

Abstract
Purpose:
To compare skeletal and dentoalveolar measurements of subjects with unilateral impacted canine versus the non-impacted contralateral side using cone beam computed tomography (CBCT).
Materials and methods:
30 CBCTs with unilaterally impacted maxillary canines (Buccal=15, Palatal=15) were selected. Skeletal and dentoalveolar variables (alveolar ridge height of incisors, dentoalveolar height, angulations of incisors and canines, basal lateral width and premolar width) were compared between the impacted and the contralateral sides. Independent t-test was used to compare the variables.
Results:
There was a significant difference in the mean basal lateral width between the impacted (28.25±1.83 mm) and non-impacted (31.64±2.18 mm) sides. Premolar width was significantly lower on the impacted side (p<0.05). The canines exhibited significantly greater angulations on the impacted side compared to the nonimpacted side. The basal lateral width was significantly higher in the buccal subgroup (29.03±1.65mm) compared to palatal (27.48±1.70mm) on the impacted side. The intra-operator reliability was found to be high (0.99%).
Conclusion:
Significant differences were seen in canine angulation, premolar width and basal lateral width between impacted vs. non impacted sides. Basal lateral width was higher in buccal impacted cases compared to palatal.
Keywords: Impacted canine , CBCT , skeletal dimensions , diagnosis , orthodontic treatment
Introduction
An impacted tooth is one that is stopped from erupting into place due to malposition, lack of space, or other obstructions, according to Mead in early 1954. Later, Peterson defined impacted teeth as teeth that do not erupt into the dental arch in the expected period. Farman defined impacted teeth as teeth that are stopped from erupting due to a physical impediment in the eruption route (1, 2). Maxillary canines, after third molars, are the second most common teeth that are impacted, with prevalence varying from 1.80% to 3.29%, depending on the demographic studied (3). According to D’Oleo-Aracena et al. (4), incidence of impacted canine is more prevalent in females with a ratio of 2:1, and the frequency in the maxilla is more than double that of the mandible.
The maxillary canine has the longest eruption route of all the teeth, beginning right below the orbit’s floor. It then takes a circuitous route into the oral cavity, guided by lateral incisor`s root. The causative factors of impacted maxillary canines include maxillary lateral incisor`s aberrant morphology, disturbance in the dental lamina of developing canines, premature development of the canine, and microform of the cleft lip and palate (5).
Palatally impacted canines are two or three times more common than buccally impacted canines (6). Palatal impactions of canines are frequently associated with the presence of enough space in the dental arch, whereas most labial impactions of canines are associated with crowding. Dental arch space insufficiency was seen in 83% of arches with labial displacement of maxillary canines, according to Jacoby (7). Guidance hypothesis and genetic theory are the two main explanations for the development of an impacted palatal canine. From a regulatory point of view, local conditions such as the primary canine retention and / or absence, malformations, or abnormalities of the maxillary lateral incisor contribute to canine eruption (5). Genetic theory, on the other hand, states that the conflict is caused by genetic predisposition, and is supported by evidence showing a link between affected canines and other phenotypic dental variants of genetic origin, such as the small size of the lateral incisor crown, lateral incisor agenesis, aplasia of premolars and third molars, distal dislocation of mandibular second premolars (8).
The impaction might cause changes in the alveolar bone’s dimensions or disrupt the dental angulations of surrounding teeth. Subjects with maxillary canine impactions showed a transverse maxillary deficit in the anterior section of the dental arch, according to McConnell et al. (9).
The effect of canine impaction on alveolar maxillary dimensions has been evaluated in several studies (4,8,10). Compared with the unaffected side, Tadinada et al. (10) found that buccal-palatal width, height of floor of nasal cavity to alveolar ridge, and dental arch perimeter were significantly reduced towards the affected side. Lateral incisor roots near the affected palatal canines are more angulated than those of the lateral incisors near canines that erupt normally, according to Kanavakis et al. (8). On the affected side, D’Oleo-Aracena et al. (4) found reduced arch width in the area of the primary premolars and increased distal angulation of lateral incisors.
