;16(13):1306–1315. doi: 10.1016/S1470-2045(15)00122-9. [DOI] [PubMed] [Google Scholar]
- 11.Heinemann V, von Weikersthal LF, Decker T, Kiani A, Vehling-Kaiser U, Al-Batran SE, Heintges T, Lerchenmüller C, Kahl C, Seipelt G, Kullmann F, Stauch M, Scheithauer W, Hielscher J, Scholz M, Müller S, Link H, Niederle N, Rost A, Höffkes HG, Moehler M, Lindig RU, Modest DP, Rossius L, Kirchner T, Jung A, Stintzing S. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(10):1065–1075. doi: 10.1016/S1470-2045(14)70330-4. [DOI] [PubMed] [Google Scholar]
- 12.Qin S, Li J, Wang L, Xu J, Cheng Y, Bai Y, Li W, Xu N, Lin LZ, Wu Q, Li Y, Yang J, Pan H, Ouyang X, Qiu W, Wu K, Xiong J, Dai G, Liang H, Hu C, Zhang J, Tao M, Yao Q, Wang J, Chen J, Eggleton SP, Liu T. Efficacy and tolerability of first-line cetuximab plus leucovorin, fluorouracil, and oxaliplatin (FOLFOX-4) versus FOLFOX-4 in patients with RAS wild-type metastatic colorectal cancer: the open-label, randomized, phase III TAILOR trial. J Clin Oncol. 2018;36(30):3031–3039. doi: 10.1200/JCO.2018.78.3183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bokemeyer C, Bondarenko I, Hartmann JT, de Braud F, Schuch G, Zubel A, Celik I, Schlichting M, Koralewski P. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: the OPUS study. Ann Oncol. 2011;22(7):1535–1546. doi: 10.1093/annonc/mdq632. [DOI] [PubMed] [Google Scholar]
- 14.Garufi C, Torsello A, Tumolo S, Ettorre GM, Zeuli M, Campanella C, Vennarecci G, Mottolese M, Sperduti I, Cognetti F. Cetuximab plus chronomodulated irinotecan, 5-fluorouracil, leucovorin and oxaliplatin as neoadjuvant chemotherapy in colorectal liver metastases: POCHER trial. Br J Cancer. 2010;103(10):1542–1547. doi: 10.1038/sj.bjc.6605940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Folprecht G, Martinelli E, Mazard T, Modest DP, Tsuji A, Esser R, Cremolini C, Falcone A. Triplet chemotherapy in combination with anti-EGFR agents for the treatment of metastatic colorectal cancer: current evidence, advances, and future perspectives. Cancer Treat Rev. 2022;102:102301. doi: 10.1016/j.ctrv.2021.102301. [DOI] [PubMed] [Google Scholar]
- 16.Sougklakos I, Vardakis NK, Kampouraki E, Kotortsi I, Androulakis NEM, Vamvakas L, et al. Phase II trial of 5-fluorouracil (5FU)/leucovorin (LV), irinotecan, and oxaliplatin (FOLFOXIRI) plus cetuximab in patients with metastatic colorectal cancer (mCRC). J Clin Oncol. 2011;29(15_suppl).
- 17.Assenat E, Desseigne F, Thezenas S, Viret F, Mineur L, Kramar A, Samalin E, Portales F, Bibeau F, Crapez-Lopez E, Bleuse JP, Ychou M. Cetuximab plus FOLFIRINOX (ERBIRINOX) as first-line treatment for unresectable metastatic colorectal cancer: a phase II trial. Oncologist. 2011;16(11):1557–1564. doi: 10.1634/theoncologist.2011-0141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Saridaki Z, Androulakis N, Vardakis N, Vamvakas L, Kabouraki E, Kalbakis K, Hatzidaki D, Voutsina A, Mavroudis D, Georgoulias V, Souglakos J. A triplet combination with irinotecan (CPT-11), oxaliplatin (LOHP), continuous infusion 5-fluorouracil and leucovorin (FOLFOXIRI) plus cetuximab as first-line treatment in KRAS wt, metastatic colorectal cancer: a pilot phase II trial. Br J Cancer. 2012;107(12):1932–1937. doi: 10.1038/bjc.2012.509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Folprecht, G., Mende, M., Liersch, T., Bechstein, W. O., Kohne, C. H., Stein, A., ... & Weitz, J. (2020). Cetuximab/irinotecan/5-FU+/-oxaliplatin or FOLFOXIRI+/-bevacizumab in patients with colorectal cancer and nonresectable liver metastases (AIO CELIM2-study).
