

Abstract
Background
Inflammatory bowel disease (IBD) has a major impact on different aspects of life of patients with IBD, but functioning in the home environment is under-reported in literature. The aim of this study was to assess the impact of IBD on household and/or family life.
Method
Adult patients with IBD from the outpatient clinic of the Erasmus MC (Rotterdam, the Netherlands) were invited to participate in this cross-sectional study between September and December 2020. A questionnaire was composed to measure the impact of IBD on functioning in the household and family life. In addition, the IBD Disability Index and Work Productivity and Activity Impairment Questionnaire were used. Data were analysed using descriptive statistics and multiple logistic regression modelling.
Results
Of 308 invited patients, 229 patients were included (response rate 74%). Sixty-eight per cent of patients were diagnosed with Crohn’s disease, 69% were female and median age was 38.0 years. Many patients reported difficulties with domestic activities (55.0%), leisure (53.9%), parenting (50.6%), sexual activities (48.4%) and interpersonal relationships (39.1%). Fatigue was associated with the experience of more severe difficulties in domestic activities (OR 16.160, 95% CI 6.053 to 43.141). Furthermore, 32.7% of patients felt that IBD influenced their desire to have children.
Conclusion
IBD has a markedly negative impact on household and/or family life in many patients. To optimise patient care, household and family related difficulties need to be considered in a holistic treatment approach.
Keywords: inflammatory bowel disease
Significance of this study.
What is already known about this subject?
Inflammatory bowel disease (IBD) can result in chronic limitations that interfere with the ability to engage in daily activities, but functioning in the home environment remains under-reported.
What are the new findings?
IBD has a large impact on household and family life, especially in the performance of household chores, participation in leisure activities, parenting and sexual activities.
How might it impact on clinical practice in the foreseeable future?
Recently, with support of the European Crohn’s and Colitis Organisation, a list with criteria was constructed to shape quality of care standards for IBD. Our research shows that functioning in the home environment, which is an essential part of the ability to engage in daily activities, can be affected by IBD and should not be overlooked in this assessment.
Introduction
Inflammatory bowel disease (IBD) is a chronic gastrointestinal condition, including both Crohn’s disease (CD) and ulcerative colitis (UC).1 2 The unpredictable, relapsing and remitting nature of the disease and troubling symptoms affect physical and mental well-being.3 IBD frequently makes its debut during adolescence or early adulthood: a stage of life when individuals are starting a professional career, forming a family and gaining other life achievements. Therefore, IBD can result in chronic limitations that interfere with the ability to engage in daily activities, referred to as disability.
To gain more insight into disability, WHO developed a conceptual framework. The International Classification of Functioning, Disability and Health (ICF) describes the impact of a disease on a patient as an ever-changing interaction between illness, environmental and personal factors. Hence, disability covers all encountered difficulties in the domains of body functions and/or structures, activity and participation.4
To fully understand the burden of IBD on a patient’s life, all the different domains of disability need to be evaluated. However, in current IBD literature, the main focus of research is on physical health and engagement with society via the ability to work.5–7 Unfortunately, functioning in the home environment, which is an essential part of everyday life, remains under-reported. Only a few studies reported on difficulties in the home management8 9 or limitations in carrying out family activities or parental duties because of IBD-related symptoms.10 11 Thereby, the presence of IBD in the home can lead to changes in the lives of family members and their habits. Another aspect that can be affected by IBD is the wish to start a family or taking care of children. Feeling unable to cope with the added responsibility of looking after a child or concerns about pregnancy, such as the risks of medication with respect to pregnancy or potential heredity of IBD, are frequently reported.12–14 These facets impose a significant extra burden on patients, while remaining challenging to quantify.
Since studies covering all the aspects of functioning in the home environment and family matters are scarce, we aimed to assess the impact of IBD on household and/or family life in adult patients with IBD.