Cone beam computed tomography (CBCT) imaging is a precise and reliable method of detecting the exact position of an impacted tooth as well as measuring alveolar bone dimensions. In cases of palatally impacted canines of one side alone, previous investigations examined alveolar bone widths and heights on the impacted and non-impacted sides (4, 10). However, none of the investigations have taken into account canines that have been impacted buccally.
Therefore, this study aims to compare the skeletal and dento-alveolar dimensions in subjects with maxillary unilateral impacted canines, buccal or palatal versus the unaffected contralateral side using CBCT. The null hypothesis of the study was there is no difference in skeletal and dento-alveolar dimensions between impacted vs. nonimpacted side and buccal vs. palatal sides.
Materials and methods
Study design and sample size estimation
This cross-sectional and retrospective study with a split mouth design was a multi-centre study. The sample consisted of CBCT’s of subjects with unilateral maxillary impacted canines sourced from the archives of dental diagnostic centres specialising in CBCT imaging. Sample size calculation considered a mean difference of 2 mm in premolar width as clinically significant. A level of significance of 0.05 and 80% power required a sample of 28 sides with impacted and non-impacted canines each. Therefore, a sample of 30 CBCT’s with unilateral canine impaction was taken for the study.
Ethical statement
The institutional ethics committee granted the ethical clearance to this study (IIEC/RP/2019/002).
Study participants
The inclusion criteria for the CBCTs were patient`s age older than 15 years of both sexes, canines fully calcified, unilateral maxillary canine impaction, fully erupted contralateral canine and no history of any previous orthodontic treatment. Points for exclusion included poor image quality, tooth agenesis evident in CBCT scan, pathologies associated with the follicle like enlargement or cystic changes, CBCT scans demonstrating mesial migration of 1st premolar or distal migration of lateral incisor in impacted canine position, or any other pathology, dento-alveolar traumas, maxillary canine transpositions, craniofacial malformations, bilateral impacted maxillary canines, and patients with multiple impacted teeth.
30 CBCT scans that fulfilled the selection criteria were distributed into two separate groups: Group I (Non impacted) and Group II (Impacted) among which 15 had palatally impacted maxillary canine (subgroup A) and 15 had buccal impaction of maxillary canine (subgroup B). Evaluating the CBCT scans in axial section with lateral incisor and first premolar as reference teeth, position of impacted canine was determined, that is, buccal or palatal.
Image acquisiton and analysis
Imaging was performed with 6 mA and 90 Kv settings using a Newtom 3D scanner (Newtom Giano, Cefla s.c., Italy). The image volume of all patients’ CBCT scans was acquired using an 11 x 08 cm field of view with 0.15 mm isotropic voxel sizes and a 25-second exposure time. The DICOM pictures were analysed using NNT (New Net Technologies Ltd, Naples, Florida) software, which contained multiplanar reconstructions as well as 3D reconstructions in volume rendering mode and anteroposterior radiographs generated from CBCTs. All measurements were taken by a single calibrated radiologist and given in millimeters (mm) and degrees (°). An experienced Oral and Maxillofacial Radiology specialist performed the calibration. Anteroposterior radiographs produced from CBCTs in MIP coronal views were used to assess the skeletal and dentoalveolar variable heights, as well as the angulations of incisors and canines (Figure 1 A,B,C,D), and the widths of dentoalveolar variables (Figure 2 A,B,C) were measured in axial sections. The mid-sagittal plane was used as a reference plane for measuring alveolar ridge height, dentoalveolar height, incisor and canine angulations, and basal lateral width, whereas the middle palatine raphe was used as a reference plane for measuring premolar width. The impacted and contralateral sides, as well as buccal and palatal impacted canines, were compared in terms of the assessed characteristics. All of the measurements were redone by the same examiner after a week.