- 20.Fornaro L, Lonardi S, Masi G, Loupakis F, Bergamo F, Salvatore L, Cremolini C, Schirripa M, Vivaldi C, Aprile G, Zaniboni A, Bracarda S, Fontanini G, Sensi E, Lupi C, Morvillo M, Zagonel V, Falcone A. FOLFOXIRI in combination with panitumumab as first-line treatment in quadruple wild-type (KRAS, NRAS, HRAS, BRAF) metastatic colorectal cancer patients: a phase II trial by the Gruppo Oncologico Nord Ovest (GONO) Ann Oncol. 2013;24(8):2062–2067. doi: 10.1093/annonc/mdt165. [DOI] [PubMed] [Google Scholar]
- 21.Bendell JC, Zakari A, Peyton JD, Boccia R, Moskowitz M, Gian V, Lipman A, Waterhouse D, LoCicero R, Earwood C, Lane CM, Meluch A. A phase II study of FOLFOXIRI plus panitumumab followed by evaluation for resection in patients with metastatic KRAS wild-type colorectal cancer with liver metastases only. Oncologist. 2016;21(3):279–280. doi: 10.1634/theoncologist.2015-0439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Pietrantonio F, Di Bartolomeo M, Cotsoglou C, Mennitto A, Berenato R, Morano F, Coppa J, Perrone F, Iacovelli R, Milione M, Alessi A, Vaiani M, Bossi I, Ricchini F, Scotti M, Caporale M, Bajetta E, de Braud F, Mazzaferro V. Perioperative triplet chemotherapy and cetuximab in patients with RAS wild type high recurrence risk or borderline resectable colorectal cancer liver metastases. Clin Colorectal Cancer. 2017;16(3):e191–e198. doi: 10.1016/j.clcc.2016.09.007. [DOI] [PubMed] [Google Scholar]
- 23.Cremolini C, Antoniotti C, Lonardi S, Aprile G, Bergamo F, Masi G, Grande R, Tonini G, Mescoli C, Cardellino GG, Coltelli L, Salvatore L, Corsi DC, Lupi C, Gemma D, Ronzoni M, Dell'Aquila E, Marmorino F, Di Fabio F, Mancini ML, Marcucci L, Fontanini G, Zagonel V, Boni L, Falcone A. Activity and safety of cetuximab plus modified FOLFOXIRI followed by maintenance with cetuximab or bevacizumab for RAS and BRAF wild-type metastatic colorectal cancer: a randomized phase 2 clinical trial. JAMA Oncol. 2018;4(4):529–536. doi: 10.1001/jamaoncol.2017.5314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Modest DP, Martens UM, Riera-Knorrenschild J, Greeve J, Florschütz A, Wessendorf S, Ettrich T, Kanzler S, Nörenberg D, Ricke J, Seidensticker M, Held S, Buechner-Steudel P, Atzpodien J, Heinemann V, Seufferlein T, Tannapfel A, Reinacher-Schick AC, Geissler M. FOLFOXIRI plus panitumumab as first-line treatment of RAS wild-type metastatic colorectal cancer: the randomized, open-label, phase II VOLFI study (AIO KRK0109) J Clin Oncol. 2019;37(35):3401–3411. doi: 10.1200/JCO.19.01340. [DOI] [PubMed] [Google Scholar]
- 25.Ogata T, Satake H, Ogata M, Hatachi Y, Maruoka H, Yamashita D, Hashida H, Hamada M, Yasui H. Safety and effectiveness of FOLFOXIRI plus molecular target drug therapy for metastatic colorectal cancer: a multicenter retrospective study. Oncotarget. 2019;10(10):1070–1084. doi: 10.18632/oncotarget.26626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Samalin E, Mazard T, Assenat E, Rouyer M, De la Fouchardiere C, Guimbaud R, Thézenas S. Triplet chemotherapy plus cetuximab as first-line treatment in RAS wild-type metastatic colorectal carcinoma patients. Ann Oncol. 2019;30:iv26–iv27. doi: 10.1093/annonc/mdz155.098. [DOI] [PubMed] [Google Scholar]
- 27.Hu H, Wang K, Huang M, Kang L, Wang W, Wang H, Qiu M, Lin R, Zhang H, Lan P, Wu X, Liu G, Wan Y, Liu M, Zhou Z, Huang Y, Li F, Zhang J, Cai Y, Ma T, Zhou J, Wang H, Ling J, Cai Y, Wu Z, Luo S, Ling L, Deng Y. Modified FOLFOXIRI with or without cetuximab as conversion therapy in patients with RAS/BRAF wild-type unresectable liver metastases colorectal cancer: the FOCULM multicenter phase II trial. Oncologist. 2021;26(1):e90–e98. doi: 10.1634/theoncologist.2020-0563. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tsuji, A., Ohori, H., Yamaguchi, T., Matsuura, M., Nishioka, A., Makiyama, A.& Fujii, M. (2021). The randomized phase II study of FOLFOXIRI plus cetuximab versus FOLFOXIRI plus bevacizumab as the first-line treatment in metastatic colorectal cancer with RAS wild-type tumors: The DEEPER trial (JACCRO CC-13). (2021): 3501-3501.