Methods
Study design
Adult patients with IBD from the outpatient clinic of the Erasmus MC (Rotterdam, the Netherlands) that had a follow-up visit at the outpatient clinic or by phone between September and December 2020 were invited to participate in this cross-sectional study. Patients were able to fill out the pen and paper questionnaire at the clinic or at home. Patients were eligible if they were 18 years or older, had a confirmed IBD diagnosis and were capable of understanding, reading and writing the Dutch language. The survey consisted of different sections, asking questions about sociodemographic characteristics, household and family life, disability and work. To evaluate clinical disease activity, the gastroenterologist made an assessment during the visit based on clinical symptoms.
Instruments
A household and family life questionnaire was composed of items of the ICF, translated in Dutch by the WHO.15 The questionnaire consists of sections on domestic activities, caregiving and parenting, household-related leisure and interpersonal relationships. Answers were given using a five-point Likert scale. The section on family planning was based on the published questionnaire by Marri et al.16 Female participants were classified as voluntary childless (VC) if they were aged between 18 and 45 years, had no desire to have children, had no children and if they reported no fertility problems or other signs of involuntary childlessness. Beside multiple choice questions, open-ended questions were used as well.
The IBD Disability Index (IBD-DI) V.2 is a validated IBD-specific instrument that measures disability in the last 7 days. It is developed according to the framework of the ICF and scores can be categorised as follows: 0–20 (no disability), 21–35 (mild disability), 36–50 (moderate disability) and 51–100 (severe disability). Question 2 of the IBD-DI was used to measure fatigue, and patients were categorised into none and mild difficulty with fatigue and moderate to extreme difficulty with fatigue.17–19
The Work Productivity and Activity Impairment Questionnaire IBD (WPAI-IBD) is a validated IBD specific measure that consists of six questions categorised into four domains: absenteeism, presenteeism, overall work impairment and activity impairment. Total scores are displayed using percentages.20
Statistics
We aimed to include at least 200 participants to ensure proper analysis in all subgroups. Data are presented as count and percentage for categorical variables, mean and SD for continuous, approximately normally distributed variables and median and IQR for non-normal continuous data. A multiple logistic regression analysis was conducted to assess the relationships between demographic and patient reported outcome variables and the outcome of having experienced at least one of three moderate to extreme difficulties in the performance of domestic activities in the past week, due to IBD. OR’s and 95% CIs are used to describe the association between these variables. Values of p<0.05 were considered to be statistical significant. All statistical analyses were performed with IBM Statistical Packages for Social Sciences (SPSS V.25.0).
Results
Patient characteristics
Of the 308 subjects that were invited to participate in the study, 289 patients provided informed consent of whom 229 patients returned the questionnaire (response rate 74%), see online supplemental figure 1. Of the participants, 67.7% had CD, 28.8% had UC and 3.5% had IBD-unclassified type. The median age of the patients was 38.0 years, with 69,0% being female. Patient characteristics are summarised in table 1.
Table 1.