Variables measured on CBCT images and their definitions
1. Anterior alveolar ridge height (AARH-CI and AARH-LI)- distance from the bone ridge of upper central incisors (CI) and lateral incisors (LI) to the floor of the nostrils towards the side of impacted canine and on the side without impaction by drawing a straight line parallel to the mid-sagittal plane.
2. Anterior dentoalveolar height (ADH) is distance from the upper incisor edge to the floor of the nostrils on the side of the impacted canine and the side without impaction by drawing a straight line parallel to the midsagittal plane.
3. Nasal cavity width(NCW)- The distance between the anterior nasal spine and the lateral wall of the nasal base on the side of the impacted canine and the canine without impaction is measured in mm.
4. Basal lateral width (BLW)- The distance between the anterior nasal spine and the outermost dentoalveolar rim on the side of the impacted canine and the side of the canine without impaction is measured in millimetres.
5. Lateral angulation of the incisors’ long axis with respect to the nasal horizontal plane (ACI and ALI)- Value of the external angle of the central incisors’ (CI) and lateral incisors’ (LI) longitudinal axes with respect to the tangent of the nostril floor in both quadrants.
6. Lateral angulation of the long axis of canines with respect to the nasal horizontal plane (AC) - Value of the external angle of the impacted canine’s longitudinal axis with regard to the tangent of the nostril floor that has no impaction.
7. Premolar width (PW) - The distance in millimetres between the canine (deciduous or permanent) and first premolar on each side, measured in the axial cut at bone crest level, from the middle palatine raphe to the proximal alveolar bone crest.
Statistical analysis
SPSS version 16.0 (Chicago, IL, USA) was used for the statistical analysis. The study groups were subjected to descriptive statistics. To see if the data was regularly distributed, the Shapiro-Wilk test was used. An independent t-test was used to compare the results. For all tests, statistical significance was determined at a level of p<0.05.
Results
13 males (mean age 20.3± 3.0 years) and 17 females (mean age 19.4±3.6 years) were included in the present study. The method of acquiring measures was performed by the second examiner, and the measurements were compared to the first examiner’s measurements using the intraclass correlation coefficient for inter-examiner reproducibility (ICC). The ICC values were found to be statistically insignificant, indicating high reliability, with a mean of 0.91 (ICC 0.88-0.94). A strong correlation was found in intra-examiner reliability analysis (ICC 0.99). In terms of the acquired results, the post hoc Power (1-err prob) was 0.8878047, indicating that the sample size was appropriate.
Table 1 shows the comparison of measured variables between the impacted vs the non-impacted sides. The basal lateral width was significantly greater on the non-impacted side compared to the impacted side whereas the angulation of canine was significantly greater on the impacted sides,in both the buccal and palatal impaction cases. In the palatal impaction cases, a significant difference was also seen in the premolar width (p=0.03) whereas a significant difference was observed in the angulation of the central incisor (p=0.002) in the buccal impaction cases.
Table 1.