- 29.Cremolini C, Schirripa M, Antoniotti C, Moretto R, Salvatore L, Masi G, Falcone A, Loupakis F. First-line chemotherapy for mCRC -a review and evidence-based algorithm. Nat Rev Clin Oncol. 2015;12(10):607–619. doi: 10.1038/nrclinonc.2015.129. [DOI] [PubMed] [Google Scholar]
- 30.Motta R, Cabezas-Camarero S, Torres-Mattos C, Riquelme A, Calle A, Montenegro P, Sotelo MJ. Personalizing first-line treatment in advanced colorectal cancer: present status and future perspectives. J Clin Transl Res. 2021;7(6):771–785. [PMC free article] [PubMed] [Google Scholar]
- 31.Lam VW, Spiro C, Laurence JM, Johnston E, Hollands MJ, Pleass HC, Richardson AJ. A systematic review of clinical response and survival outcomes of downsizing systemic chemotherapy and rescue liver surgery in patients with initially unresectable colorectal liver metastases. Ann Surg Oncol. 2012;19(4):1292–1301. doi: 10.1245/s10434-011-2061-0. [DOI] [PubMed] [Google Scholar]
- 32.Cremolini C, Antoniotti C, Stein A, Bendell J, Gruenberger T, Rossini D, Masi G, Ongaro E, Hurwitz H, Falcone A, Schmoll HJ, Di Maio M. Individual patient data meta-analysis of FOLFOXIRI plus bevacizumab versus doublets plus bevacizumab as initial therapy of unresectable metastatic colorectal cancer. J Clin Oncol. 2020;20:JCO2001225. doi: 10.1200/JCO.20.01225. [DOI] [PubMed] [Google Scholar]
- 33.Bokemeyer C, Van Cutsem E, Rougier P, Ciardiello F, Heeger S, Schlichting M, Celik I, Köhne CH. Addition of cetuximab to chemotherapy as first-line treatment for KRAS wild-type metastatic colorectal cancer: pooled analysis of the CRYSTAL and OPUS randomised clinical trials. Eur J Cancer. 2012;48(10):1466–1475. doi: 10.1016/j.ejca.2012.02.057. [DOI] [PubMed] [Google Scholar]
- 34.Pietrantonio F, Fucà G, Rossini D, Schmoll HJ, Bendell JC, Morano F, Antoniotti C, Corallo S, Borelli B, Raimondi A, Marmorino F, Niger M, Boccaccino A, Masi G, Lonardi S, Boni L, de Braud F, Di Bartolomeo M, Falcone A, Cremolini C. FOLFOXIRI-Bevacizumab or FOLFOX-panitumumab in patients with left-sided RAS/BRAF wild-type metastatic colorectal cancer: a propensity score-based analysis. Oncologist. 2021;26(4):302–309. doi: 10.1002/onco.13642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Tomasello G, Petrelli F, Ghidini M, Russo A, Passalacqua R, Barni S. FOLFOXIRI plus bevacizumab as conversion therapy for patients with initially unresectable metastatic colorectal cancer: a systematic review and pooled analysis. JAMA Oncol. 2017;3(7):e170278. doi: 10.1001/jamaoncol.2017.0278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Afrăsânie VA, Marinca MV, Alexa-Stratulat T, Gafton B, Păduraru M, Adavidoaiei AM, Miron L, Rusu C. KRAS, NRAS, BRAF, HER2 and microsatellite instability in metastatic colorectal cancer - practical implications for the clinician. Radiol Oncol. 2019;53(3):265–274. doi: 10.2478/raon-2019-0033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Arnold D, Lueza B, Douillard JY, Peeters M, Lenz HJ, Venook A, Heinemann V, Van Cutsem E, Pignon JP, Tabernero J, Cervantes A, Ciardiello F. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann Oncol. 2017;28(8):1713–1729. doi: 10.1093/annonc/mdx175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Venook AP, Niedzwiecki D, Lenz HJ, Innocenti F, Mahoney MR, O'Neil BH, Cancer and Leukemia Group B (Alliance), SWOG, and ECOG CALGB/SWOG 80405: Phase III trial of irinotecan/5-FU/leucovorin (FOLFIRI) or oxaliplatin/5-FU/leucovorin (mFOLFOX6) with bevacizumab (BV) or cetuximab (CET) for patients (pts) with KRAS wild-type (wt) untreated metastatic adenocarcinoma of the colon or rectum (MCRC) Eur Soc Med Oncol. 2014;2014:26–30. [Google Scholar]