Baseline characteristics of the 229 participants
| Characteristics | n (%) |
| Female sex | 158 (69.0) |
| Age, median ±IQR (years) | 38.0±17 |
| Ethnicity (n=226) | |
| Caucasian | 200 (88.5) |
| Non-Caucasian | 26 (11.5) |
| Current smoker | 29 (12.7) |
| Education* (n=226) | |
| Low | 41 (18.1) |
| Moderate | 83 (36.7) |
| High | 102 (45.1) |
| Employment status† | |
| Employed | 153 (66.8) |
| Unemployed | 8 (3.5) |
| Occupational disability | 39 (17.3) |
| Pensioner | 17 (7.4) |
| Student | 14 (6.1) |
| Crohn’s disease | 155 (67.7) |
| Age at diagnosis | |
| <16 years | 38 (24.5) |
| 17–40 years | 107 (69.0) |
| >40 years | 10 (6.5) |
| Disease location | |
| Ileitis | 29 (18.7) |
| Colitis | 22 (14.2) |
| Ileocolitis | 104 (67.1) |
| Upper gastrointestinal disease | 17 (11.0) |
| Disease behaviour | |
| Luminal disease | 66 (42.6) |
| Stricturing disease | 56 (36.1) |
| Penetrating disease | 48 (31.0) |
| Perianal involvement | 39 (25.2) |
| Ulcerative colitis | 66 (28.8) |
| IBD-U | 8 (3.5) |
| Disease extent‡ | |
| Proctitis | 6 (8.1) |
| Left sided colitis | 19 (25.7) |
| Pancolitis | 49 (66.2) |
| Previous IBD-related surgery | 104 (45.4) |
| Stoma | 24 (10.5) |
| Pouch | 13 (5.7) |
| IBD Medication | |
| None | 35 (15.3) |
| Aminosalicylates | 54 (23.6) |
| Corticosteroid | 46 (20.1) |
| Immunomodulator§ | 40 (17.5) |
| Tofacitinib | 4 (1.7) |
| Biological | 119 (52.0) |
| Anti-TNF | 76 (33.2) |
| Vedolizumab | 17 (7.4) |
| Ustekinumab | 22 (9.6) |
*Education status based on the Dutch Central Bureau of Statistics (low=high school and primary school education, moderate=middle-level applied education, high=higher professional education, scientific education (and/or doctorate).
†Multiple answers were available.
‡IBD-U included.
§Immunomodulator use included thiopurines and methotrexate.
IBD-U, inflammatory bowel disease unclassified; TNF, tumour necrosis factor.
flgastro-2021-102027supp002.pdf (21.5KB, pdf)
Most participants were legally married or in a relationship (164; 71.9%), and almost half had biological children or took care of children (105; 45.9%). The vast majority of patients lived with one or more household members (85.6%). For more detailed information about the household and family characteristics (see table 2).
Table 2.
Household and family characteristics of the 229 participants
| Household and family characteristics | n (%) |
| Marital status, (n=228) | |
| Married/partner | 164 (71.9) |
| Single | 48 (21.1) |
| Divorced | 10 (4.4) |
| Widow | 2 (0.9) |
| Other | 4 (1.8) |
| Family status | |
| (Biological) children or taking care of children | 105 (45.9) |
| No (biological) children or not taking care of children | 124 (54.1) |
| Household composition | |
| Living alone | 33 (14.4) |
| One or more household member | 196 (85.6) |
| (Married) partner | 161 (82.1) |
| Children | 95 (48.5) |
| Parents | 22 (11.2) |
| Siblings/other family | 14 (7.2) |
| Other | 4 (2.0) |
Outcomes
Domestic activities
Overall, 126 patients (55.0%) encountered mild to extreme difficulties in at least one of three domestic activities (eg, performance of household tasks, grocery shopping and cooking) in the past week because of IBD. The performance of household tasks was most impacted (109/224; 48.7%), see figure 1. The most common limitation per domestic activity was worries about finding a sanitary facility during grocery shopping (33/93; 35.5%), preparing simpler meals than someone would like to (40/70; 57.1%) and doing housework less often than preferred (68/109; 62.4%). Forty-three respondents had support with their household tasks because of IBD (43/218; 19.7%), of whom 51.2% received help from a domestic worker and 44.2% had support from their social network. Thirty patients had the desire to receive support (13.8%), of which all preferred help from a cleaner.
Figure 1.
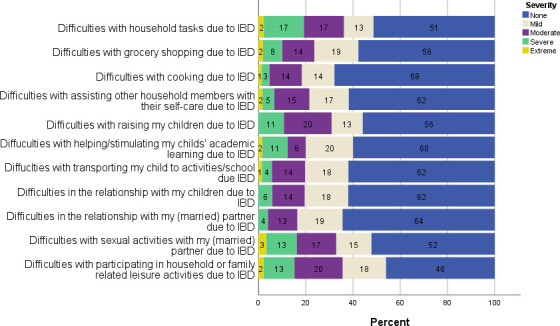
The amount of patients (%) that experienced difficulties because of IBD in the last week, and severity of these difficulties. IBD, inflammatory bowel disease.