Descriptive statistics and comparison of impacted vs. non impacted sides. Independent t-test, Significant, p less than 0.05 SD standard deviation, AARH-CI and AARH-LI: Anterior alveolar ridge height of central incisor (CI) and lateral incisor(LI), ADH: Anterior dentoalveolar height, NCW: Nasal cavity width, BLW: Basal lateral width, ACI and ALI: Lateral angulation of long axis of incisors with respect to the nasal horizontal plane, AC: Lateral angulation of long axis of canines with respect to the nasal horizontal plane, PW: Premolar width
| Palatal impacted canine | Buccal impacted canine | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Groups | N | Mean ± SD | Mean Difference | p Value | Mean ± SD | Mean Difference | p Value |
| AARH-CI | Group I | 15 | 17.11±2.72 | 0.27 | 0.78 | 17.81 ± 2.58 | -0.19 | 0.85 |
| Group II | 15 | 16.84±2.45 | 17.99 ± 2.87 | |||||
| AARH-LI | Group I | 15 | 16.83±2.64 | 0.11 | 0.92 | 18.67 ± 3.67 | 0.64 | 0.62 |
| Group II | 15 | 16.72±3.16 | 18.03 ± 3.23 | |||||
| ADH-CI | Group I | 15 | 25.17±3.48 | 0.49 | 0.7 | 26.89 ± 2.59 | 0.57 | 0.53 |
| Group II | 15 | 24.68±3.41 | 26.32 ± 2.39 | |||||
| ADH-LI | Group I | 15 | 23.63±4.16 | -0.37 | 0.79 | 25.54 ± 3.07 | 0.47 | 0.68 |
| Group II | 15 | 23.99±3.21 | 25.07 ± 3.16 | |||||
| NCW | Group I | 15 | 12.28±1.007 | 0.34 | 0.44 | 11.81 ± 1.41 | -0.33 | 0.52 |
| Group II | 15 | 11.94±1.33 | 12.14 ± 1.34 | |||||
| BLW | Group I | 15 | 30.89±1.41 | 3.43 | 0.00* | 32.39 ± 2.57 | 3.37 | 0.00* |
| Group II | 15 | 27.47±1.7 | 29.03 ± 1.66 | |||||
| ACI | Group I | 15 | 87.25±2.74 | -0.09 | 0.96 | 89.71 ± 3.31 | 4.19 | 0.002* |
| Group II | 15 | 87.34±5.76 | 85.51 ± 3.59 | |||||
| ALI | Group I | 15 | 77.1±7.62 | -1.42 | 0.65 | 77.14 ± 6.42 | 0.95 | 0.78 |
| Group II | 15 | 78.52±9.22 | 76.19 ± 11.46 | |||||
| AC | Group I | 15 | 83.59±9.44 | -30.83 | 0.00* | 75.39 ± 13.09 | -25.18 | 0.00* |
| Group II | 15 | 114.42±20.86 | 100.57 ± 20.87 | |||||
| PW | Group I | 15 | 18.5±2.44 | 2.03 | 0.03* | 19.48 ± 3.08 | 1.6 | 0.14 |
| Group II | 15 | 16.47±2.43 | 17.88 ± 2.63 |
Table 2 shows the comparison of the buccal vs the palatal canine impaction subgroups. In the non-impacted side, the angulation of central incisors (p=0.03) was greater in the buccal compared to the palatal cases by 2.45 °. On the impacted side, the basal lateral width in the buccal impaction cases was significantly higher (29.03±1.65 mm) than in the palatal impaction cases (27.47±1.70 mm).
