
Fig. 1.
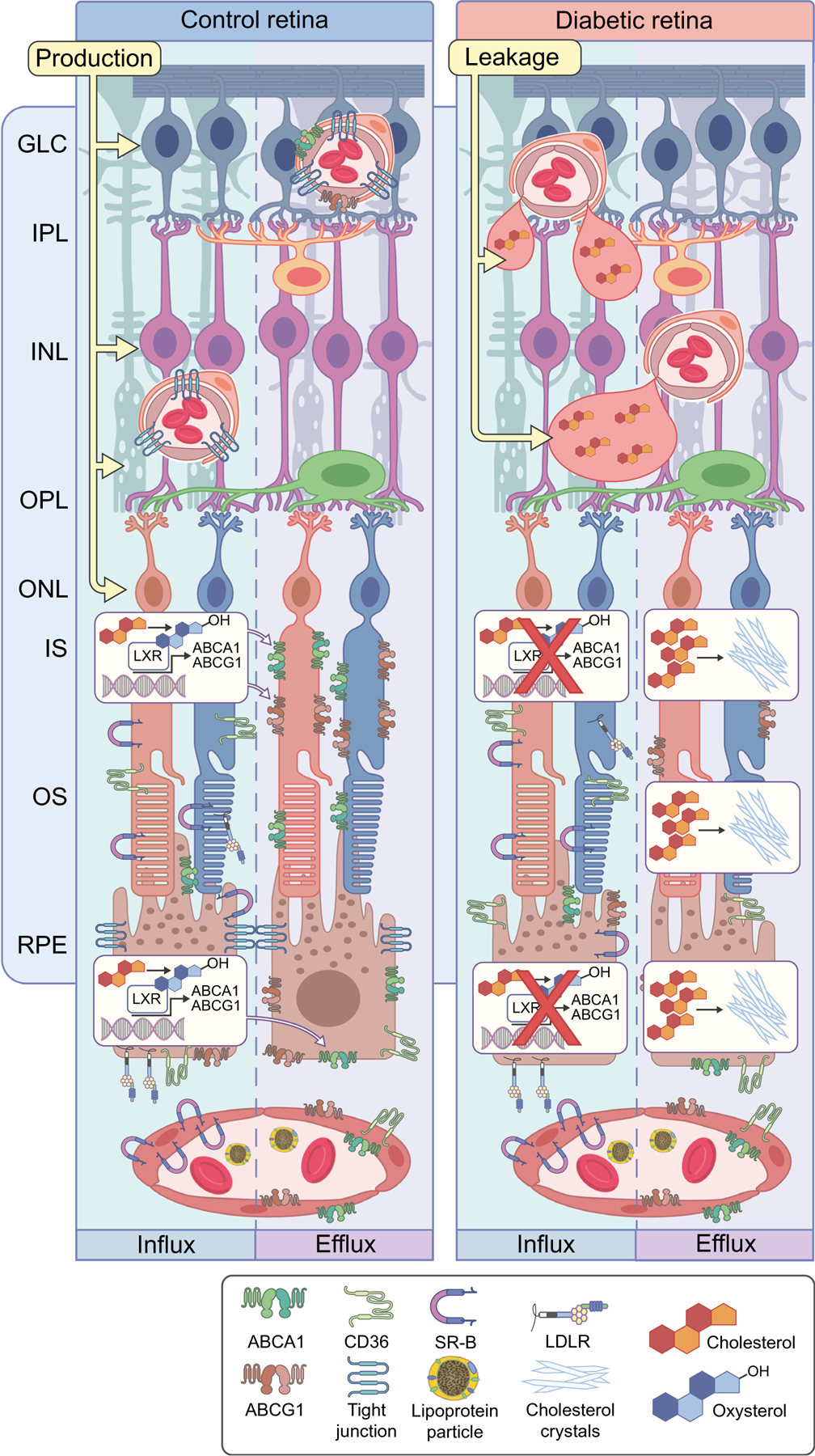
Dysregulation of cholesterol metabolism leading to cholesterol accumulation and formation of hyperreflective crystalline deposits (CCs) in diabetic retina. Cholesterol plays an important role in normal retinal function, and the balance of retinal cholesterol production, uptake by RPE cells and elimination is tightly controlled. At the outer BRB, cholesterol uptake from circulation by RPE cells through CD36, SR-B and LDLR is normally balanced by oxidation to oxysterols, LXR activation and production of ABCA1 and ABCG1, which control cholesterol efflux through RPE cells. Reduced production of oxysterols, decreased LXR expression and activity and thus decreased expression of ABC cassette cholesterol efflux transporters, collectively lead to cholesterol accumulation in the neuroretina. At high concentrations, cholesterol has the propensity to crystalise, forming proinflammatory and pro-atherogenic CCs. The endothelial cells of the inner BRB are not permeable to cholesterol uptake; however, endothelial cells express ABC cassette cholesterol efflux transporters. Inner BRB breakdown in diabetes leads to leaky blood vessels. Coupled with decreased expression of ABC transporters, this can lead to accumulation of cholesterol in the inner retina. GLC, ganglion cell layer; INL, inner nuclear layer; IPL, inner plexiform layer; IS, photoreceptor inner segment; ONL, outer nuclear layer; OPL, outer plexiform layer; OS, photoreceptor outer segment. This figure is available as part of a downloadable slideset