Table 3 shows the multivariable logistic regression analysis that investigates the relationship between variables and the outcome of having experienced at least one of three moderate to extreme difficulties in domestic activities in the past week, due to IBD. Fatigue was associated with struggling with these domestic activities with an OR of 16.160 (95% CI 6.053 to 43.141 and clinical disease activity with an OR of 2.016 (95% CI 0.981 to 4.140)), although its p value was non-significant.
Table 3.
Multiple logistic regression with the outcome of having experienced at least one of three moderate to extreme difficulties in domestic activities (grocery shopping, cooking, household task) in the past week, due to IBD
| Variable | Difficulty with domestic activities* | ||
| (n/total) % experienced | OR (95% CI) | P value | |
| Sex | |||
| Male | (20/71) 28.2 | 1.772 (0.854 to 3.675) | 0.124 |
| Female | (74/158) 46.8 | 0.991 (0.965 to 1.018) | 0.494 |
| Age† | |||
| Disease type CD | (64/155) 41.3 | 1.051 (0.510 to 2.169) | 0.892 |
| UC+IBD U | (30/74) 40.5 | ||
| Clinical disease activity | |||
| Quiescent | (60/170) 35.3 | 2.016 (0.981 to 4.140) | 0.056 |
| Active | (34/59) 57.6 | ||
| Stoma | |||
| No | (82/205) 40.0 | 1.545 (0.519 to 4.596) | 0.434 |
| Yes | (12/24) 50.0 | ||
| Employment | |||
| Not paid | (38/76) 50.0 | 0.589 (0.291 to 1.191) | 0.589 |
| Paid | (56/153) 36.6 | ||
| Household composition | |||
| No children | (48/134) 35.8 | 1.397 (0.716 to 2.726) | 0.327 |
| Children | (46/95) 48.4 | ||
| Fatigue‡ | |||
| None/mild | (5/75) 6.7 | 16.160 (6.053 to 43.141) | 0 |
| Moderate to extreme | (89/153) 58.2 | ||
Values of p<0.05 are shown in bold. Moderate to extreme difficulties experienced by 94 of 229 patients.
*Outcome of experiencing one or more moderate to extreme difficulties in domestic activities in the past week, due to IBD.
†Age displayed as a continuous variable.
‡Fatigue measured with the IBD-DI, categorised into none and mild difficulty with fatigue and moderate to extreme difficulty with fatigue.
CD, Crohn’s disease; IBD, inflammatory bowel disease; IBD-DI, Inflammatory Bowel Disease Disability Index; IBD-U, inflammatory bowel disease unclassified; UC, ulcerative colitis.
Caregiving and parenting
Over one-third of the participants who lived with household members encountered difficulties in assisting others with self-care (69/196; 38.1%), and more than half of the parents who lived with their child encountered limitations in carrying out at least one of three parental duties (43/85; 50.6%) in the past week due to IBD (see figure 1).
Interpersonal relationships
More than one-third of the patients stated that they encountered restrictions in maintaining a stable relationship with one or more household members due to IBD (72/184; 39.1%). When evaluating specific interpersonal relationships, parent-child (33/87; 37.9%) and spousal relationships (54/152; 35.5%) were impacted most (see figure 1.) Additionally, almost half of the participants who lived with their partner encountered difficulties with sexual activities in the past week as result of IBD (74/155; 47.8%).
Household-related leisure
More than half of the patients that lived together with a household member stated that they have encountered obstacles in participating in leisure activities together with their household in the past week due to IBD (103/191; 53.9%) (see figure 1).