Table 2.
Descriptive statistics and comparison of buccal vs. palatal impacted canine groups. Independent t-test, Significant, p less than 0.05 SD standard deviation, AARH-CI and AARH-LI: Anterior alveolar ridge height of central incisor (CI) and lateral incisor(LI), ADH: Anterior dentoalveolar height, NCW: Nasal cavity width, BLW: Basal lateral width, ACI and ALI: Lateral angulation of long axis of incisors with respect to the nasal horizontal plane, AC: Lateral angulation of long axis of canines with respect to the nasal horizontal plane, PW: Premolar width)
| Non impacted side | Impacted side | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Groups | N | Mean ± SD | Mean Difference | p Value | Mean ± SD | Mean Difference | p Value |
| AARH-CI | Group A | 15 | 17.11±2.72 | -0.7 | 0.48 | 16.84±2.44 | -1.15 | 0.25 |
| Group B | 15 | 17.81±2.58 | 17.99±2.86 | |||||
| AARH-LI | Group A | 15 | 16.83±2.64 | -1.84 | 0.13 | 16.72±3.16 | -1.31 | 0.27 |
| Group B | 15 | 18.67±3.67 | 18.03±3.23 | |||||
| ADH-CI | Group A | 15 | 25.17±3.48 | -1.72 | 0.13 | 24.68±3.40 | -1.64 | 0.14 |
| Group B | 15 | 26.89±2.59 | 26.32±2.39 | |||||
| ADH-LI | Group A | 15 | 23.63±4.16 | -1.91 | 0.16 | 23.99±3.20 | -1.07 | 0.36 |
| Group B | 15 | 25.54±3.07 | 25.07±3.16 | |||||
| NCW | Group A | 15 | 12.28±1.007 | 0.46 | 0.3 | 11.94±1.32 | -0.2 | 0.68 |
| Group B | 15 | 11.81±1.41 | 12.14±1.34 | |||||
| BLW | Group A | 15 | 30.89±1.41 | -1.5 | 0.06 | 27.47±1.70 | -1.56 | 0.01* |
| Group B | 15 | 32.39±2.57 | 29.03±1.65 | |||||
| ACI | Group A | 15 | 87.25±2.74 | -2.45 | 0.03* | 87.34±5.76 | 1.82 | 0.31 |
| Group B | 15 | 89.71±3.31 | 85.51±3.58 | |||||
| ALI | Group A | 15 | 77.1±7.62 | -0.04 | 0.99 | 78.52±9.22 | 2.32 | 0.54 |
| Group B | 15 | 77.14±6.42 | 76.19±11.45 | |||||
| AC | Group A | 15 | 83.59±9.44 | 8.20 | 0.06 | 114.42±20.86 | 13.85 | 0.08 |
| Group B | 15 | 75.39±13.09 | 100.57±20.87 | |||||
| PW | Group A | 15 | 18.5±2.44 | -0.98 | 0.34 | 16.47±2.42 | -1.40 | 0.14 |
| Group B | 15 | 19.48±3.08 | 17.88±2.62 |
Figure 1.
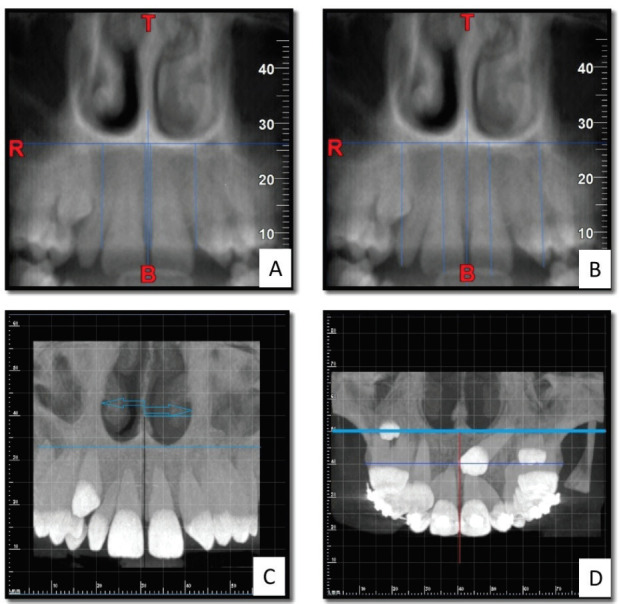
Figure 1. A- Anterior alveolar ridge height, B- Anterior dentoalveolar height, C- Nasal cavity width and D- Basal lateral width.
Figure 2.