- 39.Lenz HJ, Ou FS, Venook AP, Hochster HS, Niedzwiecki D, Goldberg RM, Kabbarah O. Impact of consensus molecular subtype on survival in patients with metastatic colorectal cancer: results from CALGB/SWOG 80405 (Alliance) J Clin Oncol. 2019;37(22):1876. doi: 10.1200/JCO.18.02258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rivera F, Karthaus M, Hecht JR, Sevilla I, Forget F, Fasola G, Canon JL, Guan X, Demonty G, Schwartzberg LS. Final analysis of the randomised PEAK trial: overall survival and tumour responses during first-line treatment with mFOLFOX6 plus either panitumumab or bevacizumab in patients with metastatic colorectal carcinoma. Int J Colorectal Dis. 2017;32(8):1179–1190. doi: 10.1007/s00384-017-2800-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Benson AB, Venook AP, Al-Hawary MM, Arain MA, Chen YJ, Ciombor KK, Cohen S, Cooper HS, Deming D, Farkas L, Garrido-Laguna I, Grem JL, Gunn A, Hecht JR, Hoffe S, Hubbard J, Hunt S, Johung KL, Kirilcuk N, Krishnamurthi S, Messersmith WA, Meyerhardt J, Miller ED, Mulcahy MF, Nurkin S, Overman MJ, Parikh A, Patel H, Pedersen K, Saltz L, Schneider C, Shibata D, Skibber JM, Sofocleous CT, Stoffel EM, Stotsky-Himelfarb E, Willett CG, Gregory KM, Gurski LA. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2021;19(3):329–359. doi: 10.6004/jnccn.2021.0012. [DOI] [PubMed] [Google Scholar]
- 42.Folprecht G, Gruenberger T, Bechstein W, Raab HR, Weitz J, Lordick F, Hartmann JT, Stoehlmacher-Williams J, Lang H, Trarbach T, Liersch T, Ockert D, Jaeger D, Steger U, Suedhoff T, Rentsch A, Köhne CH. Survival of patients with initially unresectable colorectal liver metastases treated with FOLFOX/cetuximab or FOLFIRI/cetuximab in a multidisciplinary concept (CELIM study) Ann Oncol. 2014;25(5):1018–1025. doi: 10.1093/annonc/mdu088. [DOI] [PubMed] [Google Scholar]
- 43.Lee-Ying R, Bernard B, Gresham G, Chen L, Speers C, Kennecke HF, Lim HJ, Cheung WY, Renouf DJ. A comparison of survival by site of metastatic resection in metastatic colorectal cancer. Clin Colorectal Cancer. 2017;16(2):e23–e28. doi: 10.1016/j.clcc.2016.07.018. [DOI] [PubMed] [Google Scholar]
- 44.Sagawa T, Sato Y, Hirakawa M, Hamaguchi K, Fukuya A, Okamoto K, Miyamoto H, Muguruma N, Fujikawa K, Takahashi Y, Takayama T. Clinical impact of primary tumour location, early tumour shrinkage, and depth of response in the treatment of metastatic colorectal cancer with first-line chemotherapy plus cetuximab or bevacizumab. Sci Rep. 2020;10(1):19815. doi: 10.1038/s41598-020-76756-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Cremolini C, Loupakis F, Antoniotti C, Lonardi S, Masi G, Salvatore L, Cortesi E, Tomasello G, Spadi R, Zaniboni A, Tonini G, Barone C, Vitello S, Longarini R, Bonetti A, D'Amico M, Di Donato S, Granetto C, Boni L, Falcone A. Early tumor shrinkage and depth of response predict long-term outcome in metastatic colorectal cancer patients treated with first-line chemotherapy plus bevacizumab: results from phase III TRIBE trial by the Gruppo Oncologico del Nord Ovest. Ann Oncol. 2015;26(6):1188–1194. doi: 10.1093/annonc/mdv112. [DOI] [PubMed] [Google Scholar]
- 46.Chen D, Li L, Zhang X, Gao G, Shen L, Hu J, Yang M, Liu B, Qian X. FOLFOX plus anti-epidermal growth factor receptor (EGFR) monoclonal antibody (mAb) is an effective first-line treatment for patients with RAS-wild left-sided metastatic colorectal cancer: A meta-analysis. Medicine (Baltimore). 2018;97(10):e0097. doi: 10.1097/MD.000000000001. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.