Family planning
Approximately one-third of our population felt that IBD interfered with their desire to have or care for children (74/226; 32.7%). Of those, more than 50% already had children (38/74; 51.4%). The majority of the 36 childless participants were planning to have children, despite the influence of IBD (n=19, 52.8%). In a free-text option, subjects were able to specify in which way IBD influenced their plans to have children. The most common answers given by patients who already had children or considered to have children were categorised into themes (online supplemental table 1). Noteworthy, almost a quarter of the parent population had less children than initially desired as result of IBD (25/105; 23.8%).
flgastro-2021-102027supp001.pdf (76.5KB, pdf)
Of the 50 patients who were childless and had no desire to have children, almost one-third stated that this resulted from having IBD (15/50; 30.0%). In the 18–45 age range, nineteen participants were considered to be VC, resulting in a total VC rate of 12.1% (19/157). Nine of those patients reported IBD-related reasons for choosing VC. The main reasons were concerns regarding heredity and insecurities about not being able to care for a child as result of their disease. Considering females only, the VC rate was 6.0%.
Generic disability and work disability
The mean IBD-DI score of 227 participants was 30.8 (±SD18.9). Of the patients that filled in the WPAI questionnaire, 70,5% (160/227) were employed. Overall mean values of absenteeism, presenteeism and overall work productivity loss were 8.1%, 18.1% and 20.4%, respectively.
Discussion
Our study shows that IBD has a large impact on household and family life, especially in the performance of household chores, participation in leisure activities, parenting and sexual activities. The way IBD influenced family planning in our population varied from concerns and doubts regarding pregnancy or parenthood, to the decision to have less or no children. Recently, with support of the European Crohn’s and Colitis Organisation, a list with criteria was constructed to shape quality of care standards for IBD. The proposed quality standard points include, among others, statements regarding the measurement of patients with IBD-related impairment of quality of life, social activities and working activities. Our research shows that functioning in the home environment is an essential part of the ability to engage in daily activities and should not be overlooked in this assessment.21
Fatigue was associated with the experience of more severe difficulties with domestic activities in the past week. This was underlined by free-text answers that patients provided to questions about difficulties in the performance of household tasks, grocery shopping and cooking. Although not statistically significant, clinical active disease showed a higher odds for experiencing more severe difficulties in domestic activities as well. Fatigue is an important clinical problem in patients with IBD, affecting over 40% of patients with quiescent disease and approximately 80% with active disease. The aetiology and pathophysiology of IBD-related fatigue remains unclear, which makes it difficult to effectively treat this disabling symptom.22 23 However, assessing active inflammation and optimising IBD therapy is an important and effective step in the management of fatigue.24
The relatively high percentage of moderate and severe disability in the performance of household tasks was reflected by the need for support. A third of the population needed help with their household chores because of IBD, while approximately 20% received this. Almost half of these patients stated that they received support from family or friends. As a results, a chronic unpredictable disease such as IBD can place a significant strain on the relationships between patients and their support system.25 26
Disturbingly, IBD interfered with the ability to carry out one or more parental duties in half of our population. Overall, available literature on parenting in IBD supports the findings of our study. In a cross-sectional Spanish study, 41% of the participants believed that UC affected their capacity to take care of children.11 A small exploratory qualitative study reported both positive and negative effects on parents. These parents faced problems in caring for their young children, especially when they experienced symptoms.10 A parenting questionnaire that is validated in patients with IBD is lacking, but the Parenting Disability Index (PDI) for rheumatoid arthritis (RA) patients is available. Parents with RA experienced difficulties in 41% of the parent–child activity domains during the development of the questionnaire.27 Approximately similar struggles have been described in studies focusing on parental disability in women with other immune mediated inflammatory diseases.28 Therefore, to gain more insight into parenting difficulties in IBD, a questionnaire as the PDI should be adapted to include IBD specific limitations.