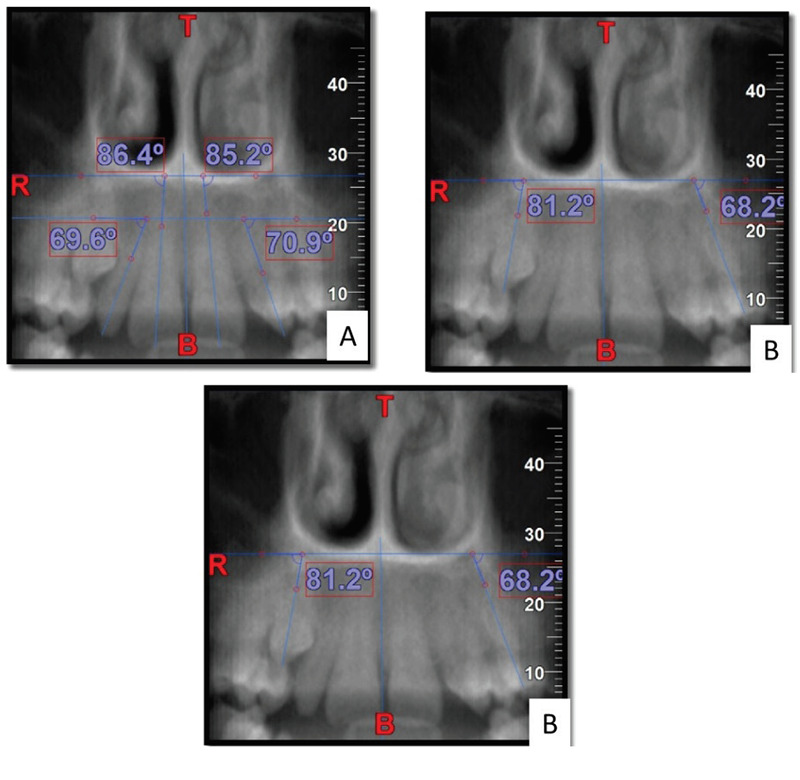
A- Lateral angulation of long axis of the incisors with respect to the nasal horizontal plane, B- Lateral angulation of long axis of canines with respect to the nasal horizontal plane, C- Premolar width.
Discussion
CBCT was used to assess skeletal and dentoalveolar variables in the maxillary arch in instances with unilaterally (buccal or palatal) impacted canines to the contra-lateral unaffected site. The accuracy of CBCT in measuring alveolar dimensions has previously been documented (4,8,10). The number of females (n=17) in the sample was higher than the number of males (n=13). This is consistent with prior research that found a higher prevalence of impacted canines in females (4,11, 12).
The study found that the side with impacted tooth and the normal sides had substantial differences in basal lateral width, premolar width, and canine angulation. However, there was no significant difference between the impacted and non-impacted groups in anterior alveolar ridge height, anterior dento- alveolar height of incisors, nasal cavity width, or incisor angulation. Because the alveolar process develops in response to tooth eruption, it’s plausible to assume that the canine tooth’s non-eruption/impaction resulted in changed alveolar dimensions on the impacted side (13, 14). In cases of unilateral palatal canine impactions, certain earlier investigations have found a variation in maxillary alveolar dimensions and tooth angulations (4,10,15, 16). When compared to the non-impacted side, Tadinada et al. (10) found that the impacted side had considerably smaller bucco-palatal width (BP), nasal floor to alveolar crest length, and arch perimeter. The bucco-palatal breadth was reduced at a level of 2mm above the alveolar crest in their study, but not at 6 or 10mm apically. The presence of impacted canine higher in the alveolar crest was the main reason for this. They claimed that bone loss was greater in the horizontal than in the vertical dimension. This is supported by our findings, which show that there were substantial changes in width measurements (basal lateral width and premolar width), but not in dento-alveolar heights. The measurement from the mid-palatal raphe to the first premolar on the afflicted side was substantially lower than the side that was normal, according to D’ Oleo-Aracena et al. (4). They also suggested that canine impaction would have little effect on alveolar heights in the incisor region since the incisors erupt before the canines. Impaction of the maxillary canine has been linked to a lack of transverse growth in the front section of the dental arch in studies by McConnell et al.(9) and Schindel and Duffy (17). The findings of these investigations suggest that when a transverse maxillary deficit is noted clinically, the possibility of maxillary canine impaction should be considered. At this point, expanding the arch could be termed an interceptive technique. The clinical importance of our findings in terms of treatment suggests that more attention should be paid to correcting asymmetries in transverse dimension, particularly at the level of the first premolar on the side with an impacted canine. Only dental alignment should be used to correct the severity of this asymmetry (about 2 mm between both sides); however, in cases of more severe asymmetry, such as unilateral cross bite, asymmetric expansion could be considered.