One of the possible complex milestone decisions in life for patients with IBD is the planning of parenthood, or the choice not to care for children. Approximately a third of our total population, and 39% of the female participants, stated that IBD has had a negative influence on their desire to have or care for children. This is somewhat lower than two studies in German speaking and American patients, that both reported that approximately 46% of their IBD women felt that their disease impacted on family planning.12 16 In the 18–45 age range in the female part of our cohort, 6.0% considered themselves VC compared with 13%–19% of the women with IBD in the available literature.13 16 29 This relatively low percentage of VC can be a result of dedicated IBD-pregnancy counselling that is offered to patients in our tertiary care centre. This argument is supported by several studies that suggest that women receiving counselling have better IBD-related pregnancy knowledge and/or lower VC rates.30–33 Therefore, knowledge is key to enable patients to make informed decisions and it is important not to neglect men in this matter. To investigate pregnancy knowledge in the IBD population and assess the effect of the counselling programme in a future study, the validated Crohn’s and Colitis Pregnancy Knowledge questionnaire could be used.34
While it is difficult to accurately specify the overall burden of IBD on a patient’s life, we added to the whole picture with the findings of our study. The importance of the impact on household and family life was also represented by our high response rate of 74%. Nevertheless, this study has several limitations. As we evaluated limitations in functioning in the household in the past week, the total impact is probably underestimated. Another potential limitation is the household and family life questionnaire that was composed of items of the ICF, but not validated in a cohort of patients with IBD. In addition, due to relatively small sample size of subgroups we were not able to investigate the relationship between patient characteristics and all of the outcomes via a regression model. Finally, this study took place in a tertiary hospital centre, therefore, it is possible that our population does not truly reflect the overall IBD population.
Conclusion
The findings of our study show that IBD has a negative impact on numerous facets of household and family life, especially in the performance of household chores, participation in leisure activities, parenting, sexual activities and family planning. Fatigue was associated with the experience of more severe difficulties in domestic activities. More attention needs to be paid to functioning in the home environment to be able to quantify the full burden of the disease.
Footnotes
Contributors: Conception and design of the study: CJvdW, EP and DC. Acquisition of data: EP and DC. Analysis and interpretation of data: EP, DC, ACdV and CJvdW. Drafting article and revising it critically: EP, DC, CJvdW and ACdV. Final approval of the version: EP, DC, CJvdW and ACdV. All authors have made substantial contributions to the conception and design of the study, the acquisition of data, the analysis and interpretation of data or drafting the article or revising it critically for important intellectual content. All authors gave final approval of the version to be submitted. CJvdW is the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: CJvdW has served on advisory boards for Abbvie, Takeda, Pfizer and Celltrion. She is supported by research funding from ZonMW, Tramedico, and Pfizer. ACdV has participated in advisory board and/or received financial compensation from the following companies: Jansen, Takeda, Abbvie and Tramedico.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
All procedures were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethical approval was received by the Ethical Committee of the Erasmus MC (MEC-2020-0635).
References
- 1. Torres J, Mehandru S, Colombel J-F, et al. Crohn’s disease. Lancet 2017;389:1741–55. 10.1016/S0140-6736(16)31711-1 [DOI] [PubMed] [Google Scholar]
- 2. Ungaro R, Mehandru S, Allen PB, et al. Ulcerative colitis. Lancet 2017;389:1756–70. 10.1016/S0140-6736(16)32126-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Knowles SR, Graff LA, Wilding H, et al. Quality of life in inflammatory bowel disease: a systematic review and Meta-analyses-Part I. Inflamm Bowel Dis 2018;24:742–51. 10.1093/ibd/izx100 [DOI] [PubMed] [Google Scholar]
- 4. Organization. WH . International classification of functioning, disability and health : ICF.: World Health Organization, 2001. Available: https://apps.who.int/iris/handle/10665/42407
- 5. Paulides E, Daker C, Frampton C, et al. Overcoming workplace disability in IBD patients: an observational study. Inflamm Intest Dis 2020;5:84–92. 10.1159/000506702 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. van Gennep S, de Boer NKH, Gielen ME, et al. Impaired quality of working life in inflammatory bowel disease patients. Dig Dis Sci 2021;66:2916–24. 10.1007/s10620-020-06647-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. De Boer AGEM, Bennebroek Evertsz' F, Stokkers PC, et al. Employment status, difficulties at work and quality of life in inflammatory bowel disease patients. Eur J Gastroenterol Hepatol 2016;28:1130–6. 10.1097/MEG.0000000000000685 [DOI] [PubMed] [Google Scholar]
- 8. Argyriou K, Kapsoritakis A, Oikonomou K, et al. Disability in patients with inflammatory bowel disease: correlations with quality of life and patient's characteristics. Can J Gastroenterol Hepatol 2017;2017:1–11. 10.1155/2017/6138105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Israeli E, Graff LA, Clara I, et al. Low prevalence of disability among patients with inflammatory bowel diseases a decade after diagnosis. Clin Gastroenterol Hepatol 2014;12:1330–7. 10.1016/j.cgh.2013.12.009 [DOI] [PubMed] [Google Scholar]
- 10. Mukherjee S, Sloper P, Turnbull A. An insight into the experiences of parents with inflammatory bowel disease. J Adv Nurs 2002;37:355–63. 10.1046/j.1365-2648.2002.02098.x [DOI] [PubMed] [Google Scholar]
- 11. Calvet X, Argüelles-Arias F, López-Sanromán A, et al. Patients' perceptions of the impact of ulcerative colitis on social and professional life: results from the UC-LIFE survey of outpatient clinics in Spain. Patient Prefer Adherence 2018;12:1815–23. 10.2147/PPA.S175026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Walldorf J, Brunne S, Gittinger FS, et al. Family planning in inflammatory bowel disease: childlessness and disease-related concerns among female patients. Eur J Gastroenterol Hepatol 2018;30:310–5. 10.1097/MEG.0000000000001037 [DOI] [PubMed] [Google Scholar]
- 13. Selinger CP, Ghorayeb J, Madill A. What factors might drive voluntary childlessness (vc) in women with IBD? does IBD-specific pregnancy-related knowledge matter? J Crohns Colitis 2016;10:1151–8. 10.1093/ecco-jcc/jjw078 [DOI] [PubMed] [Google Scholar]
- 14. Mountifield R, Bampton P, Prosser R, et al. Fear and fertility in inflammatory bowel disease: a mismatch of perception and reality affects family planning decisions. Inflamm Bowel Dis 2009;15:720–5. 10.1002/ibd.20839 [DOI] [PubMed] [Google Scholar]
- 15. Organisation. WH . Nederlandse vertaling van de ‘International Classification of Functioning, Disability and Health’: World Health Organisation, 2001. Available: https://apps.who.int/iris/bitstream/handle/10665/42407/903133913X-dut.pdf?sequence=117&isAllowed=y
- 16. Marri SR, Ahn C, Buchman AL. Voluntary childlessness is increased in women with inflammatory bowel disease. Inflamm Bowel Dis 2007;13:591–9. 10.1002/ibd.20082 [DOI] [PubMed] [Google Scholar]
- 17. Gower-Rousseau C, Sarter H, Savoye G, et al. Validation of the inflammatory bowel disease disability index in a population-based cohort. Gut 2017;66:588–96. 10.1136/gutjnl-2015-310151 [DOI] [PubMed] [Google Scholar]
- 18. Paulides E, Kim C, Frampton C, et al. Validation of the inflammatory bowel disease disability index for self-report and development of an item-reduced version. J Gastroenterol Hepatol 2019;34:92–102. 10.1111/jgh.14496 [DOI] [PubMed] [Google Scholar]