The angulations of the impacted canine were substantially bigger than those of the non-impacted canine, and the impacted canine displayed mesial tilting. Hanke et al. (3) and D’Oleo-Aracena et al. (4) observed similar findings in their previous studies. The average difference in canine angulation between the impacted and non-impacted sides ranged from 25 to 30 degrees. The angulation of the canine is very important in deciding its prognosis. The incisor angulations on the affected and non-impacted sides, however, were not significantly different. D’Oleo-Aracena et al. (4) showed a substantial difference in incisor angulation between the affected and non-impacted sides, with greater distal crown angulation on the impacted sides, whereas Kanavakis et al.(8) found a 2.5 degree mesial angulation of lateral incisors close to impacted canines.
However, according to D’Oleo-Aracena et al. (4), orthodontic treatment in unilateral impacted canines necessitates prior traction; aligning the incisors without distancing the impacted canine could expose the incisor roots to the impacted canine due to their distal angulation with respect to the opposite side without impaction. In addition, orthodontists should place a greater emphasis on rectifying transverse asymmetries, particularly at the level of the breadth between the median raphe and the first premolar on the affected side with an impacted canine.
We discovered no significant variations in the other characteristics between the buccal and palatal impacted canines, except for the basal lateral width, which was substantially greater in the buccal subgroup (29.03±1.65mm) compared to the palatal subgroup (27.48±1.70mm) on the impacted side. The distance between the mid palatine raphe and the proximal alveolar bone crest between the canine and first premolar on the impacted side was significantly shorter than the non-impacted side (p<0.05) in palatal impacted canine cases. On the other hand, there was no significant change in premolar width on the impacted side of buccally impacted canines.
The drawbacks of study include a small sample size. Moreover the study did not differentiate the impacted canines according to the severity of impaction. The extent of displacement of the canines from their normal positions in the arch may have affected the variables studied. The study excluded cases of canine impaction with presence of other dental anomalies such as peg-shaped or diminutive lateral incisors, agenesis of teeth and other anomalies to minimize confounding factors but in actuality, the impaction of canines, especially palatal ones has shown to be associated with such anomalies. Another drawback of this study is the small number of observers.
Conclusion
Within limitations, the following conclusions may be drawn from the study: Significant differences were observed in the canine angulation, premolar width and basal lateral width between the impacted vs. contra-lateral sides. Basal lateral width and premolar width were more on the non- impacted sides than impacted sides. Canine angulation on the side with impaction was substantially higher than on the contra-lateral side. On the buccal impacted sides, the basal lateral width was much bigger than on the palatal impacted sides.
Footnotes
Ethics committee approval: Ethical clearance was obtained from the institutional ethics committee (IIEC/RP/2019/002).
Informed consent:Participants provided informed constent.
Peer review:Externally peer-reviewed.
Author contributions:SKS, MS, PS participated in designing the study. SKS, MS, AS, PS, MR participated in generating the data for the study. SKS, MS, AS participated in gathering the data for the study. SKS, MS, AS participated in the analysis of the data. SKS wrote the majority of the original draft of the paper. SKS, MS, AS, PS, MR participated in writing the paper. SKS, MS, AS, PS, MR have had access to all of the raw data of the study. SKS, MS, PS have reviewed the pertinent raw data on which the results and conclusions of this study are based. SKS, MS, AS, PS, MR have approved the final version of this paper. MR guarantees that all individuals who meet the Journal’s authorship criteria are included as authors of this paper.
Conflict of interest:The authors declared no conflict of interest.
Financial disclosure:The authors declared that they did not receive any financial support.