- 19. Peyrin-Biroulet L, Cieza A, Sandborn WJ, et al. Development of the first disability index for inflammatory bowel disease based on the International classification of functioning, disability and health. Gut 2012;61:241–7. 10.1136/gutjnl-2011-300049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics 1993;4:353–65. 10.2165/00019053-199304050-00006 [DOI] [PubMed] [Google Scholar]
- 21. Fiorino G, Lytras T, Younge L, et al. Quality of Care Standards in Inflammatory Bowel Diseases: a European Crohn's and Colitis Organisation [ECCO] Position Paper. J Crohns Colitis 2020;14:1037–48. 10.1093/ecco-jcc/jjaa023 [DOI] [PubMed] [Google Scholar]
- 22. Borren NZ, van der Woude CJ, Ananthakrishnan AN. Fatigue in IBD: epidemiology, pathophysiology and management. Nat Rev Gastroenterol Hepatol 2019;16:247–59. 10.1038/s41575-018-0091-9 [DOI] [PubMed] [Google Scholar]
- 23. McGing JJ, Radford SJ, Francis ST, et al. Review article: the aetiology of fatigue in inflammatory bowel disease and potential therapeutic management strategies. Aliment Pharmacol Ther 2021;54:368–87. 10.1111/apt.16465 [DOI] [PubMed] [Google Scholar]
- 24. Kreijne JE, Lie MRKL, Vogelaar L, et al. Practical guideline for fatigue management in inflammatory bowel disease. J Crohns Colitis 2016;10:105–11. 10.1093/ecco-jcc/jjv168 [DOI] [PubMed] [Google Scholar]
- 25. Shukla R, Thakur E, Bradford A, et al. Caregiver burden in adults with inflammatory bowel disease. Clin Gastroenterol Hepatol 2018;16:7–15. 10.1016/j.cgh.2017.05.020 [DOI] [PubMed] [Google Scholar]
- 26. Zand A, Kim BJ, van Deen WK, et al. The effects of inflammatory bowel disease on caregivers: significant burden and loss of productivity. BMC Health Serv Res 2020;20:556. 10.1186/s12913-020-05425-w [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Katz PP, Pasch LA, Wong B. Development of an instrument to measure disability in parenting activity among women with rheumatoid arthritis. Arthritis Rheum 2003;48:935–43. 10.1002/art.10990 [DOI] [PubMed] [Google Scholar]
- 28. Poole JL, Rymek-Gmytrasiewicz M, Mendelson C, et al. Parenting: the forgotten role of women living with systemic lupus erythematosus. Clin Rheumatol 2012;31:995–1000. 10.1007/s10067-011-1929-5 [DOI] [PubMed] [Google Scholar]
- 29. Lee KE, Jung S-A, Yoon H, et al. Factors associated with pregnancy-related knowledge in women of reproductive age with inflammatory bowel disease. Scand J Gastroenterol 2017;52:833–9. 10.1080/00365521.2017.1310288 [DOI] [PubMed] [Google Scholar]
- 30. Laube R, Yau Y, Selinger CP, et al. Knowledge and attitudes towards pregnancy in females with inflammatory bowel disease: an international, multi-centre study. J Crohns Colitis 2020;14:1248–55. 10.1093/ecco-jcc/jjaa047 [DOI] [PubMed] [Google Scholar]
- 31. Flanagan EK, Richmond J, Thompson AJ, et al. Addressing pregnancy-related concerns in women with inflammatory bowel disease: insights from the patient's perspective. JGH Open 2021;5:28–33. 10.1002/jgh3.12442 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Huang VW, Chang H-J, Kroeker KI, et al. Does the level of reproductive knowledge specific to inflammatory bowel disease predict childlessness among women with inflammatory bowel disease? Can J Gastroenterol Hepatol 2015;29:95–103. 10.1155/2015/715354 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Carbery I, Ghorayeb J, Madill A, et al. Pregnancy and inflammatory bowel disease: do we provide enough patient education? A British study of 1324 women. World J Gastroenterol 2016;22:8219–25. 10.3748/wjg.v22.i36.8219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Selinger CP, Eaden J, Selby W, et al. Patients' knowledge of pregnancy-related issues in inflammatory bowel disease and validation of a novel assessment tool ('CCPKnow'). Aliment Pharmacol Ther 2012;36:57–63. 10.1111/j.1365-2036.2012.05130.x [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
flgastro-2021-102027supp002.pdf (21.5KB, pdf)
flgastro-2021-102027supp001.pdf (76.5KB, pdf)
Data Availability Statement
Data are available on reasonable request.