References
- 1.Juodzbalys G, Daugela P. Mandibular third molar impaction: review of literature and a proposal of a classification. J Oral Maxillofac Res. 2013. Jul;4(2):e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Abdel-Salam E, El-Badrawy A, Tawfik AM. Multi-detector dental CT in evaluation of impacted maxillary canine. Egypt J Radiol Nucl Med. 2012;43(4):527–34. 10.1016/j.ejrnm.2012.07.002 [DOI] [Google Scholar]
- 3.Hanke S, Hirschfelder U, Keller T, Hofmann E. 3D CT based rating of unilateral impacted canines. J Craniomaxillofac Surg. 2012. Dec;40(8):e268–76. 10.1016/j.jcms.2011.12.005 [DOI] [PubMed] [Google Scholar]
- 4.D Oleo-Aracena MF . Arriola-Guillén LE, Rodríguez-Cárdenas YA, Ruíz-Mora GA. Skeletal and dentoalveolar bilateral dimensions in unilateral palatally impacted canine using cone beam computed tomography. Prog Orthod. 2017;18:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jena AK, Duggal R. The pattern of maxillary canine impaction in relation to anomalous lateral incisors. J Clin Pediatr Dent. 2010;35(1):37–40. 10.17796/jcpd.35.1.uh4vm67264vv4762 [DOI] [PubMed] [Google Scholar]
- 6.Walker L, Enciso R, Mah J. Three-dimensional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2005. Oct;128(4):418–23. 10.1016/j.ajodo.2004.04.033 [DOI] [PubMed] [Google Scholar]
- 7.Jacoby H. The etiology of maxillary canine impactions. Am J Orthod. 1983. Aug;84(2):125–32. 10.1016/0002-9416(83)90176-8 [DOI] [PubMed] [Google Scholar]
- 8.Kanavakis G, Curran KM, Wiseman KC, Barone NP, Finkelman MD, Srinivasan S, et al. Evaluation of crown-root angulation of lateral incisors adjacent to palatally impacted canines. Prog Orthod. 2015. Feb;16(1):4. 10.1186/s40510-015-0074-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.McConnell TL, Hoffman DL, Forbes DP, Janzen EK, Weintraub NH. Maxillary canine impaction in patients with transverse maxillary deficiency. ASDC J Dent Child. 1996. May-Jun;63(3):190–5. [PubMed] [Google Scholar]
- 10.Tadinada A, Mahdian M, Vishwanath M, Allareddy V, Upadhyay M, Yadav S. Evaluation of alveolar bone dimensions in unilateral palatally impacted canine: a cone-beam computed tomographic analyses. Eur J Orthod. 2015. Dec;37(6):596–602. 10.1093/ejo/cju098 [DOI] [PubMed] [Google Scholar]
- 11.Bishara SE, Ortho D. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992. Feb;101(2):159–71. 10.1016/0889-5406(92)70008-X [DOI] [PubMed] [Google Scholar]
- 12.Sajnani AK, King NM. Prevalence and characteristics of impacted maxillary canines in Southern Chinese children and adolescents. J Investig Clin Dent. 2014. Feb;5(1):38–44. 10.1111/jicd.12027 [DOI] [PubMed] [Google Scholar]
- 13.Kjær I. Mechanism of human tooth eruption: review article including a new theory for future studies on the eruption process. Scientifica (Cairo). 2014;2014:341905. 10.1155/2014/341905 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wise GE. Cellular and molecular basis of tooth eruption. Orthod Craniofac Res. 2009. May;12(2):67–73. 10.1111/j.1601-6343.2009.01439.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Anic-Milosevic S, Varga S, Mestrovic S, Lapter-Varga M, Slaj M. Dental and occlusal features in patients with palatally displaced maxillary canines. Eur J Orthod. 2009. Aug;31(4):367–73. 10.1093/ejo/cjp014 [DOI] [PubMed] [Google Scholar]
- 16.Dağsuyu IM, Kahraman F, Okşayan R. Three-dimensional evaluation of angular, linear, and resorption features of maxillary impacted canines on cone-beam computed tomography. Oral Radiol. 2018. Jan;34(1):66–72. 10.1007/s11282-017-0289-5 [DOI] [PubMed] [Google Scholar]
- 17.Schindel RH, Duffy SL. Maxillary transverse discrepancies and potentially impacted maxillary canines in mixed-dentition patients. Angle Orthod. 2007. May;77(3):430–5. 10.2319/0003-3219(2007)077[0430:MTDAPI]2.0.CO;2 [DOI] [PubMed] [Google Scholar]